ECMO AND SHORT-TERM SUPPORT:
|
|
|
- Ursula Lawrence
- 5 years ago
- Views:
Transcription

1 ECMO AND SHORT-TERM SUPPORT: UTILIZATION GUIDELINES AND IMPACT OF THE NEW HEART ALLOCATION SYSTEM Jeffrey Teuteberg Section Chief of Heart Failure, Cardiac Transplant and Mechanical Circulatory Support Stanford University
2 Disclosures: Medtronic/HeartWare (ad board, speaking), Abiomed (ad board, speaking), CareDx (ad board, speaking), Abbott/Thoratec (CEC) ECMO AND SHORT-TERM SUPPORT: UTILIZATION GUIDELINES AND IMPACT OF THE NEW HEART ALLOCATION SYSTEM Jeffrey Teuteberg Section Chief of Heart Failure, Cardiac Transplant and Mechanical Circulatory Support Stanford University
3 BACKGROUND Problems Too many candidates waiting as Status 1A (3x more likely to die on waiting list) Changing landscape of HF management LVAD usage Specific patient groups may be disenfranchised Inequities in access to organs because of artificial geographic boundaries Goals Reduce waiting list mortality Better stratify candidates based on medical urgency Expand access to donors for the most critically ill patients
4 PROPOSED NEW STATUSES: HIGH LEVEL Current Status 1A 1 Proposed Status 2 3 1B Proposed statuses 1-3 are generally defined by current status 1A criteria Proposed status 4 is generally defined by current status 1B criteria Proposed status 5-6 are generally defined by current status 2 criteria 4
5 STATUSES 1-3 Status Criteria ECMO Non-dischargeable (surgically implanted) non-endovascular BiVAD MCSD with life-threatening ventricular arrhythmia Non-dischargeable, surgically implanted, non-endovascular LVAD TAH BiVAD RVAD LVAD for single ventricle MCSD with device malfunction/mechanical failure Percutaneous endovascular MCS Intra-aortic balloon pump Ventricular tachycardia/ventricular fibrillation, mechanical support not required Dischargeable LVAD for up to 30 days Multiple inotropes or single high-dose inotropes with continuous hemodynamic monitoring MCSD with device infection MCSD with hemolysis MCSD with pump thrombosis MCSD with right heart failure MCSD with mucosal bleeding MCSD with aortic insufficiency 5
6 STATUSES 4-6 Status 4 Criteria Stable LVAD candidates not using 30 day discretionary period Inotropes without hemodynamic monitoring Diagnosis of congenital heart disease (CHD) Diagnosis of ischemic heart disease with intractable angina Diagnosis of hypertrophic cardiomyopathy Diagnosis of restrictive cardiomyopathy Diagnosis of amyloidosis Retransplant 5 Combined organ transplants 6 All remaining active candidates 6
7 % DEATH WITHIN 6 MONTHS A(i) =VAD for 30 days A(ii) = TAH A(iii) = IABP A(iv) = ECMO B(i) = Thromboembolism B(ii) = Device infection B(iii) = Device malfunction B(iv) = Life-threatening ventricular arrhythmia B(v) = Other device related complication Post-TX WL Status 2 Status 1B Status 1A-(E) Status 1A-(D) Status 1A-(C) Status 1A-(B) Status 1A-(A)(iii) Status 1A-(A) Status 1A-ALL ALL Status 2 Status 1B Status 1A-(E) Status 1A-(D) Status 1A-(C) Status 1A-(B) Status 1A-(B)(iv) Status 1A-(A)(ii) Status 1A-(A) Status 1A-ALL ALL Status 1A-(B)(iv) Status 1A-(A)(iii) Status 1A-(A)(iv) Status 1A-(A)(ii) TAH ECMO Status 1A-(A)(iv) 0% 5% 10% 15% 20% 25% 30% 35% * For WL analysis, time is computed from first entry into criteria/sub-criteria, rather than time since listing. ECMO Status 2 Status 1B Status 1A-(E) Status 1A-(D) Status 1A-(C) Status 1A-(B)(v) Status 1A-(B)(iv) Status 1A-(B)(iii) Status 1A-(B)(ii) Status 1A-(B)(i) Status 1A-(B) Status 1A-(A)(iv) Status 1A-(A)(iii) Status 1A-(A)(ii) Status 1A-(A)(i) Status 1A-(A) Status 1A-ALL ALL

8 PERCUTANEOUS VAD Death rate Transplant rate
9 THE WAITLIST MORTALITY Stable VAD Patients have a 180-Day Waitlist Mortality=6.4% J Am Coll Cardiol 2012;60:36-43
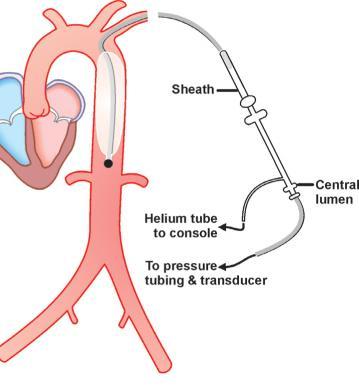
10 WHAT IS THE INDICATION? Indication Ongoing cardiogenic shock that occurs immediately (<48 hours) following acute myocardial infarction (AMI) or open heart surgery as a result of isolated left ventricular failure that is not responsive to optimal medical management and conventional treatment measures with or without an intra-aortic balloon pump Impella 2.5 & Impella CP <4 days Impella 5.0 & Impella LD <6 days Impella RP up to 14 days Leaving beyond 4, 6, or 14 days due to unforeseen circumstances is a clinical decision
11 ALL ABOUT INCENTIVES CARROT OR STICK?
12 HOW WOULD YOU APPROACH THIS PATIENT? 50 year old with NICM with progressive dyspnea despite optimal medical therapy and CRT-D. Hemodynamics RA 6 PA 53/22 (32) W 16 CO/CI 3.2/1.8 Potential management options: A. Follow closely in clinic B. Try to adjust HF medications as an outpatient C. Perform CPET D. Place RHC, start two low-dose inotropes, admit for months long hospitalization in CCU, but allow to ambulate around the unit.
13 HOW COMMON/HOW RISKY? Tier 1 Tier 2 ECMO Ventilator No d/c VAD VAD & VT IABP VT VAD dysfxn TAH R/BiVAD Tier 3 LVAD 30 1Ae RHC LVAD comp LVAD inf Days Tx Tx rate Deaths Death rate
14 IMPELLA pts, single-center 1/06-12/11 Shock CS: 32% Post-cardiotomy 68% Impella 5.0: 80% Lemaire et al. Ann Thorac Surg 2014;97:
15 SHOCK AND ACUTE SUPPORT Short-term VAD: 59% VA ECMO: 41% Impella 2.5 in 9pts LV vent in 1 pt Takayama et al. J Heart Lung Transplant 2013;32:

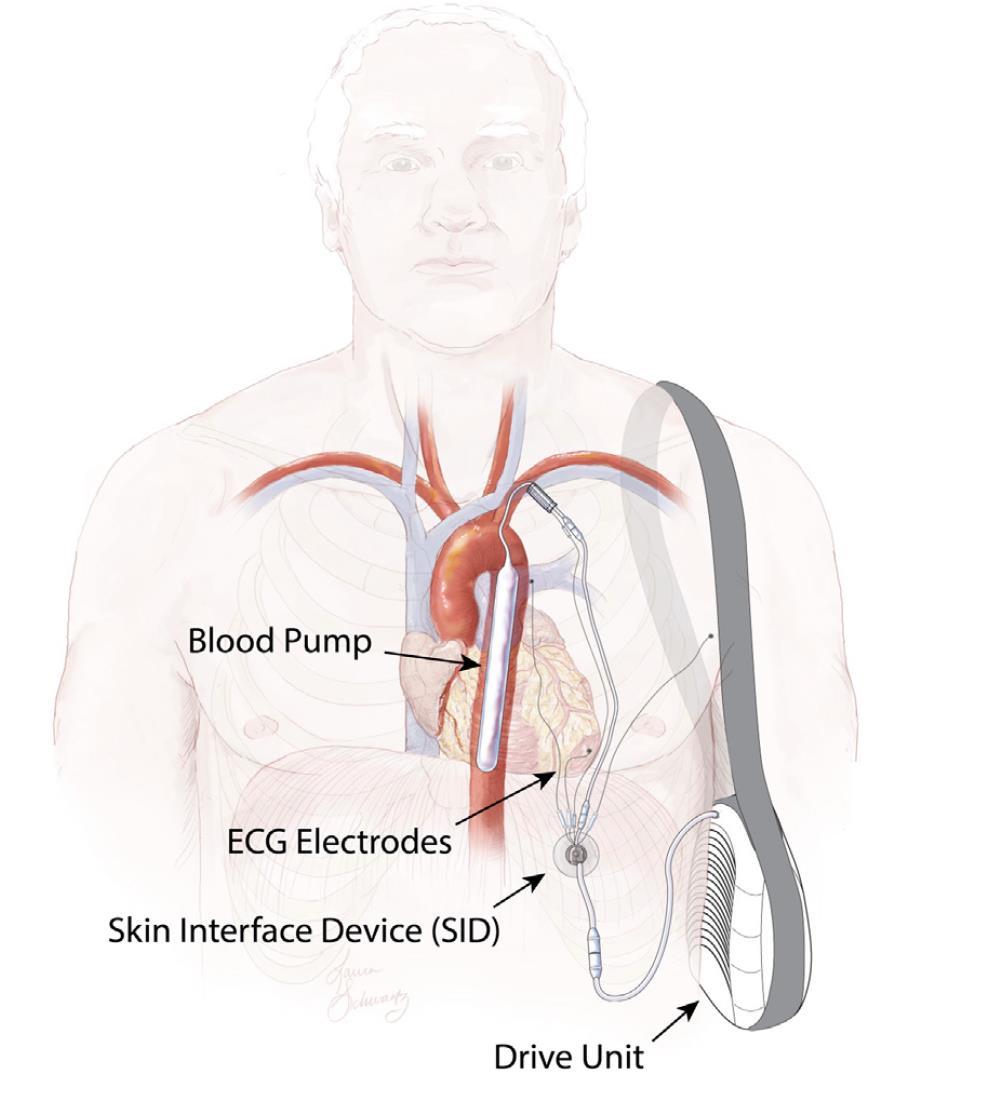
16 TECHNOLOGY IS MOVING QUICKLY
17 WE ARE ALREADY RESPONDING TO INCENTIVES Stevenson LW. J Heart Lung Transplant. 2013;32(9):861-7

18 WHO GETS THE HEARTS? Stevenson JAMA Int Med 2015;175: Dardas et al. J Heart Lung Transplant 2017;36:

19 IS IT THE SAME EVERYWHERE? Nguyen et al. J Heart Lung Transplant 2016;35:
20 HEMODYNAMIC CRITERIA ACS IMPLANTATION Within 7 days, all met in within one 24 hour period SBP < 90 mmhg Cardiac index < 1.8 L/min/m 2 without inotropes < 2.0 L/min/m 2 with inotropes Wedge >15 mmhg No hemos in 7 days, then at least one, within 24 hours prior to ECMO CPR was performed Systolic blood pressure < 70 mmhg Arterial lactate > 4 mmol/l AST or ALT >1,000 U/L
21 ACS WEANING ECMO Every 7 days, must have both 1. Demonstrated contraindication to durable MCS 2. Within 48 hours of status expiring, failed wean, at least one: 1. MAP < 60 mmhg 2. CI < 2.0 L/min/m 2 3. Wedge > 15 mmhg 4. SvO 2 < 50% measured by central venous catheter Surgical nondis VAD, Perc VAD, IABP Every 14 days, must have both 1. Demonstrated contraindication to durable MCS 2. Within 48 hours of status expiring, failed wean, at least one: 1. MAP < 60 mmhg 2. CI < 2.0 L/min/m 2 3. Wedge > 15 mmhg 4. SvO 2 < 50% measured by central venous catheter After 14 days if extension not granted or not requested, then status 3
22 HEMODYNAMIC CRITERIA STICK NOT CARROT? Dobutamine 7.6 mcg/kg/min Milrinone 0.54 mcg/kg/min Dobutamine 3.5 mcg/kg/min Milrinone 0.36 mcg/kg/min Dopamine 2.4 mcg/kg/min Parker et al. J Heart Lung Transplant 2017;36:
23 HEMODYNAMICS AND MORTALITY Parker et al. J Heart Lung Transplant 2017;36:

24 ANTICIPATING BEHAVIOR?
25 LANDSCAPE OF RISK 1A was originally intended for patients who had less than 7 days left to live without transplant, now waiting 6-12 months BTT one year mortality is 12%, about 12-14% risk of CVA, and up to 30% have been removed from waiting list at one year due to complications VAD complications (thrombus, RHF, infection, bleeding, AI) only makes you status 3 In toto is this better or worse than waiting on ambulatory ACS? Stevenson et al. J Heart Lung Transplant 2016;35:
26 THE LAST WORD The modeling for the proposed new system also reflects considerable expertise and thought based on current listing practice. However, it cannot overcome the fundamental reality that future listing behavior cannot be modeled based on previous listing behavior if the rules are changing. Lynne Stevenson Stevenson et al. J Heart Lung Transplant 2016;35:
27
28 NONDISCHARGEABLE VAD Defined non-dischargeable non-endovascular Must remain hospitalized because device is not FDA-approved for out of hospital use Duration: 14 days Extension if both: 1. Contraindication to durable MCS 2. Within 48 hours of status expiring, failed weaning by at least one: 1. MAP < 60 mmhg 2. CI < 2.0 L/min/m2 3. Wedge > 15 mmhg 4. SvO 2 < 50% measured by central venous catheter


29 CURRENT ALLOCATION Local: Status 1A, Status 1B Zone A: Status 1A, Status 1B Local: Status 2 Zone B: Status 1A, Status 1B Zone A: Status 2 Zone B: Status 2 Etc Zone C 1500 Miles Zone B 1000 Miles Zone A 500 Miles
30 PROPOSED BROADER SHARING SEQUENCE Candidate Status Status 1 adult + Status 1A ped Status 1 adult + Status 1A ped Status 2 adult Status 2 adult Status 3 adult + Status 1B ped Status 4 adult Status 3 adult + Status 1B ped Location DSA + Zone A Zone B DSA + Zone A Zone B DSA DSA Zone A 30
31
32 Should percutaneous temporary VAD patients receive higher priority? The panel agreed that there was insufficient data with the Impella device and other percutaneous VADs with regard to waitlist and post-transplant mortality. It was believed that there appears to be a trend towards higher waitlist mortality in this cohort than those on intra-aortic balloon pumps (IABP). However, opinion was mixed regarding whether percutaneous temporary VAD patients should be of higher priority. A panel member contended that temporary VAD patients priority level should depend on the reason for implantation. For those patients who are clinically stable and walking with a temporary VAD, it was argued that these patients should have lower priority over a bedbound patient who is clinically worse. Such a policy, it was agreed, would have to be carefully worded to avoid misinterpretation and gaming. Overall, it was felt by this panel member that temporary VAD patients should be prioritized highly, likely in Tier 2, below ECMO and ideally above IABP (however, it was acknowledged that as part of Tier 2, time on the waiting list would be the sole differentiator between IABP patients and temporary VAD patients). Another attendee argued that Impella and other temporary VADs were by nature short-term devices, and that when they inevitably fail, they cause the patient to be extremely ill. Therefore, temporary VADs should not be considered stable and should be accorded one of the highest priority levels, likely Tier 1. ECMO patients could therefore be bridged to a percutaneous VAD (thus preventing an extra sternotomy) without losing higher priority in this scenario. There was some agreement with this, but the point was raised that if a patient was doing well on a temporary VAD, the incentive to transplant them urgently is lower. Status 2: Acute Circulatory Support (ACS) Device The Committee reviewed data to support placing ACS candidates in status 2. The cohort used in the TSAMs includes candidates registered for a heart transplant between mid-2009 to mid This cohort pre-dates the rapid growth of heart candidates supported by ACS, so the Committee reviewed data regarding waiting list and post-transplant outcomes for candidates supported by ACS (defined as balloon pump, Impella, and CardiacAssist TandemHeart) between 2011 and During this period, about 11,000 heart-alone candidates were registered for transplant, and approximately 4% were registered with ACS at listing, most commonly with a balloon pump. For all ACS candidates combined, the death/too sick rate was 31 per 100 patient years, compared with 34 per 100 patient years for all status 1A candidates and 21 per 100 patient years for candidates on inotropes. At time of transplant, 6% of candidates were supported by an ACS device, and the vast majority of those candidates were supported by a balloon pump alone. The two-year post-transplant survival rates for candidates transplanted while supported by an ACS was 84%, midway between BiVADs (82%) and LVADs (86%). When the Committee initially designed the straw man, it placed candidates with balloon pumps in status 2 based on supporting data and clinical experience, because those candidates are not as urgent as candidates supported by ECMO. The Committee was similarly wary of assigning ACS candidates to status 1, because the death rate for Impella and TandemHeart is closer to those candidates with balloon pump, and they do not appear to be as urgent as those candidates on ECMO. Additionally, the Committee does not want to create an inadvertent incentive for transplant teams to treat with ACS in order to place their candidates in status 1. To further avoid creating an inadvertent incentive to treat with ACS, the Committee proposes a requirement that the candidate be treated with ACS specifically for cardiogenic shock, and created a hemodynamic threshold of showing the candidate had a cardiac index of less than or equal to 2.2 L/min/m 2 prior to ACS implantation. This cardiac index value was adopted based on the Centers for Medicare and Medicaid Services (CMS) threshold for coverage for administration of home inotropes. To be consistent throughout policy, each time the Committee proposed a hemodynamic requirement in addition to therapy, the Committee included the proposed threshold of a cardiac index less than or equal to 2.2 L/min/m 2. UNOS will maintain a list of qualifying ACS devices which will be reviewed annually by the Committee. The current list of ACS devices is included in Exhibit C. Status 2: Intra-aortic balloon pump (IABP) The Committee discussed whether candidates supported by IABP should be in status 2, and whether they should be in the same status as those candidates treated with TAH. Though the waiting list mortality and post-transplant survival rates for candidates supported by IABP are worse than for those candidates supported by TAH, clinical practice led Committee members to believe that these two candidate groups are reasonable in the same status, and that IABP candidates are comparable to candidates supported by ACS devices. Like the ACS device patients, for this status the Committee also proposes a requirement that the candidate be treated with IABP specifically for cardiogenic shock, and created a hemodynamic threshold of showing the candidate had a cardiac index of less than or equal to 2.2 L/min/m 2 prior to ACS implantation.
33 Decreased utilization in donor hearts is an issue Khush et al. Am J Transplant. 2015; 15:
34 Waitlist candidates added/organ transplants performed Heart transplants performed vs waitlist candidates added, USA Transplants Performed Waitlist Candidates Added Year From UNOS/SRTR data, available at
35 ECMO PRIORITY Will ECMO in highest priority incentivize increased use of ECMO? If so, will post-transplant outcomes be worse? Is there potential for outcomes to be better if ECMO patients are transplanted quicker? Assessment of net transplant benefit 35
ECMO as a Bridge to Heart Transplant in the Era of LVAD s.
 Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania ECMO as a Bridge to Heart Transplant in the Era of
Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania ECMO as a Bridge to Heart Transplant in the Era of
Meyer, D; et al. The Future Direction of the Adult Heart Allocation System in the United States. Am J Transplant 2015; Jan 15(1):
:") January Journal Watch 2015 Burhan Mohamedali, MD Rush University Chicago, Illinois, USA Burhan.mohamedali@gmail.com Rajeev Mohan, MD Scripps Clinic and Green Hospital La Jolla, California, USA Mohan.Rajeev@scrippshealth.org
January Journal Watch 2015 Burhan Mohamedali, MD Rush University Chicago, Illinois, USA Burhan.mohamedali@gmail.com Rajeev Mohan, MD Scripps Clinic and Green Hospital La Jolla, California, USA Mohan.Rajeev@scrippshealth.org
Thoracic Simulation Allocation Modeling (TSAM) of a 6-Tier Allocation Strategy for Heart Transplant
 of a 6-Tier Allocation Strategy for Heart Transplant") Thoracic Simulation Allocation Modeling (TSAM) of a 6-Tier Allocation Strategy for Heart Transplant Monica Colvin, Melissa Skeans, Liz Robbins, Leah Edwards, Jessica Zeglin, Scott Silvestry, Ryan Davies,
Thoracic Simulation Allocation Modeling (TSAM) of a 6-Tier Allocation Strategy for Heart Transplant Monica Colvin, Melissa Skeans, Liz Robbins, Leah Edwards, Jessica Zeglin, Scott Silvestry, Ryan Davies,
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Andrew Civitello MD, FACC
 Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
Mechanical Cardiac Support in Acute Heart Failure. Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research
 Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
เอกราช อร ยะช ยพาณ ชย
 30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
Cardiogenic Shock Protocol
 Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Ramani GV et al. Mayo Clin Proc 2010;85:180-95
 THERAPIES FOR ADVANCED HEART FAILURE: WHEN TO REFER Navin Rajagopalan, MD Assistant Professor of Medicine University of Kentucky Director, Congestive Heart Failure Medical Director of Cardiac Transplantation
THERAPIES FOR ADVANCED HEART FAILURE: WHEN TO REFER Navin Rajagopalan, MD Assistant Professor of Medicine University of Kentucky Director, Congestive Heart Failure Medical Director of Cardiac Transplantation
VENTRICULAR ASSIST DEVICES AND TOTAL ARTIFICIAL HEARTS
 Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-86 Effective Date: 03/26/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-86 Effective Date: 03/26/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Update on Mechanical Circulatory Support. AATS May 5, 2010 Toronto, ON Canada
 Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Right Ventricular Failure: Prediction, Prevention and Treatment
 Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Implantable Ventricular Assist Devices and Total Artificial Hearts. Policy Specific Section: June 13, 1997 March 29, 2013
 Medical Policy Implantable Ventricular Assist Devices and Total Artificial Hearts Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective
Medical Policy Implantable Ventricular Assist Devices and Total Artificial Hearts Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Echo assessment of patients with an ECMO device
 Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
The Future Direction of the Adult Heart Allocation System in the United States
 American Journal of Transplantation 2015; 15: 44 54 Wiley Periodicals Inc. Special Article C Copyright 2014 The American Society of Transplantation and the American Society of Transplant Surgeons doi:
American Journal of Transplantation 2015; 15: 44 54 Wiley Periodicals Inc. Special Article C Copyright 2014 The American Society of Transplantation and the American Society of Transplant Surgeons doi:
Counterpulsation. John N. Nanas, MD, PhD. Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece
 John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD
 A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
Policy Specific Section: May 16, 1984 April 9, 2014
 Medical Policy Heart Transplant Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Transplant Original Policy Date: Effective Date: May 16, 1984 April 9, 2014 Definitions
Medical Policy Heart Transplant Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Transplant Original Policy Date: Effective Date: May 16, 1984 April 9, 2014 Definitions
ECMO as a bridge to durable LVAD therapy. Jonathan Haft, MD Department of Cardiac Surgery University of Michigan
 ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
3/1/2017. Heart Failure is a major driver of morbidity and mortality in the US 1-7
 Approaches to Cardiogenic Shock Margarita Camacho MD, FACS Surgical Director Cardiac Transplant and Mechanical Assist Device Program RWJ/Barnabas Health Heart Centers at Newark Beth Israel Medical Center
Approaches to Cardiogenic Shock Margarita Camacho MD, FACS Surgical Director Cardiac Transplant and Mechanical Assist Device Program RWJ/Barnabas Health Heart Centers at Newark Beth Israel Medical Center
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Device Therapy for Heart Failure
 Device Therapy for Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics St Boniface General Hospital,
Device Therapy for Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics St Boniface General Hospital,
Understanding the Pediatric Ventricular Assist Device
 Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Case - Advanced HF and Shock (INTERMACS 1)
") Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Left Ventricular Assist Devices (LVADs): Overview and Future Directions
: Overview and Future Directions") Left Ventricular Assist Devices (LVADs): Overview and Future Directions FATIMA KARAKI, M.D. PGY-3, DEPARTMENT OF MEDICINE WASHINGTON UNIVERSITY IN ST. LOUIS ST. LOUIS, MISSOURI, USA St. Louis, Missouri,
Left Ventricular Assist Devices (LVADs): Overview and Future Directions FATIMA KARAKI, M.D. PGY-3, DEPARTMENT OF MEDICINE WASHINGTON UNIVERSITY IN ST. LOUIS ST. LOUIS, MISSOURI, USA St. Louis, Missouri,
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Surgical Options for Temporary MCS
 Surgical Options for Temporary MCS Michael A. Acker, MD Julian Johnson Professor of Surgery Chief of Cardiovascular Surgery Director of Heart and Vascular Center University of Pennsylvania Health System
Surgical Options for Temporary MCS Michael A. Acker, MD Julian Johnson Professor of Surgery Chief of Cardiovascular Surgery Director of Heart and Vascular Center University of Pennsylvania Health System
Mechanical Circulatory Support in the Management of Heart Failure
 Mechanical Circulatory Support in the Management of Heart Failure Feras Bader, MD, MS, FACC Associate Professor of Medicine Director, Heart Failure and Transplant Cleveland Clinic Abu Dhabi Chairman, Heart
Mechanical Circulatory Support in the Management of Heart Failure Feras Bader, MD, MS, FACC Associate Professor of Medicine Director, Heart Failure and Transplant Cleveland Clinic Abu Dhabi Chairman, Heart
Advances in Advanced Heart Failure Therapies. Disclosures. Management Algorithm for Patients in Cardiogenic Shock
 Advances in Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center May 20, 2013 Joseph G. Rogers, M.D. Associate Professor
Advances in Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center May 20, 2013 Joseph G. Rogers, M.D. Associate Professor
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Ventricular Assisting Devices in the Cathlab. Unrestricted
 Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support
 Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced
Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced
Bridge to Heart Transplantation
 Bridge to Heart Transplantation Ulf Kjellman MD, PhD Senior Consultant Surgeon Heart Centre KFSH&RC 1 Disclosure Appointed for Proctorship by Thoratec/St.Jude/Abbott 2 To run a full overall covering transplant
Bridge to Heart Transplantation Ulf Kjellman MD, PhD Senior Consultant Surgeon Heart Centre KFSH&RC 1 Disclosure Appointed for Proctorship by Thoratec/St.Jude/Abbott 2 To run a full overall covering transplant
Rhondalyn C. McLean. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume VII, A. Study Purpose and Rationale
 A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
Recovering Hearts. Saving Lives.
 Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management
 Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know!
: What Every Pharmacist Needs to Know!") Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Acute Circulatory Support Should We or Shouldn t We?
 Acute Circulatory Support Should We or Shouldn t We? Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional Research
Acute Circulatory Support Should We or Shouldn t We? Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional Research
MEDICAL POLICY No R8 VENTRICULAR ASSIST DEVICES & ARTIFICIAL HEARTS
 VENTRICULAR ASSIST DEVICES & ARTIFICIAL HEARTS Effective Date: January 29, 2018 Review Dates: 8/05, 6/06, 6/07, 6/08, 10/08, 10/09, 10/10, 10/11, 10/12, 10/13, 11/14, 11/15, 11/16, 11/17, 11/18 Date Of
VENTRICULAR ASSIST DEVICES & ARTIFICIAL HEARTS Effective Date: January 29, 2018 Review Dates: 8/05, 6/06, 6/07, 6/08, 10/08, 10/09, 10/10, 10/11, 10/12, 10/13, 11/14, 11/15, 11/16, 11/17, 11/18 Date Of
Why Children Are Not Small Adults? Treatment of Pediatric Patients Needing Mechanical Circulatory Support
 Why Children Are Not Small Adults? Treatment of Pediatric Patients Needing Mechanical Circulatory Support Utpal S Bhalala, MD, FAAP Assistant Professor and Director of Research Pediatric Critical Care
Why Children Are Not Small Adults? Treatment of Pediatric Patients Needing Mechanical Circulatory Support Utpal S Bhalala, MD, FAAP Assistant Professor and Director of Research Pediatric Critical Care
Ted Feldman, M.D., MSCAI FACC FESC
 Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Ventricular Assist Devices (VADs) and Percutaneous Cardiac Support Systems
 and Percutaneous Cardiac Support Systems") Medical Coverage Policy Effective Date... 2/15/2018 Next Review Date... 2/15/2019 Coverage Policy Number... 0054 Ventricular Assist Devices (VADs) and Percutaneous Cardiac Support Systems Table of Contents
Medical Coverage Policy Effective Date... 2/15/2018 Next Review Date... 2/15/2019 Coverage Policy Number... 0054 Ventricular Assist Devices (VADs) and Percutaneous Cardiac Support Systems Table of Contents
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Novel Devices for End-Stage Heart Failure
 Novel Devices for End-Stage Heart Failure Lynne Warner Stevenson No conflicts of interest Off-label assist devices and expanded indications will be discussed Devices for End-Stage Heart Failure New definitions
Novel Devices for End-Stage Heart Failure Lynne Warner Stevenson No conflicts of interest Off-label assist devices and expanded indications will be discussed Devices for End-Stage Heart Failure New definitions
Surgical Options for Advanced Heart Failure
 Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
A National Cardiogenic Shock Initiative (CSI):
:") A National Cardiogenic Shock Initiative (CSI): Insights from the Impella Quality (IQ) Program, cvad Registry and the Detroit CSI Experience William O Neill, MD, FACC Medical Director Structural Heart Disease
A National Cardiogenic Shock Initiative (CSI): Insights from the Impella Quality (IQ) Program, cvad Registry and the Detroit CSI Experience William O Neill, MD, FACC Medical Director Structural Heart Disease
How to mend a broken heart: transplantation or LVAD?
 SCDU DI CARDIOCHIRURGIA Università degli Studi di Torino Ospedale S. Giovanni Battista Direttore: Prof. Mauro Rinaldi How to mend a broken heart: transplantation or LVAD? Massimo Boffini Mauro Rinaldi
SCDU DI CARDIOCHIRURGIA Università degli Studi di Torino Ospedale S. Giovanni Battista Direttore: Prof. Mauro Rinaldi How to mend a broken heart: transplantation or LVAD? Massimo Boffini Mauro Rinaldi
MEDICAL POLICY No R8 VENTRICULAR ASSIST DEVICES & ARTIFICIAL HEARTS
 VENTRICULAR ASSIST DEVICES & ARTIFICIAL HEARTS Effective Date: January 29, 2018 Review Dates: 8/05, 6/06, 6/07, 6/08, 10/08, 10/09, 10/10, 10/11, 10/12, 10/13, 11/14, 11/15, 11/16, 11/17 Date Of Origin:
VENTRICULAR ASSIST DEVICES & ARTIFICIAL HEARTS Effective Date: January 29, 2018 Review Dates: 8/05, 6/06, 6/07, 6/08, 10/08, 10/09, 10/10, 10/11, 10/12, 10/13, 11/14, 11/15, 11/16, 11/17 Date Of Origin:
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Pediatric Mechanical Circulatory Support (MCS)
") Pediatric Mechanical Circulatory Support (MCS) Ivan Wilmot, MD Heart Failure, Transplant, MCS Assistant Professor The Heart Institute Cincinnati Children s Hospital Medical Center The University of Cincinnati
Pediatric Mechanical Circulatory Support (MCS) Ivan Wilmot, MD Heart Failure, Transplant, MCS Assistant Professor The Heart Institute Cincinnati Children s Hospital Medical Center The University of Cincinnati
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Total Artificial Hearts and Implantable Ventricular Assist Devices
 Total Artificial Hearts and Implantable Ventricular Assist Devices Policy Number: 7.03.11 Last Review: 12/2013 Origination: 12/2001 Next Review: 12/2014 Policy Blue Cross and Blue Shield of Kansas City
Total Artificial Hearts and Implantable Ventricular Assist Devices Policy Number: 7.03.11 Last Review: 12/2013 Origination: 12/2001 Next Review: 12/2014 Policy Blue Cross and Blue Shield of Kansas City
Heart-lung transplantation: adult indications and outcomes
 Brief Report Heart-lung transplantation: adult indications and outcomes Yoshiya Toyoda, Yasuhiro Toyoda 2 Temple University, USA; 2 University of Pittsburgh, USA Correspondence to: Yoshiya Toyoda, MD,
Brief Report Heart-lung transplantation: adult indications and outcomes Yoshiya Toyoda, Yasuhiro Toyoda 2 Temple University, USA; 2 University of Pittsburgh, USA Correspondence to: Yoshiya Toyoda, MD,
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Total Artificial Hearts and Implantable Ventricular Assist Devices
 Total Artificial Hearts and Implantable Ventricular Assist Devices Policy Number: 7.03.11 Last Review: 12/2018 Origination: 12/2001 Next Review: 12/2019 Policy Blue Cross and Blue Shield of Kansas City
Total Artificial Hearts and Implantable Ventricular Assist Devices Policy Number: 7.03.11 Last Review: 12/2018 Origination: 12/2001 Next Review: 12/2019 Policy Blue Cross and Blue Shield of Kansas City
Acute Mechanical Circulatory Support Right Ventricular Support Devices
 Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Giving your heart strength. Ventricular Assist Device.
 Giving your heart strength. Ventricular Assist Device. 1 National leader in Ventricular Assist Devices Although you may be nervous when considering heart surgery, you can rest assured knowing that UR Medicine
Giving your heart strength. Ventricular Assist Device. 1 National leader in Ventricular Assist Devices Although you may be nervous when considering heart surgery, you can rest assured knowing that UR Medicine
Overview of MCS in Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation
 Overview of MCS in 2017 Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation Technology Embracing Progress Technology Adoption Internet Adoption of Technology Pioneer in the
Overview of MCS in 2017 Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation Technology Embracing Progress Technology Adoption Internet Adoption of Technology Pioneer in the
OPTN/UNOS-Thoracic Organ Transplantation Committee: Proposed Modifications to Adult Heart Allocation
 OPTN/UNOS-Thoracic Organ Transplantation Committee: Proposed Modifications to Adult Heart Allocation What problems is the proposal attempting to solve? Each zone = 500 mile radius Heart and Lung Allocation
OPTN/UNOS-Thoracic Organ Transplantation Committee: Proposed Modifications to Adult Heart Allocation What problems is the proposal attempting to solve? Each zone = 500 mile radius Heart and Lung Allocation
Destination Therapy SO MUCH DATA IN SUCH A SMALL DEVICE. HeartWare HVAD System The ONLY intrapericardial VAD approved for DT.
 DT Destination Therapy SO MUCH DATA IN SUCH A SMALL DEVICE. HeartWare HVAD System The ONLY intrapericardial VAD approved for DT. ONLY WE HAVE THIS BREADTH OF CLINICAL EVIDENCE TO SUPPORT DESTINATION THERAPY.
DT Destination Therapy SO MUCH DATA IN SUCH A SMALL DEVICE. HeartWare HVAD System The ONLY intrapericardial VAD approved for DT. ONLY WE HAVE THIS BREADTH OF CLINICAL EVIDENCE TO SUPPORT DESTINATION THERAPY.
MANAGEMENT OF CARDIOGENIC SHOCK
 MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
Name of Policy: Ventricular Assist Devices and Total Artificial Hearts
 Name of Policy: Ventricular Assist Devices and Total Artificial Hearts Policy #: 033 Latest Review Date: February 2014 Category: Surgery Policy Grade: A Background/Definitions: As a general rule, benefits
Name of Policy: Ventricular Assist Devices and Total Artificial Hearts Policy #: 033 Latest Review Date: February 2014 Category: Surgery Policy Grade: A Background/Definitions: As a general rule, benefits
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ
 Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
The World s Smallest Heart Pump
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/the-worlds-smallest-heart-pump/3367/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/the-worlds-smallest-heart-pump/3367/
Ventricular Assist Devices
 Page 1 By Tonya Elliott, RN, MSN Background, Indications for VADs Mechanical circulatory support has become an acceptable therapy for end stage heart failure (HF) in maximally medically treated patients
Page 1 By Tonya Elliott, RN, MSN Background, Indications for VADs Mechanical circulatory support has become an acceptable therapy for end stage heart failure (HF) in maximally medically treated patients
Cardiogenic Shock and Initiatives to Reduce Mortality
 Cardiogenic Shock and Initiatives to Reduce Mortality Tanveer Rab, MD, FACC William O Neill, MD, FACC Perwaiz Meraj, MD, FACC Alex Truesdell, MD, FACC The Golden Hours? 50% dead within 10 hours Overall
Cardiogenic Shock and Initiatives to Reduce Mortality Tanveer Rab, MD, FACC William O Neill, MD, FACC Perwaiz Meraj, MD, FACC Alex Truesdell, MD, FACC The Golden Hours? 50% dead within 10 hours Overall
MEDICAL POLICY SUBJECT: VENTRICULAR ASSIST DEVICES
 MEDICAL POLICY PAGE: 1 OF: 7 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 7 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Do we really need an Artificial Heart? No!! John V. Conte, MD, Professor of Surgery Johns Hopkins University School of Medicine
 Do we really need an Artificial Heart? No!! John V. Conte, MD, Professor of Surgery Johns Hopkins University School of Medicine Division of Cardiac Surgery The Johns Hopkins Medical Institutions Conflict
Do we really need an Artificial Heart? No!! John V. Conte, MD, Professor of Surgery Johns Hopkins University School of Medicine Division of Cardiac Surgery The Johns Hopkins Medical Institutions Conflict
Donor/Recipient Risk Scores: Review of Published Approaches from Europe and the US
 Donor/Recipient Risk Scores: Review of Published Approaches from Europe and the US Michael M. Givertz, MD Medical Director, Heart Transplant and MCS Brigham and Women s Hospital Professor of Medicine,
Donor/Recipient Risk Scores: Review of Published Approaches from Europe and the US Michael M. Givertz, MD Medical Director, Heart Transplant and MCS Brigham and Women s Hospital Professor of Medicine,
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR
 PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
Transplant in Pediatric Heart Failure
 Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
EMS and Nursing Considerations in VAD Patient Care
 EMS and Nursing Considerations in VAD Patient Care B R I T T A N Y B U T Z L E R B S N R N V A D C O O R D I N A T O R F R O E D T E R T A N D T H E M E D I C A L C O L L E G E O F W I 1 0 / 2 5 / 1 8
EMS and Nursing Considerations in VAD Patient Care B R I T T A N Y B U T Z L E R B S N R N V A D C O O R D I N A T O R F R O E D T E R T A N D T H E M E D I C A L C O L L E G E O F W I 1 0 / 2 5 / 1 8
Implantable Ventricular Assist Devices and Total Artificial Hearts
 Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
LV Distension and ECLS Lungs
 LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
Candidates about. Lung Allocation Policy. for Transplant. Questions & A n s we r s TA L K I N G A B O U T T R A N S P L A N TAT I O N
 TA L K I N G A B O U T T R A N S P L A N TAT I O N Questions & A n s we r s for Transplant Candidates about Lung Allocation Policy U N I T E D N E T W O R K F O R O R G A N S H A R I N G What are the OPTN
TA L K I N G A B O U T T R A N S P L A N TAT I O N Questions & A n s we r s for Transplant Candidates about Lung Allocation Policy U N I T E D N E T W O R K F O R O R G A N S H A R I N G What are the OPTN
Total Artificial Hearts and Implantable Ventricular Assist Devices
 Total Artificial Hearts and Implantable Ventricular Assist Devices Policy Number: 7.03.11 Last Review: 12/2017 Origination: 12/2001 Next Review: 12/2018 Policy Blue Cross and Blue Shield of Kansas City
Total Artificial Hearts and Implantable Ventricular Assist Devices Policy Number: 7.03.11 Last Review: 12/2017 Origination: 12/2001 Next Review: 12/2018 Policy Blue Cross and Blue Shield of Kansas City
The Role of Mechanical Circulatory Support in Cardiogenic Shock: When to Utilize
 The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies
 : An Intro, Complications, and Emergencies") Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies ERIC T. ROME D.O. HEART FAILURE, MECHANICAL ASSISTANCE AND TRANSPLANTATION CVI Left Ventricular Assist Device An
Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies ERIC T. ROME D.O. HEART FAILURE, MECHANICAL ASSISTANCE AND TRANSPLANTATION CVI Left Ventricular Assist Device An
ECMO and VAD implantation
 1 Udine ECMO Workshop ECMO and VAD implantation Prof. Tomaso Bottio Division of Cardiac Surgery (Director Prof. Gino gerosa) ECMO Extracorporeal membrane oxygena1on (ECMO) is a rescue therapy to support
1 Udine ECMO Workshop ECMO and VAD implantation Prof. Tomaso Bottio Division of Cardiac Surgery (Director Prof. Gino gerosa) ECMO Extracorporeal membrane oxygena1on (ECMO) is a rescue therapy to support
Selecting Patients for the SynCardia temporary Total Artificial Heart Help Your Patients Live Longer, Live Better
 Selecting Patients for the SynCardia temporary Total Artificial Heart Help Your Patients Live Longer, Live Better The SynCardia Total Artificial Heart (TAH) is a clinically proven life-saving treatment
Selecting Patients for the SynCardia temporary Total Artificial Heart Help Your Patients Live Longer, Live Better The SynCardia Total Artificial Heart (TAH) is a clinically proven life-saving treatment
CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock
 CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Yoshiya Toyoda, MD, PhD William Maul Measey Professor of Surgery Chief, Cardiovascular Surgery Surgical Director, Mechanical
CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Yoshiya Toyoda, MD, PhD William Maul Measey Professor of Surgery Chief, Cardiovascular Surgery Surgical Director, Mechanical
Implantable Ventricular Assist Devices and Total Artificial Hearts
 Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA. IMP v4
 1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
What has INTERMACS Taught Us about Patient Outcomes with Durable MCS? James K. Kirklin, MD
 What has INTERMACS Taught Us about Patient Outcomes with Durable MCS? James K. Kirklin, MD Disclosure: I am Director of the Data Coordinating Center for the INTERMACS project and receive support through
What has INTERMACS Taught Us about Patient Outcomes with Durable MCS? James K. Kirklin, MD Disclosure: I am Director of the Data Coordinating Center for the INTERMACS project and receive support through
Description. Section: Surgery Effective Date: April 15, Subsection: Transplant Original Policy Date: September 13, 2012 Subject:
 Last Review Status/Date: March 2016 Page: 1 of 30 Description Mechanical devices to assist or replace a failing heart have been developed over many decades of research. A ventricular assist device (VAD)
Last Review Status/Date: March 2016 Page: 1 of 30 Description Mechanical devices to assist or replace a failing heart have been developed over many decades of research. A ventricular assist device (VAD)
Implantable Ventricular Assist Devices and Total Artificial Hearts
 Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
ORIGINAL ARTICLE. Alexander M. Bernhardt a, *, Theo M.M.H. De By b, Hermann Reichenspurner a and Tobias Deuse a. Abstract INTRODUCTION
 European Journal of Cardio-Thoracic Surgery 48 (2015) 158 162 doi:10.1093/ejcts/ezu406 Advance Access publication 29 October 2014 ORIGINAL ARTICLE Cite this article as: Bernhardt AM, De By TMMH, Reichenspurner
European Journal of Cardio-Thoracic Surgery 48 (2015) 158 162 doi:10.1093/ejcts/ezu406 Advance Access publication 29 October 2014 ORIGINAL ARTICLE Cite this article as: Bernhardt AM, De By TMMH, Reichenspurner
Ventricular Assist Devices for Permanent Therapy: Current Status and Future
 Ventricular Assist Devices for Permanent Therapy: Current Status and Future Prospects Francis D. Pagani MD PhD Professor of Cardiac Surgery University of Michigan April 28 th, 2012 Disclosures NHLBI and
Ventricular Assist Devices for Permanent Therapy: Current Status and Future Prospects Francis D. Pagani MD PhD Professor of Cardiac Surgery University of Michigan April 28 th, 2012 Disclosures NHLBI and
VENTRICULAR ASSIST DEVICES AND TOTAL ARTIFICIAL HEARTS
 VENTRICULAR ASSIST DEVICES AND TOTAL ARTIFICIAL HEARTS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures,
VENTRICULAR ASSIST DEVICES AND TOTAL ARTIFICIAL HEARTS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures,