IV drug preparation guidelines. Prepared by pharmacist Eman Elayeh
|
|
|
- Julie Gilmore
- 5 years ago
- Views:
Transcription
1 IV drug preparation guidelines Prepared by pharmacist Eman Elayeh

2 Injectable drugs guide The monographs in this book detail appropriate methods of administration for medicines that can be given via the parenteral route 2
3 Introduction Errors during pharmacy preparation of parenteral products and admixtures have frequently been reported to the ISMP National Medication Error Reporting Program (ISMP-MERP) and have also been a topic of discussion in the ISMP Medication Safety Alert! In addition, a five-hospital observational study on the accuracy of preparing small- and large-volume injectables, chemotherapy solutions, and parenteral nutrition showed a mean error rate of 9%, meaning almost 1 in 10 products was prepared incorrectly prior to dispensing 3
4 The use of parenteral therapy is part of daily practice in hospitals and increasingly so in primary care. Using the parenteral route to administer medicines requires all practitioners to work in partnership to ensure the safe, effective and economic use of parenteral therapy. 4
5 The most important issues when preparing IV medications include 1) Sodium content 2) ph 3) Compatibility (diluents and y- site) 4) Light sensitivity 5) Displacement value 6) Storage 7) Stability after preparation 8) Preparation and administration 5
6 Sodium content The sodium content of each medicine is included in this guide. Some medicines, e.g. many antibiotics, are formulated with a considerable sodium content; for example, metronidazole contains 13.15mmol/500-mg bag. This may be clinically significant and may need to be taken into account when therapeutic choices are made. In the monographs the sodium content is listed if a dose contains >=1mmol sodium 6
7 To convert mg of sodium to mg of salt, multiply the mg of sodium by 2.5. To convert mmol of sodium to mg of sodium, multiply mmol of sodium by 23. To convert mmol of sodium to mg of sodium chloride, multiply mmol of sodium by
8 Sodium content Patients with certain conditions that retain salt E.g. Congestive Heart Failure, Ascites, Renal failure.high sodium containing regimens may worsen underlying condition and result in deterioration of condition Low sodium diets while giving high sodium antibiotics is counterproductive 8

9 9 Sodium content of selected IV antibiotics

10 Sodium content of selected IV antibiotics 10
11 Sodium content Patients with history of Congestive heart Failure Avoid (Unless no treatment alternative) Piperacillin tazobactam Ampicillin sulbactam Nafcillin/oxacillin Preferred Cefepime (for GNR infections) Cefazolin (for MSSA) 11
12 Sodium content Patients with ascites/liver failure with SBP: Preferred Cefotetan or Cefepime Avoid Piperacillin tazobactam Renal failure (Not HD) Patients with CrCl < 30,not HD MSSA -Cefozolin where possible GNR -Cefepime 12
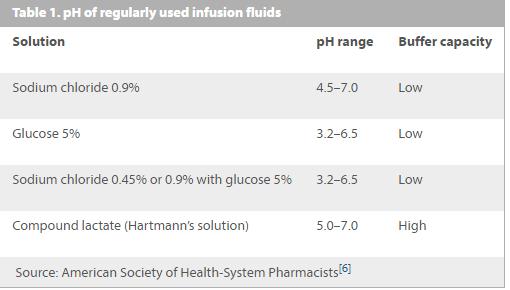
13 ph An indication of the acidity or alkalinity of injection solutions has been included in the monographs (as measured by their ph) to help practitioners predict possible Y-site incompatibilities of medicines when no compatibility information exists Injections with greatly differing ph values should not be administered concurrently down the same line as this may result in either precipitation or inactivation of the medicines for example, the ph of phenytoin injection is 12 and the ph of haloperidol injection is 3, making them incompatible; if mixed they would combine chemically to form a precipitate 13
14 14 Y site IV
15 ph The ph can also give the practitioner an indication of the irritancy of the drug. Medicines that are either highly acidic or alkaline may be harmful if extravasation into the surrounding tissue occurs, causing tissue damage. Injections in oily or other unusual vehicles do not have a ph value. This is because ph is a measure of the acidity or alkalinity of an aqueous solution and by its very nature an oily injection is not an aqueous solution. 15
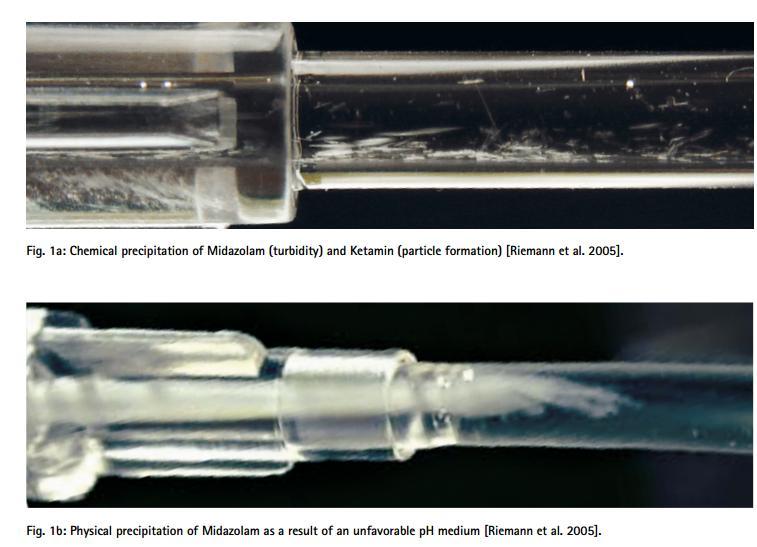
16 Incompatibility In contrast to the interaction, an incompatibility reaction occurs inside a fluid container or infusion line and is usually visible. 16
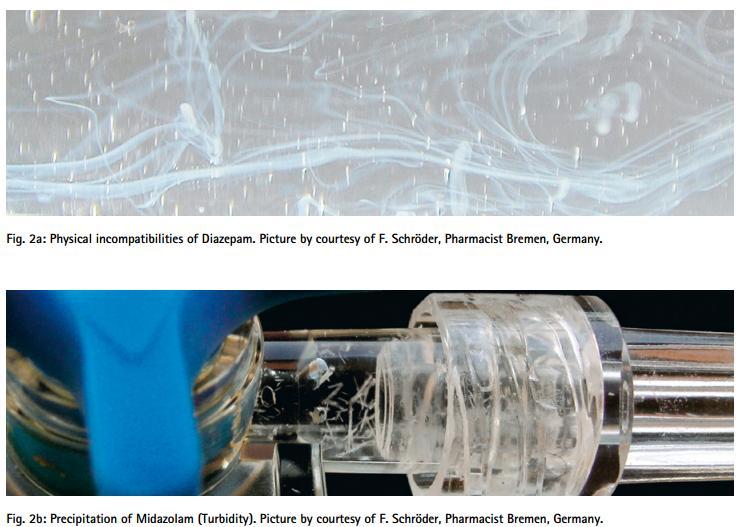
17 Types of incompatibilities Physical reactions of drugs usually refer to either phase separation or precipitation (e.g. after the dilution of alcoholic solutions) due to a change of the relation between ionization and non-ionization and solubility The ph-value and the buffer capacity (pka value) of the IV solutions and the drugs used are major factors responsible for physical interactions 17
18 18
19 19
20 20

21 21

22 22
23 23
24 Physicochemical incompatibilities ph changes A common example of ph affecting stability is with morphine sulphate. This is a weak base, but is formulated at an acidic ph of It is highly sensitive to changes in ph, and likely to precipitate out of solution in an alkaline environment. Phenytoin is a weak acid and is formulated for use in intravenous preparations as a phenytoin sodium salt, with the solution adjusted to a highly basic ph of 12. Phenytoin can precipitate if mixed with a solution that lowers its ph; for example, when mixed with glucose 5% (ph range ), phenytoin precipitates almost immediately. According to its manufacturer, phenytoin sodium can be added to sodium chloride for infusion, but administration should start immediately after preparation and must be completed within one hour. The infusion solution should be constantly monitored for haziness and precipitate. An in-line filter should also be used to prevent any precipitate entering a patient s blood. 24
25 Physicochemical incompatibilities Changes in concentration can affect the compatibility of some drug combinations (i.e. drugs that are compatible at lower concentrations can become incompatible at higher concentrations) This can be a result of an increased rate of reaction between two compounds forming an insoluble compound or if the solute concentration becomes too high. For example, when calcium and phosphate additives are added to a TPN bag there is a potential for an insoluble calcium phosphate salt to be formed above too high a concentration for either or both additives. Different amino acids in the TPN solution can also affect the concentration at which calcium phosphate is formed. Concentration is particularly important when multiple drugs are being infused subcutaneously via a syringe driver, in which minimal volumes are required. 25
26 Physicochemical incompatibilities Alcohol or lipid solvents are water-miscible organic solvents used to improve the solubility of poorly water soluble drugs. These are required not only to achieve high solubility but also to prevent drug precipitation upon dilution in an aqueous solution. Commonly used solvents include polyethylene glycol, propylene glycol, ethanol and glycerine When the formulated product is diluted in an aqueous solution, the drug may precipitate out until enough solution is added to enable dissolution without the need for a solvent. Therefore, it is often impracticable to mix drugs that are poorly water soluble with drugs that are highly water soluble. The solubility of the drug and use of an alcohol or lipid solvent can also determine how, and in what vehicle, the drug should be administered. 26
27 Physicochemical incompatibilities For example, digoxin is formulated with propylene glycol 40% and ethanol 10%. It needs to be administered diluted at least fourfold to prevent precipitation. Diazepam is insoluble in aqueous solutions and is formulated as an emulsion (e.g. Diazemuls) or in a high alcohol-containing solvent. Diazemuls can be mixed in all proportions with Intralipid 10% or 20% (a lipid emulsion, particularly useful in providing a vehicle for drugs such as diazepam to be administered), but not with saline solutions. According to the manufacturers, the alcohol-containing formulation should be diluted to a concentration of at least 10mg in 200ml. There is some evidence that higher concentrations may be stable, but these are not recommended 27
28 Physicochemical incompatibilities The creation of gas is a normal part of the reconstitution of some drugs, particularly those made with sodium carbonate as an excipient (upon reconstitution, these formulations can generate carbon dioxide). However, the creation of extensive amounts of gas can be hazardous. Metoclopramide formulated as its hydrochloride salt is incompatible with sodium bicarbonate for this reason 28
29 Physicochemical incompatibilities Fat emulsions, such as Intralipid, TPN and some drug formulations (e.g. Diazemuls), can easily be destabilised, cracked or separated when they are mixed with solutions containing highly positively charged ions. For this reason, electrolytes should only ever be added to TPN in a specialist pharmacy aseptic unit where the stability of the final product can be checked before use. Propofol is formulated as a lipid. When it is mixed with too much lidocaine, the fat droplet size increases considerably and layering occurs (fat and aqueous components of an emulsion separate over time into two distinct layers). This is caused by lidocaine disrupting the surfactant properties of the propofol vehicle 29
30 Physicochemical incompatibilities Adsorption when a drug in solution binds to the surface of its container, giving set or in-line filter reduces the amount of drug available to be administered to the patient. Large polymeric drugs (e.g. paclitaxel), proteins (e.g. insulin) and highly lipid-soluble drugs, the flow rate, concentration of drug and ph can all affect the extent to which adsorption occurs. In-line filters are required for certain medicines (e.g. phenytoin, TPN and monoclonal antibodies); this may preclude the mixing of other drugs in the same infusion. If an in-line filter becomes blocked and the fluid is prevented from running, a new infusion should be prepared as there could still be precipitate or particles in the infusion bag. Adsorption is also more likely to occur when polyvinyl chloride (PVC)-containing equipment is used. Syringes are generally PVC-free and are more suitable for use with drugs that are susceptible to adsorption. PVC-free giving sets should be obtained where possible 30
31 Chemical instability Oxidation, reduction and hydrolysis can cause the chemical degradation of a drug, resulting in a loss of potency or the formation of toxic by-products. These processes can be accelerated by: the addition of an aqueous solution when reconstituting dry powders; ultraviolet light; exposure to oxygen; and changes in temperature or ph. When erythromycin is reconstituted, it is degraded by hydrolysis and will lose potency after eight hours. This reaction is accelerated by a change in ph and therefore erythromycin should not be diluted with glucose or combined with acidic drugs, such as linezolid 31
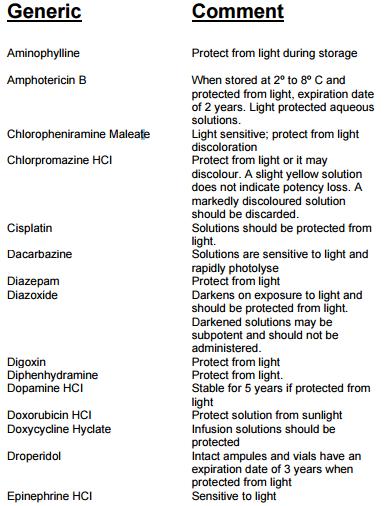
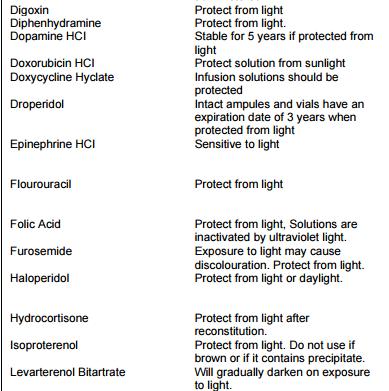
32 Light-sensitive infusions Some drugs undergo photolysis and photodegradation if exposed to natural daylight (ultraviolet radiation) and fluorescent light during administration. This can result in loss of therapeutic effect and the production of toxic products. To reduce these reactions, the products must be protected from light not only during storage but also once diluted and ready for use. The infusion bag, the syringe and sometimes the giving set need to be protected from light by covering with an opaque material or aluminium foil. Periodic visual inspection of the diluted solution for the occurrence of discoloration and/or precipitation is recommended during its infusion. Drugs that must be protected from light have this detailed in their individual monograph 32



33 w IV set for light sensitive drugs 33
34 34
35 Displacement value Injection products formulated as dry powders or lyophilised cakes must be reconstituted with a suitable diluent before administration. Sometimes the final volume of the injection is greater than the volume of liquid added to the powder. This volume difference is called the displacement value; for example: * The displacement value of amoxicillin injection 250mg is 0.2 ml. * If 4.8mL of diluent is added to a 250-mg vial, the resulting volume is 5mL, i.e. 250mg in 5 ml. * If 5mL of diluent is added, the resulting volume is 5.2 ml, i.e. 250mg in 5.2mLor mg in 5mL. Drugs that have a significant displacement have this detailed in their individual monograph and this must be taken into account when reconstituting the drug if only part of the vial is to be used. If the total content of a vial is to be given, the displacement value need not be taken into account when reconstituting the drug because the entire contents of the vial are withdrawn for administration. 35
36 Displacement value Example You are asked to calculate the volume of diluent needed to be added to 80mg of Drug X to produce a required concentration of 4mg in 1mL. The displacement volume of Drug X is 0.5mL/40mg. Step 1 Find the Final Volume If the required concentration is 4mg in 1mL, then 20mL is needed for 80mg of Drug X. Step 2 Determine the Displacement Volume If 40mg displaces 0.5mL of solution, it means that 80mg would displace 1mL. Step 3 Subtract the Displacement Volume from the Final Volume 20mL 1mL = 19mL of diluent required. 36
37 Displacement value 68mL of water is required to produce 100mL of a mixture containing 250mg of Drug X in each 5mL dose. Bearing this in mind, calculate the displacement volume for a quantity of powder equivalent to the 250mg dose of Drug X. If there is 250mg in each 5mL dose, then 100mL would have 20x this i.e. 5,000mg. If 68mL is required, it must mean 5,000mg displaces the remaining 32mL of water. Thus, 5,000mg displaces 32mL in 100mL; therefore, 250mg displaces 1.6mL in a 5mL dose. 1.6mL is displaced in a reconstituted 250mg/5mL dose. 37
38 Flushing intravenous lines and cannulas Flushing between the administration of different medicines must always be carried out to avoid any problems with incompatibilities. Flushing also ensures the total drug dose is presented for systemic effect and prolongs the viability of the cannula or line. If two drugs being administered one after the other are known to be compatible, then flushing the line or cannula need only be done before and after administration of the medicines. Commonly 5--10mL of NaCl 0.9% is used to flush the dead space of a cannula, whereas 20mL is usually needed for an administration set. The practitioner must check each monograph before deciding which flush to use, to ensure that both drugs are compatible with the chosen flush 38
39 Flushing intravenous lines and cannulas Frequent flushing of unused lines is also necessary in order to maintain patency of the line or cannula. The National Patient Safety Agency has recently recommended the exclusive use of NaCl 0.9% injection as a flush for maintaining peripheral intravenous cannulas. Occasionally NaCl with heparin is required to ensure that certain lines are kept patent (usually central lines when they are used infrequently), but such use should be kept to a minimum. If the use of a heparin flush is appropriate then it must be administered against a valid prescription. Practitioners should check their individual organization's policies in order to determine when the use of a heparin flush is appropriate. 39
40 Central versus peripheral access Before a medicine can be administered intravenously, a suitable intravenous catheter must be inserted into the patient. These can either be central intravenous catheters, peripheral intravenous catheters or peripherally inserted central intravenous catheters (PICC lines). Choice of line is often dictated by the clinical condition of the patient; for example, a critically ill patient is more likely to require central access than a patient who only requires a few days intravenous therapy. Unlike peripheral catheters, central lines are generally thought to last longer, are more consistently accessible regardless of the patient s condition and can accept more irritant solutions, e.g.hyperosmolar or vasoconstricting drugs. Central catheters also carry the advantage of allowing a rapid rate of infusion of a drug and can be used to monitor central venous pressures as well as aid the passing of pulmonary artery catheters. However, insertion of central intravenous catheters requires greater skill and the risks associated with them are greater 40
41 Intermittent intravenous infusions This is the technique used to administer an injectable drug in an intravenous infusion over a period of time ranging from 20 minutes to several hours. Repeated doses (e.g. benzylpenicillin) or single doses (e.g. furosemide) are given in this way. The infusion may be connected to the primary intravenous giving set or to a secondary administration set via a Y- connector. Administration can also be via an in-line burette, which would normally constitute a section of the primary giving set. The volume of intravenous fluid used to dilute the drug ranges from 50mL (the smallest intravenous fluid bag) up to 500 ml. In clinical practice most drugs are given in 100mL and are set to infuse over minutes. 41



42 42 In-line burette
43 Intermittent intravenous infusions The drug to be given may be compatible with one or both of these, although solubility and stability times may differ. Mixing drugs in infusion bags is not advised without compatibility data, which can be found in reference sources such as the latest edition of Trissel s Handbook on Injectable Drugs1 or via a website such as MedicinesComplete ( 43
44 Direct intravenous injections Some drug products may be administered directly into the venous circulation in a relatively small volume of fluid over less than 5 minutes. This technique is sometimes referred to as an IV push or IV bolus. Unless specifically directed otherwise by the manufacturer, a direct intravenous injection is given over 2--3 minutes, observing the patient and the injection site for signs of adverse reaction. The volume of injection is usually 5mL or less, although larger volumes may be necessary if the drug has low solubility, is likely to be an irritant to the vein or requires relatively slow administration. Bolus injections into indwelling cannulas should always be preceded and followed by at least 2--5mL of a flushing solution. 44
45 Extravasation Extravasation is a complication of intravenous injection therapy. It manifests as tissue damage or irritation caused by inadvertent placement or leakage of a drug into the area around the injected vein. Although most awareness of this problem relates to cytotoxic agents, it is important to note that it is a possibility for all drugs that can be given intravenously, e.g. antibiotics, drugs that are highly alkaline or acidic and glucose infusions 45
46 Extravasation Drugs can be classified as vesicant (literally meaning to cause blisters or blistering ) which cause direct damage to the vasculature, or as non-vesicant, which are further classified as irritant or nonirritant. Vesicants can cause extensive necrosis. Irritants can cause pain at the injection site and along the vein, with or without inflammation 46
47 Extravasation The following general rules can help to minimize the risk of extravasation: * Administration should be restricted to individuals familiar with the drugs and techniques used. * The drug should be reconstituted appropriately to avoid administration of damaging concentrations. * The drug should be given by via the injection port of free-flowing drip. * The site of administration should be selected to take into account visibility, vessel size, amount of movement and potential damage if extravasation occurs. The optimum location is usually the forearm, which has superficial veins with sufficient soft tissue to protect tendons and nerves. * The limb should be elevated with maintenance of gentle pressure after the needle is withdrawn 47

48 Extravasation Suggested administration procedure 1. Insert a 23-gauge butterfly needle into the vein; a Teflon catheter may be preferred for longer duration infusions. 2. Lightly tape the tubing in place; do not obscure the injection site by taping. 3. Connect a NaCl 0.9% infusion to the butterfly needle. Allow about 5mL of the solution to run through, then withdraw a small amount of blood to test the vein integrity and flow. Observe for extravasation and if this is obvious select another site. Avoid a distal point on the same vein. 4. Repeatedly ask the patient if he/she feels any pain or burning, and visually check the site. For an infusion, check every 2--3 minutes that it is still running. 5. Following the drug injection, reconnect the NaCl 0.9% infusion and run through at least 5mL of the solution to flush the drug from the entire tubing and needle 48
49 Extravasation If more than one drug is prescribed, inject the vesicant agent first; if all drugs are vesicant, inject the one with the smallest volume first. Separate each drug administration by a 3--5mL NaCl 0.9% flush. The rationale behind the administration of the vesicant first is that the integrity of venous access decreases with time and therefore if vesicants are administered first, all agents can be administered. 49
50 Extravasation Extravasation treatment If extravasation occurs, treatment is critical and specific antidotes may be required for some drugs. The general recommendations in the management of extravasation are: 1. Stop the infusion/injection immediately. 2. Remove the infusion bag/syringe. Do not flush. Do not remove the needle. Mark the area with an indelible pen. 3. Attempt to aspirate as much of the drug as possible with a clean syringe. 4. Apply a cool compress, which should be maintained for 1 hour. 5. Check for specific antidotes if applicable. 6. Apply hydrocortisone 1% (cream is easier to apply than ointment) topically to the affected area. 50
51 Homework Find out :preparation and administration, compatibility, ph, Na content, storage, displacement value, stability after preparation. 51

52 Important calculations Refer to this book for infusion rate calculations Print from page
53 Important videps IV Medication Administration: Reconstituting an IV Medication IV Medication Administration in a burette (microdropper) 53
54 Drip rate calculations To set up a manually controlled infusion accurately, you need to be able to count the number of drops per minute. To do this, you have to calculate the volume to be infused in terms of drops. This in turn depends upon the giving or administration set being used. Giving sets There are two giving sets: The standard giving set (SGS) has a drip rate of 20 drops per ml for clear fluids (i.e. sodium chloride, glucose) and 15 drops per ml for blood. The micro-drop giving set or burette has a drip rate of 60 drops per ml. The drip rate of the giving set is always written on the wrapper if you are not sure.
55 Drip rate calculations In all drip rate calculations, you have to remember that you are simply converting a volume to drops (or vice versa) and hours to minutes. Example??? 1 litre of sodium chloride 0.9% ( normal saline ) is to be given over 8 hours: what drip rate is required using a standard giving set (SGS), 20 drops/ml?
56 Drip rate calculations PROBLEMS Work out the drip rates for the following infusions: Question 1) 500mL of sodium chloride 0.9% over 6 hours Question 2) 1 litre of glucose 4% and sodium chloride 0.18% over 12 hours Question 3) 1 unit of blood (500 ml) over 6 hours
57 CONVERSION OF DOSAGES TO ml/hour You have an infusion of dopamine 800mg in 500 ml. The dose required is 2 mcg/kg/min for a patient weighing 68 kg. What is the rate in ml/hour? what is the rate in drops/hr?
58 CONVERSION OF DOSAGES TO ml/hour Question 4) You have a 500 ml infusion containing 50 mg nitroglycerin. A dose of 10 mcg/min is required. What is the rate in ml/hour? Question 5) You are asked to give 500 ml of lidocaine (lignocaine) 0.2% in glucose at a rate of 2 mg/min. What is the rate in ml/hour? Question 6) You have an infusion of dopamine 800mg in 500 ml. The dose required is 3 mcg/kg/min for a patient weighing 80 kg. What is the rate in ml/hour?
59 CONVERSION OF DOSAGES TO ml/hour Question 7) A patient with chronic obstructive pulmonary disease (COPD) is to have a continuous infusion of aminophylline. The patient weighs 63 kg and the dose to be given is 0.5 mg/kg/hour over 12 hours. Aminophylline injection comes as 250mg in 10mL ampoules and should be given in a 500mL infusion bag. (i) What dose and volume of aminophylline are required? (ii) What is the rate in ml/hour? What is the Rate in drops/min
60 CONVERSION OF DOSAGES TO ml/hour Question 8) You need to give aciclovir (acyclovir) as an infusion at a dose of 5 mg/kg every 8 hours. The patient weighs 86 kg and aciclovir (acyclovir) is available as 500 mg vials. Each vial needs to be reconstituted with 20mL Water for Injection and diluted further to 100 ml. The infusion should be given over 60 minutes. What dose and volume of aciclovir (acyclovir) are required for one dose? What is the rate in ml/hour for each dose?
61 CONVERSION OF DOSAGES TO ml/hour Question 9) Glyceryl trinitrate is to be given at a rate of 150 mcg/min. You have an infusion of 50mg in 50mL glucose 5%. What is the rate in ml/hour? Drops/min? Question 10 ) You have an infusion of dobutamine 250mg in 50 ml. The dose required is 6 mcg/kg/min and the patient weighs 75 kg. What is the rate in ml/hour? In drops/min?
62 CONVERSION OF DOSAGES TO ml/hour Question 11) A patient with MRSA is prescribed IV vancomycin 1 g every 24 hours. After reconstitution a 500 mg vial of vancomycin should be diluted with infusion fluid to 5 mg/ml. (i) What is the minimum volume (ml) of infusion fluid that 1 g vancomycin can be administered in? (Round this to the nearest commercially available bag size, i.e. 50 ml, 100 ml, 250 ml, 500mL or 1,000 ml.) (ii) The rate of administration not exceed 10 mg/min. Over how many minutes should the infusion be given? (iii) What is the rate in ml/hour?
63 CONVERSION OF DOSAGES TO ml/hour Question 12) You are asked to give an infusion of dobutamine to a patient weighing 73kg at a dose of 5mcg/kg/min. You have an infusion of 500mL sodium chloride 0.9% containing 250mg of dobutamine. (i) What is the dose required (mcg/min)? (ii) What is the concentration (mcg/ml) of dobutamine? (iii) What is the rate in ml/hour?
64 CONVERSION OF DOSAGES TO ml/hour Question 13) You are asked to give an infusion of isosorbide dinitrate 50mg in 500mL of glucose 5% at a rate of 2 mg/hour. (i) What is the rate in ml/hour? The rate is then changed to 5 mg/hour. (ii) What is the new rate in ml/hour?
65 CONVERSION OF ml/hour BACK TO A DOSE An infusion pump containing 250 mg dobutamine in 50 ml is running at a rate of 3.5 ml/hour. Convert this to mcg/kg/min to check that the pump is set correctly. (Patient s weight = 73 kg)
66 CONVERSION OF ml/hour BACK TO A DOSE Question 14 You have dopamine 200 mg in 50 ml and the rate at which the pump is running is 4 ml/hour. The prescribed dose is 3 mcg/kg/min. What dose is the pump delivering? (Patient s weight = 89 kg) If the dose is wrong, at which rate should the pump be set? Question 15 You have dobutamine 250 mg in 50 ml and the rate at which the pump is running is 5.4 ml/hour. The prescribed dose is 6 mcg/kg/min. What dose is the pump delivering? (Patient s weight = 64 kg) If the dose is wrong, at which rate should the pump be set?
67 CONVERSION OF ml/hour BACK TO A DOSE Question 16) You have dopexamine 50 mg in 50 ml and the rate at which the pump is running is 28 ml/hour. The prescribed dose is 6 mcg/kg/min. What dose is the pump delivering? (Patient s weight = 78 kg) If the dose is wrong, at which rate should the pump be set?
68 CALCULATING THE LENGTH OF TIME FOR IV INFUSIONS MANUALLY CONTROLLED INFUSIONS The doctor prescribes 1 liter of 5% glucose to be given over 8 hours. The drip rate for the infusion is calculated to be 42 drops/min. You wish to check the drip rate; how many hours is the infusion going to run? (SGS = 20 drops/ml)
69 CALCULATING THE LENGTH OF TIME FOR IV INFUSIONS Question 17) A 500 ml infusion of sodium chloride 0.9% is being given over 4 hours. The rate at which the infusion is being run is 42 drops/min. How long will the infusion run at the specified rate (SGS)? Question 18) A 1 litre infusion of sodium chloride 0.9% is being given over 12 hours. The rate at which the infusion is being run is 83mL/hour. How long will the infusion run at the specified rate?
70 Infusion devices 1. Gravity devices Gravity devices depend entirely on gravity to drive the infusion; the pressure for the infusion depends on the height of the liquid above the infusion site. Flow is measured by counting the drops. A gravity device should only be considered for low-risk infusions such as sodium chloride, dextrose saline and dextrose infusions. A gravity device should not be used for infusions containing potassium, or drug therapies requiring accurate monitoring or delivery of accurate volumes. Infusions, even low risk, should not be delivered to volumesensitive patients via a gravity line but must be given via an infusion pump.
71 Infusion devices 2. pumped systems Volumetric pumps Volumetric pumps are the preferred pumps for medium and large flow rate and large volume infusions; although some are designed specially to operate at low flow rates for neonatal use. The rate is given in millilitres per hour (typical range ml/hour). Typically, most volumetric pumps will perform satisfactorily at rates down to 5mL/hour.A syringe pump should be used for rates lower than 5mL/hour or when short-term accuracy is required. For delivery of low-risk infusions a gravity device should be considered rather than a volumetric pump, unless accurate monitoring is required, or the patient is at risk of fluid overload
72 Infusion devices 2. pumped systems Syringe pumps Syringe pumps are used to administer drugs or infusions in small or medium volumes, and are calibrated for delivery in millilitres per hour, typically 0.1 to 99mL/hour. Syringe pumps have better short-term accuracy than volumetric pumps and are therefore typically superior when delivering drugs at rates below 5mL/hour. Syringe pumps are used extensively where small volumes of highly concentrated drugs are required at low flow rates usually in intensive care settings.

73 Syringe pumps
74 Infusion devices 2. pumped systems Patient-controlled analgesia (PCA) pumps Patient-controlled analgesia (PCA) pumps are specifically designed to deliver analgesia to meet individual needs and to allow patients to have some control over their own analgesia. They are typically syringe pumps and the difference between a PCA pump and a normal syringe pump is that patients are able to deliver a bolus dose themselves. Clinical staff may program a PCA pump to deliver a pre-set bolus on demand, or have a pre-set lockout time between boluses. In addition, PCA pumps may also be programmed to deliver a basal (continuous, low rate) infusion. Once programmed, access to the control of the pump is usually restricted. A feature of most PCA pumps is a memory log, which enables the clinician to determine when, and how often, the patient has made a demand and what total volume of drug has been infused over a given time.
Cardiac Catheter Labs Intravenous Drug Therapy Guide
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Cardiac Catheter Lab IV Medicines Guideline Helen Buxton ( Senior Cath Lab
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Cardiac Catheter Lab IV Medicines Guideline Helen Buxton ( Senior Cath Lab
Easy way to calculate drugs MONA ALHARBI
 Easy way to calculate drugs MONA ALHARBI Objective At the end of this lecture you should be able to : Calculate dosage drugs. Calculate drip rate (drops/min). Conversion of dosages to ml/hour Calculating
Easy way to calculate drugs MONA ALHARBI Objective At the end of this lecture you should be able to : Calculate dosage drugs. Calculate drip rate (drops/min). Conversion of dosages to ml/hour Calculating
Intravenous Fluid and Drug Therapy
 11 Intravenous Fluid and Drug Therapy OUTLINE Overview Direct Intravenous Injections Continuous Intravenous Injections Solution Additives Calculating IV Components as Percentages Calculating IV Flow Rates
11 Intravenous Fluid and Drug Therapy OUTLINE Overview Direct Intravenous Injections Continuous Intravenous Injections Solution Additives Calculating IV Components as Percentages Calculating IV Flow Rates
LET - Maths, Stats & Numeracy
 Metric Conversions Here are some metric weights arranged in size order, starting with the biggest:- Kg (kilogram) g (gram) mg (milligram) mcg (microgram) Each one is a thousand (1000) times smaller than
Metric Conversions Here are some metric weights arranged in size order, starting with the biggest:- Kg (kilogram) g (gram) mg (milligram) mcg (microgram) Each one is a thousand (1000) times smaller than
Common Infusions for Neonatal Use
 Common Infusions for Neonatal Use Document Title and Reference : Common Infusions for Neonatal Use Main Author (s) Dr N B Soni Ratified by: LSC CEG Date Ratified: May 2016 Review Date: May 2018 Version:
Common Infusions for Neonatal Use Document Title and Reference : Common Infusions for Neonatal Use Main Author (s) Dr N B Soni Ratified by: LSC CEG Date Ratified: May 2016 Review Date: May 2018 Version:
Package leaflet: Information for the patient. NEGABAN 1g, powder for solution for injection or infusion Temocillin
 Package leaflet: Information for the patient NEGABAN 1g, powder for solution for injection or infusion Temocillin Read all of this leaflet carefully before you start using this medicine because it contains
Package leaflet: Information for the patient NEGABAN 1g, powder for solution for injection or infusion Temocillin Read all of this leaflet carefully before you start using this medicine because it contains
Nonparenteral medications
 Nonparenteral medications Capsules and unscored tablets are rounded to the nearest whole tablet. Scored tablets are rounded to the nearest 1/2 tablet. Liquid medications are rounded to one decimal place
Nonparenteral medications Capsules and unscored tablets are rounded to the nearest whole tablet. Scored tablets are rounded to the nearest 1/2 tablet. Liquid medications are rounded to one decimal place
INTRAVENOUS THERAPY INSTRUCTIONAL PACKAGE
 INTRAVENOUS THERAPY INSTRUCTIONAL PACKAGE WORKBOOK FOR THE CALCULATION OF FLOW RATES AND MEDICATION DOSAGES January 2014 WORKBOOK C O N T E N T S Page Professional Responsibilities 3 Methods for flowrate
INTRAVENOUS THERAPY INSTRUCTIONAL PACKAGE WORKBOOK FOR THE CALCULATION OF FLOW RATES AND MEDICATION DOSAGES January 2014 WORKBOOK C O N T E N T S Page Professional Responsibilities 3 Methods for flowrate
PACKAGE LEAFLET: INFORMATION FOR THE USER. SODIPHOS 22mEq / 10ml Concentrate for solution for infusion. Disodium phosphate dihydrate
 PACKAGE LEAFLET: INFORMATION FOR THE USER SODIPHOS 22mEq / 10ml Concentrate for solution for infusion Disodium phosphate dihydrate Read all of this leaflet carefully before you start using this medicine.
PACKAGE LEAFLET: INFORMATION FOR THE USER SODIPHOS 22mEq / 10ml Concentrate for solution for infusion Disodium phosphate dihydrate Read all of this leaflet carefully before you start using this medicine.
Chapter 64 Administration of Injectable Medications
 Chapter 64 Administration of Injectable Medications Injectable Medications Injection or intravenous (IV) infusion More invasive than administration by mouth, rectum, or through the skin Common methods
Chapter 64 Administration of Injectable Medications Injectable Medications Injection or intravenous (IV) infusion More invasive than administration by mouth, rectum, or through the skin Common methods
RECONSTITUTION, DOSING AND ADMINISTRATION
 Prescribing Information can be found within this document CORRECT RECONSTITUTION FOR SC AND IV ADMINISTRATION VELCADE (bortezomib) 3.5 mg powder for solution for injection is available for intravenous
Prescribing Information can be found within this document CORRECT RECONSTITUTION FOR SC AND IV ADMINISTRATION VELCADE (bortezomib) 3.5 mg powder for solution for injection is available for intravenous
Parenteral Products. By: Howida Kamal, Ph.D
 Parenteral Products By: Howida Kamal, Ph.D Dosage forms Route of administration Enteral INTO Parenteral ONTO Topical Dosage forms Physical form Solid Liquid Semi-solid Powder Granules Tablets Capsules
Parenteral Products By: Howida Kamal, Ph.D Dosage forms Route of administration Enteral INTO Parenteral ONTO Topical Dosage forms Physical form Solid Liquid Semi-solid Powder Granules Tablets Capsules
Southern Trust Home IV Service. Guidelines for the administration of IV antibiotics
 Southern Trust Home IV Service Guidelines for the administration of IV antibiotics Title: Author: CLINICAL GUIDELINES ID TAG Antibiotic guidelines - Southern Trust Home IV service guidelines for the administration
Southern Trust Home IV Service Guidelines for the administration of IV antibiotics Title: Author: CLINICAL GUIDELINES ID TAG Antibiotic guidelines - Southern Trust Home IV service guidelines for the administration
PRESCRIBING INFORMATION. Dextrose Injection USP. (Concentrated Dextrose for Intravenous Administration) 50% (500 mg/ml) Fluid and Nutrient Replenisher
 50% (500 mg/ml) Fluid and Nutrient Replenisher") PRESCRIBING INFORMATION Dextrose Injection USP (Concentrated Dextrose for Intravenous Administration) 50% (500 mg/ml) Fluid and Nutrient Replenisher Pfizer Canada Inc. 17300 Trans-Canada Highway Kirkland,
PRESCRIBING INFORMATION Dextrose Injection USP (Concentrated Dextrose for Intravenous Administration) 50% (500 mg/ml) Fluid and Nutrient Replenisher Pfizer Canada Inc. 17300 Trans-Canada Highway Kirkland,
CONTROLLED DOCUMENT. Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) Controlled Document Number: CG259
 Controlled Document Number: CG259") Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor:
Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor:
48 th Annual Meeting. A Review of Pharmacy Calculations for Pharmacy Technicians. Metric System of Measurement. Disclosure. Common Conversions
 48 th Annual Meeting A Review of Pharmacy Calculations for Pharmacy Technicians Nina Pavuluri, Ph.D. Navigating the Oceans of Opportunity Metric System of Measurement Base Unit Factor Name Symbol 1 (g,
48 th Annual Meeting A Review of Pharmacy Calculations for Pharmacy Technicians Nina Pavuluri, Ph.D. Navigating the Oceans of Opportunity Metric System of Measurement Base Unit Factor Name Symbol 1 (g,
Good practice for drug calculations
 Good practice for drug calculations A step-by-step guide for nurses, doctors and all other healthcare professionals Pharmacyservices 7048 Drug Cal Guide A6 Update_AW.indd 1 22/07/2014 09:55 2 Contents
Good practice for drug calculations A step-by-step guide for nurses, doctors and all other healthcare professionals Pharmacyservices 7048 Drug Cal Guide A6 Update_AW.indd 1 22/07/2014 09:55 2 Contents
Jo Kuehn, RN, MSN, CPHQ Jenell Westhoven, RN, BSN
 Jo Kuehn, RN, MSN, CPHQ Jenell Westhoven, RN, BSN Disclosure Information Intravenous Therapy and Parenteral Nutrition Administration: Nursing In- Focus Jo Kuehn, RN, MSN, CPHQ and Jenell Westhoven, RN,
Jo Kuehn, RN, MSN, CPHQ Jenell Westhoven, RN, BSN Disclosure Information Intravenous Therapy and Parenteral Nutrition Administration: Nursing In- Focus Jo Kuehn, RN, MSN, CPHQ and Jenell Westhoven, RN,
IV Fluids Nursing B23 Objectives Serum Osmolality 275 to 295 Isotonic
 1 IV Fluids Nursing B23 2 Objectives 3 Serum Osmolality Serum osmolality solute concentration of a solution Higher osmolality means greater pulling power for water Normal serum osmolality is 275 to 295
1 IV Fluids Nursing B23 2 Objectives 3 Serum Osmolality Serum osmolality solute concentration of a solution Higher osmolality means greater pulling power for water Normal serum osmolality is 275 to 295
CHEMOTHERAPY NETWORK GROUP POLICY FOR ADMINISTRATION OF CYTOTOXIC CHEMOTHERAPY
 CHEMOTHERAPY NETWORK GROUP POLICY FOR ADMINISTRATION OF CYTOTOXIC CHEMOTHERAPY Version 4.0 March 2016 Review date March 2018 Introduction It is the purpose of this policy to provide clear guidelines that
CHEMOTHERAPY NETWORK GROUP POLICY FOR ADMINISTRATION OF CYTOTOXIC CHEMOTHERAPY Version 4.0 March 2016 Review date March 2018 Introduction It is the purpose of this policy to provide clear guidelines that
IV Fluids. Nursing B23. Objectives. Serum Osmolality
 IV Fluids Nursing B23 Objectives Discuss the purpose of IV Discuss nursing interventions in IV therapy Identify complications of IV therapy Differentiate between peripheral line, central line, and PICC
IV Fluids Nursing B23 Objectives Discuss the purpose of IV Discuss nursing interventions in IV therapy Identify complications of IV therapy Differentiate between peripheral line, central line, and PICC
IV Drug Delivery Systems used in Cancer Care
 IV Drug Delivery Systems used in Cancer Care Cheri Constantino-Shor, RN, MSN, CRNI Seattle Cancer Care Alliance Nursing Staff Development Coordinator Presentation Objective Describe drug delivery devices
IV Drug Delivery Systems used in Cancer Care Cheri Constantino-Shor, RN, MSN, CRNI Seattle Cancer Care Alliance Nursing Staff Development Coordinator Presentation Objective Describe drug delivery devices
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS
 PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
ASEPTIC DISPENSING TECHNIQUES/DRUG- NUTRIENT INTERACTIONS
 ASEPTIC DISPENSING TECHNIQUES/DRUG- NUTRIENT INTERACTIONS HARBANS KAUR DHILLON PRESIDENT OF PENSMA KUALA LUMPUR MALAYSIA PENSA 2007 University Malaya Medical Centre Kuala Lumpur ASEPTIC DISPENSING Ppn
ASEPTIC DISPENSING TECHNIQUES/DRUG- NUTRIENT INTERACTIONS HARBANS KAUR DHILLON PRESIDENT OF PENSMA KUALA LUMPUR MALAYSIA PENSA 2007 University Malaya Medical Centre Kuala Lumpur ASEPTIC DISPENSING Ppn
SUMMARY OF PRODUCT CHARACTERISTICS
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE VETERINARY MEDICINAL PRODUCT Aqupharm 3 Solution for Infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Active ingredients Sodium Chloride Glucose Anhydrous
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE VETERINARY MEDICINAL PRODUCT Aqupharm 3 Solution for Infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Active ingredients Sodium Chloride Glucose Anhydrous
Guideline for the Management of Continuous IV Vancomycin Infusion in Neonates on NICU A Clinical Guideline recommended for use
 Guideline for the Management of Continuous IV Vancomycin Infusion in A Clinical Guideline recommended for use For Use in: By: For: Division responsible for document: Key words: Name and job title of document
Guideline for the Management of Continuous IV Vancomycin Infusion in A Clinical Guideline recommended for use For Use in: By: For: Division responsible for document: Key words: Name and job title of document
UTMB DEPARTMENT OF PHARMACY POLICY AND PROCEDURES Section Medication Use ADMINISTRATION OF MEDICATION BY IV PUSH
 Page 1 of 8 ADMINISTRATION OF MEDICATION BY IV PUSH AUDIENCE POLICY This document is directed to Registered Nurses (RNs), Licensed Vocational Nurses (LVN s), and physicians. The following delineates the
Page 1 of 8 ADMINISTRATION OF MEDICATION BY IV PUSH AUDIENCE POLICY This document is directed to Registered Nurses (RNs), Licensed Vocational Nurses (LVN s), and physicians. The following delineates the
Module 8: Practice Problems
 Module 8: Practice Problems 1. Convert a blood plasma level range of 5 to 20 µg/ml of tobramycin (Z = 467.52) to µmol/l. 5 µg/ml = 10.7 µmol/l 20 µg/ml = 42.8 µmol/l 2. A preparation contains in each milliliter,
Module 8: Practice Problems 1. Convert a blood plasma level range of 5 to 20 µg/ml of tobramycin (Z = 467.52) to µmol/l. 5 µg/ml = 10.7 µmol/l 20 µg/ml = 42.8 µmol/l 2. A preparation contains in each milliliter,
ADENOSINE. ADRENALINE (Epinephrine)
") ADENOSINE Notes Arrhythmias I.V. Initial dose 150 micrograms/kg stat Increase dose if required by 50 micrograms/kg to a maximum of 300 micrograms/kg (or 500 micrograms/kg if over 28 days old) ADMINISTRATION
ADENOSINE Notes Arrhythmias I.V. Initial dose 150 micrograms/kg stat Increase dose if required by 50 micrograms/kg to a maximum of 300 micrograms/kg (or 500 micrograms/kg if over 28 days old) ADMINISTRATION
IMDG CODE Poison Treatment Chest
 2018 IMDG CODE Poison Treatment Chest This document contains the complete list of medicines and medical supplies for the vessels poison treatment chest and is based on the IMDG code international maritime
2018 IMDG CODE Poison Treatment Chest This document contains the complete list of medicines and medical supplies for the vessels poison treatment chest and is based on the IMDG code international maritime
PACKAGE LEAFLET: INFORMATION FOR THE USER. Active substance: enoximone
 PACKAGE LEAFLET 1 PACKAGE LEAFLET: INFORMATION FOR THE USER Perfan Injection 100 mg/20 ml Concentrate for Solution for Injection Active substance: enoximone Read all of this leaflet carefully before you
PACKAGE LEAFLET 1 PACKAGE LEAFLET: INFORMATION FOR THE USER Perfan Injection 100 mg/20 ml Concentrate for Solution for Injection Active substance: enoximone Read all of this leaflet carefully before you
Math for Meds. College of Southern Nevada. Practice Problems. Nursing 211
 Math for Meds College of Southern Nevada Nursing 211 Name: Date: Directions: 1. Solve the dosage calculation problems utilizing the method of your choice. 2. Show your work! 3.Divide math out to the thousandth
Math for Meds College of Southern Nevada Nursing 211 Name: Date: Directions: 1. Solve the dosage calculation problems utilizing the method of your choice. 2. Show your work! 3.Divide math out to the thousandth
PARENTERAL PREPARATIONS
 PARENTERAL PREPARATIONS INTRODUCTION Parenteral (Gk, para enteron, beside the intestine) dosage forms differ from all other drug dosage forms, because they are injected directly into body tissue through
PARENTERAL PREPARATIONS INTRODUCTION Parenteral (Gk, para enteron, beside the intestine) dosage forms differ from all other drug dosage forms, because they are injected directly into body tissue through
Cumulative Math Practice Worksheet
 Name: Date: Use the following to answer questions 1-3: Fill in the blank for each pair of ratios to form a proportion: 1. How many capsules are needed to fill a prescription for three days for mefenamic
Name: Date: Use the following to answer questions 1-3: Fill in the blank for each pair of ratios to form a proportion: 1. How many capsules are needed to fill a prescription for three days for mefenamic
IMDG CODE Poison Treatment Chest
 2017 IMDG CODE Poison Treatment Chest This document contains the complete list of medicines and medical supplies for the vessels poison treatment chest and is based on the IMDG code international maritime
2017 IMDG CODE Poison Treatment Chest This document contains the complete list of medicines and medical supplies for the vessels poison treatment chest and is based on the IMDG code international maritime
Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS
 Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS PRACTICE POINTS Give the right blood product to the right patient at the right time. Failure to correctly check the patient or the pack can be fatal. At the
Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS PRACTICE POINTS Give the right blood product to the right patient at the right time. Failure to correctly check the patient or the pack can be fatal. At the
MORPHINE ADMINISTRATION
 Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Within the proportion the two outside numbers are referred to as the extremes. The two inside numbers are referred to as the means.
 Basic Formulas Speaker: Jana Ogden This lecture will demonstrate the expectations for performing a variety of the more complex calculations. You are expected to refer to your text and complete the designated
Basic Formulas Speaker: Jana Ogden This lecture will demonstrate the expectations for performing a variety of the more complex calculations. You are expected to refer to your text and complete the designated
IMMUNOGLOBULIN REPLACEMENT THERAPY: ONE SIZE DOESN T FIT ALL
 PRIMARY IMMUNODEFICIENCIES IMMUNOGLOBULINS: ONE SIZE DOESN T FIT ALL IMMUNOGLOBULIN REPLACEMENT THERAPY: ONE SIZE DOESN T FIT ALL 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS IG IPOPI IV PID SC Immunoglobulins
PRIMARY IMMUNODEFICIENCIES IMMUNOGLOBULINS: ONE SIZE DOESN T FIT ALL IMMUNOGLOBULIN REPLACEMENT THERAPY: ONE SIZE DOESN T FIT ALL 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS IG IPOPI IV PID SC Immunoglobulins
Artesunate 60 mg for injection WHOPAR part 3 November 2015 (Guilin Pharmaceutical Co., Ltd.), MA051 PATIENT INFORMATION LEAFLET
, MA051 PATIENT INFORMATION LEAFLET") PATIENT INFORMATION LEAFLET 1 PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER Artesun 60mg * Artesunate 60 mg for injection and sodium bicarbonate injection 50 mg/ml (1ml) and sodium chloride injection
PATIENT INFORMATION LEAFLET 1 PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER Artesun 60mg * Artesunate 60 mg for injection and sodium bicarbonate injection 50 mg/ml (1ml) and sodium chloride injection
NEWBORN EMERGENCY TRANSPORT SERVICE MEDICAL GUIDELINES
 WOMEN AND NEWBORN HEALTH SERVICE King Edward Memorial Hospital NEWBORN EMERGENCY TRANSPORT SERVICE MEDICAL GUIDELINES Transport Medication List Title of policy: Transport Medication List Date Revised:
WOMEN AND NEWBORN HEALTH SERVICE King Edward Memorial Hospital NEWBORN EMERGENCY TRANSPORT SERVICE MEDICAL GUIDELINES Transport Medication List Title of policy: Transport Medication List Date Revised:
NURSING PRACTICE GUIDELINES
 NURSING PRACTICE GUIDELINES ADMINISTRATION OF SUBCUTANEOUS FLUIDS INTRODUCTION The infusion of a solution into the subcutaneous tissues is called hypodermoclysis. The subcutaneous compartment (hypodermis)
NURSING PRACTICE GUIDELINES ADMINISTRATION OF SUBCUTANEOUS FLUIDS INTRODUCTION The infusion of a solution into the subcutaneous tissues is called hypodermoclysis. The subcutaneous compartment (hypodermis)
Artesunate 60 mg for injection WHOPAR part 3 June 2013 (Guilin Pharmaceutical Co., Ltd.), MA051 PATIENT INFORMATION LEAFLET
, MA051 PATIENT INFORMATION LEAFLET") PATIENT INFORMATION LEAFLET 1 PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER Artesun * Artesunate 60 mg for injection and sodium bicarbonate injection 50 mg/ml (1ml) and sodium chloride injection
PATIENT INFORMATION LEAFLET 1 PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER Artesun * Artesunate 60 mg for injection and sodium bicarbonate injection 50 mg/ml (1ml) and sodium chloride injection
Medication Calculation Practice Problems
 Medication Calculation Practice Problems Below is a section of the list of medications that are programmed in the Alaris IV Pump s Guardrail Drug Library. During your orientation you will learn more about
Medication Calculation Practice Problems Below is a section of the list of medications that are programmed in the Alaris IV Pump s Guardrail Drug Library. During your orientation you will learn more about
Home Care Services HomeMed MedEQUIP Michigan Visiting Care Michigan Visiting Nurses Wheelchair Seating Service PROCEDURE
 UNIVERSITY OF MICHIGAN HOSPITALS AND HEALTH CENTERS UMHHC-HCS: 253.054 First Approved Date: 3/2010 Home Care Services HomeMed MedEQUIP Michigan Visiting Care Michigan Visiting Nurses Wheelchair Seating
UNIVERSITY OF MICHIGAN HOSPITALS AND HEALTH CENTERS UMHHC-HCS: 253.054 First Approved Date: 3/2010 Home Care Services HomeMed MedEQUIP Michigan Visiting Care Michigan Visiting Nurses Wheelchair Seating
Neonatal Guidelines. Chapter 15: Pharmacy related Version: Date Revised: 24 th January 2017
 Neonatal Guidelines Chapter 15: Pharmacy related Version: 2017.1 Specialty: Neonatal Medicine Revised by: Katherine Wilson Edited by: Sujoy Banerjee Date Revised: 24 th January 2017 Approved by: ABMU Joint
Neonatal Guidelines Chapter 15: Pharmacy related Version: 2017.1 Specialty: Neonatal Medicine Revised by: Katherine Wilson Edited by: Sujoy Banerjee Date Revised: 24 th January 2017 Approved by: ABMU Joint
ISMP guidelines that support intravenous drug delivery system safety
 ISMP guidelines that support intravenous drug delivery system safety Michael R. Cohen, RPh, MS, ScD (hon), DPS (hon), FASHP Institute for Safe Medication Practices Sterile Compounding Errors and Patient
ISMP guidelines that support intravenous drug delivery system safety Michael R. Cohen, RPh, MS, ScD (hon), DPS (hon), FASHP Institute for Safe Medication Practices Sterile Compounding Errors and Patient
PACKAGE LEAFLET: INFORMATION FOR THE USER
 PACKAGE LEAFLET: INFORMATION FOR THE USER Ceftazidime 500 mg powder for solution for injection Ceftazidime 1 g powder for solution for injection/infusion Ceftazidime 2 g powder for solution for injection/infusion
PACKAGE LEAFLET: INFORMATION FOR THE USER Ceftazidime 500 mg powder for solution for injection Ceftazidime 1 g powder for solution for injection/infusion Ceftazidime 2 g powder for solution for injection/infusion
Unit 11. Objectives. Indications for IV Therapy. Intravenous Access Devices & Common IV Fluids. 3 categories. Maintenance Replacement Restoration
 Unit 11 Fluids, Electrolytes and Acid Base Imbalances Intravenous Access Devices & Common IV Fluids Objectives Review the purpose and types of intravenous (IV) therapy. Recall the nursing care related
Unit 11 Fluids, Electrolytes and Acid Base Imbalances Intravenous Access Devices & Common IV Fluids Objectives Review the purpose and types of intravenous (IV) therapy. Recall the nursing care related
Central Line Care and Management
 Central Line Care and Management What is a Central Line/ CVAD? (central venous access device) A vascular infusion device that terminates at or close to the heart or in one of the great vessels (aorta,
Central Line Care and Management What is a Central Line/ CVAD? (central venous access device) A vascular infusion device that terminates at or close to the heart or in one of the great vessels (aorta,
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE PARENTERAL NUTRITION ADMINISTRATION AND MONITORING SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Pharmacy Services, Nutrition Services, and Health
TITLE PARENTERAL NUTRITION ADMINISTRATION AND MONITORING SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Pharmacy Services, Nutrition Services, and Health
ATI Skills Modules Checklist for Central Venous Access Devices
 For faculty use only Educator s name Score Date ATI Skills Modules Checklist for Central Venous Access Devices Student s name Date Verify order Patient record Assess for procedure need Identify, gather,
For faculty use only Educator s name Score Date ATI Skills Modules Checklist for Central Venous Access Devices Student s name Date Verify order Patient record Assess for procedure need Identify, gather,
Review calculation procedures for the following:
 Review calculation procedures for the following: Convert in the Metric System 1000 mg = 1 gram 1000 ml = 1 liter To convert from grams to mg, move the decimal point 3 places to the right (add zeros to
Review calculation procedures for the following: Convert in the Metric System 1000 mg = 1 gram 1000 ml = 1 liter To convert from grams to mg, move the decimal point 3 places to the right (add zeros to
Pharmaceutical Calculations
 Pharmaceutical Calculations Introduction Pharmaceutical calculations dealing with: Expressions of concentration Master formulae to working quantities Changing concentrations Small quantities ( trituration)
Pharmaceutical Calculations Introduction Pharmaceutical calculations dealing with: Expressions of concentration Master formulae to working quantities Changing concentrations Small quantities ( trituration)
DRUG GUIDELINE SODIUM NITROPRUSSIDE
 DRUG GUIDELINE SODIUM NITROPRUSSIDE SCOPE (Area): FOR USE IN: Critical Care Unit, ED and Theatre EXCLUSIONS: Paediatrics (seek Paediatrician advice) and General Wards SCOPE (Staff): Medical, Nursing and
DRUG GUIDELINE SODIUM NITROPRUSSIDE SCOPE (Area): FOR USE IN: Critical Care Unit, ED and Theatre EXCLUSIONS: Paediatrics (seek Paediatrician advice) and General Wards SCOPE (Staff): Medical, Nursing and
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Risk factors and drugs/infusion commonly associated with tissue damage include: Extreme Prematurity Dextrose greater than 12.
 Neonatal Intensive Care Unit Clinical Guideline Extravasation injuries Extravasation is defined as the inadvertent leakage of infused fluid into the surrounding tissue. The resultant damage to tissue can
Neonatal Intensive Care Unit Clinical Guideline Extravasation injuries Extravasation is defined as the inadvertent leakage of infused fluid into the surrounding tissue. The resultant damage to tissue can
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: INTERMITTENT FLUID AND MEDICATION THERAPY Nursing DATE: REVIEWED: PAGES: RESPONSIBILITY: RN, LPN I, LPN II Per Job Description 03/81 8/09
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: INTERMITTENT FLUID AND MEDICATION THERAPY Nursing DATE: REVIEWED: PAGES: RESPONSIBILITY: RN, LPN I, LPN II Per Job Description 03/81 8/09
Pharmacy Instructions for Preparation
 MARQIBO (vincristine sulfate LIPOSOME injection) Pharmacy Instructions for Preparation Important Information for Preparation 1 The instructions for the constitution of MARQIBO are provided in each kit.
MARQIBO (vincristine sulfate LIPOSOME injection) Pharmacy Instructions for Preparation Important Information for Preparation 1 The instructions for the constitution of MARQIBO are provided in each kit.
SUMMARY OF PRODUCT CHARACTERISTICS. Synthamin 14, 8.5% Amino Acid Intravenous Infusion
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Synthamin 14, 8.5% Amino Acid Intravenous Infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION L-Leucine Ph. Eur 0.620% w/v L-Isoleucine
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Synthamin 14, 8.5% Amino Acid Intravenous Infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION L-Leucine Ph. Eur 0.620% w/v L-Isoleucine
From the joint NHS pharmacy technical services groups, for distribution via local NHS network groups:- Dear NHS Colleague,
 From the joint NHS pharmacy technical services groups, for distribution via local NHS network groups:- Dear NHS Colleague, Supporting document for NPSA Injectables Patient Safety Alert Attached is a document
From the joint NHS pharmacy technical services groups, for distribution via local NHS network groups:- Dear NHS Colleague, Supporting document for NPSA Injectables Patient Safety Alert Attached is a document
EZ-IO. Offline Reading Download as PDF. Welcome. Introduction. Anatomy and Physiology. Indications. Paediatric Considerations.
 EZ-IO Acknowledgement This training package was created by David Funnell, Joseph Schar, and Jordan Pring. Please direct any questions to your CSO or Team Leader. Offline Reading Download as PDF Welcome
EZ-IO Acknowledgement This training package was created by David Funnell, Joseph Schar, and Jordan Pring. Please direct any questions to your CSO or Team Leader. Offline Reading Download as PDF Welcome
Neonatal Parenteral Nutrition Guideline Dr M Hogan, Maire Cullen ANNP, Una Toland Ward Manager, Sandra Kilpatrick Neonatal Pharmacist
 CLINICAL GUIDELINES ID TAG Title: Author: Designation: Speciality / Division: Directorate: Neonatal Parenteral Nutrition Guideline Dr M Hogan, Maire Cullen ANNP, Una Toland Ward Manager, Sandra Kilpatrick
CLINICAL GUIDELINES ID TAG Title: Author: Designation: Speciality / Division: Directorate: Neonatal Parenteral Nutrition Guideline Dr M Hogan, Maire Cullen ANNP, Una Toland Ward Manager, Sandra Kilpatrick
ASSESSMENT AND CARE Monitor for the following and remove catheter if there is: redness, pain, swelling, firm tissue, exudates, bleeding or leakage.
 POLICY An Indwelling subcutaneous catheter may be inserted when an infant requires regular subcutaneous injections (At least one subcutaneous injection per day). SUPPORTIVE DATA In the NICU medications
POLICY An Indwelling subcutaneous catheter may be inserted when an infant requires regular subcutaneous injections (At least one subcutaneous injection per day). SUPPORTIVE DATA In the NICU medications
Paediatric Formulations The Clinical Perspective
 Paediatric Formulations The Clinical Perspective Tony Nunn & Sara Arenas-Lopez Paediatric Pharmacists Alder Hey Children s Hospital, Liverpool, U.K. Evelina Children s Hospital, Guy s & St Thomas NHS Foundation
Paediatric Formulations The Clinical Perspective Tony Nunn & Sara Arenas-Lopez Paediatric Pharmacists Alder Hey Children s Hospital, Liverpool, U.K. Evelina Children s Hospital, Guy s & St Thomas NHS Foundation
A step-by-step preparation guide
 A step-by-step preparation guide For needle and needle-free systems This guide provides detailed instructions on the reconstitution, dilution, and storage of VELETRI. It is intended to be used after your
A step-by-step preparation guide For needle and needle-free systems This guide provides detailed instructions on the reconstitution, dilution, and storage of VELETRI. It is intended to be used after your
** Medication exercises ** NICU Phase II
 ** Medication exercises ** NICU Phase II A) Baby A has had a bowel resection six hours ago. She weighs 3 kg. Post-op, she is quite agitated and she is on a fentanyl drip at 2 micrograms/kg/hr (#1). She
** Medication exercises ** NICU Phase II A) Baby A has had a bowel resection six hours ago. She weighs 3 kg. Post-op, she is quite agitated and she is on a fentanyl drip at 2 micrograms/kg/hr (#1). She
Clinical Calculation 5 th Edition
 Clinical Calculation 5 th Edition Chapter 6 Calculation of Oral Medications Pages 40-54 Oral Medications Medications that are administered by mouth and absorbed via the gastrointestinal tract are known
Clinical Calculation 5 th Edition Chapter 6 Calculation of Oral Medications Pages 40-54 Oral Medications Medications that are administered by mouth and absorbed via the gastrointestinal tract are known
PACKAGE LEAFLET: INFORMATION FOR THE USER. Glucose Intravenous Infusion BP 10% w/v solution for infusion Glucose (as glucose monohydrate)
") PACKAGE LEAFLET: INFORMATION FOR THE USER Glucose Intravenous Infusion BP 10% w/v solution for infusion Glucose (as glucose monohydrate) Read all of this leaflet carefully before you start using this medicine
PACKAGE LEAFLET: INFORMATION FOR THE USER Glucose Intravenous Infusion BP 10% w/v solution for infusion Glucose (as glucose monohydrate) Read all of this leaflet carefully before you start using this medicine
ADVANCED ASSESSMENT Medical Math
 ONTARIO BASE HOSPITAL GROUP ADVANCED ASSESSMENT Medical Math 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Medical Math AUTHOR Tim Dodd AEMCA, ACP Hamilton Base Hospital REVIEWERS/CONTRIBUTORS Rob
ONTARIO BASE HOSPITAL GROUP ADVANCED ASSESSMENT Medical Math 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Medical Math AUTHOR Tim Dodd AEMCA, ACP Hamilton Base Hospital REVIEWERS/CONTRIBUTORS Rob
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS EPTIFIBATIDE (INTEGRILIN) PROTOCOL
 PROTOCOL") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE S EPTIFIBATIDE (INTEGRILIN) I. PURPOSE: A. Integrilin (Eptifibatide) is a specific and potent inhibitor of the platelet receptor glycoprotein
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE S EPTIFIBATIDE (INTEGRILIN) I. PURPOSE: A. Integrilin (Eptifibatide) is a specific and potent inhibitor of the platelet receptor glycoprotein
Critical Care Standard Infusion Concentrations
 Acetylcisteine (NAC) Actrapid - Human Insulin Addiphos 20mmol Addiphos 40mmol Adrenaline (Epinephrine) vs peripheral 10 g in 50mL 200mg per ml 50 units in 50mL 1 unit per ml sodium chloride 20 mmol in
Acetylcisteine (NAC) Actrapid - Human Insulin Addiphos 20mmol Addiphos 40mmol Adrenaline (Epinephrine) vs peripheral 10 g in 50mL 200mg per ml 50 units in 50mL 1 unit per ml sodium chloride 20 mmol in
Successful IV Starts Revised February 2014
 Successful IV Starts Revised February 2014 Why Intravenous Therapy? Used for access to the body s circulation Indications: Administer fluids, blood, medications, and nutrition Obtain laboratory specimens
Successful IV Starts Revised February 2014 Why Intravenous Therapy? Used for access to the body s circulation Indications: Administer fluids, blood, medications, and nutrition Obtain laboratory specimens
DRAFT PROPOSAL FOR REVISION OF GENERAL MONOGRAPHS: PARENTERAL PREPARATIONS. (July 2012) Draft for comment
 Draft for comment") 1 2 3 4 5 DRAFT PROPOSAL FOR REVISION OF July 2012 RESTRICTED GENERAL MONOGRAPHS: PARENTERAL PREPARATIONS (July 2012) Draft for comment This document was provided by a quality control expert. Should you
1 2 3 4 5 DRAFT PROPOSAL FOR REVISION OF July 2012 RESTRICTED GENERAL MONOGRAPHS: PARENTERAL PREPARATIONS (July 2012) Draft for comment This document was provided by a quality control expert. Should you
Helping to protect you from exposure to hazardous drugs
 Helping to protect you from exposure to hazardous drugs Closed system solution: Texium closed male luer and SmartSite needle-free valve products What you can t see can hurt you The risks are well documented
Helping to protect you from exposure to hazardous drugs Closed system solution: Texium closed male luer and SmartSite needle-free valve products What you can t see can hurt you The risks are well documented
Reference ID:
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PRISMASOL and PHOXILLUM safely and effectively. See full prescribing information for PRISMASOL and
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PRISMASOL and PHOXILLUM safely and effectively. See full prescribing information for PRISMASOL and
Nab-Paclitaxel (Abraxane) and Gemcitabine For Pancreatic Adenocarcinoma Cumbria, Northumberland, Tyne & Wear Area Team
 and Gemcitabine For Pancreatic Adenocarcinoma Cumbria, Northumberland, Tyne & Wear Area Team") DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent & Rate 1 8 15 Sodium Chloride 0.9% 100ml Infusion Fast Running Dexamethasone 8mg Oral Ondansetron 8mg Oral/ IV Chlorphenamine 10mg Intravenous Slow
DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent & Rate 1 8 15 Sodium Chloride 0.9% 100ml Infusion Fast Running Dexamethasone 8mg Oral Ondansetron 8mg Oral/ IV Chlorphenamine 10mg Intravenous Slow
Policy for the safe handling and administration of cytotoxic drugs for Children, Teenagers and Young Adults with Cancer
 Policy for the safe handling and administration of cytotoxic drugs for Children, Teenagers and Young Adults with Cancer Introduction Cytotoxic drugs are used to treat cancer and a number of other disorders.
Policy for the safe handling and administration of cytotoxic drugs for Children, Teenagers and Young Adults with Cancer Introduction Cytotoxic drugs are used to treat cancer and a number of other disorders.
DBL NALOXONE HYDROCHLORIDE INJECTION USP
 Name of medicine Naloxone hydrochloride Data Sheet New Zealand DBL NALXNE HYDRCHLRIDE INJECTIN USP Presentation DBL Naloxone Hydrochloride Injection USP is a sterile, clear, colourless solution, free from
Name of medicine Naloxone hydrochloride Data Sheet New Zealand DBL NALXNE HYDRCHLRIDE INJECTIN USP Presentation DBL Naloxone Hydrochloride Injection USP is a sterile, clear, colourless solution, free from
Pharmacology Drug Dosage Calculations
 Pharmacology Drug Dosage Calculations Overview Abbreviations Metric Conversions Desired Dose Concentrations Drip Rates Medications (Dopamine and Lidocaine) Abbreviations cc- cubic centimeter DD- Desired
Pharmacology Drug Dosage Calculations Overview Abbreviations Metric Conversions Desired Dose Concentrations Drip Rates Medications (Dopamine and Lidocaine) Abbreviations cc- cubic centimeter DD- Desired
Math Practice for Paramedic Students
 Math Practice for Paramedic Students 1. You are responsible for providing the proper dose of etomidate to your partner so that he can initiate the RSI procedure for your patient. The patient weighs an
Math Practice for Paramedic Students 1. You are responsible for providing the proper dose of etomidate to your partner so that he can initiate the RSI procedure for your patient. The patient weighs an
Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet
 1 Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet 1 Name of Guideline / Policy/ Procedure MANAGEMENT OF ACUTE PAEDIATRIC ASTHMA Purpose of Procedure/
1 Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet 1 Name of Guideline / Policy/ Procedure MANAGEMENT OF ACUTE PAEDIATRIC ASTHMA Purpose of Procedure/
PACKAGE LEAFLET: INFORMATION FOR THE USER. Dopamine 40 mg/ml Sterile Concentrate
 PACKAGE LEAFLET: INFORMATION FOR THE USER Dopamine 40 mg/ml Sterile Concentrate Read all of this leaflet carefully before you start using this medicine. Keep this leaflet. You may need to read it again.
PACKAGE LEAFLET: INFORMATION FOR THE USER Dopamine 40 mg/ml Sterile Concentrate Read all of this leaflet carefully before you start using this medicine. Keep this leaflet. You may need to read it again.
For the use of only Oncologist or a Cancer Hospital or a laboratory Doxorubicin Hydrochloride Liposome Injection 2 mg/ml KEMODOXA
 For the use of only Oncologist or a Cancer Hospital or a laboratory Doxorubicin Hydrochloride Liposome Injection 2 mg/ml KEMODOXA COMPOSITION Each ml contains: Doxorubicin Hydrochloride IP...2 mg Water
For the use of only Oncologist or a Cancer Hospital or a laboratory Doxorubicin Hydrochloride Liposome Injection 2 mg/ml KEMODOXA COMPOSITION Each ml contains: Doxorubicin Hydrochloride IP...2 mg Water
Multiple IV Infusions: Research and Recommendations National Coalition for Infusion Therapy Safety Mar 12, 2015
 Multiple IV Infusions: Research and Recommendations National Coalition for Infusion Therapy Safety Mar 12, 2015 Mark Fan Sonia Pinkney Andrea Cassano-Piché Overview Introduction Research findings and recommendations
Multiple IV Infusions: Research and Recommendations National Coalition for Infusion Therapy Safety Mar 12, 2015 Mark Fan Sonia Pinkney Andrea Cassano-Piché Overview Introduction Research findings and recommendations
Education for Self Administration of Intravenous Therapy HOME IV THERAPY PICC. Portacath
 HOME IV THERAPY PICC Portacath Who To contact Cardio-Respiratory Integrated Specialist Services (CRISS) Office hours 0800 1630 hours Ph: 364 0167 Weekends and after hours, phone Christchurch Hospital operator
HOME IV THERAPY PICC Portacath Who To contact Cardio-Respiratory Integrated Specialist Services (CRISS) Office hours 0800 1630 hours Ph: 364 0167 Weekends and after hours, phone Christchurch Hospital operator
1 INJECTIONS INTRODUCTION
 1 INJECTIONS INTRODUCTION Parenteral articles are preparations intended for injection through the skin or other external boundary tissue, rather than through the alimentary canal, so that the active substances
1 INJECTIONS INTRODUCTION Parenteral articles are preparations intended for injection through the skin or other external boundary tissue, rather than through the alimentary canal, so that the active substances
Supply should only occur if requesting signature is on approved list held by the issuing pharmacy
 Trust Approved Drugs List March 2016 The following is the list of drugs that are approved by the EEAST Medicines Management Group for use by EEAST clinical staff. Pharmacies are advised that this is the
Trust Approved Drugs List March 2016 The following is the list of drugs that are approved by the EEAST Medicines Management Group for use by EEAST clinical staff. Pharmacies are advised that this is the
Drug Max dose approved for IVP Dilution Rate Monitoring Parameters. Dilution not necessary (Available in prefilled syringe)
") Drug Max dose approved for IVP Dilution Rate Monitoring Parameters Acetazolamide 500 mg Reconstitute with at least 5ml sterile water (max concentration should not exceed 100mg/ml) 100-500 mg/min Hypotension
Drug Max dose approved for IVP Dilution Rate Monitoring Parameters Acetazolamide 500 mg Reconstitute with at least 5ml sterile water (max concentration should not exceed 100mg/ml) 100-500 mg/min Hypotension
Ratios and Proportions. Calculations for Pharmacy Technicians 9/21/2017. Presented by: Antonia Kraljevic PGY2 Pharmacy Practice Resident
 Calculations for Pharmacy Technicians Presented by: Antonia Kraljevic PGY2 Pharmacy Practice Resident The speaker has no actual or potential conflict of interest in relation to this presentation. Pharmacy
Calculations for Pharmacy Technicians Presented by: Antonia Kraljevic PGY2 Pharmacy Practice Resident The speaker has no actual or potential conflict of interest in relation to this presentation. Pharmacy
September 2014 V0.17. Paediatric Daily Fluid Prescription & Balance Chart
 September 14 V0.17 Aims and outcomes of session. Aim: To provide guidance on correctly completing the paediatric daily fluid prescription & balance chart. Outcomes: Demonstrate the ability to: calculate
September 14 V0.17 Aims and outcomes of session. Aim: To provide guidance on correctly completing the paediatric daily fluid prescription & balance chart. Outcomes: Demonstrate the ability to: calculate
CENTRAL VENOUS ACCESS DEVICES. BETHANY COLTON
 CENTRAL VENOUS ACCESS DEVICES. BETHANY COLTON Aims and Objectives To know what central venous access devices (CVAD) are. Types of CVADS used in haematology. To understand why we use them To know the complications
CENTRAL VENOUS ACCESS DEVICES. BETHANY COLTON Aims and Objectives To know what central venous access devices (CVAD) are. Types of CVADS used in haematology. To understand why we use them To know the complications
High Risk Medications
 Department Policy Code: D: MM-5705 Entity: Fairview Health Services Department: Home Infusion Manual: Policies & Procedures Category: Medication Management Subject: High Risk Medications Purpose: To provide
Department Policy Code: D: MM-5705 Entity: Fairview Health Services Department: Home Infusion Manual: Policies & Procedures Category: Medication Management Subject: High Risk Medications Purpose: To provide
SCIG INFUSIONS A PRACTICAL GUIDE FOR PATIENTS
 PRIMARY IMMUNODEFICIENCIES SCIG INFUSIONS: A PRACTICAL GUIDE FOR PATIENTS SCIG INFUSIONS A PRACTICAL GUIDE FOR PATIENTS 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS IG IVIG PID SCIG Immunoglobulin Intravenous
PRIMARY IMMUNODEFICIENCIES SCIG INFUSIONS: A PRACTICAL GUIDE FOR PATIENTS SCIG INFUSIONS A PRACTICAL GUIDE FOR PATIENTS 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS IG IVIG PID SCIG Immunoglobulin Intravenous
Step-by-step instructions for intravenous (iv) infusions for patients with:
 infusions for patients with:") Step-by-step instructions for intravenous (iv) infusions for patients with: Rheumatoid Arthritis (RA) Systemic Juvenile Idiopathic Arthritis (sjia) Polyarticular Juvenile Idiopathic Arthritis (pjia) Please
Step-by-step instructions for intravenous (iv) infusions for patients with: Rheumatoid Arthritis (RA) Systemic Juvenile Idiopathic Arthritis (sjia) Polyarticular Juvenile Idiopathic Arthritis (pjia) Please
LIQUID PREPARATIONS FOR ORAL USE. Final text for addition to The International Pharmacopoeia (November 2007)
") November 2007 LIQUID PREPARATIONS FOR ORAL USE Final text for addition to The International Pharmacopoeia (November 2007) This monograph was adopted at the Forty-second WHO Expert Committee on Specifications
November 2007 LIQUID PREPARATIONS FOR ORAL USE Final text for addition to The International Pharmacopoeia (November 2007) This monograph was adopted at the Forty-second WHO Expert Committee on Specifications
Direct Intravenous (IV) Medication Administration Procedure
 Medication Administration Procedure") Approved by: Chief Medical Officer; and Chief Operating Officer Direct Intravenous (IV) Medication Administration Procedure Corporate Policy & Procedures Manual Number: VII-B-310 Date Approved January
Approved by: Chief Medical Officer; and Chief Operating Officer Direct Intravenous (IV) Medication Administration Procedure Corporate Policy & Procedures Manual Number: VII-B-310 Date Approved January
YONDELIS (trabectedin) DOSING & ADMINISTRATION GUIDE
 DOSING & ADMINISTRATION GUIDE") YONDELIS (trabectedin) DOSING & ADMINISTRATION GUIDE INDICATION YONDELIS (trabectedin) is indicated for the treatment of patients with unresectable or metastatic liposarcoma or leiomyosarcoma who received
YONDELIS (trabectedin) DOSING & ADMINISTRATION GUIDE INDICATION YONDELIS (trabectedin) is indicated for the treatment of patients with unresectable or metastatic liposarcoma or leiomyosarcoma who received
SPAGG. Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation
 SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as