Chest Pain. Scott A. Phillips, M.D. AnMed Health Carolina Cardiology
|
|
|
- Henry York
- 5 years ago
- Views:
Transcription

1 Chest Pain Scott A. Phillips, M.D. AnMed Health Carolina Cardiology
2 Cardiac Causes -Ischemic vs. Non-ischemic Non-Cardiac Causes -Pulmonary, GI, Musculoskeletal, Dermatology
3 1. Chest Wall Pain Sharp, Precisely localized Reproducible: Palpation, movement 2. Pleuritic or Respiratory CP Somatic pain, Sharp Worse with breathing/coughing 3. Visceral CP Poorly localized, aching, heaviness

4 Non-cardiac Chest Pain
5 Most common cause of non-cardiac chest pain Causes: -Esophagitis/Gastritis -Ulcers -Reflux -Esophageal Spasm (can be relieved with Nitro) -Pancreatitis -Gall bladder
6 Pleuritic (worse with breathing/coughing) Sharp/stabbing pain Causes: -Infections (bronchitis/pneumonia) -Pleural effusions (fluid around the lung) -Pulmonary Emboli (blood clots) -Pneumothorax (collapsed lung) -Malignancy
7 Costocondritis (inflammation of cartilage) Rib fracture Myalgia (muscle pains) Pain is worse with movements. May be reproducible with palpation.
8 Shingles (Herpes Zoster) Focal, dermatomal pain. Constant, burning/tingling pain. Pain starts several days before a rash is present.

9 Shingles
10 Ischemic: -Myocardial infarction (ACS) -Stable angina -Coronary vasospasm -Aortic stenosis -Hypertrophic cardiomyopathy Non-ischemic: -Pericarditis -Aortic dissection
11 Causes: -congenital -calcification -rheumatic fever Symptoms are typically exertional. Often associated with signs of heart failure. May also be associated with passing out (syncope). Loud systolic murmur heard on exam.

12
13 Abnormal thickening of the heart muscle. Hereditary Causes outflow obstruction from the left ventricle. Exertional chest pain, shortness of breath, and passing out, death. Loud murmur on exam.

14
15 Sudden onset of SEVERE ripping/tearing chest pain Radiates through to the back Associated with high blood pressure. Feeling of doom

16
17 Prinzmetal s Angina Spasms of the coronary arteries. More common in women Occurs at rest. Can look like a heart attack on EKG.

18
 Symptoms -Positional/pleuritic")
19 Causes -Infections (Viral, tuberculosis) -Kidney failure -Autoimmune diseases -Radiation -Heart attacks (Dressler s Syndrome) Symptoms -Positional/pleuritic chest pain

20 Pericarditis

21 Coronary Artery Disease

22 Plaque Rupture Thrombus Plaque rupture

23 Aspirated blood clot and plaque during MI
24 Characteristics Location Severity Duration Associated symptoms Radiation of pain Triggers (exertion, emotional distress) Relieving features (rest, aspirin, nitro)
25 Chest pain (heavy, burning, tight, pressure, sharp, tingling, stabbing, throbbing) Jaw/neck pain Arm pain/numbness Back pain Shortness of breath Nausea/vomiting, hiccups Sweating

26 Typical Anginal Pain Distribution
 Class III Marked limitation of ordinary activity Class IV Inability to carry out any physical activity without angina Angina occurs at")
27 Class I No angina with ordinary physical activity Class II Angina with strenuous/prolonged exertion Early-onset, limitation of ordinary activity (2 blocks/1 flight) Class III Marked limitation of ordinary activity Class IV Inability to carry out any physical activity without angina Angina occurs at rest
28 Pretest Probability
29 Does the pt fit into one of the following? 1. Noncardiac CP and low pretest probability No further testing needed. Pt does not have angina 2. Diagnosis of angina is established (high pretest prob) No further diagnostic testing needed. Pt needs risk stratification for prognosis 3. Diagnosis is still not clear (intermediate pretest prob) Consider the following tests to make a diagnosis

30 Algorithm for Evaluation and Management of Patients Suspected of Having ACS. Anderson J L et al. Circulation. 2011;123:e426-e579 Copyright American Heart Association, Inc. All rights reserved.
31
32
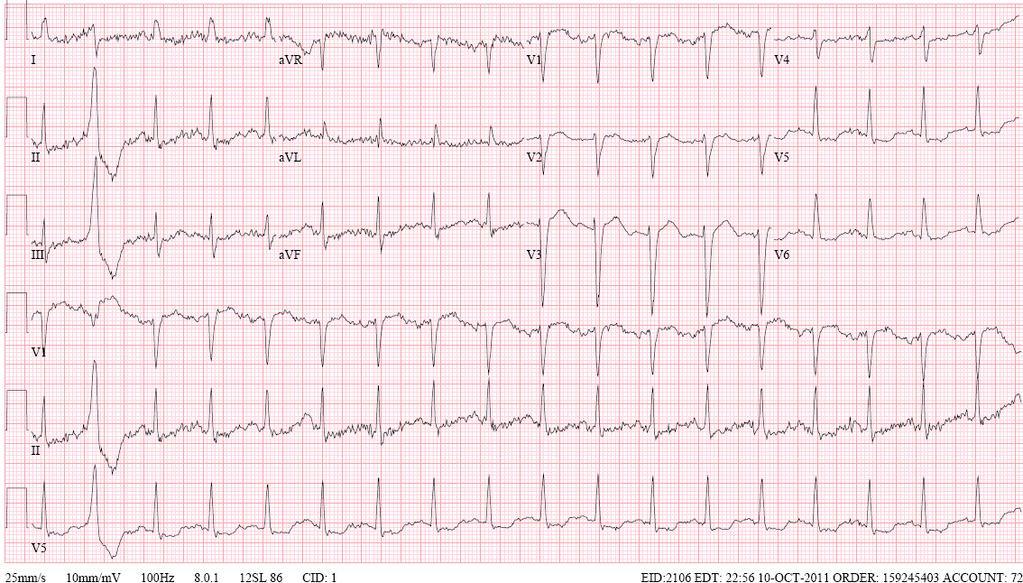
33 71 w/m with 2 month h/o exertional chest pressure. Presented to PCP office with worsening of symptoms during exertion. PMHx: Hyperlipidemia, HTN, CRI, ED Meds: Crestor, Prilosec, Cialis Allergies: NKDA FHx: None SocHx: smoker Exam: Afeb, 130/82, 85, 16, (Normal exam) Labs: BUN 20, Cr 1.0, Gluc 99, WBC 5, HCT 43, Plt 140 CXR: normal

34

35
36 63 w/m with 3 month h/o mild intermitent exertional chest pain. Worse and more frequent over past week. Severe episode with SOB prompting first time visit to PCP s office. PMHx: HTN Meds: Lisinopril, ASA. Allergies: NKDA FHx: CVA SocHx: non-smoker, rare EtOH, no illicits, pharmacist. Exam: Afeb, 149/98, 115, 18, 95% 2L NC NAD Tachycardic, 1/6 harsh syst murmur RUSB, JVD to jaw Bilateral rales half way up lung fields. Trace pedal edema, warm, 2+ pulses
37 WBC 12, HCT 43, Plt 333 BUN 21, Cr 0.8, Gluc 183 HgA1C 7.8 Chol 177, Trig 161, LDL 115, HDL 30 Trop 0.87, 1.03 CXR: pulmonary edema ECHO: EF 20%, mild AS
38

39
40 86 w/m with 6 month h/o exertional left sided chest pressure and DOE. Worsening over past 2 weeks. Presents to PCP after 2 episodes of resting pain. PMHx: HTN, COPD, Parkinson s, BPH, chronic anemia, OA. Meds: ASA, lisinopril, calcium, eye drops, combivent. Allergies: NKDA FHx: N/C SocHx: Lives with care taker, 3 sons, remains fairly active, non-smoker. Exam: Afeb, 105/70, 70, 14 Thin with mild Parkinsonian features. 2/6 syst murmur LSB. Labs: BUN 19, Cr 0.5, WBC 6, HCT 36, MCV 92, Plt 188 Imaging: CXR normal

41

42
43 76 w/f with 1 month h/o intermittent non-exertional burning mid epigastric/substernal chest discomfort partially relieved with TUMS. PMHx: HTN, hyperlipidemia, borderline DM PSHx: cholecystectomy and hysterectomy. Meds: ASA, Toprol, lisinopril, pravastatin. Allergies: NKDA FHx: CAD (father/brother) SocHx: Quit smoking 25 yrs ago. Exam: Afeb, 164/92 (didn t take a.m. meds), 59, 16 Otherwise normal exam. Labs: Normal Imaging: CXR normal.

44

45
46 Questions??????
Chest Pain. Dr. Amitesh Aggarwal. Department of Medicine
 Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Evaluation of Chest Pain in the Primary Care Setting. Joseph Hackler, DO. Disclosures
 Evaluation of Chest Pain in the Primary Care Setting Joseph Hackler, DO Disclosures I have no relevant relationships with commercial interests to disclose. 1 Objectives 1. Discuss the different etiologies
Evaluation of Chest Pain in the Primary Care Setting Joseph Hackler, DO Disclosures I have no relevant relationships with commercial interests to disclose. 1 Objectives 1. Discuss the different etiologies
Introduction to Risk Stratification
 Introduction to Risk Stratification Tim Fendler, MD, MSc Heart Failure/Transplant Fellow St. Luke s Mid America Heart Institute 1 Disclosures: No financial relationships to disclose. A 74 year-old male
Introduction to Risk Stratification Tim Fendler, MD, MSc Heart Failure/Transplant Fellow St. Luke s Mid America Heart Institute 1 Disclosures: No financial relationships to disclose. A 74 year-old male
Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria
 Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria Patient Status: Understanding Inpatient and Outpatient Observation Focusing on Chest Pain, TIAs, Syncope and Dizziness What
Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria Patient Status: Understanding Inpatient and Outpatient Observation Focusing on Chest Pain, TIAs, Syncope and Dizziness What
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Chest Pain in Children and Adolescents What an EMS Needs to Know. Frank C. Smith, M.D. Pediatric Cardiology Associates
 Chest Pain in Children and Adolescents What an EMS Needs to Know Frank C. Smith, M.D. Pediatric Cardiology Associates Chest Pain in Children and Adolescents Common in children (10-15%) Non-cardiac causes
Chest Pain in Children and Adolescents What an EMS Needs to Know Frank C. Smith, M.D. Pediatric Cardiology Associates Chest Pain in Children and Adolescents Common in children (10-15%) Non-cardiac causes
AIMS: CHEST PAIN. Causes of chest pain. Causes of chest pain: Cardiac causes: Acute coronary syndromes pericarditis thoracic aortic dissection
 CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN IS MY CHILD GOING. Thomas C. Martin MD, FAAP, FACC EMMC Pediatric Cardiology Eastern Maine Medical Center Bangor, Maine
 CHEST PAIN IN CHILDREN: IS MY CHILD GOING TO DIE? Thomas C. Martin MD, FAAP, FACC EMMC Pediatric Cardiology Eastern Maine Medical Center Bangor, Maine DISCLAIMER Presentation t ti at the Maine Chapter,
CHEST PAIN IN CHILDREN: IS MY CHILD GOING TO DIE? Thomas C. Martin MD, FAAP, FACC EMMC Pediatric Cardiology Eastern Maine Medical Center Bangor, Maine DISCLAIMER Presentation t ti at the Maine Chapter,
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
Chest Pain 101: Fine Tuning Your Differential in the Outpatient Setting. Krysten Pilkington MNSc, APRN, AG-ACNP-BC
 Chest Pain 101: Fine Tuning Your Differential in the Outpatient Setting Krysten Pilkington MNSc, APRN, AG-ACNP-BC Where do we start? Onset Location Duration Characteristics Aggravating & Alleviating factors
Chest Pain 101: Fine Tuning Your Differential in the Outpatient Setting Krysten Pilkington MNSc, APRN, AG-ACNP-BC Where do we start? Onset Location Duration Characteristics Aggravating & Alleviating factors
Ischaemic Heart Disease
 Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Heart Disorders. Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders
 Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders") Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
12 Lead EKG Chapter 4 Worksheet
 Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Cardiovascular and Respiratory Disorders
 Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Women and Vascular Disease
 Women and Vascular Disease KEVIN F. REBECK PA-C VASCULAR TRANSPLANT SURGERY 1 The Scope of the Problem One woman dies every minute from cardiovascular disease in the U.S.! The Scope of the Problem CVD
Women and Vascular Disease KEVIN F. REBECK PA-C VASCULAR TRANSPLANT SURGERY 1 The Scope of the Problem One woman dies every minute from cardiovascular disease in the U.S.! The Scope of the Problem CVD
Intensity: 0-10 (10 is the worse pain you have ever experienced in your life that you would want to jump from a building, 0 is no pain)
") Patient Questionnaire: Name: Date: Occupation: Date of Birth: Age: Sex: Male Female Referring Physician: Chief Complaint: Describe your Pain: sudden onset gradual constant intermittent worsening improving
Patient Questionnaire: Name: Date: Occupation: Date of Birth: Age: Sex: Male Female Referring Physician: Chief Complaint: Describe your Pain: sudden onset gradual constant intermittent worsening improving
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
PAEDIATRIC ACUTE CARE GUIDELINE. Chest Pain
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Chest Pain: An Approach Raja Dhar
 Chest Pain: An Approach Raja Dhar MD, MRCP (UK), MSc (EBM, UK), CCT (UK), FCCP (US) Consultant Respiratory Physician, Fortis Director, Education and Research NAABI Kolkata. The background: Chest pain is
Chest Pain: An Approach Raja Dhar MD, MRCP (UK), MSc (EBM, UK), CCT (UK), FCCP (US) Consultant Respiratory Physician, Fortis Director, Education and Research NAABI Kolkata. The background: Chest pain is
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
2/12/2011 Statistics Cardiovascular Emergencies time is myocardium! Cardiovascular disease (CVD) claimed over 1 million lives in CVD has been th
 claimed over 1 million lives in CVD has been th") Statistics Cardiovascular Emergencies time is myocardium! Cardiovascular disease (CVD) claimed over 1 million lives in 2004. CVD has been the leading cause of death for Americans since 1900. Sudden cardiac
Statistics Cardiovascular Emergencies time is myocardium! Cardiovascular disease (CVD) claimed over 1 million lives in 2004. CVD has been the leading cause of death for Americans since 1900. Sudden cardiac
Non Cardiac Chest Pain or Angina like Chest Pain. Wafaa El-Aroussy, MD Prof of Cardiovascular Medicine Cardiology Department Cairo University
 Non Cardiac Chest Pain or Angina like Chest Pain By Wafaa El-Aroussy, MD Prof of Cardiovascular Medicine Cardiology Department Cairo University Prevalence of CP 7-11 % in primary practice 25% in a life
Non Cardiac Chest Pain or Angina like Chest Pain By Wafaa El-Aroussy, MD Prof of Cardiovascular Medicine Cardiology Department Cairo University Prevalence of CP 7-11 % in primary practice 25% in a life
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Evaluation of Chest Pain in General Practice
 Evaluation of Chest Pain in General Practice Pages with reference to book, From 254 To 258 Sunita Dodani ( Department of Family Medicine, Aga Khan University Hospital, Karachi. ) Chest pain can be one
Evaluation of Chest Pain in General Practice Pages with reference to book, From 254 To 258 Sunita Dodani ( Department of Family Medicine, Aga Khan University Hospital, Karachi. ) Chest pain can be one
Pulmonary-Vascular Disease. Howard J. Sachs, MD.
 Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Cardiac Pathology & Rehabilitation
 Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Coronary Heart Disease. Raja Nursing Instructor RN, DCHN, Post RN. BSc.N
 Coronary Heart Disease Raja Nursing Instructor RN, DCHN, Post RN. BSc.N 31/03/2016 Objectives Define coronary heart disease (CHD). Identify the causes and risk factors of CHD Discuss the pathophysiological
Coronary Heart Disease Raja Nursing Instructor RN, DCHN, Post RN. BSc.N 31/03/2016 Objectives Define coronary heart disease (CHD). Identify the causes and risk factors of CHD Discuss the pathophysiological
It is what you will see most in practice and what you need to know thoroughly.
 Acute Myocardial Infarction: Pre-hospital Issues 2 CEUs By: Michelle E. Duffelmeyer, MD INTRODUCTION An in depth review of the pathophysiology, symptomatology, and treatment modalities for acute MI. It
Acute Myocardial Infarction: Pre-hospital Issues 2 CEUs By: Michelle E. Duffelmeyer, MD INTRODUCTION An in depth review of the pathophysiology, symptomatology, and treatment modalities for acute MI. It
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS:
 PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS:") 1 NAME: DATE OF BIRTH PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS: PAST MEDICAL HISTORY (YOUR MEDICAL HISTORY) :
1 NAME: DATE OF BIRTH PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS: PAST MEDICAL HISTORY (YOUR MEDICAL HISTORY) :
Coronary Artery Disease. Overview. Gary Ferenchick, MD. How Does CAD Present? Stable CAD Unstable CAD Angina MI
 Coronary Artery Disease Gary Ferenchick, MD Presentation given at the E. Lansing Campus February 14, 2003 Overview Stable CAD Unstable CAD Angina MI Pathophysiology Clinical Features Hx/PE Differential
Coronary Artery Disease Gary Ferenchick, MD Presentation given at the E. Lansing Campus February 14, 2003 Overview Stable CAD Unstable CAD Angina MI Pathophysiology Clinical Features Hx/PE Differential
Case Question. Evaluation of Chest pain in the Office and Cardiac Stress Testing
 Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
CAN T MISS ECG FINDINGS L. THOMAS RICHARDS, MD ASSISTANT PROFESSOR OF EMERGENCY MEDICINE
 Topics in Emergency Medicine 2010 CAN T MISS ECG FINDINGS L. THOMAS RICHARDS, MD ASSISTANT PROFESSOR OF EMERGENCY MEDICINE OBJECTIVES Examine three common presentations to the ED which compel the EM provider
Topics in Emergency Medicine 2010 CAN T MISS ECG FINDINGS L. THOMAS RICHARDS, MD ASSISTANT PROFESSOR OF EMERGENCY MEDICINE OBJECTIVES Examine three common presentations to the ED which compel the EM provider
The focus of this week s lab will be pathology of the cardiovascular system.
 LAB 3: THE MUSCLE AND CARDIOVASCULAR SYSTEM The focus of this week s lab will be pathology of the cardiovascular system. The cases we will cover are: A. Atherosclerosis Refer to virtual slide p_8, should
LAB 3: THE MUSCLE AND CARDIOVASCULAR SYSTEM The focus of this week s lab will be pathology of the cardiovascular system. The cases we will cover are: A. Atherosclerosis Refer to virtual slide p_8, should
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Rural STEMI System of Care Success. Nicole Huber, PA-C Cumberland Healthcare Emergency Department
 Rural STEMI System of Care Success Nicole Huber, PA-C Cumberland Healthcare Emergency Department DISCLOSURES I HAVE NO ACTUAL OR POTENTIAL CONFLICT OF INTEREST IN RELATION TO THIS PRESENTATION Ideal Process
Rural STEMI System of Care Success Nicole Huber, PA-C Cumberland Healthcare Emergency Department DISCLOSURES I HAVE NO ACTUAL OR POTENTIAL CONFLICT OF INTEREST IN RELATION TO THIS PRESENTATION Ideal Process
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Heart Disease. Signs and Symptoms
 Heart Disease The term "heart disease" refers to several types of heart conditions. The most common type is coronary artery disease, which can cause heart attack, angina, heart failure, and arrhythmias.
Heart Disease The term "heart disease" refers to several types of heart conditions. The most common type is coronary artery disease, which can cause heart attack, angina, heart failure, and arrhythmias.
Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria
 Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria Patient Status: Understanding Inpatient and Outpatient Observation Focusing on Chest Pain, TIAs, Syncope and Dizziness Which
Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria Patient Status: Understanding Inpatient and Outpatient Observation Focusing on Chest Pain, TIAs, Syncope and Dizziness Which
STS: Circulatory/Pulmonary
 STS: Circulatory/Pulmonary September 27, 2017 You have a 50 y/o male who is complaining of excruciating pain in his chest. You find him sitting down on a bench, arms in a tripod position, breathing heavily.
STS: Circulatory/Pulmonary September 27, 2017 You have a 50 y/o male who is complaining of excruciating pain in his chest. You find him sitting down on a bench, arms in a tripod position, breathing heavily.
Can be felt where an artery passes near the skin surface and over a
 1 Chapter 14 Cardiovascular Emergencies 2 Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD) claimed
1 Chapter 14 Cardiovascular Emergencies 2 Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD) claimed
The Heart of the Matter
 The Heart of the Matter Is the Heart the Matter? --Chest pain in the Pediatric Patient-- 19th Interregional Symposium November 2, 2018 Session A, 9:35-10:50 am John-Charles Loo, MD Pediatric Cardiology,
The Heart of the Matter Is the Heart the Matter? --Chest pain in the Pediatric Patient-- 19th Interregional Symposium November 2, 2018 Session A, 9:35-10:50 am John-Charles Loo, MD Pediatric Cardiology,
Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since.
 1 2 3 4 5 Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD)
1 2 3 4 5 Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD)
Cardiac Emergencies. Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington
 Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
The Gender Divide Women, Men and Heart Disease February 2017
 The Gender Divide Women, Men and Heart Disease February 2017 Nandita S. Scott, MD FACC Co-Director MGH Heart Center Corrigan Women s Heart Health Program Massachusetts General Hospital Heart Disease For
The Gender Divide Women, Men and Heart Disease February 2017 Nandita S. Scott, MD FACC Co-Director MGH Heart Center Corrigan Women s Heart Health Program Massachusetts General Hospital Heart Disease For
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Contra-indications, Risks, and Safety Precautions for Stress Testing. ACSM guidelines, pg 20 7 ACSM RISK FACTORS. Risk Classifications pg 27
 Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Cardiovascular Emergencies
 Cardiovascular Emergencies Emergency Medical Services Seattle/King County Public Health 401 5th Avenue, Suite 1200 Seattle, WA 98104 206.296.4863 2015 Last Updated January 2, 2015 Contents INTRODUCTION...
Cardiovascular Emergencies Emergency Medical Services Seattle/King County Public Health 401 5th Avenue, Suite 1200 Seattle, WA 98104 206.296.4863 2015 Last Updated January 2, 2015 Contents INTRODUCTION...
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating)
") Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Ambulatory Care Conference
 Ambulatory Care Conference David Stultz, MD August 28, 2002 Case Presentation 50 year old white female presents to ED with substernal chest pain. Pain started while driving, is left substernal in location
Ambulatory Care Conference David Stultz, MD August 28, 2002 Case Presentation 50 year old white female presents to ED with substernal chest pain. Pain started while driving, is left substernal in location
Cardiovascular Disease
 Cardiovascular Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars on the 3 rd Wednesday of each month to address topics related to risk adjustment
Cardiovascular Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars on the 3 rd Wednesday of each month to address topics related to risk adjustment
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Interviewing and Health History
 Interviewing and Health History Core Curriculum for CV Clinicians Heart House 2016 Jane A. Linderbaum MS, ARNP, AACC Assistant Professor or Medicine, Mayo Clinic, Associate Medical Editor, AskMayoExpert
Interviewing and Health History Core Curriculum for CV Clinicians Heart House 2016 Jane A. Linderbaum MS, ARNP, AACC Assistant Professor or Medicine, Mayo Clinic, Associate Medical Editor, AskMayoExpert
WE ARE STEMI HUNTERS. LearningObjectives. I have no relevant disclosures. Myth: Jennifer Carlquist PA-C, ER CAQ
 WE ARE STEMI HUNTERS Jennifer Carlquist PA-C, ER CAQ Salinas Valley Memorial, ER Central Coast Cardiology, Specializing in EP LearningObjectives How to use pattern recognition to detect ischemia Triage
WE ARE STEMI HUNTERS Jennifer Carlquist PA-C, ER CAQ Salinas Valley Memorial, ER Central Coast Cardiology, Specializing in EP LearningObjectives How to use pattern recognition to detect ischemia Triage
Acute Coronary Syndrome including STEMI
 Portage County EMS Patient Care Guidelines Acute Coronary Syndrome including STEMI Note: The goal is to deliver a STEMI patient to a cardiac center within 60 minutes of first ALS patient contact. Cardiac
Portage County EMS Patient Care Guidelines Acute Coronary Syndrome including STEMI Note: The goal is to deliver a STEMI patient to a cardiac center within 60 minutes of first ALS patient contact. Cardiac
Jeffrey Tabas, MD. sf g h. Risk Assessment Do we understand risk stratification? Are we limiting radiation /contrast with the PERC rule and D-Dimers?
 Pulmonary Embolism Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital Disclosure No Financial Relationships to Disclose No significant investments
Pulmonary Embolism Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital Disclosure No Financial Relationships to Disclose No significant investments
Cardiac Emergencies. A Review of Cardiac Compromise. Lawrence L. Lambert
 Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Risk Assessment in the Preoperative period
 Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Valve Disease Board Review Questions
 Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
YOUR GUIDE TO. Understanding Your Angina Diagnosis and Treatment
 YOUR GUIDE TO Understanding Your Angina Diagnosis and Treatment Our goal at the Mercy Health Heart Institute is to help you be well. Our experienced team includes cardiologists, cardiovascular surgeons,
YOUR GUIDE TO Understanding Your Angina Diagnosis and Treatment Our goal at the Mercy Health Heart Institute is to help you be well. Our experienced team includes cardiologists, cardiovascular surgeons,
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
ACUTE CORONARY SYNDROME
 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
Name: (Last) (First) (M.I.) Date: / / Address: City: State: Zip: Home Phone: / / Cell Phone: / / Work Phone: / /
 (First) (M.I.) Date: / / Address: City: State: Zip: Home Phone: / / Cell Phone: / / Work Phone: / /") Name: (Last) (First) (M.I.) Date: / / Address: City: State: Zip: Home Phone: / / Cell Phone: / / Work Phone: / / Email Address: Do not have email Do not wish to provide Date of Birth: / / Gender: Male
Name: (Last) (First) (M.I.) Date: / / Address: City: State: Zip: Home Phone: / / Cell Phone: / / Work Phone: / / Email Address: Do not have email Do not wish to provide Date of Birth: / / Gender: Male
Cardiomyopathy Consequences. function of the myocardium for any reason. This is a serious disease in which the heart muscle
 Becki Simmons Cardiomyopathy Consequences Cardiomyopathy, which literally means "heart muscle disease," is the deterioration of the function of the myocardium for any reason. This is a serious disease
Becki Simmons Cardiomyopathy Consequences Cardiomyopathy, which literally means "heart muscle disease," is the deterioration of the function of the myocardium for any reason. This is a serious disease
Susan P. D Anna MSN, APRN BC February 14, 2019
 Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Cardiology. the Sounds: #7 HCM. LV Outflow Obstruction: Aortic Stenosis. (Coming Soon - HCM)
") A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
That unprotected LM: To STENT or NOT to STENT. Vasilios Papademetriou, MD Professor of Medicine Georgetown University
 That unprotected LM: To STENT or NOT to STENT Vasilios Papademetriou, MD Professor of Medicine Georgetown University Vasilios Papademetriou, MD I have no relevant financial relationships Patients are complicated
That unprotected LM: To STENT or NOT to STENT Vasilios Papademetriou, MD Professor of Medicine Georgetown University Vasilios Papademetriou, MD I have no relevant financial relationships Patients are complicated
NOT ANOTHER TALK ABOUT A - FIB
 NOT ANOTHER TALK ABOUT A - FIB CASES KUDOS AND A CHALLENGE Case 1 67 y/o female s/p R mastectomy 3 months earlier Second course of adjuvant chemotherapy Muga scan E.F. 35% What do we do next? Case 1 Cardiology
NOT ANOTHER TALK ABOUT A - FIB CASES KUDOS AND A CHALLENGE Case 1 67 y/o female s/p R mastectomy 3 months earlier Second course of adjuvant chemotherapy Muga scan E.F. 35% What do we do next? Case 1 Cardiology
SAUDI FELLOWSHIP TRAINING PROGRAM. Adult Cardiology. Final Written Examination 2019
 SAUDI FELLOWSHIP TRAINING PROGRAM Adult Cardiology Final Written Examination 2019 Objectives 1. Determine the trainee has sufficient competency related to the required specialty. 2. Determine the eligibility
SAUDI FELLOWSHIP TRAINING PROGRAM Adult Cardiology Final Written Examination 2019 Objectives 1. Determine the trainee has sufficient competency related to the required specialty. 2. Determine the eligibility
Detection Of Heart. By Dr Gary Mo
 Detection Of Heart Disease By Dr Gary Mo Types Of Heart Disease A. Coronary Heart Disease B. Valvular Heart Disease C. Cardiac Arrhythmia ( Rhythm disturbance ) D. Heart Blocks ( Conduction Abnormalities
Detection Of Heart Disease By Dr Gary Mo Types Of Heart Disease A. Coronary Heart Disease B. Valvular Heart Disease C. Cardiac Arrhythmia ( Rhythm disturbance ) D. Heart Blocks ( Conduction Abnormalities
Chest Pain Accreditation ACS Education
 Chest Pain Accreditation ACS Education Objectives Recognize the Typical and Atypical Signs and Symptoms of ACS Recognize Gender and Age Differences of ACS Recognize the Risk Factors of ACS Understand Early
Chest Pain Accreditation ACS Education Objectives Recognize the Typical and Atypical Signs and Symptoms of ACS Recognize Gender and Age Differences of ACS Recognize the Risk Factors of ACS Understand Early
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Cardiology Cath Conference
 Cardiology Cath Conference David Stultz, MD Cardiology Fellow, PGY-6 February 14, 2006 Case #1 84 yo WM brought by squad this am for? syncope Pt reports Chest pain stuttering over several days. This am
Cardiology Cath Conference David Stultz, MD Cardiology Fellow, PGY-6 February 14, 2006 Case #1 84 yo WM brought by squad this am for? syncope Pt reports Chest pain stuttering over several days. This am
Understanding Inpatient and Outpatient Observation Status Determination. Focusing on Chest Pain, TIAs, Syncope and Dizziness
 Understanding Inpatient and Outpatient Observation Status Determination Focusing on Chest Pain, TIAs, Syncope and Dizziness Medicare Compliance Inpatient Admissions & Outpatient Observation Monitoring
Understanding Inpatient and Outpatient Observation Status Determination Focusing on Chest Pain, TIAs, Syncope and Dizziness Medicare Compliance Inpatient Admissions & Outpatient Observation Monitoring
Cardiovascular Diseases and Diabetes
 Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
Symptoms of Cardiovascular Disorders
 Symptoms of Cardiovascular Disorders Chest Pain http://www.beltina.org/pics/chest_pain.jpg Chest pain is a very common complaint. Many patients are well aware that it is a warning of potential life-threatening
Symptoms of Cardiovascular Disorders Chest Pain http://www.beltina.org/pics/chest_pain.jpg Chest pain is a very common complaint. Many patients are well aware that it is a warning of potential life-threatening
The NICE chest pain guideline 1 year on. Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The NICE chest pain guideline 1 year on Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust The Society for Acute Medicine, 5 th International Conference,
The NICE chest pain guideline 1 year on Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust The Society for Acute Medicine, 5 th International Conference,
Rapid access chest pain clinic (RACPC)
") Rapid access chest pain clinic (RACPC) Context Coronary heart disease (CHD) remains the common cause of death and premture death in the UK with 15% of men and 7% of women dying from the disease. UK death
Rapid access chest pain clinic (RACPC) Context Coronary heart disease (CHD) remains the common cause of death and premture death in the UK with 15% of men and 7% of women dying from the disease. UK death
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Our Million Dollar Man
 Our Million Dollar Man Paul Myers = $25M LGH Foundation = $75M Province/VCH = $100M Total Project Cost = $200M Paul Myers Acute Care Tower New Medical & Surgical Centre Single Patient Rooms New State-of-the-Art
Our Million Dollar Man Paul Myers = $25M LGH Foundation = $75M Province/VCH = $100M Total Project Cost = $200M Paul Myers Acute Care Tower New Medical & Surgical Centre Single Patient Rooms New State-of-the-Art