Evaluating the Heart before Non-Cardiac Surgery
|
|
|
- Roland Thomas
- 5 years ago
- Views:
Transcription
1 Evaluating the Heart before Non-Cardiac Surgery Dr Rob Stephens Anaesthetist UCLH + UCL the centre for Anaesthesia

2 Google UCL Stephens
3 Google UCL Stephens
4 Contents Introduction Basic Principles Guidelines: Decisions Guidelines: Putting it all together Which test? ECHO CPEx B Block? Summary
5 Introduction You re all experts! Seems big, complex Conflicting, absent and changing evidence! Problem: Assessing CVS system vs Lack of effectiveness of interventions
6 Background: Basic Principles Why assess the CVS system? Assess risk: consent + patient decisions Assess risk: specific interventions Diagnose conditions : caution Cancer surgery- time limited Test: what next? Ischaemia vs Heart Failure Probably, reasonable, is not well established
7 Guidelines ACC/AHA guideline revision ACC/AHA 2007 (small revision 2009) ESC 2009 Guidelines - Cardiology Fraud of Poldermans B Blocker story Individual Studies?ASA / RCoA / AAGBI?
8 2014 Guidelines + others MACE Major Adverse Cardiac Event Different Order to risk asses Risk Asses using NSQIP CPEX considered for elevated risk procedures in unknown functional capacity Coronary Stent Guidelines POISE 2 study no benefit in adding aspirin MINS myocardial injury after non-cardiac surgery Troponin uncertain usefulness in high risk patients


9
10 ESC 2009

11 Mythen, Biccard
12 Wait for surgery after MI? Postoperative MI 0-30 days 32.8% days 18.7% days 8.4% days 5.9% 30-day mortality 0-30 days 14.2% days 11.5% days 10.5% days 9.9% Livhits 2011
13 Vascular Surgery CARP 5859 patients screened; 510 selected revascularization vs not Postoperative 30 day mortality 3.1% vs 3.4%, rev vs not; P =.87 Long term mortality 2.8 years 22% vs 24%, rev vs not P =.92 McFalls 2004
14 Guideline 2 ACC AHA Surgery Urgency Patient Specific risks / Comorbidities Surgery Severity Patient Exercise Capacity ESC 2009 Biomarkers
15 Guideline 3 ACC AHA Surgery Urgency Patient Specific risks / Comorbidities Surgery Severity Patient Exercise Capacity ESC 2009 Biomarkers
16 Guideline 4 Surgery Urgency Emergency/ Immediate proceed
17 Urgency AHA 2014 Emergency no/little time limited clinical evaluation life or limb is threatened if no surgery within <6 hours Urgent may be time for a limited clinical evaluation when life or limb is threatened if no surgery within 6-24 Time-sensitive a delay of >1-6 week for evaluation / treatment will negatively affect outcome. Elective the procedure could be delayed for up to 1 year.

18 NCEPOD 2004
19 Guideline 5 Surgery Urgency Truly Elective time to treat / discuss Treat/refer broadly as according to nonpreoperative guidelines warn about possible delay to surgery evidence of benefit for subsequent surgery?
20 Guideline 6 Surgery Urgency (US vs NCEPOD) Cancer = time limited Consider lack of benefit from CVS interventions potential delay after CVS intervention coronary stent anticoagulation
21 Guideline 7 ACC AHA Surgery Urgency Patient Specific risks / Comorbidities Surgery Severity Patient Exercise Capacity ESC 2009 Biomarkers
22 Guideline 8 ACC AHA Patient Risk factors 3 levels: Serious / Intermediate / Minor Serious ; active cardiac conditions Recent MI/Unstable Angina New /Acute Ht Failure Serious abnormal rhythm Severe valve disease Pause and discuss with teams
23 Guideline 8 ACC AHA Patient Risk factors 3 levels: Serious / Intermediate / minor Intermediate - same as Lees rcri or Calculate NSQIP MACE score
24 Lee s rcri revised Cardiac Risk Index Major Surgery and Bowl cutting Pelvic Vascular Ischemic heart disease Cardiac Failure Cerebrovascular disease Diabetes on Insulin Renal insufficiency (>177 μmol / litre) No CVS % % % % Boersma 2005 Lee 1999
25 Guidelines 9 NSQIP Risk Calculator >1%? Think about Preoperative testing IHD If it will change your management
26
27
28 Guideline 10 ACC AHA Surgery Urgency Patient Specific risks / Comorbidities Surgery Severity Patient Exercise Capacity ESC 2009 Biomarkers
29 Guideline 11 Severity of surgery Minor Anything else proceed consider further

30 Assessing CVS disease: Guideline 4 ESC 2009
31 Guideline 12 ACC AHA Surgery Urgency Patient Specific risks / Comorbidities Surgery Severity Patient Exercise Capacity ESC 2009 Biomarkers
32 Guideline 13 Patient Exercise Capacity 4 METS without significant symptoms Operations proceed No Chest Pain No SOB Less than 4 METS consider testing
33 Guideline 14 Patient Exercise Capacity Metabolic Equivalent of Task - MET 1 MET is 0 2 uptake at rest = = 3.5 ml/min/kg 0 2 uptake 2 METS ~ 2x 0 2 uptake of 1 METS Easily Quantified by CPEx Mostly quantified by history
34 Guideline 15 Patient Exercise Capacity 2 MET Strolling 4 MET Fast flat walking, up 1 flight stairs?do everything in a normal day walking a dog, moderate gardening 6+ Most sports, running No Chest Pain No SOB Playing a heavy musical instrument while actively running in a marching band

35 Maximum 3900ml/min 0 2 uptake 82kg 3900/82 =47ml/min/kg 11 3/4 METS Rest 330ml/min 0 2 uptake 82kg 330/82 =4ml/min/kg= 1 MET
36 Guideline 16 ACC AHA Surgery Urgency Patient Specific risks / Comorbidities Patient Exercise Capacity Surgery Severity ESC 2009 Biomarkers
37 Guideline 17 Biomarkers in Guidelines 2009 and 2014 a characteristic that can be objectively measured that is an indicator of pathology or an abnormal response to treatments Troponin - myocardial cell injury BNP + pro NT BNP CRP - myocardial wall stress increases - liver and smooth muscle ESC, Biccard, Devereaux 2012
38 Guideline 18 Biomarkers in ESC Guidelines 2009 Troponin Postop small associated mortality VISION Preop predictive, no ideal cut off BNP + pro NT BNP Ht Failure /IHD / ACS - rises relate to outcome Preop adds predictive ability >48 pg/ml CRP inflammatory marker ESC, Biccard, Devereaux 2012
39 Guideline 19 AHA/ACC 2014 no data to suggest that targeting biomarkers for treatment or intervention will lower postoperative risk. Biomarkers in ESC Guidelines 2009 Higher in patients that have postoperative cardiac events or die Troponin BNP CRP
40 Assessing CVS disease: Together

41 ACC/AHA 2014
42 ACC/AHA 2009
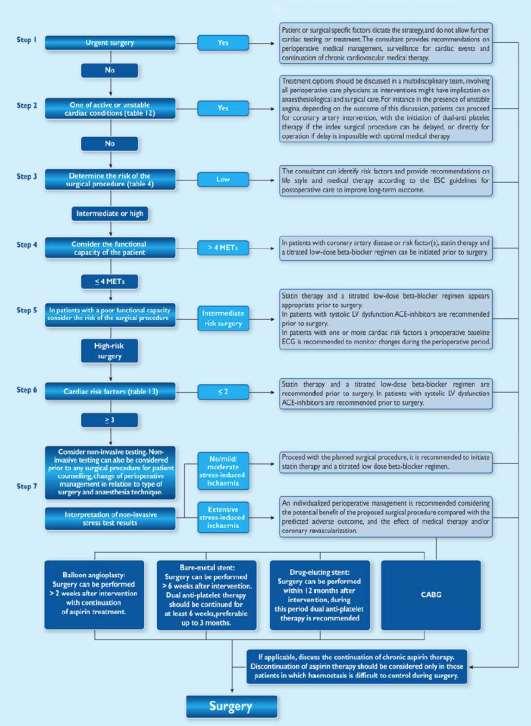
43 ESC 2009
44 Putting it together 1: Urgency Emergency or Urgent operation Time- limited or Elective consider further
45 Putting it together 2: Active Cardiac Condition
46 Putting it together 2: Active Cardiac Condition Serious = active cardiac condition Recent MI/Unstable Angina Acute LVF Serious abnormal rhythm Severe valve disease
47 Putting it together 2: Active Cardiac Condition Putting it together: 2 Active Cardiac Condition Yes Emergency operation and Rx Urgent pause & consider refer Time- limited pause & consider refer Elective pause & refer/ix/rx No Urgent Time- limited Elective consider further
48 Putting it together 3: Patient Risk Factors Patient Risk of MACE > 1%? Lees revised Cardiac Risk Index Any Ischaemic Ht Disease Any Ht Failure Any Cerebro-Vascular Disease Diabetes insulin Renal Injury (Cr 177+) More than 1% Less than 1% consider further proceed with surgery
49 Putting it together 4: Operation risk?low risk surgery Proceed operation Intermediate high consider further
50 Putting it together 5: Exercise capacity Can they do > 4 METS without symptoms probably operation Less than 4 METS or can t tell consider further
51 Putting it together: Investigations Always in the context of what next? ie will/should it change management? Consider testing ACC/AHA Stress ECHO Myocardial Perfusion Scan CPEx includes Exercise ECG Exercise ECG MRI or CT
52 ECHO Evidence Valves, Function, estimates pulmonary pressures Degree of dysfunction, regional wall motion abn LVEF <40% - 2x higher risk sensitivity 43% positive predictive 13% resting LV function was not found to be a consistent predictor of perioperative ischemic events or death But ECHO enthusiasts in preassessment.. 30% new CVS disease, Mx 20% Mx 34% Halm, Rofdhe, Canty
53 ECHO indication Routine Evaluation NO Dyspnea of unknown origin reasonable New murmur - reasonable Ht Failure with symptoms - reasonable Ht Failure clinically stable - may be considered Valves clinically stable - recommended > 1 year ACC/AHA
54 CPEx / CPET Background Functional assessment Population data survival VO 2 peak, AT, VE/VCO 2, ECG ischaemia etc But Associations with outcome and complications Most studies unblinded, small Await results of only RCT Prehabilitation studies- some positives Older, Hennis, Snowden, O Doherty
55 CPEx / CPET Background n=548 Lower anaerobic threshold worse: Raised Respiratory Equivalent: higher mortality higher mortality Mortality AT more 14 ml/min /kg 0% AT more 11 ml/min /kg but other badness 1.7% AT less 11 ml/min /kg 4.6% Older 1999
56 CPEx / CPET Background Complication AT < 10.1 AT > 10.1 p= on day 7 n= 51 n=65 Pulmonary 57% 15% < Renal 40% 11% GI 33% 11% Infective 27% 11% Cardiovascular 25% 3% Neurological 10% 5% 0.29 Hematology 8% Pain 8% Wound 4% Snowden 2010
57 CPEx / CPET use ACC/AHA 2014 considered for patients undergoing elevated risk procedures with unknown functional capacity Awaiting RCT on CPEx vs Dr Use very variable, increasing Best not to emphasise one single value VO 2 peak, AT, VE/VCO 2, ECG ischaemia Enthusiasts vs sceptics
58 B Block? background B blockers in community reduce adrenergic activity + myocardial 0 2 use associated with survival RCT Perioperative studies Mangano POISE DECREASE, Others Observational perioperative data US and European Perioperative Guidelines Mangano, London, Sear, Devereaux, Bouri
59 B Block? ESC 2009
60 Devereaux B Block?: Endpoints important! POISE Lancet patients with/at risk of, atherosclerotic disease non-cardiac surgery B Block 24 hrs preoperatively 30 days postop Metoprolol vs Placebo MI 4 2% vs 5 7% 0 84 p=0 002 Deaths 3 1% vs 2 3% 1 33 p=0 03 Stroke 1 0% vs 0 5% 2 17 p=0 005 BP 15.0% vs. 9.7% p < Bradycardia 6.6% vs. 2.4% p <

61
62
63 B Block Maintain current B Blockade Treat concomitant anaemia Meta-analysis / prospective studies don t support May use in high risk people only Those that may be on B Blockers anyway rcri >1?Atenolol or Bisoprolol Start /titrate bpm?7+ days before
64 VISION : MINS 15,065 patients > 45+ yrs; in-patient non-cardiac surgery MINS myocardial injury after non-cardiac surgery= Troponin T level of > 0.03 ng/ml MINS 30-day mortality 3.87x (adjusted hazard ratio; 95% CI, ) 8.0% had MINS 58.2% of these did not fulfill a conventional MI definition 15.8% of patients with MINS had ischemic symptoms Botto 2014
65 Summary Introduction Basic Principles Guidelines: Decisions Guidelines: Putting it all together Which test? ECHO CPEx B Block? Summary
66 Thank you For listening Please Google stephens UCL for website This full talk Some References AHA/ACC and European Guidelines
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Update on Perioperative Medicine. Update on Perioperative Medicine. Question 1: Clinical Risk Prediction. for the Office-based Practitioner
 Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Guidelines PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42. Prominent Dutch Cardiovascular Researcher Fired for Scientific Misconduct
 PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
Dr Kerry Gunn. Dr Nicola Broadbent. Anaesthesiologist Auckland City Hospital Auckland. Specialist Anaesthetist Auckland City Hospital Auckland
 Dr Kerry Gunn Anaesthesiologist Auckland City Hospital Auckland Dr Nicola Broadbent Specialist Anaesthetist Auckland City Hospital Auckland 8:30-9:25 WS #96: Optimising Patients for Surgery - Defining
Dr Kerry Gunn Anaesthesiologist Auckland City Hospital Auckland Dr Nicola Broadbent Specialist Anaesthetist Auckland City Hospital Auckland 8:30-9:25 WS #96: Optimising Patients for Surgery - Defining
SESSION 5 2:20 3:35 pm
 SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Cardiac Risk Assessment in the Preoperative period
 Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Perioperative Cardiac Management. Emma Sargsyan, MD, FACP
 Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Perioperative Infarcts: Epidemiology, predictors and post-op monitoring
 Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin
 Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin Dr. Vikas Tandon Associate Professor, Cardiology
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin Dr. Vikas Tandon Associate Professor, Cardiology
Preoperative Risk. Geoffrey C Zarrella DO FACC. Assessment
 Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Post Operative Troponin Leak: David Smyth Christchurch New Zealand
 Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver
 Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality
 Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Agenda. Disclosures. Surgical Mortality: What is High Risk?
 Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Value of troponin measurements in carotid artery revascularization
 Value of troponin measurements in carotid artery revascularization Gert J de Borst Department of Vascular Surgery Postoperative myocardial infarction after NCS: Magnitude of the problem POISE-1: 367 /8,351=
Value of troponin measurements in carotid artery revascularization Gert J de Borst Department of Vascular Surgery Postoperative myocardial infarction after NCS: Magnitude of the problem POISE-1: 367 /8,351=
Conflicts of Interest. Evaluation of Cardiac and Pulmonary Risk in the Preop Patient. Introduction. Risk Assessment. Risk Assessment: RCRI
 Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
PRE Operative Care of the High Risk Surgical Patient. Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London
 PRE Operative Care of the High Risk Surgical Patient Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London Perioperative Optimization Shoemaker oxygen delivery goal directed therapy ITS NOT
PRE Operative Care of the High Risk Surgical Patient Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London Perioperative Optimization Shoemaker oxygen delivery goal directed therapy ITS NOT
Cardiac Perioperative Risk Assessment American Heart Association Guidelines
 Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Perioperative Myocardial Infarction
 Perioperative Myocardial Infarction Which patient should UNDERGO CORONARY ANGIOGRAPHY? The Cardiologists view Hans Rickli, St.Gallen 1 Experience Standards Risk stratification Team approach.. Tightrope
Perioperative Myocardial Infarction Which patient should UNDERGO CORONARY ANGIOGRAPHY? The Cardiologists view Hans Rickli, St.Gallen 1 Experience Standards Risk stratification Team approach.. Tightrope
Preoperative tests (update)
") National Institute for Health and Care Excellence. Preoperative tests (update) Routine preoperative tests for elective surgery NICE guideline NG45 Appendix C: April 2016 Developed by the National Guideline
National Institute for Health and Care Excellence. Preoperative tests (update) Routine preoperative tests for elective surgery NICE guideline NG45 Appendix C: April 2016 Developed by the National Guideline
Agenda. Perioperative Cardiac Risk Stratification circa Surgical Mortality: What is High Risk? Presenter Disclosure Information
 9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Peri-operative Troponin Measurements - Pathophysiology and Prognosis
 Peri-operative Troponin Measurements - Pathophysiology and Prognosis Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
Peri-operative Troponin Measurements - Pathophysiology and Prognosis Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
Clinical Controversies in Perioperative Medicine!
 Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
PERIOPERATIVE CARDIAC RISK ASSESSMENT. Divya Gollapudi, MD
 PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW
 PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY
 PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
Controversies in Perioperative Medicine
 Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Perioperative Assessment in the Older Adult. Sondra Vazirani, MD, MPH
 Perioperative Assessment in the Older Adult Sondra Vazirani, MD, MPH The Preoperative Evaluation in the Older Adult Sondra Vazirani, MD, MPH, FACP* 33 rd UCLA Intensive Course in Geriatric Medicine & Pharmacy,
Perioperative Assessment in the Older Adult Sondra Vazirani, MD, MPH The Preoperative Evaluation in the Older Adult Sondra Vazirani, MD, MPH, FACP* 33 rd UCLA Intensive Course in Geriatric Medicine & Pharmacy,
Preoperative cardiac management of the patient for non-cardiac surgery: an individualized and evidence-based approach
 British Journal of Anaesthesia 107 (1): 83 96 (2011) Advance Access publication 24 May 2011. doi:10.1093/bja/aer121 Preoperative cardiac management of the patient for non-cardiac surgery: an individualized
British Journal of Anaesthesia 107 (1): 83 96 (2011) Advance Access publication 24 May 2011. doi:10.1093/bja/aer121 Preoperative cardiac management of the patient for non-cardiac surgery: an individualized
Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center
 Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center Beta-blockers: What s known 30 Years 30 Careers Physician clarity regarding
Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center Beta-blockers: What s known 30 Years 30 Careers Physician clarity regarding
Objectives. Old School. Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction?
 Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Updates & Controversies in Perioperative Medicine
 Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Updates in Perioperative Medicine Estimating mortality in surgical
Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Updates in Perioperative Medicine Estimating mortality in surgical
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL
 COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
Stress Testing:Which Study is Indicated for My Patient?
 Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
D M Y Y Y Y D D M M Y Y Y Y. Previous MI (apart from acute PCI) 0=no 1=yes 9=unknown
 0=no 1=yes 9=unknown") I Patient details and Preoperative Data Date of Informed Consent dd-mm-yyyy (Please leave blank if waived by Ethics Committee) Please enter Patient ID in this format xxx-xx-xxx 3 digit code for the country,
I Patient details and Preoperative Data Date of Informed Consent dd-mm-yyyy (Please leave blank if waived by Ethics Committee) Please enter Patient ID in this format xxx-xx-xxx 3 digit code for the country,
Update in Perioperative Medicine
 Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Preoperative Evaluation of Patients Undergoing Noncardiac Surgery
 Preoperative Evaluation of Patients Undergoing Noncardiac Surgery Shazia Khan, MD Assistant Professor of Clinical Medicine Keck School of Medicine LAC+USC Medical Center Learning Objectives Use a risk
Preoperative Evaluation of Patients Undergoing Noncardiac Surgery Shazia Khan, MD Assistant Professor of Clinical Medicine Keck School of Medicine LAC+USC Medical Center Learning Objectives Use a risk
2010, Metzler Helfried
 Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
SCIP Cardiac Measure. Lee A. Fleisher, M.D.
 SCIP Cardiac Measure Lee A. Fleisher, M.D. fleishel@uphs.upenn.edu Medicare Surgical Infection Prevention (SIP) Project Objective To decrease the morbidity and mortality associated with postoperative infection
SCIP Cardiac Measure Lee A. Fleisher, M.D. fleishel@uphs.upenn.edu Medicare Surgical Infection Prevention (SIP) Project Objective To decrease the morbidity and mortality associated with postoperative infection
PACT module High risk surgical patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module High risk surgical patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Intravascular volume effect of Ringer s lactate Double-tracer BV measurement Blood 1097
PACT module High risk surgical patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Intravascular volume effect of Ringer s lactate Double-tracer BV measurement Blood 1097
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Judicious Use of Preoperative Consultants. Relevant disclosures: None. Preoperative Consultation by Specialists: Overall Impact on Outcome?
 Judicious Use of Preoperative Consultants Changing Practice of Anesthesia Meeting 2014 Relevant disclosures: None Rachel Eshima McKay, MD Professor, Anesthesia and Perioperative Director, UCSF Mount Zion
Judicious Use of Preoperative Consultants Changing Practice of Anesthesia Meeting 2014 Relevant disclosures: None Rachel Eshima McKay, MD Professor, Anesthesia and Perioperative Director, UCSF Mount Zion
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Preoperative Cardiac Risk Calculators
 The Fort Lauderdale, Florida Preoperative Cardiac Risk Calculators Steven L. Cohn, MD, FACP, SFHM Professor Emeritus Director - Medical Consultation Service Jackson Memorial Hospital University of Miami
The Fort Lauderdale, Florida Preoperative Cardiac Risk Calculators Steven L. Cohn, MD, FACP, SFHM Professor Emeritus Director - Medical Consultation Service Jackson Memorial Hospital University of Miami
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
More acute cardiology
 Case 1 RC 86, Male More acute cardiology Dr John Chambers Consultant Cardiologist A&E: SOB at rest. No chest pain. Exertional SOB for 6/12. PMHx: HT Rx: Ramipril 5mg od Examination: Afebrile, HR = 105,
Case 1 RC 86, Male More acute cardiology Dr John Chambers Consultant Cardiologist A&E: SOB at rest. No chest pain. Exertional SOB for 6/12. PMHx: HT Rx: Ramipril 5mg od Examination: Afebrile, HR = 105,
4/27/2015. Cardiac Events #1 cause of postoperative complications/ mortality- CHF, complete heart block, MI,
 Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Anesthesia for Cardiac Patients for Non Cardiac Surgery. Kimberly Westra DNP, MSN, CRNA
 Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
DECLARATION OF CONFLICT OF INTEREST. None
 DECLARATION OF CONFLICT OF INTEREST None How low should we go to avoid harm in hypertensives with comorbidities? CORONARY ARTERY DISEASE Prof. Dr. Maria DOROBANTU, FESC,FACC CARDIOLOGY EMERGENCY HOSPITAL
DECLARATION OF CONFLICT OF INTEREST None How low should we go to avoid harm in hypertensives with comorbidities? CORONARY ARTERY DISEASE Prof. Dr. Maria DOROBANTU, FESC,FACC CARDIOLOGY EMERGENCY HOSPITAL
Pre-operative Evaluations. Objectives. General Considerations. FP Consultation Considerations. CV Credits 7/24/2017. Brian Bachelder, MD Akron, Ohio
 Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
Keywords: Troponins; Vascular surgery; Cardiac risks; Tissue loss; Statins; Biomarkers; Outcomes
 Journal of Critical Care (2012) 27, 66 72 Peak postoperative troponin levels outperform preoperative cardiac risk indices as predictors of long-term mortality after vascular surgery Troponins and postoperative
Journal of Critical Care (2012) 27, 66 72 Peak postoperative troponin levels outperform preoperative cardiac risk indices as predictors of long-term mortality after vascular surgery Troponins and postoperative
ICSS Safety Results NOT for PUBLICATION. June 2009 ICSS ICSS ICSS ICSS. International Carotid Stenting Study: Main Inclusion Criteria
 Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Perioperative Cardiac Risk Assessment & Management for Noncardiac Surgery
 Perioperative Cardiac Risk Assessment & Management for Noncardiac Surgery STEVEN L. COHN, MD, FACP, SFHM PROFESSOR EMERITUS DIRECTOR-MEDICAL CONSULTATION SERVICE JACKSON MEMORIAL HOSPITAL UNIVERSITY OF
Perioperative Cardiac Risk Assessment & Management for Noncardiac Surgery STEVEN L. COHN, MD, FACP, SFHM PROFESSOR EMERITUS DIRECTOR-MEDICAL CONSULTATION SERVICE JACKSON MEMORIAL HOSPITAL UNIVERSITY OF
Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia preope
 Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Heart Failure. Guillaume Jondeau Hôpital Bichat, Paris, France
 Heart Failure Guillaume Jondeau Hôpital Bichat, Paris, France Epidemiology Importance of PEF Europe I-PREFER study. Abstract: 2835 Prevalence of HF Preserved LV systolic Function older (65 vs 62 y, p
Heart Failure Guillaume Jondeau Hôpital Bichat, Paris, France Epidemiology Importance of PEF Europe I-PREFER study. Abstract: 2835 Prevalence of HF Preserved LV systolic Function older (65 vs 62 y, p
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
Medical Apps for Cardiology Uses. There s an App for That!
 Medical Apps for Cardiology Uses There s an App for That! Audience Participation Question #1 1. ASCVD Risk App What is the predicted 10 year CV event rate for a 57 y/o black male patient with treated
Medical Apps for Cardiology Uses There s an App for That! Audience Participation Question #1 1. ASCVD Risk App What is the predicted 10 year CV event rate for a 57 y/o black male patient with treated
Case Challenges in ACS The Very Elderly in the Cath Lab
 Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD
: What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD") Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting
Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr..
 Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Cases in Stress Echo DISCLOSURE
 Cases in Stress Echo Susan Wilansky, MD, FRCP(C), FACC, FASE Mayo Clinic, AZ DISCLOSURE Relevant Financial Relationship(s) None Off Label Usage None 1 Exercise Testing in Patients with HCM (Class IIa)
Cases in Stress Echo Susan Wilansky, MD, FRCP(C), FACC, FASE Mayo Clinic, AZ DISCLOSURE Relevant Financial Relationship(s) None Off Label Usage None 1 Exercise Testing in Patients with HCM (Class IIa)
Preoperative NT-proBNP and CRP predict perioperative major cardiovascular events in non-cardiac surgery
 1 Department of Medicine, Cardiovascular Imaging Center, Cardiac and Vascular Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea; 2 Department of Emergency Medicine,
1 Department of Medicine, Cardiovascular Imaging Center, Cardiac and Vascular Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea; 2 Department of Emergency Medicine,
Perioperative Risk Assessment Do patients really need to be cleared for the OR?
 Perioperative Risk Assessment Do patients really need to be cleared for the OR? Dr. Eric Lindley McKay-Dee Cardiology Adjunct Assistant Professor University of Utah Disclosures Consultant: Abbott vascular
Perioperative Risk Assessment Do patients really need to be cleared for the OR? Dr. Eric Lindley McKay-Dee Cardiology Adjunct Assistant Professor University of Utah Disclosures Consultant: Abbott vascular
A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart.
 November 2016 A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart. He consulted Cardiology. No attempt should be made to prognosticate
November 2016 A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart. He consulted Cardiology. No attempt should be made to prognosticate
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Managing Cardiac & Pulmonary Risk in the Surgical Patient
 Managing Cardiac & Pulmonary Risk in the Surgical Patient Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Preoperative Evaluation Guidelines Cardiac: Fleisher
Managing Cardiac & Pulmonary Risk in the Surgical Patient Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Preoperative Evaluation Guidelines Cardiac: Fleisher
THE HEART OF THE MATTER MAYANNA LUND CMH
 THE HEART OF THE MATTER MAYANNA LUND CMH CARDIOLOGY ASSESSMENT AND WHEN TO REFER CHEST PAIN - ACUTE History Examination: vital signs are vital ECG Troponin Concerns: MI, unstable angina, PE, aortic dissection
THE HEART OF THE MATTER MAYANNA LUND CMH CARDIOLOGY ASSESSMENT AND WHEN TO REFER CHEST PAIN - ACUTE History Examination: vital signs are vital ECG Troponin Concerns: MI, unstable angina, PE, aortic dissection
Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery. A prospective observational study.
 Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery A prospective observational study OBTAIN Study Statistical Analysis Plan of Final Analysis Final Version: V1.1 from
Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery A prospective observational study OBTAIN Study Statistical Analysis Plan of Final Analysis Final Version: V1.1 from
Takotsubo syndrome. Ευτυχία Σμπαρούνη, FACC, FESC
 Takotsubo syndrome Ευτυχία Σμπαρούνη, FACC, FESC Definition Takotsubo Apical ballooning Broken heart syndrome Stress cardiomyopathy Cathecholaminergic cardiomyopathy Epidemiology 1990 first report by Japanese
Takotsubo syndrome Ευτυχία Σμπαρούνη, FACC, FESC Definition Takotsubo Apical ballooning Broken heart syndrome Stress cardiomyopathy Cathecholaminergic cardiomyopathy Epidemiology 1990 first report by Japanese
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Preoperative Evaluation Guidelines and Work up
 Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Beta Blockade: Protection or Panacea
 Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Risk stratification for non-cardiac surgery
 Southern African Journal of Anaesthesia and Analgesia 2018; 24(3)(Supplement 1) Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Southern African Journal of Anaesthesia and Analgesia 2018; 24(3)(Supplement 1) Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Effect of Aliskiren on Postdischarge Outcomes Among Non-Diabetic Patients Hospitalized for Heart Failure: Insights from the ASTRONAUT Outcomes Trial
 Effect of Aliskiren on Postdischarge Outcomes Among Non-Diabetic Patients Hospitalized for Heart Failure: Insights from the ASTRONAUT Outcomes Trial Aldo P. Maggioni, MD, FESC Associazione Nazionale Medici
Effect of Aliskiren on Postdischarge Outcomes Among Non-Diabetic Patients Hospitalized for Heart Failure: Insights from the ASTRONAUT Outcomes Trial Aldo P. Maggioni, MD, FESC Associazione Nazionale Medici
Q: Do cardiac risk stratification indexes
 1-MINUTE CONSULT ROHAN MANDALIYA, MD, FACP Clinical Fellow, Division of Gastroenterology and Hepatology, Department of Medicine, Georgetown University Hospital, Washington, DC GENO MERLI, MD, MACP Professor
1-MINUTE CONSULT ROHAN MANDALIYA, MD, FACP Clinical Fellow, Division of Gastroenterology and Hepatology, Department of Medicine, Georgetown University Hospital, Washington, DC GENO MERLI, MD, MACP Professor
CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE
 CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE SSC Journée d Automne 25 novembre 2010 Dr. Charles Seydoux, spéc. FMH en médecine interne et en cardiologie, Lausanne Dr. Claudia Bösch, Oberärztin Herzinsuffizienz
CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE SSC Journée d Automne 25 novembre 2010 Dr. Charles Seydoux, spéc. FMH en médecine interne et en cardiologie, Lausanne Dr. Claudia Bösch, Oberärztin Herzinsuffizienz
Is there still a place for beta-blockers in perioperative cardioprotection?
 Is there still a place for beta-blockers in perioperative cardioprotection? 14 Michal Horacek Cardiovascular complications, such as hypertension or hypotension, myocardial infarction, left ventricular
Is there still a place for beta-blockers in perioperative cardioprotection? 14 Michal Horacek Cardiovascular complications, such as hypertension or hypotension, myocardial infarction, left ventricular
Copeptin in heart failure: Associations with clinical characteristics and prognosis
 Copeptin in heart failure: Associations with clinical characteristics and prognosis D. Berliner, N. Deubner, W. Fenske, S. Brenner, G. Güder, B. Allolio, R. Jahns, G. Ertl, CE. Angermann, S. Störk for
Copeptin in heart failure: Associations with clinical characteristics and prognosis D. Berliner, N. Deubner, W. Fenske, S. Brenner, G. Güder, B. Allolio, R. Jahns, G. Ertl, CE. Angermann, S. Störk for
I have no disclosures
 Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University