2018 Early Management of Acute Ischemic Stroke Guidelines Update
|
|
|
- Norah Goodwin
- 5 years ago
- Views:
Transcription
1 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital systems that ensure timely management of acute strokes Identify patients eligible for IV alteplase therapy and design an appropriate dosing strategy for a given patient Describe the role of antiplatelet and anticoagulation therapy to prevent early recurrence of stroke, and select an appropriate antiplatelet for a given patient Prevent complications in stroke patients by selecting appropriate blood pressure and blood glucose goals in the acute and initial post-stroke period 1
2 Technician Objectives Identify stroke symptoms and determine the appropriate action for someone in the community who you suspect may be having a stroke Explain why timely administration of IV alteplase is important for eligible patients Describe contraindications to IV alteplase therapy for acute stroke patients Discuss the pharmacologic options for providing supportive care to acute stroke patients with hypertension Stroke Background >795,000 Americans have a stroke each year ~140,000 Americans die from a stroke annually 1/20 deaths is due to stroke Stroke is a leading cause of long-term disability ~87% of strokes are ischemic strokes HTN, high cholesterol, smoking, obesity and diabetes are leading causes of stroke 2

3 Primary Topics Covered Systems of care Acute reperfusion therapy In-hospital supportive care In-hospital initiation of secondary prevention 3
4 Systems of Care Your 74 year old grandmother suddenly started slurring her speech and developed weakness in her left arm. You live less than 10-minutes from an emergency room, so drive you her there immediately and call ahead. Was this an optimal response? 4

5 93% of people recognize sudden one-sided numbness as a stroke symptom Only 38% know all major symptoms, and to call 911 if someone is having a stroke Time is Brain 5


6 Hospital Stroke Teams The primary door-to-needle goal should be 60-minutes for > 50% of patients treated with IV alteplase It may be reasonable to establish a secondary door-to-needle time of 45 minutes It is recommended to designate an acute stroke team to provide clinical assessment of stroke patients Physicians, nurses, and laboratory/radiology personnel Protocols should be developed to ensure adherence to guidelines and current standards of care Participation is a stroke data repository is recommended Initial Evaluation It is recommended to use a stroke severity scale, preferably the NIHSS Lyden et al. Stroke 1994;25:
7 Pharmacist Participation in Stroke Care Associated with Improved Door-to-Needle Times Rech et al ED or inpatient stroke codes Pharmacist presence associated with a median DTN of 48 vs. 73 minutes (p<0.01) DTN <60 minutes in 71% vs. 29% of patients (p<0.01) Gosser et al ED strokes Median DTN shorter when pharmacist present: 69.5 vs minutes(p<0.01) More strokes meeting DTN <60 minutes: 29.9% vs.15.8% of patients (p<0.01) Rech et al. Ann Pharmacother 2017;51(12) Gosser et al. J Emerg Med 2016;50(1):87-93 Initial Evaluation All patients with suspected stroke should receive brain imaging on arrival Non-contrast CT in most cases Within 20 minutes of arrival in 50% of tpa or thrombectomy candidates Only blood glucose assessment should precede the initiation of IV alteplase Hematologic and coagulation studies may be required in some patients only if there is suspicion for an abnormality Baseline EKG and troponin levels are recommended, but should not delay the administration of IV alteplase 7
 C.")
8 Which of the following patients has an absolute exclusion to tpa therapy? A. An 86 year old male that present 3.5 hours from symptom onset B. A 52 year old female that had right-sided facial droop and difficulty speaking when she woke up this morning (45 minutes ago) C. A 69 year old male with 1 prior stroke 3 years ago, whose symptoms are improving on presentation D. A 48 year old female who takes warfarin for atrial fibrillation, with an INR of 1.6 on presentation IV Alteplase (tpa) for Acute Stroke In a 2014 meta-analysis, more patients that received tpa had a good outcome 33% vs. 23% within 3 hours 35% vs. 30% from 3 to 4.5 hours In a registry of 58,000 patients, each 15-minute reduction in time to tpa associated with: 4% increase in odds of walking at discharge 4% decrease in odds of death prior to discharge Intracerebral hemorrhage in 5%-7% of patients in clinical trials Emberson et al. Lancet 2014;384(9958):1929 Saver et al. JAMA 2013;309(23):
9 tpa Recommendations tpa is recommended for selected patients who may be treated within 3-hours of stroke-symptom onset tpa is also recommended for selected patients who may be treated within 4.5-hours of stroke-symptom onset tpa dosing: 0.9 mg/kg, max dose of 90 mg 10% given as a bolus over 1 minute Remaining given over 60 minutes tpa candidates Contraindications: Time of onset > 3 or 4.5 hours Acute intracranial hemorrhage Ischemic stroke, head trauma, intracranial/spinal surgery within 3 months History of intracranial hemorrhage Subarachnoid hemorrhage BP >185/110 GI/genitourinary bleed within 21 days Coagulopathy (INR > 1.7, platelets <100,000) Treatment-dose LMWH w/in 24 hours or DOAC use within 48 hours Glucose <50mg/dL Non-compressible arterial puncture within 7 days 9
10 tpa candidates Relative contraindications Minor deficits nondisabling Seizure at onset MI within last 3 months Consider initial tpa for concurrent MI Pregnancy Stroke Mimics No longer listed Age < 18 Glucose >400 Improving symptoms tpa candidates: 3- to 4.5- hour interval It may be reasonable to give tpa to those with: Age >80 On warfarin with INR < 1.7 History of stroke and diabetes The benefit of tpa is uncertain in patients with very severe stroke symptoms (NIHSS score >25) 10
11 Which of the following patients has an absolute exclusion to tpa therapy? A. An 86 year old male that present 3.5 hours from symptom onset B. A 52 year old female that had right-sided facial droop and difficulty speaking when she woke up this morning (45 minutes ago) C. A 69 year old male with 1 prior stroke 3 years ago, whose symptoms are improving on presentation D. A 48 year old female who takes warfarin for atrial fibrillation, with an INR of 1.6 on presentation Options to treat hypertension in patients who are candidates for tpa BP > 185/110 mmhg, but otherwise tpa candidates Labetalol 10-20mg IV, may repeat x1 Nicardipine 5mg/hour, titrate every 5-15 mins to max of 15mg/hour Maintain BP <180/105 mmhg during and after tpa therapy Monitor BP every 15 minutes for 2 hours, then every 30 min for 6 hours, then hourly If SBP > mmhg or DBP > mmhg Labetalol 10mg IV followed by continuous infusion Nicardipine continuous infusion If BP not controlled Consider IV sodium nitroprusside *Other agents may be considered based on comrobities, etc. 11
 Dependent on location of the causative occlusion Patients eligible for IV alteplase should receive IV alteplase even if EVTs are")
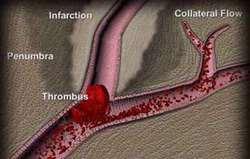
12 Mechanical Thrombectomy Patients should receive mechanical thrombectomy if they meet the following criteria: Pre-stroke mrs of 0-1 > 18 years of age NIHSS score > 6 Can be initiated within 6 hours of symptom onset (may be reasonable in up to 24 hours in select patients) Dependent on location of the causative occlusion Patients eligible for IV alteplase should receive IV alteplase even if EVTs are being considered Mechanical Thrombectomy 12
13 Antiplatelet Therapy Administration of aspirin is recommended within 24 to 48 hours of onset Delay until 24 hours in patients treated with tpa mg Treatment for 21 days with dual antiplatelet therapy can be beneficial for early secondary stroke prevention for a period of up to 90 days of symptom onset Aspirin and clopidogrel Begun within 24 hours CHANCE Trial Clopidogrel in High Risk Patients with Acute Nondisabling Cerebrovascular Events Clopidogrel + aspirin for 21 days, then clopidogrel to 90 days Less recurrent stroke at 90 days with dual antiplatelet therapy HR: 0.68, p<0.001 Durable treatment effect at 1-year Wang et al. NEJM 2013;369:
14 Anticoagulants Urgent anticoagulation with the goal of preventing early recurrence, preventing worsening of neuro symptoms or improving outcomes is not recommended for patients with acute stroke General Support 14
15 A 57-year old female presents to the ED for an acute stroke with a blood pressure of 196/102 mmhg, but is otherwise a candidate for tpa. What is the best course of action? A. Do not give tpa B. Start a nifedipine continuous infusion. You can start the tpa once her BP is <140/90 mmhg C. Start a nifedipine continuous infusion. You can start the tpa once her BP is <180/105 mmhg D. Start a nifedipine continuous infusion. You can stat the tpa once her BP is <185/110 mmhg A 57-year old female with uncontrolled hypertension presents to the ED for acute ischemic stroke with a blood pressure of 196/102 mmhg. She is outside the window for tpa use, but her neurologic symptoms seem to still be unstable. What is the best course of action? A. Start a nifedipine continuous infusion titrated to <140/90 mmhg to prevent neurologic worsening B. Start a nifedipine continuous infusion titrated to <180/105 mmhg to prevent neurologic worsening C. Start a nifedipine continuous infusion and titrate to a goal reduction of 15% in SBP to prevent neurologic worsening D. There is no need to address her blood pressure at this time 15
16 Blood Pressure Early treatment of hypertension is indicated when required by comorbid conditions. Acute coronary event, acute heart failure, aortic dissection, post-thrombolysis ICH, preeclampsia/eclampsia Lower by 15% initially If BP <220/120 mmhg and tpa not given, lowering BP does not help prevent death or dependency If BP >220/120 mmhg and tpa not given, lowering BP by 15% in the 1 st 24 hours is reasonable Reasonable to start/restart antihypertensives in patients with BP > 140/90 mmhg who are neurologically stable Blood Glucose It is reasonable to treat hyperglycemia to achieve a blood glucose in the range of mg/dl Persistent in-hospital hyperglycemia during 1 st 24 hours is associated with worse outcomes Hypoglycemia (<60 mg/dl) should be treated 16
17 Deep Vein Thrombosis (DVT) Prophylaxis Intermittent pneumatic compression is recommended in immobile stroke patients (in addition to aspirin) The benefit of pharmacologic DVT prophylaxis with subcutaneous heparin or LMWH is not established If given, drug choice is uncertain Seizures Recurrent seizures after stroke should be treated similarly as when they occur otherwise. Anti-seizure drugs should be based on patient characteristics Prophylactic use of anti-seizure drugs is not recommended 17
18 In-Hospital Initiation of Secondary Prevention Evaluation Brain imaging Routine use of MRI is not cost-effective, and not recommended for initial diagnosis or to plan subsequent treatment Vascular imaging Candidates for CEA or stenting should have noninvasive imaging of the cervical vessels within 24 hours of admission Cardiac Evaluation Cardiac monitoring is recommended to screen for atrial fibrillation/other serious arrhythmias that require intervention for at least initial 24 hours The benefit of prolonged monitoring is uncertain 18
19 Screening for Secondary Prevention Glucose: It is reasonable to screen all patients for diabetes mellitus COR IIA, LOE C-EO Cholesterol Routine measurement of lipids in all patients not taking a high-intensity statin is not recommended (COR: no benefit; LOE: B-R) Measurement of lipids may be reasonable in patients on an optimized statin regimen may be useful in identifying patients who would be candidates for a PCSK9 inhibitors (COR: IIb; LOE: B-R) Other Testing Routine screening for hyperhomocysteinemia is not indicated There is unknown utility of screening for thrombophilic states Anticoagulation may be considered in patients with abnormal findings on coagulation testing after an ischemic stroke depending on the clinical circumstances Routine testing for antiphospholipid antibodies is not recommended 19
20 It is reasonable to switch a patient who developed an ischemic stroke on 162mg of aspirin daily to warfarin to prevent further strokes A. True B. False Antithrombotic Treatment Antiplatelet agents recommended over oral anticoagulation for noncardioembolic stroke In patients with noncardioembolic stroke while on aspirin, the benefit of increasing the dose or switching to an alternative antiplatelet is not well established In patients with noncardioembolic stroke while on antiplatelet therapy, switching to warfarin is not beneficial for secondary prevention For most patients with stroke in the setting of atrial fibrillation, it is reasonable to initiate oral anticoagulation within 4-14 days after symptom onset 20
21 Antithrombotic Treatment For patients with ischemic stroke, atrial fibrillation and coronary artery disease Utility of adding antiplatelet to anticoagulation is uncertain May be warranted in unstable angina or coronary artery stenting In patients with hemorrhagic transformation, initiation/continuation of antiplatelet or anticoagulant therapy dependent on the clinical scenario In patients with stroke and extracranial carotid or vertebral arterial dissection, antiplatelet or anticoagulant therapy for 3 to 6 months may be reasonable Statins It is reasonable to initiate/continue statin therapy during the acute period High-intensity statin therapy should be initiated/continued as 1 st line therapy in patients with clinical ASCVD< 75 years of age In patients >75 years of age, it is reasonable to weigh risks vs. benefits 21

22 Questions? 22
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care
 Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Advanced Stroke Care in the context of the Cardiovascular Patient
 EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Diagnosis: Allergies with reaction type:
 Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD. Virginia Mason Medical Center March 16, 2018
 Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
When Not To Give TPA Steve Phillips Division of Neurology
 When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Recent Changes in IV TPA Recommendations. Ashish Masih, M.D Vascular Neurology
 Recent Changes in IV TPA Recommendations Ashish Masih, M.D Vascular Neurology Disclosures none 4 th leading cause of death Nearly 800,000 cases of stroke annually Statistics Leading cause of disability
Recent Changes in IV TPA Recommendations Ashish Masih, M.D Vascular Neurology Disclosures none 4 th leading cause of death Nearly 800,000 cases of stroke annually Statistics Leading cause of disability
Preoperative Management of Patients Receiving Antithrombotics
 Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Stroke Quality Measures. Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012
 1 Stroke Quality Measures Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012 2 Application of the Stroke Measure Set The stroke
1 Stroke Quality Measures Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012 2 Application of the Stroke Measure Set The stroke
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ST Elevated Myocardial Infarction- Latest AHA recommendations
 ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial
 Trial") The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
Objectives. Treatment of ACS. Early Invasive Strategy. UA/NSTEMI General Concepts. UA/NSTEMI Initial Therapy/Antithrombotic
 Objectives Treatment of ACS Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Define early invasive strategy and what patients typically receive this approach Compare/contrast the medications
Objectives Treatment of ACS Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Define early invasive strategy and what patients typically receive this approach Compare/contrast the medications
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Page 1 of 7. Intraparenchymal hemorrhage or subarachnoid hemorrhage. Consult neurosurgery
 Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Types of Stroke and Risk Factors There are two types of stroke, both of which result in a reduction in oxygen reaching the brain.
 Assessment and Management of Stroke Stroke is the fifth leading cause of death, as well as the leading cause of disability for Americans (Davis & Lockhart, 2016). Early evaluation and treatment of stroke
Assessment and Management of Stroke Stroke is the fifth leading cause of death, as well as the leading cause of disability for Americans (Davis & Lockhart, 2016). Early evaluation and treatment of stroke
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Subject Expert. Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO
 Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Table 1. Specific changes to the FDA labeling for recombinant tissue plasminogen activator (Alteplase, Activase, Genentech, inc).
.") Acute Ischemic Stroke Controversies Steven R. Messé, MD, FAAN Associate professor of Neurology, Pereleman School of Medicine at the University of Pennsylvania, Philadelphia, PA Using the term controversy
Acute Ischemic Stroke Controversies Steven R. Messé, MD, FAAN Associate professor of Neurology, Pereleman School of Medicine at the University of Pennsylvania, Philadelphia, PA Using the term controversy
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Long-Term Care Updates
 Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
WHAT IS A STROKE? What causes a stroke? What disabilities can result from a stroke?
 Know Stroke Stroke is the third leading cause of death in the United States and a leading cause of serious, long-term disability in adults. About 600,000 new strokes are reported in the U.S. each year.
Know Stroke Stroke is the third leading cause of death in the United States and a leading cause of serious, long-term disability in adults. About 600,000 new strokes are reported in the U.S. each year.
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE
 Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH