Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
|
|
|
- Annabel Woods
- 6 years ago
- Views:
Transcription
1 Tachycardias
2 Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
3 Initial Assessment Check Telemetry screen if pt on tele

4 Telemetry Strip
5 Initial Assessment Check Telemetry screen if pt on tele Vitals BP RR Oxygen Saturation Temperature EKG (maybe the nurse will do it for you)
6
7 Initial Assessment Check Telemetry screen if pt on tele Vitals EKG (maybe the nurse will do it for you) A-FIB: irregularly irregular with no P waves Look for evidence of ischemia (inferior or lateral ST- depressions) Symptoms: Chest Pain, SOB, Mental Status Exam: S3, JVD, Murmurs, Lung Crackles
8 Evaluation Stable or Unstable? Our patient: BP 105/65, RR 18, O2 sat 98% Symptomatic or Asymptomatic? Our patient: Palpitations, Dizziness Etiologies Prior A-fibA HTN CHF Valvular disease Post-surgical surgical Ischemia rare, more likely to be a consequence of afib Thyrotoxicosis - would likely have been identified on admission Stress - Hyperadrenergic state Hypokalemia/Hypomagnesemia
9 Treatment Stable Asymptomatic Pt Consider PO Lopressor or Diltiazem only Stable Symptomatic Pt Diltiazem start with mg IV over minutes, can give subsequent IV pushes q minutes (but recheck BP prior to 2 nd dose) Add PO can start with mg PO q6 Alternative: Lopressor 5 mg IV, can repeat every minutes (if BP okay) PO: mg PO q6
10 What if they are already on PO Diltiazem? Can still give IV push of Diltiazem but less likely to be effective Can give IV Lopressor and start PO Lopressor but careful with overaggressive AV nodal blockade bradycardia, heart block
11 Other Options Digoxin Onset of action in six hours so not ideal for symptomatic patient Load: 1 gram over 3 doses. Start with 0.5 mg IV and then 0.25 mg six and twelve hours later Half dose if pt with renal insufficiency (don t t use for advanced renal failure) Start PO dose (.125 mg) after load
12 Other Options Amiodarone Can cause hypotension but less than diltiazem or metoprolol Check to make sure your floor can do an amiodarone drip IV bolus: 150 mg Drip: 1.0 mg/min x 6 hours, 0.5 mg/min x 18 hours
13 Don t t Forget Repleting the electrolytes can t t hurt Pt needs to be on telemetry if not already Anticoagulation
14 Your patient is unstable DC Cardioversion: Start with J on biphasic defibrillators Can try successively higher shocks if unsuccessful If you have time, please sedate your pt Is there a CCU bed available?
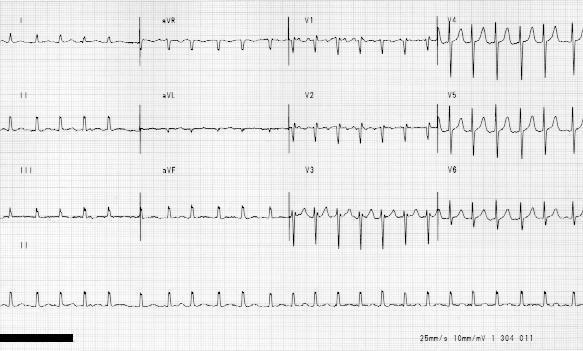
15 Case #2 66 y/o woman S/P Mitral Valve Repair admitted with pyelonephritis and borderline sepsis. Now tachycardic to 145. Other Vitals are stable EKG shows regular narrow complex tachycardia
16 Regular Narrow Complex Tachycardia What are the possible rhythms? Sinus Tachycardia
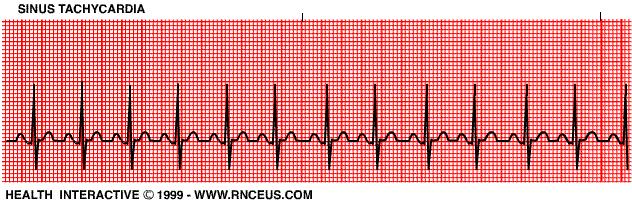
17 Sinus Tachycardia
18 Sinus Tachycardia Identify and treat the cause: Fever Pain Dehydration Bleeding Sepsis Iatrogenic: Albuterol Anxiety Don t t forget PE! Post cardiac transplant (loss of vagal enervation)
19 Regular Narrow Complex Tachycardia What are the possible rhythms? Sinus Tachycardia Atrial Flutter

20 Atrial Flutter

21 Sometimes it is less obvious Atrial Flutter with 2:1 AV block

22 Aflutter not always regular Atrial Flutter with variable conduction
 Anticoagulation usually")
23 Atrial Flutter Diagnosis Look for flutter waves Be suspicious if rate is near 150 If not sure, can use vagal maneuvers or 6 mg of IV Adenosine to slow AV conduction and reveal flutter waves Management Same as Atrial Fibrillation Can start cardioversion at 50J (don t t forget to sync) Anticoagulation usually needed
24 Regular Narrow Complex Tachycardia What are the possible rhythms? Sinus Tachycardia Atrial Flutter AVNRT AVRT
25 A review of reentry Mechanism of Reentry Bidirectional Conduction Unidirectional Block Recovery of Excitability & Reentry

26 AVNRT Reentry within AV node Rate usually P wave follows QRS complex
27 AVNRT - Treatment Stable Vagal maneuvers/carotid Massage Adenosine 6 mg IV followed by mg IV Need to flush immediately High rate of recurrence Rate control with centrally acting calcium channel blockers (Verapimil/Diltiazem) Replete electrolytes Unstable Synchronized cardioversion start with 50J

28 Termination of SVT by Vagotonic Maneuver (Carotid Sinus Massage)

29 AVRT Accessory Pathway with Ventricular Preexcitation (Wolff-Parkinson-White Syndrome) Orthodromic AV Reentrant Tachycardia Sinus beat AP Fusion activation of the ventricles Delta Wave PR <.12 s QRS.12 s Hybrid QRS shape Retrograde conduction via accessory pathway (AP) AP Anterogade conduction via normal pathway


30 AVRT Diagnosis Need to know about preexcitation on baseline EKG NSR with V Preex Orthodromic AV Reentrant Tachycardia Treatment No adenosine enhances conduction down accessory pathway Procainamide Ibutilide Cardioversion if unstable Time to call cardiology SVT: V Preex gone Note retrograde P waves in the ST segment
31 Last case 84 y/o man with COPD, transferred to floor after prolonged MICU course for pneumonia. Now HR in 130 s s and irregular
32
33 Multifocal Atrial Tachycardia 3+ p-wave p wave morphology Irregular rate Variable PR interval Usually seen in critically ill pts with pulmonary disease Treat pulmonary disease Correct electrolytes CCB if needed
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
MAT vs AFIB. Henry Clemo. Fast & Easy ECGs, 2E 2013 The McGraw-Hill Companies, Inc. All rights reserved.
 MAT vs AFIB Henry Clemo 1 Multifocal Atrial Tachycardia (MAT) > 3 P wave morphologies HR > 100 HR < 100 wandering pacemaker I 2 Multifocal Atrial Tachycardia 3 Multifocal Atrial Tachycardia 4 Multifocal
MAT vs AFIB Henry Clemo 1 Multifocal Atrial Tachycardia (MAT) > 3 P wave morphologies HR > 100 HR < 100 wandering pacemaker I 2 Multifocal Atrial Tachycardia 3 Multifocal Atrial Tachycardia 4 Multifocal
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Ablation Update and Case Studies. Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group
 Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017
 Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017 Normal EKG EKG boxes Heart Rate 1 big box = 200ms 1 small box = 40ms Big Boxes Between QRS complexes Heart
Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017 Normal EKG EKG boxes Heart Rate 1 big box = 200ms 1 small box = 40ms Big Boxes Between QRS complexes Heart
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Acute Arrhythmias in the Hospitalized Patient
 Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Atrial Fibrillation is Common. The (S)Low-down on Rapid Afib Resuscitation Step ED Dx - Rx 4/4/2017. There Are 5 Causes of Atrial Fibrillation
Low-down on Rapid Afib Resuscitation Step ED Dx - Rx 4/4/2017. There Are 5 Causes of Atrial Fibrillation") The (S)Low-down on Rapid Afib Resuscitation 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial Fibrillation
The (S)Low-down on Rapid Afib Resuscitation 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial Fibrillation
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
Episode 112 Tachydysrhythmias
 Wide & regular tachydysrhythmias Ventricular Tachycardia (VT) vs SVT with aberrancy: Assume VT Episode 112 Tachydysrhythmias With Amal Mattu & Paul Dorion Prepared by Shaun Mehta, July 2018 General Approach
Wide & regular tachydysrhythmias Ventricular Tachycardia (VT) vs SVT with aberrancy: Assume VT Episode 112 Tachydysrhythmias With Amal Mattu & Paul Dorion Prepared by Shaun Mehta, July 2018 General Approach
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
Don t Forget the Basics
 Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
3. AV Block 1. First-degree AV block 1. Delay in AV node 2. Long PR interval 3. QRS complex follows each P wave 4. Benign, no tx
 1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
EKG Rhythm Interpretation Exam
 as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
ECG Workshop. Jared W Magnani, MD, MSc University of Pittsburgh UPMC Heart and Vascular Institute Pittsburgh, PA March 24, 2017
 ECG Workshop Jared W Magnani, MD, MSc University of Pittsburgh UPMC Heart and Vascular Institute Pittsburgh, PA March 24, 2017 Overview and Objectives Review a differential for supraventricular tachycardia
ECG Workshop Jared W Magnani, MD, MSc University of Pittsburgh UPMC Heart and Vascular Institute Pittsburgh, PA March 24, 2017 Overview and Objectives Review a differential for supraventricular tachycardia
Sustained tachycardia with wide QRS
 Sustained tachycardia with wide QRS Courtesy from Prof. Antonio Américo Friedmann. Electrocardiology Service of University of Faculty of São Paulo. Opinions from colleagues Greetings to everyone, In a
Sustained tachycardia with wide QRS Courtesy from Prof. Antonio Américo Friedmann. Electrocardiology Service of University of Faculty of São Paulo. Opinions from colleagues Greetings to everyone, In a
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016
 CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016 + OBJECTIVES Diagnosis and management of ACS When to liaise with tertiary centre Complications of ACS Tachyarrhythmias Bradyarrhythmias
CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016 + OBJECTIVES Diagnosis and management of ACS When to liaise with tertiary centre Complications of ACS Tachyarrhythmias Bradyarrhythmias
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION
 RECERTIFICATION EXAMINATION") ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
Arrhythmias (I) Supraventricular Tachycardias. Disclosures
 Supraventricular Tachycardias. Disclosures") Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Arrhythmias. A/Prof Drew Richardson. The Canberra Hospital May MB BS (Hons) FACEM Grad CertHE MD
 FACEM Grad CertHE MD") Arrhythmias A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Recognise the features of the common nonlethal arrhythmias Describe the emergency treatment
Arrhythmias A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Recognise the features of the common nonlethal arrhythmias Describe the emergency treatment
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
the ECG, 6 mg of intravenous adenosine was administered as a fast bolus through a large bore intravenous cannula in
 (arrows). Electrocardiography Series Singapore Med.1 2011, 52(3) 146 CME Article Regular narrow complex tachycardia Singh D, Teo S G, Poh K K V Hr JL1 11 VL VF WA, Fig. I ECG shows regular narrow complex
(arrows). Electrocardiography Series Singapore Med.1 2011, 52(3) 146 CME Article Regular narrow complex tachycardia Singh D, Teo S G, Poh K K V Hr JL1 11 VL VF WA, Fig. I ECG shows regular narrow complex
WPW syndrome and AVRT
 WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
a lecture series by SWESEMJR
 Arrhythmias Automaticity- the ability to depolarize spontaneously. Pacemakers: Sinoatrial node: 70 bpm AV-nodal area: 40 bpm His-Purkinje: 20-40 bpm it Mechanisms of arrhythmias 1. Increased automaticity
Arrhythmias Automaticity- the ability to depolarize spontaneously. Pacemakers: Sinoatrial node: 70 bpm AV-nodal area: 40 bpm His-Purkinje: 20-40 bpm it Mechanisms of arrhythmias 1. Increased automaticity
Arrhythmia 341. Ahmad Hersi Professor of Cardiology KSU
 Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
How To Think About Rhythms and Conduction
 How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
ECGs on the acute admission ward. - Cardiology Update -
 ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Paramedic Rounds. Tachyarrhythmia's. Sean Sutton Dallas Wood
 Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
ACLS Study Guide for Precourse Self-Assessment
 20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Atrial Fibrillation Topics for Today. Clinical Controversies Management of Atrial Fibrillation. Atrial Fibrillation in the ER Topics for Today
 Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Blood pressure parameters for iv amiodarone
 Blood pressure parameters for iv amiodarone Search 17-7-2012 ICU & Fluids - Electrolytes - Nutrition: Edited by Andy S. Binder, MD, Pulmonologist, Critical Care. Contents: Electrolytes : Fluids: Dehydration.
Blood pressure parameters for iv amiodarone Search 17-7-2012 ICU & Fluids - Electrolytes - Nutrition: Edited by Andy S. Binder, MD, Pulmonologist, Critical Care. Contents: Electrolytes : Fluids: Dehydration.
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
COMMON ARRHYTHMIAS Diagnosis and Therapy
 COMMON ARRHYTHMIAS Diagnosis and Therapy Zachary D. Goldberger, MD, FACC, FHRS Assistant Professor of Medicine Division of Cardiology UW School of Medicine Harborview Medical Center FINANCIAL OR OTHER
COMMON ARRHYTHMIAS Diagnosis and Therapy Zachary D. Goldberger, MD, FACC, FHRS Assistant Professor of Medicine Division of Cardiology UW School of Medicine Harborview Medical Center FINANCIAL OR OTHER
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
ECG interpretation basics
 ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
Atrial Fibrillation. Epidemiology. Goals 11/12/2012. Faithful marker for age and underlying cardiopulmonary disease
 Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Evaluation and Initial Treatment of Supraventricular Tachycardia
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e clinical practice Evaluation and Initial Treatment of Supraventricular Tachycardia Mark S. Link, M.D. This Journal feature begins with a case vignette
T h e n e w e ngl a nd j o u r na l o f m e dic i n e clinical practice Evaluation and Initial Treatment of Supraventricular Tachycardia Mark S. Link, M.D. This Journal feature begins with a case vignette
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
VanderbiltEM.com. Atrial Fibrillation Update Don t Miss a Beat ACEP AFib. 20 Facts on Atrial Fibrillation in 20 minutes
 Atrial Fibrillation Update Don t Miss a Beat ACEP 2015 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Atrial Fibrillation Update Don t Miss a Beat ACEP 2015 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Pediatrics. Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment. Overview
 Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
WOLFF PARKINSON WHITE SYNDROME. Katarzyna Bigaj PGY-1
 WOLFF PARKINSON WHITE SYNDROME Katarzyna Bigaj PGY-1 Preexcitation is defined as a premature activation of the ventricular myocardium by an impulse that travels by an anomalous path and avoids physiologic
WOLFF PARKINSON WHITE SYNDROME Katarzyna Bigaj PGY-1 Preexcitation is defined as a premature activation of the ventricular myocardium by an impulse that travels by an anomalous path and avoids physiologic
ANTI-ARRHYTHMICS AND WARFARIN. Dr Nithish Jayakumar
 ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
Atrial Fibrillation is Common. ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat. Incidence of Atrial Fibrillation by Age
 ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial
ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial
Cardiology III 1/22/2019. Disclosures - none. But first. Objectives. Ischemia EKG s. And second
 Disclosures - none Cardiology III Matthew K Hysell, MD Spectrum Health Lakeland St Joseph, MI 1 2 Objectives Review specific high-yield EKG patterns Ischemia Ischemia mimics Electrolytes Review Cardiac/CV
Disclosures - none Cardiology III Matthew K Hysell, MD Spectrum Health Lakeland St Joseph, MI 1 2 Objectives Review specific high-yield EKG patterns Ischemia Ischemia mimics Electrolytes Review Cardiac/CV
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Making Sense of Those Little Lines Advanced ECG Interpretation
 Making Sense of Those Little Lines Advanced ECG Interpretation Cara Solodky-Hardy, ND, ANP-BC, AACC MD24 House Call Cardiology My patients www.ecglibrary.com Image Sources The Alan E. Lindsay Ecg Learning
Making Sense of Those Little Lines Advanced ECG Interpretation Cara Solodky-Hardy, ND, ANP-BC, AACC MD24 House Call Cardiology My patients www.ecglibrary.com Image Sources The Alan E. Lindsay Ecg Learning
Chapter 03: Sinus Mechanisms Test Bank MULTIPLE CHOICE
 Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
, David Stultz, MD.
 http://www.dilbert.com EKG Rounds Handouts available at http://www.drstultz.com January 5, 2004 David Stultz, MD Cardiology Fellow, PGY 4 Overview of Topics How to read an EKG Normal EKG Determination
http://www.dilbert.com EKG Rounds Handouts available at http://www.drstultz.com January 5, 2004 David Stultz, MD Cardiology Fellow, PGY 4 Overview of Topics How to read an EKG Normal EKG Determination
SHOCK THE PATIENT. Disclosures. Goals of the Talk. Tachyarrhythmias- Unstable 11/7/2017
 Disclosures Common Heart Rhythms in the Hospital Research Support: NIH, PCORI, Medtronic, Cardiogram Consulting: InCarda, Johnson & Johnson, Lifewatch Equity: InCarda Gregory M Marcus, MD, MAS Associate
Disclosures Common Heart Rhythms in the Hospital Research Support: NIH, PCORI, Medtronic, Cardiogram Consulting: InCarda, Johnson & Johnson, Lifewatch Equity: InCarda Gregory M Marcus, MD, MAS Associate
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Who Needs Admission and Who can go home?
 Who Needs Admission and Who can go home? Where is the presentation (clinic or ER)? Time of onset/duration Can symptoms be relieved? Stroke risk reduction Can adequate heart rate control be achieved? Is
Who Needs Admission and Who can go home? Where is the presentation (clinic or ER)? Time of onset/duration Can symptoms be relieved? Stroke risk reduction Can adequate heart rate control be achieved? Is
Update on Palpitations and AF February 28 th 2018
 Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,