The Role of Defibrillator Therapy in Genetic Arrhythmia Syndromes
|
|
|
- Anabel Bertina Dennis
- 5 years ago
- Views:
Transcription

1
2 The Role of Defibrillator Therapy in Genetic Arrhythmia Syndromes RHEA C. PIMENTEL, MD, FACC, FHRS UNIVERSITY OF KANSAS HOSPITAL MID AMERICA CARDIOLOGY AUGUST 19, 2012
3 Monogenic Arrhythmia Syndromes Mendelian genetics pattern Single gene mutation causes disease phenotype Cause alterations in cardiac morphology (Hypertrophic Cardiomyopathy, Arrhythmogenic RV Dysplasia) Or: Structurally normal hearts Variabilities in Genotype and Phenotype Genotype: Specific DNA alteration causing problem Phenotype: Clinical presentation No randomized trials of therapy available Registries often biased to sicker/symptomatic patients
4 Doyle MacKinnon. Science 280:69-77, 1998 FAF SIDS SUDS SSS TS DI-TdP DCM CPVT SQTS Cardiac Channelopathies LQTS - RWS - JLNS FAVCB ATS IVF BrS

5 Primary Ion Channels in the Heart Mutations in ion channel genes result in disturbances to normal heart rhythm.
6 The Challenges of Diagnosing an Inherited Cardiac Arrhythmia Syndrome Variable Clinical Expression Penetrance The extent to which individuals with the same genotype display the same phenotype Age of onset Triggers Variable Expressivity Phenotype variations with same /similar mutations Brugada syndrome vs. conduction disease in same/similar SCN5A mutations
7 Reduced Penetrance Reduced Penetrance 90% of those with mutation will have HCM 83% of those with mutation will have CPVT ~50% of those with mutation will have LQTS 37% LQTS1, 54% LQTS2, 82%LQTS3 30% of those with mutation will have clinical Brugada Syndrome
8 Current Risk Stratification Schemes Clinical Symptoms: syncope, palpitations Family history: first degree relatives EKG abnormalities Diagnostic testing: EP study, SAECG Specific genetic mutation: genetic testing
9 ICD Therapy in Genetic Arrhythmia Syndromes Increased use of defibrillators Population specific considerations Age of patient Psychosocial aspects for patient Implications for family members True risk of ICD discharge --Risk of Inappropriate shocks
10 Efficacy of ICD Therapy in Hypertrophic Cardiomyopathy Retrospective multicenter study 128 patients received ICD to prevent sudden death Mean follow up 3.1 years VT/VF is the principle mechanism of death Rate of appropriate discharge was 7% a year 25% had episodes of inappropriate discharges ICD s highly effective at preventing sudden death in HOCM patients Maron BJ et al. NEnglJ med 10Feb 2000;342(6):

11 Risk factors for SD in HOCM Bos et al. Am J Cardiol 2010;106:
12 VA Associated With Cardiomyopathies Hypertrophic Cardiomyopathy (HCM) I IIa IIb III I IIa IIb III ICD therapy should be used for treatment in patients with HCM who have sustained VT and/or VF and who are receiving chronic optimal medical therapy and who have reasonable expectation of survival with a good functional status for more than 1 year. ICD implantation can be effective for primary prophylaxis against SCD in patients with HCM who have 1 or more major risk factor for SCD and who are receiving chronic optimal medical therapy and in patients who have reasonable expectation of survival with a good functional status for more than 1 year.


13 an exhilarating moment in human history Francis Collins June 22, 2000
14 Benefits of Genetic Testing Confirm and/or Exclude Diagnosis Predict Future Disease (Asymptomatic, Predisposition) Provide Risk Estimates: Comprehensive Treatment Plan Reproductive decisions Medical decisions Risk information for family members Prophylactic Intervention
15 Impediments to Interpretation of Genetic Testing Locus Heterogeneity Many genes Increases cost and complexity Genetic Cause Not Identified in All Cases DCM (25-33%) HCM (30-40%, greater in familial cases) LQTS (65-75%) Negative Test Limits Clinical Utility Unless a familial mutation known
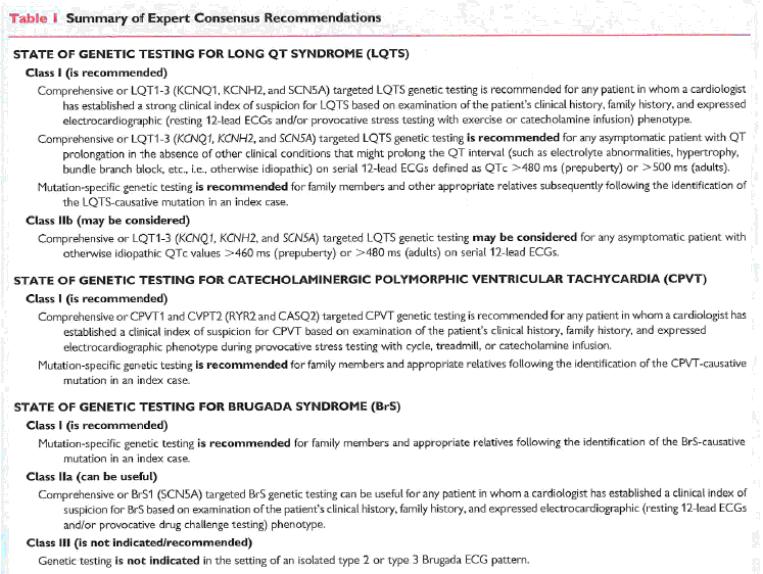
16 Current HRS Recommendations
17 Effect of Cascade Screening on Prophylactic Treatment Mutations carrying relatives of proband with an inherited arrhythmia syndrome 130 probands, 509 mutation positive relatives LQTS, CPVT, and BrS Carriers treated more aggressively LQTS (65%) and CPVT (71%) started on beta blockers 59% of LQT patients had QTc <460 msec 6% BrS treated with ICD Hofman N et al. J Am Coll Cardiol 2010 Jun 8;55(23):
18 Doyle MacKinnon. Science 280:69-77, 1998 FAF SIDS SUDS SSS TS DI-TdP DCM CPVT SQTS Cardiac Channelopathies LQTS - RWS - JLNS FAVCB ATS IVF BrS
19 Congenital Long QT Syndrome QT QT Normal QT interval Prolonged QT 1. Syncope 2. Seizures 3. Sudden death Torsades de pointes
20 Schwartz Score Schwartz et al. Circulation 1993 Aug 88(2);782-4
21

22 Torsades de Pointes Spontaneous conversion to NSR (continuous lead II monitor strip)
23 Persons (no.) 3,000 33% of gene positive carriers for LQT have normal QT intervals Normals 1 LQTS QTc (ms)
24 Molecular Basis for Long QT Syndrome JCE 1999;10:
25 Congenital Long QT Syndrome QT QT Normal QT interval Prolonged QT 1. Syncope 2. Seizures 3. Sudden death Torsades de pointes Tester Ackerman. Heart Rhythm 2: , 2005
26 CAV3-LQT (LQT9) Ch 3p25 Caveolin-3 < 1% TS1 (LQT8) Ch 1q42 CACNA1C <<1% ATS1 (LQT7) Ch 17q23 KCNJ2 <1% SCN4B-LQT (LQT10) Ch 11q23.3 NaV1.5 b4 subunit < 1% LQTS Susceptibility LQT6 Ch 21q22 KCNE2 <1% Genes LQT5 Ch 21q22 KCNE1 1% LQT1 Ch 11p15.5 KCNQ % LQT2 Ch 7q35-36 KCNH % LQT3 Ch 3p21-24 SCN5A 5-10% LQT4 Ch 4q25-27 ANK2 < 1%


27 Khositseth and Ackerman. Cardiac Repolarization Chapter 20, 2003 KCNQ1 (LQT1) Genotype-Specific Triggers? 30-35% SCN5A (LQT3) KCNH2 (LQT2) 5-10%
28 Percent (%) LQT1 LQT2 LQT3 Genotype Negative Exertion N = 124 Swimming N = 71 Postpartum N = 24 Auditory N = 24
29 KCNQ1 (LQT1) Effect of Beta Blocker Therapy % SCN5A (LQT3) KCNH2 (LQT2) +/- ++ Khositseth and Ackerman. Cardiac Repolarization Chapter 20, 2003

30 LQTS Susceptibility LQT6 Ch 21q22 KCNE2 <1% Genes LQT5 Ch 21q22 KCNE1 1% LQT1 Ch 11p15.5 KCNQ % LQT2 Ch 7q35-36 KCNH % LQT3 Ch 3p21-24 SCN5A 5-10%

 30-35% KCNH2")
31 Khositseth and Ackerman. Cardiac Repolarization Chapter 20, 2003 KCNE1 (LQT5) KCNE2 (LQT6) KCNQ1 (LQT1) < 1% < 1% SCN5A (LQT3) 30-35% KCNH2 (LQT2) 5-10% 25-30%
32 Probability of Cardiac Event Circ 2000;101:

33 High Risk (> 50%) QTc > 500 LQT1, LQT2 LQT3 Intermediate (30-49%) Low Risk (<30%) QTc < 500 QTc > 500 LQT2, LQT3 LQT3 LQT3 QTc < 500 ms LQT2 LQT1 Priori SG, Schwartz PJ, et al. NEJM 348: , 2003

34 Family History Risk in LQTS Kaufman et al. Heart Rhythm 2008;5:

35 Degree of QT prolongation Kaufman ES et al. June Heart Rhythm;5(6):
36 Probability of a Cardiac Event No. of Subjects LQT1 group LQT2 group LQT3 group Zareba W et al. NEJM 1998;339:
37 LQT1-Associated Mutations Tester Ackerman. Heart Rhythm 2: , 2005
38 Probability of a Cardiac Event LQT1-Associated Mutations Unadjusted P< TRANSMEMBRANE C-TERMINUS AGE (years) Moss, Shimizu, Wilde... Circulation 115: , 2007
39 Probability of a Cardiac Event Probability of a Cardiac Event LQT1-Associated Mutations Unadjusted Unadjusted P<0.001 P<0.001 DOMINANT NEGATIVE TRANSMEMBRANE HAPLOINSUFFICIENCY C-TERMINUS AGE AGE (years) (years) Moss, Shimizu, Wilde... Circulation 115: , 2007
40 LQT1-Associated Mutations Location and Function Matters -- HR > 2 -- * Independent of Traditional Risk Factors * Tester Ackerman. Heart Rhythm 2: , 2005
41 LQT2-Associated Mutations KCNH2/HERG N = 89 C 1159 Tester Ackerman. Heart Rhythm 2: , 2005

42 LQT2: Pore Mutations Behave Porely KCNH2/HERG N = 89 C 1159 Moss et al. Circulation 105: , 2002
43 LQT3 Gain-of-Function SCN5A Loss-of-Function BrS1
44 Long QT Syndrome I IIa IIb III I IIa IIb III Beta blockers can be effective to reduce SCD in patients with a molecular LQTS analysis and normal QT interval. Implantation of an ICD with continued use of beta blockers can be effective to reduce SCD in LQTS patients with syncope and/or VT while receiving beta blockers and who have reasonable expectation of survival with a good functional status for >1 year. I I IIa IIb III IIa IIb III Left cardiac sympathetic neural denervation may be considered for LQTS patients with syncope, torsades de pointes, or cardiac arrest while receiving beta blockers. Implantation of an ICD with the use of beta blockers may be considered for prophylaxis of SCD for patients in categories possibly associated with higher risk of cardiac arrest such as LQT2 and LQT3 and who have reasonable expectation of survival with a good functional status for >1 year.

45 (Circulation. 2005; 111: )
46 Brugada Syndrome Incidence 5/10,00 More common in Southeast Asia Mean age 41 ± 15 years, male predominance 4% of all sudden death At least 20% of sudden death in structurally normal hearts Characteristic EKG pattern Coving ST segment elevation in precordial leads V1 to V3 (>2 mm) +/- RBBB pattern Spontaneous or drug induced
47 Atrial Arrhythmias and Brugada 20% develop SVT Atrial Fibrillation in 10-20% of cases Have been described in association AVNRT WPW Prolonged SNRT Prolonged SART Slowed atrial conduction Atrial standstill

48 Brugada Syndrome (Typical ST-T abnormality V1-V2)
49 V1 V2 V3 Cardiac Channelopathies BrS
50 Genetic Factors Autosomal Dominant SCN5A More than 80 mutations linked to the syndrome since dozen associated with loss of function on Na channel SCN5A mutations account for 18-30% of Brugada Syndrome cases Negative SCN5A does not rule out causal gene mutations









51 Sodium Channel Macromolecular Complex Glycerol-3-Phosphate Dehydrogenase 1-Like Gene Loss-of-Function = BrS2 Genetic Heterogeneity Na v 1.5 in BrS Ankyrin Syntrophin BrS2 Na + Ch 3p24 GPD1L % Yield?? London et al. Circulation 2007(in press)

52 LQT3 Gain-of-Function SCN5A Loss-of-Function BrS1
53 Incidence of Sudden Death Brugada et al. Aborted sudden death Recurrence 69% at 54 ± 54 months Syncope and spontaneous Type 1 pattern 19% at 26 ± 36 months 8% risk of occurrence in initially asymptomatic patients
54 Defibrillator Implantation is only known therapy for Brugada Syndrome
55 Risk Stratification in BrS Symptoms Family History? Sodium Channel Blocker Challenge Programmed Ventricular Stimulation EKG abnormalities
56 Symptoms Predicting ICD shock

57 Age and Onset of Symptoms in Brugada Syndrome Napolitano C et al.circulation.2012apr24;125(16):

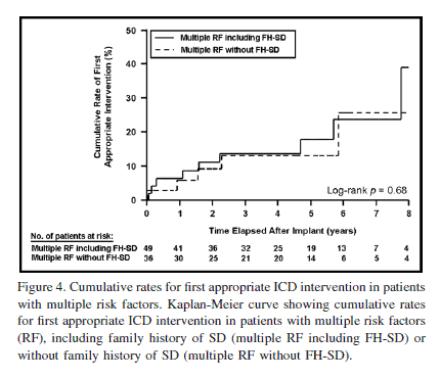
58 Role of Family History in Risk of Sudden Death in BrS Sarkozy A et al. European Heart Journal (2011) 32,
")

59 Risk Stratification in BrS Type 1 ECG 320 patients (54% with spontaneous and 46% drug induced EKG) Spontaneous type 1 ECG and syncope significantly increased risk Delise P et al. Eur Heart J 2011 Jan;32(2):
60 PRELUDE Registry 308 patients: spontaneous or drug induced type 1 ECG and no history of cardiac arrest Programmed electrical stimulation performed 14 (4.5%) arrhythmic events occurred in 34 months Arrhythmia inducibility was not a predictor of events at follow up Syncope and spontaneous type 1 ECG were significant predictors of arrhythmias Priori SG et al. J Am Coll Cardiol Jan 3;59(1):37-45.
61 Programmed Ventricular Stimulation (PVS) in BrS: a meta-analysis 15 studies comprising 1217 patients (80% male) Divided in 3 groups: cardiac arrest, syncope and asymptomatic 1036 patients (85%) underwent PVS 548 patients (53%) inducible Highest inducibility in sudden death patients (66%) Lowest inducibility in asymptomatic patients (22%) Paul M et al. European Heart J :
 in BrS: a")

62 Programmed Ventricular Stimulation (PVS) in BrS: a meta-analysis Paul M et al. European Heart J :

63 Fragmented QRS in BrS Morita et al. Circulation. 2008;118:
64 Brugada Syndrome I IIa IIb III An ICD is indicated for Brugada syndrome patients with previous cardiac arrest receiving chronic optimal medical therapy and who have reasonable expectation of survival with a good functional status for >1 year. I IIa IIb III I IIa IIb III An ICD is reasonable for Brugada syndrome patients with spontaneous ST-segment elevation in V 1, V 2, or V 3 who have had syncope with or without mutations demonstrated in the SCN5A gene and who have reasonable expectation of survival with a good functional status for >1 year. Clinical monitoring for the development of a spontaneous ST-segment elevation pattern is reasonable for the management of patients with ST-segment elevation induced only with provocative pharmacological challenge with or without symptoms.
65 Brugada Syndrome I IIa IIb III I IIa IIb III An ICD is reasonable for Brugada syndrome patients with documented VT that has not resulted in cardiac arrest and who have reasonable expectation of survival with a good functional status for >1 year. Isoproterenol can be useful to treat an electrical storm in the Brugada syndrome. I I IIa IIb III IIa IIb III EP testing may be considered for risk stratification in asymptomatic Brugada syndrome patients with spontaneous ST elevation with or without a mutation in the SCN5A gene. Quinidine might be reasonable for the treatment of electrical storm in patients with Brugada syndrome.

66 Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT) Clinical Exertion Induced Syncope or Sudden Cardiac Death No Structural Heart Defect Phenotypically Mimics Long QT Syndrome Hallmark Arrhythmia Bi-Directional Ventricular Tachycardia Priori et al. J Clin Invest 115: , 2005
67 Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT) Polymorphic ventricular tachycardia induced by adrenergic stress Exercise induced VT or syncope Classically a bidirectional VT Incidence 1:10,000 Mean age of presentation 7.8 years old 1 Baseline EKG normal No structural heart disease 1 Leenhardt a et al. Circulation 1995;91:
68 80% of Untreated CPVT Patients Become Symptomatic If left untreated, 30% of CPVT patients will develop symptoms by age 10, and ~80% by age Reference: 1. Mohamed U, Napolitano C, Priori SG. Molecular and electrophysiological bases of catecholaminergic polymorphic ventricular tachycardia. J Cardiovasc Electrophysiol. 2007;18(7): Adapted from: Napolitano C, Priori SG. Diagnosis and treatment of catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2007;4:

69 Challenges in Diagnosing CPVT Cannot be diagnosed on the basis of resting ECG. 1,2 Exercise stress testing is an important part of workup - However, in as many as 20% of CPVT patients, formal exercise stress testing will not produce ventricular ectopy. 1 During exercise stress testing, bidirectional VT with a beat-to-beat 180 degree rotation of the QRS complex is often observed 1 References: 1. Mohamed U, Napolitano C, Priori SG. Molecular and electrophysiological bases of catecholaminergic polymorphic ventricular tachycardia. J Cardiovasc Electrophysiol. 2007;18(7): Kontula K, Laitinen PJ, Lehtonen 69 A, Toivornen L, Viitasalo M, Swan H. Catecholaminergic polymorphic ventricular tachycardia: recent mechanistic insights. Cardiovasc Res. 2005;67:
70 It Is Important to Differentiate Between CPVT and LQT1 1 CPVT is an LQT1 mimicker. 2 As many as 30% of CPVT patients have been misdiagnosed as having Long QT with normal QTc. 1,3 Differentiating CPVT from LQT1 is important for: - Developing a comprehensive treatment plan - Family specific testing References: 1. Priori SG, Napolitano C, Memmi M, et al. Clinical and molecular characterization of patients with catecholaminergic polymorphic ventricular tachycardia. Circulation. 2002;106: Choi G, Kopplin LJ, Tester DJ, et al. Spectrum and frequency of cardiac channel defects in swimming-triggered arrhythmia syndromes. Circulation. 2004;110: Napolitano C, Priori SG. Diagnosis and treatment of catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2007;4:
71 Cardiac Channelopathy Mimicry Genotype Negative N = 269, 49.7% Genotype Positive N = 272, 50.3% KCNJ2 (ATS1) ANKB (LQT4) RYR2 (CPVT1) Tester Ackerman. Heart Rhythm 2: , 2005 Tester Ackerman. Heart Rhythm 2: , 2005
72 Known mutations: CPVT Cardiac ryanodine receptor gene (RYR2) Cardiac calsequestrin gene (CASQ2) Treatment: Removal of triggers: vigorous physical activity Beta blockers to decrease adrenergic tone (46% have VT recurrence) Cervical sympathectomy Implantable defibrillator: do not use without BB Flecainide: inhibits RYR2 mediated calcium release



 105 1 8 14")



73 Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT) Cellular Cell membrane Molecular Sarcoplasmic reticulum RyR2 CASQ2 Calcium Induced Calcium Release (CICR) Exons 4967 amino acids RyR2 (CPVT1, Ch 1q42.1-q43) CASQ2 (CPVT2, Ch 1p13.1) 11 Exons 339 amino acids
74 Risk Stratification in CPVT Insufficient data regarding risk Highest risk: sustained VF or unstable VT while receiving beta blockers Younger age at CPVT diagnosis 2 EP studies not helpful 1 Genetic analysis doesn t contribute to risk RyR2 mutation penetrance over 80%: treat asymptomatic carriers with beta blockers 1 Priori SG et al. Circulation2002;106: Hayashi M et al. Circulation 2009;119:
75 Beta-blockers Do Not Provide Reliable Protection Against Cardiac Arrhythmias Related to CPVT 1 However, in light of incomplete protection afforded by beta-blockers in CPVT, its distinction from long-qt is clinically relevant. 1 - S. Priori MD, 2002 Nearly 50% of CPVT patients taking a betablocker continue experiencing cardiac arrhythmias and may require an ICD. 1 Reference: 1. Priori SG, Napolitano C, Memmi M, et al. Clinical and molecular characterization of patients with catecholaminergic polymorphic ventricular tachycardia. Circulation. 2002;106:69-74.
76 Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT) I IIa IIb III Beta blockers are indicated for patients who are clinically diagnosed with CPVT on the basis of the presence of spontaneous or documented stress-induced ventricular arrhythmias. I IIa IIb III Implantation of an ICD with use of beta blockers is indicated for patients with CPVT who are survivors of cardiac arrest and who have reasonable expectation of survival with a good functional status for >1 year.
77 CPVT I IIa IIb III I IIa IIb III Beta blockers can be effective in patients without clinical manifestations when the diagnosis of CPVT is established during childhood based on genetic analysis. Implantation of an ICD with the use of beta blockers can be effective for affected patients with CPVT with syncope and/or documented sustained VT while receiving beta blockers and who have reasonable expectation of survival with a good functional status for >1 year. I IIa IIb III Beta blockers may be considered for patients with CPVT who were genetically diagnosed in adulthood and never manifested clinical symptoms of tachyarrhythmias.
78 Conclusions Genetic arrhythmia syndromes are an important cause of sudden cardiac death in young patients Implantable cardiac defibrillators have been shown to improve mortality in monogenic arrhythmia syndromes The indications for ICD implantation in this population continues to expand as the risk factors for sudden death are elucidated.

79 Thank You!
WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY
 Learning Objectives to Disclose: To CRITIQUE the ICD and its role in the treatment of BrS, CPVT, and LQTS WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY Conflicts of Interest to Disclose: Consultant
Learning Objectives to Disclose: To CRITIQUE the ICD and its role in the treatment of BrS, CPVT, and LQTS WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY Conflicts of Interest to Disclose: Consultant
Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation?
 Innovations in Interventional Cardiology and Electrophysiology Thessaloniki 2014 Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation? K. Letsas, MD, FESC
Innovations in Interventional Cardiology and Electrophysiology Thessaloniki 2014 Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation? K. Letsas, MD, FESC
Pearls of the ESC/ERS Guidelines 2015 Channelopathies
 Pearls of the ESC/ERS Guidelines 2015 Channelopathies Carina Blomstrom Lundqvist Dept Cardiology, Uppsala, Sweden Content 2015 ESC Guidelines for the Management of Patients with Ventricular Arrhythmias
Pearls of the ESC/ERS Guidelines 2015 Channelopathies Carina Blomstrom Lundqvist Dept Cardiology, Uppsala, Sweden Content 2015 ESC Guidelines for the Management of Patients with Ventricular Arrhythmias
ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ
 ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ ΣΤΕΛΙΟΣ ΠΑΡΑΣΚΕΥΑÏΔΗΣ ΔΙΕΥΘΥΝΤΗΣ ΕΣΥ Α Καρδιολογική Κλινική ΑΠΘ, Νοσοκομείο ΑΧΕΠΑ, Θεσσαλονίκη NO CONFLICT OF INTEREST Sudden Cardiac Death
ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ ΣΤΕΛΙΟΣ ΠΑΡΑΣΚΕΥΑÏΔΗΣ ΔΙΕΥΘΥΝΤΗΣ ΕΣΥ Α Καρδιολογική Κλινική ΑΠΘ, Νοσοκομείο ΑΧΕΠΑ, Θεσσαλονίκη NO CONFLICT OF INTEREST Sudden Cardiac Death
Basics of Structure/Function of Sodium and Potassium Channels Barry London, MD PhD
 Basics of Structure/Function of Sodium and Potassium Channels Barry London, MD PhD University of Pittsburgh Medical Center Pittsburgh, PA International Symposium of Inherited Arrhythmia Disorders and Hypertrophic
Basics of Structure/Function of Sodium and Potassium Channels Barry London, MD PhD University of Pittsburgh Medical Center Pittsburgh, PA International Symposium of Inherited Arrhythmia Disorders and Hypertrophic
Invasive Risk Stratification: When is it needed?
 Inherited Cardiomyopathies and Channelopathies: Who is at risk for Sudden Cardiac Death? Invasive Risk Stratification: When is it needed? Hung-Fat Tse, MD, PhD Department of Medicine The University of
Inherited Cardiomyopathies and Channelopathies: Who is at risk for Sudden Cardiac Death? Invasive Risk Stratification: When is it needed? Hung-Fat Tse, MD, PhD Department of Medicine The University of
Strength and weakness of genetic testing in clinical routine.
 Strength and weakness of genetic testing in clinical routine. Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular
Strength and weakness of genetic testing in clinical routine. Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular
Long Q. Long QT Syndrome. A Guide for
 Long Q Long QT Syndrome A Guide for Introduction Long QT syndrome (LQTS) is a genetic heart disorder due to the malfunction of cardiac ion channels that results in 4,000 deaths annually in the United States
Long Q Long QT Syndrome A Guide for Introduction Long QT syndrome (LQTS) is a genetic heart disorder due to the malfunction of cardiac ion channels that results in 4,000 deaths annually in the United States
Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association
 Genetic Testing for Page 1 of 23 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Genetic Testing for Professional Institutional Original Effective Date: August
Genetic Testing for Page 1 of 23 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Genetic Testing for Professional Institutional Original Effective Date: August
Name of Presenter: Marwan Refaat, MD
 NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010 I have no actual or potential conflict of interest in relation
NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010 I have no actual or potential conflict of interest in relation
Genetic Testing for Cardiac Ion Channelopathies
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
When VF is the endpoint, wait and see is not always the best option.
 Being free of symptoms does not necessarily mean free of arrhythmias. This Holter is from a asymptomatic 48 years old female with LQT2 When VF is the endpoint, wait and see is not always the best option.
Being free of symptoms does not necessarily mean free of arrhythmias. This Holter is from a asymptomatic 48 years old female with LQT2 When VF is the endpoint, wait and see is not always the best option.
FANS Paediatric Pathway for Inherited Arrhythmias*
 FANS Paediatric Pathway for Inherited Arrhythmias* The pathway is based on the HRS/EHRA/APHRS Expert Consensus Statement on the Diagnosis and Management of Patients with Inherited Primary Arrhythmia Syndromes
FANS Paediatric Pathway for Inherited Arrhythmias* The pathway is based on the HRS/EHRA/APHRS Expert Consensus Statement on the Diagnosis and Management of Patients with Inherited Primary Arrhythmia Syndromes
Genetic Testing for Cardiac Ion Channelopathies
 Genetic Testing for Cardiac Ion Channelopathies Policy Number: 2.04.43 Last Review: 11/2018 Origination: 6/2007 Next Review: 11/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Genetic Testing for Cardiac Ion Channelopathies Policy Number: 2.04.43 Last Review: 11/2018 Origination: 6/2007 Next Review: 11/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Prolonged QT Syndromes: Congenital and Acquired
 Prolonged QT Syndromes: Congenital and Acquired April 30, 2014 Elizabeth S. Kaufman, MD I have no financial disclosures. MetroHealth Campus, Case Western Reserve University Prolonged QT Syndromes Congenital
Prolonged QT Syndromes: Congenital and Acquired April 30, 2014 Elizabeth S. Kaufman, MD I have no financial disclosures. MetroHealth Campus, Case Western Reserve University Prolonged QT Syndromes Congenital
Genetics of Sudden Cardiac Death. Geoffrey Pitt Ion Channel Research Unit Duke University. Disclosures: Grant funding from Medtronic.
 Genetics of Sudden Cardiac Death Geoffrey Pitt Ion Channel Research Unit Duke University Disclosures: Grant funding from Medtronic Duke U N I V E R S I T Y Sudden Cardiac Death High incidence 50-100 per
Genetics of Sudden Cardiac Death Geoffrey Pitt Ion Channel Research Unit Duke University Disclosures: Grant funding from Medtronic Duke U N I V E R S I T Y Sudden Cardiac Death High incidence 50-100 per
Genetic testing in Cardiomyopathies
 Genetic testing in Cardiomyopathies Silvia Giuliana Priori Cardiovascular Genetics, Langone Medical Center, New York University School of Medicine, New York, USA and Molecular Cardiology, IRCCS Fondazione
Genetic testing in Cardiomyopathies Silvia Giuliana Priori Cardiovascular Genetics, Langone Medical Center, New York University School of Medicine, New York, USA and Molecular Cardiology, IRCCS Fondazione
Section: Effective Date: Subsection: Original Policy Date: Subject: Page: Last Review Status/Date: Background
 Genetic Testing for Cardiac Ion Last Review Status/Date: March 2014 Genetic Testing for Cardiac Ion Description Page: 1 of 22 Genetic testing is available for patients suspected of having cardiac ion channelopathies
Genetic Testing for Cardiac Ion Last Review Status/Date: March 2014 Genetic Testing for Cardiac Ion Description Page: 1 of 22 Genetic testing is available for patients suspected of having cardiac ion channelopathies
ICD in a young patient with syncope
 ICD in a young patient with syncope Konstantinos P. Letsas, MD, FESC Second Department of Cardiology Evangelismos General Hospital of Athens Athens, Greece Case presentation A 17-year-old apparently healthy
ICD in a young patient with syncope Konstantinos P. Letsas, MD, FESC Second Department of Cardiology Evangelismos General Hospital of Athens Athens, Greece Case presentation A 17-year-old apparently healthy
Description. Page: 1 of 31. Genetic Testing for Cardiac Ion Channelopathies. Last Review Status/Date: December 2015
 Genetic Testing for Cardiac Ion Last Review Status/Date: December 2015 Genetic Testing for Cardiac Ion Description Page: 1 of 31 Genetic testing is available for patients suspected of having cardiac ion
Genetic Testing for Cardiac Ion Last Review Status/Date: December 2015 Genetic Testing for Cardiac Ion Description Page: 1 of 31 Genetic testing is available for patients suspected of having cardiac ion
Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada
 Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας και Βηματοδότησης BrS: Diagnosis 5:10000 First described
Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας και Βηματοδότησης BrS: Diagnosis 5:10000 First described
Preventing Sudden Death in Young Athletes. Outline. Scope of the Problem. Causes of SCD in Young Athletes. Sudden death in the young athlete
 Preventing Sudden Death in Young Athletes Ronn E. Tanel, MD Director, Pediatric Arrhythmia Service UCSF Children s Hospital Associate Professor of Pediatrics UCSF School of Medicine Outline Sudden death
Preventing Sudden Death in Young Athletes Ronn E. Tanel, MD Director, Pediatric Arrhythmia Service UCSF Children s Hospital Associate Professor of Pediatrics UCSF School of Medicine Outline Sudden death
Παναγιώτης Ιωαννίδης. Διευθυντής Τμήματος Αρρυθμιών & Επεμβατικής Ηλεκτροφυσιολογίας Βιοκλινικής Αθηνών
 Διαστρωμάτωση κινδύνου για αιφνίδιο καρδιακό θάνατο σε ασθενείς που δεν συμπεριλαμβάνονται σε μεγάλες κλινικές μελέτες «Ασθενείς με ηλεκτρικά νοσήματα» Παναγιώτης Ιωαννίδης Διευθυντής Τμήματος Αρρυθμιών
Διαστρωμάτωση κινδύνου για αιφνίδιο καρδιακό θάνατο σε ασθενείς που δεν συμπεριλαμβάνονται σε μεγάλες κλινικές μελέτες «Ασθενείς με ηλεκτρικά νοσήματα» Παναγιώτης Ιωαννίδης Διευθυντής Τμήματος Αρρυθμιών
Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart.
 Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart. Hanne Rasmusen Consultant cardiologist, PhD Dept. of Cardiology Bispebjerg University Hospital
Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart. Hanne Rasmusen Consultant cardiologist, PhD Dept. of Cardiology Bispebjerg University Hospital
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Genetic Testing for Page 1 of 29 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Genetic Testing for Professional Institutional Original Effective Date: August 12,
Genetic Testing for Page 1 of 29 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Genetic Testing for Professional Institutional Original Effective Date: August 12,
SEMINAIRES IRIS. Sudden cardiac death in the adult. Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel. 20% 25% Cancers !
 Sudden cardiac death in the adult Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel.! " # $ % Cancers National Vital Statistics Report, Vol 49 (11), Oct. 12, 2001. 20% 25% State-specific
Sudden cardiac death in the adult Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel.! " # $ % Cancers National Vital Statistics Report, Vol 49 (11), Oct. 12, 2001. 20% 25% State-specific
Wojciech Szczepański, MD, PhD Department of Pediatrics, Endocrinology, Diabetology with Cardiology Division Medical University of Bialystok
 Channelopathies: - Long QT syndrome - Short QT syndrome - Brugada syndrome - Early repolarization syndrome - Catecholaminergic polymorphic ventricular tachycardia Wojciech Szczepański, MD, PhD Department
Channelopathies: - Long QT syndrome - Short QT syndrome - Brugada syndrome - Early repolarization syndrome - Catecholaminergic polymorphic ventricular tachycardia Wojciech Szczepański, MD, PhD Department
Silvia G Priori MD PhD
 The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
Are there low risk patients in Brugada syndrome?
 Are there low risk patients in Brugada syndrome? Pedro Brugada MD, PhD Andrea Sarkozy MD Risk stratification in Brugada syndrome In the last years risk stratification in Brugada syndrome has become the
Are there low risk patients in Brugada syndrome? Pedro Brugada MD, PhD Andrea Sarkozy MD Risk stratification in Brugada syndrome In the last years risk stratification in Brugada syndrome has become the
Genetic Testing for Cardiac Ion Channelopathies. Description
 Genetic Testing for Cardiac Ion Page: 1 of 30 Last Review Status/Date: March 2017 Genetic Testing for Cardiac Ion Description Genetic testing is available for patients suspected of having cardiac ion channelopathies
Genetic Testing for Cardiac Ion Page: 1 of 30 Last Review Status/Date: March 2017 Genetic Testing for Cardiac Ion Description Genetic testing is available for patients suspected of having cardiac ion channelopathies
Active Cascade Screening in Primary Inherited Arrhythmia Syndromes
 Journal of the American College of Cardiology Vol. 55, No. 23, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.12.063
Journal of the American College of Cardiology Vol. 55, No. 23, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.12.063
What is New in CPVT? Diagnosis Genetics Arrhythmia Mechanism Treatment. Andreas Pflaumer
 What is New in CPVT? Diagnosis Genetics Arrhythmia Mechanism Treatment Andreas Pflaumer Diagnosis of CPVT Induction of different types of VES or VT by exercise or catecholamines AND exclusion of of other
What is New in CPVT? Diagnosis Genetics Arrhythmia Mechanism Treatment Andreas Pflaumer Diagnosis of CPVT Induction of different types of VES or VT by exercise or catecholamines AND exclusion of of other
Corporate Medical Policy
 Corporate Medical Policy Genetic Testing for Cardiac Ion Channelopathies File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_cardiac_ion_channelopathies 10/2008 4/2018
Corporate Medical Policy Genetic Testing for Cardiac Ion Channelopathies File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_cardiac_ion_channelopathies 10/2008 4/2018
Brugada Syndrome: An Update
 Brugada Syndrome: An Update Osama Diab Associate professor of Cardiology Ain Shams university, Cairo, Egypt Updates Mechanism and Genetics Risk stratification Treatment 1 Brugada syndrome causes 4 12%
Brugada Syndrome: An Update Osama Diab Associate professor of Cardiology Ain Shams university, Cairo, Egypt Updates Mechanism and Genetics Risk stratification Treatment 1 Brugada syndrome causes 4 12%
Professor Eric Schulze-Bahr
 No CoI. Professor Eric Schulze-Bahr Institute for Genetics of Heart Diseases Department of Cardiology and Angiology University Hospital Münster / Germany ICD therapy in asymptomatic or borderline LQTS
No CoI. Professor Eric Schulze-Bahr Institute for Genetics of Heart Diseases Department of Cardiology and Angiology University Hospital Münster / Germany ICD therapy in asymptomatic or borderline LQTS
Case studies in Channelopathies
 Case studies in Channelopathies FABRICE CHOUTY, MD MEDICAL DIRECTOR HANNOVER-LIFE RE, PARIS (F) INTRODUCTION Thanks to the invasive electrophysiology and the progress of imaging techniques as well as the
Case studies in Channelopathies FABRICE CHOUTY, MD MEDICAL DIRECTOR HANNOVER-LIFE RE, PARIS (F) INTRODUCTION Thanks to the invasive electrophysiology and the progress of imaging techniques as well as the
Congenital long QT syndrome of particularly malignant course connected with so far unknown mutation in the sodium channel SCN5A gene
 CASE REPORT Cardiology Journal 2013, Vol. 20, No. 1, pp. 78 82 10.5603/CJ.2013.0012 Copyright 2013 Via Medica ISSN 1897 5593 Congenital long QT syndrome of particularly malignant course connected with
CASE REPORT Cardiology Journal 2013, Vol. 20, No. 1, pp. 78 82 10.5603/CJ.2013.0012 Copyright 2013 Via Medica ISSN 1897 5593 Congenital long QT syndrome of particularly malignant course connected with
Patient Resources: Cardiac Channelopathies
 Patient Resources: Cardiac Channelopathies Overview of Cardiac Channelopathies: CPVT, Long QT Syndrome and Brugada Syndrome Heart muscle cells contract because of movement of certain molecules (called
Patient Resources: Cardiac Channelopathies Overview of Cardiac Channelopathies: CPVT, Long QT Syndrome and Brugada Syndrome Heart muscle cells contract because of movement of certain molecules (called
Left cardiac sympathectomy to manage beta-blocker resistant LQT patients
 Left cardiac sympathectomy to manage beta-blocker resistant LQT patients Lexin Wang, M.D., Ph.D. Introduction Congenital long QT syndrome (LQTS) is a disorder of prolonged cardiac repolarization, manifested
Left cardiac sympathectomy to manage beta-blocker resistant LQT patients Lexin Wang, M.D., Ph.D. Introduction Congenital long QT syndrome (LQTS) is a disorder of prolonged cardiac repolarization, manifested
Asaad Khoury 2,3 MD, Monther Boulos 1,3 MD, Mahmoud Suleiman 1,3 MD, Miry Blich 1,3 MD, Michael Eldar 4 MD, Ibrahim Marai 1,3 MD,
 Flecainide therapy suppresses exercise induced ventricular arrhythmias in patients with CASQ2 associated catecholaminergic polymorphic ventricular tachycardia Asaad Khoury 2,3 MD, Monther Boulos 1,3 MD,
Flecainide therapy suppresses exercise induced ventricular arrhythmias in patients with CASQ2 associated catecholaminergic polymorphic ventricular tachycardia Asaad Khoury 2,3 MD, Monther Boulos 1,3 MD,
Protocol. Genetic Testing for Cardiac Ion Channelopathies
 Protocol Genetic Testing for Cardiac Ion Channelopathies (20443) Medical Benefit Effective Date: 04/0/8 Next Review Date: /8 Preauthorization Yes Review Dates: 05/09, 05/0, 03/, 03/2, 03/3, 03/4, 03/5,
Protocol Genetic Testing for Cardiac Ion Channelopathies (20443) Medical Benefit Effective Date: 04/0/8 Next Review Date: /8 Preauthorization Yes Review Dates: 05/09, 05/0, 03/, 03/2, 03/3, 03/4, 03/5,
Woo-Sik Yu, M.D. 1, Tae-Hoon Kim, M.D. 2, Jee won Suh, M.D. 1, Seunghwan Song, M.D. 1, Chang Young Lee, M.D. 1, Boyoung Joung, M.D., Ph.D.
 Korean J Thorac Cardiovasc Surg 2015;48:220-224 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) Case Report http://dx.doi.org/10.5090/kjtcs.2015.48.3.220 Thoracoscopic Left Cardiac Sympathetic Denervation
Korean J Thorac Cardiovasc Surg 2015;48:220-224 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) Case Report http://dx.doi.org/10.5090/kjtcs.2015.48.3.220 Thoracoscopic Left Cardiac Sympathetic Denervation
CHANNELOPATHIES IS GENETIC TESTING ESSENTIAL IN PTS MANAGEMENT
 CHANNELOPATHIES IS GENETIC TESTING ESSENTIAL IN PTS MANAGEMENT Inherited and Rare Cardiac Diseases Unit Heart Center for the Young and Athletes ONASSIS CARDIAC SURGERY CENTRE DIAGNOSIS ION CHANNEL DISEASE
CHANNELOPATHIES IS GENETIC TESTING ESSENTIAL IN PTS MANAGEMENT Inherited and Rare Cardiac Diseases Unit Heart Center for the Young and Athletes ONASSIS CARDIAC SURGERY CENTRE DIAGNOSIS ION CHANNEL DISEASE
Asymptomatic Long QT. Prof. Dr. Martin Borggrefe Mannheim
 Asymptomatic Long QT Prof. Dr. Martin Borggrefe Mannheim QT interval Distribution of QTc intervals in large population-based studies Viskin S, Heart Rhythm 2009; 6: 711-715 QT interval Distribution of
Asymptomatic Long QT Prof. Dr. Martin Borggrefe Mannheim QT interval Distribution of QTc intervals in large population-based studies Viskin S, Heart Rhythm 2009; 6: 711-715 QT interval Distribution of
Tailored therapy in long QT syndrome
 Tailored therapy in long QT syndrome Dominic Abrams St. Bartholomew s & Great Ormond Street Hospitals London, UK Disclosures None Tailored therapy in long QTS Which patients should have tailored therapy...?...
Tailored therapy in long QT syndrome Dominic Abrams St. Bartholomew s & Great Ormond Street Hospitals London, UK Disclosures None Tailored therapy in long QTS Which patients should have tailored therapy...?...
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Ripolarizzazione precoce. Torino, 24th October Non così innocente come si pensava
 Asymptomatic inherited arrhythmia syndromes: Drug induced Brugada Syndrome: when a prophylactic ICD is indicated? how high (or low) is QT the risk? Asymptomatic short Ripolarizzazione precoce. Torino,
Asymptomatic inherited arrhythmia syndromes: Drug induced Brugada Syndrome: when a prophylactic ICD is indicated? how high (or low) is QT the risk? Asymptomatic short Ripolarizzazione precoce. Torino,
IN THE NAME OF GOD. Dr.Sima Sayah
 IN THE NAME OF GOD Dr.Sima Sayah Epidemiology: Prevalence: ranging from 0.14% in the japanese to 0.61% in europeans & may reach to 3% in southeast Asia. In up to 60% of patients,the disease can be sporadic.
IN THE NAME OF GOD Dr.Sima Sayah Epidemiology: Prevalence: ranging from 0.14% in the japanese to 0.61% in europeans & may reach to 3% in southeast Asia. In up to 60% of patients,the disease can be sporadic.
Primary Therapy for High Risk LQT Patients Should Be an ICD
 Primary Therapy for High Risk LQT Patients Should Be an ICD Raul Weiss MD, FAHA, FACC, FHRS, CCDS Director, Electrophysiology Fellowship Program Associate Professor of Medicine The Ohio State University
Primary Therapy for High Risk LQT Patients Should Be an ICD Raul Weiss MD, FAHA, FACC, FHRS, CCDS Director, Electrophysiology Fellowship Program Associate Professor of Medicine The Ohio State University
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Interpretation and Consequences of Repolarisation Changes in Athletes
 Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification
 Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Stage I: Binning Dashboard
 Stage I: Binning Dashboard P[ GENE/GENE PANEL: KCNQ1, KCNH2, SCN5A DISORDER: Romano-Ward Long QT Syndrome HGNC ID: 6294, 6251, 10593 OMIM ID: 192500, 613688, 603830 ACTIONABILITY PENETRANCE 1. Is there
Stage I: Binning Dashboard P[ GENE/GENE PANEL: KCNQ1, KCNH2, SCN5A DISORDER: Romano-Ward Long QT Syndrome HGNC ID: 6294, 6251, 10593 OMIM ID: 192500, 613688, 603830 ACTIONABILITY PENETRANCE 1. Is there
Inherited Arrhythmia Syndromes
 Inherited Arrhythmia Syndromes When to perform Genetic testing? Arthur AM Wilde February 4, 2017 Which pts should undergo genetic testing? SCD victims with a likely diagnosis Pts diagnosed with an inherited
Inherited Arrhythmia Syndromes When to perform Genetic testing? Arthur AM Wilde February 4, 2017 Which pts should undergo genetic testing? SCD victims with a likely diagnosis Pts diagnosed with an inherited
Genetic Testing for Congenital Long QT Syndrome
 Genetic Testing for Congenital Long QT Syndrome Policy Number: 2.04.43 Last Review: 11/2013 Origination: 6/2007 Next Review: 11/2014 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Genetic Testing for Congenital Long QT Syndrome Policy Number: 2.04.43 Last Review: 11/2013 Origination: 6/2007 Next Review: 11/2014 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Long QT Syndrome in Children in the Era of Implantable Defibrillators
 Journal of the American College of Cardiology Vol. 50, No. 14, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.05.042
Journal of the American College of Cardiology Vol. 50, No. 14, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.05.042
Case Demonstrations in Congenital and Acquired Long QT Syndrome
 Case Demonstrations in Congenital and Acquired Long QT Syndrome Can You Make A Correct ECG Interpretation? Li Zhang, MD; 1-2 G. Michael Vincent, MD 1 1. LQTS Studies, Department t of Medicine i LDS Hospital,
Case Demonstrations in Congenital and Acquired Long QT Syndrome Can You Make A Correct ECG Interpretation? Li Zhang, MD; 1-2 G. Michael Vincent, MD 1 1. LQTS Studies, Department t of Medicine i LDS Hospital,
How to manage a patient with short QT syndrome?
 How to manage a patient with short QT syndrome? Torino, 27 ottobre2012 Carla Giustetto Division of Cardiology University of Torino QT 280 ms QTc 260 ms Narrow, tall and peaked T waves High incidence of
How to manage a patient with short QT syndrome? Torino, 27 ottobre2012 Carla Giustetto Division of Cardiology University of Torino QT 280 ms QTc 260 ms Narrow, tall and peaked T waves High incidence of
Plotse hartdood & genetica
 Onder spanning inspannen Utrecht, 17 April 2018 Plotse hartdood & genetica N. Hofman, PhD Academic Medical Centre Amsterdam, the Netherlands European Reference Network Network of centres in Europe sharing
Onder spanning inspannen Utrecht, 17 April 2018 Plotse hartdood & genetica N. Hofman, PhD Academic Medical Centre Amsterdam, the Netherlands European Reference Network Network of centres in Europe sharing
Tachycardia Devices Indications and Basic Trouble Shooting
 Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Sudden Cardiac Death and Asians Disclosures
 Sudden Cardiac Death and Asians Disclosures 7 February 2009 Asian Heart and Vascular Symposium None Zian H. Tseng, M.D., M.A.S. Assistant Professor of Medicine Cardiac Electrophysiology Section University
Sudden Cardiac Death and Asians Disclosures 7 February 2009 Asian Heart and Vascular Symposium None Zian H. Tseng, M.D., M.A.S. Assistant Professor of Medicine Cardiac Electrophysiology Section University
Medical Policy. Description/Scope. Rationale
 Subject: Document #: Current Effective Date: 03/29/2017 Status: Reviewed Last Review Date: 02/02/2017 Description/Scope This document addresses genetic testing of cardiac ion channel mutations in persons
Subject: Document #: Current Effective Date: 03/29/2017 Status: Reviewed Last Review Date: 02/02/2017 Description/Scope This document addresses genetic testing of cardiac ion channel mutations in persons
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know
 Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University
 Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University 1. Important and impact of ICD in primary prevention 2. Risk stratification for ICD
Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University 1. Important and impact of ICD in primary prevention 2. Risk stratification for ICD
Prevention of Sudden Death in ARVC
 ESC Munich, August 29, 2012 Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): Prevention of Sudden Death in ARVC Thomas Wichter, MD, FESC Professor of Medicine - Cardiology Marienhospital Osnabrück
ESC Munich, August 29, 2012 Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): Prevention of Sudden Death in ARVC Thomas Wichter, MD, FESC Professor of Medicine - Cardiology Marienhospital Osnabrück
Atrial fibrillation in Cardiac Channelopathies
 Atrial fibrillation in Cardiac Channelopathies Thejus, Jayachandran Francis, Johnson Introduction Atrial fibrillation is the commonest arrhythmia encountered in day-to-day clinical practice. Its prevalence
Atrial fibrillation in Cardiac Channelopathies Thejus, Jayachandran Francis, Johnson Introduction Atrial fibrillation is the commonest arrhythmia encountered in day-to-day clinical practice. Its prevalence
Tailored treatment in Brugada syndrome
 Tailored treatment in Brugada syndrome Lars Eckardt Department of Cardiology and Angiology Division of Experimental and Clinical Electrophysiology University of Münster, Germany 45 yr old male preoperative
Tailored treatment in Brugada syndrome Lars Eckardt Department of Cardiology and Angiology Division of Experimental and Clinical Electrophysiology University of Münster, Germany 45 yr old male preoperative
Hereditary Cardiovascular Conditions. genetic testing for undiagnosed diseases
 Hereditary Cardiovascular Conditions genetic testing for undiagnosed diseases What is Hypertrophic Cardiomyopathy (HCM)? normal heart heart with hcm Extra or thick heart muscle Typically in the left ventricle
Hereditary Cardiovascular Conditions genetic testing for undiagnosed diseases What is Hypertrophic Cardiomyopathy (HCM)? normal heart heart with hcm Extra or thick heart muscle Typically in the left ventricle
What Every Physician Should Know:
 What Every Physician Should Know: The Canadian Heart Rhythm Society estimates that, in Canada, sudden cardiac death (SCD) is responsible for about 40,000 deaths annually; more than AIDS, breast cancer
What Every Physician Should Know: The Canadian Heart Rhythm Society estimates that, in Canada, sudden cardiac death (SCD) is responsible for about 40,000 deaths annually; more than AIDS, breast cancer
Clinical and Electrocardiographic Characteristics of Patients with Brugada Syndrome: Report of Five Cases of Documented Ventricular Fibrillation
 J Arrhythmia Vol 25 No 1 2009 Original Article Clinical and Electrocardiographic Characteristics of Patients with Brugada Syndrome: Report of Five Cases of Documented Ventricular Fibrillation Seiji Takashio
J Arrhythmia Vol 25 No 1 2009 Original Article Clinical and Electrocardiographic Characteristics of Patients with Brugada Syndrome: Report of Five Cases of Documented Ventricular Fibrillation Seiji Takashio
ARVC when TO IMPLANT THE ASYMPTOMATIC PERSON
 EUROPACE 2011 INHERITED ELECTRICAL CARDIAC DISORDERS ARVC when TO IMPLANT THE ASYMPTOMATIC PERSON June 26 th 2011 Robert Lemery MD CONFLICTS of INTEREST None ASYMPTOMATIC ARVC 1. ECG 2. ASYMPTOMATIC PVC
EUROPACE 2011 INHERITED ELECTRICAL CARDIAC DISORDERS ARVC when TO IMPLANT THE ASYMPTOMATIC PERSON June 26 th 2011 Robert Lemery MD CONFLICTS of INTEREST None ASYMPTOMATIC ARVC 1. ECG 2. ASYMPTOMATIC PVC
SUDDEN CARDIAC DEATH(SCD): Definition
: Definition") SUDDEN CARDIAC DEATH EPIDEMIOLOGY, PATHOPHYSIOLOGY, PREVENTION & THERAPY Hasan Garan, M.D. Columbia University Medical Center SUDDEN CARDIAC DEATH(SCD): Definition DEATH DUE TO A CARDIAC CAUSE IN A CLINICALLY
SUDDEN CARDIAC DEATH EPIDEMIOLOGY, PATHOPHYSIOLOGY, PREVENTION & THERAPY Hasan Garan, M.D. Columbia University Medical Center SUDDEN CARDIAC DEATH(SCD): Definition DEATH DUE TO A CARDIAC CAUSE IN A CLINICALLY
Sudden Cardiac Death in the Young: Advances in Risk-stratification and Treatment
 PEDIATRIC CARDIOLOGY and CARDIAC SURGERY VOL. 25 NO. 1 (8 15) Sudden Cardiac Death in the Young: Advances in Risk-stratification and Treatment Michael J. Silka and Yaniv Bar-Cohen Division of Cardiology,
PEDIATRIC CARDIOLOGY and CARDIAC SURGERY VOL. 25 NO. 1 (8 15) Sudden Cardiac Death in the Young: Advances in Risk-stratification and Treatment Michael J. Silka and Yaniv Bar-Cohen Division of Cardiology,
State of the Art: Brugada Syndrome Novel diagnostic approaches and risk stratification
 State of the Art: Brugada Syndrome Novel diagnostic approaches and risk stratification Lars Eckardt Division Electrophysiology Department of Cardiovascular Medicine University of Münster, Germany I have
State of the Art: Brugada Syndrome Novel diagnostic approaches and risk stratification Lars Eckardt Division Electrophysiology Department of Cardiovascular Medicine University of Münster, Germany I have
ECG Workshop. Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care
 ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
Index. cardiacep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Risk Factors for Sudden cardiac Death
 Risk Factors for Sudden cardiac Death A. Arenal Arrhythmias in competitive sports Disclosure Conflict of interest Advisory board: Medtronic, Boston Scientific Research grants: Medtronic, Boston Scientific,
Risk Factors for Sudden cardiac Death A. Arenal Arrhythmias in competitive sports Disclosure Conflict of interest Advisory board: Medtronic, Boston Scientific Research grants: Medtronic, Boston Scientific,
Hereditary Conditions Predisposing to Sudden Death
 Hereditary Conditions Predisposing to Sudden Death Barry London, MD PhD University of Pittsburgh Medical Center Pittsburgh, PA SCAA/HRS/UPMC Symposium Managing the Patient at Risk for Sudden Death 10/08/10
Hereditary Conditions Predisposing to Sudden Death Barry London, MD PhD University of Pittsburgh Medical Center Pittsburgh, PA SCAA/HRS/UPMC Symposium Managing the Patient at Risk for Sudden Death 10/08/10
SUDDEN CARDIAC DEATH(SCD): Definition
: Definition") SUDDEN CARDIAC DEATH EPIDEMIOLOGY, PATHOPHYSIOLOGY, PREVENTION & THERAPY Hasan Garan, M.D. Columbia University Medical Center SUDDEN CARDIAC DEATH(SCD): Definition DEATH DUE TO A CARDIAC CAUSE IN A CLINICALLY
SUDDEN CARDIAC DEATH EPIDEMIOLOGY, PATHOPHYSIOLOGY, PREVENTION & THERAPY Hasan Garan, M.D. Columbia University Medical Center SUDDEN CARDIAC DEATH(SCD): Definition DEATH DUE TO A CARDIAC CAUSE IN A CLINICALLY
CONGENITAL LONG QT SYNDROME(CLQTS) ASSOCIATED WITH COMPLETE ATRIOVENTRICULAR BLOCK. A CASE REPORT.
 ASSOCIATED WITH COMPLETE ATRIOVENTRICULAR BLOCK. A CASE REPORT.") CONGENITAL LONG QT SYNDROME(CLQTS) ASSOCIATED WITH COMPLETE ATRIOVENTRICULAR BLOCK. A CASE REPORT. SAHA Annual Congress 2017. Samkelo Jiyana, Adele Greyling, Andile Nxele, ZM,Makrexeni,L.Pepeta. BACKGROUND
CONGENITAL LONG QT SYNDROME(CLQTS) ASSOCIATED WITH COMPLETE ATRIOVENTRICULAR BLOCK. A CASE REPORT. SAHA Annual Congress 2017. Samkelo Jiyana, Adele Greyling, Andile Nxele, ZM,Makrexeni,L.Pepeta. BACKGROUND
DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY. David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
 Division of Cardiology The University of Hong Kong") APHRS Summit 2018 in conjunction with HKCC Heart Rhythm Refresher Course DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
APHRS Summit 2018 in conjunction with HKCC Heart Rhythm Refresher Course DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
CME Article Brugada pattern masking anterior myocardial infarction
 Electrocardiography Series Singapore Med J 2011; 52(9) : 647 CME Article Brugada pattern masking anterior myocardial infarction Seow S C, Omar A R, Hong E C T Cardiology Department, National University
Electrocardiography Series Singapore Med J 2011; 52(9) : 647 CME Article Brugada pattern masking anterior myocardial infarction Seow S C, Omar A R, Hong E C T Cardiology Department, National University
Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες
 Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou
Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou
The impact of clinical and genetic findings on the management of young Brugada Syndrome patients
 12 ème Congrès Médico-Chirugical de la FCPC 21 au 24 novembre 2015 Schoelcher, Martinique The impact of clinical and genetic findings on the management of young Brugada Syndrome patients Institut du Thorax,
12 ème Congrès Médico-Chirugical de la FCPC 21 au 24 novembre 2015 Schoelcher, Martinique The impact of clinical and genetic findings on the management of young Brugada Syndrome patients Institut du Thorax,
Management of Arrhythmia Syndromes in the Newborn and Very Young Child: Unique Risks & Barriers in this Age Population
 Management of Arrhythmia Syndromes in the Newborn and Very Young Child: Unique Risks & Barriers in this Age Population Mitchell Cohen, MD FACC FHRS Co-Director Heart Center Chief of Pediatric Cardiology
Management of Arrhythmia Syndromes in the Newborn and Very Young Child: Unique Risks & Barriers in this Age Population Mitchell Cohen, MD FACC FHRS Co-Director Heart Center Chief of Pediatric Cardiology
TABLE 1. Mutations in the Cardiac Ryanodine Receptor Gene (RyR2) Associated With CPVT and ARVD2* Amino acid Nucleotide Disease Families Familial? Doma
 Associated With CPVT and ARVD2* Amino acid Nucleotide Disease Families Familial? Doma") EDITORIAL Sudden Unexplained Death Caused by Cardiac Ryanodine Receptor (RyR2) Mutations About 10% to 20% of postmortem examinations of young people who were apparently healthy but died suddenly and unexpectedly
EDITORIAL Sudden Unexplained Death Caused by Cardiac Ryanodine Receptor (RyR2) Mutations About 10% to 20% of postmortem examinations of young people who were apparently healthy but died suddenly and unexpectedly
Catecholaminergic Polymorphic Ventricular Tachycardia Looking to the Future
 Mædica - a Journal of Clinical Medicine MAEDICA a Journal of Clinical Medicine 2017; 12(4): 306-310 State of the art Catecholaminergic Polymorphic Ventricular Tachycardia Looking to the Future Andreea
Mædica - a Journal of Clinical Medicine MAEDICA a Journal of Clinical Medicine 2017; 12(4): 306-310 State of the art Catecholaminergic Polymorphic Ventricular Tachycardia Looking to the Future Andreea
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: April 15, 2018 Related Policies: None Genetic Testing for Cardiac Ion Channelopathies Description Genetic testing is available for patients suspected of having
FEP Medical Policy Manual Effective Date: April 15, 2018 Related Policies: None Genetic Testing for Cardiac Ion Channelopathies Description Genetic testing is available for patients suspected of having
3/17/2014. NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death. Objectives
 NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death Denise Pond BSN, RN The following relationships exist related to this presentation: No Disclosures Objectives Discuss
NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death Denise Pond BSN, RN The following relationships exist related to this presentation: No Disclosures Objectives Discuss
P. Brugada 1, R. Brugada 2 and J. Brugada 3. Introduction. U.S.A.; 3 Unitat d Arritmias, Hospital Clinic, Barcelona, Spain
 European Heart Journal (2000) 21, 321 326 Article No. euhj.1999.1751, available online at http://www.idealibrary.com on Sudden death in patients and relatives with the syndrome of right bundle branch block,
European Heart Journal (2000) 21, 321 326 Article No. euhj.1999.1751, available online at http://www.idealibrary.com on Sudden death in patients and relatives with the syndrome of right bundle branch block,
J Wave Syndromes. Osama Diab Lecturer of Cardiology Ain Shams University
 J Wave Syndromes Osama Diab Lecturer of Cardiology Ain Shams University J Wave Syndromes Group of electric disorders characterized by > 1 mm elevation of the J point or prominent J wave with or without
J Wave Syndromes Osama Diab Lecturer of Cardiology Ain Shams University J Wave Syndromes Group of electric disorders characterized by > 1 mm elevation of the J point or prominent J wave with or without
Genomics and Cardiac Arrhythmias
 Journal of the American College of Cardiology Vol. 47, No. 1, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.08.059
Journal of the American College of Cardiology Vol. 47, No. 1, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.08.059
Cardiac Emergencies Workshop
 Cardiac Emergencies Workshop Yolenda Westra MD FRCPC Grande Prairie Po Kee Cheung MBBS FRCP FRCPC FACC Co-Director,Cardiac Catheterization Laboratory, RAH Faculty/Presenter Disclosure Faculty: Dr. Yolande
Cardiac Emergencies Workshop Yolenda Westra MD FRCPC Grande Prairie Po Kee Cheung MBBS FRCP FRCPC FACC Co-Director,Cardiac Catheterization Laboratory, RAH Faculty/Presenter Disclosure Faculty: Dr. Yolande
SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY TRIVANDRUM, KERALA PROJECT REPORT. Dr. AAMIR RASHID. DM Trainee
 SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY TRIVANDRUM, KERALA PROJECT REPORT Submitted during the course of DM Cardiology Dr. AAMIR RASHID DM Trainee DEPARTMENT OF CARDIOLOGY Jan
SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY TRIVANDRUM, KERALA PROJECT REPORT Submitted during the course of DM Cardiology Dr. AAMIR RASHID DM Trainee DEPARTMENT OF CARDIOLOGY Jan
Genetic Testing for Heredity Cardiac Disease
 Clinical Appropriateness Guidelines Genetic Testing for Heredity Cardiac Disease EFFECTIVE DECEMBER 1, 2017 Appropriate.Safe.Affordable 2017 AIM Specialty Health 2064-1217 Table of Contents Scope... 3
Clinical Appropriateness Guidelines Genetic Testing for Heredity Cardiac Disease EFFECTIVE DECEMBER 1, 2017 Appropriate.Safe.Affordable 2017 AIM Specialty Health 2064-1217 Table of Contents Scope... 3
The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia
 The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia By Sandeep Joshi, MD and Jonathan S. Steinberg, MD Arrhythmia Service, Division of Cardiology
The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia By Sandeep Joshi, MD and Jonathan S. Steinberg, MD Arrhythmia Service, Division of Cardiology
Clinical and Molecular Characterization of Patients With Catecholaminergic Polymorphic Ventricular Tachycardia
 Clinical and Molecular Characterization of Patients With Catecholaminergic Polymorphic Ventricular Tachycardia Silvia G. Priori, MD, PhD; Carlo Napolitano, MD, PhD; Mirella Memmi, PhD; Barbara Colombi,
Clinical and Molecular Characterization of Patients With Catecholaminergic Polymorphic Ventricular Tachycardia Silvia G. Priori, MD, PhD; Carlo Napolitano, MD, PhD; Mirella Memmi, PhD; Barbara Colombi,
EPICARDIAL ABLATION IN GENETIC CARDIOMYOPATHIES: A NEW FRONTIER
 EPICARDIAL ABLATION IN GENETIC CARDIOMYOPATHIES: A NEW FRONTIER C. Pappone, M. M. Monasky, G. Ciconte Arrhythmology and Electrophysiology Department, IRCCS Policlinico San Donato, San Donato Milanese,
EPICARDIAL ABLATION IN GENETIC CARDIOMYOPATHIES: A NEW FRONTIER C. Pappone, M. M. Monasky, G. Ciconte Arrhythmology and Electrophysiology Department, IRCCS Policlinico San Donato, San Donato Milanese,