Diagnostic difficulties in inflammatory bowel disease pathology
|
|
|
- Neal Baldwin
- 5 years ago
- Views:
Transcription
1 Histopathology 2006, 48, DOI: /j x REVIEW Diagnostic difficulties in inflammatory bowel disease pathology R K Yantiss & R D Odze 1 Departments of Pathology, Weill Medical College of Cornell University, New York, NY, and 1 Brigham & Women s Hospital, Boston, MA, USA Yantiss R K & Odze R D (2006) Histopathology 48, Diagnostic difficulties in inflammatory bowel disease pathology This review summarizes some of the common diagnostic problems encountered by pathologists when evaluating patients with chronic colitis and in whom inflammatory bowel disease (IBD) is either suspected or within the differential diagnosis. Both ulcerative colitis (UC) and Crohn s disease (CD) show characteristic, but non-specific, pathological features that may overlap and result in a diagnosis of indeterminate colitis (IC). However, other reasons why pathologists may entertain a diagnosis of IC include failure to recognize or accept certain hardcore histological features as indicative of CD, an attempt to classify cases of chronic colitis based on mucosal biopsy material or in the absence of adequate clinical and radiographic information, and the presence of other disease processes that mask, or mimic, IBD. In addition, some cases of UC may show unusual CD-like features, such as discontinuous or patchy disease, ileal inflammation, extracolonic inflammation, granulomatous inflammation in response to ruptured crypts, aphthous ulcers, or transmural inflammation. Furthermore, other forms of colitis, such as microscopic colitis, diverticulitis and diversion colitis may, on occasion, also show IBD-like changes. The clinical and pathological features that aid in the distinction between these entities, and others, are covered in detail in this review. Keywords: chronic colitis, Crohn s disease, indeterminate, ulcerative Abbreviations: CC, collagenous colitis; CD, Crohn s disease; DAC, diverticular disease-associated colitis; IBD, inflammatory bowel disease; IC, indeterminate colitis; IPAA, ileal pouch anal-anastomosis; LC, lymphocytic colitis; UC, ulcerative colitis Introduction In clinical practice, the most common types of inflammatory bowel disease (IBD) are ulcerative colitis (UC) and Crohn s disease (CD). In most instances, these two disorders may be readily distinguished from each other pathologically, particularly when each exhibits classic histological features (Table 1). However, some patients with IBD show overlapping pathological features of UC and CD, which makes definite distinction between these two disorders difficult and often results in an interim diagnosis of indeterminate colitis (IC). In addition, there Address for correspondence: Dr Robert D Odze, Department of Pathology, Brigham and Women s Hospital, 75 Francis Street, Boston, MA 02215, USA. rodze@partners.org are several other types of chronic colitis, such as collagenous colitis (CC), lymphocytic colitis (LC), diverticulitis, and diversion colitis, that, in certain circumstances, may show UC- or CD-like features during the course of illness and, thus, result in diagnostic confusion (Table 2). Finally, some patients who have had an ileal pouch anal-anastomosis (IPAA) procedure for UC develop unusual inflammatory changes in their ileal pouch, such as ulcers, transmural inflammation, fistulae and stenosis, which raise doubt regarding the original diagnosis (presumably UC) and provide evidence for CD. This review addresses some of the challenges associated with interpretation of pathology specimens that demonstrate chronic colitis and provides information that may be helpful in distinguishing these different entities. Ó 2006 Blackwell Publishing Limited.
2 Diagnostic difficulties in IBD pathology 117 Table 1. Classic features of ulcerative colitis and Crohn s disease Feature Ulcerative colitis Crohn s disease Disease distribution Diffuse and continuous Segmental Rectal involvement Always (adults) Occasionally Disease severity Increased distally Patchy and variable Ileal involvement Occasional ( backwash ) Often Disease location in colonic wall Superficial (mucosal) Transmural Transmural lymphoid aggregates Rare, underneath ulcers Any location Fissures Rare, superficial in fulminant colitis Deep, any location Sinuses and fistulas Absent Present Granulomas Related to ruptured crypts Not crypt related Indeterminate colitis general comments and definition Correct classification of patients with IBD who require surgery is important since most with UC are candidates for a total colectomy and an IPAA procedure. This operation creates a functional reservoir while maintaining anal sphincter function. CD is generally considered a contraindication for this operation due to the high risk of severe pouch-associated complications. 1 Unfortunately, approximately 5% (range 1 20%) of IBD cases are difficult to classify as either UC or CD due to the fact that some resection specimens show overlapping histological features. 2,3 Under this circumstance, cases of idiopathic chronic colitis may be temporarily classified as IC until additional clinical, pathological or follow-up data are available. Fortunately, in most cases, the true nature of the underlying colitis often becomes evident later in the course of the patient s disease. For instance, in one study by Meucci et al. approximately 80% of IC cases were ultimately reclassified as either UC or CD within 8 years of follow-up. 4 pathological associations Since IC is not a distinct clinical entity, it has no specific pathological features and, thus, no diagnostic criteria. Historically, the term IC was originally used to describe the pathological findings in colectomy specimens from patients with fulminant colitis, which is a severe form of colitis associated with systemic toxicity and, occasionally, colonic dilation (toxic megacolon). Resection specimens from patients with fulminant colitis often show extensive ulceration that generally affects the transverse and right colon more severely than the distal colon, and often involves more than 50% of the mucosal surface in affected areas. 5 In most cases, the colitis is diffuse and continuous, but some may show either complete, or relative, rectal sparing. Ulcerations are often extensive and may have a fissuring appearance characterized by the presence of knife-like defects that extend into the superficial half of the muscularis propria (Figure 1). These ulcers are also often associated with transmural lymphoid inflammation. The presence of fissuring ulcers may be confusing since this is a feature typically associated with CD. In fact, some authors believe that the presence of fissuring ulcers supports a diagnosis of CD, whereas others regard them as part of the spectrum of severe UC. 3,6 8 In a recent study of 79 UC patients with severe chronic active colitis, Yantiss et al. found that 21 (27%) had superficial fissuring ulcers in their colectomy specimens, but none developed any clinical or pathological features of CD compared with a control group of UC patients without fissuring ulcers. In that study, most patients presented with clinically fulminant disease and all followed a clinical course comparable to that of UC. 9 In another study of 67 patients with fulminant IBD, Swan et al. found that 87% could be accurately classified as either UC or CD based solely upon pathological evaluation of colectomy specimens. In that study, only the presence of granulomas and transmural inflammation in regions of intact mucosa predicted the development of CD. 10 These data show that the natural history of the majority of patients with fulminant colitis is similar to that of UC and, thus, these patients should not be denied the option of an IPAA procedure unless definitive evidence of CD is present elsewhere in the patient. There are a variety of other clinical scenarios in which the diagnostic term IC is used in the general pathology community. These include: (i) failure to Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
 Fulminant colitis Diseases that may mimic IBD Infectious colitis Radiation injury Chronic recurrent ischaemic")
3 118 R K Yantiss & R D Odze Table 2. Conditions that may cause diagnostic confusion with inflammatory bowel disease (IBD) Fulminant colitis Diseases that may mimic IBD Infectious colitis Radiation injury Chronic recurrent ischaemic colitis Other Ulcerative colitis complicated by Cytomegalovirus infection Pseudomembranous colitis Medication effect Other Morphological variants of ulcerative colitis with Crohn s-like features Discontinuous disease Backwash ileitis Upper gastrointestinal tract involvement Granulomas Aphthous and superficial fissuring ulcers Transmural inflammation Crohn s disease with ulcerative colitis-like features Unusual pathological manifestations of other forms of colitis Microscopic colitis with features of IBD Diverticular disease-associated colitis Combined ulcerative colitis or Crohn s disease with diverticular disease Diversion colitis Chronic recurrent pouchitis accept previously reported hardcore criteria as definite evidence in favour of CD; (ii) an attempt by pathologists to establish a diagnosis based on mucosal biopsy specimens; (iii) insufficient clinical and radiological information; and (iv) the presence of other disease processes, such as infections, radiation enterocolitis, or chronic recurrent ischaemia, that can either mimic or mask the features of UC or CD. Finally, failure to recognize unusual manifestations, or morphological variants, of UC and CD may also be a great source of confusion, as discussed below. It is well recognized that the presence of chronic active inflammation of the ileum, transmural lymphoid aggregates in areas underlying intact mucosa, deep Figure 1. Superficial fissuring ulcer in a colectomy specimen from a patient with fulminant ulcerative colitis. The ulcer represents a knife-like vertical defect that extends into the inner half of the muscularis propria. fissuring ulcers that extend into the outer aspects of the muscularis propria, segmental involvement of the colon in a previously untreated patient, and the presence of epithelioid granulomas unassociated with ruptured crypts, are individual features that strongly favour a diagnosis of CD. Unfortunately, recognition of these hardcore features may be difficult, particularly when the findings are limited, or masked, by extensive ulceration. Nevertheless, failure to recognize and accept any of these features as definitive evidence of CD may lead to a potentially erroneous diagnosis of IC. In a study of 119 IBD patients, Farmer et al. showed that most errors in the pathological interpretation of IBD cases result from a failure to recognize the characteristic changes of CD, such as transmural inflammation and granulomas. 3 Some pathologists may be tempted to make a diagnosis of IC based on evaluation of preoperative biopsy specimens. However, this practice should be avoided because of the high potential for diagnostic error. For instance, many cases of UC and CD, particularly those that are limited to the colon, have Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,

4 Diagnostic difficulties in IBD pathology 119 overlapping clinical signs and symptoms. Pathologically, mucosal biopsy specimens are typically superficial in nature and thus provide little information regarding the depth of disease activity, the presence or absence of transmural inflammation, or the type of ulcers present. Unfortunately, the mucosal features of UC and CD are often indistinguishable. In fact, features typically associated with CD, such as relative or absolute rectal sparing, skip areas, and active ileal inflammation, may also occur in UC, as discussed below. Only the presence of epithelioid granulomas unassociated with ruptured crypts and or chronic active ileitis are features highly suggestive of CD on mucosal biopsy analysis. Several other inflammatory disorders, such as certain bacterial or parasitic infections, radiation injury and ischaemia, may mimic the histological appearances of UC or CD in biopsy or resection specimens. For instance, Salmonella or Yersinia infections may cause predominantly right-sided colitis characterized by the presence of mononuclear cell inflammation of the lamina propria associated with basal plasmacytosis, which mimic IBD. Entamoeba histolytica infection may induce mural inflammation, scarring and stricture formation during the resolution phase of colitis. Chronic radiation injury may show mucosal atrophy, pseudopyloric metaplasia, fissures, fibrosis and lymphoid aggregates, which mimic CD. Surgical resection specimens from patients with chronic ischaemia may show mural fibrosis and inflammation associated with patchy, often segmental chronic active mucosal injury, simulating IBD (Figure 2). Finally, the presence of a superimposed secondary disease may mask the true nature of the underlying IBD For example, cytomegalovirus may cause a Figure 2. Colonic resection specimen from a patient with chronic ischaemic colitis. The mucosa shows crypt architectural distortion, such as cystic dilation, branching and atrophy mimicking inflammatory bowel disease. The presence of organized thrombi within multiple serosal blood vessels is a clue to an ischaemic aetiology in this case (insert). flare of inflammation that is segmental and disproportionately severe in the right colon and or ileum, relative to the remainder of the colon in patients with IBD. 11,14 18 Not uncommonly, Clostridium difficileinduced pseudomembranous colitis may also complicate established UC. 19,20 In this situation, the finding of characteristic pseudomembranes and necrotic crypts in areas uninvolved with active IBD may help one suspect that there is a superimposed C. difficile infection. The features of coexistent diverticular disease and IBD are discussed below. natural history and outcome of ic Published data concerning the natural history of IC are variable due to the fact that this group encompasses a heterogeneous population of IBD patients including, but not limited to, those with UC or CD. Although most IC cases are likely to represent unusual examples of UC, 10 40% of IC cases ultimately prove to be CD. Furthermore, most studies that have evaluated the natural history and or outcome of IC were retrospective in design and utilized non-standardized diagnostic criteria. 2,4,10,21 26 Nevertheless, the overall risk of complications for IC patients who have undergone an IPAA procedure is approximately 20%, which is intermediate between that of patients with either UC (10%) or CD (30 40%). 21,23,27,28 In one study of 82 IC patients who underwent an IPAA procedure, 17% developed pelvic sepsis, 31% developed pouch fistulas, and 27% had a pouch failure, compared with 7%, 9% and 11% of patients with definite UC, respectively. In that study, 15% of the IC patients were ultimately reclassified with CD and, when these patients were removed from the analysis, the outcomes of IC and UC patients were comparable. 2 Similarly, Gramlich et al. evaluated 115 IC cases, which were further subclassified into those with a favoured diagnosis of UC, CD or neither of these diagnoses. They found that only IC cases with deep ulcers suggestive of CD developed unequivocal CD, pelvic abscesses or complex fistulas and none of the patients who lacked these ulcers was at increased risk for pouch failure compared with patients with UC. 29 Morphologic variants of UC There are several circumstances in which the classic morphological features of UC (noted in Table 1) may be altered or entirely absent. For example, some UC cases may show discontinuous or patchy disease, absolute or relative rectal sparing, inflammatory changes in the ileum ( backwash ileitis), extracolonic involvement, Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
5 120 R K Yantiss & R D Odze granulomatous inflammation, aphthous ulcers or mural inflammation. Naturally, the presence of these CD-like features may cause diagnostic confusion, or raise the possibility of IC if noted in a resection specimen. 3,6,7 discontinuous disease Although UC is normally a disease that affects the colon in a diffuse and continuous manner, there are several situations in which UC may appear as a discontinuous disease with either patchy or segmental involvement of the colon These include: (i) the tissue healing effect of topical or oral medical therapy, including the quiescent phase of mild chronic UC; (ii) the initial pretreatment presentation of UC in paediatric patients; and (iii) the rare instances in which left-sided UC is associated with either right-sided colonic involvement (with sparing of the transverse colon) or appendiceal involvement. For example, in a prospective controlled study by Odze et al. that evaluated the effects of enema therapy on the rectal biopsy morphology in UC, 36% of the study patients were found to have histologically normal appearing rectal biopsies, compared with 12% of control patients who received placebo enemas (P ¼ 0.005). 33 These results have since been corroborated and expanded by several other studies, which have shown that up to 60% of UC patients who receive either oral sulfasalazine and or steroids, or 5-ASA enemas, show complete reversal of morphological features of activity or chronicity in their colonic biopsies In contrast to adults, children who present initially, prior to treatment, with UC may demonstrate patchy involvement and or absolute or relative rectal sparing in their colonic biopsies. 31,38,39 In one controlled study of 73 paediatric and 38 adult patients with initial onset of UC, 26% of children had either relative or absolute rectal sparing and 21% had microscopic patchy disease at initial presentation, compared with 0% and 0% of adults, respectively. 32 In another study, Washington et al. showed that 32% of previously untreated paediatric UC patients showed only mild architectural features of chronic colitis in their initial colonic mucosal biopsies, compared with 58% of adult patients. 40 Rarely, UC patients may present with limited leftsided proctosigmoiditis and either caecal or ascending colonic involvement, but with sparing of the transverse colon This finding is often referred to as a caecal patch even though the right colon may also be involved. Although some have suggested that this pattern of involvement usually progresses to pancolitis, others have not found this to be the case. For example, in a study of 12 UC patients with proctosigmoiditis, sparing of the transverse colon and right-sided colitis, Mutinga et al. did not identify any association between this finding and the risk of subsequent pancolitis, development of CD or overall disease severity compared with a study group of 35 UC patients with limited leftsided colitis. 47 Finally, appendiceal involvement as a skip lesion in UC is relatively common, occurring in up to 86% of cases. 41,43 In fact, some investigators have suggested that the vermiform appendix plays an immunomodulatory role in UC Interestingly, a recent study demonstrated an association between the presence of appendiceal inflammation and the development of pouchitis among patients with UC. 59 backwash ileitis In contrast to CD, UC does not typically involve noncolonic areas of the gastrointestinal (GI) tract. However, it is commonly believed that, in some circumstances, severe colonic disease may lead to incompetence of the ileocaecal valve that may result in retrograde flow of colonic contents into the distal ileum and inflammation, which is often referred to as backwash ileitis. 60,61 Until recently, this proposed theory of ileal involvement in UC has never been tested. In a recent retrospective study of 200 consecutive UC patients, the prevalence rate of inflammatory changes in the ileum was 17%. In most cases (88%), inflammatory changes consisted of a mild degree of neutrophilic inflammation in the lamina propria, which was often patchy in distribution and occasionally associated with focal cryptitis, crypt abscesses and a mild degree of villous atrophy and regenerative epithelial changes. Rarely, inflammation of the ileum was associated with superficial mucosal ulceration and pseudopyloric metaplasia. However, other features normally associated with CD, such as submucosal inflammation, granulomas and deep fissuring ulcers, did not occur in any of the UC cases in that study. Interestingly, a minority of cases showed a lack of involvement of the caecum or ileocaecal valve and patchy involvement of the distal ileum. The authors suggested that, although the patterns of involvement of the ileum in UC are consistent with a backwash aetiology in the majority of instances, their data provided evidence that other non-backwash factors, such as infections, drug reactions, bacterial overgrowth, bowel preparatory effect, or perhaps primary involvement of the ileum in UC, should also be considered in the pathogenesis of ileal inflammation Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
 mild, superficial and confined to the distal 2 3 cm of ileum, and (ii) occur in a")
6 Diagnostic difficulties in IBD pathology 121 in UC. 62 Thus, inflammation in the ileum may be considered part of the spectrum of UC if the inflammatory changes are (i) mild, superficial and confined to the distal 2 3 cm of ileum, and (ii) occur in a patient in whom all of the clinical, radiological and pathological features support a diagnosis of UC. upper gi tract involvement in uc Historically, as mentioned above, the presence of inflammation in extracolonic sites within the GI tract (with the exception of the biliary tract and or liver in primary sclerosing cholangitis) has been considered strong evidence in favour of a diagnosis of CD. However, this dogma has recently been challenged by the publication of several case reports and small series suggesting that, rarely, UC patients may develop inflammatory and or ulcerative disease in the stomach, duodenum or jejunum For example, Valdez et al. described four patients with classic UC-like changes in the colon who also had chronic active duodenitis characterized by diffuse mononuclear cell infiltration of the lamina propria, crypt branching and atrophy, villous shortening, cryptitis, crypt abscesses and ulceration. 64 The results of this and other small case series highlight the rare possibility of upper GI tract involvement in UC. However, until long-term follow-up information is available, pathologists should be cautious in regarding gastric or duodenal inflammation as part of the spectrum of UC, since other coexistent diseases also may involve the upper GI tract in UC. granulomas in uc Approximately 30 40% of CD cases contain either mucosal, or mural, non-necrotic granulomas. 7,78,79 Epithelioid granulomas represent one of the few features that, when present in mucosal biopsies, may aid in the distinction between UC and CD In addition, in one recent study by Yantiss et al. colonic biopsies from CD patients showed significantly increased numbers of mucosal macrophages and microgranulomas, defined as loose clusters of CD68+ macrophages identifiable only in immunostained slides, and it was suggested that this feature may also be useful in the distinction between UC and CD. 83 Unfortunately, granulomas associated with ruptured crypts, or extravasated mucin, occur commonly in UC as well as in other non-ibd forms of colitis and may, on occasion, be difficult to distinguish from CD In these instances, multiple tissue levels can often help demonstrate the relationship between granulomatous Figure 3. In contrast to the granulomas in Crohn s disease, crypt rupture-related granulomas are often composed of a mixture of neutrophils, lymphocytes, histiocytes and extravasated mucin. inflammation and crypt epithelium. Furthermore, granulomas associated with ruptured crypts frequently contain an admixture of neutrophils and lymphocytes, in addition to foamy macrophages and multinucleated foreign body-type giant cells, which are not usually seen in CD-related granulomas (Figure 3). aphthous ulcers in uc Aphthous ulcers, which are defined as mucosal erosions or shallow ulcers overlying lymphoid aggregates, are common in CD, particularly in the terminal ileum and proximal colon. 87 However, they may also occur in association with UC, although studies designed specifically to address the frequency and significance of this finding in this disorder have not been performed. Nevertheless, in a recent study of 65 UC patients designed to evaluate histological predictors of pouchitis in UC, Yantiss et al. identified aphthous-type ulcers in 17% of colectomy specimens. In that study, none of the patients developed any manifestations of CD, nor was the presence of aphthous ulcers associated with the subsequent development of pouchitis. 59 transmural inflammation Transmural lymphoid aggregates are present in most cases of CD involving the ileum, but are less frequently encountered in the colon. In CD, transmural lymphoid aggregates may occur randomly in the wall of the bowel. Occasionally, mural mononuclear cell inflammation may be present in UC as well, particularly when superficial fissuring ulcers that extend into the deep submucosa or superficial Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
7 122 R K Yantiss & R D Odze muscularis propria are present, or in the setting of toxic megacolon when myocyte necrosis and serosal inflammation are prominent. However, in contrast to CD, mural inflammation in UC is typically not in the form of discrete lymphoid aggregates and usually underlies areas of severe ulceration. 29,88 Thus, lymphoid aggregates in areas under intact mucosa are not a feature of UC and, in fact, favour a diagnosis of CD. CD with UC-like features Approximately 50% of CD patients have colonic involvement and nearly 20% develop colitis without involvement of the oesophagus, stomach or small intestine. Unfortunately, many of the classic features of CD, such as transmural inflammation, strictures and fistulous tracts occur less commonly in the colon. Thus, some cases of CD of the colon may mimic UC by demonstrating only superficial mucosal involvement without inflammatory changes in the submucosa or muscularis propria, diffuse and continuous disease, or even pancolitis In this situation, evaluation of mucosal biopsy samples of the distal ileum and colon for evidence of other hardcore features of CD, combined with correlation with the clinical and endoscopic features of the patient (such as upper GI tract involvement), may help establish an accurate diagnosis. Microscopic colitis and IBD The term microscopic colitis refers mainly to two distinct clinicopathological entities: collagenous colitis (CC) and lymphocytic colitis (LC). 94,95 Briefly, these disorders show characteristic histological features in conjunction with a clinical syndrome consisting of chronic watery diarrhoea and normal endoscopic findings. 96,97 In CC, the histological changes tend to be expressed more dramatically in the transverse and proximal colon compared with the rectum, and are characterized by: (i) the presence of a mixed inflammatory infiltrate composed predominantly of lymphocytes and plasma cells, combined with a variable number of eosinophils within the lamina propria; (ii) infiltration of the crypt and surface epithelium by lymphocytes; (iii) epithelial injury characterized by mucin depletion and flattening of the surface epithelium; (iv) expansion of the subepithelial collagen table (> 10 lm); and (v) relative preservation of crypt architecture LC is histologically similar to CC, with the exceptions that eosinophils are usually less prominent and the subepithelial collagen layer is not thickened. 96, Rarely, distinction between CC or LC and either UC or CD may be difficult and this may be due to a variety of reasons. For example, histological patterns of CC or LC, such as thickening of the subepithelial collagen layer, may occasionally be present in isolated mucosal biopsies from patients with established CD or UC. 118 In fact, in some cases of IBD, initial biopsies may only show features of CC or LC. 100, Pokorny et al. reported the clinical and pathological features of two patients with CC who ultimately developed classical manifestations of UC upon follow-up. 122 In another recent study, Goldstein et al. reported four patients who each had mucosal biopsy findings consistent with either CC or LC, but who later developed characteristic features of CD, such as chronic ileitis, segmental colitis or perianal disease. 123 However, in these instances it remains unclear whether affected patients had CC or LC initially, which subsequently evolved into IBD, or whether the initial manifestations of IBD simply had the pathological features of CC or LC in isolated biopsy samples. In fact, in a retrospective study that evaluated the clinical course of 199 LC patients, none developed any evidence of IBD upon follow-up. 124 It has also now become clear that a small proportion of patients with microscopic colitis may show gross mucosal and or endoscopic abnormalities and histological features that mimic IBD. For example, in one large retrospective study of 79 CC and 71 LC patients, nearly one-third in each group had abnormal endoscopic findings, such as mucosal erythema, mucosal friability and or ulceration. Furthermore, features normally associated with IBD, such as cryptitis, crypt abscesses, architectural distortion or Paneth cell metaplasia, were present, at least focally, in 25%, 5%, 8% and 44% of CC and 35%, 3%, 4% and 14% LC cases, respectively (Figure 4a). 125 Saurine et al. reported the findings of four patients with microscopic colitis, all of whom had non-necrotic granulomas within the lamina propria, but without any evidence of CD during the follow-up period. 126 Rare cases of CC and LC have also been reported to show multinucleated giant cells in the lamina propria. 127 In addition, CC or LC patients may show ileal abnormalities, such as intraepithelial lymphocytosis, villous blunting and subepithelial collagen deposition. 128,129 Others have noted pseudomembranes in well-established cases of CC, in the absence of C. difficile infection, and suggested that this type of injury may be seen as a complication of microscopic colitis, perhaps as a response to antibiotic therapy (Figure 4b) In another study, Kakar et al. found that 78% of the CC patients with mucosal ulcers had a history of non-steroidal anti-inflammatory drug Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
.")

8 Diagnostic difficulties in IBD pathology 123 A diverticulitis may also be at increased risk to develop IBD B Figure 4. Some cases of collagenous colitis may show features of inflammatory bowel disease such as crypt branching (A). Surface ulceration and even pseudomembranous exudates may be present, particularly in patients who have been treated with antibiotics (B). (NSAID) use compared with 20% of CC patients without ulcers. 133 Thus, awareness of the ever-expanding constellation of pathological findings that may be seen in CC or LC may help pathologists establish a correct diagnosis in diagnostically difficult cases (Table 3). Diverticular disease-associated colitis and its relationship to IBD general comments For unknown reasons, some patients with diverticulosis of the sigmoid colon develop either asymptomatic, or symptomatic, chronic colitis in the interdiverticular luminal mucosa, termed diverticular disease-associated colitis (DAC). 134,135 In addition, diverticulosis is a relatively common disease of the elderly and, thus, both diverticulosis and IBD (either CD or UC) may coexist in the same patient. Finally, it has also recently been recognized that patients with colonic diverticulosis and either pre-existing UC or CD are at increased risk of developing diverticulitis. Conversely, patients with pathological features and differential diagnosis Pathologically, DAC is often characterized by mucosal erythema, friability and ulceration similar to that seen in UC of the sigmoid colon. The changes are typically more pronounced at the edges of diverticular orifices, but this is presumably related to the additive effect of mucosal prolapse-induced injury. Histologically, the features of DAC are variable but, in severe cases, the mucosa may appear similar to established UC, except that the rectum is normally uninvolved (Figure 5) Crypt architectural distortion, increased mixed inflammation of the lamina propria, cryptitis, crypt abscesses, Paneth cell metaplasia and basal plasmacytosis are usually present in the mucosa, to some degree, in all patients with DAC. In addition, CD-like features such as transmural inflammation, fibrosis, fissuring ulceration and granuloma formation may also be present in areas of diverticulitis. 136,149,150, Thus, DAC and UC may be indistinguishable based purely on morphological analysis of biopsy specimens. 155 However, knowledge of the distribution of the disease, particularly with regard to rectal involvement, often helps separate these two disorders since most adults with untreated UC have rectal involvement, whereas this is an uncommon finding in DAC. Unfortunately, several studies have documented cases of DAC of the sigmoid colon that subsequently evolved into classic UC, with rectal involvement. 138 In this instance, it is unclear if DAC and UC coexisted from the onset, or whether the former disorder induced the latter by creating a luminal environment, characterized by faecal stasis and bacterial overgrowth, inducive to the development of UC in a genetically susceptible individual. Distinction between DAC and CD is often more difficult. Up to 50% of CD patients also have diverticulosis, and some studies suggest that coexistence of these two diseases may, in fact, worsen the prognosis compared with patients who have either of these disorders in isolation. Unfortunately, complicated diverticular disease may mimic CD because both conditions may reveal mural inflammatory changes, such as transmural inflammation, fissuring ulcers and granulomas, the latter of which may be associated with vascular spaces similar to those described in CD. 138, In fact, some studies have shown that most patients who are thought to have coexistent CD and DAC simply represent cases of complicated Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
 Rare ulcers Segmental or diffuse erythema,")
9 124 R K Yantiss & R D Odze Feature Microscopic colitis Inflammatory bowel disease Clinical presentation Watery diarrhoea Malabsorptive or bloody diarrhoea ± systemic signs Table 3. Clinical and pathological features of microscopic colitis and inflammatory bowel disease Endoscopic appearance Normal or mildly abnormal (erythema) Rare ulcers Segmental or diffuse erythema, friability Ulcers common Pathological findings Mononuclear cell Stromal and intraepithelial Predominantly stromal inflammation Cryptitis crypt abscesses Rare and focal Common and abundant Ulceration Rare and focal Common, occasionally extensive Paneth cell metaplasia Uncommon Usually present Basal plasmacytosis Rare Usually present Basal lymphoid aggregates Rare Usually present Crypt distortion Uncommon, focal Usually present and multifocal or diffuse Granulomas Rare Present in Crohn s disease (crypt rupture-related in ulcerative colitis) Figure 5. Colonic resection specimen from a patient with diverticular disease-associated colitis. The mucosa has a diffuse increase in mononuclear cell inflammation of the lamina propria, basal lymphoplasmacytosis, Paneth cell metaplasia, crypt architectural distortion and crypt abscesses features that resemble Crohn s disease or ulcerative colitis. diverticulitis upon follow-up. 159 In a study of 25 patients with DAC, Goldstein et al. detected transmural inflammation, sinus tracts, lymphoid aggregates, serosal exudates and fissuring-type ulcers in all cases, as well as epithelioid granulomas and lymphohistiocytic vasculitis in 83% and 90% of cases, respectively. None of the patients in that study had a history of CD prior to colonic resection and only two (8%) developed classic features of CD in the small intestine and or perianal region during the follow-up period. 158 In another study by Burroughs et al. of eight cases of DAC, all cases showed transmural lymphoid aggregates, 88% showed epithelioid granulomas, and 38% showed granulomatous vasculitis, but none of the patients developed CD in the follow-up period. 157 Thus, distinction between these two disorders usually necessitates evaluation of the patient for collateral evidence of CD, such as the presence or absence of ileal or upper GI tract involvement, and segmental involvement of the colon, as evidence in favour of CD rather than DAC. Furthermore, in a limited sigmoid colonic resection, the finding of CDlike features, such as transmural inflammation, fissures and or granulomas in areas distant from inflamed diverticula, is helpful in supporting a diagnosis of combined CD and diverticular disease. Diversion colitis general comments Diversion colitis is a chronic inflammatory disorder that develops in segments of bowel that have been excluded Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,

10 Diagnostic difficulties in IBD pathology 125 from the faecal stream, such as a Hartmann s pouch. The condition usually develops within a few months to several years following surgical diversion, and typically regresses completely within 3 6 months of re-establishment of the faecal stream. 160,161 Most patients with this condition are asymptomatic; however, patients with severe colitis may complain of mucoid or bloody discharge, cramping or abdominal pain. 162 The aetiology of diversion colitis is essentially unknown, but there is some evidence to suggest that it results from a deficiency in short-chain fatty acids, which are normally derived from fermentation of dietary starches by the colonic flora. 163,164 Thus, the definitive form of treatment for this condition consists of re-establishment of the continuity of the faecal stream through the diverted segment. pathological features and differential diagnosis The pathological features of diversion colitis, particularly if severe, closely resemble those of UC and CD and include mucosal erythema, friability, nodularity and ulceration All segments of diverted bowel show, at minimum, a mild to moderate degree of lymphoid hyperplasia, characterized by prominent lymphoid aggregates with germinal centres involving the mucosa and or submucosa. In these areas, the crypts may appear atrophic (shortened) or distorted. Symptomatic patients typically show superimposed cryptitis, crypt abscesses and superficial aphthous-type erosions or frank ulceration, on a background of intense lymphoid hyperplasia. More pronounced degrees of crypt architectural distortion as well as other features of chronicity, such as Paneth cell metaplasia, and increased lymphoplasmacytic infiltration of the lamina propria may be present as well (Figure 6). 161, In fact, diversion of the faecal stream may accelerate, or exacerbate, the underlying IBD. 175,176 In addition, both mural and mucosal based nonnecrotic epithelioid granulomas, and even fissuringtype ulcers, have been reported to occur in diverted segments of colon from patients without a prior history of CD, as well as in patients with UC For example, Warren et al. found transmural inflammation (60%), fissuring ulcers (53%) and epithelioid granulomas (27%) in diverted rectal stump resection specimens from 15 patients with a prior history of UC. 177 Similarly, in a study of 82 consecutive IBD patients who underwent resection of their defunctioned rectum, Asplund et al. found mural lymphoid inflammation in patients with either UC or CD. 180 Thus, distinction of diversion colitis from either UC or CD in the diverted Figure 6. Typical biopsy appearance of diversion colitis. It is characterized by the presence of prominent reactive lymphoid aggregates, dense mononuclear cell infiltration of the lamina propria often associated with basal plasmacytosis, mild crypt distortion and atrophy. Features of activity, such as cryptitis, crypt abscesses or aphthous ulcers may also be present in symptomatic cases. segment of colon in patients with pre-existing UC or CD may be difficult, and, whenever possible, surgeons should be reminded to obtain mucosal biopsies of the segment of colon to be diverted from the faecal stream prior to surgery in order to obtain a baseline analysis of the status of this area of the colon. In a study of 16 CD patients, each of whom had normal sigmoidoscopic examination at the time of colonic diversion, Korelitz et al. found that all developed progressive mucosal friability and ulceration and some (25%) developed strictures in the diverted colonic segment. However, patients in whom the faecal flow was restored to the diverted segment subsequently showed a normal endoscopic appearance. The authors concluded that most of the inflammatory changes that occur in diverted colonic segments from IBD patients probably represent diversion colitis rather than IBD. 160 Segments of bowel involved with UC that are subsequently diverted from the faecal stream will often Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
11 126 R K Yantiss & R D Odze show marked lymphoid hyperplasia as an expression of diversion related changes superimposed on the underlying UC. Some cases may also show exacerbation of the degree of activity and ulceration as well. Unfortunately, some patients may ultimately require a test restoration of the faecal flow in order to determine, with complete certainty, the true nature of the inflammatory response in the excluded segment of bowel. In this scenario, improvement of the colitis is evidence in favour of diversion as the cause of illness, whereas a lack of improvement in the previously diverted segment usually indicates an underlying IBD. Pouchitis general comments and clinical features Up to 50% of UC patients who undergo an IPAA procedure develop at least one episode of symptomatic inflammation of their pouch mucosa, termed pouchitis, within the first year after surgery. Pouchitis is categorized as either acute (duration < 4 weeks) or chronic (duration > 4 weeks), and the pattern is further classified as intermittent (one to two episodes of acute pouchitis), relapsing (three or more acute episodes), continuous or treatment-refractory The aetiology of pouchitis is unknown. However, it probably results from an immune-mediated injury that occurs in genetically predisposed individuals Specific pathological predictors of pouchitis include the presence of colonic superficial fissuring ulcers, severe appendiceal inflammation, and severe pancolitis. 59, Approximately 12% of patients develop medically refractory pouchitis that may require immunosuppressive therapy or, ultimately, surgical resection of the pouch. 183,185,186,196, Patients with refractory pouchitis may show IBD-like manifestations, such as pouch fistulas, stenosis and anal fissures or fistulas, that raise the possibility of CD as the primary cause of the patient s illness. pathological features The diagnosis of pouchitis is based on a combination of specific clinical, endoscopic and pathological features ,197,215, The histological diagnosis of pouchitis relies on the identification of active inflammation in the lamina propria and crypt epithelium, either with or without ulceration. Mucosal erythema or ulceration overlying suture lines may also be present, but these features have been shown in most instances to represent a consequence of the surgical procedure. 228 Importantly, although chronic changes, such as architectural distortion and pseudopyloric metaplasia, are more common in the pouch mucosa of patients with clinical pouchitis, a mild degree of architectural distortion, villous shortening and increased chronic inflammation of the lamina propria develops shortly after surgery in virtually all cases and is believed to represent an adaptive form of colonic metaplasia in response to the new luminal environment. 229 Unfortunately, some patients with treatmentunresponsive pouchitis may develop clinical and pathological complications that closely mimic CD. These include proximal strictures, pouch stenosis or fistulas, perianal fissures or fistulas, and even some extraintestinal manifestations of IBD, such as iridocyclitis, arthritis and pyoderma gangrenosum. 22,196,202,207,214,216,227,228, In these settings, pathologists may be tempted to question the validity of their original diagnosis (presumably UC) and entertain the possibility of CD instead. Further complicating the matter is the fact that some patients with CD are subjected to an IPAA procedure because the initial diagnosis of UC was incorrect. In an effort to address these issues, Goldstein et al. evaluated eight cases of presumed UC who developed one or more of the abovementioned complications after an IPAA procedure. They found that the histological findings in the patient s original colectomy specimen were indistinguishable from those of UC patients who did not develop complications following an IPAA procedure, and thus concluded that Crohn s-like complications probably result from chronic pouchitis and do not necessarily represent a mistaken diagnosis of UC. 228 In another study, Subramani et al. blindly reviewed colectomy specimens from 15 patients with treatmentrefractory pouchitis and did not find any pathological features that reliably distinguished these cases from UC patients who did not develop this complication. 230 IPAA procedures are occasionally performed in CD patients. In this situation, distinguishing between CD (in patients in whom the original diagnosis was felt to be UC) and CD-like complications in confirmed UC patients may be difficult. Some investigators have shown that the presence of inflammation and or ulceration in the afferent limb of intestine located proximal to the pouch often represents recurrent CD. 229,230,234 Wolf et al. evaluated mucosal biopsies from both the pouch and proximal limb mucosa from 87 IBD patients who had a colectomy followed by an IPAA procedure. Twenty-seven patients were classified as CD, which was determined retrospectively upon re-review of the colectomy specimens and or the development of CD-related complications after IPAA for presumed UC. They found that afferent limb ulcers Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
12 Diagnostic difficulties in IBD pathology 127 were present in 45% of patients who were ultimately confirmed to have CD, compared with only 14% of UC patients. Interestingly, all of the UC patients with proximal limb ulcers also had been taking NSAIDs. 234 Finally, some pathologists have noted, anecdotally, that the presence of non-necrotic epithelioid granulomas unassociated with ruptured crypts may be seen in ileal pouch biopsies from patients with established UC and does not necessarily imply CD. However, the only study that evaluated the significance of this finding in pouch mucosa found that most affected patients were subsequently reclassified as CD, based upon re-review of the colectomy specimens and upon follow-up. Unfortunately, this study was published only in abstract form. 235 Thus, in difficult diagnostic situations, a careful review of all of the patient s clinical, endoscopic and previous biopsy or resection pathology material may help resolve the issue. References 1. Braveman JM, Schoetz DJ Jr, Marcello PW et al. The fate of the ileal pouch in patients developing Crohn s disease. Dis. Colon Rectum 2004; 47; Yu CS, Pemberton JH, Larson D. Ileal pouch-anal anastomosis in patients with indeterminate colitis: long-term results. Dis. Colon Rectum 2000; 43; Farmer M, Petras RE, Hunt LE et al. The importance of diagnostic accuracy in colonic inflammatory bowel disease. Am. J. Gastroenterol. 2000; 95; Meucci G, Bortoli A, Riccioli FA et al. Frequency and clinical evolution of indeterminate colitis: a retrospective multi-centre study in northern Italy. GSMII (Gruppo di Studio per le Malattie Infiammatorie Intestinali). Eur. J. Gastroenterol. Hepatol. 1999; 11; Odze RD. Pathology of indeterminate colitis. J. Clin. Gastroenterol. 2004; 38; S Geboes K. Crohn s disease, ulcerative colitis or indeterminate colitis how important is it to differentiate? Acta Gastroenterol. Belg. 2001; 64; Goldman H. Ulcerative colitis and Crohn s disease. In Ming S, Goldman H eds. Pathology of the gastrointestinal tract. Baltimore: Williams & Wilkins 1998; Odze RD. Diagnostic problems and advances in inflammatory bowel disease. Mod. Pathol. 2003; 16; Yantiss RK, Farraye FA, O Brien MJ et al. Prognostic significance of superficial fissuring ulceration in patients with severe indeterminate colitis. Am. J. Surg. Pathol. 2005; in press. 10. Swan NC, Geoghegan JG, O Donoghue DP et al. Fulminant colitis in inflammatory bowel disease: detailed pathologic and clinical analysis. Dis. Colon Rectum 1998; 41; Hommes DW, Sterringa G, van Deventer SJ et al. The pathogenicity of cytomegalovirus in inflammatory bowel disease: a systematic review and evidence-based recommendations for future research. Inflamm. Bowel Dis. 2004; 10; Pokorney BH, Nichols TW Jr. Pseudomembranous colitis. A complication of sulfasalazine therapy in a patient with Crohn s colitis. Am. J. Gastroenterol. 1981; 76; Torres J, Bannura G, Pisano R. [Toxic megacolon secondary to ischemic colitis. Report of a case]. Rev. Med. Chil. 1996; 124; Hookey LC, Depew W, Boag A et al. 6-mercaptopurine and inflammatory bowel disease: hidden ground for the cytomegalovirus. Can. J. Gastroenterol. 2003; 17; Kambham N, Vij R, Cartwright CA et al. Cytomegalovirus infection in steroid-refractory ulcerative colitis: a case control study. Am. J. Surg. Pathol. 2004; 28; Kishore J, Ghoshal U, Ghoshal UC et al. Infection with cytomegalovirus in patients with inflammatory bowel disease: prevalence, clinical significance and outcome. J. Med. Microbiol. 2004; 53; Papadakis KA, Tung JK, Binder SW et al. Outcome of cytomegalovirus infections in patients with inflammatory bowel disease. Am. J. Gastroenterol. 2001; 96; Berk T, Gordon SJ, Choi HY et al. Cytomegalovirus infection of the colon: a possible role in exacerbations of inflammatory bowel disease. Am. J. Gastroenterol. 1985; 80; Garcia-Osogobio S, Takahashi T, Gamboa-Dominguez A et al. Toxic pseudomembranous colitis in a patient with ulcerative colitis. Inflamm. Bowel Dis. 2000; 6; Wang A, Takeshima F, Ikeda M et al. Ulcerative colitis complicating pseudomembranous colitis of the right colon. J. Gastroenterol. 2002; 37; Sagar PM, Dozois RR, Wolff BG. Long-term results of ileal pouch-anal anastomosis in patients with Crohn s disease. Dis. Colon Rectum 1996; 39; Grobler SP, Hosie KB, Affie E et al. Outcome of restorative proctocolectomy when the diagnosis is suggestive of Crohn s disease. Gut 1993; 34; McIntyre PB, Pemberton JH, Wolff BG et al. Indeterminate colitis. Long-term outcome in patients after ileal pouch-anal anastomosis. Dis. Colon Rectum 1995; 38; Pezim ME, Pemberton JH, Beart RW Jr. et al. Outcome of indeterminant colitis following ileal pouch-anal anastomosis. Dis. Colon Rectum 1989; 32; Koltun WA, Schoetz DJ Jr, Roberts PL et al. Indeterminate colitis predisposes to perineal complications after ileal pouchanal anastomosis. Dis. Colon Rectum 1991; 34; Kangas E, Matikainen M, Mattila J. Is indeterminate colitis Crohn s disease in the long-term follow-up? Int. Surg. 1994; 79; Panis Y, Poupard B, Nemeth J et al. Ileal pouch anal anastomosis for Crohn s disease. Lancet 1996; 347; Peyregne V, Francois Y, Gilly FN et al. Outcome of ileal pouch after secondary diagnosis of Crohn s disease. Int. J. Colorectal Dis. 2000; 15; Gramlich T, Delaney CP, Lynch AC et al. Pathological subgroups may predict complications but not late failure after ileal pouch-anal anastomosis for indeterminate colitis. Colorectal Dis. 2003; 5; Spiliadis CA, Lennard-Jones JE. Ulcerative colitis with relative sparing of the rectum. Clinical features, histology, and prognosis. Dis. Colon Rectum 1987; 30; Markowitz J, Kahn E, Grancher K et al. Atypical rectosigmoid histology in children with newly diagnosed ulcerative colitis. Am. J. Gastroenterol. 1993; 88; Glickman JN, Bousvaros A, Farraye FA et al. Pediatric patients with untreated ulcerative colitis may present initially with unusual morphologic findings. Am. J. Surg. Pathol. 2004; 28; Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
13 128 R K Yantiss & R D Odze 33. Odze R, Antonioli D, Peppercorn M et al. Effect of topical 5-aminosalicylic acid (5-ASA) therapy on rectal mucosal biopsy morphology in chronic ulcerative colitis. Am. J. Surg. Pathol. 1993; 17; Bernstein CN, Shanahan F, Anton PA et al. Patchiness of mucosal inflammation in treated ulcerative colitis: a prospective study. Gastrointest. Endosc. 1995; 42; Kleer CG, Appelman HD. Ulcerative colitis: patterns of involvement in colorectal biopsies and changes with time. Am. J. Surg. Pathol. 1998; 22; Kim B, Barnett JL, Kleer CG et al. Endoscopic and histological patchiness in treated ulcerative colitis. Am. J. Gastroenterol. 1999; 94; Scheppach W, Sommer H, Kirchner T et al. Effect of butyrate enemas on the colonic mucosa in distal ulcerative colitis. Gastroenterology 1992; 103; Robert ME, Tang L, Hao LM et al. Patterns of inflammation in mucosal biopsies of ulcerative colitis: perceived differences in pediatric populations are limited to children younger than 10 years. Am. J. Surg. Pathol. 2004; 28; Schumacher G, Kollberg B, Sandstedt B. A prospective study of first attacks of inflammatory bowel disease and infectious colitis. Histologic course during the 1st year after presentation. Scand. J. Gastroenterol. 1994; 29; Washington K, Greenson JK, Montgomery E et al. Histopathology of ulcerative colitis in initial rectal biopsy in children. Am. J. Surg. Pathol. 2002; 26; Matsumoto T, Nakamura S, Shimizu M et al. Significance of appendiceal involvement in patients with ulcerative colitis. Gastrointest. Endosc. 2002; 55; D Haens G, Geboes K, Peeters M et al. Patchy cecal inflammation associated with distal ulcerative colitis: a prospective endoscopic study. Am. J. Gastroenterol. 1997; 92; Groisman GM, George J, Harpaz N. Ulcerative appendicitis in universal and nonuniversal ulcerative colitis. Mod. Pathol. 1994; 7; Jahadi MR, Shaw ML. The pathology of the appendix in ulcerative colitis. Dis. Colon Rectum 1976; 19; Kroft SH, Stryker SJ, Rao MS. Appendiceal involvement as a skip lesion in ulcerative colitis. Mod. Pathol 1994; 7; Okawa K, Aoki T, Sano K et al. Ulcerative colitis with skip lesions at the mouth of the appendix: a clinical study. Am. J. Gastroenterol. 1998; 93; Mutinga ML, Odze RD, Wang HH et al. The clinical significance of right-sided colonic inflammation in patients with left-sided chronic ulcerative colitis. Inflamm. Bowel Dis. 2004; 10; Ekbom A, Helmick C, Zack M et al. The epidemiology of inflammatory bowel disease: a large, population-based study in Sweden. Gastroenterology 1991; 100; Davison AM, Dixon MF. The appendix as a skip lesion in ulcerative colitis. Histopathology 1990; 16; Yang SK, Jung HY, Kang GH et al. Appendiceal orifice inflammation as a skip lesion in ulcerative colitis: an analysis in relation to medical therapy and disease extent. Gastrointest. Endosc. 1999; 49; Goldblum JR, Appelman HD. Appendiceal involvement in ulcerative colitis. Mod. Pathol. 1992; 5; Sandler RS. Appendectomy and ulcerative colitis. Lancet 1998; 352; Andersson RE, Olaison G, Tysk C et al. Appendectomy and protection against ulcerative colitis. N. Engl. J. Med. 2001; 344; Duggan AE, Usmani I, Neal KR et al. Appendectomy, childhood hygiene, Helicobacter pylori status, and risk of inflammatory bowel disease: a case control study. Gut 1998; 43; Russel MG, Dorant E, Brummer RJ et al. Appendectomy and the risk of developing ulcerative colitis or Crohn s disease: results of a large case control study. South Limburg Inflammatory Bowel Disease Study Group. Gastroenterology 1997; 113; Rutgeerts P, D Haens G, Hiele M et al. Appendectomy protects against ulcerative colitis. Gastroenterology 1994; 106; Smithson JE, Radford-Smith G, Jewell GP. Appendectomy and tonsillectomy in patients with inflammatory bowel disease. J. Clin. Gastroenterol. 1995; 21; Minocha A, Raczkowski CA. Role of appendectomy and tonsillectomy in pathogenesis of ulcerative colitis. Dig. Dis. Sci. 1997; 42; Yantiss RK, Sapp HL, Farraye FA et al. Histologic predictors of pouchitis in patients with chronic ulcerative colitis. Am. J. Surg. Pathol. 2004; 28; McCready F, Bargen A, Dockerty MB et al. Involvement of the ileum in chronic ulcerative colitis. N. Engl. J. Med. 1949; 240; Saltzstein S, Rosenberg BF. Ulcerative colitis of the ileum and regional enteritis of the colon: a comparative histopathologic study. Am. J. Clin. Pathol. 1963; 40; Haskell H, Andrews CW, Reddy S et al. Pathology of the ileum in chronic ulcerative colitis. Am. J. Surg. Pathol. 2005; in press. 63. Binder V, Soltoft J, Gudmand-Hoyer E. Histological and histochemical changes in the jejunal mucosa in ulcerative colitis. Scand. J. Gastroenterol. 1974; 9; Valdez R, Appelman HD, Bronner MP et al. Diffuse duodenitis associated with ulcerative colitis. Am. J. Surg. Pathol. 2000; 24; Mitomi H, Atari E, Uesugi H et al. Distinctive diffuse duodenitis associated with ulcerative colitis. Dig. Dis. Sci. 1997; 42; Nakayama S, Matsuoka M, Yoshida Y et al. [A case of pouchitis, duodenitis and pancreatitis showing diffuse irregular narrowing of main pancreatic duct after total colectomy for ulcerative colitis]. Nippon Shokakibyo Gakkai Zasshi 2004; 101; Sasaki M, Okada K, Koyama S et al. Ulcerative colitis complicated by gastroduodenal lesions. J. Gastroenterol. 1996; 31; Gidaiatov AA, Alieva SA. [Upper gastrointestinal tract lesions in patients with nonspecific ulcerative colitis]. Klin. Med. (Mosk.) 2003; 81; Honma J, Mitomi H, Murakami K et al. Nodular duodenitis involving CD8+ cell infiltration in patients with ulcerative colitis. Hepatogastroenterology 2001; 48; Tobin JM, Sinha B, Ramani P et al. Upper gastrointestinal mucosal disease in pediatric Crohn disease and ulcerative colitis: a blinded, controlled study. J. Pediatr. Gastroenterol. Nutr. 2001; 32; Terashima S, Hoshino Y, Kanzaki N et al. Ulcerative duodenitis accompanying ulcerative colitis. J. Clin. Gastroenterol. 2001; 32; Thompson JW 3rd, Bargen JA. Ulcerative duodenitis and chronic ulcerative colitis: report of two cases. Gastroenterology 1960; 38; Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
14 Diagnostic difficulties in IBD pathology Ruuska T, Vaajalahti P, Arajarvi P et al. Prospective evaluation of upper gastrointestinal mucosal lesions in children with ulcerative colitis and Crohn s disease. J. Pediatr. Gastroenterol. Nutr. 1994; 19; Korelitz BI, Rajapakse R. Ulcerative duodenitis with ulcerative colitis: is it Crohn s disease or really ulcerative colitis? J. Clin. Gastroenterol. 2001; 32; Kinekawa F, Minami A, Yoshida M et al. [A case of ulcerative colitis after total colectomy associated with diffuse duodenitis]. Nippon Shokakibyo Gakkai Zasshi 1997; 94; Kaufman SS, Vanderhoof JA, Young R et al. Gastroenteric inflammation in children with ulcerative colitis. Am. J. Gastroenterol. 1997; 92; Manier JW, Reyes CN, Olsen TG. Ulcerative colitis and ulcerative gastritis. Am. J. Gastroenterol. 1972; 58; Heresbach D, Alexandre JL, Branger B et al. Frequency and significance of granulomas in a cohort of incident cases of Crohn s disease. Gut 2005; 54; Pierik M, De Hertogh G, Vermeire S et al. Epithelioid granulomas, pattern recognition receptors, and phenotypes of Crohn s disease. Gut 2005; 54; de Silva HJ, Jones M, Prince C et al. Lymphocyte and macrophage subpopulations in pelvic ileal pouches. Gut 1991; 32; Rotterdam H, Korelitz BI, Sommers SC. Microgranulomas in grossly normal rectal mucosa in Crohn s disease. Am. J. Clin. Pathol. 1977; 67; Yao K, Yao T, Iwashita A et al. Microaggregate of immunostained macrophages in noninflamed gastroduodenal mucosa: a new useful histological marker for differentiating Crohn s colitis from ulcerative colitis. Am. J. Gastroenterol. 2000; 95; Yantiss RK, Yang T, Baker SP, Wang HH, Farraye FA, Odze RD. Increased CD68 positive macrophages and macrophage microaggregates are prevalent in Crohn s colitis and aid in its distinction from ulcerative colitis. Mod. Pathol. 2005; 18; 123A. 84. Lee FD, Maguire C, Obeidat W et al. Importance of cryptolytic lesions and pericryptal granulomas in inflammatory bowel disease. J. Clin. Pathol. 1997; 50; Mahadeva U, Martin JP, Patel NK et al. Granulomatous ulcerative colitis: a re-appraisal of the mucosal granuloma in the distinction of Crohn s disease from ulcerative colitis. Histopathology 2002; 41; Warren BF, Shepherd NA, Price AB et al. Importance of cryptolytic lesions and pericryptal granulomas in inflammatory bowel disease. J. Clin. Pathol. 1997; 50; Tacla M. Colonoscopy in Crohn s disease of the colon. Arq. Gastroenterol. 1990; 27; Price AB. Overlap in the spectrum of non-specific inflammatory bowel disease colitis indeterminate. J. Clin. Pathol. 1978; 31; Harpaz N, Friedman S, George J. Superficial Crohn s colitis: pathological and clinical features including long-term followup. Mod. Pathol. 2001; 14; 86A. 90. Guy TS, Williams NN, Rosato EF. Crohn s disease of the colon. Surg. Clin. North Am. 2001; 81; , ix. 91. Kleer CG, Appelman HD. Surgical pathology of Crohn s disease. Surg. Clin. North Am. 2001; 81; 13 30, vii. 92. Linssen A, Tytgat GN. Fulminant onset of Crohn s disease of the colon (CDC). An observation of six cases. Dig. Dis. Sci. 1982; 27; Morpurgo E, Petras R, Kimberling J et al. Characterization and clinical behavior of Crohn s disease initially presenting predominantly as colitis. Dis. Colon Rectum 2003; 46; Read NW, Krejs GJ, Read MG et al. Chronic diarrhea of unknown origin. Gastroenterology 1980; 78; Lindstrom CG. Collagenous colitis with watery diarrhoea a new entity? Pathol. Eur. 1976; 11; Giardiello FM, Bayless TM, Yardley JH. Collagenous colitis. Compr. Ther. 1989; 15; Lazenby AJ, Yardley JH, Giardiello FM et al. Pitfalls in the diagnosis of collagenous colitis: experience with 75 cases from a registry of collagenous colitis at the Johns Hopkins Hospital. Hum. Pathol. 1990; 21; Bayless TM, Giardiello FM, Lazenby A et al. Collagenous colitis. Mayo Clin. Proc. 1987; 62; Jessurun J, Yardley JH, Giardiello FM et al. Chronic colitis with thickening of the subepithelial collagen layer (collagenous colitis): histopathologic findings in 15 patients. Hum. Pathol. 1987; 18; Robert ME. Microscopic colitis: pathologic considerations, changing dogma. J. Clin. Gastroenterol. 2004; 38; S Zins BJ, Sandborn WJ, Tremaine WJ. Collagenous and lymphocytic colitis: subject review and therapeutic alternatives. Am. J. Gastroenterol. 1995; 90; Zins BJ, Tremaine WJ, Carpenter HA. Collagenous colitis: mucosal biopsies and association with fecal leukocytes. Mayo Clin. Proc. 1995; 70; Carpenter HA, Tremaine WJ, Batts KP et al. Sequential histologic evaluations in collagenous colitis. Correlations with disease behavior and sampling strategy. Dig. Dis. Sci. 1992; 37; Lazenby AJ, Yardley JH, Giardiello FM et al. Lymphocytic ( microscopic ) colitis: a comparative histopathologic study with particular reference to collagenous colitis. Hum. Pathol. 1989; 20; Taccari E, Spada S, Giuliani A et al. Co-occurrence of psoriatic arthritis with collagenous colitis: clinicopathologic findings of a case. Clin. Rheumatol. 2002; 21; Benucci M, Bardazzi G, Magaro L et al. A case report of a man with rheumatoid factor positive rheumatoid arthritis associated with collagenous colitis. Clin. Exp. Rheumatol. 2001; 19; Breen EG, Farren C, Connolly CE et al. Collagenous colitis and coeliac disease. Gut 1987; 28; DuBois RN, Lazenby AJ, Yardley JH et al. Lymphocytic enterocolitis in patients with refractory sprue. Jama 1989; 262; Giardiello FM, Lazenby AJ. The atypical colitides. Gastroenterol. Clin. North Am. 1999; 28; , x Giardiello FM, Lazenby AJ, Yardley JH et al. Increased HLA A1 and diminished HLA A3 in lymphocytic colitis compared to controls and patients with collagenous colitis. Dig. Dis. Sci. 1992; 37; Weidenhiller M, Muller S, Schwab D et al. Microscopic (collagenous and lymphocytic) colitis triggered by food allergy. Gut 2005; 54; Wolber R, Owen D, Freeman H. Colonic lymphocytosis in patients with celiac sprue. Hum. Pathol. 1990; 21; Roubenoff R, Ratain J, Giardiello F et al. Collagenous colitis, enteropathic arthritis, and autoimmune diseases: results of a patient survey. J. Rheumatol. 1989; 16; Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
15 130 R K Yantiss & R D Odze 114. Giardiello FM, Lazenby AJ, Bayless TM. The new colitides, collagenous, lymphocytic, and diversion colitis. Gastroenterol. Clin. North Am. 1995; 24; Giardiello FM, Bayless TM, Jessurun J et al. Collagenous colitis: physiologic and histopathologic studies in seven patients. Ann. Intern. Med. 1987; 106; Giardiello FM, Lazenby AJ, Bayless TM et al. Lymphocytic (microscopic) colitis. Clinicopathologic study of 18 patients and comparison to collagenous colitis. Dig. Dis. Sci. 1989; 34; Fine KD, Do K, Schulte K et al. High prevalence of celiac spruelike HLA-DQ genes and enteropathy in patients with the microscopic colitis syndrome. Am. J. Gastroenterol. 2000; 95; Wang HH, Owings DV, Antonioli DA et al. Increased subepithelial collagen deposition is not specific for collagenous colitis. Mod. Pathol. 1988; 1; Giardiello FM, Jackson FW, Lazenby AJ. Metachronous occurrence of collagenous colitis and ulcerative colitis. Gut 1991; 32; Chandratre S, Bramble MG, Cooke WM et al. Simultaneous occurrence of collagenous colitis and Crohn s disease. Digestion 1987; 36; Muggia RA, Peppercorn MA, Wang H et al. Segmental macroscopic colitis associated with collagenous colitis. J. Clin. Gastroenterol. 1992; 14; Pokorny CS, Kneale KL, Henderson CJ. Progression of collagenous colitis to ulcerative colitis. J. Clin. Gastroenterol. 2001; 32; Goldstein NS, Gyorfi T. Focal lymphocytic colitis and collagenous colitis: patterns of Crohn s colitis? Am. J. Surg. Pathol. 1999; 23; Olesen M, Eriksson S, Bohr J et al. Lymphocytic colitis: a retrospective clinical study of 199 Swedish patients. Gut 2004; 53; Ayata G, Ithamukkala S, Sapp H et al. Prevalence and significance of inflammatory bowel disease-like morphologic features in collagenous and lymphocytic colitis. Am. J. Surg. Pathol. 2002; 26; Saurine TJ, Brewer JM, Eckstein RP. Microscopic colitis with granulomatous inflammation. Histopathology 2004; 45; Libbrecht L, Croes R, Ectors N et al. Microscopic colitis with giant cells. Histopathology 2002; 40; Padmanabhan V, Callas PW, Li SC et al. Histopathological features of the terminal ileum in lymphocytic and collagenous colitis: a study of 32 cases and review of literature. Mod. Pathol. 2003; 16; Sapp H, Ithamukkala S, Brien TP et al. The terminal ileum is affected in patients with lymphocytic or collagenous colitis. Am. J. Surg. Pathol. 2002; 26; Fiel MI, Robbins D, Harpaz N. Pseudomembranous variant of collagenous colitis. Mod. Pathol. 2003; 16; 118A Giardiello FM, Hansen FC 3rd, Lazenby AJ et al. Collagenous colitis in setting of nonsteroidal antiinflammatory drugs and antibiotics. Dig. Dis. Sci. 1990; 35; Yuan S, Reyes V, Bronner MP. Pseudomembranous collagenous colitis. Am. J. Surg. Pathol. 2003; 27; Kakar S, Pardi DS, Burgart LJ. Colonic ulcers accompanying collagenous colitis: implication of nonsteroidal anti-inflammatory drugs. Am. J. Gastroenterol. 2003; 98; Imperiali G, Meucci G, Alvisi C et al. Segmental colitis associated with diverticula: a prospective study. Gruppo di Studio per le Malattie Infiammatorie Intestinali (GSMII). Am. J. Gastroenterol. 2000; 95; Shepherd NA. Diverticular disease and chronic idiopathic inflammatory bowel disease: associations and masquerades. Gut 1996; 38; Gore S, Shepherd NA, Wilkinson SP. Endoscopic crescentic fold disease of the sigmoid colon: the clinical and histopathological spectrum of a distinctive endoscopic appearance. Int. J. Colorectal Dis. 1992; 7; Jani N, Finkelstein S, Blumberg D et al. Segmental colitis associated with diverticulosis. Dig. Dis. Sci. 2002; 47; Makapugay LM, Dean PJ. Diverticular disease-associated chronic colitis. Am. J. Surg. Pathol. 1996; 20; Pereira MC. Diverticular disease-associated colitis: progression to severe chronic ulcerative colitis after sigmoid surgery. Gastrointest. Endosc. 1998; 48; Berridge FR, Dick AP. Effect of Crohn s disease on colonic diverticula. Br. J. Radiol. 1976; 49; Gelb AM, Finkelstein WE. Differential diagnosis of diverticulitis and granulomatous colitis. Exacerbation of granulomatous colitis after sigmoid resection. Am. J. Gastroenterol. 1974; 62; Naouri A, Maroun J, Tissot E. [Diverticulosis and Crohn s disease of the sigmoid]. Ann. Chir. 1992; 46; Hoffman WA, Rosenberg MA. Granulomatous colitis in the elderly. Am. J. Gastroenterol. 1972; 58; Marshak RH, Janowitz HD, Present DH. Granulomatous colitis in association with diverticula. N. Engl. J. Med. 1970; 283; Marshak RH, Lindner AE, Maklansky D. Paracolic fistulous tracts in diverticulitis and granulomatous colitis. Jama 1980; 243; Petros JG, Happ RA. Crohn s colitis in patients with diverticular disease. Am. J. Gastroenterol. 1991; 86; Polit SA. Chronic segmental colitis in association with diverticulosis: a clinical syndrome in the elderly? J. Am. Geriatr. Soc. 1993; 41; Van Rosendaal GM, Andersen MA. Segmental colitis complicating diverticular disease. Can. J. Gastroenterol. 1996; 10; Sladen GE, Filipe MI. Is segmental colitis a complication of diverticular disease? Dis. Colon Rectum 1984; 27; Peppercorn MA. Drug-responsive chronic segmental colitis associated with diverticula: a clinical syndrome in the elderly. Am. J. Gastroenterol. 1992; 87; Peppercorn MA. The overlap of inflammatory bowel disease and diverticular disease. J. Clin. Gastroenterol. 2004; 38; S West AB, Losada M. The pathology of diverticulosis coli. J. Clin. Gastroenterol. 2004; 38; S11 S Appelman HD, Weaver DK. Pathology: colitis vs. diverticulitis. N. Engl. J. Med. 1971; 284; McCue J, Coppen MJ, Rasbridge SA et al. Coexistent Crohn s disease and sigmoid diverticulosis. Postgrad. Med. J. 1989; 65; Klein S, Mayer L, Present DH et al. Extraintestinal manifestations in patients with diverticulitis. Ann. Intern. Med. 1988; 108; Gledhill A, Dixon MF. Crohn s-like reaction in diverticular disease. Gut 1998; 42; Burroughs SH, Bowrey DJ, Morris-Stiff GJ et al. Granulomatous inflammation in sigmoid diverticulitis: two diseases or one? Histopathology 1998; 33; Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
16 Diagnostic difficulties in IBD pathology Goldstein NS, Leon-Armin C, Mani A. Crohn s colitis-like changes in sigmoid diverticulitis specimens is usually an idiosyncratic inflammatory response to the diverticulosis rather than Crohn s colitis. Am. J. Surg. Pathol. 2000; 24; Berman IR, Corman ML, Coller JA et al. Late onset Crohn s disease in patients with colonic diverticulitis. Dis. Colon Rectum 1979; 22; Korelitz BI, Cheskin LJ, Sohn N et al. Proctitis after fecal diversion in Crohn s disease and its elimination with reanastomosis: implications for surgical management. Report of four cases. Gastroenterology 1984; 87; Komorowski RA. Histologic spectrum of diversion colitis. Am. J. Surg. Pathol. 1990; 14; Ferguson CM, Siegel RJ. A prospective evaluation of diversion colitis. Am. Surg. 1991; 57; Kiely EM, Ajayi NA, Wheeler RA et al. Diversion procto-colitis: response to treatment with short-chain fatty acids. J. Pediatr. Surg. 2001; 36; Harig JM, Soergel KH, Komorowski RA et al. Treatment of diversion colitis with short-chain-fatty acid irrigation. N. Engl. J. Med. 1989; 320; Lu ES, Lin T, Harms BL et al. A severe case of diversion colitis with large ulcerations. Am. J. Gastroenterol. 1995; 90; Lusk LB, Reichen J, Levine JS. Aphthous ulceration in diversion colitis. Clinical implications. Gastroenterology 1984; 87; Geraghty JM, Charles AK. Aphthoid ulceration in diversion colitis. Histopathology 1994; 24; Bosshardt RT, Abel ME. Proctitis following fecal diversion. Dis. Colon Rectum 1984; 27; Haque S, Eisen RN, West AB. The morphologic features of diversion colitis: studies of a pediatric population with no other disease of the intestinal mucosa. Hum. Pathol. 1993; 24; Haque S, West AB. Aphthoid ulceration in diversion colitis. Histopathology 1994; 25; Haque S, West AB. Diversion colitis 20 years a-growing. J. Clin. Gastroenterol. 1992; 15; Yeong ML, Bethwaite PB, Prasad J et al. Lymphoid follicular hyperplasia a distinctive feature of diversion colitis. Histopathology 1991; 19; Grant NJ, Van Kruiningen HJ, Haque S et al. Mucosal inflammation in pediatric diversion colitis: a quantitative analysis. J. Pediatr. Gastroenterol. Nutr. 1997; 25; Geraghty JM, Talbot IC. Diversion colitis: histological features in the colon and rectum after defunctioning colostomy. Gut 1991; 32; Korelitz BI, Cheskin LJ, Sohn N et al. The fate of the rectal segment after diversion of the fecal stream in Crohn s disease: its implications for surgical management. J. Clin. Gastroenterol. 1985; 7; Lim AG, Langmead FL, Feakins RM et al. Diversion colitis: a trigger for ulcerative colitis in the in-stream colon? Gut 1999; 44; Warren BF, Shepherd NA, Bartolo DC et al. Pathology of the defunctioned rectum in ulcerative colitis. Gut 1993; 34; Feakins RM. Diversion proctocolitis with granulomatous vasculitis in a patient without inflammatory bowel disease. Histopathology 2000; 36; Ma CK, Gottlieb C, Haas PA. Diversion colitis: a clinicopathologic study of 21 cases. Hum. Pathol. 1990; 21; Asplund S, Gramlich T, Fazio V et al. Histologic changes in defunctioned rectums in patients with inflammatory bowel disease: a clinicopathologic study of 82 patients with long-term follow-up. Dis. Colon Rectum 2002; 45; Mahadevan U, Sandborn WJ. Diagnosis and management of pouchitis. Gastroenterology 2003; 124; Sandborn WJ. Pouchitis: definition, risk factors, frequency, natural history, classification, and public perspectives. In McLeod RS, Martin F, Sutherland LR, Wallace JL, Williams CN, eds. Trends in inflammatory bowel disease Lancaster: Kluwer Academic Publishers 1997; Sandborn WJ, Tremaine WJ, Batts KP et al. Pouchitis after ileal pouch-anal anastomosis: a Pouchitis Disease Activity Index. Mayo Clin. Proc. 1994; 69; Shen B, Achkar JP, Connor JT et al. Modified pouchitis disease activity index: a simplified approach to the diagnosis of pouchitis. Dis. Colon Rectum 2003; 46; Shen B, Achkar JP, Lashner BA et al. Endoscopic and histologic evaluation together with symptom assessment are required to diagnose pouchitis. Gastroenterology 2001; 121; Shen B, Achkar JP, Lashner BA et al. A randomized clinical trial of ciprofloxacin and metronidazole to treat acute pouchitis. Inflamm. Bowel Dis. 2001; 7; Shen B, Achkar JP, Lashner BA et al. Irritable pouch syndrome: a new category of diagnosis for symptomatic patients with ileal pouch-anal anastomosis. Am. J. Gastroenterol. 2002; 97; Fleshner PR, Vasiliauskas EA, Kam LY et al. High level perinuclear antineutrophil cytoplasmic antibody (panca) in ulcerative colitis patients before colectomy predicts the development of chronic pouchitis after ileal pouch-anal anastomosis. Gut 2001; 49; Reumaux D, Colombel JF, Masy E et al. Anti-neutrophil cytoplasmic auto-antibodies (ANCA) in ulcerative colitis (UC): no relationship with disease activity. Inflamm. Bowel Dis. 2000; 6; Yang P, Oresland T, Jarnerot G et al. Perinuclear antineutrophil cytoplasmic antibody in pouchitis after proctocolectomy with ileal pouch-anal anastomosis for ulcerative colitis. Scand. J. Gastroenterol. 1996; 31; Aisenberg J, Wagreich J, Shim J et al. Perinuclear anti-neutrophil cytoplasmic antibody and refractory pouchitis. A case control study. Dig. Dis. Sci. 1995; 40; Aitola P, Matikainen M, Mattila J et al. Chronic inflammatory changes in the pouch mucosa are associated with cholangitis found on peroperative liver biopsy specimens at restorative proctocolectomy for ulcerative colitis. Scand. J. Gastroenterol. 1998; 33; Bulois P, Tremaine WJ, Maunoury V et al. Pouchitis is associated with mucosal imbalance between interleukin-8 and interleukin-10. Inflamm. Bowel Dis. 2000; 6; Carter MJ, Di Giovine FS, Cox A et al. The interleukin 1 receptor antagonist gene allele 2 as a predictor of pouchitis following colectomy and IPAA in ulcerative colitis. Gastroenterology 2001; 121; Facklis K, Plevy SE, Vasiliauskas EA et al. Crohn s diseaseassociated genetic marker is seen in medically unresponsive ulcerative colitis patients and may be associated with pouch- Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,
17 132 R K Yantiss & R D Odze specific complications. Dis. Colon Rectum 1999; 42; ; discussion Korsgen S, Keighley MR. Causes of failure and life expectancy of the ileoanal pouch. Int. J. Colorectal Dis. 1997; 12; Luukkonen P, Jarvinen H, Tanskanen M et al. Pouchitis recurrence of the inflammatory bowel disease? Gut 1994; 35; Merrett MN, Mortensen N, Kettlewell M et al. Smoking may prevent pouchitis in patients with restorative proctocolectomy for ulcerative colitis. Gut 1996; 38; Nicholls RJ, Banerjee AK. Pouchitis: risk factors, etiology, and treatment. World J. Surg. 1998; 22; Ruseler-van Embden JG, Schouten WR, van Lieshout LM. Pouchitis: result of microbial imbalance? Gut 1994; 35; Simchuk EJ, Thirlby RC. Risk factors and true incidence of pouchitis in patients after ileal pouch-anal anastomoses. World J. Surg. 2000; 24; Teixeira WG, da Silva JH, Teixeira MG et al. Pouchitis: extracolonic manifestation of ulcerative colitis? Rev. Hosp. Clin. Fac. Med. Sao Paulo 1999; 54; Penna C, Dozois R, Tremaine W et al. Pouchitis after ileal pouch-anal anastomosis for ulcerative colitis occurs with increased frequency in patients with associated primary sclerosing cholangitis. Gut 1996; 38; Salemans JM, Nagengast FM, Lubbers EJ et al. Postoperative and long-term results of ileal pouch-anal anastomosis for ulcerative colitis and familial polyposis coli. Dig. Dis. Sci. 1992; 37; Dozois RR, Kelly KA, Welling DR et al. Ileal pouch-anal anastomosis: comparison of results in familial adenomatous polyposis and chronic ulcerative colitis. Ann. Surg. 1989; 210; ; discussion Barton JG, Paden MA, Lane M et al. Comparison of postoperative outcomes in ulcerative colitis and familial polyposis patients after ileoanal pouch operations. Am. J. Surg. 2001; 182; Heuschen UA, Autschbach F, Allemeyer EH et al. Long-term follow-up after ileoanal pouch procedure: algorithm for diagnosis, classification, and management of pouchitis. Dis. Colon Rectum 2001; 44; Penna C, Tiret E, Kartheuser A et al. Function of ileal J pouchanal anastomosis in patients with familial adenomatous polyposis. Br. J. Surg. 1993; 80; Schmidt CM, Lazenby AJ, Hendrickson RJ et al. Preoperative terminal ileal and colonic resection histopathology predicts risk of pouchitis in patients after ileoanal pull-through procedure. Ann. Surg. 1998; 227; ; discussion Samarasekera DN, Stebbing JF, Kettlewell MG et al. Outcome of restorative proctocolectomy with ileal reservoir for ulcerative colitis: comparison of distal colitis with more proximal disease. Gut 1996; 38; Gustavsson S, Weiland LH, Kelly KA. Relationship of backwash ileitis to ileal pouchitis after ileal pouch-anal anastomosis. Dis. Colon Rectum 1987; 30; Hurst RD, Molinari M, Chung TP et al. Prospective study of the incidence, timing and treatment of pouchitis in 104 consecutive patients after restorative proctocolectomy. Arch. Surg. 1996; 131; ; discussion Joelsson M, Andersson M, Bark T et al. Allopurinol as prophylaxis against pouchitis following ileal pouch-anal anastomosis for ulcerative colitis. A randomized placebo-controlled double-blind study. Scand. J. Gastroenterol. 2001; 36; MacRae HM, McLeod RS, Cohen Z et al. Risk factors for pelvic pouch failure. Dis. Colon Rectum 1997; 40; Sandborn WJ, McLeod R, Jewell DP. Medical therapy for induction and maintenance of remission in pouchitis: a systematic review. Inflamm. Bowel Dis. 1999; 5; Stein RB, Lichtenstein GR. Complications after ileal pouch-anal anastomosis. Semin. Gastrointest. Dis. 2000; 11; Stocchi L, Pemberton JH. Pouch and pouchitis. Gastroenterol. Clin. North Am. 2001; 30; Rubinstein MC, Fisher RL. Pouchitis: pathogenesis, diagnosis, and management. Gastroenterologist 1996; 4; Scott AD, Phillips RK. Ileitis and pouchitis after colectomy for ulcerative colitis. Br. J. Surg. 1989; 76; Shepherd NA. The pelvic ileal reservoir: pathology and pouchitis. Neth. J. Med. 1990; 37 (Suppl. 1); S Zuccaro G Jr, Fazio VW, Church JM et al. Pouch ileitis. Dig. Dis. Sci. 1989; 34; Meuwissen SG, Hoitsma H, Boot H et al. Pouchitis (pouch ileitis). Neth. J. Med. 1989; 35 (Suppl. 1); S Fruin AB, El-Zammer O, Stucchi AF et al. Colonic metaplasia in the ileal pouch is associated with inflammation and is not the result of long-term adaptation. J. Gastrointestinal Surg. 2003; 7; de Silva HJ, Gatter KC, Millard PR et al. Crypt cell proliferation and HLA-DR expression in pelvic ileal pouches. J. Clin. Pathol. 1990; 43; de Silva HJ, Millard PR, Kettlewell M et al. Mucosal characteristics of pelvic ileal pouches. Gut 1991; 32; de Silva HJ, Millard PR, Soper N et al. Effects of the faecal stream and stasis on the ileal pouch mucosa. Gut 1991; 32; Tytgat GN, van Deventer SJ. Pouchitis. Int. J. Colorectal Dis. 1988; 3; Goldstein NS, Sanford WW, Bodzin JH. Crohn s-like complications in patients with ulcerative colitis after total proctocolectomy and ileal pouch-anal anastomosis. Am. J. Surg. Pathol. 1997; 21; Shen B, Fazio VW, Remzi FH et al. Comprehensive evaluation of inflammatory and noninflammatory sequelae of ileal pouchanal anastomoses. Am. J. Gastroenterol. 2005; 100; Subramani K, Harpaz N, Bilotta J et al. Refractory pouchitis: does it reflect underlying Crohn s disease? Gut 1993; 34; Achkar JP, Shen B. Medical management of postoperative complications of inflammatory bowel disease: pouchitis and Crohn s disease recurrence. Curr. Gastroenterol. Report 2001; 3; Belliveau P, Trudel J, Vasilevsky CA et al. Ileoanal anastomosis with reservoirs: complications and long-term results. Can. J. Surg. 1999; 42; Hallak A, Baratz M, Santo M et al. Ileitis after colectomy for ulcerative colitis or carcinoma. Gut 1994; 35; Wolf JM, Achkar JP, Lashner BA et al. Afferent limb ulcers predict Crohn s disease in patients with ileal pouch-anal anastomosis. Gastroenterology 2004; 126; MacNeill KN, Guindi M, Riddell RH. Is transmural inflammation in the ileoanal pouch significant? Mod. Pathol. 2004; 17; 123A. Ó 2006 Blackwell Publishing Ltd, Histopathology, 48,

18
19

20 Atypical Forms of Ulcerative Colitis (and Crohn s) Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA
21 Lecture Outline 1. Typical (classic) features of IBD 2. Atypical IBD resections Indeterminate (fulminant) colitis Non-IBD mimics 3. Atypical UC biopsies 4. Summary practical suggestions
22 Classic Microscopic Features of Untreated Ulcerative Colitis and Crohn s Disease Ulcerative Colitis Crohn s Disease Diffuse, continuous disease Rectal involvement Disease worse distally No fissures No transmural aggregates No ileal involvement (exception: backwash ) Crypt-rupture (mucin) granulomas Segmental disease Variable rectal involvement Variable disease severity Fissures, sinuses, fistulous tracts Transmural lymphoid aggregates Upper GI tract involvement Epithelioid granulomas (unrelated to crypts)





23 Ulcerative Colitis


24 Crohn s Colitis
25 Indeterminate Colitis % IBD show overlapping features 2. No diagnostic criteria 3. Provisional (Interum) diagnosis
26 Overlap in the Spectrum of Non-specific IBD- Colitis Indeterminate (Price J, Clin Pathol 1978;(31): ) 30 cases 27(90%) urgent surgery (35% toxic megacolon) Accepted CD criteria (fissures, TLA, skip) found in UC Diagnostic difficulties resolved in many by evaluation of biopsy material
27 Indeterminate Colitis Diagnostic Scenario 1. Fulminant colitis 2. Insufficient clinical/pathologic info 3. Attempt to establish diagnosis in biopsy studies 4. Failure to recognize unusual variants 5. Failure to utilize hard diagnostic criteria 6. IBD mimics or secondary disease
28 Informal Survey 10 GI Pathologists Def n of Indeterminate Colitis IBD: unclear if UC or Crohn s pathologically 5 Acute fulminant colitis (with fissures) 3 Cause of IBD unclear clinically and pathologically 2 Resections only 8 Biopsy or resections 2
29 Fulminant Colitis 1. Severe colitis with systemic toxicity 2. +/- colonic dilatation 3. Some Crohn s like features Superficial fissuring ulcers Transmural inflammation Rectal sparing (relative)




30



31



32

33





34




35
36 Clinical and Prognostic Significance of Early Fissuring Ulceration in Chronic UC Feature Colitis with Colitis without Fissures Fissures N=21 N=58 Pancolitis 91% 55% Serositis 41% 5% Backwash 64% 27% Appendicitis 20% 10% Pouchitis 50% 9% Crohn s (F/U) 0% 0% Yantiss et al, Am J Surg Pathol 2006;30(2):
37 Pouch Complications in Indeterminate and Ulcerative Colitis* Author IC UC Pouch Failure N N IC/UC Yu (2000) %/11% Delaney (2002) %/3.5% Rudolph (2002) %/6% Dayton (2002) %/1.2% Gramlich (2003) %/2.1% Pishori (2004) %/2.1% Brown (2005) %/6% *Adapted from Martland et al, Histopath 2007
38 Ileal Pouch-Anal Anastomosis in Patients with Indeterminate Colitis Variable Ulcerative Indeterminate Crohn s Colitis Colitis Colitis Any complication 48% 58% 90%* Sepsis 7% 16% 24%* Fistula 8% 21% 65%* Obstruction 20% 28% 21% Stricture 20% 20% 34% Pouchitis 50% 52% 53% Failure 10% 16% 52%* Yu et al, Dis Colon Rectum 2000;43:
39 Pathologic Features of Indeterminate Colitis (Bruce Wolff The case for IPAA for IC, IBD 2002) Wolff Criteria for IC Odze Diagnosis 1. UC-like with microscopic skip areas UC 2. UC-like with longitudinal ulcers UC 3. UC-like with mild transmural inflam focally UC 4. Severe colitis, most severe transverse colon, fissures, rectum less involved UC 5. Focal non-specific ileal ulcer, microscopic patchy colonic disease, no UC granulomas 6. Two skip areas without mucosal involvement, microscopic appearance UC c/w UC 7. Chronic IBD, features of UC, but focal mild transmural inflammation UC 8. Severe IBD with deep knife-like ulcers, dense submucosal inflammation, CD thickened bowel wall, narrow lumen, but no granulomas 9. Segmental mucosal colitis, deep linear ulcers, skip areas CD
40 Value of Serologic Markers in IC: A Prospective Follow-up Study* (Joossens et al, Gastroenterology 2002) (N=97) Feature CD (N=17) UC(N=14) ASCA+/ANCA- ASCA-/ANCA+ Sensitivity 67% 78% Specificity 78% 67% PPV 80% 64% NPV 64% 80% * 49% of IC patients neg for ASCA and ANCA * 40 pts remain with IC to date
41 New Serologic Markers Disease OMPC *1 cbirl *2 (ANCA+) (anti-flagellin) Anti I 2 CD 55% 44% 54% UC 11% 4% 10% Controls 5% - 19% *1 Internal perforating CD *2 Internal perforating and fibrostenosing
42 Indeterminate Colitis 1. Ulcerative colitis: 60-90% 2. Crohn s disease: 10-30% 3. Ischemic colitis: <1% 4. Infectious colitis: <1% 5. Radiation colitis: <1% 6. Diverticular disease: <1% 7. Microscopic colitis: <1% 8. Drug-induced colitis: <1%
43 IBD Mimics Unusual Pathologic Manifestations of other forms of colitis Ischemia Radiation Microscopic colitis with features of IBD Diverticular disease-associated chronic colitis Infectious colitis (Yersinia) Diversion colitis Drug induced colitis mimicking IBD Vasculitis (Behcet s) Acute self-limited colitis Polyposis disorders that may mimic IBD Solitary rectal ulcer syndrome Inflammatory cap polyposis Juvenile polyposis

44 Ischemic colitis

45 Ischemic colitis

46 Microscopic colitis


47 Microscopic colitis
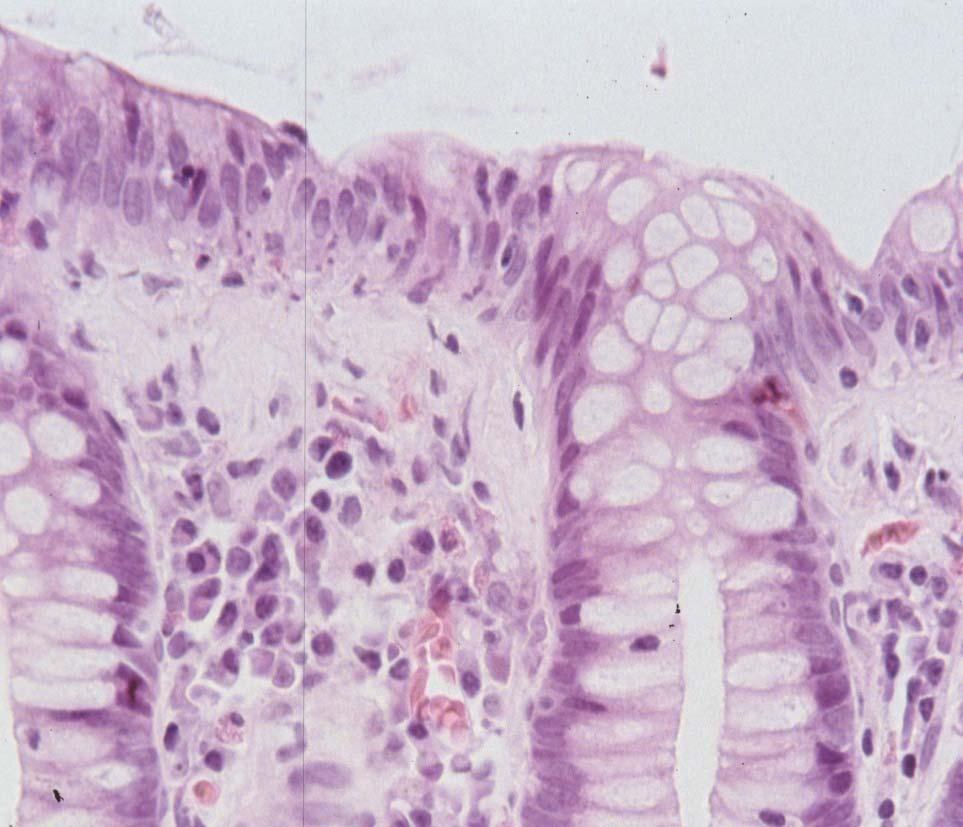

48 Microscopic colitis


49 Microscopic colitis
50 Prevalence and Significance of Inflammatory Bowel Disease-Like Morphologic Features in Collagenous and Lymphocytic Colitis Collagenous colitis Lymphocytic colitis Feature (No. of patients [%]) (No. of patients [%]) Surface ulceration 2/79 (2.5%) 0/71 (0%) Active crypt inflammation 24/79 (30%) 27/71 (38%) Paneth cell metaplasia 32/72 (44%) 9/63 (14%) Crypt atrophy or irregularity 6/79 (7.6%) 3/71 (4.2%) Lymphoid nodules 51/71 (65%) 47/71 (69%) Ayata et al, Am J Surg Pathol 2002;26(11):





51 Ulcerative Colitis




52 Lymphocytic colitis



53 Diverticular disease-associated colitis



54 Diverticular disease-associated colitis

55 Ulcerative colitis with clostridium Difficile and CMV

56 CMV
57 CMV in IBD Resections Author Prevalence* Rate Maroni et al 22% Alcala et al 18% Kaufman et al 4.6% Eyre-Brook et al 11.5% Swarbrick et al 0% Cooper et al 13% * in steroid refractory cases Adapted from Hommes et al, IBD (2004)




58





59 Polyposis-like Crohn s
60 Indeterminate Colitis Summary Most represent fulminant colitis (?UC) Expanded IC diagnosis often due to lack of clinical/path info Not a biopsy diagnosis Pouch complication rate acceptable Pouch procedure recommended
61 Atypical Ulcerative Colitis: Biopsies
62 Summary of Causes of Unusual (Crohn s like) Patterns of Disease in Ulcerative Colitis Effect of oral/topical therapy Disease (often mild) in remission Rt colon/appendix involvement in sub-total colitis Pediatric UC (initial presentation) Ileitis in UC ( backwash, other causes) UGI tract involvement (e.g., duodenitis) Crohn s like Apthous ulcers/granulomas in UC Primary sclerosing cholangitis Fulminant colitis
63 Effect of 5ASA Therapy on Rectal Biopsy Morphology in CUC % patients with % normal Treatment group >1 normal biopsy biopsies 5-ASA (n=11) 64% 36% Placebo (n=3) 66% 12% Total (n= 14) 64% 29% 5-ASA vs placebo; p= Odze et al, Am J Surg Pathol 1993;17(9):
64 UC: Patterns of Involvement in Colorectal Biopsies with Time (Kleer et al, Am J Surg Pathol 1998) Extent of Colitis Distribution of disease N Diffuse Non-diffuse (Patchy) Pancolitis 30 2(7%) 28(93%) Left-sided 8 1(13%) 7(87%) Proctosigmoiditis 3 0(0%) 3(100%) Total 41 3(7%) 38(93%)
65 Rectal Sparing and Patchy Disease in UC N=56 Endoscopy Biopsy Colectomy Rectal sparing 18(32.1%) 17(30.4%)* 3(5.4%)** absolute N/A 3(5.4%) 0(0%) relative N/A 14(25%)* 3(5.4%)** Patchiness of disease 17(30.4%) 14(25%)* 6(10.7%) absolute N/A 2(3.6%) 4(7.1%) relative N/A 12(21.4%)* 2(3.6%) N/A, not applicable; *P<0.01 compared with endoscopy series; ** P<0.05 compared with biopsy series (Joo et al, Mod Pathol 2008;21(s1):560A)
66 Other Skip Lesions in Subtotal Ulcerative Colitis 1. Appendiceal involvement: 21-86% 2. Ascending colon : 4% 3. Cecum/periappendix : 10-75%
67 Right Colon Involvement in Patients with Left-Sided UC Left-sided colitis Left-sided and Colitis Feature Ascending colitis only N=14 N=35 Appendectomy 7% 0% NSAID use 64% 50% Prednisone use 0% 7% Progression (pancolitis) 0% 3% Dysplasia 7% 0% Crohn s disease (F/U) 0% 0% Mutinga et al, Inflam Bowel Dis 2004;10:
68 Atypical Presentation of Pediatric Patients With UC Feature Children Adults N=70 N=44 Chronic-active proctitis 79% 95%* Microscopic skip areas 23% 0%* Relative rectal sparing 34% 5%* Complete rectal sparing 3% 0% Glickman et al, Am J Surg Pathol 2004;28(2):
69 Ileitis in UC Bowel Prep Drugs (NSAIDs) Backwash Infection Bacterial Overgrowth Ischemia Primary Involvement?

70

71
72 Pathologic Features and Clinical Significance of Backwash Ileitis in Ulcerative Colitis Feature UC with UC Ileitis Without ileitis (N=34) (N=66) Pancolitis 94% 50%* Severe/fulminant colitis 65% 67% Distal severe disease 24% 25% Appendix involved 50% 34% Pouch complications 30% 37% Neoplasia 3% 15% Crohn s upon F/U 0% 4% Haskell, et al, Am J Surg Pathol 2005;29(11):


73 Duodenojejunitis in UC Diffusely granular Diffuse inflammation & distortion
74 Granulomas in UC Up to 20% of UC cases Most crypt-rupture related Other etiologies - barium, particulate matter, - infections, drugs, etc.




75
76 Superficial (UC-like) Crohn s Colitis 1. Poorly defined criteria 2. Ambiguous or Crohn s-like features clinically 3. UC-like features pathologically 4. Often shows 1 classic Crohn s features (granulomas, perianal disease, etc)




77





78





79
80 Pathologic Features of UC in PSC A Case Control Study (Joo et al, Am J Surg Pathol, In Press) Feature UC-PSC UC only P value N=40 N=40 Age at dx Pancolitis 85% 45%.001 Mean colitis grade Mean proctitis grade Rectal Sparing (relative) 27% 25% NS Ileitis 36% 27% NS Dysplasia 15% 7.5% NS
81 Summary I When Evaluating Resections for IBD Obtain all clinical/pathologic (biopsy) material Rule out non-ibd causes of chronic colitis For fulminant cases, recognize (normal) presence of Crohn s-like features: pouch procedure O/K For non-fulminant cases, evaluate carefully for Crohn s features Use term IC or colitis of uncertain type (etiology) only for resections (+/- features of CD) Most cases represent UC
82 Summary II When Evaluating Biopsies for IBD Primary goal: Location (colon, ileum) Extent Severity (inactive, mild, mod, severe) Dysplasia/carcinoma Secondary goal: (mainly pre-treatment) Type of IBD (UC vs CD) Continuity of disease (pre-treatment) Ileal/UGI involvement Granulomas



83



84

85

86

87

88
89
90
91 Colitis Indeterminate (Price, J Clin Pathol 1978;(31): ) Feature IC UC CD N=30 N=60 N=32 Discontinuous disease Granulomas Crohn s fissures Early fissures 28 20* 32 Transmural inflam Microscopic skip lesions 18 6* 0 *had fulminant disease
92 Indeterminate Colitis Pouch complications 1. Ulcerative colitis: 8-10% 2. Indeterminate colitis: 10-20% 3. Crohn s colitis: 30-40%
93 Equivalent function, quality of life and pouch survival rates after IPAA for IC and UC Complications Indeterminate Ulcerative Colitis Colitis (n=79) (n=565) Cuff abscess 1.3% 1.6% Pouch leak 5.1% 2.3% Abscess 0% 1.1% Stricture 7.6% 4.8% Fistular 2.5% 1.6% SBO 6.3% 5.5% Pouchitis 34.2% 25% Crohn s 1.3% 0.7% Pouch loss 2.5% 1.2% Delaney et al, Annals of Surg 236(1):43, 2002
94 Crohn s Disease and Pouch Success (Brown et al, Dis Col Rect 2005) Disease Pouch N Complications Failure UC % 6% CD 36 64% 56% IC 21 43% 10%
95 Crohn s Disease and Pouch Success (Brown et al, Dis Col Rect 2005) Feature Pouch failure N=20 Pouch success N=16 Pancolitis 75% 63% Granulomas 5% 19% Transmural inflam 20% 19% Skip lesions 15% 44% Deep ulcers 10% 25% Rectal sparing 0% 6% All not significant
96 Indeterminate Colitis Adjunctive tests Test UC CD ANCA 60-70% 10-40% ASCA <10% 50-60% Anti-cBir1* 6% 50% *associated with S. Intestine, internalpenetrating and fibrostenosing disease
97 Serologic Markers in IBD CD UC Author N ASCA+/ANCA- ASCA-/ANCA+ Sens Spec Sens Spec Quinton Linskens Koutobakis Sandborn Peeters Adapted from Bossuyt, Clin Chem 2006




98 Lymphocytic colitis
99 Diverticular Disease-Associated Colitis Disease limited to area with diverticulosis Mucosal colitis (UC-like) only, rectal sparing Pathogenesis uncertain Treatment similar to UC Rare cases similar to Crohn s (but do not develop Crohn s upon follow-up)
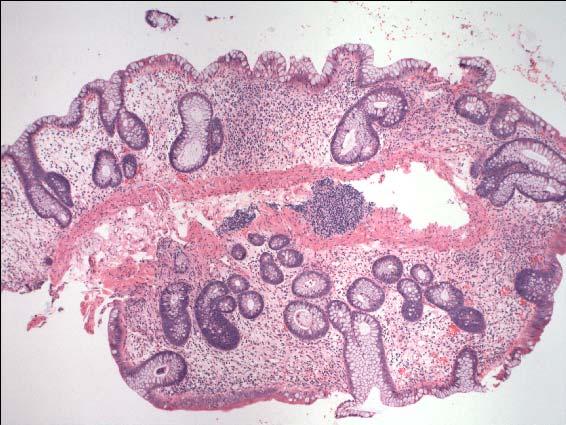
100 Mycophenylate colitis

101 Mycophenylate colitis




102
103 Treated Ulcerative Colitis 1. Patchiness of disease/rectal sparing occurs in up to 70% of patients 2. May be enhanced by oral/enema medication 3. Patchiness/rectal sparing does not imply Crohn s disease 4. Data applies (mainly) to biopsy studies
104 Ulcerative Appendicitis in Universal and Non-universal UC Feature Pancolitis Pancolitis Subtotal (Adult) (children) Colitis Patent appendix 83% 11% 21% Appendicitis 87% 64% 86% Groisman et al, Modern Pathol 1994(7):
105 Backwash Ileitis <20% of UC Mostly mild, rare ulcers Distal few cms only No increased risk of cancer Not all backwash patients have pancolitis? Ileal manifestation of UC, drugs, infection, bowel prep, etc.
106 Upper GI Involvement in UC 1. Extremely rare, unclear etiology 2. Stomach/duodenum 3. UC-like histology
107 UC-like Crohn s disease* (Soucy et al, DDW 2009) M/F 5/3 Mean age 38 years Severe disease 4(50%) Subtotal colitis 2(25%) Left sided colitis 6(75%) Macroscopic skip lesions 3(38%) Granulomas 2(25%) Perianal disease 3(38%) Pouch fistula 1(13%) Recurrent disease (colon) 1(13%) Pouch breakdown 0(0%) ASCA+, mucosal disease, no fissures, mural inflam, or UGI involvement
108
109
110

111
112 Effect of 5ASA Therapy on Rectal Biopsy Morphology in CUC Diagnosis No. of biopsies (n=123) Chronic inactive 53 (43.1%) Chronic active 32 (26.0%) Active 2 (1.6%) Normal 36 (29.3%) Odze et al, Am J Surg Pathol 1993;17(9):
113 Patchiness/Rectal Sparing in Treated Ulcerative Colitis Author # Patients Histologic Feature Patchiness Rectal Sparing Bernstein (1995) 39 33% 15% Kleer (1998) 41 30% -- Kim (1999) 32 38% 44%
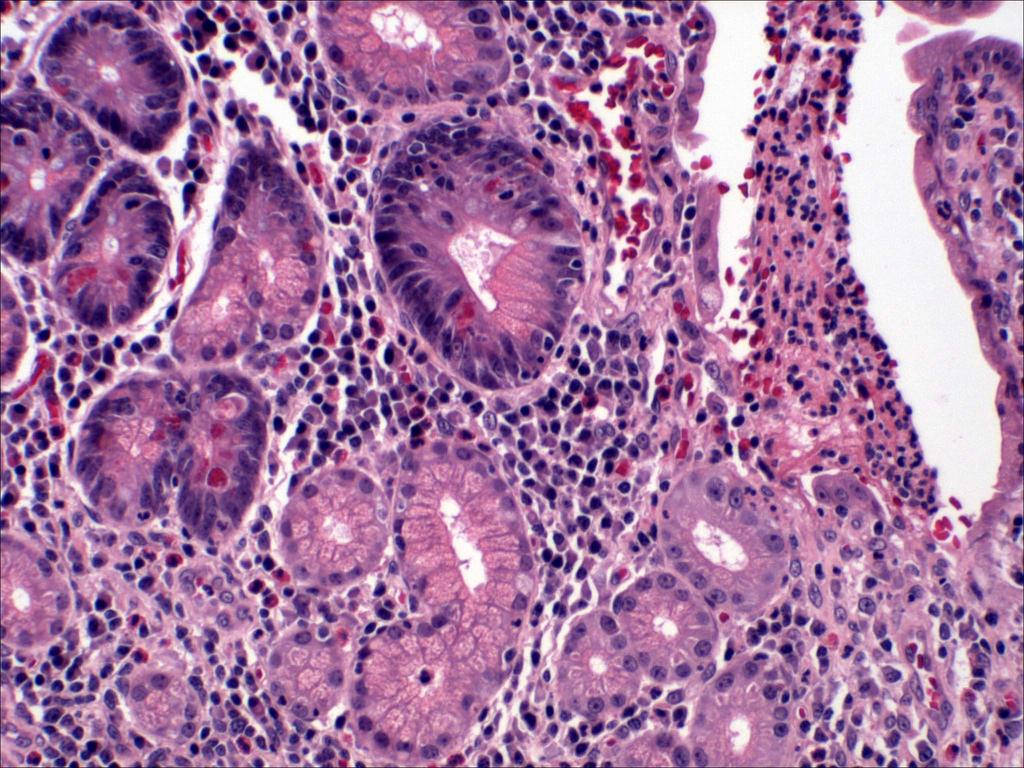
114

115





116
117 Ischemic colitis

118 Ischemic colitis



119 Radiation colitis
120 Microscopic Colitis vs IBD Feature Microscopic Colitis IBD Cryptitis/crypt abscesses +/- (focal) Prominent Crypt distortion +/- (focal) Prominent Basal plasmacytosis + ++ Basal lymphoid aggregates +/- ++ Paneth cell metaplasia + + Prominent lymphocytic/plasmacytic ++ + inflammation Neutrophils in lamina propria +/- ++ Prominent eosinophils + (cc) +/- Thickened/irregular subepithelial ++ (cc) +/- (focal) collagen layer Ulcer/erosion +/- (rare) ++ (common) cc = collagenous colitis

121 Yersinia ileo-colitis

122 Yersinia ileo-colitis

123 Yersinia ileo-colitis

124 Yersinia ileo-colitis

125 Diversion colitis

126 Mycophenylate colitis
127 Mycophenolate Used to prevent kidney allograft rejection Small percentage get chronic diarrhea Active metabolite (mycophenolic acid) enters biliary/intestinal system deconjugated by bacteria reabsorbed Bind to membrane proteins on absorptive cells Promotes cytokine production,? Genotoxic
128 Mycophenolate Toxicity Differential Diagnosis Acute GVHD Infectious Colitis (CMV) Other Drug/Toxic Colitis IBD Radiation Colitis HIV Enteropathy

129 Solitary rectal Ulcer syndrome

130 Cap polyposis
131 Integrated Clinical, Molecular, Serologic Classification of IBD: Montreal WCOG 2005 Use IBD unclassified for ambiguous clinical cases Use IC for resections only Prefer term colitis of uncertain type
132 Pathology Sign-Out Recommendations Use generic diagnoses - chronic, active, chronic-active Avoid indeterminate term Presence/absence dysplasia Favor specific diagnosis (Crohn s) if ileal/ugi involvement, granulomas or discontinuous disease pre-treatment Be cognitive of unusual variants




133
134 Indeterminate Colitis Summary 1. <1% (with Hard Core criteria) 2. Not a biopsy diagnosis 3. Most are fulminant UC 4. Pouch failure rate acceptable - pouchitis 5. Pouch procedure recommended
135 Outcome of IC (Gramlich et al, Colorectal Disease 2002) Disease N Perianal fistula Pelvic abscess Pouch failure Pouch loss CD upon follow-up IC, favor UC* %* 10%* 2% 1% 6%* IC 8 0% 0% 0% 12.5% 12.5% IC, favor CD % 0% 0% 0% 0% UC (controls) % 2.2% 1.4% 2.1% 1.3% * 1 Deep ulcer associated with fistula, pelvic abscess and CD upon follow-up compared to controls.
136 Outcome of IC Post Pouch Procedure (Pishori et al, Dis Col Rect 2004) Disease N Complications Fistula SBO Pouchitis UC % 4% 9% 5% CD 5 60% 20% IC 13 31% 8% 8% 0%
137 Outcome of IC (Rudolph et al, Dis Col Rectum 2002) Pouch status Fulminant Colitis Disease N Failure Fistula Pouchitis UC 71 8% 10% 60% 8% CD % - 72% 50% IC 35 0% 26% 30% 76%
138 CMV in IBD IBD pts at risk for CMV IHC for CMV on tissue is gold standard Prevalence rate: 21-34% in acute severe colitis : 33-36% in steroid refractory Antiviral therapy remission rates: %
139 Fulminant Colitis (Indeterminate) Clinically toxic Extensive ulceration Transverse colon most severe Relative rectal sparing Superficial fissures, transmural inflammation Dilated colon in some cases
140 Int Organization of IBD (IOIBD) Working Party (2008) Prefer term IBD unclassified for chronic colitis (IBD) without definitive features of CD or UC
141 Indeterminate Colitis Summary A precise dx of UC or CD not always possible after all clinical/pathologic (resection) info available Severe fulminant disease, children, PSC Development of characteristic features of CD or UC usually occurs, but may take time Eliminate superimposed (CMV, pseudomembranous) or alternative (microscopic colitis, ischemic colitis, etc.) diagnoses Not a biopsy diagnosis In most patients, pouch procedure is successful



142 Rectal sparing Cecal patches: skip lesions

143

144
145
146

147



148



149



150



151

152
IBD. Crohn s. Outline. Ulcerative colitis versus Crohn s disease: is biopsy useful? UC vs. Crohn s? Is it easy? Biopsy settings 21/07/2017 IBD
 Outline Ulcerative colitis versus Crohn s disease: is biopsy useful? Roger Feakins Colorectal biopsies Ileal and upper GI biopsies Special situations New techniques Summary Inflammatory bowel disease (IBD)
Outline Ulcerative colitis versus Crohn s disease: is biopsy useful? Roger Feakins Colorectal biopsies Ileal and upper GI biopsies Special situations New techniques Summary Inflammatory bowel disease (IBD)
하부위장관비종양성질환의 감별진단 주미인제의대일산백병원
 하부위장관비종양성질환의 감별진단 주미인제의대일산백병원 Solutions for diagnostic problems in Colitis : Please ask yourself five questions Normal or Inflamed? Acute or Chronic? IBD or Other chronic colitis? Ulcerative colitis or
하부위장관비종양성질환의 감별진단 주미인제의대일산백병원 Solutions for diagnostic problems in Colitis : Please ask yourself five questions Normal or Inflamed? Acute or Chronic? IBD or Other chronic colitis? Ulcerative colitis or
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
GUIDELINES FOR THE INITIAL BIOPSY DIAGNOSIS OF CHRONIC IDIOPATHIC INFLAMMATORY BOWEL DISEASE A STRUCTURED APPROACH TO COLORECTAL BIOPSY ASSESSMENT
 Guidelines for the Initial Biopsy Diagnosis of Chronic Idiopathic Inflammatory Bowel Disease 1 GUIDELINES FOR THE INITIAL BIOPSY DIAGNOSIS OF CHRONIC IDIOPATHIC INFLAMMATORY BOWEL DISEASE A STRUCTURED
Guidelines for the Initial Biopsy Diagnosis of Chronic Idiopathic Inflammatory Bowel Disease 1 GUIDELINES FOR THE INITIAL BIOPSY DIAGNOSIS OF CHRONIC IDIOPATHIC INFLAMMATORY BOWEL DISEASE A STRUCTURED
BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease
 BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease David A Owen University of British Columbia CAUSES OF DIARRHEA DIARRHEA COLITIS PRESENT COLITIS ABSENT INFECTIOUS NON-INFECTIOUS
BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease David A Owen University of British Columbia CAUSES OF DIARRHEA DIARRHEA COLITIS PRESENT COLITIS ABSENT INFECTIOUS NON-INFECTIOUS
Pitfalls in the Diagnosis of Inflammatory Bowel Disease
 Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Case History B Female patient 1970 Clinical History : crampy abdominal pain and episodes of bloody diarrhea Surgical treatment
 Case History B-1325945 Female patient 1970 Clinical History : crampy abdominal pain and episodes of bloody diarrhea Surgical treatment Case History B-1325945 Pathology Submucosa & Muscularis Endometriosis
Case History B-1325945 Female patient 1970 Clinical History : crampy abdominal pain and episodes of bloody diarrhea Surgical treatment Case History B-1325945 Pathology Submucosa & Muscularis Endometriosis
Kids Like to Break the Rules: Gastrointestinal Pathology in Children
 Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
T he distinction between ulcerative colitis
 1233 REVIEW Indeterminate colitis M Guindi, R H Riddell... Indeterminate colitis (IC) originally referred to those 10 15% of cases of inflammatory bowel disease (IBD) in which there was difficulty distinguishing
1233 REVIEW Indeterminate colitis M Guindi, R H Riddell... Indeterminate colitis (IC) originally referred to those 10 15% of cases of inflammatory bowel disease (IBD) in which there was difficulty distinguishing
Patterns of Colonic Involvement at Initial Presentation in Ulcerative Colitis A Retrospective Study of 46 Newly Diagnosed Cases
 Anatomic Pathology / PATTERNS OF INVOLVEMENT IN ULCERATIVE COLITIS Patterns of Colonic Involvement at Initial Presentation in Ulcerative Colitis A Retrospective Study of 46 Newly Diagnosed Cases Marie
Anatomic Pathology / PATTERNS OF INVOLVEMENT IN ULCERATIVE COLITIS Patterns of Colonic Involvement at Initial Presentation in Ulcerative Colitis A Retrospective Study of 46 Newly Diagnosed Cases Marie
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
11/1/2017. Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota. Cerilli & Greenson
 Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota Acute infectious (self-limited) colitis Focal active colitis Pseudomembranous colitis Ischemic colitis Collagenous
Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota Acute infectious (self-limited) colitis Focal active colitis Pseudomembranous colitis Ischemic colitis Collagenous
The pathology of IBD and its modification by liver disease. Roger Feakins ESP/H-ECCO
 The pathology of IBD and its modification by liver disease Roger Feakins ESP/H-ECCO Enterprise Interest None IBD UC [IBDU] Crohn s IBD: distribution of disease Ulcerative colitis continuous Crohn s colitis
The pathology of IBD and its modification by liver disease Roger Feakins ESP/H-ECCO Enterprise Interest None IBD UC [IBDU] Crohn s IBD: distribution of disease Ulcerative colitis continuous Crohn s colitis
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Biopsy Evaluation of Non- Neoplastic Diseases of the Large Bowel: an algorithmic approach
 Biopsy Evaluation of Non- Neoplastic Diseases of the Large Bowel: an algorithmic approach Laura W. Lamps, M.D. Godfrey D. Stobbe Professor and Director of GI Pathology University of Michigan Health System
Biopsy Evaluation of Non- Neoplastic Diseases of the Large Bowel: an algorithmic approach Laura W. Lamps, M.D. Godfrey D. Stobbe Professor and Director of GI Pathology University of Michigan Health System
Review Histological evaluation in ulcerative colitis
 Gastroenterology Report 2 (2014) 178 192, doi:10.1093/gastro/gou031 Advance access publication 18 June 2014 Review Histological evaluation in ulcerative colitis Tom C. DeRoche 1, Shu-Yuan Xiao 2 and Xiuli
Gastroenterology Report 2 (2014) 178 192, doi:10.1093/gastro/gou031 Advance access publication 18 June 2014 Review Histological evaluation in ulcerative colitis Tom C. DeRoche 1, Shu-Yuan Xiao 2 and Xiuli
Pouchitis and Cuffitis A bloody mess. Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board
 Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
IATROGENIC AND DRUG INDUCED PATHOLOGY IN THE SMALL INTESTINE. Claude Cuvelier N. Goormaghtigh Institute of Pathology
 IATROGENIC AND DRUG INDUCED PATHOLOGY IN THE SMALL INTESTINE Claude Cuvelier N. Goormaghtigh Institute of Pathology Content Iatrogenic pathology Radiation Chemotherapy Graft-Versus-Host disease Changes
IATROGENIC AND DRUG INDUCED PATHOLOGY IN THE SMALL INTESTINE Claude Cuvelier N. Goormaghtigh Institute of Pathology Content Iatrogenic pathology Radiation Chemotherapy Graft-Versus-Host disease Changes
What is your diagnosis? a. Lymphocytic colitis. b. Collagenous colitis. c. Common variable immunodeficiency (CVID) associated colitis
 associated colitis") Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
The Morphologic Profile of Inflammatory Bowel Disease and the Diagnostic Problem of Crohn s Disease versus TB Colitis A Case Series
 OPEN ACCESS CASE REPORT The Morphologic Profile of Inflammatory Bowel Disease and the Diagnostic Problem of Crohn s Disease versus TB Colitis A Case Series Maria Lourdes Tilbe, Francia Victoria De Los
OPEN ACCESS CASE REPORT The Morphologic Profile of Inflammatory Bowel Disease and the Diagnostic Problem of Crohn s Disease versus TB Colitis A Case Series Maria Lourdes Tilbe, Francia Victoria De Los
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
INFLAMMATORY BOWEL DISEASE. Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic
 INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children
 Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Normal small intestine Variations
 THE HISTOPATHOLOGICAL DIAGNOSIS OF THE TERMINAL ILEUM BIOPSY K. Geboes, MD, PhD, AGAF, dr. H.C. Belgium Normal small intestine Variations Duodenum Ileum 1 Proliferative compartment Normal variations 2
THE HISTOPATHOLOGICAL DIAGNOSIS OF THE TERMINAL ILEUM BIOPSY K. Geboes, MD, PhD, AGAF, dr. H.C. Belgium Normal small intestine Variations Duodenum Ileum 1 Proliferative compartment Normal variations 2
CT Evaluation of Bowel Wall Thickening. Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University.
 CT Evaluation of Bowel Wall Thickening By Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University. The CT findings of bowel wall thickening includes 1 Degree of thickening.
CT Evaluation of Bowel Wall Thickening By Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University. The CT findings of bowel wall thickening includes 1 Degree of thickening.
Inflammatory Bowel Disease Ischemic bowel disease
 Inflammatory Bowel Disease Ischemic bowel disease Inflammatory Bowel Disease The two disorders that comprise IBD are: ulcerative colitis Crohn disease The distinction between ulcerative colitis and Crohn
Inflammatory Bowel Disease Ischemic bowel disease Inflammatory Bowel Disease The two disorders that comprise IBD are: ulcerative colitis Crohn disease The distinction between ulcerative colitis and Crohn
Original Article. Atypical histological features of ulcerative colitis. Siddharth N Shah, 1 Anjali D Amarapurkar, 1 N Shrinivas, 2 Rathi PM 2 ABSTRACT
 Tropical Gastroenterology 2011;32(2):107 111 Original Article Atypical histological features of ulcerative colitis Siddharth N Shah, 1 Anjali D Amarapurkar, 1 N Shrinivas, 2 Rathi PM 2 ABSTRACT Department
Tropical Gastroenterology 2011;32(2):107 111 Original Article Atypical histological features of ulcerative colitis Siddharth N Shah, 1 Anjali D Amarapurkar, 1 N Shrinivas, 2 Rathi PM 2 ABSTRACT Department
Crohn's disease and ulcerative colitis in the same patient
 Gut, 1983, 24, 857-862 Case report Crohn's disease and ulcerative colitis in the same patient C L WHITE III, S R HAMILTON, M P DIAMOND, AND J L CAMERON From the Departments of Pathology, Medicine, and
Gut, 1983, 24, 857-862 Case report Crohn's disease and ulcerative colitis in the same patient C L WHITE III, S R HAMILTON, M P DIAMOND, AND J L CAMERON From the Departments of Pathology, Medicine, and
Terumitsu; Nagayasu, Takeshi
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation A rare case of segmental ulcerative Tominaga, Tetsuro; Nonaka, Takashi; Shuichi; Kunizaki, Masaki; Sumida, Terumitsu; Nagayasu, Takeshi Acta medica
NAOSITE: Nagasaki University's Ac Title Author(s) Citation A rare case of segmental ulcerative Tominaga, Tetsuro; Nonaka, Takashi; Shuichi; Kunizaki, Masaki; Sumida, Terumitsu; Nagayasu, Takeshi Acta medica
What do we need for diagnosis of IBD
 What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
INTERNATIONAL COURSE ON THE PATHOLOGY OF THE DIGESTIVE SYSTEM VICTOR BABES NATIONAL INSTITUTE OF PATHOLOGY BUCHAREST 7-8 BUCHAREST 2014
 INTERNATIONAL COURSE ON THE PATHOLOGY OF THE DIGESTIVE SYSTEM VICTOR BABES NATIONAL INSTITUTE OF PATHOLOGY BUCHAREST 7-8 BUCHAREST 2014 Endoscopic biopsy samples of naïve colitides patients: Role of basal
INTERNATIONAL COURSE ON THE PATHOLOGY OF THE DIGESTIVE SYSTEM VICTOR BABES NATIONAL INSTITUTE OF PATHOLOGY BUCHAREST 7-8 BUCHAREST 2014 Endoscopic biopsy samples of naïve colitides patients: Role of basal
The Spectrum of IBD. Inflammatory Bowel Disease. Symptoms. Epidemiology. Tests for IBD. CD or UC? Inflamatory Bowel Disease. Fernando Vega, M.D.
 The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases?
 How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease
 The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
GRANULOMATOUS COLITIS: SIGNIFICANCE OF INVOLVEMENT OF THE TERMINAL ILEUM
 GASTROENTEROLOGY 64: 1071-1076, 1973 Copyright 1973 by The Williams & Wilkins Co. Vol. 64, No.6 Printed in U.S.A. GRANULOMATOUS COLITIS: SIGNIFICANCE OF INVOLVEMENT OF THE TERMINAL ILEUM JAMES A. NELSON,
GASTROENTEROLOGY 64: 1071-1076, 1973 Copyright 1973 by The Williams & Wilkins Co. Vol. 64, No.6 Printed in U.S.A. GRANULOMATOUS COLITIS: SIGNIFICANCE OF INVOLVEMENT OF THE TERMINAL ILEUM JAMES A. NELSON,
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue
 A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue UCSF Liver and Gastrointestinal Pathology Update Sept. 4, 2009 How to Go Wrong When Evaluating Small Bowel Biopsies, Based on
A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue UCSF Liver and Gastrointestinal Pathology Update Sept. 4, 2009 How to Go Wrong When Evaluating Small Bowel Biopsies, Based on
Ileo-rectal anastomosis for Crohn's disease of
 Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Endoscopic mucosal biopsies are useful in distinguishing granulomatous colitis due to Crohn s disease from tuberculosis
 Gut 1999;45:537 541 537 Wellcome Research Unit, Department of Gastrointestinal Sciences, Christian Medical College and Hospital, Vellore 632 004, Tamilnadu, India A B Pulimood B S Ramakrishna G Kurian
Gut 1999;45:537 541 537 Wellcome Research Unit, Department of Gastrointestinal Sciences, Christian Medical College and Hospital, Vellore 632 004, Tamilnadu, India A B Pulimood B S Ramakrishna G Kurian
MicroRNA expression patterns in indeterminate inflammatory bowel disease
 148 & 2013 USCAP, Inc All rights reserved 0893-3952/13 $32.00 MicroRNA expression patterns in indeterminate inflammatory bowel disease Jingmei Lin 1, Qi Cao 2, Jianjun Zhang 3, Yong Li 2, Bo Shen 4, Zijin
148 & 2013 USCAP, Inc All rights reserved 0893-3952/13 $32.00 MicroRNA expression patterns in indeterminate inflammatory bowel disease Jingmei Lin 1, Qi Cao 2, Jianjun Zhang 3, Yong Li 2, Bo Shen 4, Zijin
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Interpretation of inflammatory colorectal biopsies has
 The of Colitis in Endoscopic Biopsy Specimens A Review Article Lisa A. Cerilli, MD; Joel K. Greenson, MD Context. A variety of inflammatory disorders may affect the colon, with widely differing clinical
The of Colitis in Endoscopic Biopsy Specimens A Review Article Lisa A. Cerilli, MD; Joel K. Greenson, MD Context. A variety of inflammatory disorders may affect the colon, with widely differing clinical
study was undertaken to assess the epidemiology, course and outcome of UC patients attending a hospital in Jordan.
 Ulcerative colitis (UC) is a relatively uncommon, chronic, recurrent inflammatory disease of the colon or rectal mucosa [1]. Often a lifelong illness, the condition can have a profound emotional and social
Ulcerative colitis (UC) is a relatively uncommon, chronic, recurrent inflammatory disease of the colon or rectal mucosa [1]. Often a lifelong illness, the condition can have a profound emotional and social
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Chapter 8 Ischemic Colitis
 Chapter 8 Ischemic Colitis Peter Van Eyken, Daniela Fanni, and Clara Gerosa Abstract The large bowel accounts for roughly half of all episodes of gastrointestinal ischemia. Three major manifestations of
Chapter 8 Ischemic Colitis Peter Van Eyken, Daniela Fanni, and Clara Gerosa Abstract The large bowel accounts for roughly half of all episodes of gastrointestinal ischemia. Three major manifestations of
GASTROENTEROLOGY. Official Publication of the American Gastroenterological Association. CoPYRIGHT 1975 THE WILLIAMS & WILKINS Co.
 GASTROENTEROLOGY Official Publication of the American Gastroenterological Association CoPYRIGHT 1975 THE WILLIAMS & WILKINS Co. Vol68 April 1975 Number 4 ALIMENTARY TRACT CLINICAL PATTERNS IN CROHN'S DISEASE:
GASTROENTEROLOGY Official Publication of the American Gastroenterological Association CoPYRIGHT 1975 THE WILLIAMS & WILKINS Co. Vol68 April 1975 Number 4 ALIMENTARY TRACT CLINICAL PATTERNS IN CROHN'S DISEASE:
ABC of Colorectal Diseases
 ABC of Colorectal Diseases NON-SPECIFIC INFLAMMATORY BOWEL DISEASE S Pettit, M H Irving Non-specific inflammatory bowel diseases are those for which there is no discernible aetiological agent. The two
ABC of Colorectal Diseases NON-SPECIFIC INFLAMMATORY BOWEL DISEASE S Pettit, M H Irving Non-specific inflammatory bowel diseases are those for which there is no discernible aetiological agent. The two
Index. Surg Clin N Am 87 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
11/13/11. Biologics for CD and CUC: The Impact on Surgical Outcomes. Principles of Successful Intestinal Surgery
 Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
The granuloma in Crohn's disease
 The granuloma in Crohn's disease T. J. CHAMBERS AND B. C. MORSON From the Department ofpathology, St Mark's Hospital, London Gut 1979, 2, 269-274 SUMMARY The number of granulomas in sections of bowel involved
The granuloma in Crohn's disease T. J. CHAMBERS AND B. C. MORSON From the Department ofpathology, St Mark's Hospital, London Gut 1979, 2, 269-274 SUMMARY The number of granulomas in sections of bowel involved
Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent
 Gastroenterology Research and Practice Volume 2010, Article ID 860394, 4 pages doi:10.1155/2010/860394 Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent Jessica
Gastroenterology Research and Practice Volume 2010, Article ID 860394, 4 pages doi:10.1155/2010/860394 Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent Jessica
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis
 doi: 10.2169/internalmedicine.1607-18 http://internmed.jp CASE REPORT A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis Rumiko Tsuboi,
doi: 10.2169/internalmedicine.1607-18 http://internmed.jp CASE REPORT A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis Rumiko Tsuboi,
Mimics of Inflammatory Bowel Disease. Dr Catriona McKenzie Royal Prince Alfred Hospital, Camperdown
 Mimics of Inflammatory Bowel Disease Dr Catriona McKenzie Royal Prince Alfred Hospital, Camperdown Mimics of IBD: Overview Infections Drugs Autoimmune Other Infections Diagnostic Histopathology, 2015 Case
Mimics of Inflammatory Bowel Disease Dr Catriona McKenzie Royal Prince Alfred Hospital, Camperdown Mimics of IBD: Overview Infections Drugs Autoimmune Other Infections Diagnostic Histopathology, 2015 Case
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND. Fabrizio Parente
 NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
Inflammatory Bowel Disease: Updates and Controversies CASE #1 CASE #1 8/6/2015. What is the most likely diagnosis?
 Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Oncologist-induced Disease of the GI tract: New Developments
 Oncologist-induced Disease of the GI tract: New Developments Jeffrey D Goldsmith, MD Children s Hospital Boston, Beth Israel Deaconess Medical Center, Harvard Medical School Boston, MA Everyone s on drugs
Oncologist-induced Disease of the GI tract: New Developments Jeffrey D Goldsmith, MD Children s Hospital Boston, Beth Israel Deaconess Medical Center, Harvard Medical School Boston, MA Everyone s on drugs
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Focally Enhanced Gastritis in Newly Diagnosed Pediatric Inflammatory Bowel Disease
 Focally Enhanced Gastritis in Newly Diagnosed Pediatric Inflammatory Bowel Disease The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters
Focally Enhanced Gastritis in Newly Diagnosed Pediatric Inflammatory Bowel Disease The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
The revised Porto criteria for diagnosing
 R E S E A R C H P A P E R Long-term Outcome of Inflammatory Bowel Disease Unclassified in Children SIBA PROSAD PAUL AND BHUPINDER KAUR SANDHU From Bristol Royal Hospital for Children, Upper Maudlin Street,
R E S E A R C H P A P E R Long-term Outcome of Inflammatory Bowel Disease Unclassified in Children SIBA PROSAD PAUL AND BHUPINDER KAUR SANDHU From Bristol Royal Hospital for Children, Upper Maudlin Street,
Segmental colonoscopic biopsies in the differentiation of ileocolic tuberculosis from Crohn s disease
 Blackwell Science, LtdOxford, UKJGHJournal of Gastroenterology and Hepatology0815-93192005 Blackwell Publishing Asia Pty LtdMay 2005205688696Original ArticleSegmental biopsies in and Crohn s diseaseab
Blackwell Science, LtdOxford, UKJGHJournal of Gastroenterology and Hepatology0815-93192005 Blackwell Publishing Asia Pty LtdMay 2005205688696Original ArticleSegmental biopsies in and Crohn s diseaseab
children Crohn s disease in MR enterography for GI Complications Microscopy Characterization Primary sclerosing cholangitis Anorectal fistulae
 MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Diagnostic difficulty arising from rectal recovery
 J Clin Pathol 1996;49:319-323 319 Cellular Pathology, Northwick Park and St Mark's NHS Trust, Harrow T S Levine A B Price Gastroenterology S Mitchell Histopathology, Heraklion University General Hospital,
J Clin Pathol 1996;49:319-323 319 Cellular Pathology, Northwick Park and St Mark's NHS Trust, Harrow T S Levine A B Price Gastroenterology S Mitchell Histopathology, Heraklion University General Hospital,
Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma?
 17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
Surgical Treatment of Inflammatory Bowel Disease (IBD)
") Surgical Treatment of Inflammatory Bowel Disease (IBD) JMAJ 45(2): 55 62, 2002 Tetsuichiro MUTO Vice-Director, Cancer Institute Hospital Abstract: IBD, especially ulcerative colitis (UC) and Crohn s disease
Surgical Treatment of Inflammatory Bowel Disease (IBD) JMAJ 45(2): 55 62, 2002 Tetsuichiro MUTO Vice-Director, Cancer Institute Hospital Abstract: IBD, especially ulcerative colitis (UC) and Crohn s disease
2015 복영증례 51/M C.C. Past Hx: DM, HTN (1998), Lab: WBC (11500/ μl ), CRP (0.71 mg/dl) 순천향서울병원황지영, 홍성숙 APCT (HAD #1) APCT (HAD#1) APCT (HAD #15)
, Lab: WBC (11500/ μl ), CRP (0.71 mg/dl) 순천향서울병원황지영, 홍성숙 APCT (HAD #1) APCT (HAD#1) APCT (HAD #15)") Case 1 2015 복영증례 순천향서울병원황지영, 홍성숙 51/M C.C Abdominal pain and chilling (1 week ago) Diarrhea (a month ago) Past Hx: DM, HTN (1998), Alcoholic liver disease (2008) Lab: WBC (11500/ μl ), CRP (0.71 mg/dl)
Case 1 2015 복영증례 순천향서울병원황지영, 홍성숙 51/M C.C Abdominal pain and chilling (1 week ago) Diarrhea (a month ago) Past Hx: DM, HTN (1998), Alcoholic liver disease (2008) Lab: WBC (11500/ μl ), CRP (0.71 mg/dl)
Endoscopy in IBD. F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M.
 Frankfurt/M.") F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
Research Article Temporary Fecal Diversion in the Management of Colorectal and Perianal Crohn s Disease
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Crohn's disease CAUSES COURSE OF CROHN'S DISEASE TREATMENT. Sulfasalazine
 Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
For the past 40 years, it has been standard practice to obtain
 ORIGINAL ARTICLE: GASTROENTEROLOGY Good Agreement Between Endoscopic Findings and Biopsy Reports Supports Limited Tissue Sampling During Pediatric Colonoscopy Michael A. Manfredi, Hongyu Jiang, Lawrence
ORIGINAL ARTICLE: GASTROENTEROLOGY Good Agreement Between Endoscopic Findings and Biopsy Reports Supports Limited Tissue Sampling During Pediatric Colonoscopy Michael A. Manfredi, Hongyu Jiang, Lawrence
Crohn's disease of the colon and its distinction from diverticulitis
 Crohn's disease of the colon and its distinction from diverticulitis G. T. SCHMIDT, J. E. LENNARD-JONES, B. C. MORSON, AND A. C. YOUNG From St. Mark's Hospital, London Crohn's disease may affect segments
Crohn's disease of the colon and its distinction from diverticulitis G. T. SCHMIDT, J. E. LENNARD-JONES, B. C. MORSON, AND A. C. YOUNG From St. Mark's Hospital, London Crohn's disease may affect segments
Restorative proctocolectomy with ileal reservoir: pathological and histochemical study of mucosal biopsy specimens
 J Clin Pathol 1987;40:601-607 Restorative proctocolectomy with ileal reservoir: pathological and histochemical study of mucosal biopsy specimens N A SHEPHERD,* J R JASS,*t I DUVAL,T R L MOSKOWITZ,t R J
J Clin Pathol 1987;40:601-607 Restorative proctocolectomy with ileal reservoir: pathological and histochemical study of mucosal biopsy specimens N A SHEPHERD,* J R JASS,*t I DUVAL,T R L MOSKOWITZ,t R J
ISPUB.COM. Quick Review: Crohn's Disease. T Fujii, B Phillips DEFINITION ETIOLOGY
 ISPUB.COM The Internet Journal of Gastroenterology Volume 2 Number 1 Quick Review: Crohn's Disease T Fujii, B Phillips Citation T Fujii, B Phillips. Quick Review: Crohn's Disease. The Internet Journal
ISPUB.COM The Internet Journal of Gastroenterology Volume 2 Number 1 Quick Review: Crohn's Disease T Fujii, B Phillips Citation T Fujii, B Phillips. Quick Review: Crohn's Disease. The Internet Journal
Crohn's disease: natural history and treatment J. E. LENNARD-JONES. College and St Mark's Hospitals, London
 Postgrad. med. J. (September 1968) 44, 674-678. University Crohn's disease: natural history and treatment J. E. LENNARD-JONES AN EXrENSIVE literature is now available on the pathological anatomy and its
Postgrad. med. J. (September 1968) 44, 674-678. University Crohn's disease: natural history and treatment J. E. LENNARD-JONES AN EXrENSIVE literature is now available on the pathological anatomy and its
GRANULOMATOUS COLITIS AND ATYPICAL ULCERATIVE COLITIS
 GASTROENTEROLOGY Copyright 1966 by The Williams & Wilkin. Co. Vol. 50, No.2 Printed in U.S.A. GRANULOMATOUS COLITIS AND ATYPICAL ULCERATIVE COLITIS Histological features, behavior, and prognosis K. LEWIN,
GASTROENTEROLOGY Copyright 1966 by The Williams & Wilkin. Co. Vol. 50, No.2 Printed in U.S.A. GRANULOMATOUS COLITIS AND ATYPICAL ULCERATIVE COLITIS Histological features, behavior, and prognosis K. LEWIN,
Chronic Colitis Pattern Christina A. Arnold, M.D. The Ohio State University Wexner Medical Center Columbus, Ohio
 Chronic Colitis Pattern Christina A. Arnold, M.D. The Ohio State University Wexner Medical Center Columbus, Ohio Identify this medication resin: A. Bile Acid Sequestrant B. Kayexalate C. Sevelamer D. Renvela
Chronic Colitis Pattern Christina A. Arnold, M.D. The Ohio State University Wexner Medical Center Columbus, Ohio Identify this medication resin: A. Bile Acid Sequestrant B. Kayexalate C. Sevelamer D. Renvela
Fibrin thrombi, a cause of clindamycin-associated
 Gut, 1976, 17, 483487 Fibrin thrombi, a cause of clindamycin-associated colitis? W. V. BOGOMOLETZ From the Department of Pathology, Queen Mary's Hospital, London summary Rectal biopsies from five patients
Gut, 1976, 17, 483487 Fibrin thrombi, a cause of clindamycin-associated colitis? W. V. BOGOMOLETZ From the Department of Pathology, Queen Mary's Hospital, London summary Rectal biopsies from five patients
-2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency
 rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency") SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה
 ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
An Unusual Complication of Crohn s Disease. Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008
 An Unusual Complication of Crohn s Disease Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008 Case Presentation 70 year old lady k/c of Crohns disease h/o of Hartmann s procedure
An Unusual Complication of Crohn s Disease Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008 Case Presentation 70 year old lady k/c of Crohns disease h/o of Hartmann s procedure
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
DIGESTIVE TRACT ESOPHAGUS
 DIGESTIVE TRACT From the lower esophagus to the lower rectum four fundamental layers comprise the wall of the digestive tube: mucosa, submucosa, muscularis propria (externa), and adventitia or serosa (see
DIGESTIVE TRACT From the lower esophagus to the lower rectum four fundamental layers comprise the wall of the digestive tube: mucosa, submucosa, muscularis propria (externa), and adventitia or serosa (see
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX
 Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Non-Neoplastic Disorders. of the Intestines. Laura W. Lamps, M.D. University of Arkansas Little Rock, AR
 Non-Neoplastic Disorders Laura W. Lamps, M.D. University of Arkansas Little Rock, AR Audrey J. Lazenby, M.D. University of Alabama Birmingham, AL Joel K. Greenson, M.D. University of Michigan Ann Arbor,
Non-Neoplastic Disorders Laura W. Lamps, M.D. University of Arkansas Little Rock, AR Audrey J. Lazenby, M.D. University of Alabama Birmingham, AL Joel K. Greenson, M.D. University of Michigan Ann Arbor,
ANATOMIC PATHOLOGY Original Article
 ANATOMIC PATHOLOGY Original Article Histology of the Mucosa in Sigmoid Colon Specimens With Diverticular Disease Observations for the Interpretation of Sigmoid Colonoscopic Biopsy Specimens NEAL S. GOLDSTEIN,
ANATOMIC PATHOLOGY Original Article Histology of the Mucosa in Sigmoid Colon Specimens With Diverticular Disease Observations for the Interpretation of Sigmoid Colonoscopic Biopsy Specimens NEAL S. GOLDSTEIN,
Opportunistic Infections of the Colon in
 Opportunistic Infections of the Colon in Inflammatory Bowel Disease Dr SM Bigby Laboratory Services, Middlemore Hospital, Auckland Second European Consensus on prevention, diagnosis and management of infections
Opportunistic Infections of the Colon in Inflammatory Bowel Disease Dr SM Bigby Laboratory Services, Middlemore Hospital, Auckland Second European Consensus on prevention, diagnosis and management of infections
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Treating Crohn s and Colitis in the ASC
 Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
Rectal biopsy as an aid to cancer control in ulcerative colitis
 Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a