Rectal Prolapse: A 10-Year Experience
|
|
|
- Silvester Owens
- 5 years ago
- Views:
Transcription
1 24 The Ochsner Journal

2 Volume 7, Number 1, Spring
 A. B. the patient lean forward or using a long rod to which a mirror is attached placed between the patient s legs to view the prolapse.")
3 Rectal Prolapse: A 10-Year Experience Figure 2. Physical examination. A. Concentric folds of prolapsed rectum. B. Radial folds of hemorrhoids (mucosal prolapse). (From Beck DE, Whitlow CB. Rectal prolapse and intussusception. In Beck DE, ed. Handbook of Colorectal Surgery, 2nd ed. New York: Marcel Dekker, 2003: With permission.) A. B. the patient lean forward or using a long rod to which a mirror is attached placed between the patient s legs to view the prolapse. Another option is to place a flexible endoscope into the toilet with the viewing end pointed toward the perineum. Full-thickness prolapse is distinguished by its concentric rings and grooves as opposed to the radially oriented grooves associated with mucosal prolapse (Fig. 2). Inspection should also include examining the perianal skin for any maceration or excoriations. A thorough digital rectal examination is important to detect concomitant anal pathology and to determine adequacy of resting tone and squeeze pressure of the anal sphincters and function of the puborectalis muscle. All patients with rectal prolapse should have endoscopic examination of the colon and rectum. The entire colon should be evaluated prior to any surgery on that organ by colonoscopy or by the combination of sigmoidoscopy and an air contrast barium enema. A biopsy should be performed for any abnormalities. Proctitis, colitis cystica profunda, and solitary rectal ulceration are conditions found in patients with prolapse that may require biopsy to differentiate them from rectal neoplasms or inflammatory bowel disease (11). In patients who present with significant constipation in addition to prolapse, a colonic transit marker study is indicated. After the patient ingests a capsule containing 24 radiopaque rings, a plain abdominal radiograph is obtained within 24 hours of ingestion and again at one, three and five days later. Normal patients should have no more than four rings remaining at five days. At seven days, no rings should remain. Abnormal results fall into one of two patterns: pancolonic slow transit (colonic inertia) with rings distributed throughout the colon, or pelvic outlet obstruction with clustering of the remaining rings in the rectosigmoid. Either pattern may be seen in patients with prolapse (12). Occult rectal prolapse should be suspected in patients with symptoms of tenesmus, incomplete evacuation, fecal impaction, or unexplained constipation, or those found to have the solitary rectal ulcer syndrome. Defecography should be performed to confirm this diagnosis (13). Sigmoidorectal intussusception, puborectalis function, and perineal descent may be evaluated using this technique. A standard caulking gun is used to instill 200 ml of barium paste into the rectum. The patient sits on a radiolucent commode, and defecation is recorded with cineradiography or fluoroscopy with video recording. Variable amounts of sphincter dysfunction have been found in patients with rectal prolapse using anorectal manometry. In two studies, resting and squeeze pressures were shown to be lower in prolapse patients than in control subjects (14,15). In addition, Metcalf and Loenig-Baucke (14) found that patients with prolapse had decreased rectal capacity, as measured by decreased critical volume (mean rectal volume producing a lasting urge to defecate), decreased volume to produce constant relaxation, and decreased volume on the saline incontinence test. These findings, along with the decreased sphincter pressures, may explain why many prolapse patients experience incontinence before the sensation of the urge to defecate. Two studies have failed to show a return to normal of resting or squeeze pressures following repair of prolapse by rectopexy (16,17). Pudendal nerve terminal motor latency is also lengthened in patients with rectal prolapse, suggesting that nerve stretch contributes to sphincter dysfunction (18). The studies described play an important role in our understanding of the causes of prolapse and incontinence associated with prolapse. Few studies have thoroughly evaluated treatment options based on the results of preoperative and postoperative physiologic testing. Treatment The choice of surgical treatment for rectal prolapse depends on the condition of the patient, preoperative anatomic and physiologic testing, presence of incontinence or constipation, prior prolapse repairs, and the surgeon s preference. Over 50 surgical procedures for the correction of rectal prolapse have been described (3,5). Control of prolapse and restoration of the underlying anatomic support mechanisms are the objectives of surgical intervention. These objectives can be achieved by resection and/or fixation of the 26 The Ochsner Journal
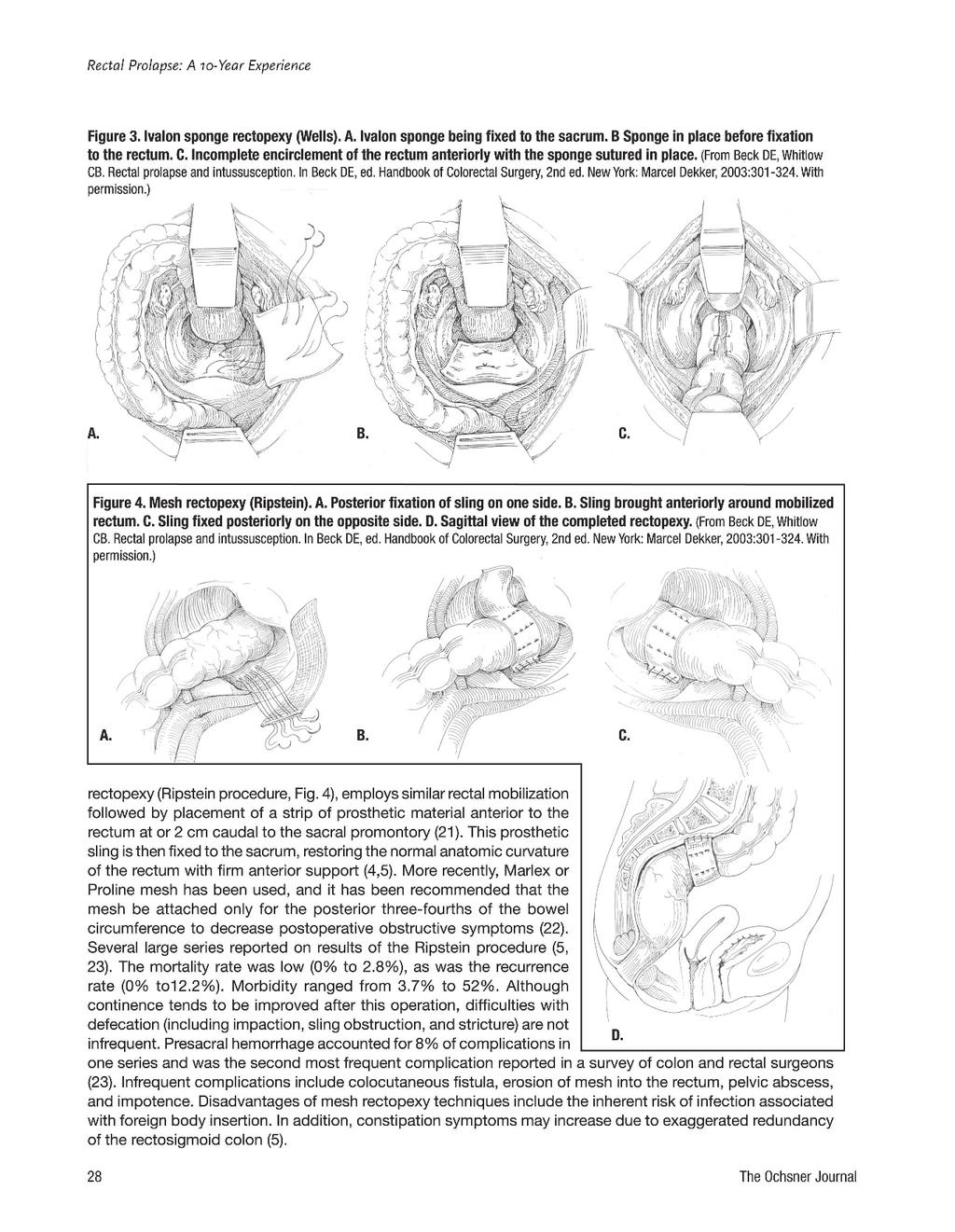
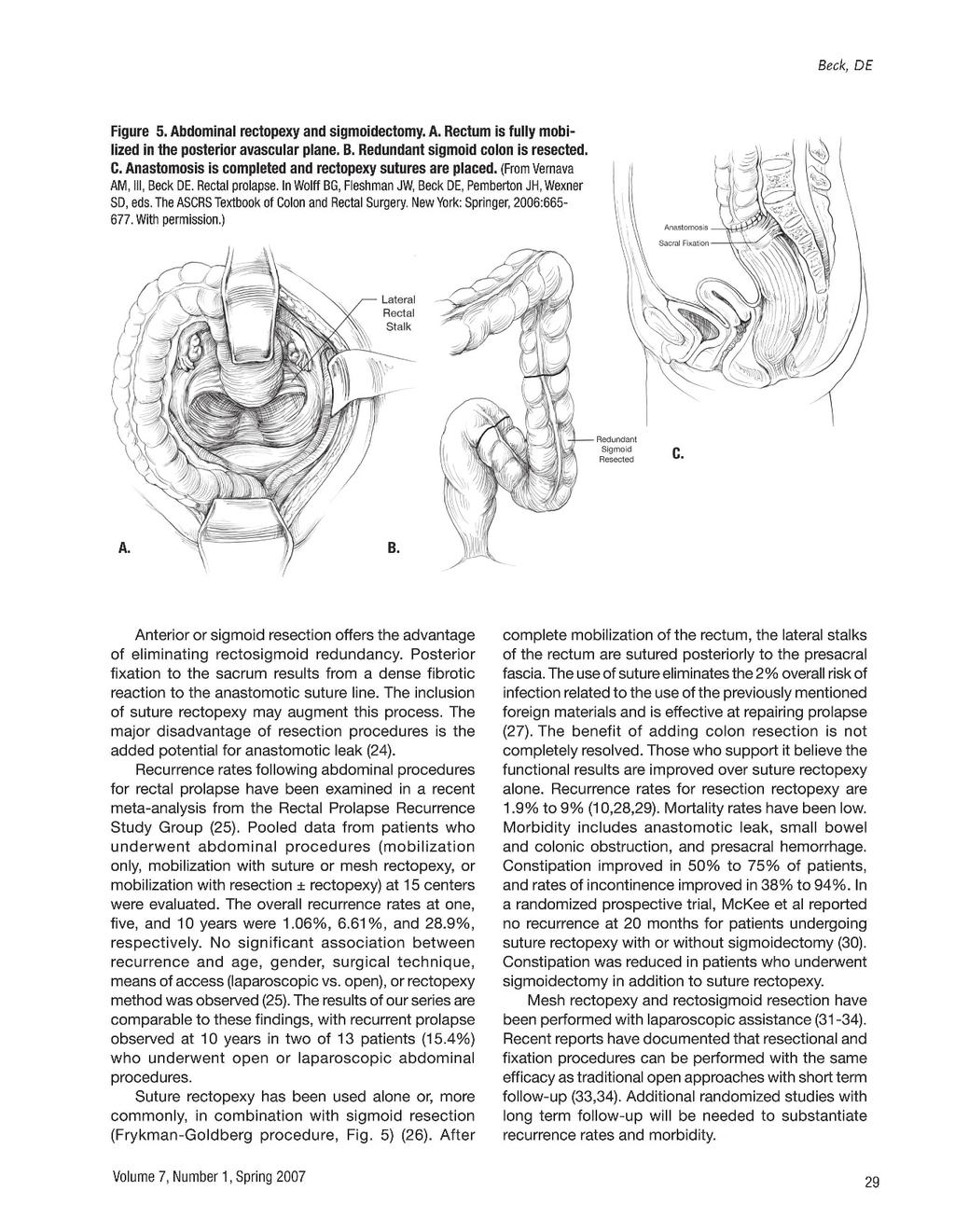
4 Beck, DE Table 1. Treatment options. Treatment Advantages Disadvantages Abdominal Anterior resection Low recurrence Resection required Ripstein mesh sling No resection Impaction, constipation, foreign body Well s Ivalon sponge No resection Constipation persists, foreign body Orr-Loygue No resection Constipation persists Sigmoid colectomy Low recurrence Resection required with suture rectopexy Perineal Altemeier (perineal Low morbidity/mortality, General/regional anesthesia, rectosigmoidectomy) low recurrence continued incontinence, anastomosis Altemeier with Low morbidity/mortality, General/regional anesthesia, levatorplasty low recurrence, incontinence improved anastomosis Delorme procedure Low morbidity/mortality, High recurrence rates, local anesthesia continued incontinence Thiersch anal Low morbidity/mortality, Fecal impaction, encirclement local anesthesia infection, wire breakage, erosion rectum to the sacrum. Surgical repair of full-thickness rectal prolapse can be accomplished by perineal or transabdominal techniques. Perineal approaches have less morbidity associated with them, but in general have high recurrence rates, and have therefore been typically reserved for high-risk elderly patients. Comparison of results from various series in patients with prolapse can be confusing. Some series record recurrence only in patients with full-thickness prolapse, whereas others include both full-thickness and mucosal prolapse. Length of follow-up differs from one report to another; those with longer follow-up report recurrences as late as 16 years postoperatively (19). Incontinence and constipation may be improved or worsened by most procedures. When comparing the effects of a procedure on bowel or sphincter function, it is important to note the preoperative status of patients. This is often omitted or recorded with different endpoints, making comparison between series impossible. Preoperative preparation was the same for most prolapse operations: a mechanical and antibiotic bowel preparation the day before surgery and perioperative broad-spectrum intravenous antibiotics. Patients undergoing an abdominal procedure were placed in the supine modified lithotomy position. Perineal procedures were performed in the prone-jackknife, lithotomy, or left lateral positions. A Foley catheter should be placed in all patients before the operation begins. Operative treatment options, along with their respective advantages and disadvantages, are summarized in Table 1. Abdominal Procedures Abdominal procedures for rectal prolapse are an excellent option for patients who are fit to undergo laparotomy. Surgical techniques may include mobilization and resection of the rectosigmoid colon, fixation of the rectum to the sacrum, or a combination of these procedures. Rectopexy alone can be performed using suture material or prosthetic mesh. Suture rectopexy involves thorough rectal mobilization to the level of the levators, followed by upward suture fixation of the rectum to the presacral fascia. Posterior mesh rectopexy (Wells procedure, Fig. 3) utilizes prosthetic material, such as polypropylene or Marlex mesh, to augment rectal fixation to the sacral promontory (20). An alternative technique, the anterior sling Volume 7, Number 1, Spring
5
6

7 Rectal Prolapse: A 10-Year Experience Figure 6. Perineal rectosigmoidectomy (Altemeier). A, B. Incision of rectal wall. C. Division of vessel adjacent to bowel wall. D. Mesenteric vessels ligated. Stay sutures previously placed in distal edge of outer cylinder are placed in cut edge of inner cylinder. E. Anastomosis of distal aspect of remaining colon to the short rectal stump. (From Beck DE, Whitlow CB. Rectal prolapse and intussusception. In Beck DE, ed. Handbook of Colorectal Surgery, 2nd ed. New York: Marcel Dekker, 2003: With permission.) A. B. C. Perineal Procedures In the late 19th and early 20th centuries, several perineal procedures for the treatment of prolapse were described (24). Their use declined as abdominal surgery under general anesthesia became safe and it became clear that recurrence rates were lower with abdominal repairs. However, these procedures still play a role for the elderly with significant medical problems, for whom a major abdominal procedure carries a prohibitive risk. In addition, modern trends toward minimizing invasiveness and outpatient management have led to an increasing number of these procedures being performed in young and low-risk patients. The two most commonly performed perineal-based procedures are the Altemeier procedure and the Delorme procedure. Both procedures may be performed under general, spinal, or local anesthesia with the patient in prone-jackknife, lithotomy, or left lateral decubitus positions. The Altemeier technique (perineal rectosigmoidectomy) requires exteriorization of the prolapse followed by a circumferential incision through all layers of the rectal wall 1-2 cm cephalad to the dentate line (Fig. 6). The rectum is further delivered using gentle downward traction, and circumferential dissection with division and ligation of the mesentery is continued until no additional intestinal prolapse can be achieved. If the pouch of Douglas is encountered anteriorly, the hernia sac is opened and a high ligation may be performed. A levator repair can be performed anterior and/or posterior to the rectum. At this point, the bowel is divided and an anastomosis is created between the cut end and the rectal stump with sutures or staples (35,36). A regular diet is allowed on postoperative day 1, and the Foley catheter is generally removed by postoperative day 1 or 2. Mortality in several series has been extremely low, and D. E. morbidity ranged from 0% to 25%. Complications are mostly medical but have included anastomotic dehiscence and bleeding. Recurrence rates have been reported between 0% and 10%. Incontinence has improved in a large percentage of patients in series in which levatorplasty has been used (36). A randomized trial by Deen et al compared abdominal resection and rectopexy with perineal rectosigmoidectomy with pelvic floor repair in patients older than 50 years of age (37). There were no deaths or anastomotic leaks. One patient developed an anastomotic stricture following perineal rectosigmoidectomy. There was one recurrence in the perineal group, and none in the abdominal group, at a median follow-up of 17 months. More patients who underwent perineal rectosigmoidectomy experienced fecal soiling (six, versus two in the abdominal 30 The Ochsner Journal
.")
. The mucosa edges are then sutured together (Fig. 7).")
8 Beck, DE resection group). Maximal resting and maximal squeeze pressure decreased postoperatively after perineal repair. These pressures increased after abdominal repair. The advantage of perineal rectosigmoidectomy was a shorter hospital stay (mean 5 days versus 11 days, p < 0.05). Delorme s procedure is performed in a similar manner, except that only the mucosa and submucosal layers are dissected off the muscularis, divided, and excised. The muscular bowel wall remains intact and is plicated within interrupted sutures, reapproximating the cut edges of mucosa (35,36). The mucosa edges are then sutured together (Fig. 7). The Delorme procedure has also been used for internal prolapse. Recent series have shown a mortality rate for the Delorme procedure of 0% to 2.5% when it is performed on elderly patients who have significant medical problems (24). Morbidity (4% to 33%) has included bleeding, anastomotic dehiscence, stricture, diarrhea, and urinary retention. Recurrence rates have ranged from 7% to 22%, and recurrences have frequently been treated with a repeat Delorme procedure. Incontinence improved in 40% to 50% of patients who were incontinent preoperatively, and generally incontinence was not worsened by the procedure. Constipation was not a problem in most series. The postoperative convalescence following perineal procedures for rectal prolapse is typically shorter than that which should be expected following a laparatomy. Patients are permitted to ambulate and begin a regular diet on postoperative day 1, and are discharged within 2 to 3 days, as demonstrated in our current series. The major disadvantage of these techniques is a higher rate of recurrent prolapse (0%-16% for Altemeier, 4%-38% for Delorme) (35-38). Similar results were demonstrated by our current series, with an overall 10-year recurrence rate of 16% (16.7% for Altemeier, 14.3% for Delorme) observed. CONCLUSION Rectal prolapse and intussusception are infrequently encountered problems. The causes of prolapse, as well as its ideal treatment, remain uncertain. Selection of the best procedure for a given patient depends on the patient s medical condition, the presence of incontinence or constipation, and prior surgery for prolapse. The surgeon weighs these factors, along with a knowledge of the available surgical options, to arrive at a treatment decision. Our group has demonstrated proficiency in the surgical management of rectal prolapse over the past 10 years, with recurrence rates for abdominal and perineal-based procedures comparable to those previously reported in the surgical literature. Figure 7. Mucosal proctectomy (Delorme). A. Subcutaneous infiltration of dilute epinephrine solution. B. Circumferential mucosal incision. C. Dissection of mucosa off muscular layer. D. Plicating stitch approximating cut edge of mucosa, muscular wall, and mucosa just proximal to dentate line. E. Plicating stitch tied. F. Completed anastomosis. (From Beck DE, Whitlow CB. Rectal prolapse and intussusception. In Beck DE, ed. Handbook of Colorectal Surgery, 2nd ed. New York: Marcel Dekker, 2003: With permission.) A. B. C. D. E. F. Volume 7, Number 1, Spring
9 32 The Ochsner Journal
Summary and conclusion. Summary And Conclusion
 Summary And Conclusion Summary and conclusion Rectal prolapse remain a disorder for which no single ideal treatment was approved for all cases. Complete rectal prolapse (procidentia) is the circumferential
Summary And Conclusion Summary and conclusion Rectal prolapse remain a disorder for which no single ideal treatment was approved for all cases. Complete rectal prolapse (procidentia) is the circumferential
Hemorrhoids. Carlos R. Alvarez-Allende PGY-III Colorectal Surgery
 Hemorrhoids Carlos R. Alvarez-Allende PGY-III Colorectal Surgery Overview Anatomy Classification Etiology Incidence Symptoms Differential Diagnosis Medical Management Surgical Management Anatomy Anal canal
Hemorrhoids Carlos R. Alvarez-Allende PGY-III Colorectal Surgery Overview Anatomy Classification Etiology Incidence Symptoms Differential Diagnosis Medical Management Surgical Management Anatomy Anal canal
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Colorectal procedure guide
 Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com 2 INDEX Anal fistula repair Using the Biodesign plug with no button.... 4 Anal fistula repair Using
Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com 2 INDEX Anal fistula repair Using the Biodesign plug with no button.... 4 Anal fistula repair Using
Although disparate topics, these two different pathologic
 34 H E M O R R H O I D S A N D R E C T A L P R O L A P S E CHARLES N. HEADRICK MICHAEL J. STAMOS Although disparate topics, these two different pathologic entities are commonly misdiagnosed by both layperson
34 H E M O R R H O I D S A N D R E C T A L P R O L A P S E CHARLES N. HEADRICK MICHAEL J. STAMOS Although disparate topics, these two different pathologic entities are commonly misdiagnosed by both layperson
Robotic Ventral Rectopexy
 Robotic Ventral Rectopexy What is a robotic ventral rectopexy? The term rectopexy refers to an operation in which the rectum (the part of the bowel nearest the anus) is put back into its normal position
Robotic Ventral Rectopexy What is a robotic ventral rectopexy? The term rectopexy refers to an operation in which the rectum (the part of the bowel nearest the anus) is put back into its normal position
Pelvic Floor Disorders. Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon
 Consultant Colorectal and General Surgeon") Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Fecal Incontinence. What is fecal incontinence?
 Scan for mobile link. Fecal Incontinence Fecal incontinence is the inability to control the passage of waste material from the body. It may be associated with constipation or diarrhea and typically occurs
Scan for mobile link. Fecal Incontinence Fecal incontinence is the inability to control the passage of waste material from the body. It may be associated with constipation or diarrhea and typically occurs
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Prolaps: Anteriore Rektopexie nach D Hoore. Prof. Dr. med. F. Hetzer
 Prolaps: Anteriore Rektopexie nach D Hoore Prof. Dr. med. F. Hetzer franc.hetzer@spital-linth.ch Rectal prolapse pathophysiology 24 22 20 18 congenital female pathology (90%) 16 14 straining weakened pelvic
Prolaps: Anteriore Rektopexie nach D Hoore Prof. Dr. med. F. Hetzer franc.hetzer@spital-linth.ch Rectal prolapse pathophysiology 24 22 20 18 congenital female pathology (90%) 16 14 straining weakened pelvic
Outlet syndrome: is there a surgical option?'
 Journal of the Royal Society of Medicine Volume 77 July 1984 559 Outlet syndrome: is there a surgical option?' M R B Keighley MS FRCS P Shouler FRCS Department of Surgery, General Hospital, Birmingham
Journal of the Royal Society of Medicine Volume 77 July 1984 559 Outlet syndrome: is there a surgical option?' M R B Keighley MS FRCS P Shouler FRCS Department of Surgery, General Hospital, Birmingham
Diagnosis of Impaired Defecatory Function with Special Reference to Physiological Tests
 Defecatory Dysfunction Diagnosis of Impaired Defecatory Function with Special Reference to Physiological Tests JMAJ 46(9): 373 377, 2003 Masatoshi OYA, Masashi UENO, and Tetsuichiro MUTO Department of
Defecatory Dysfunction Diagnosis of Impaired Defecatory Function with Special Reference to Physiological Tests JMAJ 46(9): 373 377, 2003 Masatoshi OYA, Masashi UENO, and Tetsuichiro MUTO Department of
TYPES OF RECTAL PROLAPSE
 RECTAL PROLPASE Rectal prolapse describes a condition where either the lining or entire wall of the rectum becomes loose and falls into, or even out of, the rectum through the anus. TYPES OF RECTAL PROLAPSE
RECTAL PROLPASE Rectal prolapse describes a condition where either the lining or entire wall of the rectum becomes loose and falls into, or even out of, the rectum through the anus. TYPES OF RECTAL PROLAPSE
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
What the radiologist needs to know!
 What the radiologist needs to know! Clare Molyneux Sam Treadway Sathi Sukumar Wal Baraza Abhiram Sharma Karen Telford University Hospital of South Manchester Manchester UK Introduction Indications Investigations
What the radiologist needs to know! Clare Molyneux Sam Treadway Sathi Sukumar Wal Baraza Abhiram Sharma Karen Telford University Hospital of South Manchester Manchester UK Introduction Indications Investigations
Anorectal Diagnostic Overview
 Anorectal Diagnostic Overview 11-25-09 3.11.2010 2009 2010 Anorectal Manometry Overview Measurement of pressures and the annotation of rectal sensation throughout the rectum and anal canal to determine:
Anorectal Diagnostic Overview 11-25-09 3.11.2010 2009 2010 Anorectal Manometry Overview Measurement of pressures and the annotation of rectal sensation throughout the rectum and anal canal to determine:
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
POSTERIOR LEVATOR REPAIR AND RECTAL SUSPENSION FOR RECURRENT RECTAL PROLAPSE: AUTHOR'S EXPERIENCE
 POSTERIOR LEVATOR REPAIR AND RECTAL SUSPENSION FOR RECURRENT RECTAL PROLAPSE: AUTHOR'S EXPERIENCE *Shyam B. Sharma 1&2 and Rahul Gupta 2 1 Department of Pediatric Surgery SMS Medical College 2 Pediatric
POSTERIOR LEVATOR REPAIR AND RECTAL SUSPENSION FOR RECURRENT RECTAL PROLAPSE: AUTHOR'S EXPERIENCE *Shyam B. Sharma 1&2 and Rahul Gupta 2 1 Department of Pediatric Surgery SMS Medical College 2 Pediatric
Single Stage Transanal Pull-Through for Hirschsprung s Disease in Neonates: Our Early Experience
 Journal of Neonatal Surgery 2013;2(4):39 ORIGINAL ARTICLE Single Stage Transanal Pull-Through for Hirschsprung s Disease in Neonates: Our Early Experience Pradeep Bhatia,* Rakesh S Joshi, Jaishri Ramji,
Journal of Neonatal Surgery 2013;2(4):39 ORIGINAL ARTICLE Single Stage Transanal Pull-Through for Hirschsprung s Disease in Neonates: Our Early Experience Pradeep Bhatia,* Rakesh S Joshi, Jaishri Ramji,
Surgical Management for Defecation Dysfunction
 Defecatory Dysfunction Surgical Management for Defecation Dysfunction JMAJ 46(9): 378 383, 2003 Tatsuo TERAMOTO Professor, 1st Department of Surgery, School of Medicine, Toho University Abstract: Typical
Defecatory Dysfunction Surgical Management for Defecation Dysfunction JMAJ 46(9): 378 383, 2003 Tatsuo TERAMOTO Professor, 1st Department of Surgery, School of Medicine, Toho University Abstract: Typical
Clinical Study Delorme s Procedure for Complete Rectal Prolapse: A Study of Recurrence Patterns in the Long Term
 Surgery Research and Practice Volume 215, Article ID 92154, 6 pages http://dx.doi.org/1.1155/215/92154 Clinical Study Delorme s Procedure for Complete Rectal Prolapse: A Study of Recurrence Patterns in
Surgery Research and Practice Volume 215, Article ID 92154, 6 pages http://dx.doi.org/1.1155/215/92154 Clinical Study Delorme s Procedure for Complete Rectal Prolapse: A Study of Recurrence Patterns in
CHAU KHAC TU M.D., Ph.D.
 CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
Delorme's operation plus sphincteroplasty for complete rectal prolapse associated with traumatic fecal incontinence
 Available online at www.jbr-pub.org Open Access at PubMed Central The Journal of Biomedical Research, 2015, 29(4):326-331 Original Article Delorme's operation plus sphincteroplasty for complete rectal
Available online at www.jbr-pub.org Open Access at PubMed Central The Journal of Biomedical Research, 2015, 29(4):326-331 Original Article Delorme's operation plus sphincteroplasty for complete rectal
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Laparoscopic Ventral. Mesh Rectopexy (LVMR)
") Laparoscopic Ventral Mesh Rectopexy (LVMR) Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard
Laparoscopic Ventral Mesh Rectopexy (LVMR) Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard
GI Physiology - Investigating and treating patients with pelvic floor dysfunction. Lynne Smith Department of GI Physiology NGH Sheffield
 GI Physiology - Investigating and treating patients with pelvic floor dysfunction Lynne Smith Department of GI Physiology NGH Sheffield Aims o o o To give an overview of lower GI investigations To demonstrate
GI Physiology - Investigating and treating patients with pelvic floor dysfunction Lynne Smith Department of GI Physiology NGH Sheffield Aims o o o To give an overview of lower GI investigations To demonstrate
Saint-Petersburg State Pediatric Medical University, Saint-Petersburg, Russia
 Saint-Petersburg State Pediatric Medical University, Saint-Petersburg, Russia Modern technologies in treatment of fecal incontinence in children Komissarov Igor Alexeevich- Ph.D, M.D, Prof. Kolesnikova
Saint-Petersburg State Pediatric Medical University, Saint-Petersburg, Russia Modern technologies in treatment of fecal incontinence in children Komissarov Igor Alexeevich- Ph.D, M.D, Prof. Kolesnikova
JNM Journal of Neurogastroenterology and Motility
 JNM Journal of Neurogastroenterology and Motility J Neurogastroenterol Motil, Vol. 19 No. 1 January, 2013 pissn: 2093-0879 eissn: 2093-0887 http://dx.doi.org/10.5056/jnm.2013.19.1.78 Original Article Successful
JNM Journal of Neurogastroenterology and Motility J Neurogastroenterol Motil, Vol. 19 No. 1 January, 2013 pissn: 2093-0879 eissn: 2093-0887 http://dx.doi.org/10.5056/jnm.2013.19.1.78 Original Article Successful
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 6, Issue 1 Article 3 Starr Surgery In ODS: A Case Series Of 500 ODS Patients Operated At India s Largest Proctology Clinic Ashwin Dhanarajji Porwal Paresh Manilal
World Journal of Colorectal Surgery Volume 6, Issue 1 Article 3 Starr Surgery In ODS: A Case Series Of 500 ODS Patients Operated At India s Largest Proctology Clinic Ashwin Dhanarajji Porwal Paresh Manilal
Stapled transanal rectal resection for obstructed defaecation syndrome
 Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Surgery for complete(full-thickness) rectal prolapse in adults(review)
 rectal prolapse in adults(review)") Cochrane Database of Systematic Reviews Surgery for complete(full-thickness) rectal prolapse in adults (Review) TouS,BrownSR,NelsonRL TouS,BrownSR,NelsonRL. Surgery for complete(full-thickness) rectal
Cochrane Database of Systematic Reviews Surgery for complete(full-thickness) rectal prolapse in adults (Review) TouS,BrownSR,NelsonRL TouS,BrownSR,NelsonRL. Surgery for complete(full-thickness) rectal
Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy
 Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy Marie Fidela R. Paraiso, M.D. Professor of Surgery Section Head, Urogynecology and Reconstructive Pelvic Surgery Cleveland, OH Disclosures
Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy Marie Fidela R. Paraiso, M.D. Professor of Surgery Section Head, Urogynecology and Reconstructive Pelvic Surgery Cleveland, OH Disclosures
Perineale Rektumprolapsoperation: Gute Resultate bei geringem Aufwand! F.H. Hetzer
 Perineale Rektumprolapsoperation: Gute Resultate bei geringem Aufwand! F.H. Hetzer STARR: Wunderwaffe beim Obstructed Defecation Syndrom (ODS) F.H. Hetzer Stapled TransAnal Rectal Resection STARR PPH 01
Perineale Rektumprolapsoperation: Gute Resultate bei geringem Aufwand! F.H. Hetzer STARR: Wunderwaffe beim Obstructed Defecation Syndrom (ODS) F.H. Hetzer Stapled TransAnal Rectal Resection STARR PPH 01
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
RECTAL INJURY IN UROLOGIC SURGERY. Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences.
 RECTAL INJURY IN 27 UROLOGIC SURGERY Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences. With good mechanical bowel preparation plus antibiotic
RECTAL INJURY IN 27 UROLOGIC SURGERY Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences. With good mechanical bowel preparation plus antibiotic
The Milestones provide a framework for the assessment
 The Colon and Rectal Surgery Milestone Project The Milestones provide a framework for the assessment of the development of the resident physician in key dimensions of the elements of physician competency
The Colon and Rectal Surgery Milestone Project The Milestones provide a framework for the assessment of the development of the resident physician in key dimensions of the elements of physician competency
ACG Clinical Guideline: Management of Benign Anorectal Disorders
 ACG Clinical Guideline: Management of Benign Anorectal Disorders Arnold Wald, MD, MACG 1, Adil E. Bharucha, MBBS, MD 2, Bard C. Cosman, MD, MPH, FASCRS 3 and William E. Whitehead, PhD, MACG 4 1 Division
ACG Clinical Guideline: Management of Benign Anorectal Disorders Arnold Wald, MD, MACG 1, Adil E. Bharucha, MBBS, MD 2, Bard C. Cosman, MD, MPH, FASCRS 3 and William E. Whitehead, PhD, MACG 4 1 Division
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
The American Society of Colon and Rectal Surgeons
 CLINICAL PRACTICE GUIDELINES Downloaded from https://journals.lww.com/dcrjournal by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3IJrtBKuSsQVRz8fA4yAY0a8W1YLRn6mHykFpaZ5LFvI= on 03/16/2018
CLINICAL PRACTICE GUIDELINES Downloaded from https://journals.lww.com/dcrjournal by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3IJrtBKuSsQVRz8fA4yAY0a8W1YLRn6mHykFpaZ5LFvI= on 03/16/2018
Constipation. (Medical Aspects)
") Constipation (Medical Aspects) By Dr. Ehab Abdel Khalik MD. Anatomy of the anorectum The rectum is 12-15 15 cm. long. It connects with the sigmoid colon by the rectosigmoid junction which is believed to
Constipation (Medical Aspects) By Dr. Ehab Abdel Khalik MD. Anatomy of the anorectum The rectum is 12-15 15 cm. long. It connects with the sigmoid colon by the rectosigmoid junction which is believed to
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 6, Issue 5 2016 Article 8 Sigmoidocele: A Rare Cause Of Constipation In Males Noor Shah MD Milind Kachare MD Craig Rezac MD Rutgers Robert Wood Johnson Medical
World Journal of Colorectal Surgery Volume 6, Issue 5 2016 Article 8 Sigmoidocele: A Rare Cause Of Constipation In Males Noor Shah MD Milind Kachare MD Craig Rezac MD Rutgers Robert Wood Johnson Medical
Abdominal Wall Modification for the Difficult Ostomy
 Abdominal Wall Modification for the Difficult Ostomy David E. Beck, M.D. 1 ABSTRACT A select group of patients with major stomal problems may benefit from operative modification of the abdominal wall.
Abdominal Wall Modification for the Difficult Ostomy David E. Beck, M.D. 1 ABSTRACT A select group of patients with major stomal problems may benefit from operative modification of the abdominal wall.
REVIEW ARTICLE. Surgical Management of Rectal Prolapse. the anus. 1 Complete or
 REVIEW ARTICLE Surgical Management of Rectal Prolapse Thandinkosi E. Madiba, MMed(Chir), FCS(SA); Mirza K. Baig, FRCS; Steven D. Wexner, MD, FACS, FRCS, FRCS(Edin) Background: The problem of complete rectal
REVIEW ARTICLE Surgical Management of Rectal Prolapse Thandinkosi E. Madiba, MMed(Chir), FCS(SA); Mirza K. Baig, FRCS; Steven D. Wexner, MD, FACS, FRCS, FRCS(Edin) Background: The problem of complete rectal
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
PAPER. Long-term Follow-up of the Modified Delorme Procedure for Rectal Prolapse
 PAPER Long-term Follow-up of the Modified Delorme Procedure for Rectal Prolapse Brian P. Watkins, MD, MS; Jeffrey Landercasper, MD; G. Eric Belzer, MD; Paula Rechner, MD; Rebecca Knudson, BA; Marilu Bintz,
PAPER Long-term Follow-up of the Modified Delorme Procedure for Rectal Prolapse Brian P. Watkins, MD, MS; Jeffrey Landercasper, MD; G. Eric Belzer, MD; Paula Rechner, MD; Rebecca Knudson, BA; Marilu Bintz,
By:Dr:ISHRAQ MOHAMMED
 By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
LONG TERM OUTCOME OF ELECTIVE SURGERY
 LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
Common Gastrointestinal Problems in the Elderly
 Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Index of subjects. bilesalt, malabsorption, incontinence in 147
 Index of subjects alcoholism, neuronal damage in 118 Alzheimer dementia, faecal incontinence in 113 anal fissure, manometry in 5 anal retractor, reduction of resting pressure 128 Angelchick prosthesis,
Index of subjects alcoholism, neuronal damage in 118 Alzheimer dementia, faecal incontinence in 113 anal fissure, manometry in 5 anal retractor, reduction of resting pressure 128 Angelchick prosthesis,
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Case Study Review #2!
 1 Case Study Review #2! Based on your feedback for more SCQR-specific education, we are offering this common case scenario with frequently asked SCQR questions and misinterpreted variables. The case study
1 Case Study Review #2! Based on your feedback for more SCQR-specific education, we are offering this common case scenario with frequently asked SCQR questions and misinterpreted variables. The case study
Our Experience in Management of Complete Rectal Prolapse in Children by Delorme Procedure
 Med. J. Cairo Univ., Vol. 84, No. 1, December: 1357-1362, 2016 www.medicaljournalofcairouniversity.net Our Experience in Management of Complete Rectal Prolapse in Children by Delorme Procedure MOHAMED
Med. J. Cairo Univ., Vol. 84, No. 1, December: 1357-1362, 2016 www.medicaljournalofcairouniversity.net Our Experience in Management of Complete Rectal Prolapse in Children by Delorme Procedure MOHAMED
MCOMPASS ANAL MANOMETRY AN OVERVIEW
 MCOMPASS ANAL MANOMETRY AN OVERVIEW ANAL MANOMETRY MEASURES PRESSURE ALLOWS INTERPRITATION SENSATION RAIR RECTAL COMPLIANCE MOTIVATION OF THE PATIENT FUNCTION OF THE PUDENDAL NERVE WHEN TO USE ANAL MANOMETRY
MCOMPASS ANAL MANOMETRY AN OVERVIEW ANAL MANOMETRY MEASURES PRESSURE ALLOWS INTERPRITATION SENSATION RAIR RECTAL COMPLIANCE MOTIVATION OF THE PATIENT FUNCTION OF THE PUDENDAL NERVE WHEN TO USE ANAL MANOMETRY
MCOMPASS ANAL MANOMETRY AN OVERVIEW
 MCOMPASS ANAL MANOMETRY AN OVERVIEW ANAL MANOMETRY MEASURES PRESSURE ALLOWS INTERPRITATION SENSATION RAIR RECTAL COMPLIANCE MOTIVATION OF THE PATIENT FUNCTION OF THE PUDENDAL NERVE WHEN TO USE ANAL MANOMETRY
MCOMPASS ANAL MANOMETRY AN OVERVIEW ANAL MANOMETRY MEASURES PRESSURE ALLOWS INTERPRITATION SENSATION RAIR RECTAL COMPLIANCE MOTIVATION OF THE PATIENT FUNCTION OF THE PUDENDAL NERVE WHEN TO USE ANAL MANOMETRY
3D Dynamic Ultrasound In Obstructed Defecation
 3D Dynamic Ultrasound In Obstructed Defecation By Ramy Salahudin Abdelkader Assist. Lecturer of General Surgery Cairo University Introduction Pelvic floor is complex system, with passive and active components
3D Dynamic Ultrasound In Obstructed Defecation By Ramy Salahudin Abdelkader Assist. Lecturer of General Surgery Cairo University Introduction Pelvic floor is complex system, with passive and active components
Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee
 Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee MD, MMed (S'pore), FRCS (Edin) Associate Consultant Department of Surgery 9 January 2016 Incidence
Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee MD, MMed (S'pore), FRCS (Edin) Associate Consultant Department of Surgery 9 January 2016 Incidence
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015
 Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder).
.") An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder). Mederi Therapeutics has developed this kit to help you raise awareness of
An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder). Mederi Therapeutics has developed this kit to help you raise awareness of
Surgical repair of vaginal wall prolapse using mesh
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland
 Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland 16:30-17:25 WS #168: Modern Treatment of Haemorrhoids 17:35-18:30 WS #180: Modern Treatment of Haemorrhoids (Repeated) BOTTOMS Science and
Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland 16:30-17:25 WS #168: Modern Treatment of Haemorrhoids 17:35-18:30 WS #180: Modern Treatment of Haemorrhoids (Repeated) BOTTOMS Science and
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
The use of conventional defecography in clinical practice
 The use of conventional defecography in clinical practice Poster No.: C-1564 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Šmite, R. Laguns ; Lielvarde/LV, Riga/LV Keywords: Pelvic floor dysfunction,
The use of conventional defecography in clinical practice Poster No.: C-1564 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Šmite, R. Laguns ; Lielvarde/LV, Riga/LV Keywords: Pelvic floor dysfunction,
The use of conventional defecography in clinical practice
 The use of conventional defecography in clinical practice Poster No.: C-1564 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Šmite, R. Laguns ; Lielvarde/LV, Riga/LV Keywords: Pelvic floor dysfunction,
The use of conventional defecography in clinical practice Poster No.: C-1564 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Šmite, R. Laguns ; Lielvarde/LV, Riga/LV Keywords: Pelvic floor dysfunction,
Billing Guideline. Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16
 Effective Date: 1/1/14 Last revision effective 4/16") Billing Guideline Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16 Florida Hospital Care Advantage plans include full coverage of in-network
Billing Guideline Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16 Florida Hospital Care Advantage plans include full coverage of in-network
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Constipation. H. David Vargas, MD. Overview
 Constipation H. David Vargas, MD Overview Constipation is a very common complaint affecting upwards of 15% of all Americans. Fortunately, constipation usually is simple to avoid and easy to treat when
Constipation H. David Vargas, MD Overview Constipation is a very common complaint affecting upwards of 15% of all Americans. Fortunately, constipation usually is simple to avoid and easy to treat when
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Anorectal malformations include a wide spectrum of
 JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUES Volume 20, Number 1, 2010 ª Mary Ann Liebert, Inc. DOI: 10.1089=lap.2008.0343 Laparoscopic-Assisted Pull-Through for Congenital Rectal Stenosis
JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUES Volume 20, Number 1, 2010 ª Mary Ann Liebert, Inc. DOI: 10.1089=lap.2008.0343 Laparoscopic-Assisted Pull-Through for Congenital Rectal Stenosis
Accidental Bowel Leakage (Fecal Incontinence)
") Accidental Bowel Leakage (Fecal Incontinence) What is Accidental Bowel Leakage (ABL)? Accidental bowel leakage is the inability to control solid or liquid stool. This is the inability to control gas and
Accidental Bowel Leakage (Fecal Incontinence) What is Accidental Bowel Leakage (ABL)? Accidental bowel leakage is the inability to control solid or liquid stool. This is the inability to control gas and
DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis.
 DISCHARGE SUMMARY DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis. OPERATIONS/PROCEDURES: Living related renal transplantation. HISTORY: For full details
DISCHARGE SUMMARY DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis. OPERATIONS/PROCEDURES: Living related renal transplantation. HISTORY: For full details
Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives
 Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives 1 Aims of this self assessment competency To equip Midwives with the knowledge and skills to teach pelvic floor
Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives 1 Aims of this self assessment competency To equip Midwives with the knowledge and skills to teach pelvic floor
High-field (3T) magnetic resonance defecography with functional assessment of the evacuation phase: A pictorial essay
 magnetic resonance defecography with functional assessment of the evacuation phase: A pictorial essay") High-field (3T) magnetic resonance defecography with functional assessment of the evacuation phase: A pictorial essay Poster No.: C-430 Congress: ECR 2009 Type: Educational Exhibit Topic: Abdominal and
High-field (3T) magnetic resonance defecography with functional assessment of the evacuation phase: A pictorial essay Poster No.: C-430 Congress: ECR 2009 Type: Educational Exhibit Topic: Abdominal and
Duhamel operation for Hirschsprung s disease; laparoscopic modified Duhamel procedure with Z-shaped anastomosis
 Review Article Page 1 of 5 Duhamel operation for Hirschsprung s disease; laparoscopic modified Duhamel procedure with Z-shaped anastomosis Go Miyano, Yuta Yazaki, Takanori Ochi, Soichi Shibuya, Yuichiro
Review Article Page 1 of 5 Duhamel operation for Hirschsprung s disease; laparoscopic modified Duhamel procedure with Z-shaped anastomosis Go Miyano, Yuta Yazaki, Takanori Ochi, Soichi Shibuya, Yuichiro
Operative Technique: Karen Horvath, MD, FACS. SCOAP Retreat June 17, 2011
 Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
REPAIR OF LARGE CYSTOCELE
 REPAIR OF LARGE CYSTOCELE WITH RAZ SUSPENSION 17 VAGINAL INCISION AND DISSECTION Premarin cream application to the anterior vagina daily for 1 month before cystocele repair enriches the vasculature and
REPAIR OF LARGE CYSTOCELE WITH RAZ SUSPENSION 17 VAGINAL INCISION AND DISSECTION Premarin cream application to the anterior vagina daily for 1 month before cystocele repair enriches the vasculature and
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
Instructions for Use
 CONTINENCE RESTORATION SYSTEM Instructions for Use Humanitarian Device Authorized by Federal (USA) Law for use in the treatment of fecal incontinence in patients who are not candidates for or have previously
CONTINENCE RESTORATION SYSTEM Instructions for Use Humanitarian Device Authorized by Federal (USA) Law for use in the treatment of fecal incontinence in patients who are not candidates for or have previously
Inflammatory Bowel Disease: Updates and Controversies CASE #1 CASE #1 8/6/2015. What is the most likely diagnosis?
 Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
JNM Journal of Neurogastroenterology and Motility
 ㅋ JNM Journal of Neurogastroenterology and Motility J Neurogastroenterol Motil, Vol. 17 No. 4 October, 2011 pissn: 2093-0879 eissn: 2093-0887 http://dx.doi.org/10.5056/jnm.2011.17.4.416 How to Interpret
ㅋ JNM Journal of Neurogastroenterology and Motility J Neurogastroenterol Motil, Vol. 17 No. 4 October, 2011 pissn: 2093-0879 eissn: 2093-0887 http://dx.doi.org/10.5056/jnm.2011.17.4.416 How to Interpret
Long-Term Bowel Symptoms Following Corrective Surgery
 HIRSCHSPRUNG'S DISEASE Samuel Nurko MD MPH Center for Motility and Functional Gastrointestinal Disorders Children s Hospital Medical Center, Boston Ma Long-Term Bowel Symptoms Following Corrective Surgery
HIRSCHSPRUNG'S DISEASE Samuel Nurko MD MPH Center for Motility and Functional Gastrointestinal Disorders Children s Hospital Medical Center, Boston Ma Long-Term Bowel Symptoms Following Corrective Surgery
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Local Excision of Rectal Cancer Techniques and Outcomes
 Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Novel Options for the Management of Fecal Incontinence
 Novel Options for the Management of Fecal Incontinence Arnold Wald, MD, MACG University of Wisconsin School of Medicine and Public Health, Madison WI ANORECTAL CONTINENCE MECHANISMS Reservoir Elements
Novel Options for the Management of Fecal Incontinence Arnold Wald, MD, MACG University of Wisconsin School of Medicine and Public Health, Madison WI ANORECTAL CONTINENCE MECHANISMS Reservoir Elements
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF)
") Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF) Blair B. Washington MD, MHA Urogynecology & Reconstructive Pelvic Surgery Virginia Mason Medical Center Disclosures
Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF) Blair B. Washington MD, MHA Urogynecology & Reconstructive Pelvic Surgery Virginia Mason Medical Center Disclosures
PREPARING FOR ANORECTOAL MANOMETRY. ManoScan Anorectal Manometry System
 PREPARING FOR ANORECTOAL MANOMETRY ManoScan Anorectal Manometry System WHAT IS ANORECTAL MANOMETRY? Anorectal manometry is a test used to evaluate the function and coordination of the sphincter and pelvic
PREPARING FOR ANORECTOAL MANOMETRY ManoScan Anorectal Manometry System WHAT IS ANORECTAL MANOMETRY? Anorectal manometry is a test used to evaluate the function and coordination of the sphincter and pelvic
A Case of Fecal Incontinence: Medical and Interventional Treatment Options
 A Case of Fecal Incontinence: Medical and Interventional Treatment Options HPI JP is a 69 year-old F with a 12-month history of FI. Her symptoms began after a colonoscopy She has been experiencing passive
A Case of Fecal Incontinence: Medical and Interventional Treatment Options HPI JP is a 69 year-old F with a 12-month history of FI. Her symptoms began after a colonoscopy She has been experiencing passive
Management of Neurogenic Bowel Dysfunction. Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders
 Management of Neurogenic Bowel Dysfunction Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders DEFECATION Delivery of colon contents to the rectum Rectal compliance
Management of Neurogenic Bowel Dysfunction Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders DEFECATION Delivery of colon contents to the rectum Rectal compliance
Incidence of Colorectal Cancers- Australia. Anterior Resection 5/23/2018. What spurs us to investigate?
 Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
Rectal Prolapse: Review According to the Personal Experience
 Review Journal of the Korean Society of DOI: 10.3393/jksc.2011.27.3.107 pissn 2093-7822 eissn 2093-7830 Rectal Prolapse: Review According to the Personal Experience Department of Surgery, Seoul Song Do
Review Journal of the Korean Society of DOI: 10.3393/jksc.2011.27.3.107 pissn 2093-7822 eissn 2093-7830 Rectal Prolapse: Review According to the Personal Experience Department of Surgery, Seoul Song Do
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Fig. 1. Clinical condition. before operation.
 PLATE IX. Fig. 1. Clinical condition before operation. A CASE OF RECTAL PROLAPSE. BY D. Robertson, M.B., Ch.B. (Edin.), AND D. G. C. Tasker, M.S. (Lond.), F.R.C.S. (Eng.). On many occasions in the practice
PLATE IX. Fig. 1. Clinical condition before operation. A CASE OF RECTAL PROLAPSE. BY D. Robertson, M.B., Ch.B. (Edin.), AND D. G. C. Tasker, M.S. (Lond.), F.R.C.S. (Eng.). On many occasions in the practice