Management of Arrhythmia Syndromes in the Newborn and Very Young Child: Unique Risks & Barriers in this Age Population
|
|
|
- Sylvia Atkins
- 6 years ago
- Views:
Transcription



1 Management of Arrhythmia Syndromes in the Newborn and Very Young Child: Unique Risks & Barriers in this Age Population Mitchell Cohen, MD FACC FHRS Co-Director Heart Center Chief of Pediatric Cardiology Phoenix Children s Hospital Clinical Professor of Child Health University of Arizona College of Medicine-Phoenix
2 Disclosures: None
3 Channelopathies in the Young Long QT Syndrome Catecholamine Polymorphic VT Brugada Syndrome Short QT
4 Arrhythmia Syndromes in the VERY Young Challenges in diagnosing channelopathy conditions in newborns Management of neonatal channelopathies is a serious problem Generates major anxiety to families and physicians Treatment ranges from conservative management to more aggressive and invasive approaches

5 LONG QT SYNDROME
6 Diagnosing LQT is easy, when..
7 Challenges in Diagnosing LQTS Electrocardiogram Variability 30% of patients with gene-positive LQT mutations have a QTc that overlapsnormal healthy children % of healthy individuals have a QTc above a value of 440 msec Difficult to make EKG diagnosis before DOL #4 A QTc >500 msec diagnosis is easy, the challenges often occur in the QTc msec > moving beyond the EKG
8 Challenges in Diagnosing LQTS Disease Variability Approximately 30% of patients with LQT mutations will never have a symptom. Clinical signs, symptoms, and ECG characteristics do not adequately differentiate subtypes of LQTS. Differentiating LQTS subtype may help risk prediction & aid in treatment options.



9 genotype patients 75%

10 LQT Outcomes in the 1 st Year of Life
11 3,323 Infants with LQT in the 1 st year of life SCD (20) Aborted Cardiac Syncope (34) No LQT Event (16) symptoms 8 F All had QTc 500 4/20 had an earlier events 2.3 x risk of ACA/SCD between 1-10 year of age Not associated with ACA/LQT related SCD Syncope within last 2 years and a QTc 500 increased risk SCD within 1 st Yr (3,253) Beta-blockers risk reduction of >65% in this sub-cohort Beta-blockers should be first line of therapy Beta blockers are not ALWAYS effective in the young
12 Cumulative Probability of ACA/LQT Related Death QTc >500, female sex, HR < 100 predictors of cardiac events

13 Infants are Unique Children are not small adults Infants are not small children Symptomatic infants with LQT are HIGH RISK Tend to be sicker and can t vocalize symptoms Beta-blockers are not uniformly 100% protective ICDs are a challenge to implant LCSD may be reasonable, but the infant is in a state of rapidly evolving autonomic development (sleep cycle, sleep position, barorecpetors)
14 Scenario #1: My Pragmatic Approach to Diagnosing and Managing LQT in the Young Child A parent has a known LQT diagnosis (genotype known) Any fetal issues VT? Bradycardia? YES Assume same diagnosis Management Based on Clinical Situation AWAITING GENETIC TESTING CONFIRMATION
15 Scenario #1: My Pragmatic Approach to Diagnosing and Managing LQT in the Young Child A parent has a known LQT diagnosis (genotype known) Genetic Testing (cascade testing pending) Close Observation (Don t rush discharge) Any fetal issues VT? Bradycardia? NO ECG Telemetry Holter (All Normal) Frequent Follow-Up (syncope awareness) YES Assume same diagnosis Management Based on Clinical Situation Avoid QT prolonging medications AWAITING GENETIC TESTING
16 The Nursery stable management Anticipatory Questions & Guidance o o o o o o o o o o o o o What is the QT interval? What is the heart rate? Is the patient having any significant bradycardia? Is the patient having any ventricular arrhythmias? How long to watch in the nursery/nicu? What is the disposition (how far do they live)? What medications to start? CPR training for the parents? Who will be giving the meds? Dose adjustment for weight gain? How is the baby feeding (breast?) Medications to avoid What to tell the pediatrician
17 Scenario #1: My Pragmatic Approach to Diagnosing and Managing LQT in the Young Child A parent has a known LQT diagnosis (genotype known) Any fetal issues VT? Bradycardia? NO ECG Telemetry Holter Abnormal Findings Beta-blockers Pacemaker ICD LCSD Lido/Mexilitine Magnesium Observation Management Based on Clinical Situation AWAITING GENETIC TESTING
18 Scenario #2: My Pragmatic Approach to Diagnosing and Managing LQT in the Young Child No concerning family history of a channelopathy ECG obtained for incidental reasons *patient is completely asymptomatic QT Prolongation (<480) QT Prolongation (>480) QT Prolongation (>550) +/- Beta-blockers reassess at 1 year Close Observation Genetic Testing Avoid QT meds Frequent Follow-up Beta-blockers Won t be asymptomatic for long Manage accordingly
 Beta-blockers Pacemaker ICD Left cardiac sympathetic denervation Lido/Mexilitine")
19 Scenario #3: My Pragmatic Approach to Diagnosing and Managing LQT in the Young Child No concerning family history of a channelopathy Normal fetal course ECG obtained because someone noticed: Bradycardia AV block Non-sustained VT QT prolonged Bizarre T waves Non-sustained VT (TdP) Beta-blockers Pacemaker ICD Left cardiac sympathetic denervation Lido/Mexilitine Magnesium


20 Don t Forget to Do a Physical Exam Timothy Syndrome Spontaneous mutation in CACNA1C. QT prolongation Fingers and toes syndactyly Thin upper lip Autism, developmental delay



21 Occurrence of Gene-Specific Triggers Percent EXERCISE EMOTION REST 0 LQT 1 LQT 2 LQT 3 LQT1 LQT2 LQT3 Circ 2001;103:89-95


22 No Sleep Do Not Forget Mom in Hereditary LQT

23 Approach to the Asymptomatic Young Patient with LQT

24 Not All Beta-Blockers Are Equal Atenolol, Nadolol, Metoprolol, Propanolol LQT2: Nadolol only BB significant risk-reduction in 1 st cardiac event LQT1: no difference in 1 st -cardiac event amongst 4 BB Propanolol the least effective against recurrent cardiac events

25 Not All Beta-Blockers Are Equal Nadolol, Metoprolol, Propanolol Evaluated only LQT 1 & 2 Patients Excluded anyone on BB < 1 year of age Propanolol had the greatest effect on QTc shortening Propanolol & Nadolol equally effective Metroprolol should NOT be used for symptomatic LQT 1 or LQT 2
 Anti-arrhythmics procainamide, amiodarone, sotalol Anti-histamine astemizole, terfenedine Anti-fungal & anti-microbial ketoconazole trimetheprim/sulfa Psychotropic medications")
26 Management: Drug Avoidance in Long QT AVOID: Certain drugs may provoke life-threatening arrhythmias in patients with LQT ( Anti-arrhythmics procainamide, amiodarone, sotalol Anti-histamine astemizole, terfenedine Anti-fungal & anti-microbial ketoconazole trimetheprim/sulfa Psychotropic medications haloperidol, tricyclics Avoid nonessential OTC medications in LQT
 Tends to cause more bradycardia, BB OK?")
27 Long QT3 (gain function Na channel) Most of what we have talked about regarding BB has related to LQT 1 & 2. Long QT is NOT one disease entity Genotype & phenotype differences (age/sex) Tends to cause more bradycardia, BB OK? Multicenter Study:406 LQT3 pts (Wilde A Circ 2016) Followed LQT3 patients after 1 year 12 patients symptomatic in 1 st year-of-life 7 syncope 6 had ACA (4 died) Symptomatic LQT3 in year 1 very concerning
28 Approach to the Symptomatic Young Patient with LQT Are we dealing with bradycardia? Sinus bradycardia? 2:1 AV block? Are we dealing with VT? Pause-dependent? How bad is the QT? >500 msec? >600 msec?

29 Challenging Case #1 Term newborn at 48 hours noted to have bradycardia (85 bpm) and some respiratory distress. Also noted by the OB to have some bradycardia at 30 weeks gestation. No family history of syncope or SCD

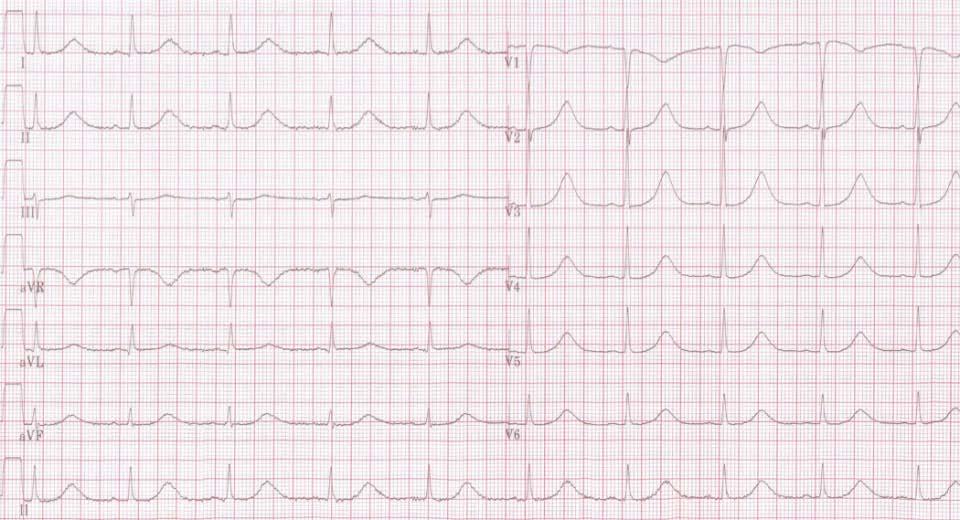
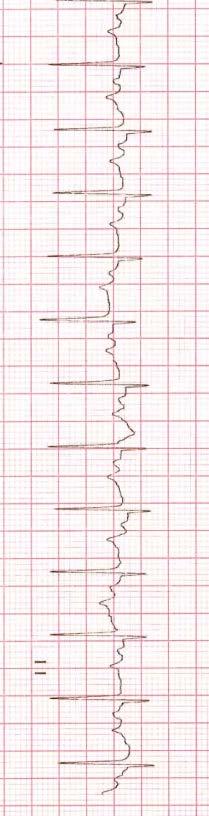
30 ECG in age of 2 days

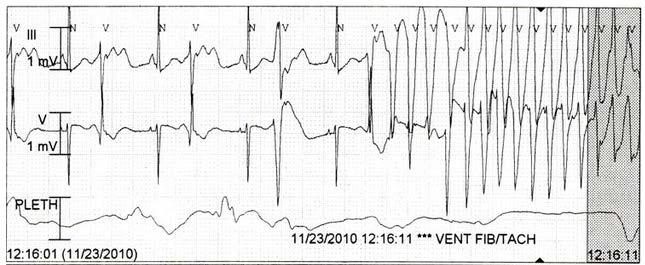
31 30 minute after arrival in ICU Defibrillation Intubation Chest compressions (brief)
32 Options Beta-blockers Mexilitine Beta-blockers and Mexilitine Beta-blockers and pacemaker Pacemaker only Left sympathetic denervation ICD Combination of the above All of the above
33 Clinical Course IV beta-blockers (Esmolol 100ug/kg/min) No further episodes of TdP IV lidocaine given (? shortening of QT) Suspicious this was LQT 3 Mexiltine added to propanolol


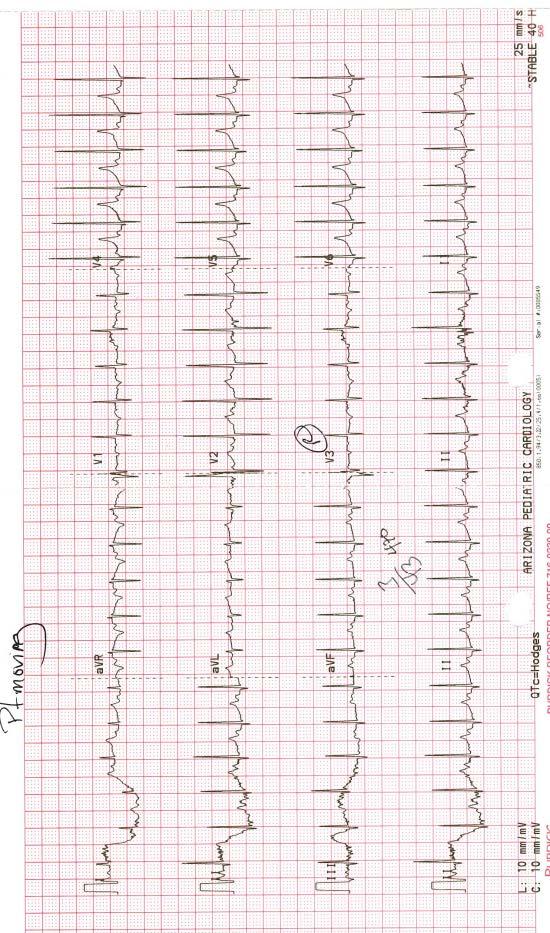
34 Follow-Up EKG SCN5A 9c.5314C>G QTc msec Stayed in hospital for 1 month No further episodes Doing well
35 Challenging Case #2 Called from a remote clinic with a 37 week 2.7 kg baby born via emergent c/s secondary to bradycardia. Bradycardia lasted for about 90 min and now the HR has returned to 130 bpm (regular) and the neonate appears well with a normal cardiovascular examination. Baby is transferred to the NICU at the children s hospital clinically remains well- no further bradycardia over a period of 3 days

36 Electrocardiogram (immediately after birth)
37 Family History: 2 older sisters both healthy, mom has a history of vagal-like events a number of years ago and a seizure when she was 16. No other family history of syncope, seizures, sudden cardiac death. Physical Examination: 2.7 kg, HR 138, BP 62/38 Normal examination Echocardiogram: structurally normal heart; excellent bi-ventricular function. Laboratory Studies: Electrolytes Normal

38 While getting a rhythm strip..

39

40 D.O.L #4 while on telemetry.. that was it never happened again Heart rate maybe a little slower, but not necessarily true pause-dependent TdP Started IV Esmolol
41 Electrocardiogram (DOL #5)
42 Options Beta-blockers Beta-blockers and Mexilitine Beta-blockers and pacemaker Pacemaker only Left sympathetic denervation ICD Combination of the above All of the above Pray your week of service ends today
43 Options Beta-blockers Beta-blockers and Mexilitine Beta-blockers and pacemaker Pacemaker only Left sympathetic denervation ICD Combination of the above All of the above Pray your week of service ends today
44 Gene Test: KCNH2 (LQT 2) Continue on propanolol 4mg/kg/day Left AAI paced at bpm At age 4 years (still asymptomatic) routine interrogation of her PM early ventricular couplets noted. Underwent PM removal, addition of an epicardial coil, ICD system Changed to nadolol No events in the last year
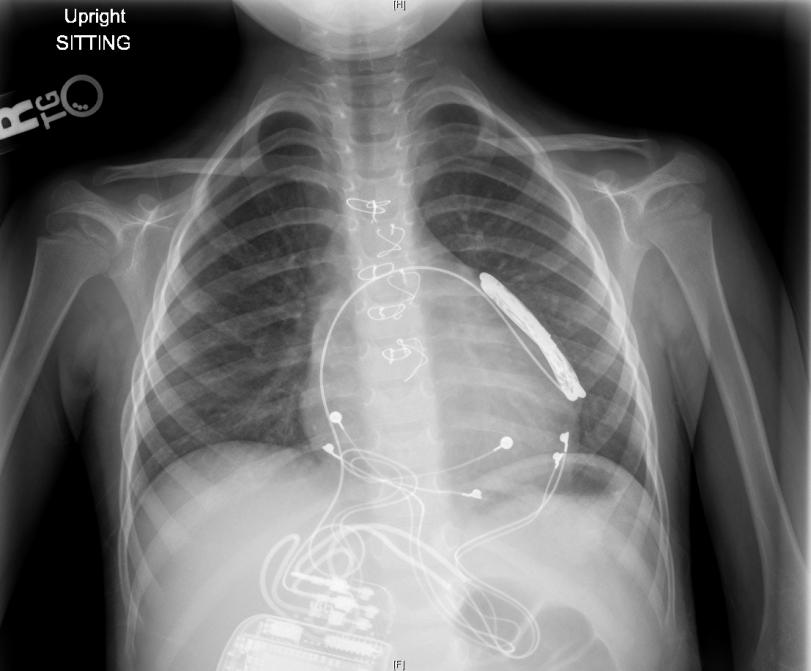
45
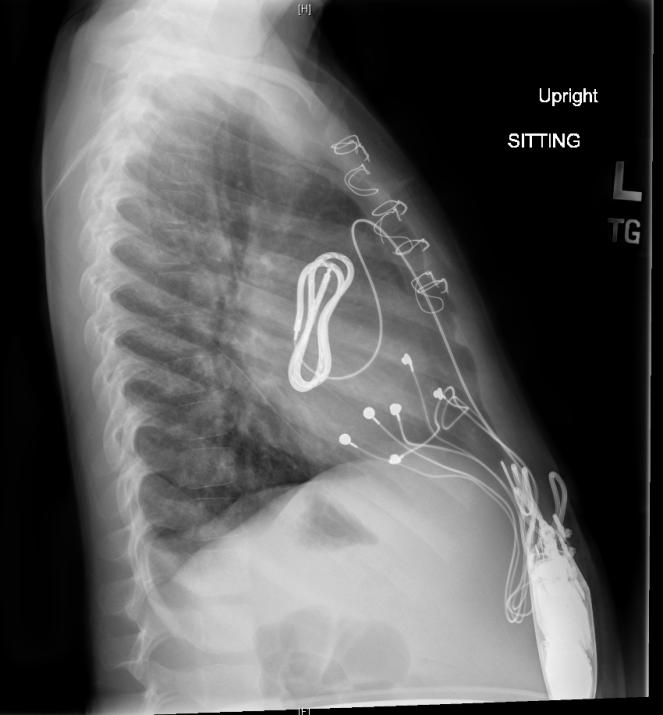
46
 N=8 (67%) received a permanent pacemaker N=3 (25%)")
47 Long QT with 2:1 AV block is rare 4.5% of congenital LQT diagnosis 12 patients diagnosed DOL #1 (QTc range msec) N=8 (67%) received a permanent pacemaker N=3 (25%) received ICD for TdP while on beta-blockers No mortality QTc shortens overtime even in initially high-risk patients

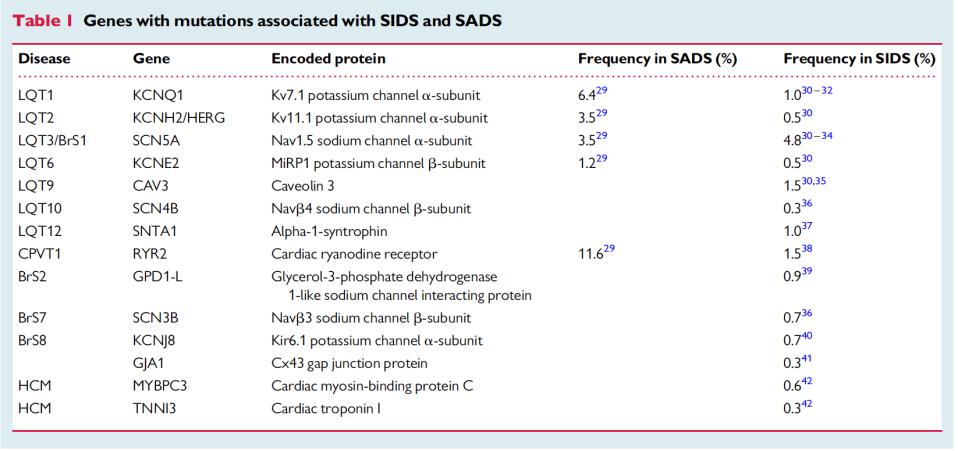
48 Can we go from Sudden Cardiac Death to Sudden Infant Death?

49 Despite the drastic reduction still the 3 rd most common cause of infant mortality in the US
50 Sudden Infant Death Syndrome and Long QT Syndrome Zealots Naysayers



51 Physiological Factors Quiet sleep prolongs the QT interval Pediatr Res 1979;13: QTc significantly shortens during quiet sleep supine but not prone Pediatrics 2003
52 Peak Incidence months Circ 1982


53 Physical & Emotional Stress Can Prolong the QT
.")
54 clinical retrospective Link between SIDS & LQT 42 sets of parents with at least one infant with SIDS QT prolongation was present in at least one member of 11 (26%). In families where a parent had prolongation of QT interval, 36% of siblings also had QT prolongation

55 clinical prospective link between SIDS & LQT
56 ODDS RATIO FOR SCD (QTc >440 msec) Females:33 Males: 47

57 Postmortem molecular analysis of 93 SIDS victims Searched for SCN5A ONLY 2 mutations 4 week-old and 6 week old SIDS attributable to 2% mutations in SCN5A


58 Guthrie Cards N=19 cases of SCD in New Zealand 6/19 (31%) identified as having a channelopathy
59



60 close to 1,000 molecular autopsy SIDS cases 1 in 5 SIDS victims caries a mutation of a cardiac related ion-channel gene defect Genetic analysis should be performed in cases of sudden infant death syndrome and sudden cardiac death


61
Tailored therapy in long QT syndrome
 Tailored therapy in long QT syndrome Dominic Abrams St. Bartholomew s & Great Ormond Street Hospitals London, UK Disclosures None Tailored therapy in long QTS Which patients should have tailored therapy...?...
Tailored therapy in long QT syndrome Dominic Abrams St. Bartholomew s & Great Ormond Street Hospitals London, UK Disclosures None Tailored therapy in long QTS Which patients should have tailored therapy...?...
CONGENITAL LONG QT SYNDROME(CLQTS) ASSOCIATED WITH COMPLETE ATRIOVENTRICULAR BLOCK. A CASE REPORT.
 ASSOCIATED WITH COMPLETE ATRIOVENTRICULAR BLOCK. A CASE REPORT.") CONGENITAL LONG QT SYNDROME(CLQTS) ASSOCIATED WITH COMPLETE ATRIOVENTRICULAR BLOCK. A CASE REPORT. SAHA Annual Congress 2017. Samkelo Jiyana, Adele Greyling, Andile Nxele, ZM,Makrexeni,L.Pepeta. BACKGROUND
CONGENITAL LONG QT SYNDROME(CLQTS) ASSOCIATED WITH COMPLETE ATRIOVENTRICULAR BLOCK. A CASE REPORT. SAHA Annual Congress 2017. Samkelo Jiyana, Adele Greyling, Andile Nxele, ZM,Makrexeni,L.Pepeta. BACKGROUND
WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY
 Learning Objectives to Disclose: To CRITIQUE the ICD and its role in the treatment of BrS, CPVT, and LQTS WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY Conflicts of Interest to Disclose: Consultant
Learning Objectives to Disclose: To CRITIQUE the ICD and its role in the treatment of BrS, CPVT, and LQTS WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY Conflicts of Interest to Disclose: Consultant
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification
 Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Pearls of the ESC/ERS Guidelines 2015 Channelopathies
 Pearls of the ESC/ERS Guidelines 2015 Channelopathies Carina Blomstrom Lundqvist Dept Cardiology, Uppsala, Sweden Content 2015 ESC Guidelines for the Management of Patients with Ventricular Arrhythmias
Pearls of the ESC/ERS Guidelines 2015 Channelopathies Carina Blomstrom Lundqvist Dept Cardiology, Uppsala, Sweden Content 2015 ESC Guidelines for the Management of Patients with Ventricular Arrhythmias
FANS Paediatric Pathway for Inherited Arrhythmias*
 FANS Paediatric Pathway for Inherited Arrhythmias* The pathway is based on the HRS/EHRA/APHRS Expert Consensus Statement on the Diagnosis and Management of Patients with Inherited Primary Arrhythmia Syndromes
FANS Paediatric Pathway for Inherited Arrhythmias* The pathway is based on the HRS/EHRA/APHRS Expert Consensus Statement on the Diagnosis and Management of Patients with Inherited Primary Arrhythmia Syndromes
Long Q. Long QT Syndrome. A Guide for
 Long Q Long QT Syndrome A Guide for Introduction Long QT syndrome (LQTS) is a genetic heart disorder due to the malfunction of cardiac ion channels that results in 4,000 deaths annually in the United States
Long Q Long QT Syndrome A Guide for Introduction Long QT syndrome (LQTS) is a genetic heart disorder due to the malfunction of cardiac ion channels that results in 4,000 deaths annually in the United States
Long QT Syndrome in Children in the Era of Implantable Defibrillators
 Journal of the American College of Cardiology Vol. 50, No. 14, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.05.042
Journal of the American College of Cardiology Vol. 50, No. 14, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.05.042
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Primary Therapy for High Risk LQT Patients Should Be an ICD
 Primary Therapy for High Risk LQT Patients Should Be an ICD Raul Weiss MD, FAHA, FACC, FHRS, CCDS Director, Electrophysiology Fellowship Program Associate Professor of Medicine The Ohio State University
Primary Therapy for High Risk LQT Patients Should Be an ICD Raul Weiss MD, FAHA, FACC, FHRS, CCDS Director, Electrophysiology Fellowship Program Associate Professor of Medicine The Ohio State University
When VF is the endpoint, wait and see is not always the best option.
 Being free of symptoms does not necessarily mean free of arrhythmias. This Holter is from a asymptomatic 48 years old female with LQT2 When VF is the endpoint, wait and see is not always the best option.
Being free of symptoms does not necessarily mean free of arrhythmias. This Holter is from a asymptomatic 48 years old female with LQT2 When VF is the endpoint, wait and see is not always the best option.
Patient Resources: Cardiac Channelopathies
 Patient Resources: Cardiac Channelopathies Overview of Cardiac Channelopathies: CPVT, Long QT Syndrome and Brugada Syndrome Heart muscle cells contract because of movement of certain molecules (called
Patient Resources: Cardiac Channelopathies Overview of Cardiac Channelopathies: CPVT, Long QT Syndrome and Brugada Syndrome Heart muscle cells contract because of movement of certain molecules (called
Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation?
 Innovations in Interventional Cardiology and Electrophysiology Thessaloniki 2014 Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation? K. Letsas, MD, FESC
Innovations in Interventional Cardiology and Electrophysiology Thessaloniki 2014 Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation? K. Letsas, MD, FESC
Acute Arrhythmias in the Hospitalized Patient
 Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Adult Complexities of the Channelopathies
 Adult Complexities of the Channelopathies Andrew Krahn MD FHRS Sauder Family and Heart and Stroke Foundation Chair in Cardiology Paul Brunes Chair in Heart Rhythm Disorders University of British Columbia
Adult Complexities of the Channelopathies Andrew Krahn MD FHRS Sauder Family and Heart and Stroke Foundation Chair in Cardiology Paul Brunes Chair in Heart Rhythm Disorders University of British Columbia
Silvia G Priori MD PhD
 The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
Prolonged QT Syndromes: Congenital and Acquired
 Prolonged QT Syndromes: Congenital and Acquired April 30, 2014 Elizabeth S. Kaufman, MD I have no financial disclosures. MetroHealth Campus, Case Western Reserve University Prolonged QT Syndromes Congenital
Prolonged QT Syndromes: Congenital and Acquired April 30, 2014 Elizabeth S. Kaufman, MD I have no financial disclosures. MetroHealth Campus, Case Western Reserve University Prolonged QT Syndromes Congenital
Mitchell Cohen MD FACC FHRS Co-Director of the Heart Center Section Chief, Pediatric Cardiology Phoenix Children s Hospital Professor of Child Health
 10 Annoying Reasons an Electrophysiologist Gets Called to the Cardiac ICU Mitchell Cohen MD FACC FHRS Co-Director of the Heart Center Section Chief, Pediatric Cardiology Phoenix Children s Hospital Professor
10 Annoying Reasons an Electrophysiologist Gets Called to the Cardiac ICU Mitchell Cohen MD FACC FHRS Co-Director of the Heart Center Section Chief, Pediatric Cardiology Phoenix Children s Hospital Professor
ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ
 ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ ΣΤΕΛΙΟΣ ΠΑΡΑΣΚΕΥΑÏΔΗΣ ΔΙΕΥΘΥΝΤΗΣ ΕΣΥ Α Καρδιολογική Κλινική ΑΠΘ, Νοσοκομείο ΑΧΕΠΑ, Θεσσαλονίκη NO CONFLICT OF INTEREST Sudden Cardiac Death
ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ ΣΤΕΛΙΟΣ ΠΑΡΑΣΚΕΥΑÏΔΗΣ ΔΙΕΥΘΥΝΤΗΣ ΕΣΥ Α Καρδιολογική Κλινική ΑΠΘ, Νοσοκομείο ΑΧΕΠΑ, Θεσσαλονίκη NO CONFLICT OF INTEREST Sudden Cardiac Death
ICD in a young patient with syncope
 ICD in a young patient with syncope Konstantinos P. Letsas, MD, FESC Second Department of Cardiology Evangelismos General Hospital of Athens Athens, Greece Case presentation A 17-year-old apparently healthy
ICD in a young patient with syncope Konstantinos P. Letsas, MD, FESC Second Department of Cardiology Evangelismos General Hospital of Athens Athens, Greece Case presentation A 17-year-old apparently healthy
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
How to manage a patient with short QT syndrome?
 How to manage a patient with short QT syndrome? Torino, 27 ottobre2012 Carla Giustetto Division of Cardiology University of Torino QT 280 ms QTc 260 ms Narrow, tall and peaked T waves High incidence of
How to manage a patient with short QT syndrome? Torino, 27 ottobre2012 Carla Giustetto Division of Cardiology University of Torino QT 280 ms QTc 260 ms Narrow, tall and peaked T waves High incidence of
The impact of clinical and genetic findings on the management of young Brugada Syndrome patients
 12 ème Congrès Médico-Chirugical de la FCPC 21 au 24 novembre 2015 Schoelcher, Martinique The impact of clinical and genetic findings on the management of young Brugada Syndrome patients Institut du Thorax,
12 ème Congrès Médico-Chirugical de la FCPC 21 au 24 novembre 2015 Schoelcher, Martinique The impact of clinical and genetic findings on the management of young Brugada Syndrome patients Institut du Thorax,
Invasive Risk Stratification: When is it needed?
 Inherited Cardiomyopathies and Channelopathies: Who is at risk for Sudden Cardiac Death? Invasive Risk Stratification: When is it needed? Hung-Fat Tse, MD, PhD Department of Medicine The University of
Inherited Cardiomyopathies and Channelopathies: Who is at risk for Sudden Cardiac Death? Invasive Risk Stratification: When is it needed? Hung-Fat Tse, MD, PhD Department of Medicine The University of
Case Demonstrations in Congenital and Acquired Long QT Syndrome
 Case Demonstrations in Congenital and Acquired Long QT Syndrome Can You Make A Correct ECG Interpretation? Li Zhang, MD; 1-2 G. Michael Vincent, MD 1 1. LQTS Studies, Department t of Medicine i LDS Hospital,
Case Demonstrations in Congenital and Acquired Long QT Syndrome Can You Make A Correct ECG Interpretation? Li Zhang, MD; 1-2 G. Michael Vincent, MD 1 1. LQTS Studies, Department t of Medicine i LDS Hospital,
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Tachycardia Devices Indications and Basic Trouble Shooting
 Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know
 Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
3/17/2014. NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death. Objectives
 NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death Denise Pond BSN, RN The following relationships exist related to this presentation: No Disclosures Objectives Discuss
NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death Denise Pond BSN, RN The following relationships exist related to this presentation: No Disclosures Objectives Discuss
Asymptomatic Long QT. Prof. Dr. Martin Borggrefe Mannheim
 Asymptomatic Long QT Prof. Dr. Martin Borggrefe Mannheim QT interval Distribution of QTc intervals in large population-based studies Viskin S, Heart Rhythm 2009; 6: 711-715 QT interval Distribution of
Asymptomatic Long QT Prof. Dr. Martin Borggrefe Mannheim QT interval Distribution of QTc intervals in large population-based studies Viskin S, Heart Rhythm 2009; 6: 711-715 QT interval Distribution of
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Unknown ECGs for the Clinician
 Unknown ECGs for the Clinician 2016 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board for Medtronic
Unknown ECGs for the Clinician 2016 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board for Medtronic
The Role of Defibrillator Therapy in Genetic Arrhythmia Syndromes
 The Role of Defibrillator Therapy in Genetic Arrhythmia Syndromes RHEA C. PIMENTEL, MD, FACC, FHRS UNIVERSITY OF KANSAS HOSPITAL MID AMERICA CARDIOLOGY AUGUST 19, 2012 Monogenic Arrhythmia Syndromes Mendelian
The Role of Defibrillator Therapy in Genetic Arrhythmia Syndromes RHEA C. PIMENTEL, MD, FACC, FHRS UNIVERSITY OF KANSAS HOSPITAL MID AMERICA CARDIOLOGY AUGUST 19, 2012 Monogenic Arrhythmia Syndromes Mendelian
CHANNELOPATHIES IS GENETIC TESTING ESSENTIAL IN PTS MANAGEMENT
 CHANNELOPATHIES IS GENETIC TESTING ESSENTIAL IN PTS MANAGEMENT Inherited and Rare Cardiac Diseases Unit Heart Center for the Young and Athletes ONASSIS CARDIAC SURGERY CENTRE DIAGNOSIS ION CHANNEL DISEASE
CHANNELOPATHIES IS GENETIC TESTING ESSENTIAL IN PTS MANAGEMENT Inherited and Rare Cardiac Diseases Unit Heart Center for the Young and Athletes ONASSIS CARDIAC SURGERY CENTRE DIAGNOSIS ION CHANNEL DISEASE
Prenatal diagnosis of long QT syndrome: Implications for delivery room and neonatal management
 Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
Cardiac Disease in Organic Acidemias
 Cardiac Disease in Organic Acidemias Kathryn Chatfield, MD, PhD Assistant Professor of Pediatrics Division of Cardiology University of Colorado School of Medicine Children s Hospital Colorado Introduction
Cardiac Disease in Organic Acidemias Kathryn Chatfield, MD, PhD Assistant Professor of Pediatrics Division of Cardiology University of Colorado School of Medicine Children s Hospital Colorado Introduction
Interpretation and Consequences of Repolarisation Changes in Athletes
 Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
Left cardiac sympathectomy to manage beta-blocker resistant LQT patients
 Left cardiac sympathectomy to manage beta-blocker resistant LQT patients Lexin Wang, M.D., Ph.D. Introduction Congenital long QT syndrome (LQTS) is a disorder of prolonged cardiac repolarization, manifested
Left cardiac sympathectomy to manage beta-blocker resistant LQT patients Lexin Wang, M.D., Ph.D. Introduction Congenital long QT syndrome (LQTS) is a disorder of prolonged cardiac repolarization, manifested
Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart.
 Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart. Hanne Rasmusen Consultant cardiologist, PhD Dept. of Cardiology Bispebjerg University Hospital
Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart. Hanne Rasmusen Consultant cardiologist, PhD Dept. of Cardiology Bispebjerg University Hospital
Basics of Structure/Function of Sodium and Potassium Channels Barry London, MD PhD
 Basics of Structure/Function of Sodium and Potassium Channels Barry London, MD PhD University of Pittsburgh Medical Center Pittsburgh, PA International Symposium of Inherited Arrhythmia Disorders and Hypertrophic
Basics of Structure/Function of Sodium and Potassium Channels Barry London, MD PhD University of Pittsburgh Medical Center Pittsburgh, PA International Symposium of Inherited Arrhythmia Disorders and Hypertrophic
Hereditary Cardiovascular Conditions. genetic testing for undiagnosed diseases
 Hereditary Cardiovascular Conditions genetic testing for undiagnosed diseases What is Hypertrophic Cardiomyopathy (HCM)? normal heart heart with hcm Extra or thick heart muscle Typically in the left ventricle
Hereditary Cardiovascular Conditions genetic testing for undiagnosed diseases What is Hypertrophic Cardiomyopathy (HCM)? normal heart heart with hcm Extra or thick heart muscle Typically in the left ventricle
Asaad Khoury 2,3 MD, Monther Boulos 1,3 MD, Mahmoud Suleiman 1,3 MD, Miry Blich 1,3 MD, Michael Eldar 4 MD, Ibrahim Marai 1,3 MD,
 Flecainide therapy suppresses exercise induced ventricular arrhythmias in patients with CASQ2 associated catecholaminergic polymorphic ventricular tachycardia Asaad Khoury 2,3 MD, Monther Boulos 1,3 MD,
Flecainide therapy suppresses exercise induced ventricular arrhythmias in patients with CASQ2 associated catecholaminergic polymorphic ventricular tachycardia Asaad Khoury 2,3 MD, Monther Boulos 1,3 MD,
Rhythm and Blues Drugs and QT Prolongation
 Rhythm and Blues Drugs and QT Prolongation Dr Martin Quinn St Vincents University Hospital Irish Medication Safety Network conference Farmleigh 18 Oct 2013 Drugs and QT Prolongation Anti-psychotic, antidepressant,
Rhythm and Blues Drugs and QT Prolongation Dr Martin Quinn St Vincents University Hospital Irish Medication Safety Network conference Farmleigh 18 Oct 2013 Drugs and QT Prolongation Anti-psychotic, antidepressant,
The patient with electric storm
 The complex patient in the cardiac care unit: The patient with electric storm Helmut U. Klein University of Rochester Medical Center Heart Research Follow-up Program and Isar Heart Center Muenchen Presenter
The complex patient in the cardiac care unit: The patient with electric storm Helmut U. Klein University of Rochester Medical Center Heart Research Follow-up Program and Isar Heart Center Muenchen Presenter
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013
 Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
FANS Long QT Syndrome Investigation Protocol (including suspected mutation carriers)
") Clinical Features FANS Long QT Syndrome Investigation Protocol (including suspected mutation carriers) History Syncope or presyncope compatible with ventricular tachyarrhythmia, especially relating to
Clinical Features FANS Long QT Syndrome Investigation Protocol (including suspected mutation carriers) History Syncope or presyncope compatible with ventricular tachyarrhythmia, especially relating to
Beware the Red Flags in the Management of Syncope
 Beware the Red Flags in the Management of Syncope Mitchell Cohen MD FACC FHRS Co-Director of the Pediatric Heart Program Director of Pediatric Arrhythmia Services Inova Fairfax Children s Hospital President,
Beware the Red Flags in the Management of Syncope Mitchell Cohen MD FACC FHRS Co-Director of the Pediatric Heart Program Director of Pediatric Arrhythmia Services Inova Fairfax Children s Hospital President,
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Professor Eric Schulze-Bahr
 No CoI. Professor Eric Schulze-Bahr Institute for Genetics of Heart Diseases Department of Cardiology and Angiology University Hospital Münster / Germany ICD therapy in asymptomatic or borderline LQTS
No CoI. Professor Eric Schulze-Bahr Institute for Genetics of Heart Diseases Department of Cardiology and Angiology University Hospital Münster / Germany ICD therapy in asymptomatic or borderline LQTS
SEMINAIRES IRIS. Sudden cardiac death in the adult. Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel. 20% 25% Cancers !
 Sudden cardiac death in the adult Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel.! " # $ % Cancers National Vital Statistics Report, Vol 49 (11), Oct. 12, 2001. 20% 25% State-specific
Sudden cardiac death in the adult Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel.! " # $ % Cancers National Vital Statistics Report, Vol 49 (11), Oct. 12, 2001. 20% 25% State-specific
Is There a Genomic Basis to Acquired Channelopathic disease
 Is There a Genomic Basis to Acquired Channelopathic disease Yaniv Bar-Cohen, M.D. Associate Professor of Pediatrics Division of Cardiology / Electrophysiology Children s Hospital Los Angeles Keck School
Is There a Genomic Basis to Acquired Channelopathic disease Yaniv Bar-Cohen, M.D. Associate Professor of Pediatrics Division of Cardiology / Electrophysiology Children s Hospital Los Angeles Keck School
Return to Titanic: Irregular Heart Beats. Ric Samson, MD Children s Heart Center - Nevada
 Return to Titanic: Irregular Heart Beats Ric Samson, MD Children s Heart Center - Nevada The Titanic RMS Titanic largest ship ever built up to that time maiden voyage April 1912 travelling from Southampton
Return to Titanic: Irregular Heart Beats Ric Samson, MD Children s Heart Center - Nevada The Titanic RMS Titanic largest ship ever built up to that time maiden voyage April 1912 travelling from Southampton
Clinical and Electrocardiographic Characteristics of Patients with Brugada Syndrome: Report of Five Cases of Documented Ventricular Fibrillation
 J Arrhythmia Vol 25 No 1 2009 Original Article Clinical and Electrocardiographic Characteristics of Patients with Brugada Syndrome: Report of Five Cases of Documented Ventricular Fibrillation Seiji Takashio
J Arrhythmia Vol 25 No 1 2009 Original Article Clinical and Electrocardiographic Characteristics of Patients with Brugada Syndrome: Report of Five Cases of Documented Ventricular Fibrillation Seiji Takashio
Different indications for pacemaker implantation are the following:
 Patient Resources: ICD/Pacemaker Overview ICD/Pacemaker Overview What is a pacemaker? A pacemaker is a device that uses low energy electrical pulses to prompt the heart to beat whenever a pause in the
Patient Resources: ICD/Pacemaker Overview ICD/Pacemaker Overview What is a pacemaker? A pacemaker is a device that uses low energy electrical pulses to prompt the heart to beat whenever a pause in the
Lee Chee Wan. Senior Consultant Pacing and Cardiac Electrophysiology. GP Symposium 2 nd April 2016
 Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association
 Genetic Testing for Page 1 of 23 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Genetic Testing for Professional Institutional Original Effective Date: August
Genetic Testing for Page 1 of 23 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Genetic Testing for Professional Institutional Original Effective Date: August
Risk for Life-Threatening Cardiac Events in Patients With Genotype-Confirmed Long-QT Syndrome and Normal-Range Corrected QT Intervals
 Journal of the American College of Cardiology Vol. 57, No. 1, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.07.038
Journal of the American College of Cardiology Vol. 57, No. 1, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.07.038
La strategia diagnostica: il monitoraggio ecg prolungato. Michele Brignole
 La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University
 Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University 1. Important and impact of ICD in primary prevention 2. Risk stratification for ICD
Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University 1. Important and impact of ICD in primary prevention 2. Risk stratification for ICD
Are there low risk patients in Brugada syndrome?
 Are there low risk patients in Brugada syndrome? Pedro Brugada MD, PhD Andrea Sarkozy MD Risk stratification in Brugada syndrome In the last years risk stratification in Brugada syndrome has become the
Are there low risk patients in Brugada syndrome? Pedro Brugada MD, PhD Andrea Sarkozy MD Risk stratification in Brugada syndrome In the last years risk stratification in Brugada syndrome has become the
Genetic Testing for Cardiac Ion Channelopathies
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Section: Effective Date: Subsection: Original Policy Date: Subject: Page: Last Review Status/Date: Background
 Genetic Testing for Cardiac Ion Last Review Status/Date: March 2014 Genetic Testing for Cardiac Ion Description Page: 1 of 22 Genetic testing is available for patients suspected of having cardiac ion channelopathies
Genetic Testing for Cardiac Ion Last Review Status/Date: March 2014 Genetic Testing for Cardiac Ion Description Page: 1 of 22 Genetic testing is available for patients suspected of having cardiac ion channelopathies
Clinical Cardiac Electrophysiology
 Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Cardiac Disease in Fatty Acid Oxidation Disorders
 Cardiac Disease in Fatty Acid Oxidation Disorders Kathryn Chatfield, MD, PhD Assistant Professor of Pediatrics Division of Cardiology University of Colorado School of Medicine Children s Hospital Colorado
Cardiac Disease in Fatty Acid Oxidation Disorders Kathryn Chatfield, MD, PhD Assistant Professor of Pediatrics Division of Cardiology University of Colorado School of Medicine Children s Hospital Colorado
Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada
 Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας και Βηματοδότησης BrS: Diagnosis 5:10000 First described
Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας και Βηματοδότησης BrS: Diagnosis 5:10000 First described
BHRS Prep course Pub style Quiz NOT A
 BHRS Prep course Pub style Quiz NOT A Round 1 Quiz questions Common ECG s in CRM Colin Cunnington Over the past 3 months, a 24-yearold man who works as a truck driver has had frequent episodes of pre-syncope
BHRS Prep course Pub style Quiz NOT A Round 1 Quiz questions Common ECG s in CRM Colin Cunnington Over the past 3 months, a 24-yearold man who works as a truck driver has had frequent episodes of pre-syncope
Remote Monitoring & the Smart Home of the 21 Century
 Cardiostim EHRA Europace 2016, Nice - June 8-11, 2016 Remote Monitoring & the Smart Home of the 21 Century Antonio Raviele, MD, FESC, FHRS President ALFA -Alliance to Fight Atrial fibrillation- Venezia
Cardiostim EHRA Europace 2016, Nice - June 8-11, 2016 Remote Monitoring & the Smart Home of the 21 Century Antonio Raviele, MD, FESC, FHRS President ALFA -Alliance to Fight Atrial fibrillation- Venezia
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital
 Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Woo-Sik Yu, M.D. 1, Tae-Hoon Kim, M.D. 2, Jee won Suh, M.D. 1, Seunghwan Song, M.D. 1, Chang Young Lee, M.D. 1, Boyoung Joung, M.D., Ph.D.
 Korean J Thorac Cardiovasc Surg 2015;48:220-224 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) Case Report http://dx.doi.org/10.5090/kjtcs.2015.48.3.220 Thoracoscopic Left Cardiac Sympathetic Denervation
Korean J Thorac Cardiovasc Surg 2015;48:220-224 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) Case Report http://dx.doi.org/10.5090/kjtcs.2015.48.3.220 Thoracoscopic Left Cardiac Sympathetic Denervation
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Brugada Syndrome: An Update
 Brugada Syndrome: An Update Osama Diab Associate professor of Cardiology Ain Shams university, Cairo, Egypt Updates Mechanism and Genetics Risk stratification Treatment 1 Brugada syndrome causes 4 12%
Brugada Syndrome: An Update Osama Diab Associate professor of Cardiology Ain Shams university, Cairo, Egypt Updates Mechanism and Genetics Risk stratification Treatment 1 Brugada syndrome causes 4 12%
Don t Forget the Basics
 Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
SHOCK THE PATIENT. Disclosures. Goals of the Talk. Tachyarrhythmias- Unstable 11/7/2017
 Disclosures Common Heart Rhythms in the Hospital Research Support: NIH, PCORI, Medtronic, Cardiogram Consulting: InCarda, Johnson & Johnson, Lifewatch Equity: InCarda Gregory M Marcus, MD, MAS Associate
Disclosures Common Heart Rhythms in the Hospital Research Support: NIH, PCORI, Medtronic, Cardiogram Consulting: InCarda, Johnson & Johnson, Lifewatch Equity: InCarda Gregory M Marcus, MD, MAS Associate
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Case studies in Channelopathies
 Case studies in Channelopathies FABRICE CHOUTY, MD MEDICAL DIRECTOR HANNOVER-LIFE RE, PARIS (F) INTRODUCTION Thanks to the invasive electrophysiology and the progress of imaging techniques as well as the
Case studies in Channelopathies FABRICE CHOUTY, MD MEDICAL DIRECTOR HANNOVER-LIFE RE, PARIS (F) INTRODUCTION Thanks to the invasive electrophysiology and the progress of imaging techniques as well as the
Bryan Heart. Unknown ECGs for the Clinician. Disclaimer 9/2/2015
 Bryan Heart Unknown ECGs for the Clinician 2015 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board
Bryan Heart Unknown ECGs for the Clinician 2015 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board
Syncope. Charles DeBerardinis, DO Iredell Health Systems
 Syncope Charles DeBerardinis, DO Iredell Health Systems Syncope Syncope loss of consciousness Vertigo sensation of motion Drop attacks fall without loss of consciousness seizure Syncope Constatino n=670
Syncope Charles DeBerardinis, DO Iredell Health Systems Syncope Syncope loss of consciousness Vertigo sensation of motion Drop attacks fall without loss of consciousness seizure Syncope Constatino n=670
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
Arrhythmias. Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium.
 Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Stage I: Binning Dashboard
 Stage I: Binning Dashboard P[ GENE/GENE PANEL: KCNQ1, KCNH2, SCN5A DISORDER: Romano-Ward Long QT Syndrome HGNC ID: 6294, 6251, 10593 OMIM ID: 192500, 613688, 603830 ACTIONABILITY PENETRANCE 1. Is there
Stage I: Binning Dashboard P[ GENE/GENE PANEL: KCNQ1, KCNH2, SCN5A DISORDER: Romano-Ward Long QT Syndrome HGNC ID: 6294, 6251, 10593 OMIM ID: 192500, 613688, 603830 ACTIONABILITY PENETRANCE 1. Is there
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
The patient with (without) an ICD and heart failure: Management of electrical storm
 an ICD and heart failure: Management of electrical storm") ISHNE Heart Failure Virtual Symposium April 2008 The patient with (without) an ICD and heart failure: Management of electrical storm Westfälische Wilhelms-Universität Münster Günter Breithardt, MD, FESC,
ISHNE Heart Failure Virtual Symposium April 2008 The patient with (without) an ICD and heart failure: Management of electrical storm Westfälische Wilhelms-Universität Münster Günter Breithardt, MD, FESC,
Wojciech Szczepański, MD, PhD Department of Pediatrics, Endocrinology, Diabetology with Cardiology Division Medical University of Bialystok
 Channelopathies: - Long QT syndrome - Short QT syndrome - Brugada syndrome - Early repolarization syndrome - Catecholaminergic polymorphic ventricular tachycardia Wojciech Szczepański, MD, PhD Department
Channelopathies: - Long QT syndrome - Short QT syndrome - Brugada syndrome - Early repolarization syndrome - Catecholaminergic polymorphic ventricular tachycardia Wojciech Szczepański, MD, PhD Department
Name of Presenter: Marwan Refaat, MD
 NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010 I have no actual or potential conflict of interest in relation
NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010 I have no actual or potential conflict of interest in relation
An Approach to the Patient with Syncope. Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva
 An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
Drug induced QT prolongation and Torsades de Pointes (TdP) Mark Friesen, PharmD March 13, 2013
 Mark Friesen, PharmD March 13, 2013") Drug induced QT prolongation and Torsades de Pointes (TdP) Mark Friesen, PharmD March 13, 2013 None Conflict of Interest TdP: Learning objectives To review the pathophysiology of QT prolongation and TdP
Drug induced QT prolongation and Torsades de Pointes (TdP) Mark Friesen, PharmD March 13, 2013 None Conflict of Interest TdP: Learning objectives To review the pathophysiology of QT prolongation and TdP
Acquired conduction disturbance in structurally normal heart in children. Mi Young Han, M.D.,PhD. Kyung Hee University Hospital
 Acquired conduction disturbance in structurally normal heart in children Mi Young Han, M.D.,PhD. Kyung Hee University Hospital 1 Incidence Cardiac conduction disturbances detected in a pediatric population
Acquired conduction disturbance in structurally normal heart in children Mi Young Han, M.D.,PhD. Kyung Hee University Hospital 1 Incidence Cardiac conduction disturbances detected in a pediatric population
QUESTION: In a patient with different QT intervals, which one will give the highest prognostic accuracy? REPLY:
 QUESTION: In a patient with different QT intervals, which one will give the highest prognostic accuracy? REPLY: First, there are two possibilities: I) It is not known, if the patient (subject) presented
QUESTION: In a patient with different QT intervals, which one will give the highest prognostic accuracy? REPLY: First, there are two possibilities: I) It is not known, if the patient (subject) presented
Syncope Update Dr Matthew Lovell, Consultant in Cardiology
 Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Idiopathic Ventricular Tachycardia Need for an Update in EHRA/HRS Consensus?
 Idiopathic Ventricular Tachycardia Need for an Update in EHRA/HRS Consensus? Arash Arya, M.D. Department of Interventional Electrophysiology Heart Center University of Leipzig Disclosures: NONE Idiopathic
Idiopathic Ventricular Tachycardia Need for an Update in EHRA/HRS Consensus? Arash Arya, M.D. Department of Interventional Electrophysiology Heart Center University of Leipzig Disclosures: NONE Idiopathic
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
How agressively should we treat asymptomatic patients with Brugada syndrome. Josep Brugada Medical Director Hospital Clínic, University of Barcelona
 How agressively should we treat asymptomatic patients with Brugada syndrome Josep Brugada Medical Director Hospital Clínic, University of Barcelona The ECG in Brugada syndrome - Prolonged PR - RBBB - ST
How agressively should we treat asymptomatic patients with Brugada syndrome Josep Brugada Medical Director Hospital Clínic, University of Barcelona The ECG in Brugada syndrome - Prolonged PR - RBBB - ST
Antony French Consultant Cardiologist & Electrophysiologist
 Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Long QT syndrome diagnosed in the postpartum period (RCD code: VII-V-1A.2)
") Journal of Rare Cardiovascular Diseases 2014; 1 (6): 15 20 www.jrcd.eu CASE REPORTS Cardiovascular diseases in pregnancy Long QT syndrome diagnosed in the postpartum period (RCD code: VII-V-1A.2) Piotr
Journal of Rare Cardiovascular Diseases 2014; 1 (6): 15 20 www.jrcd.eu CASE REPORTS Cardiovascular diseases in pregnancy Long QT syndrome diagnosed in the postpartum period (RCD code: VII-V-1A.2) Piotr
Clinical Guidance. Extrasystoles in the neonatal period. Author: Peter Lillitos
 1 Clinical Guidance Extrasystoles in the neonatal period Author: Peter Lillitos Contents Page 2: Definition of extrasystoles/ectopic beats Page 3: Algorithm of management Page 4-5: Ordering investigations
1 Clinical Guidance Extrasystoles in the neonatal period Author: Peter Lillitos Contents Page 2: Definition of extrasystoles/ectopic beats Page 3: Algorithm of management Page 4-5: Ordering investigations
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the