Jamie Rickards, PharmD, MBA, BCPS, CPP PGY-2 Geriatric Pharmacy Resident
|
|
|
- Joella Payne
- 5 years ago
- Views:
Transcription

1 Jamie Rickards, PharmD, MBA, BCPS, CPP PGY-2 Geriatric Pharmacy Resident
2 Background 1,2 Dyspnea- derives from Greek dys - abnormal/difficult and pnoia meaning breath Defined as uncomfortable sensation or awareness of breathing: Air Hunger ~ Suffocation ~ Shortness of Breath Dyspnea one of the most common symptoms reported in end of life care A subjective symptom similar to pain Dyspnea Tachypnea
 correlates highly with disability Prevents patient involvement with any activities, including talking in")
3 Effects of Dyspnea 3 Physical Fatigue and tiredness Decrease in functional status (low Karnofsky performance score) Emotional Social Distressing to family and patient More likely to be anxious and depressed Associated with anger, helplessness, loneliness Dyspnea (rather than lung function) correlates highly with disability Prevents patient involvement with any activities, including talking in severe cases Spiritual Positive correlation with spiritual distress
4 Dyspnea and Life Expectancy 4,5 Dyspnea may predict shortened survival in cancer patients Patients with cancer presenting to ED with dyspnea had median overall survival of 12 weeks Lung cancer- 4 weeks Breast cancer- 22 weeks Elevated pulse and respiratory rate along with cancer-related dyspnea correlated with a predicted mean survival of < 2 weeks
5 Etiology 6 Increase in respiratory effort needed to overcome obstruction/restrictive disease; more respiratory muscles required to maintain adequate breathing; increase in ventilatory need Terminally illnesses commonly reporting dyspnea Advanced malignant disease COPD Heart Failure Deconditioning Pneumonia AIDS

6 Regulation of Normal Breathing 2,7
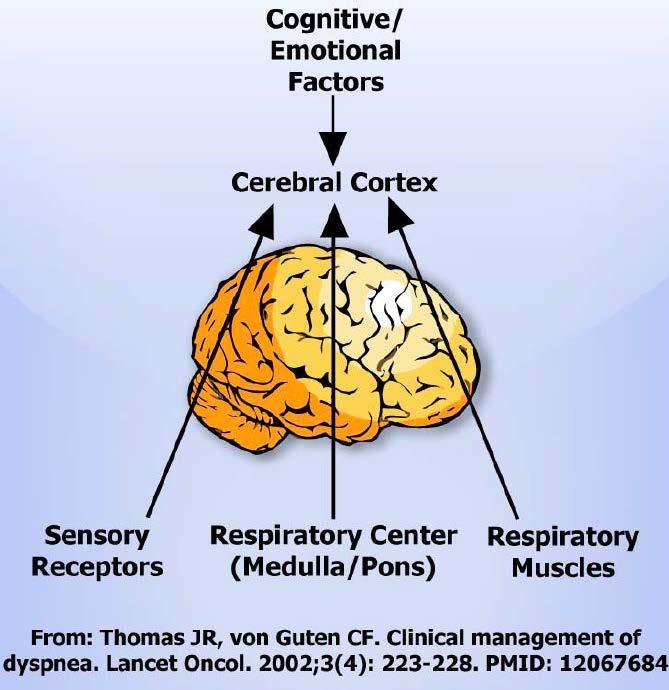
7 2
8 Main Abnormalities in Mechanical Impairment Dyspnea 6,8 Increased resistance requiring increased workload COPD, Bronchial Obstruction Workload Increase in the proportion of respiratory muscles needed to sustain workload Weakened respiratory muscles (cachexia, neuromuscular weakness) Ventilator Demand Increase in ventilatory demand Hypoxia, hypercapnia, metabolic acidosis, anemia
9 Goal Standard: Patient self-report Objective signs include Areas of pulmonary dullness or crackles Inability to clear secretions Stridor Bronchospasm (wheezing) Central or peripheral cyanosis Intercostal retractions Tachypnea Assessment 2
10 Goals of Therapy 9 Identify and treat underlying cause of dyspnea if applicable Fully address all other concomitant symptoms, stressors, and spiritual distress

11 Biopsychosocial Model of Dyspnea Management 9
12 The City of Hope QOL Model
13 Bronchoconstriction = Albuterol/ipratropium nebulizers Hypoxia = Oxygen Nicotine cravings = Nicotine patch/clonidine patch Treat Underlying Cause Fluid overload/chf = Diuretics COPD exacerbation; superior vena cava obstruction; lymphangitic carcinomatosis = Steroids Cough = Antitussives/opioids Pneumonia/infectious process (not terminal pneumonia) = antibiotics 3,9,10



14 Symptom Palliation 9,11 Dyspnea Opioids Nonpharmacologic Options Fan; Elevating head of bed; Reducing environmental irritants
15 Dyspnea Anxiety Opioids should remain first line when anxiety is a component Benzodiazepines should not be used first line as mono-therapy for dyspnea. Benzodiazepines may be used as adjunct therapy when opioids are not fully successful Lorazepam: initial mg PO, SL, buccal, or SC q 1 h PRN and titrate to effect. Once the TDD established, provide 1/3 q 8 h routinely. 8,12
16 MOA of Opioids in Dyspnea Mechanism not completely understood- multiple theories e May reduce the sensitivity and responsiveness of the medullary respiratory centers to hypoxia and hypercapnia Addition of 100% oxygen can induce apnea May inhibit stimulus-evoked release of ACh Mu and delta opioid receptors Opioid receptors are located throughout the respiratory tract and must abundantly in the aveolar walls May active opioid receptors associated with pulmonary afferents on vagal C-fibers believed to be within the aveolar wall
17 Opioids 2,9,13,14 Much lower doses are needed to relieve dyspnea than that which can cause respiratory depression Opioid naïve patient Morphine 10 to 15mg po q1h PRN and titrate to effect Possible alternative: hydromorphone 2.5mg orally q6h On baseline opioids Increase opioid dose by 25%and titrate to effect Chronic dyspnea ER formulation for baseline control w/ 10% of TDD for breakthrough dyspnea
18 Inhaled Opioids Inhaled opioids have shown mixed results in improving dyspnea with most showing minimal effect Rapid administration of morphine can produce pulmonary venoconstriction secondary to histamine release Studies have shown that the opioid lung receptor density is altered in sensitized airways and may contain a nonconventional opioid receptor. Decrease in delta receptors w/ sensitized tissues Mucus secretions not inhibited by kappa agonists
19 Summary of Treatment Options for Dypsnea 9
20 References 1. Bruera E, Schmitz B, Pither J, et al.: The frequency and correlates of dyspnea in patients with advanced cancer. J Pain Symptom Manage 19 (5): , Dyspnea. Self study module 3j. Education in Palliative and End-of-life Care for Oncology(EPIC -O). e-3/module-3j-pdf 3. Palliative Distress. Palliative Care. Stanford School of Medicine. Accessed June 5, 2014http://palliative.stanford.edu/dyspnea-how-to-assess-andpalliate-dyspnea-air-hunger/patient-distress/ 4. Escalante CP, Martin CG, Elting LS, et al.: Dyspnea in cancer patients. Etiology, resource utilization, and survival-implications in a managed care world. Cancer. 1996; 78 (6): Escalante CP, Martin CG, Elting LS, et al.: Identifying risk factors for imminent death in cancer patients with acute dyspnea. J Pain Symptom Manage. 2000;20 (5): Ripamonti C: Management of dyspnea in advanced cancer patients. Support Care Cancer. 1999;7 (4):
21 References 7. Dudgeon DJ, Lertzman M. Dyspnea in the advanced cancer patient. J Pain Symptom Manage. 1998;16: Symptom Management. Last days of life. National Cancer Institute at the NIH. Accessed June 8,2014 at hprofessional/page2#reference Kamal AH, Maguire JM, Wheeler JL, et al. Dyspnea review for the palliative care professional: Treatment goals and Therapeutic Options. J Palliative Medicine. 2012; 15(1): Clemens KE, Quednau I, Klaschik E: Use of oxygen and opioids in the palliation of dyspnea in hypoxic and nonhypoxic palliative care patients: A prospective study. Support Care Center 2009;17: Galbraith S, Fagan P, Perkins P, et al. Does the use of a handheld fan improve chronic dyspnea? A randomized controlled, crossover trial. J Pain Symptom Manage. 2010;39(5): Navigante AH, Cerchietti LC, Castro MA, Lutteral MA, Cabalar ME: Midazolam as adjunct therapy to morphine in the alleviation of severe dyspnea perception in patients with advanced cancer. J Pain Symptom Manage 2006;31:
22 References 13. Currow DC, McDonald C, Oaten S, Kenny B, Allcroft P, Frith P, Briffa M, Johnson MJ, Abernethy AP: Once-daily opioids for chronic dyspnea: A dose increment and pharmacovigilance study. J Pain Symptom Manage 2011;42: Clemens KE, Klaschik E: Effect of hydromorphone on ventilation in palliative care patients with dyspnea. SupportCare Cancer 2008;16: Charles MA, Reymond L, Israel Jennings AL, Davies AN, Higgins JP, Gibbs JS, Broadley KE: A systematic review of the use of opioids in the management of dyspnea. Thorax. 2002;57: Ben-Aharon I, Gafter-Gvili A, Paul M, Leibovici L, Semmer SM: Interventions for alleviating cancer-related dyspnea: A systematic review. J Clin Oncol 2008;26: Viola R, Kiteley C, Lloyd NS, Mackay JA, Wilson J, Wong RK: The management of dyspnea in cancer patients: A systematic review. Support Care Cancer 2008;16: Kohara H, Ueoka H, Aoe K, et al. Effect of nebulized furosemide in terminally ill cancer patients with dyspnea. J Pain Symptom Manage. 2003;2(4):
Dyspnea. Stephanie Lindsay
 Dyspnea Stephanie Lindsay What is dyspnea? An unpleasant sensation of difficult, labored breathing Shortness of air Dyspnea is not the same as tachypnea therefore patients may not present with rapid breathing
Dyspnea Stephanie Lindsay What is dyspnea? An unpleasant sensation of difficult, labored breathing Shortness of air Dyspnea is not the same as tachypnea therefore patients may not present with rapid breathing
Breathlessness in advanced disease. February 2017
 Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Dyspnea: Evaluation and Management
 Dyspnea: Evaluation and Management Sandra Whitlock, M.D. Four Seasons Palliative Care Course Handouts & Post Test o To download presentation handouts, click on the attachment icon o Presenter discloses
Dyspnea: Evaluation and Management Sandra Whitlock, M.D. Four Seasons Palliative Care Course Handouts & Post Test o To download presentation handouts, click on the attachment icon o Presenter discloses
Management of Dyspnea and Cough in Lung Cancer
 Management of Dyspnea and Cough in Lung Cancer Dr. Chris Ogaranko Lung Cancer Educational Event November 2013 Presenter Disclosure Faculty: Dr. Chris Ogaranko Relationships with commercial interests: Grants/Research
Management of Dyspnea and Cough in Lung Cancer Dr. Chris Ogaranko Lung Cancer Educational Event November 2013 Presenter Disclosure Faculty: Dr. Chris Ogaranko Relationships with commercial interests: Grants/Research
Palliative Emergencies. Ken Stakiw
 Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
TREATING RESPIRATORY SYMPTOMS IN PEDIATRIC PALLIATIVE CARE: Objectives 10/23/18 FROM DYSPNEA TO NOISY BREATHING
 TREATING RESPIRATORY SYMPTOMS IN PEDIATRIC PALLIATIVE CARE: FROM DYSPNEA TO NOISY BREATHING Kris Catrine, MD, FAAP, HMDC October 24, 2018 Objectives Discuss pathophysiology of common respiratory symptoms
TREATING RESPIRATORY SYMPTOMS IN PEDIATRIC PALLIATIVE CARE: FROM DYSPNEA TO NOISY BREATHING Kris Catrine, MD, FAAP, HMDC October 24, 2018 Objectives Discuss pathophysiology of common respiratory symptoms
Title: Pharmacological Management for Dyspnea in Palliative Cancer Patients: Clinical Review and Guidelines
 Title: Pharmacological Management for Dyspnea in Palliative Cancer Patients: Clinical Review and Guidelines Date: 10 July 2008 Context and policy issues: Dyspnea, defined as a subjective experience of
Title: Pharmacological Management for Dyspnea in Palliative Cancer Patients: Clinical Review and Guidelines Date: 10 July 2008 Context and policy issues: Dyspnea, defined as a subjective experience of
Dyspnea: The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program
 : The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program Faculty / Presenter Disclosure Faculty: Dr. Lawrence Lee Relationships with commercial
: The top things you need to you know! Dr. Megan Sellick & Dr. Lawrence Lee Edmonton Zone Palliative Care Program Faculty / Presenter Disclosure Faculty: Dr. Lawrence Lee Relationships with commercial
BREATHLESSNESS MANAGEMENT
 Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Sam H Ahmedzai Academic Unit of Supportive Care Department of Oncology The University of Sheffield & Sheffield Teaching Hospitals NHS Foundation
 Sam H Ahmedzai Academic Unit of Supportive Care Department of Oncology The University of Sheffield & Sheffield Teaching Hospitals NHS Foundation Trust Overview Which drugs? How much? How to give? Adverse
Sam H Ahmedzai Academic Unit of Supportive Care Department of Oncology The University of Sheffield & Sheffield Teaching Hospitals NHS Foundation Trust Overview Which drugs? How much? How to give? Adverse
Dr. A. Kerigan BREATHLESSNESS AT THE END OF LIFE
 Dr. A. Kerigan BREATHLESSNESS AT THE END OF LIFE Faculty/Presenter Disclosure Faculty: Dr. A. Kerigan Relationships with commercial interests:* - Grants/Research Support: None - Speakers Bureau/Honoraria:
Dr. A. Kerigan BREATHLESSNESS AT THE END OF LIFE Faculty/Presenter Disclosure Faculty: Dr. A. Kerigan Relationships with commercial interests:* - Grants/Research Support: None - Speakers Bureau/Honoraria:
Respiratory Issues at End-of-Life. Jerry Boltz, FNP January 27, L N E C Geriatric Curriculum
 Respiratory Issues at nd-of-life Jerry Boltz, FNP January 27, 2012 L N C Geriatric Curriculum nd-of-life Nursing ducation Consortium Module 3: Nonpain Symptoms at the nd of Life Part I Common Respiratory
Respiratory Issues at nd-of-life Jerry Boltz, FNP January 27, 2012 L N C Geriatric Curriculum nd-of-life Nursing ducation Consortium Module 3: Nonpain Symptoms at the nd of Life Part I Common Respiratory
Management of Dyspnea/Breathlessness for the Medical and Hematological Oncologist
 Management of Dyspnea/Breathlessness for the Medical and Hematological Oncologist Author: Jeff Myers MD, CCFP, MSEd Program Head Integrated Psychosocial, Supportive, Palliative Care Program Odette Cancer
Management of Dyspnea/Breathlessness for the Medical and Hematological Oncologist Author: Jeff Myers MD, CCFP, MSEd Program Head Integrated Psychosocial, Supportive, Palliative Care Program Odette Cancer
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital.
 Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Gestione della dispnea nell insufficienza respiratoria end-stage
 Gestione della dispnea nell insufficienza respiratoria end-stage Salvatore M. Maggiore, MD, PhD salvatore.maggiore@unich.it Anesthesia and Intensive Care SS. Annunziata Hospital Gabriele d Annunzio University
Gestione della dispnea nell insufficienza respiratoria end-stage Salvatore M. Maggiore, MD, PhD salvatore.maggiore@unich.it Anesthesia and Intensive Care SS. Annunziata Hospital Gabriele d Annunzio University
Jeffrey B. Rubins, MD Director, Palliative Medicine, HCMC Professor of Medicine, UMN
 Jeffrey B. Rubins, MD Director, Palliative Medicine, HCMC Professor of Medicine, UMN Mechanisms of dyspnea otreat reversible causes opalliation of refractory dyspnea Dyspnea Analogous to pain Dyspnea is
Jeffrey B. Rubins, MD Director, Palliative Medicine, HCMC Professor of Medicine, UMN Mechanisms of dyspnea otreat reversible causes opalliation of refractory dyspnea Dyspnea Analogous to pain Dyspnea is
Nebulized Versus Subcutaneous Morphine for Patients with Cancer Dyspnea: A Preliminary Study
 Vol. 29 No. 6 June 2005 Journal of Pain and Symptom Management 613 Clinical Note Nebulized Versus Subcutaneous Morphine for Patients with Cancer Dyspnea: A Preliminary Study Eduardo Bruera, MD, Raul Sala,
Vol. 29 No. 6 June 2005 Journal of Pain and Symptom Management 613 Clinical Note Nebulized Versus Subcutaneous Morphine for Patients with Cancer Dyspnea: A Preliminary Study Eduardo Bruera, MD, Raul Sala,
Approach to symptom control near the end-of-life
 Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Hospice and Palliative Nurses Association (HPNA) Clinical Practice Forum October 23 24, 2015
 Clinical Practice Forum October 23 24, 2015") Dyspnea Assessment and Treatment at the End of Life Margaret L. Campbell, PhD, RN, FPCN Professor, Wayne State University Detroit, MI Disclosures Margaret Campbell has no real or perceived conflicts of
Dyspnea Assessment and Treatment at the End of Life Margaret L. Campbell, PhD, RN, FPCN Professor, Wayne State University Detroit, MI Disclosures Margaret Campbell has no real or perceived conflicts of
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011
 Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011 Kathy Witmer, MN, ARNP Swedish Cancer Institute Thoracic Surgery - Oncology Dyspnea The word denotes disordered breathing
Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011 Kathy Witmer, MN, ARNP Swedish Cancer Institute Thoracic Surgery - Oncology Dyspnea The word denotes disordered breathing
Regional Breathlessness Audit - Case Note Survey. 1. Introduction. Regional Breathlessness Audit - Case Note Survey. 2.
 Regional Breathlessness Audit - Case te Survey 1. Introduction Please complete this form for your case note review. Cases used may be PROSPECTIVE AND/OR RETROSPECTIVE. Please log as many cases as you can.
Regional Breathlessness Audit - Case te Survey 1. Introduction Please complete this form for your case note review. Cases used may be PROSPECTIVE AND/OR RETROSPECTIVE. Please log as many cases as you can.
Effect of Nebulized Furosemide in Terminally Ill Cancer Patients with Dyspnea
 962 Journal of Pain and Symptom Management Vol. 26 No. 4 October 2003 Clinical Note Effect of Nebulized Furosemide in Terminally Ill Cancer Patients with Dyspnea Hiroyuki Kohara, MD, PhD, Hiroshi Ueoka,
962 Journal of Pain and Symptom Management Vol. 26 No. 4 October 2003 Clinical Note Effect of Nebulized Furosemide in Terminally Ill Cancer Patients with Dyspnea Hiroyuki Kohara, MD, PhD, Hiroshi Ueoka,
PRACTICAL DYSPNEA MANAGEMENT Margot Sondermann BScPT, MEd. Palliative Consultant for End-Stage Lung Disease, Calgary Zone
 PRACTICAL DYSPNEA MANAGEMENT Margot Sondermann BScPT, MEd. Palliative Consultant for End-Stage Lung Disease, Calgary Zone Faculty / Presenter Disclosure Faculty: Margot Sondermann Relationships with commercial
PRACTICAL DYSPNEA MANAGEMENT Margot Sondermann BScPT, MEd. Palliative Consultant for End-Stage Lung Disease, Calgary Zone Faculty / Presenter Disclosure Faculty: Margot Sondermann Relationships with commercial
5/3/2012 PRESENTATION GOALS RESPIRATORY THERAPISTS ROLE IN END OF LIFE CARE FOR THE PULMONARY PATIENT
 RESPIRATORY THERAPISTS ROLE IN END OF LIFE CARE FOR THE PULMONARY PATIENT Presented by Carrie Black Bourassa, LRT, RRT PRESENTATION GOALS Define palliative care Define hospice care Discuss pulmonary hospice
RESPIRATORY THERAPISTS ROLE IN END OF LIFE CARE FOR THE PULMONARY PATIENT Presented by Carrie Black Bourassa, LRT, RRT PRESENTATION GOALS Define palliative care Define hospice care Discuss pulmonary hospice
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Dyspnea. Latest Research in Management of Breathlessness and Current Use of Diagnostic Tools Elissa Tiller, MD Karin Lee Hughes, MD
 Foundations in Palliative Medicine Palliative Care Interdisciplinary Curriculum Colorado, November 2017 Dyspnea Latest Research in Management of Breathlessness and Current Use of Diagnostic Tools Elissa
Foundations in Palliative Medicine Palliative Care Interdisciplinary Curriculum Colorado, November 2017 Dyspnea Latest Research in Management of Breathlessness and Current Use of Diagnostic Tools Elissa
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
FACULTY OBJECTIVES 12/4/2017. Women > Men in recent years END-OF-LIFE CARE IN LUNG DISEASE.
 END-OF-LIFE CARE IN LUNG DISEASE STEPHEN A. LEEDY, MD MA HMDC FAAHPM FACULTY STEPHEN A. LEEDY, MD MA HMDC FAAHPM PRESIDENT & CEO Helping Hospices Excel www.upstreaminghealthcare.com OBJECTIVES Leading
END-OF-LIFE CARE IN LUNG DISEASE STEPHEN A. LEEDY, MD MA HMDC FAAHPM FACULTY STEPHEN A. LEEDY, MD MA HMDC FAAHPM PRESIDENT & CEO Helping Hospices Excel www.upstreaminghealthcare.com OBJECTIVES Leading
APHN. Shortness of breath. Ednin Hamzah CEO, Hospis Malaysia.
 APHN Shortness of breath Ednin Hamzah CEO, Hospis Malaysia ednin@hospismalaysia.org What is it? a subjective experience of difficult and uncomfortable breathing American Thoracic Society What do the patients
APHN Shortness of breath Ednin Hamzah CEO, Hospis Malaysia ednin@hospismalaysia.org What is it? a subjective experience of difficult and uncomfortable breathing American Thoracic Society What do the patients
Peripheral mechanisms of dyspnoea
 Peripheral mechanisms of dyspnoea Miriam Johnson 2012 A complex interaction respiratory motor areas of the brain receive information and commands required ventilation ascending copy of descending motor
Peripheral mechanisms of dyspnoea Miriam Johnson 2012 A complex interaction respiratory motor areas of the brain receive information and commands required ventilation ascending copy of descending motor
Using Evidence Based Medicine to Ethically Provide End of Life Symptom Control
 Using Evidence Based Medicine to Ethically Provide End of Life Symptom Control Erin Zimny, MD Emergency Medicine Hospice and Palliative Medicine Henry Ford Hospital Disclosures I do NOT have any financial
Using Evidence Based Medicine to Ethically Provide End of Life Symptom Control Erin Zimny, MD Emergency Medicine Hospice and Palliative Medicine Henry Ford Hospital Disclosures I do NOT have any financial
GUIDELINES & PROTOCOLS
 GUIDELINES & PROTOCOLS ADVISORY COMMITTEE Palliative Care for the Patient with Incurable Cancer or Advanced Disease Part 2: Pain and Symptom Management Dyspnea Effective Date: September 30, 2011 Scope
GUIDELINES & PROTOCOLS ADVISORY COMMITTEE Palliative Care for the Patient with Incurable Cancer or Advanced Disease Part 2: Pain and Symptom Management Dyspnea Effective Date: September 30, 2011 Scope
Symptom Management and Palliative Care for Lung Cancer
 Symptom Management and Palliative Care for Lung Cancer DorAnne Donesky, PhD, ANP-BC, ACHPN Professor of Clinical Nursing Dept of Physiological Nursing Disclosures The presenter has no relevant financial
Symptom Management and Palliative Care for Lung Cancer DorAnne Donesky, PhD, ANP-BC, ACHPN Professor of Clinical Nursing Dept of Physiological Nursing Disclosures The presenter has no relevant financial
Oxygen Use in Palliative Care Guideline and Flowchart
 Oxygen Use in Palliative Care Guideline and Flowchart Reviewed: October 2013 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy. Title Keywords Ratified Oxygen Use in Palliative
Oxygen Use in Palliative Care Guideline and Flowchart Reviewed: October 2013 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy. Title Keywords Ratified Oxygen Use in Palliative
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Dyspnea: Assessment and Management
 Dyspnea: Assessment and Management Page 1 of 7 Table of Contents Introduction for the Learner (Resident/Oncology Fellow).............................................. 2 Introduction for Clinical Faculty
Dyspnea: Assessment and Management Page 1 of 7 Table of Contents Introduction for the Learner (Resident/Oncology Fellow).............................................. 2 Introduction for Clinical Faculty
To Drain or Not to Drain: An Evidence-Based Approach to Palliative Procedures for the Management of Malignant Pleural Effusions
 Vol. 44 No. 2 August 2012 Journal of Pain and Symptom Management 301 Palliative Care Rounds Edited by Erik K. Fromme, MD, and Robert M. Arnold, MD, on behalf of Society of General Internal Medicine End-of-Life
Vol. 44 No. 2 August 2012 Journal of Pain and Symptom Management 301 Palliative Care Rounds Edited by Erik K. Fromme, MD, and Robert M. Arnold, MD, on behalf of Society of General Internal Medicine End-of-Life
Morphine Versus Midazolam as Upfront Therapy to Control Dyspnea Perception in Cancer Patients While Its Underlying Cause Is Sought or Treated
 820 Journal of Pain and Symptom Management Vol. 39 No. 5 May 2010 Original Article Morphine Versus Midazolam as Upfront Therapy to Control Dyspnea Perception in Cancer Patients While Its Underlying Cause
820 Journal of Pain and Symptom Management Vol. 39 No. 5 May 2010 Original Article Morphine Versus Midazolam as Upfront Therapy to Control Dyspnea Perception in Cancer Patients While Its Underlying Cause
COPD AND PALLIATIVE CARE JEAN WATERS FNP-BC SENTARA RMH PALLIATIVE CARE JANUARY 13, 2018
 COPD AND PALLIATIVE CARE JEAN WATERS FNP-BC SENTARA RMH PALLIATIVE CARE JANUARY 13, 2018 THOUGHTS TO CONSIDER What is Palliative Care? COPD and impact on Quality of Life. Prognosis and impact of co-morbidities
COPD AND PALLIATIVE CARE JEAN WATERS FNP-BC SENTARA RMH PALLIATIVE CARE JANUARY 13, 2018 THOUGHTS TO CONSIDER What is Palliative Care? COPD and impact on Quality of Life. Prognosis and impact of co-morbidities
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Dyspnea: Should we use BIPAP?
 Dyspnea: Should we use BIPAP? Thomas R. Gildea MD, MS FCCP Head Section of Bronchoscopy Respiratory Institute Transplant Center Disclosure SuperDimension Inc. PI for single center study Others: Aeris,
Dyspnea: Should we use BIPAP? Thomas R. Gildea MD, MS FCCP Head Section of Bronchoscopy Respiratory Institute Transplant Center Disclosure SuperDimension Inc. PI for single center study Others: Aeris,
A Visual Approach to Simplifying Respiratory Drug Regimens
 Adverse Effects of Inhaled Medications A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP June 28, 2017 Drug Category Beta 2 agonists antagonists Adverse Effects
Adverse Effects of Inhaled Medications A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP June 28, 2017 Drug Category Beta 2 agonists antagonists Adverse Effects
10/17/16. Acute Respiratory Failure in the Acute Care Setting. Margaret Rosales, APRN-CNP, FNP
 Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
A Visual Approach to Simplifying Respiratory Drug Regimens
 A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP October 23, 2017 Learning Objectives Be able to list at least 3 major adverse effects of inhaled medications
A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP October 23, 2017 Learning Objectives Be able to list at least 3 major adverse effects of inhaled medications
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
I have no financial disclosures.
 Palliative Medicine: Year(s) in Review I have no financial disclosures. Lynn A Flint, MD Staff Physician, SFVAMC Assistant Clinical Professor Division of Geriatrics Advances in Internal Medicine 2012 2
Palliative Medicine: Year(s) in Review I have no financial disclosures. Lynn A Flint, MD Staff Physician, SFVAMC Assistant Clinical Professor Division of Geriatrics Advances in Internal Medicine 2012 2
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Overview of COPD INTRODUCTION
 Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
Evidence-based practice of palliative care for patients with chronic chest diseases
 Evidence-based practice of palliative care for patients with chronic chest diseases Dr KS Lau Consultant (Respiratory Med & Palliative Care) Integrated Medical Services RTSKH Hong Kong Palliative Care
Evidence-based practice of palliative care for patients with chronic chest diseases Dr KS Lau Consultant (Respiratory Med & Palliative Care) Integrated Medical Services RTSKH Hong Kong Palliative Care
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
The Role of Palliative Care in Advanced Lung Disease
 The Role of Palliative Care in Advanced Lung Disease Timothy B. Short, MD, FAAFP, FAAHPM Associate Professor, Palliative Medicine University of Virginia Learning Objectives Describe palliative care s approach
The Role of Palliative Care in Advanced Lung Disease Timothy B. Short, MD, FAAFP, FAAHPM Associate Professor, Palliative Medicine University of Virginia Learning Objectives Describe palliative care s approach
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Chapter 7. Anticholinergic (Parasympatholytic) Bronchodilators. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Bronchodilators. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.") Chapter 7 Anticholinergic (Parasympatholytic) Bronchodilators Clinical Indications for Use Indication for anticholinergic bronchodilator COPD maintenance Indication for combined anticholinergic and β-agonist
Chapter 7 Anticholinergic (Parasympatholytic) Bronchodilators Clinical Indications for Use Indication for anticholinergic bronchodilator COPD maintenance Indication for combined anticholinergic and β-agonist
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Chapter 16. Objectives. Objectives. Respiratory Emergencies
 Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
YU DTW, Chan ACM, Poon MWY, Lau PMY. Physiotherapy Departments Kowloon Central Cluster
 YU DTW, Chan ACM, Poon MWY, Lau PMY Physiotherapy Departments Kowloon Central Cluster Prevalence of Ca Lung and COPD Hong Kong Cancer Registry Hospital Authority Annual Report 2012-13 Breathlessness /
YU DTW, Chan ACM, Poon MWY, Lau PMY Physiotherapy Departments Kowloon Central Cluster Prevalence of Ca Lung and COPD Hong Kong Cancer Registry Hospital Authority Annual Report 2012-13 Breathlessness /
Non Pharmacological Breathlessness and Fatigue Management
 Non Pharmacological Breathlessness and Fatigue Management Breathlessness BREATHLESSNESS Breathlessness is the subjective sensation of breathing discomfort that varies in intensity Thoracic Society Dyspnoea-
Non Pharmacological Breathlessness and Fatigue Management Breathlessness BREATHLESSNESS Breathlessness is the subjective sensation of breathing discomfort that varies in intensity Thoracic Society Dyspnoea-
Continuous Intravenous Morphine Infusion for Severe Dyspnea in Terminally Ill Interstitial Pneumonia Patients
 ORIGINAL ARTICLE Continuous Intravenous Mphine Infusion f Severe Dyspnea in Terminally Ill Interstitial Pneumonia Patients Makiko Takeyasu, Atsushi Miyamoto,DaisukeKato 2, Yui Takahashi, Kazumasa Ogawa,
ORIGINAL ARTICLE Continuous Intravenous Mphine Infusion f Severe Dyspnea in Terminally Ill Interstitial Pneumonia Patients Makiko Takeyasu, Atsushi Miyamoto,DaisukeKato 2, Yui Takahashi, Kazumasa Ogawa,
CLINICAL GUIDELINES FOR END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES
 CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Attitudes toward opioids for refractory dyspnea in COPD among Dutch chest physicians
 Original Article Attitudes toward opioids for refractory dyspnea in COPD among Dutch chest physicians Chronic Respiratory Disease 2015, Vol. 12(2) 85 92 ª The Author(s) 2015 Reprints and permission: sagepub.co.uk/journalspermissions.nav
Original Article Attitudes toward opioids for refractory dyspnea in COPD among Dutch chest physicians Chronic Respiratory Disease 2015, Vol. 12(2) 85 92 ª The Author(s) 2015 Reprints and permission: sagepub.co.uk/journalspermissions.nav
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Objectives. Ethical Issues at EOL: Deciding When to Use Oxygen and Antibiotics. Dyspnea. To Palliate 4/28/2014
 Objectives Ethical Issues at EOL: Deciding When to Use Oxygen and Antibiotics Marcia Levetown, MD, FAAHPM HealthCare Communication Associates mlevetown@earthlink.net Understand the evidence based use of
Objectives Ethical Issues at EOL: Deciding When to Use Oxygen and Antibiotics Marcia Levetown, MD, FAAHPM HealthCare Communication Associates mlevetown@earthlink.net Understand the evidence based use of
Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS
 Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS Asthma Usually acquire before the age of 10 These patients exhibit hyper-reactive airways Spasm Constriction Swelling Secretions are
Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS Asthma Usually acquire before the age of 10 These patients exhibit hyper-reactive airways Spasm Constriction Swelling Secretions are
Palliative Care Emergencies. Additional module if needed
 Palliative Care Emergencies Additional module if needed Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline
Palliative Care Emergencies Additional module if needed Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline
Palliative Sedation An ICU Perspective. William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC
 Department of Critical Care Thunder Bay Regional HSC") Palliative Sedation An ICU Perspective William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC Conflict Disclosure Information: Presenter: Dr. Will Anderson I have no financial
Palliative Sedation An ICU Perspective William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC Conflict Disclosure Information: Presenter: Dr. Will Anderson I have no financial
Infectious: (including pericarditis, pleurisy, pneumonia) atypical mycobacterium (MAC) CMV fungi. herpes zoster
 atypical mycobacterium (MAC) CMV fungi. herpes zoster") HIV/AIDS Palliative Care Module CARDIO-RESPIRATORY PROBLEMS homeopathy: coffea 12 ch bid in evening spaced 3 hrs apart before bedtime, allow 4 days to assess, increase to 30 ch, if needed massages relaxation
HIV/AIDS Palliative Care Module CARDIO-RESPIRATORY PROBLEMS homeopathy: coffea 12 ch bid in evening spaced 3 hrs apart before bedtime, allow 4 days to assess, increase to 30 ch, if needed massages relaxation
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Dyspnea Review for the Palliative Care Professional: Treatment Goals and Therapeutic Options
 JOURNAL OF PALLIATIVE MEDICINE Volume 15, Number 1, 2012 ª Mary Ann Liebert, Inc. DOI: 10.1089/jpm.2011.0110 Palliative Care Review Feature Editor: Vyjeyanthi S. Periyakoil Dyspnea Review for the Palliative
JOURNAL OF PALLIATIVE MEDICINE Volume 15, Number 1, 2012 ª Mary Ann Liebert, Inc. DOI: 10.1089/jpm.2011.0110 Palliative Care Review Feature Editor: Vyjeyanthi S. Periyakoil Dyspnea Review for the Palliative
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
The adult with recurrent breathlessness. A/Prof Gerald Chua Medicine NTFGH
 The adult with recurrent breathlessness A/Prof Gerald Chua Medicine NTFGH Dyspnoea Subjective experience of breathing discomfort Variable among individuals with apparently similar degrees of impairment
The adult with recurrent breathlessness A/Prof Gerald Chua Medicine NTFGH Dyspnoea Subjective experience of breathing discomfort Variable among individuals with apparently similar degrees of impairment
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Pulmonary Rehabilitation and Palliative Care. Sindhu Mukku, MD Pulmonary/Critical Care Fellow, PGY-5 February 26, 2013
 Pulmonary Rehabilitation and Palliative Care Sindhu Mukku, MD Pulmonary/Critical Care Fellow, PGY-5 February 26, 2013 Outline 1. Define palliative care and end of life care Palliative Care in COPD 2. Patient
Pulmonary Rehabilitation and Palliative Care Sindhu Mukku, MD Pulmonary/Critical Care Fellow, PGY-5 February 26, 2013 Outline 1. Define palliative care and end of life care Palliative Care in COPD 2. Patient
3. Identify the importance in the prehospital setting for the administration of nebulized bronchodilator.
 TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
Breathlessness in adults: epidemiology, mechanisms and management
 Breathlessness in adults: epidemiology, mechanisms and management AIMS Prof. Miriam Johnson Hertford Building University of Hull Kingston upon Hull HU6 7RU Hull UNITED KINGDOM miriam.johnson@hyms.ac.uk
Breathlessness in adults: epidemiology, mechanisms and management AIMS Prof. Miriam Johnson Hertford Building University of Hull Kingston upon Hull HU6 7RU Hull UNITED KINGDOM miriam.johnson@hyms.ac.uk
Objectives. Pulmonary Assessment 12/13/2017
 Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
EXACERBATION ASSESSMENT FORM
 EXACERBATION ASSESSMENT FORM ID NUMBER: 0a) Form Completion Date... 0b) Staff Code... Administrative Information 1) Date of clinic visit: 2) What type of Event is this?... Participant/HCU-triggered...
EXACERBATION ASSESSMENT FORM ID NUMBER: 0a) Form Completion Date... 0b) Staff Code... Administrative Information 1) Date of clinic visit: 2) What type of Event is this?... Participant/HCU-triggered...
The Respiratory System
 130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
Breathlessness: what we know, and what we don t know
 Breathlessness: what we know, and what we don t know Miriam Johnson Dansk Selskab for Palliativ Medicin 2014 ST CATHERINE S HOSPICE Overview epidemiology impact and assessment management ST CATHERINE S
Breathlessness: what we know, and what we don t know Miriam Johnson Dansk Selskab for Palliativ Medicin 2014 ST CATHERINE S HOSPICE Overview epidemiology impact and assessment management ST CATHERINE S
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
EXACERBATION ASSESSMENT FORM
 EXACERBATION ASSESSMENT FORM ID NUMBER: VERSION: 1.0 05/27/14 0a) Form Completion Date... 0b) Staff Code... Instructions: This form should be completed when a participant comes to the clinical center for
EXACERBATION ASSESSMENT FORM ID NUMBER: VERSION: 1.0 05/27/14 0a) Form Completion Date... 0b) Staff Code... Instructions: This form should be completed when a participant comes to the clinical center for
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Palliative Care Pearls: What Works, What Doesn t
 : Steven Pantilat, MD Kates-Burnard and Hellman Distinguished Professor of Palliative Care Director, Palliative Care Program and Palliative Care Quality Network Department of Medicine University of California,
: Steven Pantilat, MD Kates-Burnard and Hellman Distinguished Professor of Palliative Care Director, Palliative Care Program and Palliative Care Quality Network Department of Medicine University of California,
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
NONOPIOID THERAPY FOR CANCER RELATED DYSPNEA PALLIATION IN THE ED: A RANDOMIZED DOUBLE BLIND CLINICAL TRIAL
 Acta Medica Mediterranea, 2017, 33: 1099 NONOPIOID THERAPY FOR CANCER RELATED DYSPNEA PALLIATION IN THE ED: A RANDOMIZED DOUBLE BLIND CLINICAL TRIAL SERKAN YILMAZ, ELIF YAKA, MELIH YUKSEL, NURETTIN OZGUR
Acta Medica Mediterranea, 2017, 33: 1099 NONOPIOID THERAPY FOR CANCER RELATED DYSPNEA PALLIATION IN THE ED: A RANDOMIZED DOUBLE BLIND CLINICAL TRIAL SERKAN YILMAZ, ELIF YAKA, MELIH YUKSEL, NURETTIN OZGUR
Airway and Breathing
 Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
Symptom Control in Heart Failure. Dr Claire L Hookey
 Symptom Control in Heart Failure Dr Claire L Hookey Heart Failure symptoms Class III/IV CHF, mean 67.1 years, mean EF 22.3% Most prevalent symptoms:- lack of energy (66%) dry mouth (62%) shortness of breath
Symptom Control in Heart Failure Dr Claire L Hookey Heart Failure symptoms Class III/IV CHF, mean 67.1 years, mean EF 22.3% Most prevalent symptoms:- lack of energy (66%) dry mouth (62%) shortness of breath