ACT AMBULANCE SERVICE
|
|
|
- Kristian Osborne Burns
- 6 years ago
- Views:
Transcription

1 ACT AMBULANCE SERVICE CLINICAL MANAGEMENT MANUAL POCKET EDITION 1
2 CLINICAL MANAGEMENT GUIDELINES Contents PAGE NO. Glasgow Coma Scale 1 ACTAS Approved Abbreviations 2 Clinical Management Guideline Index 5 Failed Intubation Drill procedure 55 Rapid Sequence Induction Procedure 56 Drugs for Airway Management Summary Sheet 60 ACTAS Pharmacology Index 61 Drug Dose Calculator 101 Medication Calculator 102 Drug Reference Key List 104 Patient Assessment General Approach 115 Time Critical Patient Guideline 116 Suicide Risk Assessment 118 Mental Health Status Assessment 119 Mental Competency Checklist 120 APGAR Score 121 Paediatric Reference Card 122 PEEP Values 123 Spinal Immobilisation flow chart 124 Spinal Cord Injury 125 Differentiation of Wide Complex Tachycardias 126 Maximum QT Interval Chart Lead ECG Placement Chart Lead ECG Placement Chart 130 STEMI Bypass Flow chart 131 STEMI Bypass Check List 132 Acute Myocardial Infarction Table 133 Infarction Overview 134 Capnography 144 2
3 Wave Forms 146 Respiratory Status Assessment Chart 147 Burns Assessment Chart / Rule of Nines 148 Paediatric Burns Assessment Chart 149 Normal Blood Values 150 External Pacing procedure 151 Significant Contact Numbers 152 Motorola XTS 3000 Portable Radio - Duress Alarm Procedure 155 Hazchem Chart 157 Mass Casualty Triage Flow Chart 159 Ambulance Roles at a Mass Casualty Incident (MCI) 160 3
4 GLASGOW COMA SCALE EYE OPENING INFANT CHILD ADULT Spontaneous To speech To pain Nil Spontaneous To command To pain Nil Spontaneous To command To pain Nil BEST MOTOR RESPONSE INFANT CHILD ADULT Spontaneous Withdraws from touch Withdraws from pain Flexion Extension No response Obeys commands Localises Withdraws from pain Flexion Extension No response Obeys commands Localises Withdraws from pain Flexion Extension No response BEST VERBAL RESPONSE INFANT CHILD ADULT Coos, babbles, smiles Irritable, crying Cries, screams to pain Moans, grunts No response Orientated Confused Inappropriate words Incomprehensible No response Orientated Confused Inappropriate words Incomprehensible No response
5 ACT Ambulance Service Approved Abbreviations Only standard street name abbreviations, those listed below and on the Patient Care Record, in the context defined, are permitted for use. # fracture & and +, ++, +++ to an increased degree < less than = equal to > greater than female male increasing(ly) decreasing(ly), continuing disease n/24 hours n/7 days n/52 weeks n/12 months x (n) number of times Y/O years old /c /s 1 HB 2 HB 3 HB A ACTAS ACTSES ACTFB AFP AAA AF AFl ALS am AMI ANR with without first degree heart block second degree heart block third degree heart block asystole A.C.T. Ambulance Service A.C.T. State Emergency Service A.C.T. Fire Brigade Australian Federal Police abdominal aortic aneurism atrial fibrillation atrial flutter Advanced Life Support morning acute myocardial infarction Ambulance not required 2 BBB b.d. BGL BLS BNO BO BP BSL C/O Ca CABG CAL Calv. CAT CCF CCU cm CNS CO CO 2 Code 5 CP CPAP CPR CSF CVA DCCS Dr. Dx bundle branch block twice a day blood glucose level Basic Life Support bowels not open bowels open blood pressure blood sugar level complains(ing) of Cancer coronary artery bypass graft Chronic Airflow Limitation (Chronic Obstructive Airways Disease COAD; Chronic Obstructive Pulmonary Disease - COPD) Calvary Hospital Computerised Axial Tomography congestive cardiac failure Coronary Care Unit centimetres central nervous system Carbon Monoxide Carbon Dioxide person deceased chest pain continuous positive airways pressure Cardio-Pulmonary Resuscitation cerebrospinal fluid cerebrovascular accident Direct Current Counter Shock doctor diagnosis
6 EAR ECC ECG ED EDC EEG EMD ENT ESA ETT GCS GI GP Gx Px Hb HR H/T Hx ICP ICS ICU IGT IH IM IMI Inh. IO IPPV IU IV IVU IVR expired air resuscitation external cardiac compressions electrocardiograph Emergency Department (Accident and Emergency department) expected date of confinement electroencephalograph electromechanical dissociation Ear, Nose and Throat Emergency Services Agency endotracheal tube Glasgow Coma Score gastrointestinal general practitioner gravida No. para No. haemoglobin heart rate hypertension history intracranial pressure intercostal space Intensive Care Unit intragastric tube ischaemic heart disease intramuscular intramuscular injection inhaled intraosseous intermittent positive pressure ventilation International Unit intravenous intravenous unsuccessful idioventricular rhythm (L) Lev.OC LLQ LMP LOC lpm L LUQ LVF m mane MAP mcg mg ml mm mmol MRI MS mth MVA neb NFR NGT NICU NKA N o. nocte NOF N/S O O/A obs O/E O 2 left level of consciousness left lower quadrant last menstrual period loss of consciousness litres per minute litre left upper quadrant left ventricular failure metre morning mean arterial pressure microgram milligram millilitres millimetres millimol Magnetic Resonance Imaging Multiple Sclerosis month motor vehicle accident nebule / nebulised not for resuscitation nasogastric tube Neonatal Intensive Care Unit no known allergies number night neck of femur Normal Saline oral on arrival observations on examination Oxygen JR JVP junctional rhythm jugular venous pressure KED KTD kg km kph Kendrick Extrication Device Kendrick Traction Device kilogram kilometre kilometres per hour 3
7 P PA PAC PEA PEARL PEEP PHx PID PJC pulse per axilla premature atrial contraction pulseless electrical activity pupils equal & reacting to light positive end expiratory pressure past history pelvic inflammatory disease premature junctional contraction URTI UTI V/S VEB VF VT wt upper respiratory tract infection urinary tract infection vital signs ventricular ectopic beat ventricular fibrillation ventricular tachycardia weight pm PO PR prn pt PU PV PVC afternoon per oral per rectum as required patient passed urine per vagina premature ventricular contraction Q.I.D. 4 x times daily (R) RICE RLQ ROM RSI RTA RTC RUQ Rx right rest, ice, compression & elevation right lower quadrant range of movement rapid sequence induction road traffic accident road traffic crash right upper quadrant treatment S/C S/L SB SOB speep SR ST SVT subcutaneous sublingual sinus bradycardia shortness of breath spontaneous PEEP sinus rhythm sinus tachycardia supraventricular tachycardia T or Temp TCH tds TKVO TMC TNR Tx temperature The Canberra Hospital three times a day to keep vein open threatened miscarriage transport not required transport 4
8 Clinical Management Guideline Index 01 General Care 02 Pain Management 03 Airway Management 04 Cardiac Arrest 05 Paediatric Cardiac Arrest 06 Cardiac Arrhythmias 07 Bradyarrhythmias 08 Tachycardias 09 Respiratory Distress 10 Diabetic Emergencies 11 Temperature Abnormalities 12 Upper Airway Obstruction 13 Abdominal Emergencies 14 Shock & Hypotension 15 Decreased Level of Consciousness 16 Chest Pain / Suspected ACS 17 Chest Injuries 18 Spinal Injuries 23 Stroke 24 Near Drowning 25 Diving Emergencies 26 Obstetrical & Gynaecological Emergencies 27 Hyperkalaemia 28 Home Dialysis Emergencies 29 Allergic & Anaphylactic Reactions 30 Crush Syndrome 31 Electric Shock 32 Assault 33 Behavioural & Psychiatric Emergencies 34 C.B.R. Incident 35 Poisoning, Envenomation & Overdose 36 Extended Care 37 Combative / Agitated Patients 38 Meningococcal Disease 39 Adult Agonal Trauma Patients 18a Autonomic Hyperreflexia 40 Bariatric Patients (in development) 19 Limb Injuries 20 Eye Injuries 21 Burns 41 Headache (in development) 42 Back Pain (in development) 43 Dehydration (in development) 22 Seizures 5
9 CLINICAL MANAGEMENT GUIDELINE 1 GENERAL CARE Primary survey Haemorrhage control Posture Oxygen therapy Monitor & assess as required: Vital signs ECG/12-15 Lead Blood glucose O 2 saturations Temperature EtCO 2 Specific observations & assessment as per patient condition Treatment as required: Cervical collar Bandaging Splinting Pelvic splint Temperature control Reassurance Cannulate IV fluids as per perfusion & hydration assessment Pain relief Antiemetic Notify and transport to nearest appropriate hospital. NOTE: T R A N S P O R T I S T R E A T M E N T! Identify time-critical patients Actual based on vital signs, pattern of injury; lack of response to treatment. Potential based on history; mechanism of injury. NOTE: time-critical applies to both trauma and medical cases. The following conditions warrant absolute minimum scene times and urgent transport to hospital: Cardiac arrest following penetrating trauma (reference: Agonal Trauma Guideline) Unrelieved upper airway obstruction Head injuries with significant deterioration in levels of consciousness Chest injuries with respiratory deterioration Internal blood loss sufficient to cause significant hypotension Heatstroke Cardiac arrest in advanced pregnancy (gestation > 20 / 52 ) Prolapsed umbilical cord, or complicated labour Continuing or worsening acute hypoxia, unresponsive to treatment Generalised seizures, unresponsive to treatment Carbon monoxide poisoning with decreased level of consciousness (List is not exclusive or exhaustive!) NOTE: time-critical does not just mean rapid transport! 6
10 CLINICAL MANAGEMENT GUIDELINE 2 PAIN MANAGEMENT General Care Guideline RELIEF OF PAIN & SUFFERING IS A PRIME GOAL OF AMBULANCE CARE Pain is what the patient says it is! Always offer pain relief to the patient Pain assessment (PQRST) Quantitate if possible (scale & description) Document on case sheet Basic care is fundamental to pharmacological management: Reassurance Posture Splinting Cooling of burns Occlusive dressings Control of temperature (especially the cold) Gentle handling If possible, pharmacology should be directed at the apparent underlying cause: GTN S/L for ischaemic chest pain. Methoxyflurane for mild to moderate pain; patients unable to have narcotics; management of labour; often best for paediatrics. Morphine Ischaemic chest pain and for all other pain unless contraindicated. Midazolam small doses may be added to analgesia for musculo-skeletal pain. Ketamine for pain management in selected patients. May be used with alternate small doses of Morphine. ISCHAEMIC CHEST PAIN; LIMB PAIN; BURNS: aim for abolition of pain UNDIAGNOSED CONDITIONS: aim for control of pain to a bearable level of discomfort 7
11 CLINICAL MANAGEMENT GUIDELINE 3 AIRWAY MANAGEMENT General Care Guideline THE PRIMARY GOALS OF AIRWAY MANAGEMENT ARE: OXYGENATION VENTILATION AIRWAY PROTECTION in this order of priority Start basic and work up. However, it is permissible to leap-frog steps if, in your clinical judgement, the patient s condition warrants this Basic airway manoeuvres posture, suction, oral airway, nasopharyngeal airway. Mild sedation to permit basic airway management (Midazolam). Cold endotracheal intubation. Rapid sequence induction: Suxamethonium / Midazolam*. ( NOTE: If the patient has already had Midazolam for sedation do not give a repeat dose with Suxamethonium; or give a smaller dose.) Morphine / Midazolam if no relaxants, in patients with no suspected acute intracranial pathology. Fall-back alternatives: Failed Intubation Drill: Digital oral ETT placement*; LMA*; Surgical airway* Remember the primary goals! These will determine how aggressive your approach needs to be. Always have a fall-back position. The end point is not necessarily placement of an endotracheal tube. If an ETT is placed, confirmation of correct placement & maintenance of placement is imperative. End Tidal CO 2 is to be used. Use cervical collar to assist in maintaining ETT/LMA position. There are to be multiple checks of ETT position, using multiple methods, by multiple people. 8
12 CLINICAL MANAGEMENT GUIDELINE 4 ADULT CARDIAC ARREST CPR IPPV 100% O 2 Monitor ECG (a) Ventricular Fibrillation/Tachycardia (b) Asystole (c) Pulseless Electrical Activity Precordial thump if monitored & witnessed Shock Cannulate Adrenaline 1mg Shock Amiodarone 300 mg IV Shock Adrenaline Shock Adrenaline Shock For refractory or persistent VF: consider MgSO 4 For Torsades: MgSO 4 as the 1 st drug; no Amiodarone In prolonged arrest consider Sodium Bicarbonate 0.5 mmol/kg Shock Decision to transport Intubate when sufficient assistance Adrenaline every 2 minutes during transport Shock between medications Check alternate leads / lead selector Cannulate Atropine 2mg + Adrenaline 1mg Adrenaline Adrenaline In prolonged arrest consider Sodium Bicarbonate 0.5 mmol/kg Adrenaline Adrenaline Decision to transport Intubate when sufficient assistance Adrenaline every 2 minutes during transport 9 Check aggressively for correctable causes: Profound hypovolaemia Tension pneumothorax Continuing profound hypoxia Acidosis / Hyperkalaemia Gas trapping Cannulate Atropine 2mg + Adrenaline 1mg Adrenaline Adrenaline In prolonged arrest consider Sodium Bicarbonate 0.5 mmol/kg Adrenaline Adrenaline Decision to transport Intubate when sufficient assistance Adrenaline every 2 minutes during transport
13 CLINICAL MANAGEMENT GUIDELINE 5 PAEDIATRIC CARDIAC ARREST CPR IPPV 100% O 2 Monitor ECG (a) Ventricular Fibrillation/Tachycardia (b) Asystole (c) Pulseless Electrical Activity Precordial thump if monitored & witnessed Shock 2 j/kg Cannulate / Intraosseous Adrenaline 0.01 mg/kg Shock 4 j/kg Amiodarone 5 mg/kg IV Shock 4 j/kg Adrenaline Shock 4 j/kg Adrenaline Shock 4 j/kg For Torsades: MgSO 4 as the 1 st drug; no Amiodarone In prolonged arrest consider Sodium Bicarbonate 0.5 mmol/kg Shock 4 j/kg Intubate when sufficient assistance Transport Adrenaline every 2 minutes during transport. Shock between medications. Check alternate leads Cannulate / Intraosseous Adrenaline 0.01 mg/kg If hypoxia is not the apparent cause of arrest: Normal Saline 20 ml/kg Adrenaline Adrenaline In prolonged arrest consider Sodium Bicarbonate 0.5 mmol/kg Adrenaline Adrenaline Intubate when sufficient assistance Transport Adrenaline every 2 minutes during transport. 10 Check for correctable causes: Cannulate / Intraosseous Adrenaline 0.01 mg/kg If hypoxia is not the apparent cause of arrest: Normal Saline 20 ml/kg Adrenaline Adrenaline In prolonged arrest consider Sodium Bicarbonate 0.5 mmol/kg Adrenaline Adrenaline Intubate when sufficient assistance Transport Adrenaline every 2 minutes during transport.
14 GENERAL RESUSCITATION CARE This page has been intentionally left blank insert to follow 11
15 CLINICAL MANAGEMENT GUIDELINE 6 CARDIAC ARRHYTHMIAS General Care Guideline (a) - PACs / PVCs (b) - Accelerated IVR (c) - Bizarre No specific treatment required Monitor rhythm & patient condition No specific treatment required Monitor rhythm & patient condition Rate & perfusion determines the type of treatment. Pulse is absent, with normal rate treat as for cardiac arrest (usually PEA) Rate less than 50, poor perfusion treat as for bradyarrhythmias. Rate greater than 150, regular, with wide QRS complexes, and patient is significantly compromised treat as for VT. Rate greater than 150, regular, with narrow QRS complexes, and patient is symptomatic treat as for SVT. If unable to decide which specific therapy is required general care; observe; prompt transport. 12
16 CLINICAL MANAGEMENT GUIDELINE 7 BRADYARRHYTHMIAS General Care Guideline Consider treatment if heart rate is less than 50 in adults NOTE: Hypotension is an important determinant of perfusion status with Bradyarrhythmias If poorly perfused or symptomatic: Atropine 0.01 mg/kg Check for signs of failure. If no LVF: Consider IV fluid 5 10 ml/kg, prior to 2 nd dose of Atropine Repeat Atropine x 1 as required If perfusion remains poor Adrenaline infusion: 1 mg in 1000 ml Normal Saline ( = 1mcg/ml) Titrate to response. (20dpm = 1ml/min = 1 mcg/min) Paediatric use a burette OR external pacing, especially post cardiac arrest, and sedation with Morphine and Midazolam as required 13
17 CLINICAL MANAGEMENT GUIDELINE 8 TACHYCARDIAS General Care Guideline (a) Narrow QRS Complex Consider: Sinus tachycardia; SVT; AF; AFl; MAT Use 12 lead ECG Valsalva x 2 If SVT: Adenosine 6 mg IV Adenosine 12 mg IV, if required If rapid AF or AFl, refer to treatment algorithm: Notify and prompt transport to nearest appropriate hospital. (b) Wide QRS Complex Consider: VT; SVT with aberrancy; rapid AF or AFl with aberrancy. Make differentiation: (12 lead ECG if time) If aberrant SVT, AF or AFl - treat as per 8(a) If rapid, symptomatic VT: Amiodarone 150 mg IV No pulse: Treat as VF cardiac arrest Torsades de Pointes: MgSO 4 IV instead of Amiodarone Notify and prompt transport to nearest appropriate hospital. IV Amiodarone given over 10 minutes via Springfusor (If the patient is extremely compromised and in VT, it may be given over 5 mins by slow IV injection Consider pharmacological treatment if heart rate is above 150 in adults or 170 in children. Consider IV fluids in all tachycardic patients if hypotensive, not in LVF & unresponsive to pharmacological management. Any rapid rhythm (over 200), in an unconscious patient with no pulse shock. Paediatric doses: Adenosine: 0.05 mg/kg; then 0.1 mg/kg Amiodarone: 5 mg/kg (to a total of 150 mg) continues over 14
18 CLINICAL MANAGEMENT GUIDELINE 8 (continued) TREATMENT ALGORITHM FOR RAPID ATRIAL FIBRILLATION OR FLUTTER General Care Guideline Establish diagnosis: ensure - Atrial fibrillation or flutter - rapid rate ( > 150 ) - recent onset (reliably < 24 hours) No significant compromise Hypotension Ischaemic chest pain Pulmonary Oedema Rapid AF or AFl apparently secondary to an acute cerebral event Observe Check for evidence of LVF If no LVF: treat with IV fluids, 5 10 mls/kg Treat chest pain as appropriate Treat pulmonary oedema as appropriate These patients will present with a decreased LOC, & may be hypotensive Check for evidence of LVF Do NOT use Amiodarone in these patients If LVF + hypotension: treat cautiously with Amiodarone Treat rapid rate with Amiodarone concurrently Treat rapid rate with Amiodarone concurrently If no LVF: treat hypotension with IV fluids, 5 10 mls/kg Do NOT use Amiodarone in these patients. NOTE: Monitor BP closely the combination of drug treatments for pulmonary oedema may cause hypotension. NOTE: Unconscious patients post cardiac arrest in rapid AF may be treated with Amiodarone unless otherwise contraindicated. Allow several minutes for rhythms to stabilise before administering Amiodarone. 15
19 (a) Bronchospasm CLINICAL MANAGEMENT GUIDELINE 9 RESPIRATORY DISTRESS General Care Guideline (b) Pulmonary oedema Mild to Moderate: Salbutamol and Ipratropium puffer with spacer initially Moderate to Severe: Nebulised Salbutamol + Ipratropium. Repeat Salbutamol as required. Add Ipratropium to every second dose as required. Significant hypoxia nebulise with 100% O 2 and PEEP. Hydrocortisone 200 mg IV / IM (Paed: 4 mg/kg to maximum of 200 mg) Severe to life-threatening: Adrenaline: Adult: 0.5 mg IM Paediatric: 0.01 mg/kg IM (to 50 kg) Repeat IM dose x 1 as required Adrenaline infusion: 1 mg in 1000 mls Normal Saline ( = 1mcg/ml) Titrate to response. ( 20dpm = 1ml/min = 1 mcg/min) Paediatric use burette If the patient is critically ill, slow IV, up to 0.01 mg/kg,no faster than 50mcg/minute Consider fluid bolus for patients with moderate to severe asthma. Notify and transport to nearest appropriate hospital. Assist ventilation with IPPV + 100% O 2 as required Add PEEP: 5cm (THIS IS IMPORTANT) Increase PEEP by 5 cm as required If LVF: Sit patient with legs dependent if possible Treat significant cardiac arrhythmias GTN S/L: May be repeated x 1 after 5 minutes Morphine: 0.05 mg/kg IV (especially if using PEEP and patient is distressed) dose may be repeated after 10 minutes,if patient remains in severe distress: Frusemide: On diuretics: 1 mg/kg IV Not on diuretics: 0.5 mg/kg IV If wheezing is present, do not give nebulised bronchodilators until after the first two doses of GTN If no IV, Frusemide may be given IM If symptoms persist, may give third dose of GTN Notify and transport to nearest appropriate hospital. NOTE: IV Adrenaline in anaphylaxis & asthma should be used very cautiously. If IPPV is required use a slow rate with slow, gentle lateral chest squeezes on exhalation. 16 continues over
20 CLINICAL MANAGEMENT GUIDELINE 9 (continued) RESPIRATORY DISTRESS General Care Guideline (c) Non specific respiratory distress (d) Hyperventilation due to anxiety. Assess the patient carefully Administer Salbutamol + Ipratropium Repeat Salbutamol - as required Add Ipratropium to every second dose - as required Significant hypoxia - nebulise with 100% O 2 PEEP Fully assess the patient for pathological causes of hyperventilation. NOTE: Anxiety may accompany an underlying pathological cause for hyperventilation. O 2 at low flow rate via Hudson mask Monitor SaO 2, ECG and check E t CO 2 Remove source of anxiety if possible Reassurance Notify and transport to nearest appropriate hospital. Notify and transport to nearest appropriate hospital. 17
21 CLINICAL MANAGEMENT GUIDELINE 10 DIABETIC EMERGENCIES General Care Guideline CHECK BLOOD GLUCOSE LEVEL: (a) BGL < 4 mmol/l If symptomatic: Oral glucose, if conscious & laryngeal reflexes intact. If decreased LOC: Glucose 10% up to 2.5 ml/kg IV (0.25 g/kg) Re-check BGL & LOC. Repeat Glucose dose if required. (b) BGL > 15 mmol/l Normal Saline 10 ml/kg IV over contact time If shocked & hypotensive: IV resuscitation Notify and transport to nearest appropriate hospital. Ensure oral intake of carbohydrate if patient is not transported. Glucagon IM, if no IV available: Patient wt > 20 kg: 1 IU Patient wt < 20 kg: 0.5 IU Notify and transport to nearest appropriate hospital. NOTE: Recovery may be slow if hypoglycaemia has been prolonged. 18
22 CLINICAL MANAGEMENT GUIDELINE 11 TEMPERATURE ABNORMALITIES General Care Guideline CHECK PATIENT S TEMPERATURE: (a) Heat abnormalities Minor heat syndromes: Normal or transient disturbances in LOC; sweating; core temp < approx 39 o C Heatstroke: Decreased LOC; no sweating; core temp > approx 39 o C Gentle cooling Cease exertion Move patient to cool location Oral rehydration: - allow small sips only Rapid cooling; aggressive as possible IV resuscitation; cool fluids if possible Treat significant arrhythmias Check BGL IV rehydration if: - nauseated &/or vomiting; - significant dehydration; - multiple patients. Aggressively manage seizures or shivering Notify and transport to nearest appropriate hospital. Notify and urgent transport to nearest appropriate hospital. 19
23 CLINICAL MANAGEMENT GUIDELINE 11 (continued) TEMPERATURE ABNORMALITIES General Care Guideline (b) Cold abnormalities Exposure: Normal LOC; shivering; core temp > approx 33.5 o C Hypothermia: Decreased LOC; no shivering; core temp < approx 33 o C More rapid warming is acceptable Warm oral fluids Gentle exercise if possible Handle patient gently Remove wet clothing if sheltered; dry patient off Wrap in warm blankets; then space blanket If IPPV do not hyperventilate If in VF: Shock Cardiac drugs if core temperature > 32 o C Do not cease resuscitation Notify and transport to nearest appropriate hospital. Notify and transport to nearest appropriate hospital. 20
24 CLINICAL MANAGEMENT GUIDELINE 12 UPPER AIRWAY OBSTRUCTION General Care Guideline (a) Foreign body PARTIAL OBSTRUCTION: Maximise Oxygen therapy Encourage coughing Prompt transport Minimum intervention COMPLETE OBSTRUCTION: Conscious patient: Four modified chest thrusts; if fails turn into lateral position. 4 back blows. if possible, position with head down to utilise gravity; if fails repeat the sequence x 2; if fails urgent transport 100% Oxygen Unconscious patient: Extricate foreign body with laryngoscope & Magill forceps; if fails supine position (for children, use head down position, if possible) 4 modified chest thrusts; if fails lateral position 4 back blows; if fails repeat sequence x 2; if fails attempt intubation to push foreign body into (R) or (L) main bronchus. (Insert tube as far as possible use uncut tube if possible). Notify hospital and urgent transport 100% Oxygen. Consider surgical airway as a last resort. OBSTRUCTION RELIEVED: provide Oxygen therapy prompt transport 21 (b) Swelling Causes: croup / epiglottitis; insect sting; anaphylaxis; trauma; oral / pharyngeal infection; burns. Maximise oxygenation Do not attempt close examination of mouth / throat area Do not unnecessarily distress the patient If severely obstructed: nebulised Adrenaline: wt > 10 kg 5 mls Adrenaline 1:1000 wt < 10kg 0.5 ml/kg Adrenaline 1:1000 (Make volume up to 5 mls with Saline, as required) If swelling is due to anaphylaxis or local insect sting: IV / IM Adrenaline For partial airway obstruction: prompt transport For complete airway obstruction: give 100% O 2 and attempt I.P.P.V. notify hospital and urgent transport. consider surgical airway as a last resort.
25 CLINICAL MANAGEMENT GUIDELINE 13 ABDOMINAL EMERGENCIES General Care Guideline Posture flat knees may be flexed. IV resuscitation as required. Pain relief. Cover any open wounds with dry, sterile dressing; protruding viscera with saline-moistened sterile dressings. If an impaled object is in situ do not remove it move the patient with the object in situ. Notify and prompt transport to nearest appropriate hospital. 22
26 CLINICAL MANAGEMENT GUIDELINE 14 SHOCK & HYPOTENSION General Care Guideline Assess the patient carefully to determine possible cause. Consider assessment of postural changes (a) Hypovolaemic (b) Cardiogenic (c) Distributive (d) Obstructive High concentration O 2 High concentration O 2 High concentration O 2 High concentration O 2 If severely shocked, with a non-compressible bleeding lesion early, rapid transport IV fluids to maintain adequate cerebral perfusion (consider age, co-morbidities & concurrent injuries) Consider pelvic splint where appropriate 12 lead ECG STEMI management as indicated Treat significant arrhythmias Pain relief Assess for LVF IV fluids with caution Adrenaline if suspected anaphylaxis Posture with care if suspected spinal injuries IV fluids (keep BP no higher than mmhg if spinal injuries are suspected) Decompress tension pneumothorax if suspected If severely shocked early, rapid transport IV fluids Notify and prompt transport to nearest appropriate hospital. Notify and prompt transport to nearest appropriate hospital. Notify and prompt transport to nearest appropriate hospital. Notify and prompt transport to nearest appropriate hospital. 23
27 (a) History of trauma Head Injury Cervical spine precautions Airway management guideline If GCS below 12: maintain O 2 saturations > 95% BP systolic (MAP > 90) Check BGL CLINICAL MANAGEMENT GUIDELINE 15 DECREASED LEVEL OF CONSCIOUSNESS General Care Guideline Assess the patient carefully (b) No history of trauma Check BGL Posture º head up Consider poisoning or O/D Consider cervical spine precautions Airway management guideline If GCS below 12: maintain O 2 saturations > 95% BP systolic (MAP > 90) (c) Apparent syncope Assess thoroughly for more significant causes in all patients Check BGL 12 lead ECG if no obvious alternate cause Posture by perfusion or comfort Consider cervical spine precautions Notify and transport to nearest appropriate hospital. Notify and transport to nearest appropriate hospital. Notify and transport to nearest appropriate hospital. Evidence of a rapidly decreasing level of consciousness is a flag for a time-critical patient therefore, minimise scene time and transport urgently to hospital. 24
28 CLINICAL MANAGEMENT GUIDELINE 16 CHEST PAIN / SUSPECTED ACUTE CORONARY SYNDROMES General Care Guideline Assess thoroughly for possible Acute Coronary Syndrome (ACS) i.e. 12 lead ECG if STEMI initiate appropriate management without delay. Possible Acute Coronary Syndrome Monitor closely 12 lead ECG (15 lead as appropriate) Aspirin GTN Antiemetic Morphine Pain management - aim to abolish pain or discomfort Notify hospital AS EARLY AS POSSIBLE if STEMI is suspected* Treat haemo-dynamically significant arrhythmias Prompt transport Pain assessed as probable non-acs Assess for possible threat to life. Utilise 12 lead ECG If in any doubt treat for ischaemic heart disease Otherwise manage as for undiagnosed pain Prompt transport Give Aspirin, even if on regular slow-release Aspirin. Give a 150mg dose if already on Warfarin. Watch for non-typical or silent presentations of ischaemic heart disease, especially in females, the elderly & patients with diabetes. Silent or atypical ACS presentations should be treated in the same manner as a typical presentation. Aim to minimise scene time while still providing reassurance & effective pain relief. *STEMI bypass procedure notification, Heparin and Prasugrel / Clopidogrel 25
29 IV resuscitation as required Pain relief as required CLINICAL MANAGEMENT GUIDELINE 17 CHEST INJURIES General Care Guideline Pneumothorax If suspected avoid coughing, Valsalva manoeuvres or IPPV Suspect a tension pneumothorax in a patient with diminished air entry & significant respiratory or cardiovascular compromise. Decompress tension as indicated NOTE: diminished air entry may be an unreliable sign if the patient is receiving positive pressure ventilation. Open chest wound Cover, seal on 3 sides only, or use chest seal Flail chest Stabilise the chest wall Posture patient with affected side down, or by manual pressure Effective pain relief Notify and transport to nearest appropriate hospital. 26
30 CLINICAL MANAGEMENT GUIDELINE 18 SPINAL INJURIES General Care Guideline Instruct the patient to refrain from moving his head avoid flexion of the neck and rotation of the head all other movements must be minimised maintain head in the neutral position Oxygen therapy 100% if suspected cord lesion IPPV, if hypoventilating Posture supine Cervical Collar Extricate with spine board or Kendrick Extrication Device Lift with board or scoop stretcher Do not routinely transport patients on the spine board/scoop stretcher. Transportation on a spine board/scoop stretcher is only permissible where there is a short extrication and travel time to hospital (no longer than 10 minutes). If this occurs, ensure that the patient and board are restrained during transport. IV resuscitation as required DO NOT OVER-INFUSE a systolic blood pressure of 80mmHg is acceptable in high spinal injuries With suspected cord lesion - administer antiemetic Insert IGT & urinary catheter prior to secondary, air or extended transports If transport is prolonged, ensure pressure area care is attended Notify and transport to nearest appropriate hospital. 27
31 CLINICAL MANAGEMENT GUIDELINE 18a AUTONOMIC HYPERREFLEXIA This occurs in established High Paraplegics or Quadriplegics, therefore, assess the patient for Autonomic Hyperreflexia. The sudden onset of any of the following is significant. Sudden hypertension, (this may fall within the normal limits for the rest of the population); pounding headache, bradycardia, flushing/blotching of skin; profuse sweating above level of lesion; skin pallor and piloerection below level of lesion; chills without fever; nasal congestion, blurred vision; shortness of breath, sense of apprehension and/or anxiety. Causes Bladder: Bowel: Skin: Other: Distended due to blocked or kinked catheter, UTI, bladder or kidney stones. Constipation, faecal impaction, rectal irritation. Burns, pressure areas, tight clothing e.g. TED stockings. Fractures, distended stomach, labour, severe menstrual cramping. Actions Ask patient and carer if they suspect a cause. Elevate patient s head and position with legs dependent, if possible. Loosen any constrictive clothing. Check bladder drainage equipment for kinks or obstruction: if found drain 500mls initially, then a further 250mls every 15 minutes until the bladder is empty. Monitor BP every 2 5 minutes. Avoid pressing over the bladder. Treatment If the BP remains elevated (ranging between mmHg), commence treatment with: IV Midazolam 0.05 mg/kg, over one minute. This may be repeated once after 10 minutes if there is no fall in BP. Give 0.1 mg/kg IM if unable to cannulate. Midazolam should be given with extreme caution while constantly monitoring the patient s vital signs. NOTE: Treatment with Midazolam mandates transport to hospital. Notify and transport to nearest appropriate hospital. 28
32 CLINICAL MANAGEMENT GUIDELINE 19 LIMB INJURIES General Care Guideline Check arterial circulation in the limb: If the distal pulse is absent gently re-align fractured segments until pulse returns or alignment is near normal. Immobilise all fractures unless the patient is otherwise time-critical. Elevate the limb, if possible. Do not attempt to reduce dislocations. IV resuscitation where indicated. Pain relief Midazolam as required. Ketamine as appropriate. Partially severed limb: carefully protect limb keep distal portion of limb dry, wrapped and cool. Completely severed limb: Keep severed part dry, wrapped and cold. Place in a dry sealed plastic bag, then place within another bag or bucket filled with iced water at approx 4 o C. DO NOT immerse the part directly in ice. DO NOT attempt to clean or disinfect the severed part. Notify and transport to nearest appropriate hospital. 29
33 CLINICAL MANAGEMENT GUIDELINE 20 EYE INJURIES General Care Guideline Trauma: ENSURE OXYGENATION Do not remove protruding foreign bodies. If the eyeball is extruded, do not push it back into the socket. If tolerated, transport the patient lying flat. The injured eye must be protected from rubbing pressure. Use an eye shield, or a loosely taped eye patch. Cover both eyes if the patient can tolerate this. Severe eye injuries - administer IV antiemetic prior to transport. Chemical Burns: Irrigate immediately with copious quantities of water or saline for at least ten minutes. The eyelids must be pulled apart to ensure the fluid washes completely over the eye. Scalds and Electrical Flash Burns: No dressing is required, ice packs can be beneficial. Foreign Bodies in Cornea: Protect the eye with a shield or pad. Do not attempt to remove the foreign body. Notify and transport to nearest appropriate hospital. 30
34 CLINICAL MANAGEMENT GUIDELINE 21 BURNS General Care Guideline If there is still heat left in the skin, cool with cold water or saline. Watch for development of hypothermia. Utilise watergel burns dressings after cooling. Check & replace if they become warm. Cover the burnt area with clean dressing/sheets. If a limb is burnt, remove all rings, tight clothing, shoes, and elevate the part. Consider space blanket. Check for potential upper airway obstruction, especially if the face is burnt. Hoarse voice Inspiratory stridor See-saw breathing Treat bronchospasm or airway obstruction via relevant management guideline. If decreased level of consciousness: Suspect Carbon Monoxide poisoning (especially if burnt in a confined space). Administer 100% O 2 ; with PEEP. Pain relief IM Ketamine, if no IV access is available. Cannulate Normal Saline for Adults with burn > 15% BSA; children > 10% BSA. (full or partial thickness) Adults: % BSA burned x wt (kg) in mls over 4 hours from time of burn. Children: 10 ml/kg. If upper airway involvement is present reduce fluids to ½ of what would otherwise be administered. Transport suspected smoke inhalation patients to hospital as delayed pulmonary oedema may occur. Notify and transport to nearest appropriate hospital. Prompt transport for any evidence of upper airway burns. 31
35 CLINICAL MANAGEMENT GUIDELINE 22 SEIZURES General Care Guideline Protect the patient from injury. Blood glucose estimation early, especially if no history of seizures. Midazolam (IM if no IV access). Treat any injuries secondary to the seizure. Pregnant patient, no history of previous seizure activity prompt treatment with 5mg MgSO 4. Children with seizure and or fever >38 C: Remove excessive clothing Cool with tepid water Place cool cloths in axillae, groin, wrist and neck; change as required Do not allow child to shiver Treat with Paracetamol 20 mg/kg or 15mg/kg if Paracetamol has been administered in the last 48 hours Notify and transport to nearest appropriate hospital. 32
36 CLINICAL MANAGEMENT GUIDELINE 23 STROKE General Care Guideline Posture o head up Airway management guideline Cannulate: - blood glucose estimation treat hypoglycaemia cautiously; avoid hyperglycaemia Treat seizures promptly & aggressively Minimise scene time Notify hospital early and promptly transport to nearest appropriate hospital. 33
37 CLINICAL MANAGEMENT GUIDELINE 24 NEAR DROWNING General Care Guideline Cardiac arrest - treat by specific guideline. Use the highest concentration of Oxygen practicable. PEEP, if possible Cervical collar as required. IGT if possible. Consider hypothermia/other related conditions. Notify and transport to nearest appropriate hospital. NOTE: Late pulmonary oedema may occur. * Transport is always required following near drowning episodes * CLINICAL MANAGEMENT GUIDELINE 25 DIVING EMERGENCIES General Care Guideline Consider the possibility of spinal injury. Lie flat and keep flat, do not sit up. If unconscious, assume the possibility of an air embolus - posture left lateral, with a head-down tilt. Oxygen therapy: highest concentration practicable. Exclude pneumothorax. Patients are always dehydrated re-hydrate with IV Normal Saline 10 ml/kg promptly. Ascertain dive profile (number and sequence of dives; time at depth; breathing mixtures; decompression stops and any uncontrolled ascent.) Remember to check dive partner. Monitor symptom progression. Pain relief analgesics may mask symptom changes; aim for minimal analgesia. 34
38 CLINICAL MANAGEMENT GUIDELINE 26 OBSTETRICAL & GYNAECOLOGICAL EMERGENCIES General Care Guideline Unscheduled Normal Field Birth The most important ambulance role in a field delivery is to appear calm! The preferred management is birth at a hospital but if birth is imminent, reassure the mother & help her to a comfortable position. Ensure full history Oxygen Pain relief as required Provide support and guidance during birth of baby s head while encouraging gentle grunty pushes or controlled breathing to ease the head out slowly and gently. As the head is born have your hand close to the top of the baby s head you do not need to touch it unless the woman gives an uncontrolled push and the baby would otherwise shoot out (especially important if the baby is preterm < 37 weeks). Observe for cord around the baby s neck. If present the baby may be born through the loop of cord. If the cord is loose, it may be slipped forward over the head, taking care not to stretch it or tear it. Rarely the cord is so tight that it stops the baby s descent and in this situation it may need to be clamped in two places and cut between the clamps. Great care is necessary not to injure the baby or woman while doing this. Place the baby straight up on to the mother s chest noting time of birth. Dry baby and maintain warmth by keeping the baby close to the mother s skin. Place warm blankets over the baby and mother. Assess the baby s Apgar score at 1 and 5 minutes after birth. Cord should not be routinely cut but, if necessary, apply plastic clamp (x2) at 3cm from the umbilicus, milk the cord gently back from the clamp 3cm, taking care not to pull on the umbilicus. Apply plastic clamp (x2) then cut the cord using clean scissors. continues over 35
39 Complicated Birth Prolapsed cord: Posture in the knee to chest position (often easier in the all fours knee to chest position) 100%Oxygen Advise hospital early Urgent transport Do not encourage pushing Breech presentation: Normal, unassisted birth may not always be possible. Where possible, do not encourage the woman to push but to breathe through her contractions. Notify and urgently transport to hospital. Once legs and body have been born, support the baby s body as it hangs downward while waiting for the gentle, slow birth of the head. (Do not apply downward traction). Encourage the mother to breathe her baby s head out. If head is not born with the next contraction, encourage her to push whilst gently supporting the baby as it hangs downward. Other presentations: Recognise! Normal, unassisted delivery may not always be possible. Notify and urgently transport to nearest appropriate hospital. P.V. Haemorrhage Not pregnant / early pregnancy: Manage as per perfusion status Advanced pregnancy Manage as per perfusion status Left lateral position Do not attempt to massage the fundus of the uterus Notify and prompt transport to nearest appropriate hospital Seizures due to eclampsia 5mg MgSO4 IV Cardiac arrest in advanced pregnancy Position with wedge under right hip to obtain o leftwards tilt. Give fluid bolus early. Urgent transport as soon as backup has arrived. If performing CPR, increase CPR compression force due to the chest wall compliance secondary to breast hypertrophy. Ensure hospital is notified as early as possible that the patient is pregnant. Women in more advanced pregnancy (approx 20+ weeks gestation) are generally best treated/transported in the left lateral position, regardless of the problem. 36
40 CLINICAL MANAGEMENT GUIDELINE 27 HYPERKALAEMIA General Care Guideline Consider in these situations: Renal failure/dialysis Crush syndrome, including situations of prolonged unconsciousness Occasionally diabetic ketoacidosis ECG signs are unreliable, frequently do not follow expected progressions, and do not always show good correlation with serum K + levels. Monitor the ECG for signs of hyperkalaemia, which may include: Tall peaked T waves No P waves Wide QRS Sine wave pattern (VT) VF / Asystole Arrhythmias, especially bradycardias, are common. If ECG changes are present: Nebulised Salbutamol (continuously). Calcium Chloride 10 mg/kg IV over 2 minutes. Follow with: Sodium Bicarbonate 8.4% 0.5 mmol/kg IV over 2 minutes. If ECG changes persist after minutes: repeat Calcium Chloride & Sodium Bicarbonate x 1 NOTE: Treatment is determined by patient presentation, ECG changes and the clinical setting. 37
41 CLINICAL MANAGEMENT GUIDELINE 28 HOME DIALYSIS EMERGENCIES Dialysis is a Renal Replacement Therapy used when kidney function no longer sustains life. The client is required to undergo treatment on a regular basis (typically 3 times per week for 4 hours). SOME IMPORTANT CONSIDERATIONS: Clients who are dialysed at home have undergone extensive training and maintain a record of their treatment. Use this and any further information provided by the patient and/or carer they are very familiar with the process. Fistula access is the patient s life line. Vessels should be preserved for future fistula creation therefore, ONLY cannulate if necessary and use the cubital fossa or hand. Most calls to dialysis clients are not related to their dialysis. REMOVE CLIENT FROM MACHINE BY: Clamping machine blood lines (x2) and cannula (x2) Unscrew lines from cannula. (Pump will stop and machine will alarm) Do not turn machine off until client is removed Use either cannula as access for fluid and medications (as both are sitting in an arterialised vein) Attach giving set to cannula and administer IV fluid. Remember clients are often on fluid restriction mls often resolves a hypotensive situation. Consult the client s treatment record to ascertain usual BP Leave cannula in situ if time is an issue. However, reinforce with taping and protect during transit, as these are metal needles and can cause damage to the vessels if mishandled When removing cannulae, remember there is a high flow-in access (1000 mls/minute) so use a protective mask and goggles. Moderate pressure is needed on the exit site for minutes 38 continues over
42 CALLS TO CLIENTS ON DIALYSIS. Problems include: 1. Hypotensive episode: This can occur due to excess fluid removal. Assess the situation. If the client/helper can replace fluid, this is the best option. When the Paramedic is required to replace fluid: Place the client in the Trendelenberg position (supine with head lower than feet). Administer O 2 Remove client from machine Follow ACTAS Clinical Management Guideline for fluid replacement 2. Chest pain: This may be caused by excess fluid removal during dialysis or other cardiac event. Stop dialysis and ask helper to return client s blood or remove client as above when necessary Use cannula as access. Withdraw 10mls of blood and discard before using cannula for blood-taking (to remove saline in the line) Follow ACTAS Clinical Management Guideline for chest pain 3. Bleeding: This may occur due to excess thinning of the blood due to Heparin used in dialysis. Heparin has half life of 92 minutes. Only light pressure on cannula site is required (10 15 minutes) DO NOT cut off the flow-in access as it will clot Use Diastop/Tip stop devices where available. Digital pressure is the best option DO NOT APPLY TIGHT BANDAGES continues over 39
43 4. Venous air embolism: Suspected if there is air in the venous return line. Stop treatment (stop machine by opening pump door) Treat with 100% Oxygen; posture in the left lateral position with a 30 o head down tilt. Remove client from machine as above 5. Haemolysis: Caused by damage to the blood cells due to an inappropriate dialysate (overheating, toxins such as Copper, Chloramines, bleach, Formaldehyde). Signs & Symptoms chest pain/back pain dyspnoea localised burning and pain in access return site the blood turns a characteristic port wine colour Treatment stop dialysis. disconnect client. give O 2 if indicated. check for arrhythmias, fluid volume replacement if indicated. Reference: Molzahn, A. E (2006) Contemporary Nephrology Nursing Principles and Practice. American Nephrology Nurses Association. New Jersey 40
44 CLINICAL MANAGEMENT GUIDELINE 29 ALLERGIC & ANAPHYLACTIC REACTIONS General Care Guideline Pressure immobilisation bandage / splint over the area of injection, sting or bite if appropriate. Adrenaline is the drug of choice for cases where there are potentially life-threatening signs (hypotension; upper airway swelling; bronchospasm unresponsive to nebulised bronchodilators) Consider the use of IM Adrenaline in the first instance IV use should be with caution If IV use is considered, a diluted infusion is the preferred method of administration. Manage, as appropriate, using ACTAS guidelines for respiratory distress; shock & hypotension; upper airway obstruction. The fundamental principles are: O 2 therapy; Adrenaline; IV fluids * CLINICAL MANAGEMENT GUIDELINE 30 CRUSH SYNDROME General Care Guideline This is rarely a problem with less than 45 minutes of compression of a significant muscle mass. Acute volume loss on release is generally considered of greater clinical importance than hyperkalemia and acidosis. Immediately prior to removal of the compressive force: consider the use of an arterial tourniquet to the compressed limb increase IV infusion rate observe ECG Following the removal of the compressive force: release the tourniquets carefully; check for ECG changes. Manage, as appropriate, using ACTAS guidelines for shock & hypotension, hyperkalaemia, and limb injuries. 41
45 CLINICAL MANAGEMENT GUIDELINE 31 ELECTRIC SHOCK General Care Guideline DO NOT BECOME A VICTIM YOURSELF! LOW VOLTAGE (<1000 Volts) - Appliance in house or main supply to house - pull out plug; pull conductor away from patient; pull patient clear; switch off at mains. METHOD: grasp clothes if dry; avoid contact with skin or conductor; use dry fibre rope or dry blankets or similar non-conducting material. HIGH VOLTAGE (>1000 Volts) Request assistance from Electricity Authority. Use short steps to approach a victim. Retreat immediately if tingling is felt. High Voltage consider possible spinal injury. Check for exit burns. Treat other injuries as required. Electrical burns usually cause greater tissue damage than the appearance of the skin surface would suggest. Therefore, always transport the patient to hospital. 42
46 CLINICAL MANAGEMENT GUIDELINE 32 ASSAULT General Care Guideline Be aware of risks to yourself & others. Ensure scene control & safety. Attention to detail (such as full name, location, times; others present) is very important. Treat injuries where indicated. Specifically for sexual assault: Be aware some patients may resent physical contact from carers; Avoid any judgemental comments; Articles of evidence, such as clothing must be taken with the patient (use a paper bag); Discourage the patient from showering; The patient should not be left alone at any time; Do not give details of the assault over the radio. 43
47 CLINICAL MANAGEMENT GUIDELINE 33 BEHAVIOURAL & PSYCHIATRIC EMERGENCIES General Care Guideline Identify yourself clearly. If concerned about your safety, or others, call for police assistance. Be reassuring and non-judgemental when conversing with the patient. Speak quietly do not shout. One officer should talk privately with the patient where possible. Do not leave the patient alone. Consider / exclude: hypoxia hypoglycaemia head injury drug overdose post-ictal state Treat as appropriate. Consider use of CMG 37 Management of combative or agitated patients. Arrange for appropriate support services e.g. CAT Team. Notify and transport to nearest appropriate hospital. 44
48 CLINICAL MANAGEMENT GUIDELINE 34 C.B.R. INCIDENT General Care Guideline A CBR incident may be indicated by: - Physical indicators: e.g. unusual pools of liquid, clouds or fogs, unusual colours, strange devices or recent explosion. - Medical signs and symptoms or unusual behaviour being displayed by a number of people. - Dead birds or animals in the area. STEP 123 is Safety Trigger for Emergency Personnel : - one patient with cholinergic symptoms is suspicious, - two patients indicate a CBR, - three patients is a CBR. PROTECT YOURSELF; DO NOT ENTER THE CONTAMINATED AREA IF THIS CAN BE DETERMINED. If you find yourself in a contaminated area: cover your nose and mouth with a damp cloth; take frequent shallow breaths; don t Taste, Eat, Smell, or Touch anything in the area; seek shielding if radioactivity is present; leave the scene immediately and proceed to a safe upwind, uphill area; be aware of the possibility of secondary devices. continues over 45
49 CLINICAL MANAGEMENT GUIDELINE 34 (continued) C.B.R. INCIDENT Remain clear of the contaminated area (Designated HOT& WARM zones) unless authorised to enter by the Incident Commander. You must be equipped with appropriate personal protective equipment (PPE) and have suitable training in its use. Only authorised and trained personnel will operate in the HOT& WARM zones. To decontaminate: Remove clothing and discard into a special HAZMAT container; Skin must be cleaned by thorough washing or preferably showering; Pay special attention to hair and parts of the body with opposing skin surfaces, e.g. the buttocks. It is preferred that patients and personnel be decontaminated PRIOR to treatment. Initial antidote can be administered prior to decontamination by suitably protected personnel. Treatment: Assist ventilation (only if small number of casualties); Obidoxime combo-pen if a nerve agent is identified (cholinergic symptoms), if unavailable, use Atropine. Midazolam to treat seizure patients; Treat associated injuries: burns; blast injuries; fractures. Ensure hospital is notified of possible contaminated patients. 46
50 CLINICAL MANAGEMENT GUIDELINE 35 POISONING, ENVENOMATION & OVERDOSE General Care Guideline SPECIFIC AGENTS: Opioids: IM Naloxone, followed by IV Tricyclic antidepressants: Watch for arrhythmias, seizures and coma. If present: - administer 0.5 mmol/kg Sodium Bicarbonate - treat seizures first with Midazolam and tachyarrthymias with Magnesium Sulphate Digoxin: Treat tachyarrhythmias with Magnesium Sulphate. Organophosphates: Take care not to become contaminated. Consider the possibility of other affected workers, occupants or first-aiders. Where feasible remove contaminated clothing, and wash skin with soap and water. If cholinergic effects are present (salivation, sweating, nausea, bradycardia), administer Atropine lv or IM. Repeat as required. Ensure hospital is notified of contaminated patient. continues over 47
51 Envenomation: CLINICAL MANAGEMENT GUIDELINE 35 (continued) POISONING, ENVENOMATION & OVERDOSE General Care Guideline Utilise pressure/immobilisation technique if appropriate. Treat signs and symptoms as they arise e.g. Cholinergic symptoms with some spider bites. Identification the creature should be brought to the hospital but only if this can be done safely. DO NOT rely on non-expert identification. With the positive identification of a Red Back Spider, pressure immobilisation is not required. Iced compresses should be applied to the area (but not directly onto the skin). Carbon monoxide / smoke inhalation: Beware of hazards self-asphyxiation and/or explosion; remove patient from danger Treat according to respiratory distress or upper airway obstruction guideline 100% oxygen, with PEEP, if Carbon Monoxide is suspected Consider the possibility of other affected workers, occupants or first-aiders Any person who has suffered an inhalation injury of toxic substances is to be transported to hospital. (Pulmonary oedema may be a late complication) Urgently transport if there is a decreased level of consciousness 48
52 CLINICAL MANAGEMENT GUIDELINE 36 EXTENDED CARE This guideline will apply in the following circumstances: where patient contact has, or is likely to, extend beyond (approx) minutes, andthe patient cannot be managed adequately within the limits of existing guidelines and pharmacology. It must be noted that the extended care guideline does not permit Paramedics to extend their scope of practice to procedures, which they have not been trained to perform. IV FLUIDS: IV Replacement: Replacement of estimated or continuing losses with Normal Saline. Aim for systolic BP of 90 mmhg. IV Maintenance: Normal Saline Baseline of 1 ml/kg/hr; Titrated to: Perfusion and hydration assessment Any continuing fluid losses Environmental conditions Urine output, if available (aim for 1 ml/kg/hr). ANTIEMETIC: Odansetron: Further IV dose, after 3 to 4 hours. May be given IM repeat after 4 hours. 49 ANALGESIA: Morphine: Following initial doses of IV Morphine, further doses of 0.05 mg/kg may be given at 15 minute intervals, titrated against: pain assessment history & presenting problem perfusion status level of consciousness & respiratory status (no further doses if GCS is 13 or below, or if respiratory rate drops below 10) Intramuscular: same provisos as general pharmacology; 0.1mg/kg dose; repeat after 30 minutes as required; thereafter at minimum of 90 minute intervals Midazolam: Can repeat initial doses as per Morphine titration, with care! Ketamine: Follow Ketamine dose chart Methoxyflurane: 6ml/day 15ml/week I.G. TUBE: Consider placement in the following patients, if patient contact is likely to be prolonged: cervical & thoracic spinal cord lesions burns patients, BSA over 20%b (especially if there is respiratory tract involvement)
53 CLINICAL MANAGEMENT GUIDELINE 37 MANAGEMENT OF COMBATIVE AND AGITATED PATIENTS CMG 37a GENERAL AMBULANCE OPERATIONS For use in situations where the patient cannot be managed due to agitation or combativeness. If concerned about safety, call for police assistance. Consider/exclude: hypoxia; hypoglycaemia; head injury; drug overdose; post-ictal state; infection. Treat as appropriate. Speak quietly - do not shout. Do not leave the patient alone. Attempt quiet reassurance in an attempt to persuade the patient to accept treatment. If reassurance and persuasion are ineffective or impractical, move to pharmacological management. This should be a last resort: Ensure adequate control of the limb and the patient. Midazolam up to 0.1mg/kg. Usually IM. May repeat dose after 10 minutes if necessary. If agitated state is thought to be due to psycho-stimulant use: Midazolam up to 0.2 mg/kg. May repeat after 10 minutes if required. Reduce the dose of Midazolam for elderly patients with: known or suspected hypotension; general debility - usually half the dose. Limb restraints are to be utilised in conjunction with pharmacological restraint. MENTAL HEALTH PATIENTS: Wherever possible, obtain an Emergency Order for the management of mental health patients. (AFP; medical practitioner; CAT Team) If not practical, proceed with pharmacological control if there is genuine concern for the welfare of the patient and/or others. PATIENTS MANAGED WITH PHARMACOLOGICAL CONTROL MUST BE TRANSPORTED TO HOSPITAL Notify and transport to nearest appropriate hospital. Monitoring once restrained and on O 2 : ECG, Temperature (watch for hypothermia), O 2 saturation, E t CO 2 NOTE Ensure thorough documentation on PCR All patients managed with CMG 37a will require an incident report to be submitted to the Clinical Services Section. 50
54 CLINICAL MANAGEMENT GUIDELINE 37 (continued) MANAGEMENT OF COMBATIVE AND AGITATED PATIENTS CMG 37b AERO-MEDICAL PATIENTS A lower threshold for intervention with sedation applies to patients who are transported by air. Identify and correct possible causes of agitation prior to flight wherever possible. If unable to obtain agreement on sedation prior to flight, advise pilot of your concerns. If still no decision to sedate patient and in your opinion there is still an unacceptable risk, do not fly. Electrolyte imbalance Hypoxia Hypovolaemia Pain Hypoglycaemia Cold Advise all crew and ACTAS Duty Manager. Duty Manager to discuss with CRRS consultant. If still agitated - sedate prior to flight. In flight agitation and combativeness is to be managed as a matter of urgency. Inform the pilot in command. Note : All patients managed with CMG 37 will require an incident report to be submitted to ACTAS Clinical Services Proceed immediately to pharmacological management. Do not use physical restraint beyond the time required to pharmacologically manage the patient. 51
55 CLINICAL MANAGEMENT GUIDELINE 38 MENINGOCOCCAL DISEASE Prompt identification of meningococcal disease & commencement of pre-hospital treatment can be life-saving. A high index of suspicion is advisable, but only in critically ill patients. Consider meningococcal disease in the following circumstances: febrile illness with sudden onset & disturbed level of consciousness. + / - haemorrhagic, purpuric or petechial rash; + / - tachycardia, hypotension, peripherally shut down. Other signs & symptoms are often non-specific, especially in young children. Such as: headache; photophobia; neck stiffness; vomiting; painful or swollen joints; focal signs; and seizures. Deterioration can be rapid Management Ensure personal protection gloves; mask; gown; and eye protection, especially if airway care is being attended. General care Ensure minimum scene time Cannulate 10 ml/kg Normal Saline; Repeat as required. Ceftriaxone 50 mg/kg IV or IM, to maximum of 2g Check BGL Urgent transport NOTE: Deterioration is possible following antibiotic administration. This would be unusual during average ambulance contact. It will most likely be a decrease in LOC and/or BP. Be prepared; manage with IV fluid. If deterioration continues consider Adrenaline infusion. 52
56 CLINICAL MANAGEMENT GUIDELINE 39 ADULT AGONAL TRAUMA PATIENTS An agonal trauma patient is described as: a trauma patient who presents on scene without cardiac output, and there is some evidence that this has been for a short time only,(e.g. witness information; short response time; arrest in ambulance care) or trauma patient immediately prior to arrest (faint central pulse, gasping/no respirations) It is acknowledged that the history of loss of cardiac output can be unreliable. It is also assumed that there are no obvious, non-survivable injuries. Be wary of situations where a cardiac event may have preceded the trauma event. BLUNT TRAUMA 1: Establish no cardiac output PENETRATING TRAUMA 1: Establish no cardiac output If there are other patients on scene with serious injuries & if there are not sufficient resources to deal with all patients, the agonal blunt trauma patient is to be triaged out. If there are other patients on scene with serious injuries & if there are not sufficient resources to deal with all patients, the agonal penetrating trauma patient is to be triaged out. If other patients have minor injuries or there are no other patients, then the agonal trauma patient is to be managed in the following manner. If other patients have minor injuries or there are no other patients, then the agonal trauma patient is to be managed in the following manner. 2: Determine if cardiac death has occurred. 2: Determine if cardiac death has occurred. Monitor patient with leads. Monitor patient with leads. If a narrow complex electrical activity with heart rate greater than 20 is observed then cardiac death has not occurred and attempts to resuscitate the patient should be considered. If a narrow complex electrical activity with heart rate greater than 20 is observed then cardiac death has not occurred and attempts to resuscitate the patient should be attempted. If slow, wide complex rhythm, or asystole, consider no resuscitation. 3: Resuscitate rapidly (if possible simultaneous procedures): If slow, wide complex rhythm, or asystole, consider resuscitation 3: Resuscitate rapidly (if possible simultaneous procedures): Cannulate; rapid infusion of greater than 2 litres of crystalloid. (pump set) Cannulate; rapid infusion of greater than 2 litres of crystalloid. (pump set) 53
57 CLINICAL MANAGEMENT GUIDELINE 39 (continued) ADULT AGONAL TRAUMA PATIENTS BLUNT TRAUMAMA (continued) PENETRATING TRAUMA (continued) Secure definitive airway ETT / LMA Aggressive oxygenation Secure definitive airway ETT/LMA Aggressive oxygenation If any doubt about air entry - chest decompression with a large bore cannula into the mid clavicular line 2 nd intercostal space on affected side/s. NOTE: If IPPV is being performed, the absence of air entry is an unreliable sign of tension pneumothorax. If chest penetration + any doubt about air entry - chest decompression with a large bore cannula into the mid clavicular line 2 nd intercostal space. Drugs Drugs 4: If at this point no restoration of cardiac output has occurred, cessation of resuscitation should be seriously considered. Agonal blunt trauma patients should not generally be transported if active CPR needs to be performed en route. The likelihood that these patients will survive from this point is effectively nil. Transport of these patients may not be in the best interest of staff and the community. 4: Facilitate urgent transport to trauma centre. Ensure notification. Continue active resuscitation. If more than 15 minutes transport time from trauma centre, go to closest hospital. If cardiac output restored, continue to trauma centre. Agonal penetrating trauma patients may be considered for transport, as survival is possible. Exceptions: - close to trauma centre - Paramedic clinical judgement Exceptions: - penetrating wounds to the head are to be treated as for blunt agonal trauma - if more than 15 minutes transport time from any hospital, & no cardiac output regained, consider ceasing resuscitation - Paramedic clinical judgement 54
58 in development... CLINICAL MANAGEMENT GUIDELINE 40 BARIATRIC PATIENTS CLINICAL MANAGEMENT GUIDELINE 41 HEADACHE CLINICAL MANAGEMENT GUIDELINE 42 BACK PAIN CLINICAL MANAGEMENT GUIDELINE 43 DEHYDRATION 55
59 If intubation is not successful the following Failed Intubation Drill MUST BE FOLLOWED Were vocal cords visualised during initial laryngoscopy? Insert OP airway and ventilate with 100% O 2 No Yes Check head /neck position BURP manoeuvre Re-attempt intubation under direct vision, after suction or removal of foreign body, as required Objective confirmation of tracheal placement (ODD, E T CO 2 ) No Yes Immediately remove ETT and insert OP or NP airway and re-ventilate with 100% O 2 Continue management in accordance with the relevant CMG DO NOT CONTINUE WITH FRUITLESS ATTEMPTS TO INTUBATE UNDER DIRECT VISION Able to oxygenate and ventilate? Yes Attempt digital placement (on appropriate patients) No If unsuccessful, insert LMA CONSIDER Able to oxygenate and ventilate? CRICOTHYROTOMY No Yes Continue management in accordance with the relevant CMG An incident report must be submitted 56
60 RAPID SEQUENCE INDUCTION (RSI) INDICATIONS THIS IS A PROCEDURE OF LAST RESORT! EXPLORE ALL OTHER OPTIONS AND ALTERNATIVES FIRST! The unconscious patient with unequivocal, life threatening airway compromise and clinical evidence of severe hypoxia. OR The unconscious patient with potential airway compromise where extrication procedures will make it impossible to provide adequate airway control. CONSIDERATIONS The following essential considerations must be taken into account prior to utilisation of this guideline. Clinical need airway compromise, clear & obvious Glasgow Coma Score < 9 hypoxia Oxygen saturation < 90% OR centrally cyanosed time to hospital (should include extrication, load & transport time) Patients who are not trapped or where extrication is not difficult, and are within 5 6 minutes time to hospital, WOULD NOT be candidates for rapid sequence induction. Assessment of the difficulty of intubation Based on: anatomical, acquired and situational factors. confidence and experience of the operator. Response to basic treatment try everything posture, guedels, nasal, suction, O 2, ventilation by mask, etc. give basic options a chance to work. only proceed to rapid sequence induction if patient remains critical. Consequences and outcomes Worse case scenario: Breathing patient with compromised airway; becomes a can t intubate, can t ventilate scenario. continues over 57
61 Fall back position Do not continue with futile attempts to intubate. Return to basics & re-ventilate. Attempt placement with: Digital placement LMA Surgical airway as a last resort. Paediatrics ONE attempt at endotracheal intubation only. PROCEDURE Basic airway management. Oxygenation aim for the highest O 2 saturations by the most efficient method. IV access establish a fast flowing line that is reliable & secure. a second IV line is sound insurance. Prepare patient: The most experienced operator is to tube. Do not debate this issue - make a choice and proceed! This is not a teaching opportunity for intubation skills. 1. Correct any hypotension / hypovolaemia 10 ml/kg Normal Saline unless in pulmonary oedema. 2. Pre-oxygenate 3. Monitor Patient; ECG / Oximetry 4.Correct any bradycardia 5. Prepare and check equipment This is vital and includes: Laryngoscope Suction ETT - syringe, ties etc. LMA Surgical airway kit 6. Brief your assistant continues over 58
62 7. Check allergies 8. Draw up drugs and check 9. Ask assistant to apply cricothyroid pressure 10. Commence intubation 11. Check tube position Visualisation of tube between cords Oesophageal detector device Auscultation Chest movement Misting in the tube E t CO 2 Pulse oximetry 12. Tie in securely DRUG SEQUENCE Adult Midazolam 0.05 mg/kg, Slow IV dose NOTE: Watch BP! Prior to Suxamethonium, if bradycardic rate < 50 Atropine 0.01mg/kg, fast push. Suxamethonium 1.5 mg/kg, over seconds. Post intubation to maintain tube and level of sedation, Alternating doses of: Midazolam up to 0.1mg/kg, slow IV dose Morphine up to 0.05 mg/kg, slow IV dose NOTE: Watch BP! Suxamethonium causes bradycardia, if patient is still bradycardic once ETT is tied in, consider a dose of Atropine. Paediatric Midazolam 0.05 mg/kg As slowly as possible. NOTE: Watch BP! Atropine 0.01mg/kg, fast push Suxamethonium 1.5 mg/kg, over seconds Post intubation to maintain tube and level of sedation alternating doses of: Midazolam up to 0.1mg/kg, slow IV dose Morphine up to 0.05 mg/kg, slow IV dose NOTE: Watch BP! continues over 59
63 IF INTUBATION FAILS Re-oxygenate / re-ventilate the patient utilise basic techniques. There is no second dose of Suxamethonium! If intubation is still unsuccessful move to a fallback option, following the Failed Intubation Drill procedure. Digital Placement LMA Surgical Airway Consider urgent transport FOLLOW UP 1. All relevant details will be carefully documented on the PCR. This especially applies to details concerning the need for sedation, the checks on correct placement of the ETT and the results of the procedure. 2. An Incident Report must be sent to the Clinical Support Section by the end of shift; the hard copy is to be sent via satchel. There are no exceptions. 3. All pharmacologically facilitated intubations will be subject to routine, mandatory Clinical Advisory Committee Review. FINAL NOTE As stated previously, this is a procedure of last resort! It is anticipated that this procedure will only be utilised in the most exceptional of circumstances. 60
64 DRUGS FOR AIRWAY MANAGEMENT - SUMMARY SHEET SEDATION FOR BASIC AIRWAY MANAGEMENT: Midazolam Dose: up to 0.1 mg/kg, slow IV dose. ( NOTE: If patient has already had Midazolam for sedation do not give a repeat dose with Suxamethonium; or give a smaller dose.) RAPID SEQUENCE INDUCTION Suxamethonium & Midazolam: Adult: Midazolam 0.05 mg/kg, slow IV dose. NOTE: Check BP as soon as practical - Reduce Midazolam dose if patient is over 60 or BP <100. Prior to Suxamethonium, if bradycardic (rate < 50) Atropine 0.01 mg/kg, fast push Suxamethonium 1.5 mg/kg, over seconds Paediatric: Midazolam 0.05 mg/kg, slow IV dose. NOTE: Check BP as soon as practical Atropine 0.01 mg/kg, fast push. Suxamethonium 1.5 mg/kg, over seconds NOTE: Watch BP! Suxamethonium causes bradycardia, if the patient is still bradycardic once the ETT is tied in, consider a dose of Atropine. SEDATE TO INTUBATE Morphine & Midazolam: Pre-infuse IV bolus of fluid, irrespective of BP Adults: IF - normal size & weight & age < 75 with a BP > 100 Morphine 10 mg IV, Midazolam 10 mg IV. Fast push. IF - small adult or BP or age 75 Morphine 5 mg IV, Midazolam 5 mg IV. Fast push. IF - BP < 70 Morphine 2.5 mg IV, Midazolam 2.5 mg IV. Fast Push. Flush dose with rapid IV fluid bolus. Paediatrics: Morphine 0.05 mg/kg IV, Midazolam 0.1 mg/kg IV If hypovolaemia is suspected: give half the calculated dose of each drug. Flush dose with rapid IV fluid bolus. Doses may be repeated x 1. (Prepare the second doses) 61
65 POST INTUBATION to maintain ET tube and level of sedation: Alternating doses of: Midazolam up to 0.1 mg/kg, slow IV dose Morphine up to 0.05 mg/kg, slow IV dose NOTE: Monitor BP closely 62
66 A.C.T. AMBULANCE SERVICE PHARMACOLOGY NOTES INDEX ACETYLSALICYLIC ACID (ASPIRIN) ADENOSINE ADRENALINE AMIODARONE ATROPINE SULPHATE CALCIUM CHLORIDE CEFTRIAXONE CLOPIDOGREL FRUSEMIDE (LASIX) GLUCAGON GLUCOSE 10% GLYCERYLTRINITRATE (ANGININE) HEPARIN HYDROCORTISONE INFLUENZA VACCINE IPRATROPIUM BROMIDE (ATROVENT) KETAMINE LIGNOCAINE MAGNESIUM SULPHATE METHOXYFLURANE (PENTHRANE) MIDAZOLAM (HYPNOVEL) MORPHINE SULPHATE NALOXONE (NARCAN) NORMAL SALINE OBIDOXIME ONDANSETRON (ZOFRAN) PARACETAMOL (PANDOL) PRASUGREL (EFFIENT) SALBUTAMOL (VENTOLIN) SODIUM BICARBONATE SUXAMETHONIUM Drug Calculator 63
67 ACETYLSALICYLIC ACID (ASPIRIN) TYPE: PRESENTATION: ACTIONS: Non-steroidal anti-inflammatory drug [S2] Tablet 300 mg 1. Inhibits platelet function (up to 7 days). Suppresses inflammation, reduces fever, relieves pain. Rapidly absorbed from the stomach and small bowel. USE: ADVERSE EFFECTS: Suspected Myocardial Ischaemia - reducing platelet aggregation and limiting clot development. Allergic reactions e.g. asthma, Angioneurotic oedema, urticaria, rhinitis, shock. CHECK FOR PREVIOUS REACTIONS Aggravation of bleeding tendencies. Gastric irritation (unlikely with 1 tablet only). CONTRA-INDICATIONS: Known or suspected allergy to Salicylates Known or suspected active bleeding Known bleeding tendency Chest pain associated with psychostimulant OD (due to an increased risk of cerebral haemorrhage) DOSE: 1 tablet (300 mg) chewed and swallowed, or dissolved in a small amount of water. ½ tablet (150mg) if on warfarin Single dose only SPECIAL NOTE: Administer even when patient is on slow release Aspirin. 64
68 ADENOSINE TYPE: PRESENTATION: ACTION: USE: ADVERSE EFFECTS: (ADENOCOR) Endogenous purine nucleoside, found in all body cells [S4] 6 mg in 2ml ampoules Causes transient inhibition of conduction in the heart, especially in the A-V node. Onset: 5 10 seconds - Duration: approx 10 seconds Treatment of supraventricular tachycardia Not for the treatment of Atrial Flutter or Fibrillation; however, if mistakenly administered to patients in these arrhythmias, the decrease in A-V conduction may unmask atrial activity. Common, although transient & generally minor. Arrhythmias at the time of conversion are common (up to 55% pts) - including PVCs, PACs, sinus brady, A-V blocks. Transient flushing of the skin; mild dyspnoea; chest tightness, nausea & headache, feelings of apprehension & fear. CONTRA-INDICATIONS: 2 or 3 heart block Known hypersensitivity PRECAUTIONS: DOSE: Asthma - may exacerbate bronchospasm. Pregnancy - use only if very poorly perfused. Antagonised by: Theophylline Potentiated by: Dipyridamole (Persantin) Carbamezapine (Carbium, Tegretol, Teril) Symptomatic adults only: 6 mg IV - rapid bolus (1 2 seconds) give into a fast-flowing pump set If 1 st dose unsuccessful, give 2 nd dose 12 mg IV (2 minutes between doses) Paediatric: 0.05 mg/kg 2 nd dose: 0.1 mg/kg SPECIAL NOTE: Use only after unsuccessful Valsalva manoeuvre x 2. Record a 12 lead ECG prior to the use of Adenosine. Rapid injection with a pump set increases the likelihood of success. Elevate limb if possible. Even if the arrhythmia is successfully converted the patient should still be transported to hospital as the incidence of recurrent arrhythmias is quite high (10-15%). If patient has previously had an unpleasant (fearful) experience with Adenosine consider a pre-dose of Midazolam 1 1.5mg IV. 65
69 ADRENALINE TYPE: A naturally occurring catecholamine [S3] PRESENTATION: 1: mg in 10 ml IMS Mini-jet 1: mg in 1 ml ampoules ACTIONS: 1. Peripheral vasoconstriction ( effect) 2. Increased rate of sinus node 3. Increased myocardial contractility 4. Increased AV conduction 5. Increased myocardial irritably ( 1 effect) 6. Bronchodilatation 7. Vasodilatation of skeletal muscle ( 2 effect) Onset: 30 seconds IV; IM: seconds Max effect: 3 5 minutes IV; IM: 4 10 minutes Endotracheal use: slightly longer times USES: ADVERSE EFFECTS: Ventricular fibrillation Asystole Pulseless Electrical Activity (PEA) Anaphylaxis Severe life-threatening asthma Bradyarrhythmias resistant to Atropine Severe upper airway obstruction due to swelling Tachycardia Tachyarrhythmias Hypertension CONTRA-INDICATIONS: Known hypersensitivity PRECAUTIONS: These apply to patients with cardiac output only: Care with patients with history of hypertension. Care with patients with history of ischaemic heart disease. Give extremely slowly to patients on MAO Inhibitor antidepressants (e.g.: Marplan, Parstelin, Marsilid, Nardil, Parnate) as Adrenaline may provoke a greatly exaggerated response. Generally, patients on MAOIs with cardiac output should receive no more than ¼ normal dose of adrenaline, titrated to response. continues over 66
70 ADRENALINE (cont) DOSE: Cardiac Arrest Adult: 1 mg, IV fast push Paediatric: 0.01 mg/kg IV / IO fast push (If no IV or IO access, administer via endotracheal tube) No limit on the number of doses in cardiac arrest Anaphylaxis / Severe life-threatening asthma: Adult: 0.5 mg IM Paediatric: 0.01 mg/kg IM (to 50 kg) Repeat IM dose x 1 as required (The preferred IM site for anaphylaxis is the thigh) If required, IV Adrenaline by infusion:1 mg in 1000 mls Normal Saline ( = 1mcg/ml)Titrate to response (20 dpm = 1 ml/min = 1mcg/min) Paediatric - use burette If the patient is critically ill, slow IV, up to 0.01 mg/kg, no faster than 50mcg/minute. NOTE: IV Adrenaline in anaphylaxis & asthma should be used very cautiously. Bradyarrhythmias resistant to Atropine: IV Adrenaline by infusion: 1 mg in 1000 mls Normal Saline ( = 1mcg/ml) Titrate to response (20 dpm = 1ml/min = 1mcg/min) Paediatric - use burette Severe upper airway swelling: Adrenaline 1:1000: wt > 10 kg - nebulise 5 mls Adrenaline 1:1000 wt < 10 kg - nebulise 0.5 ml/kg Adrenaline 1:1000 (make volume up to 5 mls with saline, as required) Single dose only SPECIAL NOTE: Adrenaline in 1000ml flask is to have medication label attached! 67
71 AMIODARONE TYPE: PRESENTATION: ACTIONS: USE: ADVERSE EFFECTS: CONTRA-INDICATIONS: DOSE: Potent anti-arrhythmic agent [S4] Ampoule 150 mg/3ml Complex electrophysiological & pharmacological profile: 1. Prolongs the action potential duration; increases the refractoriness of all cardiac tissue 2. Also blocks Na + channels (Class I action) 3. Has some anti-adrenergic effects (Class II action) Ca 2+ blockade (Class IV) 4. Prolongs QT interval reflects global prolongation of repolarisation 5. When given IV, there is a significant effect on the AV node which causes a delay in nodal conduction 6. Also effective for accessory pathway conduction Effective for both supraventricular & ventricular arrhythmias ACTAS USE: to slow ventricular rate in AF and AFl to treat VT & VF IV: can cause vasodilatation & negative inotropic effects; hypotension. (dose & rate dependent) Occasionally may cause: 1. Bradycardia ( especially in older pts) 2. Phlebitis3. Hot flushes / sweating Known hypersensitivity Cross sensitivity to Iodine SPECIAL NOTE: VF: Adult: 300 mg IV push dose (over seconds) Paediatric: 5 mg/kg IV VT, AF and AFl: 150 mg IV via Springfuser (over 10 minutes, approx. 7 mls) Paediatric: 5 mg/kg IV (VT - If extremely compromised, may be given over 5 mins by slow IV injection) No repeat doses for either treatment regimen Significant potential drug interactions:the following may potentiate the actions of Amiodarone: Digoxin; Phenytoin (Dilantin); Blockers; Ca 2+ Channel Blockers; & other anti-arrhythmics. 68
72 ATROPINE SULPHATE TYPE: PRESENTATION: ACTIONS: Parasympathetic blocking agent [S4] 1 mg in 10mls IMS Mini-jet Large number of actions. Those important in the pre-hospital setting: 1. Blocks the action of the vagus nerve on the heart 2. Increases the rate of the sinus node 3. Increases speed of conduction through the AV node 4. Reduces the amount of secretions from some glands: (e.g. tear & salivary glands). Onset IV: 2 minutes Max effect: 5 minutes IM/ET slightly longer USES: 1. Bradyarrhythmias with poor perfusion 2. Asystole/PEA 3. Organophosphate poisoning/spider bite (to increase heart rate irrespective of BP and/or assist airway maintenance by reducing excessive salivation) 4. To prevent bradycardia with Suxamethonium use ADVERSE EFFECTS: tachycardia; palpitations; blurred vision; dry mouth; confusion, urinary retention; increased body temperature (by decreasing perspiration). CONTRA-INDICATIONS: Known hypersensitivity PRECAUTIONS: Care needed in patients with Glaucoma Aim not to increase heart rate above 100/minute continues over 69
73 ATROPINE SULPHATE (cont) DOSE: Bradyarrhythmias: Adult: IV mg/kg fast push ET: 0.01 mg/kg, if no immediate IV access. Repeat x 1 as necessary Paediatric: Not used Asystole/PEA: Adult: 2 mg IV/ET Paediatric: Not used Organophosphate poisoning/cholinergic symptoms of spider bite: Adult/Paediatric: 0.01 mg/kg IV fast push Repeat as required. No upper limit on doses. Continue use even if BP is not low. May be used IM in these circumstances if IV access is not available or if there are multiple patients affected. To treat bradycardia with Suxamethonium use: Adult/Paediatric: 0.01 mg/kg IV fast push 70
74 CALCIUM CHLORIDE TYPE: PRESENTATION: ACTION: Electrolyte utilised in both electrical & mechanical actions of the myocardium. [No schedule] 1g in 10mls (10% solution) IMS Mini-jet Opposes action of high serum Potassium on the myocardium. Onset: IV: Several minutes Duration: minutes USES: 1. Emergency treatment of Hyperkalaemia 2. Prolonged hypotension, post Magnesium administration, unresponsive to fluid ADVERSE EFFECTS: Rare with nominated use 1. Tissue necrosis if extravasates from vein 2. Precipitates out in contact with Bicarbonate CONTRA-INDICATIONS: Known hypersensitivity DOSE: Adult/Paediatric: 10 mg/kg IV, over 2 minutes Repeat x 1 as required 71
75 CEFTRIAXONE (ROCEPHIN) TYPE: 3rd generation cephalosporin antibiotic [S4] PRESENTATION: Vial 1g Ceftriaxone powder for reconstitution ACTIONS: 1. Broad spectrum antibiotic Especially effective against gram-negative bacteria (e.g. Meningococcus) 2. Effective crossing of blood-brain barrier USE: Suspected meningococcal disease, in acutely ill patients ADVERSE EFFECTS: 1. Hypersensitivity reactions (not common) 2. Diarrhoea 3. Skin rash PRECAUTIONS: It is possible that 20% patients with a Penicillin allergy may be sensitive to Ceftriaxone. CONTRA-INDICATIONS: Known sensitivity to cephalosporins DOSE: 50 mg/kg, to a total of 2g IV preferred. But can also be given IO Make up to 10ml with water for injection; give slowly over 2 4 minutes May be administered IM: Dilute a maximum of 1g in 3mls of 1% Lignocaine prior to administration. Give two injections if dose is over 1g (i.e. over 3 mls volume). SPECIAL NOTE: An incident report should be submitted to Clinical Services if Ceftriaxone is administered. 72
76 CLOPIDOGREL TYPE: PRESENTATION: ACTION: (PLAVIX) Potent inhibitor of platelet aggregation Tablet 75 mg A specific and potent inhibitor of platelet aggregation. It does this by binding specifically and irreversibly to the platelet P2RY12 purinergic receptor, inhibiting Adenosine Diphosphate (ADP) mediated platelet activation and aggregation. Onset : >30 minutes USE: ADVERSE EFFECTS: CONTRA-INDICATIONS: Patients with an acute ST elevation myocardial infarction who meet the requirements for early percutaneous coronary intervention (PCI) procedure. 1. Headache 2. Dizziness 3. Stomach disturbances/pain 4. Diarrhoea or constipation 1. Known allergy 2. Known internal bleed within 6 months, 3. Current use of anticoagulants (excluding Aspirin or Clopidogrel), DOSE: 8 x 75 mg tablets (600 mg) taken orally Not to be dissolved but can be taken with water. 73
77 GLUCOSE 10% TYPE: Hypertonic Glucose solution; containing 0.1 g Dextrose per ml. [No schedule] PRESENTATION: Glucose in 500ml plastic flask ACTION: Glucose is the main energy source for the body cells, especially the brain. Onset: seconds USE: Treat hypoglycaemia; following blood glucose estimation if BGL < 4, & patient unable to eat or drink ADVERSE EFFECTS 1. Tissue necrosis if allowed to escape from the vein 2. Hyperglycaemia/hyperosmolality CONTRA-INDICATIONS: Known hypersensitivity DOSE: Up to 2.5 ml/kg IV (0.25 g/kg) slowly over 5 minutes Continue to check patency of vein May repeat dose x 1 if level of consciousness or BGL has not improved NOTE: Patients who respond to 10% Glucose should eat to prevent later development of further hypoglycaemia. Re-check BGL following treatment. 74
78 FRUSEMIDE (LASIX) TYPE: PRESENTATION: ACTIONS: Loop diuretic [S4] 80 mg in 8ml IMS Mini-jet 1.Potent diuretic when given IV, Lasix increases urine output within 5 10 minutes; and can last up to 3 hours 2. Causes venous dilatation decreases venous return. This effect occurs within 5 minutes. USE: Severe Acute Cardiogenic Pulmonary Oedema unresponsive to previous treatment to decrease venous return and promote loss of fluid. ADVERSE EFFECTS: 1. If given too rapidly, may lead to hypotension. 2. If marked diuresis occurs, the resulting fluid loss may lead to hypovolaemic shock, especially in hypovolaemic patients. 3. Potassium loss may occur may aggravate arrhythmias (esp. if previously hypokalaemic). CONTRA-INDICATIONS: 1. Systolic BP < 90mmHg 2. Hypersensitivity (Note possible cross-sensitivity to sulphonamides) DOSE Adult: On diuretics: 1 mg/kg IV over 2 minutes Adult Not on diuretics: 0.5 mg/kg IV over 2 minutes Single dose only NOTE: If the patient is in severe pulmonary oedema & IV access is not available, IM administration is acceptable. (use 2 separate sites if the volume is greater than 4mls). Paediatric: Not used 75
79 GLUCAGON TYPE: PRESENTATION: ACTION: Pancreatic hormone [S4] Vial containing 1 International Unit of Glucagon, as a dry powder, with a syringe containing 1 ml of diluting solution. Causes the liver to metabolise stores of glycogen to Glucose, resulting in a rise in the blood glucose level. Only effective if liver glycogen is available. Onset: IM 5 20 minutes USE: ADVERSE EFFECTS: Treatment of hypoglycaemia, BGL < 4 mmol/l, when oral or intravenous Glucose cannot be administered. Very rare 1. Nausea and vomiting 2. Very occasional hypersensitivity CONTRA-INDICATIONS: Known hypersensitivity DOSE: Adult: 1 International Unit (IU), IM Paediatric: wt < 20kg (approx. 5 yrs): 0.5 International Unit IM Single dose only wt > 20kg: 1 International Unit IM NOTE: Patients who respond to Glucagon should eat, to prevent later development of further hypoglycaemia. Recheck BGL following treatment. 76
80 GLYCERYL TRINITRATE (ANGININE) TYPE: PRESENTATION: ACTIONS: USES: ADVERSE EFFECTS: Nitrate smooth muscle relaxant and vasodilator [S3] White 600 mcg sublingual tablet 1. Arterial and venous vasodilatation 2. Dilatation of collateral coronary vessels 1. Relieve cardiac pain of ischaemic origin 2. Relieve pulmonary oedema 1. Hypotension 2. Headache 3. Flushing of skin 4. Occasionally bradycardia CONTRA-INDICATIONS: 1. Do not administer if systolic BP is < Do not administer if HR < Do not administer if Sildenafil (Viagra) or Vardenafil (Levitra) have been taken within 24 hours 4. Following the last dose of Tadalafil (Cialis), do not administer within 4 to 5 days in the elderly and those with renal impairment; or 3 to 4 days in all other patients. 5. Known hypersensitivity DOSE: Chest Pain: 1 tablet sublingually (600 mcg) Repeat x 1 as necessary Acute Cardiogenic Pulmonary Oedema: 1 tablet sublingually (600 mcg) Repeat x1 after approx 10 minutes if in severe respiratory distress If: 90 > Systolic BP < 100, or the patient has not previously used any nitrate medication give 1 / 2 tablet for either chest pain or APO Repeat 1 / 2 tablet x 1 as necessary NOTE: Tablet should fizz under the tongue if it is still potent. Use tablets within 3 months of opening bottle. The container MUST be dated when first opened. 77
81 HEPARIN TYPE: Unfractionated Heparin anticoagulant PRESENTATION: Ampoule 1 ml with 5000u Heparin ACTIONS: 1. Inhibits blood clotting 2. Combines with antithrombin III, a naturally occurring anti-clotting factor in plasma, and inhibits the conversion of prothrombin to thrombin 3. It also interferes with the actions of other clotting factors and with fibrin stabilising factor. USE: Patients with an acute ST elevation myocardial infarction who meet the requirements for early percutaneous coronary intervention (PCI) ADVERSE EFFECTS: 1. Bleeding 2. Anaphylactoid reactions (rare) 3. Thrombocytopenia CONTRA-INDICATIONS: Use PCI checklist PRECAUTIONS: DOSE: SPECIAL NOTE: Use with care in patients with extensive history of allergies Adults: 5000u IV, over seconds This treatment should not delay transport time to hospital 78
82 HYDROCORTISONE (SODIUM SUCCINATE) TYPE: Adrenocorticosteroid [S4] PRESENTATION: 100 mg powder in 2ml vial Reconstitute with 2ml sterile water or Normal Saline ACTIONS: Numerous & widespread ACTAS administration is for the anti-inflammatory effect on the airways USES: 1. Moderate to severe bronchospasm due to asthma, anaphylaxis or chronic airways disease 2. Patients with a history of Addison s Disease who present with a problem likely to precipitate a stress response e.g. AMI, fractures, asthma, gastroenteritis. ADVERSE EFFECTS: Nil significant with single use CONTRA-INDICATIONS: Known previous reaction to corticosteroids DOSE: Adult: 200 mg IV slow over 2 minutes Paed: 4 mg/kg IV slow over 2 minutes (to total 200mg) May be administered IM SPECIAL NOTE: Hydrocortisone is not a first-line priority drug in the management of severe bronchospasm. It is only to be given after aggressive oxygenation, inhaled bronchodilators & (where necessary) Adrenaline. 79
83 INFLUENZA VACCINE TYPE: PRESENTATION: ACTION: Influenza Virus Vaccine 0.5 ml (pre-prepared syringe) Provides antibody response and provides protection against clinical illness. Because the influenza virus is capable of significant changes in its antigenic behaviour from time to time, protection is afforded by the vaccine, limited to the strains from which the vaccine was prepared, or closely related strains. USE: Prevention of Influenza virus, types A and B, in appropriate population groups ADVERSE EFFECTS: Local reactions: Swelling, redness, ecchymosis, induration, tenderness/pain. Systemic reactions: Fever of short duration, malaise, shivering, tiredness, headache, sweating, myalgia, arthralgia, and lymphadenopathy. Allergic reactions have been reported. CONTRA-INDICATIONS: Should not be given to persons known to be allergic to fowl proteins (eggs, feathers or chicken meat) PRECAUTIONS: DOSE: Caution should be exercised if the vaccine is to be given to persons with an allergic condition such as asthma or dermatitis. Infants 6 months to 2 years ml deep subcutaneous Children 2 to 6 years 0.25 ml IMI Adults and children over 6 years 0.5 ml IMI 80
84 IPRATROPIUM BROMIDE (ATROVENT) TYPE: PRESENTATION: Anticholinergic bronchodilator [S4] 1 ml plastic nebule; containing 250 mcg Ipratropium Bromide ACTIONS: 1. Bronchodilator 2. Blocks vagal reflexes which mediate bronchoconstriction 3. Possibly more effective when used in combination with Salbutamol Onset: Duration: 3 5 minutes 2 4 hours USE: ADVERSE EFFECTS: CONTRA-INDICATIONS: PRECAUTIONS: Bronchospasm from any cause; as an adjunct to Salbutamol Rare with single use Occasionally urine retention Known hypersensitivity Care needed with use in patients with glaucoma DOSE: Adult: 500 mcg mixed with 1 st, then 3 rd and 5 th doses of Salbutamol Paediatric: 250 mcg mixed with 1 st, then 3 rd and 5 th doses of Salbutamol Use with MDI/Spacer mild to moderate, no hypoxia and familiar with use 1. Adult >6 yrs 4 x 21mcg (4 puffs) 2. Child < 6 yrs 2 x 21mcg ( 2 puffs) 81
85 KETAMINE HYDROCHLORIDE (KETLAR) TYPE: PRESENTATION: ACTIONS: USES: ADVERSE EFFECTS Dissociative anaesthetic agent [S8] 200 mg in 2ml vial Complex, multiple actions: 1. Analgesic; sedative agent 2. Marked amnesia 3. Has bronchodilating properties 4. Does not tend to cause respiratory depression 5. Does not tend to cause hypotension (via sympathetic stimulation) Onset of action is rapid: 1 2 minutes IV 3 5 minutes IM 1. Pain management, especially in patients who are hypotensive or unable to have narcotics, & if no alternative is available. 2. Particularly useful for trapped patients with limb injuries, especially if BP is borderline for narcotics. 3. Adjunct to Morphine, with alternating doses. 1. Transient Laryngospasm 2. Hypersalivation 3. Emergence reactions 4. Muscle twitching & purposeless movements 5. Occasionally respiratory depression apnoea 6. Occasionally hypotension if given rapidly to a hypovolaemic patient PRECAUTIONS: 1. Use with care in patients where a rise in BP may be hazardous (e.g. stroke, cerebral trauma) 2. Known glaucoma 3. Previous psychoses 4. Hyperthyroidism 5. Elderly and paediatric patients 6. Patients previously administered narcotics 82
86 KETAMINE HYDROCHLORIDE (cont) CONTRA-INDICATIONS: 1. Known sensitivity 2. Active cardiac disease (myocardial ischaemia, LVF, uncontrolled hypertension.) 3. Children under 1 year old DOSE: See attached Dose Chart NOTE: Ketamine can be used with alternating doses of Morphine. SPECIAL NOTE: Patients who have received Ketamine may still have a significant awareness, despite an appearance of unconsciousness. They may be able to hear and have some recall. Patients should be advised that they will experience strange/unusual sensations. Patients who become agitated may be managed with small repeat doses of Midazolam. Ketamine is a Drug of Dependence. Its use must be checked by both crew members. Under the Drugs of Dependence Act, recording and accounting for Ketamine use is a legal requirement. The unused portion of the dose must be appropriately disposed of & the disposal recorded. 83
87 KETAMINE DOSE CHART DOSES: Initial IV Repeat IV Initial IM Adult Elderly (> 65 yrs) Paediatric > 20 kg Paediatric < 20 kg Up to 1 mg/kg. Increments of up to 20 mg at intervals of seconds. Up to 1 mg/kg. Increments of up to 10 mg at intervals of seconds. Up to 1 mg/kg. Increments of up to 10 mg at intervals of seconds. Up to 1 mg/kg. Increments of up to 5 mg at intervals of seconds. After 5 10 minutes; increments of up to 20 mg as before. No upper limit. After 5 10 minutes; increments of up to 10 mg as before. No upper limit. After 5 10 minutes; increments of up to 10 mg as before. No upper limit. After 5 10 minutes; increments of up to 5 mg as before. No upper limit. 1 mg/kg 0.5 mg/kg 0.5 mg/kg 0.5 mg/kg Repeat IM After 5 10 minutes; 1 mg/kg After 5 10 minutes; 0.5 mg/kg After 5 10 minutes; 0.5 mg/kg After 5 10 minutes; 0.5 mg/kg Previous opiates IV: Up to 10 mg increments as before. IM: 0.5 mg/kg IV: Up to 5 mg increments as before. IM: 0.25 mg/kg IV: Up to 5 mg increments as before. IM: 0.25 mg/kg IV: Up to 2.5 mg increments as before. IM: 0.25 mg/kg All IV doses are to be given slowly, over 30 seconds. Recommended dilutions: Adult IV: 200 mg diluted up to 10ml; = 20 mg/ml Adult IM: 100 mg diluted up to 2ml. Discard excess dose before IM use. Elderly pt IV: 100 mg diluted up to 10ml; = 10 mg/ml Elderly pt IM: 100 mg diluted up to 2ml. Discard excess dose before IM use. Children IV: 50 mg diluted to 10ml; = 5 mg/ml Children IM: 50 mg diluted to 2ml. Discard excess dose before IM use. 84
88 LIGNOCAINE TYPE: PRESENTATION: ACTIONS: 1. Local anaesthetic 2. Anti-arrhythmic [S4] 50 mg in 5ml plastic ampoule 1. Local anaesthetic effects 2. Suppresses ventricular arrhythmias Onset S/C: 1 4 minutes Max effect: 5 10 minutes IV: 1 3mins USES: 1. Local anaesthesia prior to invasive procedures 2. VT with cardiac output, in patients who cannot have Amiodarone 3. First flush for IO in an aware patient ADVERSE EFFECTS: These effects are extremely unlikely in usual subcutaneous doses, especially if the syringe is continually aspirated. More likely if given IV. 1. C.N.S. effects stimulation followed by depression drowsiness, agitation, muscle twitching,seizures & coma 2. Cardiac effects hypotension, bradycardia, heart block, asystole CONTRA-INDICATIONS: PRECAUTIONS: DOSE: Known hypersensitivity Nil Local anaesthesia: Adult and Paediatric - up to 5mls subcutaneously VT with cardiac output: 1 mg/kg slow IV (over 2 minutes) IO in an aware patient: Adult: 2-4mls first flush Paediatric: 1-2mls first flush 85
89 MAGNESIUM SULPHATE TYPE: PRESENTATION: ACTION: USES: ADVERSE EFFECTS: CONTRA-INDICATIONS: PRECAUTIONS: Electrolyte solution [No schedule] 50% solution (10mMol) 2.5g in 5ml vial Magnesium is the 2 nd most abundant intracellular cation. Less than 1% is present in extracellular fluid. Magnesium is involved in the processes regulating Sodium and Potassium movement across cell membranes and, as such, it may promote myocardial cell membrane stability. 1. Torsades de pointes (polymorphic VT) (Often associated with prolonged QT interval) 2. Refractory VF 3. Digoxin and Tricyclic antidepressant toxicity 4. Seizures due to eclampsia Rare; more common if serum Mg is normal. Respiratory depression; nausea & vomiting; hypotension; confusion; bradycardia. AV block; renal failure; hepatic failure Myaesthenia gravis DOSE: Adult: Cardiac output: Dilute up to 10mls with N/Saline; 2.5g IV, over 5 minutes No cardiac output: 2.5g IV, over seconds Siezures due to Eclampsia: 5mg dilute up to 10ml IV Paediatric: (unusual) Dose is 50 mg/kg, to maximum of 2.5g Dilute to 10mls = 250 mg/ml Cardiac output: give calculated dose IV over 3 5 minutes No cardiac output: give calculated dose IV over seconds SPECIAL NOTE: Prolonged hypotension post-magnesium administration; if unresponsive to fluids, patient may be treated with IV Calcium 86
90 METHOXYFLURANE (PENTHRANE) TYPE: PRESENTATION: Volatile inhalation anaesthetic and analgesic agent [S4] 3ml bottle ACTION: Central Nervous System depressant Onset: 3 5 mins Offset: 3 5 mins USE: For relief of pain of all origins ADVERSE EFFECTS: 1. Altered consciousness 2. Renal dysfunction } rare with once only 3. Jaundice } Ambulance use CONTRA-INDICATIONS: 1. Depressed level of consciousness 2. Known hypersensitivity PRECAUTIONS: 1. Renal disease 2. Diabetes 3. Antibiotic or barbiturate use 4. Caution if patient unable to self-administer DOSE: Up to 3mls, self administered via Penthrox inhaler, with up to 8 L/minute of Oxygen Repeat x 1 as required Dose should not exceed 6mls/day or 15mls/week NOTE: May be used with Midazolam for musculo-skeletal pain. 87
91 METOCLOPRAMIDE (MAXOLON) TYPE: PRESENTATION: ACTION: USES: ADVERSE EFFECTS: PRECAUTIONS: CONTRA-INDICATIONS: DOSE: Antiemetic [S4] 10 mg in 2ml ampoules Antiemetic centrally acting on brain stem increases gastric emptying Onset: 3 15 minutes (IV) Duration: 30 minutes 1. Prevent vomiting: when narcotic analgesic is to be administered 2. High spinal injury 3. Serious eye injury 4. Suspected ischaemic chest pain 5. Treat nausea & vomiting Uncommon with usual doses Occasionally: 1. Drowsiness 2. Lethargy 3. Dry mouth 4. Oculogyric crisis, facial spasms 5. Speech difficulties. Side effects may be more common in dehydrated adolescents. Concomitant phenothiazide tranquilliser use will increase the likelihood of side effects. 1. Previous reaction 2. G.I. bleeding Adult dose: 10 mg lv over 2 minutes IM 10 mg Give prior to narcotic administration Single dose only Paediatric dose: Not used 88
92 MIDAZOLAM TYPE: PRESENTATION: ACTIONS: USES: ADVERSE EFFECTS: CONTRA-INDICATIONS PRECAUTIONS (HYPNOVEL) Anticonvulsant and sedative agent [S4] 5 mg in 5ml ampoules 15 mg in 3ml ampoules 1. Anticonvulsant reduces seizure activity 2. Minor tranquilliser 3. Muscle relaxant Onset (IV) 1 5 mins Duration: 2 3 hours Onset (IM) 2 5 mins Duration:? 2 3 hours 1. Status epilepticus - in a patient who has continual or prolonged seizures. 2. Sedation to manage airway, RSI, sedation of a previously intubated patient. 3. Adjunct to analgesia for injuries wheresignificant muscle spasm is present. 4. To manage agitated & combative patients. 5. To manage autonomic hyperreflexia. 6. Antiemetic (especially in paediatric patients). Depression of level of consciousness - leading to: 1. Respiratory depression 2. Loss of airway control 3. Hypotension Known hypersensitivity 1. Haemodynamic instability 2. Respiratory depression DOSE: Seizures: Adult dose: Up to 0.1 mg/kg lv, over 2 minutes, until fitting ceases. Repeat if fitting continues or recurs. Paediatric dose: Up to 0.1 mg/kg IV, over 2 minutes, until fitting ceases. Repeat if fitting continues or recurs. I.M: 0.1 mg/kg Repeat x 1 after 10 minutes as necessary. continues over 89
93 Adjunct to analgesic use with muscle spasm: Following 1 dose of Penthrane or 2 doses of Morphine, if severe pain & muscle spasm are still present Up to 0.05 mg/kg IV over 2 minutes Repeat x 1 as required Further analgesic doses are to be given with caution Mild sedation to facilitate basic airway management: Up to 0.1 mg/kg over 2 minutes When used with Morphine to sedate for airway management in selected patients: Adult: 10 mg IV rapid push (adjusted for patient weight, age and BP) Paediatric: 0.1 mg/kg rapid push Repeat x 1 as required When used with Suxamethonium: 0.05 mg/kg IV When used to manage a combative or agitated patient:: Up to 0.1 mg/kg IV, until manageable. May repeat as required to continue management IM: 0.1 mg/kg May repeat as required to continue management If agitation & combativeness is thought due to psychostimulant use: Up to 0.2 mg/kg IV, until manageable May repeat as required to continue management IM: 0.2 mg/kg * May repeat as required to continue management * Use 0.2 mg/kg dose with caution All agitated patient management doses may be reduced if there is known or suspected hypotension or hypovolaemia; in frail or elderly patients, or patients with general debility. continues over 90
94 When used to manage a patient with Autonomic Hyperreflexia: After identifying causes and trying appropriate actions and if BP remains elevated then: IV: 0.05 mg/kg, over one minute, May be repeated once after 10 minutes if no fall in BP IM: 0.1 mg/kg When used as an antiemetic: 0.05 mg/kg IV SPECIAL NOTE: 1: When administering lv for fitting, do not draw up total calculated dose. Administer first 5 mg ampoule; wait briefly for response before giving complete dose. 2: When using 0.2 mg/kg IM doses, the 15 mg/3ml formulation should be used. Exercise caution that this is only used in these circumstances. 3: Elderly patients may be especially sensitive to Midazolam, and advanced age is often a better guide to dosing than weight. 91
95 MORPHINE SULPHATE TYPE: PRESENTATION: ACTIONS: USES: ADVERSE EFFECTS: CONTRA-INDICATIONS: Narcotic analgesic [S8] 10 mg in 1ml ampoule 1. Decreases pain perception and anxiety 2. Vasodilatation Onset: (IV) 2 5 mins Duration: 1 2 hours (IM) 5+ mins Duration: 2 3 hours 1. To relieve severe pain 2. Acute pulmonary oedema 3. RSI 4. Sedation of a previously intubated patient 5. Chest Pain 1. Nausea and vomiting 2. Drowsiness 3. Respiratory depression 4. Hypotension 5. Dependence 6. Pin point pupils 7. Bradycardia 1. Depressed level of consciousness (GCS 13 or less)* Pain relief only. 2. Respiratory depression * Pain relief only. 3. Known hypersensitivity 4. BP < 70mmHg (pain relief) 5. BP < 90mmHg (pulmonary oedema) 6. Acute asthma attacks 7. Pain management in labour PRECAUTIONS: 1. Elderly patients (may be sensitive) 2. Patients with COAD 3. Hypovolaemic patients (hypovolaemia should be corrected before Morphine administration) 4. Patients with systolic BP 70 90mmHg (see below) 5. Children under 1 year 92
96 DOSE: Pain relief: Adult: Up to 0.05 mg/kg lv, over 2 minutes May be repeated at 5 minute intervals, until pain is managed. Paediatric: Up to 0.05 mg/kg IV, over 2 minutes May be repeated at 5 minute intervals, until pain is relieved. Use with caution under 1 yr of age. Morphine administration can be used alternately with Ketamine. Intramuscular administration: Pain relief only. Not for chest pain if cardiac ischaemia suspected No IV available No hypotension Patient contact estimated > than 20 minutes Dose: 0.1 mg/kg Repeat x 1 after minutes as required Patient with pain; systolic BP of 70 90mmHg: IV use only hypovolaemic patients must be receiving fluids up to half a calculated 0.05 mg/kg dose, given slowly may be repeated as required, with great care, and with an appropriate time interval between doses, titrated to response. no further doses to be given if systolic BP drops 10mmHg or more with half dose, even if it remains above 70 (e.g. initial BP 85mmHg; following Morphine dose BP now 75 mmhg) continues over 93
97 Pulmonary Oedema: 0.05 mg/kg lv, over 2 minutes May be repeated x 1 after 10 minutes, if required. When used with Midazolam for RSI: Adult: 10 mg IV rapid push (dose adjusted for patient weight, age and BP). Paediatric: 0.05 mg/kg rapid push Repeat x 1 if required. To maintain sedation post intubation: 0.05 mg/kg lv, slow IV dose SPECIAL NOTE: 1. Morphine is a Drug of Dependence. Use must be checked by both crew members. 2. Under the Drugs of Dependence Act, recording and accounting for its use is a legal requirement. 3. The unused portion of the dose must be appropriately disposed of & the disposal recorded. 4. Side effects may be reversed by use of Naloxone, although it is desirable to avoid this unless absolutely necessary. 5. Elderly patients may be especially sensitive to Morphine, and advanced age is often a better guide to dosing than weight. 94
98 NALOXONE TYPE: PRESENTATION: ACTION: USES: ADVERSE EFFECTS: (NARCAN) Narcotic antagonist [S4] 0.4 mg in 1ml IMS Mini-jet Reverses the effects of narcotic analgesics Onset IV: 1 2 minutes Duration: minutes IM: unknown; but thought to have a slightly longer onset and duration than when given lv. 1. Coma 2. Drug overdose and poisoning 3.Use in situations where there is significant decrease in level of consciousness; where there is hypoventilation, and/or loss of protective reflexes; & where overdose of narcotics cannot be positively excluded. 1 May precipitate acute withdrawal syndrome in narcotic addicts. 2. Occasional aggressive behaviour following reversal. 3. Nausea and vomiting. CONTRA-INDICATIONS: Known hypersensitivity DOSE: Adult: 0.4 mg IM, then 0.4 mg lv increments, fast push May repeat IV dose x 3 (to maximum of 2 mg) SPECIAL NOTE: Paediatric: 0.01 mg/kg lv, fast push Maximum paediatric dose: 3 doses All doses may be administered IM or IV as the situation demands. When used IV, the effect may wear off rapidly, especially if a large dose of narcotic has been taken. An IM dose is highly recommended if the patient is likely to refuse transport. Special care is needed if long-acting agents are known or suspected to have been used (eg. MS Contin; Methadone). In this case, give a larger IM dose and strongly encourage transport to hospital. 95
99 NORMAL SALINE TYPE: Isotonic crystalloid solution of 0.9% Sodium Chloride solution. Contains 151mMol Sodium & 151 mmol Chloride per litre. [No schedule] PRESENTATION: 500 or 1000mls of 0.9% Sodium Chloride solution in a collapsible plastic flask. ACTIONS: 1. Plasma volume expander 2. Also expands interstitial fluid volume 3. Plasma volume effect is only temporary as most of the saline moves out of the blood vessels quite quickly USES: 1. Initial replacement fluid, in volume depleted or dehydrated patients. Volume depletion may be due to loss of blood, plasma or fluid and electrolytes. 2. Maintenance of hydration during prolonged patient contact time. 3. To keep vein open, as IV route for drugs. ADVERSE EFFECTS: Fluid overload DOSE: IV fluid resuscitation: Adult: 10 ml/kg lv then reassess patient Rate of administration is dependent on the condition of patient. Aim to keep BP at about 90mmHg systolic No limit on amount, dependent on condition of patient. Paediatric: 10 ml/kg lv or IO then reassess patient Paediatric cardiac arrest: 20 ml/kg TKVO: Adult and Paediatric: 10 drops per minute (10ml/hr with a standard drip set). 96
100 OBIDOXIME TYPE: PRESENTATION: ACTION: USES: Oxime [No schedule] 220 mg Obidoxime/2 mg Atropine auto injector Reactivating inhibited acetylcholinesterase 1. To treat super toxic organophosphate poisoning (nerve agents) by relieving the symptoms of skeletal neuromuscular blocking that occurs during a cholinergic crisis. 2. Used in combination with Atropine, as combination auto-injector, or with Atropine separately administered. ADVERSE EFFECTS: 1. Hypotension, menthol-like sensation, warm feeling to the face, dull pain at site of injection. 2. Multiple doses can cause hepatic dysfunction. DOSE: Adult: Up to 660 mg IM over 30 minutes (Three doses via the auto-injector) Paediatric: Single dose of 220 mg IM SPECIAL NOTE: The preferred site for administration is the upper thigh. The auto injector needs to be held in place for 10 seconds when discharged to ensure the total dose has been administered. 97
101 ONDANSETRON TYPE: PRESENTATION: ACTIONS: (ZOFRAN) Potent anti-nauseant & antiemetic [S4] 4 mg/2 ml ampoule 4 mg wafers 1. Potent, highly selective histamine receptor antagonist. 2. Precise mode of action in control of nausea & vomiting is not known. Likely to have actions peripherally and in the Central Nervous System. 3. Maximum effect is approximately 10 minutes following IV administration. 4. Hepatic metabolism. USE: For the prevention or treatment of nausea & vomiting PRECAUTIONS: Not recommended in pregnancy ADVERSE EFFECTS: Uncommon Headache; flushing of skin; occ. reaction at the site of IV injection; drowsiness; anxiety & agitation; transient visual disturbances. CONTRA-INDICATIONS: Known hypersensitivity DOSE: Adult: 4 mg IV, slowly over 2 minutes Paediatric: 0.1 mg/kg IV, slowly over 2 minutes (to total of 4 mg). May be administered IM if necessary. May repeat x 1 if required, after approx. 10 minutes Wafers: 4 mg sublingually 98
102 PARACETAMOL TYPE: PRESENTATION: ACTIONS: USE: PRECAUTIONS: ADVERSE EFFECTS: (PANADOL) Simple analgesic / antipyretic 48 mg/ml Colour Free Liquid 1. Antipyretic 2. Mild analgesic Pyrexia in children who have had or may have a febrile convulsion (For ACTAS treatment, pyrexia is generally > 38 o C) 1. Impaired hepatic function 2. Impaired renal function Rare none of these side effects have been confirmed or refuted as being linked to the casual use of Paracetamol: Dyspepsia, nausea, allergic and haematological reactions CONTRA-INDICATIONS: DOSE: 1. Known or suspected allergy to Paracetamol 2. Previous Paracetamol dose in last 4 hours 3. Children who do not have a sufficient gag reflex to swallow the measured dose 4. Not to be given to children < 1 month old 20 mg/kg given orally by 3ml syringe SPECIAL NOTE: It is envisaged that the administration of Panadol Liquid will be for children that are post-ictal / post febrile convulsion, or who are likely to have a febrile convulsion and are not responding to non-medical treatment. Paracetamol does not necessarily prevent febrile convulsions. Active cooling measure should still be carried out as well as checking for the reason for pyrexia (URTI, Meningococcal disease). As a general rule, if children are administered Paracetamol, they should not be left at home. Do not exeed 60mg/kg/24hours 99
103 PRASUGREL (EFFIENT) TYPE: Thienopyridine class inhibitor of platelet activation and aggregation PRESENTATION: Tablet 10 mg ACTION: Prasugrel is an inhibitor of platelet activation and aggregation through the irreversible binding of its active metabolite to the P2Y12 class of ADP receptors on platelets. Peak concentration occurs approximately 30 minutes after dosing. USE: ADVERSE EFFECTS: CONTRA-INDICATIONS: Patients with an acute ST elevation myocardial infarction who meet the requirements for early percutaneous coronary intervention (PCI) procedure. 1. Purpura 2. Headache 3. Dizziness 4. Stomach disturbances/pain 5. Diarrhoea or constipation 1. Hepatic failure 2. Pathologic bleeding 3. Any known or suspected CVA / TIA 4. Weight < 60kg 5. Age > Current use of anticoagulants (excluding Aspirin or Clopidogrel), DOSE: 6 x 10 mg tablets (60 mg) taken orally Not to be dissolved but can be taken with water. SPECIAL NOTE: This treatment should not delay transport time to hospital 100
104 SALBUTAMOL TYPE: PRESENTATION: ACTIONS: (VENTOLIN) Synthetic 2 receptor stimulant [S4] Plastic nebules: 5 mg in 2.5ml nebuliser solution 2.5 mg in 2.5ml nebuliser solution 1. Bronchodilatation 2. Relaxation of involuntary muscle 3. Moves K + from extra-cellular to intra-cellular space Onset (neb): 5 minutes Max effect: minutes USES: ADVERSE EFFECTS: CONTRA-INDICATIONS: 1. Bronchospasm from any cause 2. Emergency treatment of suspected hyperkalaemia Rarely seen with usual nebulised therapeutic doses: 1. Tachycardia 2. Tremors 3. Hypotension Known hypersensitivity DOSE Via nebuliser, with Oxygen at 6 8 L/minute Adult: 5 mg nebule Paed: 2.5 mg nebule Use MDI/Spacer mild to moderate, no hypoxia and familiar with use Adult >6 yrs 10 x 100mcg (10 puffs) Child < 6 yrs 5 x 100mcg ( 5 puffs) With moderate to severe bronchospasm; or suspected hyperkalaemia give continuous nebulised Salbutamol. SPECIAL NOTE: With significant hypoxia, Salbutamol should be administered with 100% Oxygen. 101
105 SODIUM BICARBONATE TYPE: PRESENTATION: ACTIONS: USES: Hypertonic alkaline solution; 8.4% Sodium Bicarbonate solution; contains 1 mmol/ml Sodium & 1 mmol/ml Bicarbonate. [No schedule] 50ml Sodium Bicarbonate solution, IMS Mini-jet 1. Neutralizes metabolic acidosis as a result of cardiac arrest or poor perfusion 2. Causes movement of K + into cells swaps with H + ions Onset: seconds (IV) 1. To combat acidosis in prolonged cardiac arrest. 2. For emergency treatment of hyperkalaemia. 3. For treatment of arrhythmias, seizures or coma in Tricyclic antidepressant and Digoxin overdose patients. 4. To combat acidosis and hyperkalaemia in crush syndrome. ADVERSE EFFECTS: 1. Metabolic alkalosis 2. High Sodium content may lead to fluid overload & cardiac failure. 3. Interacts with some other drugs - (especially Calcium & Adrenaline); always flush well through the line before & after administration. Consider a second line. CONTRAINDICATIONS: Known hypersensitivity DOSE: Adult & paediatric: 0.5 mmol/kg IV; repeat x 1 as required Given as a fast push in cardiac arrest; and over 2 5 minutes to patients with a cardiac output. 102
106 SUXAMETHONIUM TYPE: PRESENTATION: ACTION: Depolarising muscle relaxant [S4] Ampoules 100 mg/2ml Acts like the neurotransmitter Acetylcholine at the neuromuscular junction. Persists for a period long enough to exhaust the motor endplate by prolonged depolarisation. Onset: IV: approx 45 seconds Duration: IV: 5 7 minutes USE: ADVERSE EFFECTS: CONTRAINDICATIONS: PRECAUTIONS: To facilitate airway management in selected patients with a GCS of less than 9 Bradycardia; Potassium release; increased intraocular & intragastric pressure. Occasionally prolonged paralysis. Has been associated with malignant hyperthermia. Previous reaction to Suxamethonium Suspected hyperkalaemia Elderly patients Neuromuscular disease Care with use in children Select patients carefully; always have a fallback position! DOSE:SPECIAL NOTE: 1.5 mg/kg IV; over seconds To be used only following completion of the ACTAS designated training programme. Paediatric: Give Atropine 0.01 mg/kg IV prior to Suxamethonium Adults: if heart rate less than 50, give Atropine prior to Suxamethonium (Bradycardia maybe a result of the head injury and raised ICP - thus BP will be elevated. In this case there is no requirement for Atropine regardless of the degree of bradycardia). Prior to administration, give IV Midazolam 0.05 mg/kg Follow up with additional Midazolam after intubation 103
107 DRUG DOSE CALCULATOR DOSE CALCULATION NOTES 50 mg/kg Dose = Weight x mg/kg Dose = Weight x 10 NOTE: Maximum dose of: 2g for Ceftriaxone, & 2.5g for Magnesium 5 mg/kg Dose = Weight x 5 4 mg/kg Dose = Weight x mg/kg Dose = Weight x mg/kg 1 mmol/kg 0.5 mg/kg 0.5 ml/kg 0.25 mg/kg 0.1 mg/kg 0.05 mg/kg 0.01 mg/kg Dose = Weight 1 Dose = Weight 2 Dose = Weight 4 Dose = Weight 10 Dose = Weight 20 Dose = Weight
108 DRUG REFERENCE KEY There have been a significant number of both additions & deletions from this list since it was last compiled. This listing covers medications that are commonly prescribed in the community, as well as some that may only be used in hospital. It is up to date as of the beginning of Every effort has been made to ensure accuracy - however, it is possible transcription errors may have occurred. Care should be taken not to rely totally on this guide. It does not include street or illicit drugs. Many drugs will have several numbers next to them, as they are used in different clinical settings, or may have these effects when taken in overdose. It does not include antibacterial agents; cytotoxics or immuno-modifying agents. Generally, no drugs given regularly by injection are included (exception - insulins). There are now a number of generic items on the market, with the generic name + the company that produces it as the drug name. e.g. Healthsense Captopril; Diltiazem BC. The generic firms are: BC; Chem Mart; DBL; GenRx; Healthsense; Terry White Chemists; 1 = Anabolic steroids 2 = Antianginal 3 = ACE inhibitors 4 = Antiarrhythmics 5 = Anticoagulants 6 = Antidepressants 6A = 5HT uptake inhibitor 6B = MAO inhibitor 6C = Tetracyclic 6D = Tricyclic 7 = Antiemetics 8 = Antihypertensives 9 = Anti-inflamatory - non steroidal 10 = Antiparkinson agents 11 = Antiplatelet agents 12 = Beta blockers 13 = Calcium channel antagonists 14 = Bronchodilators 14A = Theophylline derivative B = Non Theophylline derivative 14C = Preventative aerosols 15 = Oral contraceptives 16 = Corticosteroids 17 = Diuretic (loop) 18 = Diuretic (potassium sparing) 19 = Diuretic (thiazide) 20 = Diuretic (thiazide analogue) 21 = Anti gout agents 22 = Histamine 2 antagonist 23 = Antilipid agents 24 = Hypnotics 25 = Hypoglycaemic agents 26 = Insulin preparations 27 = Sedatives 28 = Tranquillisers 29 = Vasodilator 30 = Antihistamines 31 = Analgesics 32 = Antipsychotic 33 = Angiotensin II antagonist 34 = Antiulcerant agents 35 = Benzodiazepine 36 = Migraine prophylaxis and therapy 37 = Anticonvulsant 38 = Bone & Calcium modifying agent 39 = Hormones 40 = Dementia agents 41 = CNS stimulants 42 = Anticholinergic type agents 43 = Glaucoma preparations 44 = Weight Reducing Agents Product Name Serial Number ABILIFY 32 ACCOLATE 14 ACCUPRIL 3,8 ACCURETIC 3,8 ACENORM 3,8 ACIMAX 34 ACLIN 9,31 ACQUIN 3,8 ACT-3 9,31 ACTIFED 30 ACTION 30 ACTIPROFEN 9 ACTIQ 31 ACTONEL 38 ACTOS 25
109 Product Name Serial Number ACTRAPID 26 ADALAT 2,8,13 ADDOS 2,8,13 ADEFIN 2,8 ADENOCOR 4 ADRONAT 38 ADVIL 9,31 AERODIOL 39 AERON 14B AGGRASTAT 5 AGON SR 2,8,13 AIROMIR 14B AKINETON 10, 42 ALDACTONE 8,18 ALDAZINE 28,32 ALDOMET 8 ALENDROBELL 38 ALENDRONATE 38 ALEPAM 28,35 ALEVE 9 ALLEGRON 6D ALLERMAX 16, 30 ALLOHEXAL 21 ALLOPURINOL BC 21 ALLORIN 21 ALLOSIG 21 ALODORM 24,27,35 ALPHAGAN 43 ALPHAPRESS 8,29 ALPHAPRIL 3, 8 ALPRAX 27,28,35 ALPRAZOLAM 27,28,35 ALVESCO 16 AMARYL 25 AMFAMOX 22,34 AMISULPRIDE 32 AMIZIDE 8,18 ALMO 13 AMLOPIDINE 13 AMPRACE 3,8 AMYTAL 24 ANAFRANIL 6D ANAGRAINE 36 ANAMORPH 31 ANAPROX 9,31,35 ANATENSOL 28,32 ANDRIOL 39 ANDROCUR 39 Product Name Serial Number ANDRODERM 39 ANDRUMIN 7 ANGELIQ 39 ANGININE 2,29 ANGIOMAXIN 5 ANPEC 2,4,8,13 ANSELOL 2,4,8,12 ANTENEX 27,28,35 ANZEMET 7 APIDRA 26 APOVEN 14B APRESOLINE 8,29 APRINOX 8,19 ARATAC 4 ARAVA 9 AREDIA 38 ARICEPT 40 ARIMA 6B ARIPIPRAZOLE 32 ARIXTRA 5 AROPAX 6A ARTANE 10, 34, 42 ARTHREXIN 9,21,31 ARTHROTEC 50 9 ASASANTIN SR 11, 5 ASIG 3,8 ASMOL 14B ASPALGIN 31 ASTRIX , 5 ATACAND 33, 8 ATEHEXAL 2,4, 8,12 ATENOLOL BC 2, 4, 8, 12 ATIVAN 27,28,35 ATROBEL 42 ATTENTA 41 AURORIX 6B AUSCAP 6A AUSCARD 2,13 AUSFAM 22, 34 AUSGEM 23 AUSPRIL 3, 8 AUSRAN 34 AVANDAMET 25 AVANDIA 25 AVANZA 6 AVAPRO 8,33 AVIL 30 AVOMINE 7 106
110 Product Name Serial Number AXIT 6A AYLIDE 25 AZOL 39 AZOPT 43 BARBLOC 2,4, 8,12 BECLOFORTE 14C,16 BECONASE 16 BECOTIDE 14C,16 BENADRYL 30 BENZTROP 10,42 BEROTEC 14B BETAGAN 43 BETALOC 2,4,8,12,36 BETOPIC 43 BETOQUIN 43 BICOR 12 BIOGLAN 44 BIPHASIL 15 BONDRONAT 38 BONEFOS 38 BRENDA 35 15,39 BREVIBLOC 4,12 BREVINOR 15 BRICANYL 14B BROMOHEXAL 10 BROMOLACTIN 10, 39 BRONDECON 14A BRUFEN 9,31 BUGESIC 9 BURINEX 17 BUSCOPAN 42 BUSPAR 28 BUTALGIN 9,31 BUTAMOL 14B BYETTA 25 CABESAR 10 CAFERGOT 36 CALCIJEX 38 CALCITRIOL 38 CADUET 13 CANDYL 9,31 CAPADEX 31 CAPOTEN 3,8 CAPTOHEXAL 3,8 CAPTOPRIL BC 3,8 CAPURATE 21 CARAFATE 34 Product Name Serial Number CARBAMAZEPINE 32,37 CARDINORM 4 CARDIPRIN 11, 5 CARDIZEM 2,8,13 CARDOL 4,12 CARTIA 11, 5 CATAPRES 8,36 CELEBREX 9 CELESTONE 16 CELICA 6A CELPRAM 6A CHOLSTAT 23 CHLORPROMAZINE 32,42 CIALIS 29 CIAZIL 6A CIMEHEXAL 22,34 CIMETIDINE BC 22, 34 CIPRAMIL 6A CITALOBELL 6A CITALOPRAM 20 CITRACAL 38 CITRIHEXAL 38 CLARAMAX 30 CLARATYNE 30 CLARINASE 30 CLEXANE 5 CLIMARA 39 CLIMEN 39 CLINORIL 9,31 CLOBEMIX 6B CLOMIPRAMINE 6D CLONAC 9 CLOPINE 32 CLOPIXOL 32 CLOPRAM 6D CLOSYN 32 CLOZARIL 32 CODALGIN 31 CODAPANE 31 CODIPHEN 31 CODIS 31 CO-DIOVAN 3,8,33 CODOX 31 COGENTIN 10, 42 COGNEX 40 COLESE 42 COLESTID 23 COLGOUT
111 Product Name Serial Number COLOFAC 42 COMBIGAN 43 COMBIVENT 14B COMTAN 10 CONCORZ 6A CORALAN 2 CORAS 2,13 CORBETON 2,4,8,12 CORDARONE 4 CORDILOX 2,4,8,13 CORTATE 16 COSOPT 43 COUMADIN 5 COVERSYL 3,8 COZAAR 8,33 CRESTOR 23 CROMESE 14C CRYSANAL 9 CYMBABLTA 6A CYPRONE 39 CYPROSTAT 39 CYPROHEXAL 39 CYTOTEC 34 DANOCRINE 39 DAONIL 25 DAPA-TABS 8 DECA-DURABOLIN 1 DECANOATE 32 DEMAZIN 30 DEPO DUR 31 DEPO MEDROL 16 DEPO NISOLONE 16 DEPO PROVERA 15 DEPO RALOVERA 15 DEPTRAN 6D DERALIN 2,4,8,12,36 DERMESTRIL 39 DESERIL 36 DEXAMPHETAMINE 41 DEXAMETHSON 16 DIABEX 25 DIAFORMIN 25 DIAMICRON 25 DIAMOX 37, 43 DIANE 15, 39 DIAPRIDE 25 DIAZEPAM 35 Product Name Serial Number DIBENYLINE 29 DICLOFENAC 9 DICLOHEXAL 9,31 DIDROCAL 38 DIDRONEL 38 DIGESIC 31 DIHYDERGOT 36 DILANTIN 37 DILASIG 8,12 DILATREND 12, 8 DILAUDID 31 DILOSYN 30 DILTAHEXAL 2,13 DILTIAZEM BC 2, 13 DILZEM 2,13 DIMETAPP 30 DIMIREL 25 DIMETRIOSE 39 DINAC 9 DINDEVAN 5 DIOVAN 33 DITHIAZIDE 19 DITROPAN 42 DOLAPRIL 3 DOLASED 31 DOLOBID 9,31 DOLAFORTE 31 DOLOXENE 31 DONNALIX 42 DONNATAB 7, 42 DORMIZOL 24 DOTHEP 6D DOZILE 27 DRAMAMINE 7 DROLEPTAN 32 DUCENE 27,28,35 DUPHASTON 39 DURABOLIN 1 DURIDE 2 DUROGESIC 31 DUROMINE 44 DUROTRAM 31 DYMADON 31 DYNASTAT 9 EDECRIN 8,17 EDRONAX 6A ECOTRIN 5,11,31 EFEXOR 6A 108
112 Product Name Serial Number ELDEPRYL 10 ELEMENDOS 37 ELEVA 6A ELMENDOS 37 EMETROL 7 ELMIRON 5 EMEND 7 ENAHEXAL 3, 8 ENALABELL 3,8 ENALAPRIL 3, 8 ENBREL 9 ENDECRIN 17 ENDEP 6D ENDONE 31 ENIDIN 43 EPAC 14B EPHIDRINE HYDROC. 14B EPILIM 32,37 ERGODRYL 36 ESIPRAM 6A ESTALIS 39 ESTELLE 35 ED 39 ESTRACOMBI 39 ESTRADERM 39 ESTRADOT 39 ESTROFEM 39 EUTROXSIG 39 EVISTA 38 EXELON 40 EXFORGE 13,33 EXOLISE 44 EXTINE 6A EZETROL 23 FAMOHEXAL 34 FAMOTIDINE 34 FAVERIN 6A FELDENE 9,31 FELODIL 8,13 FELODUR 8,13 FEMODEN 15 FEMOSTON 39 FEMTRAN 39 FENAC 9,31 FENAMINE 30 FEXAL 30 FEXO-TABS 30 FIBSOL 3, 8 Product Name Serial Number FILPRIL 3,8 FIORINAL 31 FLECATAB 4 FLIXOTIDE 14C16 FLORINEF 16 FLUANXOL 32 FLUOHEXAL 6A FLUOXEBELL 6A FLUOXETINE BC 6A FLUOXETINE DBL 6A FORADILE 14B,14C FORMET 25 FORTEO 38,39 FORTRAL 31 FOSAMAX 38 FOSPRIL 3,8 FOSINOPRIL 3,8 FRAGMIN 5 FRISIUM 27,28,35 FRUSEHEXAL 17 FRUSID 17 GABAHEXAL 37 GABAPENTIN 37 GABARAN 37 GABATINE 37 GABITRIL 37 GANTIN 37 GEMFIBROZIL BC 23 GEMHEXAL 23 GEMIFIBROMAX 23 GENORAL 39 GENOTROPIN 39 GENOX 39 GLIMEL 25 GLUCOBAY 25 GLUCOHEXAL 25 GLUCOMET 25 GLUCOPHAGE 25 GLUCOVANCE 25 GLYADE 25 GOPTEN 3,8 HALCION 35 HALDOL 32 HELIDAC 34 HEPARIN 5 HUMALOG 26 HUMANOTROPE 39 HUMIRA 9 109
113 Product Name Serial Number HUMULIN 26 HYDOPA 8 HYDRENE 8,18,19 HYDROCORTISONE 16 HYFORIL 3,19 HYGROTON 8,20 HYPNODORM 24,27,35 HYPURIN ISOPHANE 26 HYPURIN NEUTRAL 26 HYSONE 16 HYTRIN 8 IBUPROFEN 9 IKOREL 2 IMDUR DURULES 2 IMFLAC 9 IMIGRAN 36 IMPROVIL 15 IMOVANE 24, 27 IMREST 24,27 IMTRATE SR 2 INDAHEXAL 8 INDAPAMIDE 8 INDERAL 2,4,8,12,36 INDOCID 9,21,31 INDOPRIL 3,8 INSIG 8 INSOMN 24,27 INTEGRILIN 11 INTAL 14C INVEGA 32 INZA 9,31 IOPIDINE 43 IPRATRIN 14B IPRAVENT 14B ISCOVER 11, 5 ISMELIN 29,31 ISOMONIT 2, 29 ISOPTIN 2,4,8,13 ISOPTO CARBACHOL 43 ISOPTO CARPINE 43 ISORDIL 2,29 ISOSORBIDE MON. 2 JEZIL 23 JULIET 35 15, 39 KALMA 27,28,35 KALURIL 8,18 KAPANOL 31 Product Name Serial Number KARVEA 8,33 KARVEZIDE 8,33 KEPPRA 37 KINIDIN DURULES 4 KINERET 9 KINSON 10 KLACID 34 KLIOGEST 39 KLIOVANCE 39 KONAKION 5 KOSTEO 38 KREDEX 8,12 KRIPTON 10 KWELLS 7, 42 KYTRIL 7 LAMIDUS 37 LAMICTAL 37 LAMITRIN 37 LAMOGINE 37 LAMOTRIGINE 37 LANOXIN 4 LANTUS 26 LARGACTIL 7,28,32, 40 LASIX 8,17 LEGOUT 21 LESCOL 23 LEVEMIR 39 LEVLEN ED 15 LEVOHEXAL 10 LEXAPRO 6A LEXOTAN 27,28,35 LIPAZIL 23 LIPEX 23 LIPIDIL 23 LIPITOR 23 LIPOSTAT 23 LIPRACE 3,8 LIPRACHOL 23 LIQUIGESIC CO 31 LISINOBELL 3,8 LISINOPRIL 3,8 LISINOTRUST 3,8 LISODUR 3,8 LITHICARB 32 LIVIAL 39 LOCILAN 15 LOETTE 15 LOGICIN
114 Product Name Serial Number LOGYNON 15 LONAVAR 1 LONITEN 8 LOPID 23 LOPRESOR 2,4,8,12,36 LORASTYNE 30 LOSEC 34 LOVAN 6A LUMIGAN 43 LUMIN 6C LURSELLE 23 LUVOX 6A LYCINATE 2 LYRICA 37 MADOPAR 10 MAGICUL 22, 34 MAOSIG 6B MAREVAN 5 MARVELON 15 MAXOLON 7 MAXOR 34 MEDROXYHEXAL 15 MEFIC 9,31 MEGACE 39 MELIPRAMINE 6D MELIZIDE 25 MELLERIL 28,32 MELLIHEXAL 25 MELOXIBELL 9 MENOREST 39 MEPRAZOL 34 MERBENTYL 42 MERSYNDOL 31 METAMAX 36 METFORBELL 25 METFORMIN BC 25 METHYLPHENIDATE 41 METOCLOPRAMIDE 7 METOHEXAL 2,4,8,12,36 METOPROLOL BC 2,4,8,12,36 MEXITIL 4 MIACALCIC 38 MICARDIS 8,33 MICROGYNON 15 MICROLUT 15 MICRONOR 15 MICROVAL 15 Product Name Serial Number MIDAMOR 8,18 MINAX 2,4,8,12,36 MINIDIAB 25 MINIMS PILOCARP. 43 MINIPRESS 8 MINITRAN 2,29 MINULET 15 MIRENA 15, 39 MIRTAZON 6B MIXTARD 26 MOBIC 9 MOBILIS 9,31 MOCLOBEMIDE 6B MODAVIGIL 41 MODECATE 28,32 MODURETIC 8,18,19 MOGADON 24,27,35 MOHEXAL 6B MONACE 3 MONODUR DURULES 2 MONOFEME 15 MONOPLUS 3,8 MONOPREM 39 MONOPRIL 3,8 MONOTARD 26 MORPHALGIN 31 MOTILIUM 7 MOVALIS 9 MOVELAT 9 MOVOX 6B MOXICAM 9 MS CONTIN 31 MS MONO 31 MURELAX 27,28,35 MYSOLINE 37 NAPAMIDE 8 NAPROGESIC 9,31,36 NAPROSYN 9,31,36 NARAMIG 36 NARDIL 6B NASONEX 16 NATRILIX 8 NAVANE 32 NAVOBAN 7 NEUPRO 10 NEO-MERCAZOLE 39 NEO-SYNEPHRINE 43 NEULACTIL 28,32 111
115 Product Name Serial Number NEUTRAL PILOCARP. 43 NEURONTIN 37 NEXIUM 34 NICOTINIC ACID 23 NIDEM 25 NIFECARD 8,13 NIFEDIPINE BC 8,13 NIFEHEXAL 8,13 NIMOTOP 13 NITRO-DUR 2,29 NITROLINGUAL SPRAY 2,29 NITROSTAT 2 NIZAC 22,34 NORDETTE 15 NORDITROPIN 39 NORFLEX 43 NORGESIC 43 NORIDAY 15 NORIMIN 15 NORINYL 15 NORMISON 24,27,35 NORSPAN 31 NOLVADEX 39 NORVASC 2,8,13 NOTEN 2,4,8,12 NOVARAP 26 NOVNORM 25 NOVONORM 25 NOVOMIX 26 NOVORAPID 26 NUELIN 14A NUPENTIN 37 NUROFEN 9,31 NUROLASTS 9,31 NYEFAX 8,13 ODRIK 3,8 OGEN 39 OLMETEC 33 OMEPRAL 34 OMEPRAZOLE 34 OMNITROPE 39 ONDAZ 7 OPTIMOL 43 ORAP 28,32 ORAP 28,32 ORDINE 31 ORGARAN 5 Product Name Serial Number OROXINE 39 ORUDIS 9,31 ORUVAIL SR 9,31 OSPOLOT 37 OSSMAX 38 OVESTIN 39 OXANDRIN 1 OXETINE 6A OXIS 14B,14C OXYCONTIN 31 OXYNORM 31 OZLODIP 2,8,13 PALFIUM 31 PAMACID 34 PAMISOL 38 PANACORT 16 PANAFCORTELONE 16 PANAFEN PLUS 9 PANALGESIC 31 PANAMAX 31 PARACODIN 31 PARADEX 31 PARAHEXAL 31 PARALGIN 31 PARIET 34 PARLODEL 10 PARNATE 6B PAROXETINE 6A PAXAM 35,37 PAXTINE 6A PEETALIX 30 PENDINE 37 PEPCID 22,34 PEPCIDINE 22,34 PEPZAN 34 PERIACTIN 30,36 PERINDO 3,8 PERINDOPRIL 3,8 PERIVASC 2,8,13 PERMAX 10 PERSANTIN 5,11,29 PEXSIG 2 PHENOBARBITONE 37 PHENERGAN 7,27,30 PHOSPHATE-SANDOZ 38 PHYSEPTONE 31 PHYSIOTENS 8 PILOCARPINE
116 Product Name Serial Number PILOPT 43 PROPINE 43 PIROHEXAL 9,31 PIROXICAM 9 PLACIL 6D PLAVIX 5,11 PLENDIL 8,13 POLARAMINE 30 PONSTAN 9,31 PRAMIN 7 PRASIG 8 PRATSIOL 8 PRAVACHOL 23 PRAVASTATIN 23 PRAZOHEXAL 8 PRAZOSIN BC 8 PREDMIX 16 PREDSOLONE 16 PREGNYL 39 PRESOLOL 8,12 NYOGEL 43 PREMARIN 39 PREMIA 5 39 PRESOLOL 8,12 PRESSIN 8 PREXIGE 31 PRILACE 2,3 PRIMOBOLAN 1 PRIMOLUT 39 PRINIVIL 3,8 PRITOR 8, 33 PROCID 21 PRO-BANTHINE 42 PROBITOR 34 PROCUR 39 PRODEINE 31 PROGOUT 21 PROGYNOVA 39 PROLODONE 31 PROMETHAZINE 30 PRONESTYL 4 PROPYLTHIOURACIL 39 PROTAPHANE 26 PROTHIADEN 6D PROTOS 38 PROVERA 39 PROVEN 9,31 Product Name Serial Number PROVIRON 39 PROXEN 9,31 PROZAC 6A PULMICORT 14C,16 P.V. CARPINE 43 PYRALIN 9 QUESTRAN LITE 23 QUILONUM SR 32 QUINAPRIL 3,8 QVAR 14C,16 RAFEN 9,31 RALOVERA 39 RAMACE 3,8 RAMIPRIL 2,3 RANI 22,34 RANIHEXAL 34 RANSIM 23 RANITIDINE DBL 22,34 RANOXYL 34 RANZEPAM 35 RAPIFEN 31 REDIPRED 16 REDUCTIL 44 REFLUDAN 5 REGITINE 29 REMERON 6A REMINYL 40 RENITEC 3,8 REOPRO 5 RESPOCORT 16 RESTAVIT 27 RHINOCORT 16 RISPERDAL 32, 40 RITALIN 41 RITHMIK 4 RIVOTRIL 37 ROCALTROL 38 ROSIG 9,31 RUBESAL 9 RYTHMODAN 4 SABRIL 37 SAIZEN 39 SANDOMIGRAN 36 SANDRENA 39 SEAZE 37 SELGENE 10 SEQUILAR ED
117 Product Name Serial Number SERC 29,30 SERENACE 7,28,32 SEREPAX 27,28,35 SERETIDE 14B,14C SEREVENT 14B,14C SEROQUEL 32 SERTA 6A SERTRALINE 6A SERTATRUST 6A SETRONA 6A SETACOL 42 SETAMOL 31 SEVREDOL 31 SICAL 38 SIFROL 10 SIGMAXIN 4 SIGMETADINE 22,34 SIMVABELL 23 SIMVAHEXAL 23 SIMVAR 23 SIMVASTIN 23 SIMVATRUST 23 SINEASE 30 SINEMET 10 SINEQUAN 6D SINGULAIR 14 SITRIOL 38 SKELID 38 SNUZAID 27 SODIUM OIDIDE 39 SOLAVERT 4, 12 SOLIAN 32 SOLONE 16 SOLPRIN 5,11,31 SOMAC 34 SOMIDEM 24 SONE 16 SORBIDIN 2,29 SOTACOR 4,12 SOTAHEXAL 4,12 SOTALOL BC 4, 12 SPIRACTIN 8,18 SPIRIVA 14C SPREN 11,31 STALEVO 10 STELAZINE 7,28,32 STEMETIL 7,32 Product Name Serial Number STEMZINE 7,32 STILDEM 24 STILNOX 24 SUBLIMAZE 31 SUMAGRON 36 SUMATAB 36 SURGAM 9,31 SURMONTIL 6D SUSTANON 39 SUVULAN 36 SYMBICORT 14C SYMMETREL 10 SYNAREL 39 SYNPHASIC 15 TACIDINE 34 TAGAMET 22,34 TALAM 6A TALOHEXAL 6A TAMBOCOR 4 TARKA 2,4, 8,13 TAZAC 22,34 TEGRETOL 32,37 TELFAST 30 TELNASE 16 TEMAZE 24,27,35 TEMGESIC 31 TEMTABS 24.27,35 TENOPT 43 TENORMIN 2,4,8,12 TENSIG 2,4,8,12 TENSODENINE 31 TENUATE 45 TERIL 32,37 TERTROXIN 39 TETRABENAZINE 43 TEVETEN 8, 33 THEO-DUR 14 TICLID 5,11 TICLOPIDINE HEXAL 5,11 TILADE 14C TILCOTIL 9 TILODENE 5,11 TIMOPTOL 43 TIMPILO 43 TITRALAC 34 TOFRANIL 6D TOLERADE 6D TOLVON 6C 114
118 Product Name Serial Number TOPACE 3, 8 TOPAMAX 35,37 TOPROL 12 TORADOL 9 TRAMAL 31 TRANALPHA 3,8 TRANDATE 8,12 TRANDOLAPRIL 3,8 TRANSIDERM-NITRO 2,29 TRAVACALM 7,42 TRAVATAN 43 TRYZAN 3,8 TRENTAL TRI PROFEN 9,31 TRIASYN 3,8,13 TRIFEME 15 TRILEPTAL 37 TRIPHASIL 15 TRIQUILAR 15 TRISEQUENS 39 TRITACE 3,8 TRUSOPT 43 TRYPTANOL 6D TYLENOL 31 ULCAID 34 ULCYTE 34 ULTAC 34 ULTRATARD 26 UNISOM 24,27 UREMIDE 8,17 UREX 8,17 VALIUM 27,28,35 VALLERGAN 27,30 VALPAM 35 VALPRO 32,37 VASOCARDOL CD 2,8,13, 33 VASTORAN 23 VASTIN 23 VEGANIN 31 VERACAPS 2,8,13 VIAGRA 29 VIOXX 9 VISKEN 2,4,8,12 VOLFAST 9,31 VOLTAREN 9,31 VOXAM 6A VYTORIN 23 Product Name Serial Number XALACOM 43 XALATAN 43 XANAX 27,28,35 XYDEP 6A XYLOCARD 8 XYVION 39 YASMIN 15 YAZ 15 ZACTIN 6A ZADINE 30 ZAMHEXAL 27,28,35 ZAN EXTRA 3,8,13 ZANIDIP 8, 13 ZANTAC 22,34 ZARONTIN 37 ZELDOX 32 ZENICAL 44 ZESTRIL 3,8 ZIMSTAT 23 ZOCOR 23 ZOFRAN 7 ZOLOFT 6A ZOMIG 36 ZOLIBELL 24 ZOLPIDEM 24 ZOMETA 38 ZOTON 34 ZUMENON 39 ZYDEP 6A ZYLOPRIM 21 ZYDOL 31 ZYPREXA
119 PATIENT ASSESSMENT GENERAL APPROACH AND TREATMENT Initial Assessment Initial Treatment Secondary Assessment Secondary Treatment Danger Response Alert Voice Pain Unconscious Formal GCS Airway + Cervical spine care Chin lift; head tilt; jaw thrust; Hold head still. Suction; clear airway Oral / nasal airway ETT Cervical collar KED Board / scoop Breathing Look, Listen, Feel. I.P.P.V. Oxygen Respiratory rate Pulse oximetry Breath sounds Pleural decompression Stabilise flail segment Circulation Control bleeding Central pulse Skin signs Cardiac compressions ECG Monitor D.C.C.S. Pulse rate BP Analyse ECG IV Fluids Cannula History of: Event Patient Bystanders Utilise bystanders Full history Expose injuries Obtain medications Bring relatives along Drugs BGL Formal drug therapy Transport Call backup if required Assess time critical Prepare for transport Transport Notify hospital 116
120 TIME CRITICAL PATIENT GUIDELINE The following patients can be considered actually or potentially Time Critical. This requires a minimum scene time, treatment en-route wherever possible and prompt transport to a designated Trauma Centre for trauma patients. This is a guideline only, and does not represent a complete and exclusive list of time critical patients. 1: TRAUMA PATIENTS Vital signs: adults (Actual time critical indicators) Respiratory distress (rate > 29, or < 10/minute), or Altered L.O.C. (GCS < 13), or Hypotensive (systolic BP < 90mmHg), and/or Revised Trauma Score < 12 Pattern of injury: (Actual time critical indicators) Penetrating injury head; neck; torso; axilla, groin Amputation above the wrist or ankle Fractures to TWO or more proximal long bones, or a fractured pelvis Suspected crush syndrome Paralysis or significant weakness of limbs Significant injury to single body region (e.g. head, abdomen, chest), or lesser injuries to 2 or more body regions Burns > 10% body surface; special areas (e.g. eyes, genitals; or respiratory tract involvement) continues over 117
121 Mechanism of injury: (Potential time critical indicators) Motor vehicle Pedestrian - high speed (> 60 kph), with significant intrusion into passenger compartment - rollover - patient ejected from vehicle - death / serious injury of another occupant - trapped, with actual extrication time > 20 minutes. struck by a vehicle at > 30 kph Pedal / motorcyclist Other impact speed > 30 kph Fall > twice patient height Struck by object falling > 5m (related to weight of object) Explosion / blast 2: OTHER PATIENTS chest pain suggestive of ischaemia unrelieved upper airway obstruction aortic aneurysm or dissection worsening hypotension (from any cause) significant arrhythmias, unresponsive to treatment generalised seizures, unresponsive to treatment stroke acute hypoxia, unresponsive to treatment deteriorating L.O.C. (from any cause) heatstroke or significant hypothermia prolapsed umbilical cord or complicated labour Carbon Monoxide poisoning with decreased L.O.C. Cardiac arrest in advanced pregnancy (gestation > 20 / 52 ) Modifying factors for all time critical patients: age < 5 yrs or > 60 yrs previous medical conditions lack of response to current treatment 118
122 GUIDE TO SUICIDE RISK ASSESSMENT SUICIDE RISK QUESTIONS MEANS: Is the method available? METHOD: Is the method lethal? Level of detail? PLANS: Rehearsals? Time/Date? Place? INTENT: Plans to carry through? Plans to actually die? THOUGHTS: Anxious Turmoil? Worthlessness? Hopelessness? SUPPORTS: Friends? Family? Case Worker? Social Worker? HISTORY: Personal/Family History? Previous Attempts? Other Illness? 119
123 GUIDE TO MENTAL HEALTH STATUS ASSESSMENT APPEARANCE Grooming, Posture, Build, Clothing, Cleanliness BEHAVIOUR Eye Contact, Mannerisms, Gait, Activity Level SPEECH Rate, Volume, Pitch, Tone Flow, Pressure MOOD Emotion as described: Anxious, Depressed, Cheerful AFFECT Emotion as observed: Restrictive, Blunted, Labile THOUGHT FORM Amount, Rate, Derailment, Flight of ideas THOUGHT CONTENT Disturbance, Delusions, Suicidal, Obsessions PERCEPTION Illusions, Thought Insertion/Broadcasting, Hallucinations- Auditory, Olfactory, Tactile, Visual or Gustatory INSIGHT & JUDGEMENT Cognition, understanding of illness, its causes & effect 120
124 A.C.T. AMBULANCE SERVICE MENTAL COMPETENCY ASSESSMENT APPLICATION GUIDELINES (For patients refusing Ambulance care or treatment where there is a known or suspected medical condition causing concern) 1: Was patient assessed in accordance with the ACTAS patient assessment standard? (if not document why) YES / NO 2: Has the medical condition or concern been fully explained to the patient, including level of concern; alternatives & options; risks / consequences of their decision? (if not document why) YES / NO 3: Does the patient acknowledge and appear to comprehend the information given to them? (i.e. Are they able to repeat it back to you in their own words?) YES / NO 4: Is the patient able to accurately recall this information when asked after a period of time (approx 5 10 mins later)? YES / NO 5: Does the patient communicate in a consistent manner on the issues of the medical condition, over the ambulance contact time? YES / NO All yes = the patient is most likely to have the capacity to make an informed decision 1 x No = the patient may not be competent 2 or more No = a higher likelihood patient is not competent (or they are uncooperative!) FULLY DOCUMENT THE RESULTS OF THIS PROCESS! 121
125 APGAR SCORE SCORE Colour Blue / pale Pink: Extremities blue Completely pink Respiration Absent Slow: irregular Good; crying Heart Rate Absent Below 100 Above 100 Muscle Tone Limp Some flexion of extremities Active motion Reflex Irritability No response Grimace Vigorous cry, cough, sneeze Assess Apgar score at 1minute and 5 minutes after birth 122
126 Age Weight (kg) A.C.T. AMBULANCE SERVICE - PAEDIATRIC REFERENCE CARD Resps Heart Rate Systolic BP E.T.T. size (mm) E.T.T. Length (cm) Fluid 10ml/kg Defib 2 j/kg Neonate months months years years years years years years Weight formula Age < 9 years: Approx weight (kg) = (age x 2) + 9 Age > 9 years Approx weight (kg) = age x 3 Fluid resuscitation 10 ml/kg bolus - Normal Saline Thereafter Normal Saline bolus DO NOT use pump set in children under 15 kg - use 3-way tap and syringe Defibrillation E.T.T. Size: Age / = diameter in mm E.T.T Length: Age / = length in cm Defib 4 j/kg All values are approximate only Rounded off to closest energy setting References - Paediatric Fluid Reference Card Children s Hospital of Pittsburgh - Drug Doses in Paediatrics Royal Children s Hospital Melbourne 123
127 PEEP VALUES 5 cm 10 cm 15 cm Cardiac arrest for adults, infants & children Intubated patients (not if suspected raised ICP, and if O 2 sats > 90%) Start level for: - pulmonary oedema - near drowning - CO poisoning - asthma - CAL Maximum level for infants & children Next level for: - pulmonary oedema - near drowning - CO poisoning - asthma (max) - CAL (max) if not responding to 5cm Final level for: - pulmonary oedema - near drowning - CO poisoning only if still desaturated with 10cm 124
128 ACT AMBULANCE SERVICE SPINAL IMMOBILISATION LOW RISK ASSESSMENT FLOWCHART 1: Patient mentation Decreased level of consciousness? No Alcohol / drug impairment? No Loss of consciousness involved? No Yes Immobilise Yes Immobilise Yes Immobilise 2: Subjective assessment Cervical Thoracic Lumbar spinal pain? No Numbness / tingling / weakness No Yes Immobilise or burning sensation? Yes Immobilise 3: Objective assessment Cervical Thoracic Lumbar spinal tenderness? No Other painful injury or significant distraction? No Pain with spine range of motion? # Yes Immobilise Yes Immobilise No Yes Immobilise MAY TRANSPORT WITHOUT SPINAL IMMOBILISATION # Range of motion is only to be checked if all other criteria are negative! NOTE:Exercise care if a patient is seen very soon after the event. - Significant distraction can be something other then a physical injury e.g. significant injury to a loved one or significant damage to car - Recheck the patient before clearing, if not transporting. Your clinical judgement may still be exercised to utilise spinal immobilisation, even if the algorithm clears the patient. Pre-existing spinal disease and older age should increase the level of suspicion even with a clear process. 125
129 Spinal Cord Injury It is vital to carry out motor and sensory examinations as the patient may have motor damage without sensory damage and vice versa. Sensory Examination The level at which sensation is altered or absent is the level of injury. Examine the patient with light touch and response to pain. Use the forehead as a guide to what is normal sensation. When conducting the examination ensure you check both upper limbs and hands and both lower limbs and feet. T4 examination must be carried out in the mid-axillary line and not the midclavicular line as C2, C3 and C4 all provide sensation to the nipple line. Motor Examination Upper limb motor examination Lower limb motor examination 1. Shrug shoulders C4 Flex hip L1 & L2 2. Bend the elbow C5 Extend knee L3 3. Push wrist back C6 Pull foot up L4 4. Open/close hands C8 Push foot down L5 & S1 For thoracic and abdominal motor examination, look for activity of the intercostal and abdominal muscles. Diagnosis of spinal cord injury in the unconscious patient 1. Look for diaphragmatic respiration. A quadriplegic has lost intercostal muscles and relies on the diaphragm to breathe. 2. Flaccid limbs. 3. Loss of response to painful stimuli below the level of the lesion. 4. Loss of reflexes below the level of the lesion. 5. Erection in the unconscious male. 6. Low BP (Systolic less than 100) associated with a normal pulse or bradycardia indicates that the patient MAY be a quadriplegic. 126
130 DIFFERENTIATION OF WIDE COMPLEX TACHYCARDIAS. The more of these present, greater the chance of VT. If in doubt, treat as VT, especially if sick. 1: History of: - Ischaemic heart disease - Cardiac failure - Cardiomyopathy + increasing age 2: Atrio-ventricular dissociation 3: Capture beats or fusion beats 4: Very wide QRS (> 0.14secs) 5: Bizarre or extreme axis = VT (a positive complex in AVR strongly supports this) 6: Negative concordance across chest leads = VT Positive concordance tends towards VT Non-concordance = 50:50 7: V 1 - monophasic R, or biphasic RS - taller left (initial) peak on rabbits ears = VT; - if second peak is taller = 50:50 - fat initial R wave (0.04 secs or >) lean towards VT 8: V6 - monophasic QS or - biphasic QR - suggests VT 9: Triphasic V 1 & V6 = < 10% VT 127
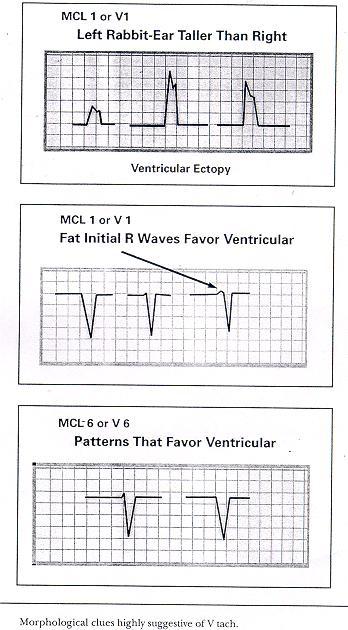
131 128
132 129 MAXIMUM Q T INTERVALS Heart Rate (per min) Maximum Q-T Interval (sec) (Males) (Females)


133 12 Lead ECG Placement 130
134 15 Lead ECG Placement Post 12-lead ECG 1. Locate V 4 R position: 5 th intercostal space; right side mid-clavicular line. 2. Move V 1 lead to V 4 R position 3. Locate V 8 position: in line with the anterior 5 th intercostal space mid scapular line 4. Move V 5 lead to V 8 position 5. Locate V 9 position: in line with V 8 position left paraspinal border 6. Move V 6 lead to V 9 position 7. Acquire 15 lead ECG: Press on Insert the limb lead and the precordial lead attachments into the main cable. Insert the cable connector into the green connector on the monitor. Encourage the patient to remain as still as possible. Press 12 lead 12 lead/age menu appears Select age 8. Monitor will detect and print the 15 lead ECG 9. Re-label the 3 altered leads on ECG strip 131
135 A.C.T. Ambulance Service STEMI Bypass Flow chart 1: Identified STEMI patient by Intensive Care Paramedic (ICP) via 12 lead ECG and appropriate clinical evidence 2: Transmit ECG to TCH ED with phone number attached 3: ECG to be reviewed by Admitting Officer (AO) 4: AO to call back transmitting phone number within 5 minutes 5: No call back from AO within 5 minutes... Proceed to TCH; Patient to be treated according to STEMI by-pass guidelines Complete check list! 6: Confirmation from AO... Proceed to TCH; Patient to be treated according to STEMI by-pass guidelines Complete check list! 7: Unclear decision between AO & ICP... Proceed to TCH; treat according to normal ACTAS guidelines 8: Ambulance to radio TCH ED to alert them of STEMI patient and time to hospital 9: On arrival at TCH ED... AO to review patient. Decision made whether ACTAS takes patient straight to catheter lab or offloads in ED. 132
136 PATIENT DETAILS Surname A.C.T. Ambulance Service STEMI Bypass Check List Given name Age Date Case number INDICATIONS if answer is NO or UNSURE to ANY of the following, do NOT administer Heparin, Prasugrel or Clopidogrel. Discuss with A/O Symptoms less than 6 hours duration? 12 lead ECG, with ST elevation in 2 contiguous leads, 1 mm in limb leads, &/or 2 mm in chest leads? Systolic BP less than 180mmHg? Diastolic BP less than 110mmHg? GCS = 15? CONTRA-INDICATIONS for PRASUGREL If yes - move to Clopidogrel Known allergy to prasugrel Age over 75 years Weight under 60kg ANY history of TIA / CVA (or unable to reliably ascertain) CONTRAINDICATIONS for CLOPIDOGREL or HEPARIN Known allergy to heparin or clopidogrel Current use of anti coagulants (excluding aspirin or clopidogrel) Pregnancy or delivery in last 2 weeks Active pathologic bleeding of any origin Severe renal or hepatic disease Head injury or facial trauma in the last 3 months Non compressible vascular punctures? Clotting problem (haemophilia etc)? Yes No Unsure Yes No Unsure Officer name:. Signature:. Contra- indications may be relative rather than absolute. Discuss with Admitting Officer during phone call back. This completed form must be submitted with the review (2 nd ) copy of the ACTAS PCR. 133
137 Acute Myocardial Infarction >1mthe limb leads and >2mm in the V leads in >2 consecutive leads Acute Myocardial injury presents as raised ST Commonly this is an acute ischaemic injury. Significant ST elevation >1mm in the limb leads and >2mm in the V leads in greater than 2 contiguous leads Infarction can present as pathological Q wave (older sign of full thickness infarction - >=.04 wide; deeper than 25% of height of R wave). Infarction may also present with T wave changes - inverted - large, hyperacute. ST depression may indicate myocardial ischaemia; occasionally myocardial infarction. ECG changes + reliable or suspicious clinical story may indicate myocardial ischaemia/infarction. I Lateral avr V 1 Septal V 4 Anterior II Inferior avl Lateral V 2 Septal V 5 Lateral III Inferior avf Inferior V 3 Anterior V 6 Lateral 134
138 INFARCTION OVERVIEW SITE INDICATIVE LEADS Inferior II, III, avf Septal V 1 - V 2 Anterior V 3 V 4 Antero-septal V 1 V 4 Lateral I, avl, V 6 (V 5 ) Antero-lateral I, avl, V 3 V 6 Right ventricular Posterior V 3 R, V 4 R, V 5 R, V 6 R (usually seen with inferior changes) Reciprocal changes in anterior leads Indicative changes V 8, V 9 135

139 INFERIOR AMI 136
140 ANTERO-SEPTAL AMI 137
141 ANTERO-LATERAL AMI 138

142 LATERAL AMI 139
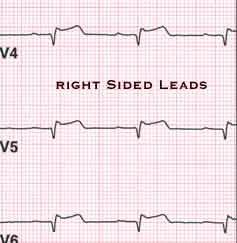
143 RIGHT VENTRICULAR AMI 140

144 POSTERIOR AMI (1) STANDARD 12 lead ECG 141
 V7 V9 LEADS")
145 POSTERIOR AMI (2) V7 V9 LEADS 142

146 RIGHT BUNDLE BRANCH BLOCK 143

147 LEFT BUNDLE BRANCH BLOCK 144
148 USES OF CAPNOGRAPHY (ACTAS) Verify initial position of ETT Monitor continuing tracheal position of ETT Assist in assessment of adequacy of chest compressions Assist with confirmation of ROSC Aid in determination of cessation of resuscitation efforts Monitor effective IPPV in patients with critical CO 2 requirements MONITORING PROCEDURE 1. Open CO 2 connector door, connect Microstream tubing by turning clockwise. (The monitor will sense the presence of the tubing and activate the E T CO 2 function automatically. Self-test, auto-zeroing and warm up may take up to 2 ½ minutes) 2. Connect the tubing to the patient (proximal to bacterial filter is preferred) 3. Display E T CO 2 waveform on Channel 3 4. Adjust scale if required Monitor is configured to Autoscale. This means that the monitor will overselect the scale based on the measured E T CO 2 measurement. The E T CO 2 is displayed in mmhg. A respiratory rate is also displayed. (No respiratory rate is displayed if the E T CO 2 is less than 8mmHg. The waveform is still valid). NOTE: Rapid altitude changes may cause the machine to attempt to purge the tubing. If this occurs, disconnect the tubing briefly from the monitor, and then reconnect it. 145
149 INTERPRETATION OF RESULTS It is important to utilise the waveform to assist in interpretation of information, not just relying on the numerical reading. NOTE: P A CO 2 is generally 3 mmhg higher than E T CO 2. Critical values in critical patients: Cardiac arrest: E T CO 2 consistently above 15 mmhg seems to have some positive correlation with ROSC. Patients with acute intracranial pathology: P A CO 2 should be in range of mmhg E T CO 2 should be in range of mmhg. DOCUMENTATION OF RESULTS Serial E T CO 2 readings may be recorded in the appropriate section of the ACTAS PCR. Waveform printouts (important for verification of ETT placement) may be attached to the PCR from either a screen print or the code summary. E T CO 2 values will be included in the vital signs summary printout for later reference. 146
150 Wave Forms 147
151 RESPIRATORY STATUS AND PERFUSION ASSESSMENT NORMAL RESPIRATORY DISTRESS (#) General appearance Calm, quiet, not anxious Distressed, anxious, obviously fighting for breath, exhausted. Decreased level of consciousness Speech Normal sentences, with no difficulty Short sentences phrases words only none Respiratory Noises (heard without a stethoscope) Quiet, no noises Cough Audible wheeze on exhalation; Crackly moist sounds; Inspiratory stridor. Chest auscultation Quiet, no wheezes or crackles Wheeze: expiratory; occ inspiratory as well Crackles fine coarse; bases mid zone full field Silent chest one side, or bilateral Respiratory rate Respiratory effort Pulse rate Skin Adults: / minute Kids: / minute Babies: / minute Minimal apparent effort; small chest / abdo movement Adults: / min Kids: Babies: Pink; normal Tachypnoea - adults > 24 / min - kids > 35 / min - babies > 50 / min Marked chest / abdo movement; use of accessory muscles; intercostal recession; sternal retraction; tracheal tug (NOTE: chest movement may be minimal with some conditions) (*)Tachycardia - adults > 100 / min - kids > babies > 150 (slow pulse rate is a late sign in severe cases) Sweaty; sometimes pale May be flushed Cyanosis is a late sign Conscious state Alert; orientated Altered Oximetry 96% + on room air 90 95% on room air; < 90% = serious hypoxia NOTE: This assessment applies to patients with respiratory distress from any cause (#) Any of these features may indicate respiratory distress. The more that are present, the greater the degree of respiratory distress. (*) Some patients, especially older patients, may be on medication that prevent the development of tachycardia. 148

152 RULE OF NINES FOR ADULTS 149
153 Relative Percentage of Body Surface Area affected by Growth AREA Age ADULT A = ½ of head 9 ½ 8 ½ 6 ½ 5 ½ 4 ½ 3 ½ B = ½ of one thigh 2 ¾ 3 ¼ 4 4 ½ 4 ½ 4 ¾ C = ½ of one leg 2 ½ 2 ½ 2 ¾ 3 3 ¼ 3 ½ 150
154 NORMAL BLOOD VALUES Arterial Blood Gases: ph PaO mm Hg PaCO mm Hg O 2 content vols% CO 2 content vols% Biochemistry: Sodium Potassium Calcium Magnesium Bicarbonate Creatinine Urea Glucose mmol/l mmol/l mmol/l mmol/l mmol/l mmol/l mmol/l mmol/l (fasting) Haematology: Haemoglobin Male: g/l Female: g/l Haematocrit Male: 42 52% Female: 37 48% Red cell count million White cell count thousand Platelet count thousand 151
155 EXTERNAL PACING PROCEDURE Indications: Bradycardia with poor perfusion: - unresponsive to Atropine or IV fluids; or - where IV access cannot be obtained. (Pacing is preferred over an Adrenaline infusion for post cardiac arrest bradycardia). Procedure: 1: Explain procedure to the patient and family 2: Set up Adrenaline infusion, if IV access obtained 3: Ensure ECG electrodes are well off the chest 4: Prepare skin for pacing electrodes (clip - no shaving; no alcohol) 5: Anterior electrode in approx V 2 V 3 12 lead position, horizontally (Avoid the nipple, sternum & diaphragm) 6: Posterior electrode at (L) vertebral edge, below bony prominence of scapula, vertically 7: Set current at 0mA, demand mode, rate approx 50% over initial bradycardia 8: Ensure pacer is sensing (markers on QRS complexes) 9: Slowly increase current output in 5mA increments (use selector wheel) until electrical capture occurs (rarely under 60mA) 10: Ensure electrical capture (change in QRS; wide QRS; big T wave) 11: Check mechanical capture (pulse; LOC; BP) 12: Increase current output by 5mA over initial capture value 13: Ensure analgesia is provided (use alternating small doses of Midazolam / Morphine) 14: Continue to check electrical and mechanical capture 15: Adjust rate and current output as required 152
156 153
157 154
158 155

159 ACCESS TO BUSES &COACHES Roof hatches (emergency exits) Off-side Window Emergency Exit (towards rear on the Driver s side) Rear Window Emergency Exit (if fitted) Rear-mounted engine Batteries on other side at REAR on most coaches or buses, Batteries are located near the engine. External Emergency Release valves or switches under bumper The fuel tank is usually mounted here for rear engine coaches (However, for mid or front engines, the tank is towards the rear) 156
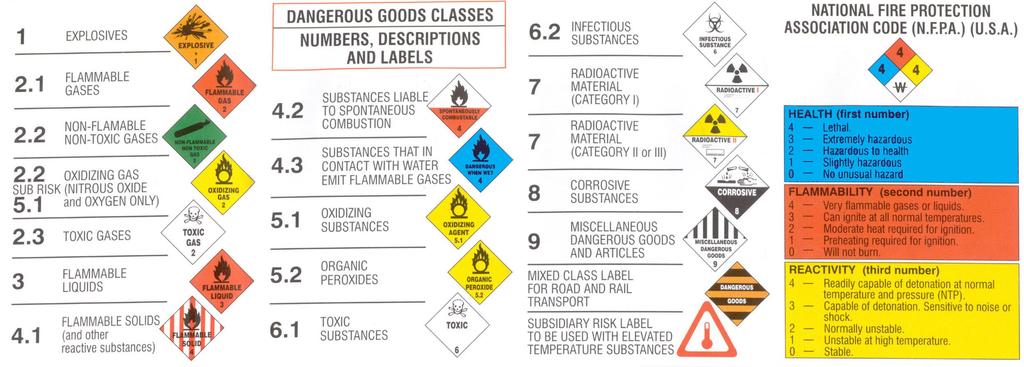
160 157
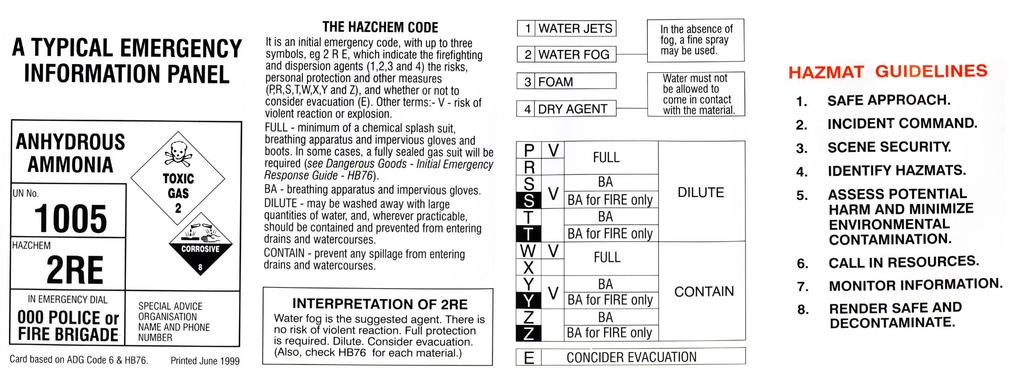
161 158
Z19.2 Cross Reference to Patient Care Maps & Clinical Care Procedures
 2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
MEDICAL KIT - ALGORITHMS
 MEDICAL KIT - ALGORITHMS Page 2 : BRONCHOSPASM / ASTHMA Page 3 : TENSION PNEUMOTHORAX Page 4 : Page 5 : Page 6 : CONGESTIVE HEART FAILURE/ PULMONARY EDEMA ANAPHYLACTIC SHOCK / ALLERGIC REACTION ANGINA
MEDICAL KIT - ALGORITHMS Page 2 : BRONCHOSPASM / ASTHMA Page 3 : TENSION PNEUMOTHORAX Page 4 : Page 5 : Page 6 : CONGESTIVE HEART FAILURE/ PULMONARY EDEMA ANAPHYLACTIC SHOCK / ALLERGIC REACTION ANGINA
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
ACT AMBULANCE SERVICE
 ACT AMBULANCE SERVICE CLINICAL MANAGEMENT MANUAL POCKET EDITION Fourth Edition August 2007 1 CLINICAL MANAGEMENT GUIDELINES Contents Case Category 1 Patient Categories Medical 2 Patient Categories Trauma
ACT AMBULANCE SERVICE CLINICAL MANAGEMENT MANUAL POCKET EDITION Fourth Edition August 2007 1 CLINICAL MANAGEMENT GUIDELINES Contents Case Category 1 Patient Categories Medical 2 Patient Categories Trauma
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
HEALTH PROFESSIONS COUNCIL OF SOUTH AFRICA PROFESSIONAL BOARD FOR EMERGENCY CARE CAPABILITIES OF EMERGENCY CARE PROVIDERS: JUNE 2016
 HEALTH PROFESSIONS COUNCIL OF SOUTH AFRICA PROFESSIONAL BOARD FOR EMERGENCY CARE CAPABILITIES OF EMERGENCY CARE PROVIDERS: JUNE 2016 CAPABILITIES Airway Management Finger sweep Head-tilt-chin lift Jaw-thrust
HEALTH PROFESSIONS COUNCIL OF SOUTH AFRICA PROFESSIONAL BOARD FOR EMERGENCY CARE CAPABILITIES OF EMERGENCY CARE PROVIDERS: JUNE 2016 CAPABILITIES Airway Management Finger sweep Head-tilt-chin lift Jaw-thrust
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
APPLY FIRST AID ONLINE WORKBOOK
 APPLY FIRST AID ONLINE WORKBOOK STUDENT NAME: ADDRESS: PHONE CONTACT: DATE OF COURSE: Welcome to CYNERGEX GROUP pre-learning package for the APPLY FIRST AID course. This workbook is to be completed in
APPLY FIRST AID ONLINE WORKBOOK STUDENT NAME: ADDRESS: PHONE CONTACT: DATE OF COURSE: Welcome to CYNERGEX GROUP pre-learning package for the APPLY FIRST AID course. This workbook is to be completed in
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
VAO BASIC SUPPORT CLINICAL APPROACH TO THE PATIENT HANDOUT
 CLINICAL APPROACH TO THE PATIENT HANDOUT 1 I am the most important part of patient care. How can you expect to treat a patient appropriately if you don t follow through on basic primary care? Remember:
CLINICAL APPROACH TO THE PATIENT HANDOUT 1 I am the most important part of patient care. How can you expect to treat a patient appropriately if you don t follow through on basic primary care? Remember:
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2
 CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Clinical Procedures and Guidelines
 Clinical Procedures and Guidelines Pocket Edition 2013-2015 2 foreword These are the Clinical Procedures and Guidelines (CPGs) for the New Zealand ambulance sector. This is the pocket edition of the Clinical
Clinical Procedures and Guidelines Pocket Edition 2013-2015 2 foreword These are the Clinical Procedures and Guidelines (CPGs) for the New Zealand ambulance sector. This is the pocket edition of the Clinical
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
HealthCare Training Service
 HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
Pediatric Trauma Care
 2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
MICHIGAN. Table of Contents. State Protocols. Adult Treatment Protocols
 MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Frontline First Aid 2012 Emergency Care Manual Treatments
 Heart Attack/Angina (p. 132) 1. Recognize signals of a heart attack 2. Assist with Nitroglycerin 3. Assist with ASA 4. Rest and Comfort 6. More advanced medical care Breathing Emergencies (p. 105) Anaphylaxis
Heart Attack/Angina (p. 132) 1. Recognize signals of a heart attack 2. Assist with Nitroglycerin 3. Assist with ASA 4. Rest and Comfort 6. More advanced medical care Breathing Emergencies (p. 105) Anaphylaxis
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD
 ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
BLS ROUTINE MEDICAL CARE
 BLS ROUTINE MEDICAL CARE Scene safety # Assure scene safety prior to patient contact C-spine # Perform manual cervical spine stabilization if indicated (Follow the cervical spine protocol.) ABCs # Assess
BLS ROUTINE MEDICAL CARE Scene safety # Assure scene safety prior to patient contact C-spine # Perform manual cervical spine stabilization if indicated (Follow the cervical spine protocol.) ABCs # Assess
Pediatric advanced life support. Management of decreased conscious level in children. Virgi ija Žili skaitė 2017
 Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
VENTRICULAR FIBRILLATION. 1. Safe scene, standard precautions. 2. Establish unresponsiveness, apnea, and pulselessness. 3. Quick look (monitor)
") LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL
 CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
Paediatric Emergency Prompt Cards
 Paediatric Emergency Prompt Cards Introduced July 2016 Prompt cards are designed to be used by any member of the resus team If you have any comments or suggestions, please contact helen.collyer-merritt@sash.nhs.uk
Paediatric Emergency Prompt Cards Introduced July 2016 Prompt cards are designed to be used by any member of the resus team If you have any comments or suggestions, please contact helen.collyer-merritt@sash.nhs.uk
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
IRECA BLS Challenge 2015 Scenario 1
 Scenario 1 Team Name Team Number Captain Name Judge 1 # Judge 2 # JUDGE S SHEET Overview: This scenario challenges the competitors to use basic triage techniques and then to do the most good for the most
Scenario 1 Team Name Team Number Captain Name Judge 1 # Judge 2 # JUDGE S SHEET Overview: This scenario challenges the competitors to use basic triage techniques and then to do the most good for the most
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
Post Resuscitation (ROSC) Care
 Care") Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
Module Summaries: The emergency plan is a crucial part of the total sports program.
 Module Summaries: Summary - The Emergency Plan The emergency plan is a crucial part of the total sports program. Prior to each season and game, those individuals responsible for the program and athletes
Module Summaries: Summary - The Emergency Plan The emergency plan is a crucial part of the total sports program. Prior to each season and game, those individuals responsible for the program and athletes
Thrombolysis Delivery, Care, and Monitoring. 5 Acute Trusts - 6 Primary Care Trusts Ambulance Trust 4 Local Authorities
 Thrombolysis Delivery, Care, and Monitoring Documentation & Pathways Need to follow locally agreed policies and procedures Follow thrombolysis pathway? Need to complete Sits database Weight Dose matters!
Thrombolysis Delivery, Care, and Monitoring Documentation & Pathways Need to follow locally agreed policies and procedures Follow thrombolysis pathway? Need to complete Sits database Weight Dose matters!
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Medical Emergencies and Current Management in Dentistry. Prof. Mark Greenwood Newcastle University
 Medical Emergencies and Current Management in Dentistry Prof. Mark Greenwood Newcastle University Lancaster 1.02.12 PREVENTION! Attitude and environment Usually a clue in the history PREVENTION! Attitude
Medical Emergencies and Current Management in Dentistry Prof. Mark Greenwood Newcastle University Lancaster 1.02.12 PREVENTION! Attitude and environment Usually a clue in the history PREVENTION! Attitude
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
MICHIGAN. State Protocols
 MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
Cardiovascular Emergencies. Chapter 12
 Cardiovascular Emergencies Chapter 12 Cardiovascular Emergencies Cardiovascular disease (CVD) claimed 931,108 lives in the US during 2001. 2,551 per day Almost two people per minute! CVD accounts for 38.5%
Cardiovascular Emergencies Chapter 12 Cardiovascular Emergencies Cardiovascular disease (CVD) claimed 931,108 lives in the US during 2001. 2,551 per day Almost two people per minute! CVD accounts for 38.5%
Johnson County Emergency Medical Services Page 23
 Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
2
 1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
68W COMBAT MEDIC POCKET GUIDE
 GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
ADULT TREATMENT GUIDELINES
 A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
Advanced Resuscitation - Adolescent
 C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG. TargetSolutions. Technology with a Purpose
 EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG 1 Technology with a Purpose TargetSolutions delivers employee training that helps organizations achieve compliance, mitigate We risk, believe reduce a well-trained
EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG 1 Technology with a Purpose TargetSolutions delivers employee training that helps organizations achieve compliance, mitigate We risk, believe reduce a well-trained
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
WESTMEAD Cardiac QUESTIONS PRACTICE SAQ
 QUESTION 1 A 65-year-old man presents to the emergency department with a history of palpitations. His vital signs are: BP 105/60 mmhg HR 156 beats/min RR 26 /min Temperature 36.2 o C His ECG is on the
QUESTION 1 A 65-year-old man presents to the emergency department with a history of palpitations. His vital signs are: BP 105/60 mmhg HR 156 beats/min RR 26 /min Temperature 36.2 o C His ECG is on the
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket
 BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
Advanced Life Support
 Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Mesa County EMS Protocol Test 2016
 Mesa County EMS Protocol Test 2016 1. Which of the following is incorrect? a. Each EMS and Fire agency should have protocols in place for evaluation of personnel involved in fire suppression operations
Mesa County EMS Protocol Test 2016 1. Which of the following is incorrect? a. Each EMS and Fire agency should have protocols in place for evaluation of personnel involved in fire suppression operations
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Anaphylaxis: Treatment in the Community
 : Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
: Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
Pediatric Resuscitation
 Pediatric Resuscitation Section 24 Pediatric Cardiac Arrest Protocol The successful resuscitation of a child in cardiac arrest is dependent of a systematic approach of initiating life-saving CPR, recognition
Pediatric Resuscitation Section 24 Pediatric Cardiac Arrest Protocol The successful resuscitation of a child in cardiac arrest is dependent of a systematic approach of initiating life-saving CPR, recognition
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Platelet aggregation inhibitor. Cardiac chest pain or suspected Myocardial Infarction.
 s Aspirin Platelet aggregation inhibitor. Anti-inflammatory agent and an inhibitor of platelet function. Useful agent in the treatment of various thromboembolic diseases such as acute myocardial infarction.
s Aspirin Platelet aggregation inhibitor. Anti-inflammatory agent and an inhibitor of platelet function. Useful agent in the treatment of various thromboembolic diseases such as acute myocardial infarction.
IMMEDIATE EMERGENCY BURN CARE » THERMAL BURNS » ELECTRICAL BURNS » CHEMICAL BURNS FIRST AID FOR THE THREE MAJOR CATEGORIES
 IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
In accordance with protocols, this patient should be transported to which medical facility?
 NOTE: Please select the most appropriate answer based on the Westchester Regional On-Line Medical Control Physician (OLMC) Regional System Overview, as well as current regional and state EMS protocols
NOTE: Please select the most appropriate answer based on the Westchester Regional On-Line Medical Control Physician (OLMC) Regional System Overview, as well as current regional and state EMS protocols
PAEDIATRIC ACUTE CARE GUIDELINE. Resuscitation Coma
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Resuscitation Coma Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Resuscitation Coma Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Homework Assignment Complete and Place in Binder
 Homework Assignment Complete and Place in Binder Chapter # 34/35: Pediatric & Geriatric Emergencies 1. The first month of life after birth is referred to as the: A) neonatal period. B) toddler period.
Homework Assignment Complete and Place in Binder Chapter # 34/35: Pediatric & Geriatric Emergencies 1. The first month of life after birth is referred to as the: A) neonatal period. B) toddler period.
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Pediatric Advanced E.M.T. Treatment Protocol
 Pediatric Advanced E.M.T. Treatment Protocol Important: Use Broselow tape for all pediatric and neonatal drug dosages and for equipment sizes. 06/12 Code 50 Emergency Childbirth Labor and Delivery Obtain
Pediatric Advanced E.M.T. Treatment Protocol Important: Use Broselow tape for all pediatric and neonatal drug dosages and for equipment sizes. 06/12 Code 50 Emergency Childbirth Labor and Delivery Obtain
Emergency First Response (EFR) Skills Assessment Sheets V4 June 2017
 Skills Assessment Sheets V4 June 2017") Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3