Adult Acute Myocardial. Infarction
|
|
|
- Camron Higgins
- 6 years ago
- Views:
Transcription
1 Adult Acute Myocardial Infarction
2 Preclinical stable CAD Acute Coronary Syndrome No cardiac enzyme elevation cardiac enzyme elevation Ischemia Cell Injurydeath UA NSTEMI STEMI
3 Definition of Coronary Artery Disease CAD IHD Acute coronary syndrome All patients with coronary artery atherosclerosis Cardiac disease as a result of myocardial ischemia (imbalance between oxygen requirements and supply) 1. Unstable angina 2. Non-ST elevation MI 3. ST elevation MI
4 Clinical Presentation of ACS Classical Angina Unstable angina Angina equivalent - dyspnea (LV failure) - arrhythmia, faint, tiredness Acute myocardial infarction Atypical chest pain - musculoskeletal, pleuritic features etc
5 Rest Angina New-onset Angina Increasing Angina Unstable Angina Occurrence of angina Class I : Strenuous, rapid or prolonged exercise Class II : Slight limitation of ordinary activity Class III : Mark limitation of ordinary physical activity Class IV : At rest

6 Definition of AMI Necrosis of a portion of heart muscle due to inadequate blood supply Diagnosis: Clinical Investigations
7 Complications of UA, AMI Evolving AMI Congestive heart failure Malignant arrhythmia bradyarrhythmia, tachyarrhythmia Pulmonary edema Cardiogenic shock
8 The first healthcare providers to encounter the ACS pt can have a big impact on pt s outcome Reduce myocardial necrosis Prevent and treat major complications e.g. VF, VT, pulm edema, shock, unstable bradyarrhythmia or tachyarrhythmia Reduce subsequent heart failure, death
9 first healthcare providers can ensure: Efficient risk stratification Initial stabilization BCLS, ACLS if necessary Referral for immediate cardiology care
10 Diagnosis of AMI Typical history Suggestive ECG changes Positive biomakers Others e.g. Cardiac Imagings
11 Based on history Pain > 15 minutes Crushing, chocking, tight; substernal Unrelieved by rest or nitroglycerin Radiation to arms, neck, back, jaw, epigastrium Associated sighs: diaphoresis, shortness of breath, anxiety Feeling of impending doom, death



12 Pain > 15 mins crushing, tight Unrelieved by rest or GTN Radiation of pain Associated signs : diaphoresis, shortness of breath, anxiety, impending doom
13 Based on ECG Normal ECG does not rule out AMI When in doubt, repeat the ECG 15 min to 30 min later 2 adjacent leads with > 1mm ST segment elevation, or new LBBB ( STEMI ) ST depression > 0.5 mm or dynamic T inversion ( UA or NSTEMI )
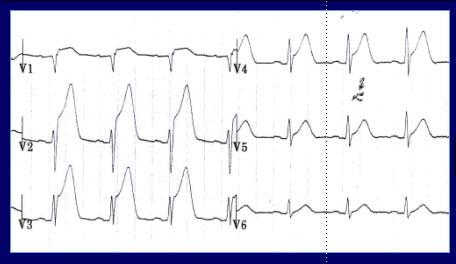
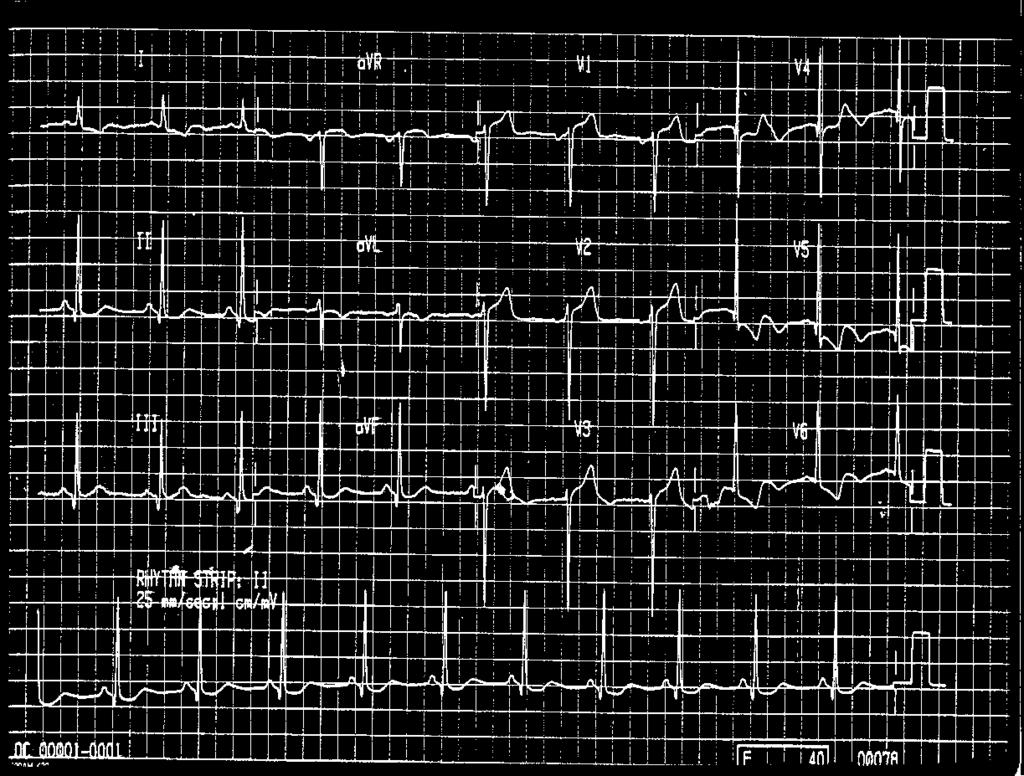
14



15 Pts with normal or non-diagnostic ECG with symptoms of ACS usually are at low risk or intermediate risk Aims: to risk stratify with diagnostic tests and to provide appropriate Rx e.g. cardiac biomarkers, TMX, stress echo, sestamibi scan
16 Based on biomarkers Cardiac enzymes e.g. CK-MB, troponin T or I Insensitive during the first 4-6 hrs of presentation. Hence may need serial testing Troponin elevation correlates with increased risk of adverse outcome, increased thrombus burden & microvascular embilization, increased risk of death

17 As it takes time for biomarkers to appear, an early, normal level does not exclude AMI
18 Action in Emergency Department (soon) Chest x-ray Blood studies (e.g. electrolytes, cardiac enzymes, renal function, coagulation studies) Avoid arterial punctures
19 Pts with STEMI usually have complete occlusion of an epicardial coronary artery Mainstay of treatment is reperfusion Rx fibrinolytics, or primary PCI Aims:rapidly identify pts with STEMI quickly screen them for indications or contraindications for reperfusion therapy
20 Thrombolytic Agents Currently available - Streptokinase - Recombinant tissue plasminogen activator (r-tpa) - APSAC (anisoylated plasminogen-streptokinase activator complex)
21 Eligibility Criteria for Thrombolytic Therapy C ntraindications Active internal bleeding Suspected aortic dissection Significant head injury within 3 months Intracranial neoplasm or hemorrhage or AVM Stroke < 3 months History bleeding diathesis
22 Eligibility Criteria for Thrombolytic Therapy Relative Contraindications Recent trauma or major surgery < 3 months Traumatic or prolonged (>10 mins) CPR Pregnancy Severe HT (BP >180/110 mmhg) Recent internal bleeding > 1 month Active peptic ulcer disease Stroke > 3 months Current use of warfarin Significant liver or renal dysfunction
23 Pts with UA or NSTEMI usually have critical but incomplete occlusion of an epicardial coronary artery Mainstay of treatment is not fibrinolysis, But optimized medical therapy, or early invasive strategies
24 Symptoms & signs of ACS 12 lead ECG ST elevation > 0.1 mv in > 2 adjacent limb leads > 0.2 mv in > 2 adjacent chest limbs Other or normal ECG Raised cardiac enzymes + ve Normal cardiac enzymes -ve STEMI NSTEMI UAP
25 Symptoms & signs of ACS & suggestive ECG Pain Rx: : nitrate, morphine Antiplatelets Rx STEMI NSTEMI / UAP Thrombolysis Sx < 3 hrs & PCI delay > 60 mins No contraindication & PCI delay > 90 mins PC I Sx < 3 hrs & PCI delay < 60 mins Sx > 3 hrs & PCI delay < 90 mins Early invasive Delayed invasive, or conservative Cardiogenic shock within 36 hrs heparin heparin heparin heparin Gp IIb/IIIa Gp IIb/IIIa Gp Iib/IIIa
26 Initial general therapy (1) M O N A Morphine Oxygen Nitrates ( S/L, aerosol spray, I.V.) Aspirin
27 Initial general therapy (2) Clopidogrel b-blockers Heparin (unfractionated, low-molecular-weight) Glgcoprotein IIb / IIIa Calcium channel blockers ACE inhibitors Statins
28 Initial general therapy (3) Management of rhythm disturbances VT, VF Asystole, heart blocks Bradyarrhythmia Tachyarrhythmia narrow complex broad complex
29 Diagnosis of Atrial Arrhythmia & Management of Narrow Complex Tachycardia
30 Atrial Ectopics Diagnostic features : Usually earlier than normal (ie premature) P wave morphology different from sinus P. May be lost or deform preceding T wave PR interval may be short or long QRS usually normal unless aberrantly conducted When early may be blocked - blocked atrial ectopic Assessment : Symptomatic? Associated AF Underlying heart disease Respiratory disease Usually no treatment necessary

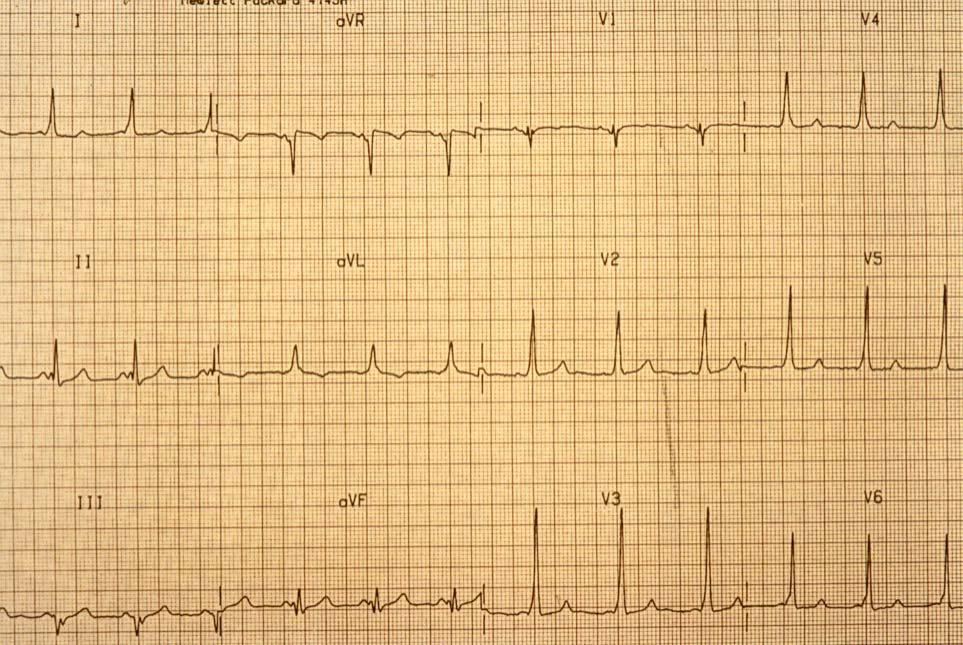
31 Sinus Arrhythmia Rate : Usually beats/min but may be faster or slower Rhythm : IRREGULAR P waves : Uniform and upright in appearance One preceding each QRS complex PRI : sec QRS : <.10
32 Junctional Rhythm Rate is slower than sinus rhythm Rhythm is regular No preceding P wave Infrequently P wave may precede or be just after the QRS (The P waves are inverted in II, III, avf) QRS usually narrow unless aberrantly conducted
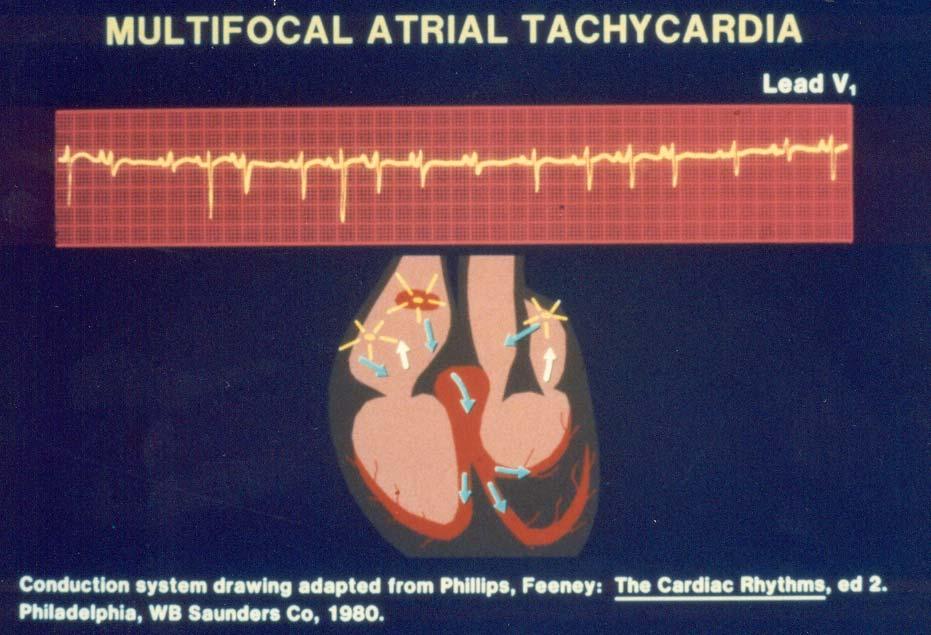
33 Tachycardia Regular Irregular Narrow Complex Broad Complex Narrow Complex Broad Complex Sinus Tachycardia or PSVT or Atrial Flutter Ventricular Tachycardia or SVT with Aberrancy or Preexcitation Atrial Fibrillation or Atrial Flutter with varying Block or Multifocal AT Polymorphic VT or Torsade De Pointes or Preexited AF
34 Sinus Tachycardia Rate : beats/min Rhythm : Regular P waves : Uniform and upright in appearance One preceding each QRS complex PRI : sec QRS : <.10
35 Pain - analgesia Anxiety - sedation Sinus Tachycardia Symptoms and Treatment Hyperdynamic state - ß blockade Hypovolemia - volume replacement Extensive myocardial damage - hemodynamic monitoring and drug therapy
36

37 Paroxysmal Supraventricular Tachycardia
38 Supraventricular Tachycardia Rate : Rhythm : P waves : PRI : QRS : / min Regular Atrial P waves differ from sinus P waves P waves are usually identifiable at the lower end of the rate range but seldom identifiable at rates > 200 May be lost in preceding T wave Usually not measurable because the P wave is difficult to distinguish from the preceding T wave; if measurable, is <..10 sec
39
40 WPW paths & associated rhythms
41
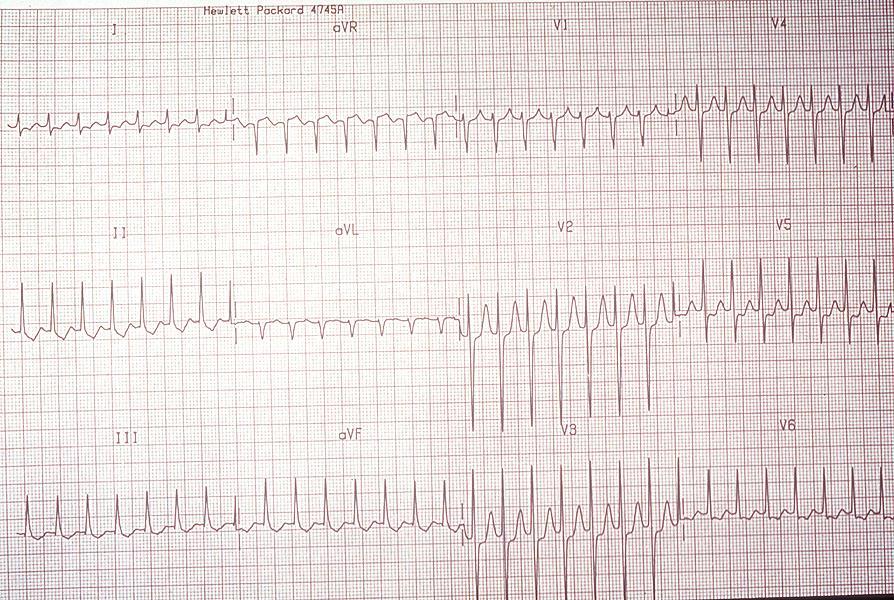
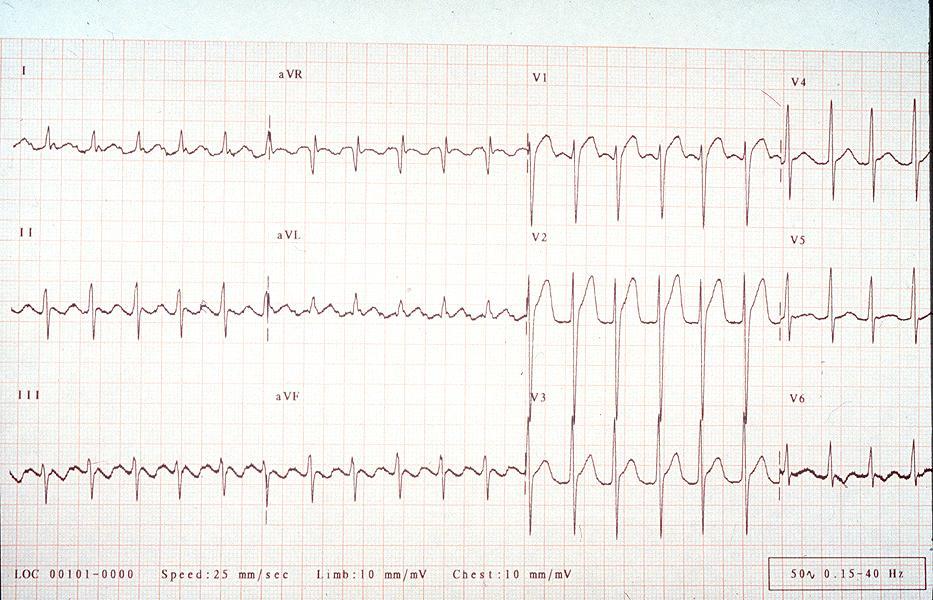
42 Atrial Flutter Rate : Rhythm : P waves : PRI : QRS : Atrial rate / min Ventricular rate variable Atrial rhythm regular Ventricular rhythm usually regular but may be irregular Saw-toothed, flutter waves Not measurable Usually <..10 but may be widened if flutter waves are buried in the QRS complex
43
44 Atrial Flutter Flutter - saw tooth P waves Flutter rate usually about 300/min Best seen in II, III, avf Ventricular rate usually 150/min with 2:1 AV block Rarely 1:1 or higher degree AV block (3:1, 4:1)
45 Tachycardia Regular Irregular Narrow Complex Broad Complex Narrow Complex Broad Complex Sinus Tachycardia or PSVT or Atrial Flutter Ventricular Tachycardia or SVT with Aberrancy or Preexcitation Atrial Fibrillation or Atrial Flutter with varying Block or Multifocal AT Polymorphic VT or Torsade De Pointes or Preexited AF


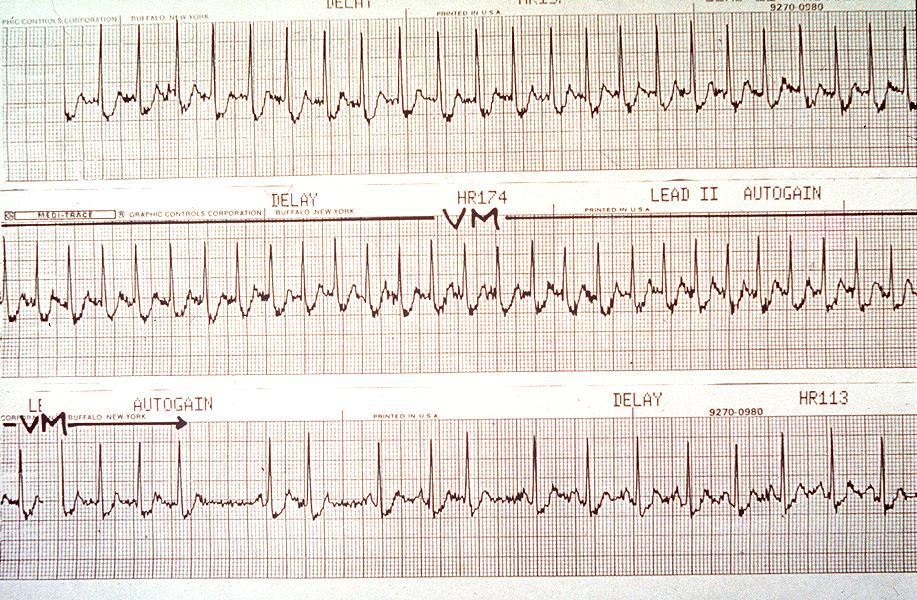
46 Three Variations of Atrial Fibrillation Atrial Fibrillation Lead II Atrial Fibrillation With Slow Ventricular Response V 1 Atrial Fibrillation With Regular Ventricular Response V 1
47 Absent P waves Atrial Fibrillation Chaotic irregular baseline - fibrillatory waves Irregularly irregular RR cycles - fast or slow AF Wide QRS due to aberrancy may occur intermittently (Ashman s phenomenon)
48
49 Narrow Complex Tachycardia Algorithm Step 1 : Access the patient Step 2 : Identify the arrhythmia Step 3 : Treat the arrhythmia
50 Assess the patient for Serious Signs and Symptoms Chest pain / AMI Shortness of breath / CHF Hypotension Decreased level of consciousness Shock
51 Treatment Unstable Synchronised Cardioversion 100 J, 200 J, 300 J, 360 J SVT and Atrial Flutter start with 50 J Stable Valsalva maneuver Carotid sinus massage Drugs
52
53 Narrow Complex Tachycardia Narrow Narrow Complex Complex Tachycardia Tachycardia Atrial Atrial fibrillation fibrillation Atrial Atrial flutter flutter Paroxysmal Paroxysmal supraventricular supraventricular tachycardia tachycardia (PSVT) (PSVT) Use Use rate rate controlled controlled drugs drugs eg: eg: amiodarone, amiodarone, Diltiazem, Diltiazem, Verapamil Verapamil or or Digoxin. Digoxin. Consider Consider anti-coagulation/aspirin anti-coagulation/aspirin Vagal Vagal maneuvers maneuvers * either drug depending on availability and experience * * Adenosine Adenosine 6 6 mg mg rapid rapid IV IV push push Adenosine Adenosine 12mg 12mg rapid rapid iv iv push push * * Verapamil Verapamil 1mg 1mg / / min min (up (up to to max max mg) mg)
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Diagnosis and Management of Acute Myocardial Infarction
 Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Arrhythmias. A/Prof Drew Richardson. The Canberra Hospital May MB BS (Hons) FACEM Grad CertHE MD
 FACEM Grad CertHE MD") Arrhythmias A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Recognise the features of the common nonlethal arrhythmias Describe the emergency treatment
Arrhythmias A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Recognise the features of the common nonlethal arrhythmias Describe the emergency treatment
Acute Coronary Syndrome
 Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
ST Elevation Myocardial Infarction (STEMI) Reperfusion Order Set
 Reperfusion Order Set") Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
Final Written Exam ASHI ACLS
 Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient
 MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
2018 Acute Coronary Syndrome. Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute
 2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
ACLS Emergency Cardiac Drug Therapy (bolded = changes based on 2005 AHA ACLS Guidelines) revised 01/18/07
 revised 01/18/07") Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Myocardial infarction
 CHAPTER-I CARDIOVASCULAR SYSTEM Myocardial infarction SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. Venugopal Pharm.D Assistant Professor Department of Pharm.D Kriahna Teja Pharmacy College,Tirupati. Definition
CHAPTER-I CARDIOVASCULAR SYSTEM Myocardial infarction SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. Venugopal Pharm.D Assistant Professor Department of Pharm.D Kriahna Teja Pharmacy College,Tirupati. Definition
Acute Arrhythmias in the Hospitalized Patient
 Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016
 CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016 + OBJECTIVES Diagnosis and management of ACS When to liaise with tertiary centre Complications of ACS Tachyarrhythmias Bradyarrhythmias
CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016 + OBJECTIVES Diagnosis and management of ACS When to liaise with tertiary centre Complications of ACS Tachyarrhythmias Bradyarrhythmias
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
12 Lead ECG Interpretation: The Basics and Beyond
 12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
A Review of Cardiac Pathophysiology and EKG. Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS
 A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Chest Pain. Dr. Amitesh Aggarwal. Department of Medicine
 Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Chapter 03: Sinus Mechanisms Test Bank MULTIPLE CHOICE
 Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
When the learner has completed this module, she/he will be able to:
 Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
Cardiac Drugs: Chapter 9 Worksheet Cardiac Agents. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate.
 Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
ANTI-ARRHYTHMICS AND WARFARIN. Dr Nithish Jayakumar
 ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Acute Myocardial Infarction. Willis E. Godin D.O., FACC
 Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Practitioner Education Course
 2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
Rate: The atrial and ventricular rates are equal; heart rate is greater than 100 bpm (usually between bpm).
.") Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
ACLS Study Guide for Precourse Self-Assessment
 20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
Pre Hospital and Initial Management of Acute Coronary Syndrome
 Pre Hospital and Initial Management of Acute Coronary Syndrome Dr. Muhammad Fadil, SpJP 3rd SymCARD 2013 Classification of ACS ESC Guidelines for the management of Acute Coronary Syndrome in patients without
Pre Hospital and Initial Management of Acute Coronary Syndrome Dr. Muhammad Fadil, SpJP 3rd SymCARD 2013 Classification of ACS ESC Guidelines for the management of Acute Coronary Syndrome in patients without
Don t Forget the Basics
 Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 26 Caring for Clients with Coronary Heart Disease and Dysrhythmias Coronary Heart Disease (CHD) Leading
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 26 Caring for Clients with Coronary Heart Disease and Dysrhythmias Coronary Heart Disease (CHD) Leading
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
2018 HPN Provider Summary Guide. Adult Cardiology Patients (18 Years and Older) Referral Guidelines
 Referral Guidelines") 12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
Acute myocardial infarction (AMI) and unstable angina
 and unstable angina") Part 8: Stabilization of the Patient With Acute Coronary Syndromes Acute myocardial infarction (AMI) and unstable angina (UA) are part of a spectrum of clinical disease collectively identified as acute
Part 8: Stabilization of the Patient With Acute Coronary Syndromes Acute myocardial infarction (AMI) and unstable angina (UA) are part of a spectrum of clinical disease collectively identified as acute
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies
 Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug