Congenital Heart Disease. Mohamed Waheed Elsharief.
|
|
|
- Ginger York
- 5 years ago
- Views:
Transcription


1 Congenital Heart Disease Mohamed Waheed Elsharief.

2 Objectives l By the end of this lecture you should be able to
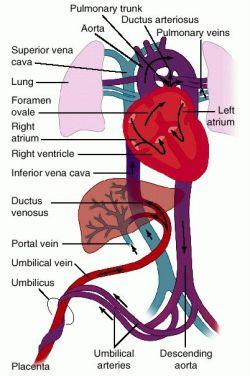
3 Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little work l RV & LV contribute equally to the systemic circulation and pump against similar resistance l Shunts are necessary for survival ductus venosus (bypasses liver) foramen ovale (R L atrial level shunt) ductus arteriosus (R L arterial level shunt)
4
5 100% 90/ 60 20/8 75% 75% 100% 20/ 90/ l No shunts l No pressure gradients l Normal AV valves l Normal semilunar valves l If this patient was desaturated what would you think?
6 Definition and etiology l Any deviation in the sequence of embryogenesis structural, functional or positional defect presents at birth which manifest any time after birth. l Normal embryogenesis depend genes, enivroment infections
7 Congenital Heart Disease (CHD) l Occurs in 8: 1000 of all live births l Simple way to classify is: L R shunts (Acyanotic) Cyanotic CHD (R L shunts) Obstructive lesions
 l Atrioventricular Septal Defect (AV Canal) l Patent Ductus")
8 Acyanotic Congenital Heart Disease Left-to-Right Shunt Lesions l Atrial Septal Defect (ASD) l Ventricular Septal Defect (VSD) l Atrioventricular Septal Defect (AV Canal) l Patent Ductus Arteriosus (PDA)

9 Atrial Septal Defect l ASD is an opening in the atrial septum permitting free communication of blood between the atria. Seen in 10% of all CHD.
10 Atrial Septal Defect l There are 3 major types: l Secundum ASD at the Fossa Ovalis, most common. Primum ASD lower in position & is a form of ASVD, MV cleft. Sinus Venosus ASD high in the atrial septum, associated w/partial anomalous venous return & the least common.


11 Atrial Septal Defect l Secundum ASD l Sinus Venosus ASD
12 Atrial Septal Defect Clinical Signs & Symptoms l Rarely presents with signs of CHF or other cardiovascular symptoms. Most are asymptomatic but may have easy fatigability or mild growth failure. Cyanosis does not occur unless pulmonary HTN is present.
13 Atrial Septal Defect Clinical Signs & Symptoms Hyperactive precordium, RV heave, fixed widely split S2. II-III/VI systolic ejection LSB. Mid-diastolic murmur heard over LLSB.

14 Atrial Septal Defect Treatment: l Surgical or catherization laboratory closure is generally recommended for secundum ASD Closure is performed electively between ages 2 & 5 yrs to avoid late complications. Surgical correction is done earlier in children w/ CHF or significant Pulm HTN.
15 Atrial Septal Defect Treatment Once pulmonary HTN w/ shunt reversal occurs this is considered too late. Mortality is < 1%.

16 Ventricular Septal Defect l VSD is an abnormal opening in the ventricular septum, which allows free communication between the Rt & Lt ventricles. Accounts for 30% of CHD.
17 Ventricular Septal Defect l 4 Types l Perimembranous (or membranous) Most common. l Infundibular (subpulmonary or supracristal VSD) involves the RV outflow tract. Muscular VSD can be single or multiple. AVSD inlet VSD, almost always involves AV valvular abnormalities.
18 Ventricular Septal Defect Hemodynamics l The left to right shunt occurs secondary to PVR being < SVR, not the higher pressure in the LV. l This leads to elevated RV & pulmonary pressures & volume hypertrophy of the LA & LV.
19 Ventricular Septal Defect Clinical Signs & Symptoms Small - moderate VSD, >5mm, are usually asymptomatic and 50% will close spontaneously by age 2yrs. Moderate 10-5 large VSD, almost always have symptoms and will require surgical repair.
20 Ventricular Septal Defect Clinical Signs & Symptoms II-III/VI harsh holosystolic murmur heard along the LSB, more prominent with small VSD, maybe absent with a very Large VSD. Prominent P2, Diastolic murmur. CHF, FTT, Respiratory infections, exercise intolerance hyperactive precordium. Symptoms develop between 1 6 months
21 Ventricular Septal Defect Treatment Small VSD - no surgical intervention, no physical restrictions, just reassurance and periodic follow-up and endocarditis prophylaxis. Symptomatic VSD - Medical treatment initially with afterload reducers & diuretics.
22 Ventricular Septal Defect Treatment l Indications for Surgical Closure: l Large VSD w/ medically uncontrolled symptomatology & continued FTT. l Ages 6-12 mo w/ large VSD & Pulm. HTN l Age > 24 mo w/ Qp:Qs ratio > 2:1. l Supracristal VSD of any size, secondary to risk of developing AV insufficiency.
23 Atrioventricular Septal Defect l AVSD results from incomplete fusion the the endocardial cushions, which help to form the lower portion of the atrial septum, the membranous portion of the ventricular septum and the septal leaflets of the triscupid and mitral valves. l They account for 4% OF ALL CHD.
24 Atrioventricular Septal Defect l Question: What genetic disease is AVSD more commonly seen in? Answer: Down s Syndrome (Trisomy 21), Seen in 20-25% of cases.

25 Atrioventricular Septal Defect l Complete AVSD
26 Atrioventricular Septal Defect Clinical Signs & Symptoms l Incomplete AVSD maybe indistinguishable from ASD - usually asymptomatic. l Congestive heart failure in infancy. l Recurrent pulmonary infections. l Failure to thrive. l Exercise intolerance, easy fatigability. l Late cyanosis from pulmonary vascular disease w/ R to L shunt.
27 Atrioventricular Septal Defect Clinical Signs & Symptoms l Hyperactive precordium l Normal or accentuated 1 st hrt sound l Wide, fixed splitting of S2 l Pulmonary systolic ejection murmur w/thrill l Holosystolic apex w/radiation to axilla l Mid-diastolic rumbling LSB l Marked cardiac enlargement on CX-Ray
28 Atrioventricular Septal Defect Treatment l Surgery is always required. l Treat congestive symptoms. l Pulmonary banding maybe required in premature infants or infants < 5 kg. l Correction is done during infancy to avoid irreversible pulmonary vascular disease. l Mortality low w/incomplete 1-2% & as high as 5% with complete AVSD.
29 Patent Ductus Arteriosus l PDA Persistence of the normal fetal vessel that joins the PA to the Aorta. l Normally closes in the 1 st wk of life. l Accounts for 10% of all CHD, seen in 10% of l Female : Male ratio of 2:1 l Often associated w/ coarctation & VSD.
30 Patent Ductus Arteriosus l Question: What TORCH infection is PDA associated with? Answer: Rubella
31 Patent Ductus Arteriosus Hemodynamics l As a result of higher aortic pressure, blood shunts L to R through the ductus from Aorta to PA. l Extent of the shunt depends on size of the ductus & PVR:SVR. l Small PDA, pressures in PA, RV, RA are normal.
32 Patent Ductus Arteriosus Hemodynamics l Large PDA, PA pressures are equal to systemic pressures. In extreme cases 70% of CO is shunted through the ductus to pulmonary circulation. l Leads to increased pulmonary vascular disease.
33 Patent Ductus Arteriosus Clinical Signs & Symptoms l Small PDA s are usually asymptomatic l Large PDA s can result in symptoms of CHF, growth restriction, FTT. l Bounding arterial pulses l Widened pulse pressure l Enlarged heart, prominent apical impulse l Classic continuous machinary systolic murmur l Mid-diastolic murmur at the apex

34 Patent Ductus Arteriosus Treatment l Indomethacin, inhibitor of prostaglandin synthesis can be used in premature infants. l PDA requires surgical or catheter closure. l Closure is required treatment heart failure & to prevent pulmonary vascular disease. l Usually done by ligation & division or intra vascular coil. l Mortality is < 1%
35
36 Obstructive Heart Lesions l Pulmonary Stenosis l Aortic Stenosis l Coarctation of the Aorta

37 Pulmonary Stenosis l Pulmonary Stenosis is obstruction in the region of either the pulmonary valve or the subpulmonary ventricular outflow tract. l Accounts for 7-10% of all CHD. l Most cases are isolated lesions l Maybe biscuspid or fusion of 2 or more leaflets. l Can present w/or w/o an intact ventricular septum.
38 Pulmonary Stenosis l Question: What syndrome is PS associated with? l Answer: Noonan s Syndrome, secondary to valve dysplasia.
39 Pulmonary Stenosis Hemodynamics l RV pressure hypertrophy RV failure. l RV pressures maybe > systemic pressure. l Post-stenotic dilation of main PA. l W/intact septum & severe stenosis R-L shunt through PFO cyanosis. l Cyanosis is indicative of Critical PS.
40 Pulmonary Stenosis Clinical Signs & Symptoms l Depends on the severity of obstruction. l Asymptomatic w/ mild PS < 30mmHg. l Mod-severe: 30-60mmHg, > 60mmHg l Prominent jugular a-wave, RV lift l Split 2 nd hrt sound w/ a delay l Ejection click, followed by systolic murmur. l Heart failure & cyanosis seen in severe cases.
41 Pulmonary Stenosis Treatment l Mild PS no intervention required, close follow-up. l Mod-severe require relieve of stenosis. l Balloon valvuloplasty, treatment of choice. l Surgical valvotomy is also a consideration.
42 Aortic Stenosis l Aortic Stenosis is an obstruction to the outflow from the left ventricle at or near the aortic valve that causes a systolic pressure gradient of more than 10mmHg. Accounts for 7% of CHD. l 3 Types l Valvular Most common. l Subvalvular(subaortic) involves the left outflow tract. l Supravalvular involves the ascending aorta is the least common.
43 Aortic Stenosis l Question: Which syndrome is supravalvular stenosis found in? l Answer: Williams Syndrome

44 Aortic Stenosis Hemodynamics l Pressure hypertrophy of the LV and LA with obstruction to flow from the LV. l Mild AS l Moderate AS l Severe AS 0-25mmHG 25-50mmHg 50-75mmHg l Critical AS > 75mmHg
45 Aortic Stenosis Clinical Signs & Symptoms l Mild AS may present with exercise intolerance, easy fatigabiltity, but usually asymptomatic. l Moderate AS Chest pain, dypsnea on exertion, dizziness & syncope. l Severe AS Weak pulses, left sided heart failure, Sudden Death.
46 Aortic Stenosis Clinical Signs & Symptoms l LV thrust at the Apex. l Systolic rt base/suprasternal notch. l Ejection click, III-IV/VI systolic RSB/LSB w/ radiation to the carotids.
47 Aortic Stenosis Treatment l Because surgery does not offer a cure it is reserved for patients with symptoms and a resting gradient of 60-80mmHg. l For subaortic stenosis it is reserved for gradients of 40-50mmHg because of it s rapidly progressive nature. l Balloon valvuloplasty is the standard of treatment.
48 Aortic Stenosis Treatment l Aortic insufficiency & re-stenosis is likely after surgery and may require valve replacement. l Activity should not be restricted in Mild AS. l Mod-severe AS, no competitive sports.
49 Coarctation of the Aorta l Coarctation- is narrowing of the aorta at varying points anywhere from the transverse arch to the iliac bifurcation. l 98% of coarctations are juxtaductal l Male: Female ratio 3:1. l Accounts for 7 % of all CHD.

50 Coarctation of the Aorta l Question: What other heart anomaly is coarctation associated with? l Answer: Bicuspid aortic valve, seen in > 70% of cases.
51 Coarctation of the Aorta l Question: What genetic syndrome is coarctation seen in? l Answer: Turner s Syndrome

52 Coarctation of the Aorta Hemodynamics l Obstruction of left ventricular outflow pressure hypertrophy of the LV.
53 Coarctation of the Aorta Clinical Signs & Symptoms l Classic signs of coarctation are diminution or absence of femoral pulses. l Higher BP in the upper extremities as compared to the lower extremities. l 90% have systolic hypertension of the upper extremities. l Pulse discrepancy between rt & lt arms.
54 Coarctation of the Aorta Clinical Signs & Symptoms l With severe coarc. LE hypoperfusion, acidosis, HF and shock. l Differential cyanosis if ductus is still open l II/VI systolic ejection LSB. l Cardiomegaly, rib notching on X-ray.

55 Coarctation of the Aorta
56 Coarctation of the Aorta Treatment l With severe coarctation maintaining the ductus with prostaglandin E is essential. l Surgical intervention, to prevent LV dysfunction. l Angioplasty is used by some centers. l Re-coarctation can occur, balloon angioplasty is the procedure of choice.
57 Cyanotic Heart Diseases Eisenmenger s Syndrome
58 l Anatomic Defects Ventricular septal defect Overriding Aorta Pulmonary artery stenosis Right ventricular hypertrophy Tetralogy of Fallot Picture:
59 Tetralogy of Fallot l Pathophysiology: Increased resistance by the pulmonary stenosis causes deoxygenated systemic venous return to be diverted from RV, through VSD to the overriding aorta and systemic circulation à systemic hypoxemia and cyanosis Picture:
60 Tetralogy of Fallot l Symptoms: Dyspnea on exertion or when crying Tet spells: irritability, cyanosis, hyperventilation and sometimes syncope or convulsions due to cerebral hypoxemia. Patients learn to alleviate symptoms by squatting which increases systemic resistance and decreases the right-to-left shunt and directs more blood to the pulmonary circulation.
61 Tetralogy of Fallot l Physical exam: Clubbing of the fingers and toes Systolic ejection murmur heard at the upper left sternal border created by turbulent blood flow through stenotic RV outflow tract l Lab Studies: High PCV CXR: prominent RV EKG: RVH, right axis deviation ECHO: displays and quantifies extent of RV outflow tract obstruction
62 What is the difference between these two films?- both are infants with congenital heart disease.
63 Tetralogy of Fallot l Treatment: Antibiotic with procedures Surgical closure of the VSD and enlargement of the pulmonary outflow tract -Patient given beta blockers for prophylaxis against Tet spells - Treat spells by - Position knee chest - Oxygen - Fluids - Morphine - B blockers - Complications Brain abscess thrombosis, iron deficiency - Q can they present with heart failure?

64 Transposed Great Arteries l Blue. Presents with cyanosis when the duct closes.
65 24 Hours to 2 Weeks Cyanotic Ductal-Dependent Lesions l CXR helps in diagnosis - oligaemic lungfields PS, pulmonary atresia etc - plethoric lungfields TGA - congestion TAPVD - massive cardiomegaly Ebstein s
66 What is the difference between these two films?- both are infants with congenital heart disease.
67 Cyanotic infant- a lung problem or a heart problem? l Investigations- suggests heart if: - CXR- clear lung fields and - ECG- normal and - Hyperoxia test normal ( breathing 100% oxygen, if po 2 >150mmHg very unlikely to be cyanotic heart disease) - (Echocardiogram is the definitive test)

68 24 Hours to 2 Weeks Heart failure Ductal-Dependent Lesions l Heart failure is due to left heart obstruction NOT L-R shunts at this age! eg. Coarctation Critical Aortic stenosis Hypoplastic left heart Mitral stenosis (rare)
69 كل عام وانتم l بخير
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acyanotic Congenital Heart Lesions. These podcasts are designed to give medical students an overview of key topics in
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acyanotic Congenital Heart Lesions. These podcasts are designed to give medical students an overview of key topics in
بسم هللا الرحمن الرحيم. The cardio vascular system By Dr.Rawa Younis Mahmood
 بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Paediatric Cardiology. Acyanotic CHD. Prof F F Takawira
 Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Most common fetal cardiac anomalies
 Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
DORV: The Great Chameleon. Heart Conference October 15, 2016 Tina Kwan, MD
 DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
Congenital Heart Disease: Cyanotic Lesions. Amitesh Aggarwal
 Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Ummeenatrbilaoiasetptiwmsaiiri
 atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
SPECIFIC HEART DEFECTS
 A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Adult Congenital Heart Disease for the Internist
 Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist
 Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Nursing Care of Children and their Families: Alterations in Cardiac Function
 Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Upon completion of this presentation, the participant will be able to:
 B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
FANNP 28TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW OCTOBER 17-21, 2017
 Neonatal Cardiology Review Nicole Bowie, NNP/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL B12 The speaker has signed a disclosure statement indicating that she has no significant
Neonatal Cardiology Review Nicole Bowie, NNP/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL B12 The speaker has signed a disclosure statement indicating that she has no significant
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
Notes: 1)Membranous part contribute in the formation of small portion in the septal cusp.
Membranous part contribute in the formation of small portion in the septal cusp.") Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
List of Videos. Video 1.1
 Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
APPROACH TO CARDIAC HISTORY TAKING. Index
 Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Neonatal Cardiac Anomalies
 Objectives Neonatal Cardiac Anomalies Karen Knuth, RNC, MN, NNP-BC, ARNP Seattle Childrens Hospital What is CHD? Normal anatomy and circulation Clinical presentation: signs and symptoms Diagnostics Common
Objectives Neonatal Cardiac Anomalies Karen Knuth, RNC, MN, NNP-BC, ARNP Seattle Childrens Hospital What is CHD? Normal anatomy and circulation Clinical presentation: signs and symptoms Diagnostics Common
Congenital Heart Disease. Children s Hospital Zhejiang University School of Medicine
 Congenital Heart Disease Children s Hospital Zhejiang University School of Medicine Cardiovascular Development Key periods:the 2 nd ~8 th weeks Fetal Circulation Physiological Changes in the Circulation
Congenital Heart Disease Children s Hospital Zhejiang University School of Medicine Cardiovascular Development Key periods:the 2 nd ~8 th weeks Fetal Circulation Physiological Changes in the Circulation
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Congenital Heart Disease
 Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
CONGENITAL HEART LESIONS ((C.H.L
 CONGENITAL HEART LESIONS ((C.H.L BY THE BOOKS: 0.8 IN FACT: 3-5% INCLUDING: - BICUSPID AORTIC VALVE MITRAL VALVE PROLAPSE LATE DIAGNOSIS - :INCREASED INCIDENCE IN ADULTS BETTER DIAGNOSIS IN INFANCY BETTER
CONGENITAL HEART LESIONS ((C.H.L BY THE BOOKS: 0.8 IN FACT: 3-5% INCLUDING: - BICUSPID AORTIC VALVE MITRAL VALVE PROLAPSE LATE DIAGNOSIS - :INCREASED INCIDENCE IN ADULTS BETTER DIAGNOSIS IN INFANCY BETTER
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS
 Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS iib6@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition
Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS iib6@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease. Pregnancy and Cardiovascular Disease MCQ
 Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Cardiovascular Pathophysiology:
 Learning Objectives Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS iib6@columbia.edu Learn the relationships between pressure, blood flow, and resistance Review the transition
Learning Objectives Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS iib6@columbia.edu Learn the relationships between pressure, blood flow, and resistance Review the transition
NCC Review Cardiac 8/22/12. Intrauterine Blood Flow. Topics
 NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Cardiac Ausculation in the Elderly
 Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
COMBINED CONGENITAL SUBAORTIC STENOSIS AND INFUNDIBULAR PULMONARY STENOSIS*
 COMBINED CONGENITAL SUBAORTIC STENOSIS AND INFUNDIBULAR PULMONARY STENOSIS* BY HENRY N. NEUFELD,t PATRICK A. ONGLEY, AND JESSE E. EDWARDS From the Sections of Pa?diatrics and Pathological Anatomy, Mayo
COMBINED CONGENITAL SUBAORTIC STENOSIS AND INFUNDIBULAR PULMONARY STENOSIS* BY HENRY N. NEUFELD,t PATRICK A. ONGLEY, AND JESSE E. EDWARDS From the Sections of Pa?diatrics and Pathological Anatomy, Mayo
Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley
 Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley Course Contents Purpose Objectives Introduction Fetal Circulation Neonatal Circulation
Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley Course Contents Purpose Objectives Introduction Fetal Circulation Neonatal Circulation
Cardiac Examination. Pediatrics Clinical Examination
 Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
A SURGEONS' GUIDE TO CARDIAC DIAGNOSIS
 A SURGEONS' GUIDE TO CARDIAC DIAGNOSIS PART II THE CLINICAL PICTURE DONALD N. ROSS B. Sc., M. B., CH. B., F. R. C. S. CONSULTANT THORACIC SURGEON GUY'S HOSPITAL, LONDON WITH 53 FIGURES Springer-Verlag
A SURGEONS' GUIDE TO CARDIAC DIAGNOSIS PART II THE CLINICAL PICTURE DONALD N. ROSS B. Sc., M. B., CH. B., F. R. C. S. CONSULTANT THORACIC SURGEON GUY'S HOSPITAL, LONDON WITH 53 FIGURES Springer-Verlag
What s That Sound? Pediatric Murmur Evaluation
 What s That Sound? Pediatric Murmur Evaluation Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director, Pediatric
What s That Sound? Pediatric Murmur Evaluation Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director, Pediatric
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Coarctation of the aorta
 T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
Case submission for CSI Asia-Pacific Case 2
 Case submission for CSI Asia-Pacific 2018- Case 2 Title Page Case category: Coarctation and ducts, valves Title: Simultaneous balloon aortic valvuloplasty with transcatheter closure of large hypertensive
Case submission for CSI Asia-Pacific 2018- Case 2 Title Page Case category: Coarctation and ducts, valves Title: Simultaneous balloon aortic valvuloplasty with transcatheter closure of large hypertensive
Heart sounds and murmurs. Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct
 Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Aortic Valve Lesions
 Version 1.0 Valvular Heart Disease 25/03/2012 Aortic Stenosis Aortic Valve Lesions General Most common isolated affected valve, esp elderly 4M:1F Unrecognised can be important cause of anaesthetic & obstetric
Version 1.0 Valvular Heart Disease 25/03/2012 Aortic Stenosis Aortic Valve Lesions General Most common isolated affected valve, esp elderly 4M:1F Unrecognised can be important cause of anaesthetic & obstetric
Pamela Heggie, RN BN Clinic Coordinator Northern Alberta Adult Congenital Heart (NAACH) Clinic Mazankowski Heart Institute
 Clinic Mazankowski Heart Institute") Pamela Heggie, RN BN Clinic Coordinator Northern Alberta Adult Congenital Heart (NAACH) Clinic Mazankowski Heart Institute Brief Overview of Congenital Heart Disease Spectrum disorder Treatment & Impact
Pamela Heggie, RN BN Clinic Coordinator Northern Alberta Adult Congenital Heart (NAACH) Clinic Mazankowski Heart Institute Brief Overview of Congenital Heart Disease Spectrum disorder Treatment & Impact
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray
 Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Murmurs and the Cardiac Physical Exam. Carolyn A. Altman Texas Children s Hospital Advanced Practice Provider Conference Houston, TX April 6, 2018
 Murmurs and the Cardiac Physical Exam Carolyn A. Altman Texas Children s Hospital Advanced Practice Provider Conference Houston, TX April 6, 2018 The Cardiac Physical Exam Before applying a stethoscope..
Murmurs and the Cardiac Physical Exam Carolyn A. Altman Texas Children s Hospital Advanced Practice Provider Conference Houston, TX April 6, 2018 The Cardiac Physical Exam Before applying a stethoscope..
Approach to a baby with cyanosis
 Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Cong.heart_desiases.docx. Олена Костянтинівна Редько
 Cong.heart_desiases.docx Олена Костянтинівна Редько 2015 Ключові терміни: 3 Зміст Ключові терміни: Acyanotic Congenital Heart Disease Heart and Main Vessels Atrioventricular Septal Defects (Ostium Primum
Cong.heart_desiases.docx Олена Костянтинівна Редько 2015 Ключові терміни: 3 Зміст Ключові терміни: Acyanotic Congenital Heart Disease Heart and Main Vessels Atrioventricular Septal Defects (Ostium Primum
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
The role of intraoperative TOE in congenital cardiac surgery
 The role of intraoperative TOE in congenital cardiac surgery Justiaan Swanevelder Dept of Anaesthesia Groote Schuur and Red Cross War Memorial Children s Hospitals University of Cape Town, South Africa
The role of intraoperative TOE in congenital cardiac surgery Justiaan Swanevelder Dept of Anaesthesia Groote Schuur and Red Cross War Memorial Children s Hospitals University of Cape Town, South Africa
THE SOUNDS AND MURMURS IN TRANSPOSITION OF THE
 Brit. Heart J., 25, 1963, 748. THE SOUNDS AND MURMURS IN TRANSPOSITION OF THE GREAT VESSELS BY BERTRAND WELLS From The Hospital for Sick Children, Great Ormond Street, London W. C.J Received April 18,
Brit. Heart J., 25, 1963, 748. THE SOUNDS AND MURMURS IN TRANSPOSITION OF THE GREAT VESSELS BY BERTRAND WELLS From The Hospital for Sick Children, Great Ormond Street, London W. C.J Received April 18,