Orthopaedic Manual Physical Therapy Series Orthopaedic Manual Physical Therapy Series
|
|
|
- Peregrine Wheeler
- 5 years ago
- Views:
Transcription




1 THE KNEE Michael McMurray PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville Reproduction Without Consent 1





2 Anterior Cruciate Ligament ACL reconstructions in % non contact Account for more than $500 million in healthcare costs per year Females x Originates at posteromedial corner of the medial side of the lateral femoral condyle, attaches in a fossa anterolateral to the tibial spine Function: Limits anterior tibial translation (85% at 30/90 degrees) Secondary limitation of tibial IR, varus/valgus Ultimate strength of a native ACL is ~2000N Anatomy Anteromedial bundle Tight throughout flexion Anterior instability Smaller Posterolateral bundle Tight in extension Greatest restraint to anterior translation from ext to 20deg flexion Rotary instability Larger Both Secondary restraint to varus/valgus/tibial IR Primary restraint to valgus force when MCL unable Reproduction Without Consent 2

; coupled with tibial rotation CKC IR/Valgus without HS co")


3 Innervation: Posterior articular branches of the tibial nerve Vascularization Branches of the middle genicular artery Infrapatellar Fat pad Synovium ACL Injury Mechanism: Acceleration/deceleration at full extension or slight flexion (Excess Quad, Decr HS activation); coupled with tibial rotation CKC IR/Valgus without HS co contraction Medial tibial rotation ACL winds around PCL Lateral tibial rotation ACL stretches over lateral condyle Rehab Before ACL Reconstruction? 6 week prehabilitation program prior to ACLR resulted in significantly increased KOOS scores and increased hop tests which remained 12 weeks after surgery compared to a control group Reproduction Without Consent 3

4 Reproduction Without Consent 4


5 Reproduction Without Consent 5





6 The healing process It s a dead piece of tissue! Graft needs to be re-vascularized Ligamentization occurs Vascular synovial layer wraps around graft in 4-6 weeks Autologous ACL grafts don t transition through necrotic stage Weakest link fixation 4-6 weeks Soft tissue graft to bone: 12 weeks Bone autograft to bone: 8 weeks Complete re-vascularization of the graft takes ~20 weeks Remodeling occurs: By one year histological and biochemical properties of ACLR native ACL Healing Rate of Tissues Times affected by age, comorbities, etc Reproduction Without Consent 6


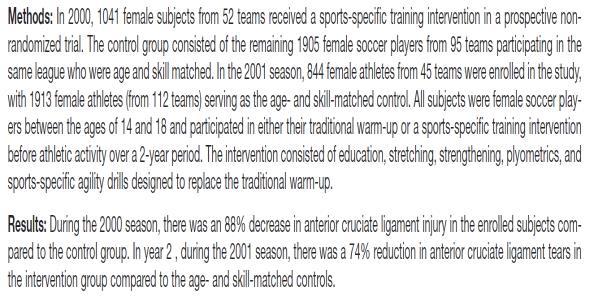
7 Prevention Reproduction Without Consent 7





8 Investigated 14 years after ACL Repair Control was contralateral healthy knee Risk factors investigated for OA: Weight Other injuries Sex Age Time between injury and repair Graft type Graft type and time between injury and repair were not factors Meniscal resection was a significant risk factor 3 fold increase in OA in surgical knee vs control Mostly medial compartment Reproduction Without Consent 8

9 REHABILITATION Orthopaedic Manual Physical Therapy Series Charlottesville Reproduction Without Consent 9
10 Reproduction Without Consent 10

 Bicycling Peak strain 1.2%-2.1% Lachman produced 3-3.")
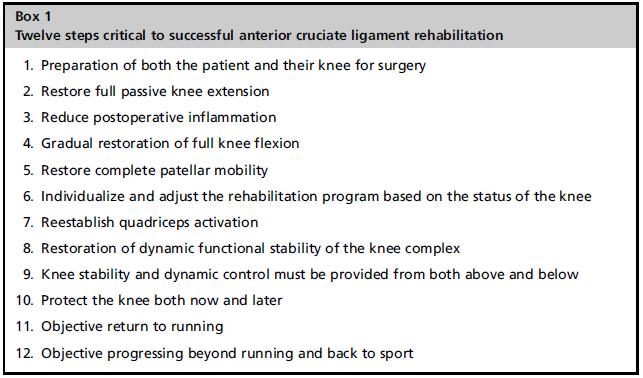
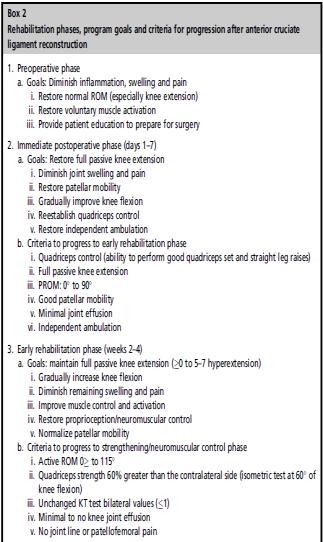
11 Seated Knee Extension Peak strain 3.2%-4.4% occurring at 10-30deg of knee flexion Increases ~1% with 10lb weight Increases 2x if weight placed at ankle vs prox tibia Seated Knee Flexion No strain Single or Double Knee Squats Minimal or no strain No change with weight If squat on toes is over 3x more loading through ACL With trunk flexion of 30-40deg decreased load on ACL vs upright posture Forward/Side Lunges ACL loading is minimal Leg Press Minimal to no loading No change with increased weight or different foot positions (high or low/wide or narrow) Bicycling Peak strain 1.2%-2.1% Lachman produced 3-3.5% strain Plyometric 250N force with double leg jump from 60cm platform Similar to load from seated knee extension For both NWB and WB greater loading occurs at lower knee flexion angles (10-30deg) Decreases from 30-60deg of knee flexion None at above 60deg of knee flexion NWB exercises produce significantly more load on ACL than WB in same range of motion Use a forward trunk lean of 30-40deg with all WB therex Increases HS recruitment to unload ACL Anterior knee translation beyond toes (>8cm) increases ACL load Goals: Full knee extension immediately Hyperextension returned equal By Graft Type: to other side by week 2 Less aggressive with soft tissue grafts Restore Patellar Mobility Return to running,plyo and Reduce post op inflammation sports is slower Range of Motion Slower to aggressive activities for allograft vs 0-90deg 5-7days post op autograft 0-100deg 7-10 days post op Increased healing time due Reestablish voluntary quad control to longer for fixation of soft NMES tissue as it heals in bone Restore Neuromuscular control tunnel Proprioceptive training by week 2 Reproduction Without Consent 11



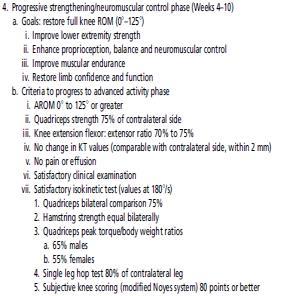
12 With this protocol 75% of patients had knee function w/i normal ranges at 6mo 87% by 1 year 40% of preoperative non copers passed return to sport by 6mo 73% by 12mo 90% or above on self report outcome questionnaires 70% at 3mo 92.5% at 6mo Quad strength ~90% by 6mo post op Typically 80% at 6 mo Running Progression Starts at 8 weeks if Quad strength 80% of uninvolved side Trace effusion Understanding of soreness rules Full AROM Normal gait More specific goals for each phase of rehab and specific return to sport guidelines Addition of guidelines for concomitant injuries Ligamentous, meniscal or chondral Reproduction Without Consent 12


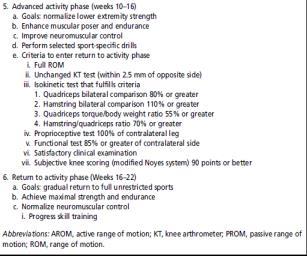
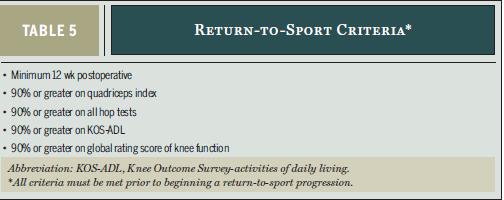
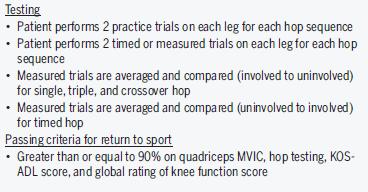
13 RETURN TO SPORT JOSPT Patient Perspective December 2014 Orthopaedic Manual Physical Therapy Series Charlottesville Recommendations: Less than 10% deficit in strength of QS vs HS on isokinetic at 180 and 300deg/sec Less than 15% deficit in symmetry on single leg hop testing Single hop, triple hop, crossover hop, timed hop Less than 3mm increased A-P tibial displacement on Lachman or arthrometer testing Greater than 60% knee separation distance on video dropjump test No effusion Normal ROM/patellar mobility No or slight patellar crepitus No pain or swelling with all activities Reproduction Without Consent 13


14 Less Reproduction Without Consent 14




15 POSTERIOR CRUCIATE LIGAMENT Orthopaedic Manual Physical Therapy Series Charlottesville Reproduction Without Consent 15
 Tight")
 In full extension bears ~93%of posterior directed")
 Ext Rot tibia (secondary) 90% multi lig injury MVA Dashboard injury")

16 Anatomy Anterior View Posterior View Lateral aspect of medial femoral condyle to posterior tibial spine Anterolateral bundle and Posteromedial bundle Anterolateral Larger (95%) Tight in flexion Posteromedial Smaller (5%) Tight in extension Injury Mechanism Function: Limits. Posterior Tibial translation (primary 90%) In full extension bears ~93%of posterior directed force Most important at 70-90deg of flexion due to laxity of secondary restraints (MCL, popliteus, capsule) Ext Rot tibia (secondary) 90% multi lig injury MVA Dashboard injury Contact sports Fall on a bent knee with their foot plantar flexed. The tibia hits the ground first and it translates posteriorly. Hyper flexion in external rotation Reproduction Without Consent 16



17 Treatment Non Operative Indicated for: Grade I-II isolated tears Non displaced grade II avulsion from tibia Brace immobilization x2-4weeks Focus on ROM, quad activation and limiting HS overactivity initially progressing to closed chain strengthening/proprioception/quad strength Slow progression compared to ACL Treatment Operative Indicated for: All grade III injuries; either isolated or with combined instability Bony avulsion that requires ORIF Some isolated grade II lesions in high demand athletes Reproduction Without Consent 17





18 MEDIAL COLLATERAL LIGAMENT Orthopaedic Manual Physical Therapy Series Charlottesville Anatomy Medial aspect femur (proximal-posterior to medial femoral epicondyle) courses distal and attaches anterior to posteriomedial tibial crest, distal to medial tibial plateau 3 tissue layers Superficial Deep Posterior Oblique Multiple connections to joint capsule, med meniscus, muscle-tendon units Anatomy Deep Anatomy Posterior Oblique Superficial Reproduction Without Consent 18






19 MCL Function 57% Valgus stability at 5 degrees knee flexion 78% Valgus stability at 25 degrees knee flexion Due to decreased contribution from posterior capsule MCL Valgus blow CKC - plant/cut valgus stress 7.9% of all athletic injuries Most common NFL/alpine skiing Second in collegiate hockey, women's rugby Grade III injury ~80% concomitant lig injury 95% of the time ACL MCL Treatment guidelines Grade I/II Non operative Rest/ice Hinged brace Early ROM Strength/Proprioception Early weightbearing Avg. return to football 20 days (grade II) 74% return to pre injury activity level at 3mo Grade III Rx controversial Most treated non operatively Indications for surgery» Avulsion fx with bony fragment» Laxity affecting sports performance/daily activities» Consistently positive stress radiographs for MCL ACL + MCL (standard of care reconstruct ACL, not MCL) MCL Bracing Reproduction Without Consent 19

 Orthopaedic Manual")
20 LATERAL COLLATERAL LIGAMENT Orthopaedic Manual Physical Therapy Series Charlottesville Anatomy Attaches equidistant from posterior and distal border of lateral femoral condyle and distally to superior and lateral facing V-shaped plateau on the fibular head Function Resists varus 0 and 30 degrees 55% of varus load at 5deg Posterior lateral capsule 13%,ITB 5%, cruciate ligs the remaining amount 69% of varus load at 25deg Posterior structures on slack in flexionpreferred test Secondary: limit ER of a flexed knee Injury Mechanism: Least commonly injured knee ligament Incidence of 4% Usually with a soft tissue avulsion off prox femur or bony avulsion off fibular head Typically with more extensive PLC injury LCL POSTEROLATERAL CORNER (PLC) Orthopaedic Manual Physical Therapy Series Charlottesville Reproduction Without Consent 20


 Hyperextension PLC Treatment Injury Mechanism: Blow to anteromedial")

21 Anatomy Muscles: Popliteus Lateral Head of Gastrocnemius Short head of Biceps Femoris Ligaments: Fibular Collateral Lig Arcuate Ligament Misc: Lateral Meniscus Lateral Retinaculum One of the most common multi-ligament injuries Isolated injuries to PLC 1.6% of all ligament injuries Concomitant PLC and other ligament injury: 43-80% Vehicular Trauma: 64% Athletic Injury: 46% Commonly missed with failed ACL Prevents: Primary: Varus Tibial ER Secondary Assists PCL with posterior tibial translation (30 degrees) Hyperextension PLC Treatment Injury Mechanism: Blow to anteromedial aspect tibia near or at full extension Forced hyperextension/varus Valgus force on flexed knee Severe tibial ER in flex or extension Grade I and II Good results non-operatively Grade III Good results operatively if performed within 3weeks of injury Better success operatively of acute vs chronic injuries Reproduction Without Consent 21

22 Non Operative Treatment Phase I Edema management QS activation ROM return Phase II Gait mechanics Increase strength QS, HS, GS, Popliteus, Hip, Lumbopelvic Phase III Neuromuscular control Control of varus and tibial ER at increased angles of knee flexion Phase IV Sport specific training Post Operative Treatment NWB x6weeks Immobilizer locked out for 1-2 weeks ROM 0-90 in 2 weeks Full in 6weeks Full body squats permitted at 12weeks Until 4 months, no. CKC therex at greater than 70deg knee flexion Tibial ER Resisted or repetitive HS in knee flexion MENISCUS Orthopaedic Manual Physical Therapy Series Charlottesville Reproduction Without Consent 22



23 Meniscus Second most common knee injury Incidence of 12-14% 10-20% of all orthopaedic surgeries in US involve meniscus patients a year Reproduction Without Consent 23
 Medial C shaped Less mobile Connected to")


24 Anatomy Anatomy Lateral Circular More mobile than medial Connected to: medial meniscus anteriorly by transverse lig patella by patellomeniscal lig posteriorly to popliteus mm and PCL medial femoral condyle by meniscofemoral lig (Ligament of Wrisberg) Medial C shaped Less mobile Connected to transverse and meniscofemoral ligs like lateral semimembranosus mm anterior horn attached to ACL posterior horn to PCL Anatomy Cover 2/3 of tibial plateau Red Zone: lateral 1/3 Good blood supply from capsular arteries White Zone: remaining 2/3 Poor blood supply Function Load transmission Manage 70% of load across knee during activities Shock absorption Stability Congruence Proprioceptive Transmit joint compressive forces 50% EXT 90 degrees During flexion move posteriorly, extension move anteriorly During rotation, follow motion of femur Most likely due to meniscofemoral ligs Reproduction Without Consent 24
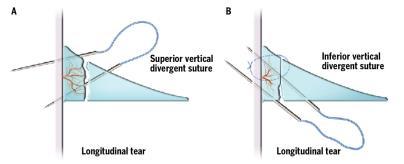
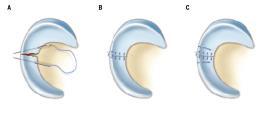
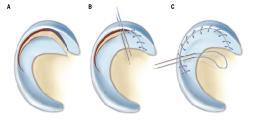
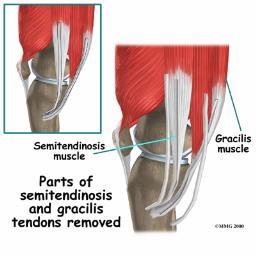
25 Semimembranosus and Popliteus pull on medial and lateral meniscus during flexion of the knee Meniscal Repair Radial Tear Repair Flap Tear Repair Reproduction Without Consent 25




26 Meniscal Transplantation Rehab Dependent on type and location of repair/transplant Physician directed Generally Long leg brace x6 weeks Restricted weight bearing atleast 3 weeks Flexion ROM restricted to 90 week 1, 120 week 4, 135 week 6 Biking week 7, straight running month 4, cutting month 5, return to sport month 5 Reproduction Without Consent 26





27 ARTICULAR CARTILAGE Orthopaedic Manual Physical Therapy Series Charlottesville Articular Cartilage Incidence 60-70% Isolated 30% Non isolated 70% Most commonly at medial femoral condyle and patella articular surface Medial meniscus tears and ACL rupture most common concomitant injuries 37% and 36% Anatomy Reproduction Without Consent 27


28 Treatment Options Through Subchondral Plate Conservative/Palliative Debridement/Lavage Reparative Subchondral Drilling Microfracture Restorative OATS ACI/MACI Treatment Options Debridement/Lavage Marrow Stimulating Autologous Chondrocyte Implantation Osteochondral Grafting Reproduction Without Consent 28

 with 1-2 mm between to allow soft tissue in growth to")

29 Micro fracture Marrow stimulation technique Most common Simple, safe, cheap Injury/inflammatory response Fibrous Clot formed < 2-4 cm lesion Successful Outcome 1. Remove calcified cartilage layer Do not abrade subchondral bone OATS/Mosaicplasty 2. Penetrate Subchondral bone (awl) with 1-2 mm between to allow soft tissue in growth to adhere 3. Maintain post op ROM (CPM) 4. Post op partial weight bearing (50% x 6 weeks) 5. Realignment/stabilizing procedure concurrently DJD, Patellar tracking, ligt repair/reconstruction Reproduction Without Consent 29





30 Autologous Chondrocyte Implantation (ACI) 2 surgical stages: Chondral biopsy Implantation of cells into lesion Full thickness lesions Femoral condyle, trochlear groove Unipolar lesions <50 yrs old Larger lesions 2-8 cm Normal alignment/stability Hyaline cartilage = Better Outcomes? Matrix Induced ACI ACI surgery but without periosteum harvest 2 stage surgery Harvest of cells Implantation of membrane Use fibrin glue to adhere membrane Reproduction Without Consent 30

 Lack of conclusive research on best approach Reproduction Without")
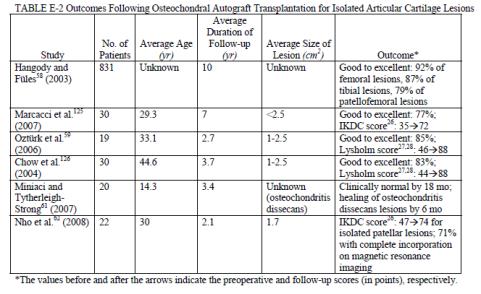
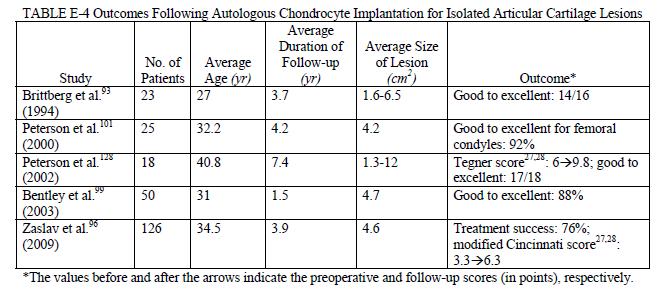
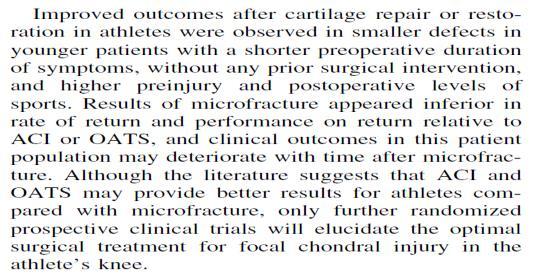
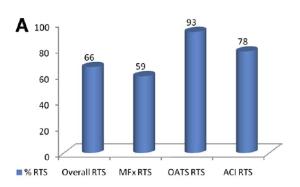
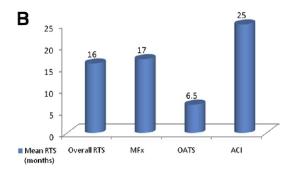
31 Graft Healing Course Following MACI Summary Improved outcomes for <30yo Improved outcomes for more active individuals For lesions >4cm, better outcomes with ACI or MACI All surgical interventions showed improved outcome measures short and long term Return to sport fastest with OATS (7mo), longest with ACI (18-25mo) Lack of conclusive research on best approach Reproduction Without Consent 31
32 Reproduction Without Consent 32


33 Phases of Healing and Rehab Rehabilitation Biologic Phase Phase I Graft integration and stimulation Phase II Matrix production and organization Phase III Repair cartilage maturation and adaptation Rehab Phase Phase I Protection and joint activation Phase II Progressive loading and functional joint restoration Phase III Activity restoration Phase I Protection and Joint Activation Weeks 1-6 Effusion control Partial weightbearing NMES/Quad activation therex Gradual improving ROM Reproduction Without Consent 33


 Excellent resource for rehabilitation protocol and progression")
34 Rehabilitation Phase II Progressive loading and functional joint restoration Week 6-6month Full ROM/weightbearing Progress proprioceptive training Progress concentric to eccentric and static to dynamic strengthening and neuromuscular control Introduce progressive plyometrics /loading activities Rehabilitation Phase III Activity restoration Sport specific/on field rehab 6-18 months (depending procedure, graft size, healing via imaging) Excellent resource for rehabilitation protocol and progression Reproduction Without Consent 34
ACL Athletic Career. ACL Rupture - Warning Features Intensive pain Immediate swelling Locking Feel a Pop Dead leg Cannot continue to play
 FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
ACL AND PCL INJURIES OF THE KNEE JOINT
 ACL AND PCL INJURIES OF THE KNEE JOINT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery,
ACL AND PCL INJURIES OF THE KNEE JOINT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery,
Financial Disclosure. Medial Collateral Ligament
 Matthew Murray, M.D. UTHSCSA Sports Medicine Financial Disclosure Dr. Matthew Murray has no relevant financial relationships with commercial interests to disclose. Medial Collateral Ligament Most commonly
Matthew Murray, M.D. UTHSCSA Sports Medicine Financial Disclosure Dr. Matthew Murray has no relevant financial relationships with commercial interests to disclose. Medial Collateral Ligament Most commonly
Anterior Cruciate Ligament Surgery
 Anatomy Anterior Cruciate Ligament Surgery Roger Ostrander, MD Andrews Institute Anatomy Anatomy Function Primary restraint to anterior tibial translation Secondary restraint to internal tibial rotation
Anatomy Anterior Cruciate Ligament Surgery Roger Ostrander, MD Andrews Institute Anatomy Anatomy Function Primary restraint to anterior tibial translation Secondary restraint to internal tibial rotation
The Knee. Prof. Oluwadiya Kehinde
 The Knee Prof. Oluwadiya Kehinde www.oluwadiya.sitesled.com The Knee: Introduction 3 bones: femur, tibia and patella 2 separate joints: tibiofemoral and patellofemoral. Function: i. Primarily a hinge joint,
The Knee Prof. Oluwadiya Kehinde www.oluwadiya.sitesled.com The Knee: Introduction 3 bones: femur, tibia and patella 2 separate joints: tibiofemoral and patellofemoral. Function: i. Primarily a hinge joint,
The Knee. Tibio-Femoral
 The Knee Tibio-Femoral Osteology Distal Femur with Proximal Tibia Largest Joint Cavity in the Body A modified hinge joint with significant passive rotation Technically, one degree of freedom (Flexion/Extension)
The Knee Tibio-Femoral Osteology Distal Femur with Proximal Tibia Largest Joint Cavity in the Body A modified hinge joint with significant passive rotation Technically, one degree of freedom (Flexion/Extension)
Knee Multiligament Rehabilitation
 Knee Multiligament Rehabilitation Orlando Valle, PT, MSPT, SCS, CSCS Director Ironman Sports Medicine Institute TMC Orlando.Valle@memorialhermann.org 4 Major Ligaments ACL PCL MCL LCL (PLC) Anatomy Function
Knee Multiligament Rehabilitation Orlando Valle, PT, MSPT, SCS, CSCS Director Ironman Sports Medicine Institute TMC Orlando.Valle@memorialhermann.org 4 Major Ligaments ACL PCL MCL LCL (PLC) Anatomy Function
The Knee. Two Joints: Tibiofemoral. Patellofemoral
 Evaluating the Knee The Knee Two Joints: Tibiofemoral Patellofemoral HISTORY Remember the questions from lecture #2? Girth OBSERVATION TibioFemoral Alignment What are the consequences of faulty alignment?
Evaluating the Knee The Knee Two Joints: Tibiofemoral Patellofemoral HISTORY Remember the questions from lecture #2? Girth OBSERVATION TibioFemoral Alignment What are the consequences of faulty alignment?
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction
 Reconstruction") Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
Prevention and Treatment of Injuries. Anatomy. Anatomy. Chapter 20 The Knee Westfield High School Houston, Texas
 Prevention and Treatment of Injuries Chapter 20 The Knee Westfield High School Houston, Texas Anatomy MCL, Medial Collateral Ligament LCL, Lateral Collateral Ligament PCL, Posterior Cruciate Ligament ACL,
Prevention and Treatment of Injuries Chapter 20 The Knee Westfield High School Houston, Texas Anatomy MCL, Medial Collateral Ligament LCL, Lateral Collateral Ligament PCL, Posterior Cruciate Ligament ACL,
ACL Rehabilitation and Return To Play
 ACL Rehabilitation and Return To Play Seth Gasser, MD Director of Sports Medicine Florida Orthopaedic Institute Introduction Return to Play: the point in recovery from an injury when a person is safely
ACL Rehabilitation and Return To Play Seth Gasser, MD Director of Sports Medicine Florida Orthopaedic Institute Introduction Return to Play: the point in recovery from an injury when a person is safely
Anatomy and Sports Injuries of the Knee
 Anatomy and Sports Injuries of the Knee I. Anatomy II. Assessment III. Treatment IV. Case Study V. Dissection Anatomy Not a hinge joint 6 degrees of freedom Flexion/Extension Rotation Translation Anatomy
Anatomy and Sports Injuries of the Knee I. Anatomy II. Assessment III. Treatment IV. Case Study V. Dissection Anatomy Not a hinge joint 6 degrees of freedom Flexion/Extension Rotation Translation Anatomy
W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco
 Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
Reconstruction of the Ligaments of the Knee
 Reconstruction of the Ligaments of the Knee Contents ACL reconstruction Evaluation Selection Evolution Graft issues Notchplasty Tunnel issues MCL PCL Posterolateral ligament complex Combined injuries Evaluation
Reconstruction of the Ligaments of the Knee Contents ACL reconstruction Evaluation Selection Evolution Graft issues Notchplasty Tunnel issues MCL PCL Posterolateral ligament complex Combined injuries Evaluation
Posterolateral Corner Injuries of the Knee: Pearls and Pitfalls
 Posterolateral Corner Injuries of the Knee: Pearls and Pitfalls Robert A. Arciero,MD,Col,ret Professor, Orthopaedics University of Connecticut Incidence of PLC Injuries with ACL Tears Fanelli, 1995 12%
Posterolateral Corner Injuries of the Knee: Pearls and Pitfalls Robert A. Arciero,MD,Col,ret Professor, Orthopaedics University of Connecticut Incidence of PLC Injuries with ACL Tears Fanelli, 1995 12%
Overview Ligament Injuries. Anatomy. Epidemiology Very commonly injured joint. ACL Injury 20/06/2016. Meniscus Tears. Patellofemoral Problems
 Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Knee Injury Assessment
 Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Rehabilitation Protocol:
 Rehabilitation Protocol: Patellofemoral resurfacing: Osteochondral Autograft Transplantation (OATS), Autologous Chondrocyte Implantation (ACI) and Microfracture Department of Orthopaedic Surgery Lahey
Rehabilitation Protocol: Patellofemoral resurfacing: Osteochondral Autograft Transplantation (OATS), Autologous Chondrocyte Implantation (ACI) and Microfracture Department of Orthopaedic Surgery Lahey
Joints of the Lower Limb II
 Joints of the Lower Limb II Lecture Objectives Describe the components of the knee and ankle joint. List the ligaments associated with these joints and their attachments. List the muscles acting on these
Joints of the Lower Limb II Lecture Objectives Describe the components of the knee and ankle joint. List the ligaments associated with these joints and their attachments. List the muscles acting on these
Differential Diagnosis
 Case 31yo M who sustained an injury to L knee while playing Basketball approximately 2 weeks ago. He describes pivoting and hyperextending his knee, which swelled over the next few days. He now presents
Case 31yo M who sustained an injury to L knee while playing Basketball approximately 2 weeks ago. He describes pivoting and hyperextending his knee, which swelled over the next few days. He now presents
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 43 rd Annual Symposium on Sports Medicine UT Health Science Center San Antonio School of Medicine January 22-23, 2016 Intra-articular / Extra-synovial 38 mm length / 13 mm width Fan-shaped structure narrowest-midportion
43 rd Annual Symposium on Sports Medicine UT Health Science Center San Antonio School of Medicine January 22-23, 2016 Intra-articular / Extra-synovial 38 mm length / 13 mm width Fan-shaped structure narrowest-midportion
Appendix 2: KNGF Evidence Statement for anterior cruciate ligament reconstruction rehabilitation
 Appendix 2: KNGF Evidence Statement for anterior cruciate ligament reconstruction rehabilitation Inclusion and exclusion criteria for rehabilitation according to the Evidence Statement Inclusion of patients
Appendix 2: KNGF Evidence Statement for anterior cruciate ligament reconstruction rehabilitation Inclusion and exclusion criteria for rehabilitation according to the Evidence Statement Inclusion of patients
MCL Injuries: When and How to Repair Scott D. Mair, MD
 MCL Injuries: When and How to Repair Scott D. Mair, MD Professor and Team Physician: Orthopaedic Surgery University of Kentucky School of Medicine Disclosure Institution: Research/Education Smith-Nephew
MCL Injuries: When and How to Repair Scott D. Mair, MD Professor and Team Physician: Orthopaedic Surgery University of Kentucky School of Medicine Disclosure Institution: Research/Education Smith-Nephew
Ligamentous and Meniscal Injuries: Diagnosis and Management
 Ligamentous and Meniscal Injuries: Diagnosis and Management Daniel K Williams, MD Franciscan Physician Network Orthopedic Specialists September 29, 2017 No Financial Disclosures INTRODUCTION Overview of
Ligamentous and Meniscal Injuries: Diagnosis and Management Daniel K Williams, MD Franciscan Physician Network Orthopedic Specialists September 29, 2017 No Financial Disclosures INTRODUCTION Overview of
On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective
 On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective Jessica Condliffe Physiotherapist / Clinic Manager TBI Health Wellington Presentation Outline Knee anatomy review
On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective Jessica Condliffe Physiotherapist / Clinic Manager TBI Health Wellington Presentation Outline Knee anatomy review
REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING A TWO TUNNEL GRAFT. Brace E-Z Wrap locked at zero degree extension, sleep in Brace
 Therapist Phone REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING A TWO TUNNEL GRAFT I. IMMEDIATE POST-OPERATIVE PHASE (Week 1) Control Swelling and Inflammation Obtain Full Passive Knee Extension
Therapist Phone REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING A TWO TUNNEL GRAFT I. IMMEDIATE POST-OPERATIVE PHASE (Week 1) Control Swelling and Inflammation Obtain Full Passive Knee Extension
ACL Reconstruction Protocol (Allograft)
") ACL Reconstruction Protocol (Allograft) Week one Week two Initial Evaluation Range of motion Joint hemarthrosis Ability to contract quad/vmo Gait (generally WBAT in brace) Patella Mobility Inspect for
ACL Reconstruction Protocol (Allograft) Week one Week two Initial Evaluation Range of motion Joint hemarthrosis Ability to contract quad/vmo Gait (generally WBAT in brace) Patella Mobility Inspect for
9180 KATY FREEWAY, STE. 200 (713)
") AUTOLOGOUS CHONDROCYTE IMPLANTATION Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protect healing tissue from load and shear forces - Decrease pain and effusion
AUTOLOGOUS CHONDROCYTE IMPLANTATION Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protect healing tissue from load and shear forces - Decrease pain and effusion
3/21/2011 PCL INJURY WITH OPERATIVE TREATMENT A CASE STUDY PCL PCL MECHANISM OF INJURY PCL PREVALENCE
 PCL PCL INJURY WITH OPERATIVE TREATMENT A CASE STUDY K. Anderson, S. Hjortedal, Y. Jingi, E. Sutcliffe & S. Witschen Washington State University Origin Posterior aspect of tibia Insertion Medial femoral
PCL PCL INJURY WITH OPERATIVE TREATMENT A CASE STUDY K. Anderson, S. Hjortedal, Y. Jingi, E. Sutcliffe & S. Witschen Washington State University Origin Posterior aspect of tibia Insertion Medial femoral
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribution.
 42 ND Annual Symposium on Sports Medicine UT Health Science Center San Antonio School of Medicine January 22-24, 2015 PCL injuries- only 5 to 10% of all knee ligament injuries. Incidence of PCL injury
42 ND Annual Symposium on Sports Medicine UT Health Science Center San Antonio School of Medicine January 22-24, 2015 PCL injuries- only 5 to 10% of all knee ligament injuries. Incidence of PCL injury
Knee Injuries. PSK 4U Mr. S. Kelly North Grenville DHS. Medial Collateral Ligament Sprain
 Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION
 OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION FEMORAL CONDYLE REHABILITATION PROGRAM PHASE I - PROTECTION PHASE (WEEKS 0-6) Protection of healing tissue from load and shear forces Decrease pain and effusion
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION FEMORAL CONDYLE REHABILITATION PROGRAM PHASE I - PROTECTION PHASE (WEEKS 0-6) Protection of healing tissue from load and shear forces Decrease pain and effusion
King Khalid University Hospital
 King Khalid University Hospital Rehabilitation Department Ortho Group Rehabilitation Protocol: PCL RECONSTRUCTION +/- ACL / MCL / LCL / POSTEROLATERAL CORNER 1. General Guidelines: Time lines in this rehabilitation
King Khalid University Hospital Rehabilitation Department Ortho Group Rehabilitation Protocol: PCL RECONSTRUCTION +/- ACL / MCL / LCL / POSTEROLATERAL CORNER 1. General Guidelines: Time lines in this rehabilitation
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING Allograft
 Sports Medicine and Rehabilitation Center Therapist Phone REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING Allograft I. IMMEDIATE POST-OPERATIVE PHASE (Week 1) Control Swelling and Inflammation
Sports Medicine and Rehabilitation Center Therapist Phone REHABILITATION PROTOCOL FOLLOWING PCL RECONSTRUCTION USING Allograft I. IMMEDIATE POST-OPERATIVE PHASE (Week 1) Control Swelling and Inflammation
Rehabilitation Protocol: Distal Femoral/Proximal Tibial Microfracture and Osteochondral Autograft Transplantation (OATS)
") Rehabilitation Protocol: Distal Femoral/Proximal Tibial Microfracture and Osteochondral Autograft Transplantation (OATS) Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650
Rehabilitation Protocol: Distal Femoral/Proximal Tibial Microfracture and Osteochondral Autograft Transplantation (OATS) Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
UNUSUAL ACL CASE: Tibial Eminence Fracture in a Female Collegiate Basketball Player
 UNUSUAL ACL CASE: Tibial Eminence Fracture in a Female Collegiate Basketball Player Cheri Drysdale, MEd,, ATC Margot Putukian,, MD Jeffery Bechler,, MD Princeton University How many of you have done an
UNUSUAL ACL CASE: Tibial Eminence Fracture in a Female Collegiate Basketball Player Cheri Drysdale, MEd,, ATC Margot Putukian,, MD Jeffery Bechler,, MD Princeton University How many of you have done an
SOFT TISSUE INJURIES OF THE KNEE: Primary Care and Orthopaedic Management
 SOFT TISSUE INJURIES OF THE KNEE: Primary Care and Orthopaedic Management Gauguin Gamboa Australia has always been a nation where emphasis on health and fitness has resulted in an active population engaged
SOFT TISSUE INJURIES OF THE KNEE: Primary Care and Orthopaedic Management Gauguin Gamboa Australia has always been a nation where emphasis on health and fitness has resulted in an active population engaged
King Khalid University Hospital
 King Khalid University Hospital Rehabilitation Department Ortho Group Rehabilitation Protocol: ACL RECONSTRUCTION +/- MENSICAL REPAIR 1. General Guidelines: Time lines in this rehabilitation protocol are
King Khalid University Hospital Rehabilitation Department Ortho Group Rehabilitation Protocol: ACL RECONSTRUCTION +/- MENSICAL REPAIR 1. General Guidelines: Time lines in this rehabilitation protocol are
The Meniscus. History. Anatomy. Anatomy. Blood Supply. Attachments
 History The Meniscus W. Randall Schultz, MD, MS Austin, TX January 23, 2016 Meniscus originally thought to represent vestigial tissue 1883 first reported meniscal repair (Annandale) Total menisectomy treatment
History The Meniscus W. Randall Schultz, MD, MS Austin, TX January 23, 2016 Meniscus originally thought to represent vestigial tissue 1883 first reported meniscal repair (Annandale) Total menisectomy treatment
Jennifer L. Cook, MD
 Jennifer L. Cook, MD Florida Joint Replacement and Sports Medicine Center 5243 Hanff Lane New Port Richey, FL 34652 Phone: (727)848-4249 Fax: (727) 841-8934 ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION POST-OPERATIVE
Jennifer L. Cook, MD Florida Joint Replacement and Sports Medicine Center 5243 Hanff Lane New Port Richey, FL 34652 Phone: (727)848-4249 Fax: (727) 841-8934 ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION POST-OPERATIVE
9180 KATY FREEWAY, STE. 200 (713)
") OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION Patella/Trochlea Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protection of healing tissue from load and shear forces - Decrease pain
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION Patella/Trochlea Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protection of healing tissue from load and shear forces - Decrease pain
Patellofemoral Pathology
 Patellofemoral Pathology Matthew Murray, MD UT Health Science Center/UT Medicine Sports Medicine and Arthroscopic Surgery I have disclosed that I am a consultant for Biomet Orthopaedics. Anterior Knee
Patellofemoral Pathology Matthew Murray, MD UT Health Science Center/UT Medicine Sports Medicine and Arthroscopic Surgery I have disclosed that I am a consultant for Biomet Orthopaedics. Anterior Knee
Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair
 Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore
Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction & PCL Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore
These are rehabilitation guidelines for OSU Sports Medicine patients. Please contact us at if you have any questions.
 OSU Sports Medicine Knee Microfracture Rehabilitation Guidelines These are rehabilitation guidelines for OSU Sports Medicine patients. Please contact us at 614-293-2385 if you have any questions. Rehabilitation
OSU Sports Medicine Knee Microfracture Rehabilitation Guidelines These are rehabilitation guidelines for OSU Sports Medicine patients. Please contact us at 614-293-2385 if you have any questions. Rehabilitation
Management of Knee Dislocations
 Management of Knee Dislocations Thomas J. Gill, MD Chief, Sports Medicine Service Massachusetts General Hospital Associate Professor of Orthopedic Surgery Harvard Medical School Complex Challenging Multi-Ligament
Management of Knee Dislocations Thomas J. Gill, MD Chief, Sports Medicine Service Massachusetts General Hospital Associate Professor of Orthopedic Surgery Harvard Medical School Complex Challenging Multi-Ligament
Doron Sher. 160 Belmore Rd, Randwick Burwood Rd, Concord. MBBS, MBiomedE, FRACS FAOrthA
 Doron Sher MBBS, MBiomedE, FRACS FAOrthA 160 Belmore Rd, Randwick 47 49 Burwood Rd, Concord www.kneedoctor.com.au www.orthosports.com.au Medial PatelloFemoral (MPFL) And AnteroLateral Ligament (ALL) Reconstruction
Doron Sher MBBS, MBiomedE, FRACS FAOrthA 160 Belmore Rd, Randwick 47 49 Burwood Rd, Concord www.kneedoctor.com.au www.orthosports.com.au Medial PatelloFemoral (MPFL) And AnteroLateral Ligament (ALL) Reconstruction
Grant H Garcia, MD Sports and Shoulder Surgeon
 What to Expect from your Anterior Cruciate Ligament Reconstruction Surgery A Guide for Patients Grant H Garcia, MD Sports and Shoulder Surgeon Important Contact Information Grant Garcia, MD Wallingford:
What to Expect from your Anterior Cruciate Ligament Reconstruction Surgery A Guide for Patients Grant H Garcia, MD Sports and Shoulder Surgeon Important Contact Information Grant Garcia, MD Wallingford:
Imaging the Athlete s Knee. Peter Lowry, MD Musculoskeletal Radiology University of Colorado
 Imaging the Athlete s Knee Peter Lowry, MD Musculoskeletal Radiology University of Colorado None Disclosures Knee Imaging: Radiographs Can be performed weight-bearing or non-weight-bearing View options
Imaging the Athlete s Knee Peter Lowry, MD Musculoskeletal Radiology University of Colorado None Disclosures Knee Imaging: Radiographs Can be performed weight-bearing or non-weight-bearing View options
40 th Annual Symposium on Sports Medicine. Knee Injuries In The Pediatric Athlete. Disclosure
 40 th Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio Knee Injuries In The Pediatric Athlete Disclosure Dr. Travis Murray
40 th Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio Knee Injuries In The Pediatric Athlete Disclosure Dr. Travis Murray
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes
 Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
TREATMENT GUIDELINES FOR GRADE 3 PCL TEAR
 GENERAL CONSIDERATIONS Posterior cruciate ligament (PCL) injuries occur less frequently than anterior cruciate ligament (ACL) injuries, but are much more common than previously thought. The PCL is usually
GENERAL CONSIDERATIONS Posterior cruciate ligament (PCL) injuries occur less frequently than anterior cruciate ligament (ACL) injuries, but are much more common than previously thought. The PCL is usually
KNEE MICROFRACTURE CLINICAL PRACTICE GUIDELINE
 KNEE MICROFRACTURE CLINICAL PRACTICE GUIDELINE Progression is time and criterion-based, dependent on soft tissue healing, patient demographics and clinician evaluation. Contact Ohio State Sports Medicine
KNEE MICROFRACTURE CLINICAL PRACTICE GUIDELINE Progression is time and criterion-based, dependent on soft tissue healing, patient demographics and clinician evaluation. Contact Ohio State Sports Medicine
Disclosures. Outline. The Posterior Cruciate Ligament 5/3/2016
 The Posterior Cruciate Ligament Christopher J. Utz, MD Assistant Professor of Orthopaedic Surgery University of Cincinnati Disclosures I have no disclosures relevant to this topic. Outline 1. PCL Basic
The Posterior Cruciate Ligament Christopher J. Utz, MD Assistant Professor of Orthopaedic Surgery University of Cincinnati Disclosures I have no disclosures relevant to this topic. Outline 1. PCL Basic
Knee Movement Coordination Deficits. ICD-9-CM: Sprain of cruciate ligament of knee
 1 Knee Movement Coordination Deficits Anterior Cruciate Ligament ACL Tear ICD-9-CM: 844.2 Sprain of cruciate ligament of knee ACL Insufficiency ICD-9-CM: 717.83 Old disruption of anterior cruciate ligament
1 Knee Movement Coordination Deficits Anterior Cruciate Ligament ACL Tear ICD-9-CM: 844.2 Sprain of cruciate ligament of knee ACL Insufficiency ICD-9-CM: 717.83 Old disruption of anterior cruciate ligament
FUNCTIONAL ANATOMY: Knee and Leg
 ACSM Team Physician Course San Antonio Feb 2015 FUNCTIONAL ANATOMY: Knee and Leg Marlene DeMaio, MD Professor, Orthopaedic Surgery Marshall University VAMC Huntington, WV Mary Lloyd Ireland, MD Professor
ACSM Team Physician Course San Antonio Feb 2015 FUNCTIONAL ANATOMY: Knee and Leg Marlene DeMaio, MD Professor, Orthopaedic Surgery Marshall University VAMC Huntington, WV Mary Lloyd Ireland, MD Professor
The Knee Joint By Prof. Dr. Muhammad Imran Qureshi
 The Knee Joint By Prof. Dr. Muhammad Imran Qureshi Structurally, it is the Largest and the most complex joint in the body because of the functions that it performs: Allows mobility (flexion/extension)
The Knee Joint By Prof. Dr. Muhammad Imran Qureshi Structurally, it is the Largest and the most complex joint in the body because of the functions that it performs: Allows mobility (flexion/extension)
Lateral knee injuries
 Created as a free resource by Clinical Edge Based on Physio Edge podcast episode 051 with Matt Konopinski Get your free trial of online Physio education at Orthopaedic timeframes Traditionally Orthopaedic
Created as a free resource by Clinical Edge Based on Physio Edge podcast episode 051 with Matt Konopinski Get your free trial of online Physio education at Orthopaedic timeframes Traditionally Orthopaedic
STATE OF THE ART OF ACL SURGERY (Advancements that have had an impact)
") STATE OF THE ART OF ACL SURGERY (Advancements that have had an impact) David Drez, Jr., M.D. Clinical Professor of Orthopaedics LSU School of Medicine Financial Disclosure Dr. David Drez has no relevant
STATE OF THE ART OF ACL SURGERY (Advancements that have had an impact) David Drez, Jr., M.D. Clinical Professor of Orthopaedics LSU School of Medicine Financial Disclosure Dr. David Drez has no relevant
No Disclosures. Topics. Pediatric ACL Tears
 Knee Injuries in Skeletally Immature Athletes No Disclosures Zachary Stinson, M.D. 2 Topics ACL Tears and Tibial Eminence Fractures Meniscus Injuries Discoid Meniscus Osteochondritis Dessicans Patellar
Knee Injuries in Skeletally Immature Athletes No Disclosures Zachary Stinson, M.D. 2 Topics ACL Tears and Tibial Eminence Fractures Meniscus Injuries Discoid Meniscus Osteochondritis Dessicans Patellar
9/24/2012. Greg Bennett, PT, DSc Excel Physical Therapy Marymount University
 Greg Bennett, PT, DSc Excel Physical Therapy Marymount University Hx often diagnostic Least to most threatening Sx trump exam Develop consistent routine Don t inflame inflamed tissue 1 1. ESTABLISH OR
Greg Bennett, PT, DSc Excel Physical Therapy Marymount University Hx often diagnostic Least to most threatening Sx trump exam Develop consistent routine Don t inflame inflamed tissue 1 1. ESTABLISH OR
Imaging the Knee 17/10/2017. Friction syndrome Common in runners or cyclists Fluid between ITB and Lateral femoral condyle
 17/10/2017 Imaging the Knee Alicia M. Yochum RN, DC, DACBR, RMSK Iliotibial Band Syndrome Ligamentous Tears (ACL, PCL, MCL, LCL) Meniscal Tears Cartilage Degeneration Quadriceps/Patellar tendinosis Osteochondral
17/10/2017 Imaging the Knee Alicia M. Yochum RN, DC, DACBR, RMSK Iliotibial Band Syndrome Ligamentous Tears (ACL, PCL, MCL, LCL) Meniscal Tears Cartilage Degeneration Quadriceps/Patellar tendinosis Osteochondral
Knee Contusions and Stress Injuries. Laura W. Bancroft, M.D.
 Knee Contusions and Stress Injuries Laura W. Bancroft, M.D. Objectives Review 5 types of contusion patterns Pivot shift Dashboard Hyperextension Clip Lateral patellar dislocation Demonstrate various stress
Knee Contusions and Stress Injuries Laura W. Bancroft, M.D. Objectives Review 5 types of contusion patterns Pivot shift Dashboard Hyperextension Clip Lateral patellar dislocation Demonstrate various stress
Anterior Cruciate Ligament (ACL)
") Anterior Cruciate Ligament (ACL) The anterior cruciate ligament (ACL) is one of the 4 major ligament stabilizers of the knee. ACL tears are among the most common major knee injuries in active people of
Anterior Cruciate Ligament (ACL) The anterior cruciate ligament (ACL) is one of the 4 major ligament stabilizers of the knee. ACL tears are among the most common major knee injuries in active people of
Imaging of the Athle/c Knee: injuries associated with ACL disrup/on
 Imaging of the Athle/c Knee: injuries associated with ACL disrup/on Brian Petersen, MD Associate Professor of Radiology and Orthopaedics Chief of MSK Radiology University of Colorado CU Sports Medicine
Imaging of the Athle/c Knee: injuries associated with ACL disrup/on Brian Petersen, MD Associate Professor of Radiology and Orthopaedics Chief of MSK Radiology University of Colorado CU Sports Medicine
42 nd Annual Symposium on Sports Medicine. Knee Injuries In The Pediatric Athlete. Disclosure
 42 nd Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio January 23, 2015 Knee Injuries In The Pediatric Athlete Disclosure
42 nd Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio January 23, 2015 Knee Injuries In The Pediatric Athlete Disclosure
Brennen Lucas, M.D. Advanced Orthopaedic Associates
 Brennen Lucas, M.D. Advanced Orthopaedic Associates 2778 N. Webb Rd. Wichita, KS 67226 316-631-1600 Fax: (316) 631-1674 1 (800) 362-0591 GUIDELINES FOR REHABILITATION FOLLOWING SURGICAL RECONSTRUCTION
Brennen Lucas, M.D. Advanced Orthopaedic Associates 2778 N. Webb Rd. Wichita, KS 67226 316-631-1600 Fax: (316) 631-1674 1 (800) 362-0591 GUIDELINES FOR REHABILITATION FOLLOWING SURGICAL RECONSTRUCTION
Athletic Preparation ACL Reconstruction - Accelerated Rehabilitation. Autologous Bone-Tendon-Bone, Patella Tendon Graft
 Orthopaedic Sports Specialists, P.C. Michael E. Joyce, M.D. 84 Glastonbury Blvd., Suite 101, Glastonbury, Connecticut 06033 Voice: 860-652-8883, Fax: 860-652-8887 Athletic Preparation ACL Reconstruction
Orthopaedic Sports Specialists, P.C. Michael E. Joyce, M.D. 84 Glastonbury Blvd., Suite 101, Glastonbury, Connecticut 06033 Voice: 860-652-8883, Fax: 860-652-8887 Athletic Preparation ACL Reconstruction
Rehabilitation Following Acute ACL, PCL, LCL, PL & Lateral Hamstring Repair
 Page 1 of 7 Rehabilitation Following Acute ACL, PCL, LCL, PL & Lateral Hamstring Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore normal range of motion (gradual knee
Page 1 of 7 Rehabilitation Following Acute ACL, PCL, LCL, PL & Lateral Hamstring Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore normal range of motion (gradual knee
REHABILITATION FOLLOWING ACL PTG RECONSTRUCTION
 REHABILITATION FOLLOWING ACL PTG RECONSTRUCTION I. IMMEDIATE POST OPERATIVE PHASE POD 1 POD 2 to 3 Brace: EZ Wrap brace locked at zero degrees extension or Protonics Rehab System (PRS) as directed by physician
REHABILITATION FOLLOWING ACL PTG RECONSTRUCTION I. IMMEDIATE POST OPERATIVE PHASE POD 1 POD 2 to 3 Brace: EZ Wrap brace locked at zero degrees extension or Protonics Rehab System (PRS) as directed by physician
Medical Diagnosis for Michael s Knee
 Medical Diagnosis for Michael s Knee Introduction The following report mainly concerns the diagnosis and treatment of the patient, Michael. Given that Michael s clinical problem surrounds an injury about
Medical Diagnosis for Michael s Knee Introduction The following report mainly concerns the diagnosis and treatment of the patient, Michael. Given that Michael s clinical problem surrounds an injury about
ACL RECONSTRUCTION HAMSTRING METHOD. Presents ACL RECONSTRUCTION HAMSTRING METHOD. Multimedia Health Education
 HAMSTRING METHOD Presents HAMSTRING METHOD Multimedia Health Education Disclaimer Stephen J. Incavo MD This movie is an educational resource only and should not be used to make a decision on Anterior Cruciate
HAMSTRING METHOD Presents HAMSTRING METHOD Multimedia Health Education Disclaimer Stephen J. Incavo MD This movie is an educational resource only and should not be used to make a decision on Anterior Cruciate
POSTEROLATERAL CORNER RECONSTRUCTION WHEN AND HOW?
 OTHER KNEE SURGERIES POSTEROLATERAL CORNER RECONSTRUCTION WHEN AND HOW? Written by Jacques Ménétrey, Eric Dromzée and Philippe M. Tscholl, Switzerland Injury of the posterolateral corner (PLC) is relatively
OTHER KNEE SURGERIES POSTEROLATERAL CORNER RECONSTRUCTION WHEN AND HOW? Written by Jacques Ménétrey, Eric Dromzée and Philippe M. Tscholl, Switzerland Injury of the posterolateral corner (PLC) is relatively
Rehab Considerations: Meniscus
 Rehab Considerations: Meniscus Steve Cox, PT, DPT Department of Orthopaedics School of Medicine University of Texas Health Science Center at San Antonio 1 -Anatomy/ Function/ Injuries -Treatment Options
Rehab Considerations: Meniscus Steve Cox, PT, DPT Department of Orthopaedics School of Medicine University of Texas Health Science Center at San Antonio 1 -Anatomy/ Function/ Injuries -Treatment Options
Chapter 20 The knee and related structures
 Chapter 20 The knee and related structures Athletic Training Spring 2014 Jihong Park Bones & joints Femur, tibia, fibula, & patella Femur & tibia Weight bearing & muscle attachment Patella functions Anterior
Chapter 20 The knee and related structures Athletic Training Spring 2014 Jihong Park Bones & joints Femur, tibia, fibula, & patella Femur & tibia Weight bearing & muscle attachment Patella functions Anterior
ORTHOPEDIC SURGERY, SPORTS MEDICINE, AND ARTHROSCOPY
 WWW.MATTDRISCOLLMD.COM ORTHOPEDIC SURGERY, SPORTS MEDICINE, AND ARTHROSCOPY ACL Reconstruction Rehab Protocol The intent of this protocol is to provide a general framework for ACL rehabilitation. Within
WWW.MATTDRISCOLLMD.COM ORTHOPEDIC SURGERY, SPORTS MEDICINE, AND ARTHROSCOPY ACL Reconstruction Rehab Protocol The intent of this protocol is to provide a general framework for ACL rehabilitation. Within
Anterolateral Ligament. Bradd G. Burkhart, MD Orlando Orthopaedic Center Sports Medicine
 Anterolateral Ligament Bradd G. Burkhart, MD Orlando Orthopaedic Center Sports Medicine What in the world? TIME magazine in November 2013 stated: In an age filled with advanced medical techniques like
Anterolateral Ligament Bradd G. Burkhart, MD Orlando Orthopaedic Center Sports Medicine What in the world? TIME magazine in November 2013 stated: In an age filled with advanced medical techniques like
Accelerated Rehabilitation Following ACL-PTG Reconstruction with Medial Collateral Ligament Repair
 Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore normal range of
Page 1 of 7 Accelerated Rehabilitation Following ACL-PTG Reconstruction with Medial Collateral Ligament Repair PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore normal range of
l. Initiate early proprioceptive activity and progress by means of distraction techniques: i. eyes open to eyes closed ii. stable to unstable m.
 Meniscus Repair 1. Defined a. Sutures or bioabsorbable fixation devices (arrows, darts, screws, etc.) bring together and fixate the edges of a tear in the meniscus in order to maintain the shock absorption
Meniscus Repair 1. Defined a. Sutures or bioabsorbable fixation devices (arrows, darts, screws, etc.) bring together and fixate the edges of a tear in the meniscus in order to maintain the shock absorption
Advances in cartilage and soft tissue injuries of the knee
 Advances in cartilage and soft tissue injuries of the knee Dr Tim McMeniman BSc(Med)/MBBS (UNSW), FRACS (Orth) Senior Lecturer, University of Queensland Declarations Mater Health Services Visiting Medical
Advances in cartilage and soft tissue injuries of the knee Dr Tim McMeniman BSc(Med)/MBBS (UNSW), FRACS (Orth) Senior Lecturer, University of Queensland Declarations Mater Health Services Visiting Medical
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
REHABILITATION PROTOCOL Criteria-Based Postoperative ACL Reconstruction Rehabilitation Protocol
 REHABILITATION PROTOCOL Criteria-Based Postoperative ACL Reconstruction Rehabilitation Protocol Phase I (Days 1 7) WEIGHTBEARING STATUS 1- Two crutches, weightbearing as tolerated. Exercises 1- Heel slides/wall
REHABILITATION PROTOCOL Criteria-Based Postoperative ACL Reconstruction Rehabilitation Protocol Phase I (Days 1 7) WEIGHTBEARING STATUS 1- Two crutches, weightbearing as tolerated. Exercises 1- Heel slides/wall
ACL Reconstruction with Hamstring Autograft Rehabilitation Protocol
 Brennen Lucas, M.D. Advanced Orthopaedic Associates 316-631-1600 Fax: (316) 631-1674 2778 N. Webb Rd. Wichita, KS 67226 www.aoaortho.com ACL Reconstruction with Hamstring Autograft Rehabilitation Protocol
Brennen Lucas, M.D. Advanced Orthopaedic Associates 316-631-1600 Fax: (316) 631-1674 2778 N. Webb Rd. Wichita, KS 67226 www.aoaortho.com ACL Reconstruction with Hamstring Autograft Rehabilitation Protocol
In the name of god. Knee. By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions. Heat: Dr. Babakhani. Nov.
 In the name of god Knee By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions Heat: Dr. Babakhani Nov. 2014 1 Anatomy-Bones Bones Femur Medial/lateral femoral condyles articulate
In the name of god Knee By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions Heat: Dr. Babakhani Nov. 2014 1 Anatomy-Bones Bones Femur Medial/lateral femoral condyles articulate
PRINCIPLES OF EXAMNINIG THE KNEE
 Welcome! Pignon, Haiti IS IT. GOOD MORNING LORD! OR GOOD LORD, MORNING! PRINCIPLES OF EXAMNINIG THE KNEE Greg Bennett, PT, DSc Excel Physical Therapy Marymount University Rules Hx often diagnostic Least
Welcome! Pignon, Haiti IS IT. GOOD MORNING LORD! OR GOOD LORD, MORNING! PRINCIPLES OF EXAMNINIG THE KNEE Greg Bennett, PT, DSc Excel Physical Therapy Marymount University Rules Hx often diagnostic Least
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
Femoral Condyle Rehabilitation Guidelines
 Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Brace: Protect healing tissue from load and shear forces Decrease pain and effusion Restore full passive knee extension
Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Brace: Protect healing tissue from load and shear forces Decrease pain and effusion Restore full passive knee extension
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
Anterior Cruciate Ligament (ACL) Rehabilitation
 Rehabilitation") Thomas D. Rosenberg, M.D. Vernon J. Cooley, M.D. Anterior Cruciate Ligament (ACL) Rehabilitation Dear Enclosed you will find a copy of our Anterior Cruciate Ligament (ACL) Rehabilitation program and the
Thomas D. Rosenberg, M.D. Vernon J. Cooley, M.D. Anterior Cruciate Ligament (ACL) Rehabilitation Dear Enclosed you will find a copy of our Anterior Cruciate Ligament (ACL) Rehabilitation program and the
BASELINE QUESTIONNAIRE (SURGEON)
") SECTION A: STUDY INFORMATION Subject ID: - - Study Visit: Baseline Site Number: Date: / / Surgeon ID: SECTION B: INITIAL SURGEON HISTORY B1. Previous Knee Surgery: Yes No Not recorded B2. Number of Previous
SECTION A: STUDY INFORMATION Subject ID: - - Study Visit: Baseline Site Number: Date: / / Surgeon ID: SECTION B: INITIAL SURGEON HISTORY B1. Previous Knee Surgery: Yes No Not recorded B2. Number of Previous
KNEE INJURIES IN SPORTS MEDICINE
 KNEE INJURIES IN SPORTS MEDICINE Irving Raphael, MD June 13, 2014 RSM Medical Associates Head Team Physician Syracuse University Outline Meniscal Injuries anatomy Exam Treatment ACL Injuries Etiology Physical
KNEE INJURIES IN SPORTS MEDICINE Irving Raphael, MD June 13, 2014 RSM Medical Associates Head Team Physician Syracuse University Outline Meniscal Injuries anatomy Exam Treatment ACL Injuries Etiology Physical
ACL Reconstruction Rehabilitation Bone Patellar Tendon Bone Graft Kyle F. Chun, MD
 ACL Reconstruction Rehabilitation Bone Patellar Tendon Bone Graft Kyle F. Chun, MD [ ] Meniscus Repair (If checked, WBAT in brace in full extension, ROM 0-90 x 6 wks; WBAT 0-90, ROM 0-120 weeks 7-12; WBAT/ROMAT
ACL Reconstruction Rehabilitation Bone Patellar Tendon Bone Graft Kyle F. Chun, MD [ ] Meniscus Repair (If checked, WBAT in brace in full extension, ROM 0-90 x 6 wks; WBAT 0-90, ROM 0-120 weeks 7-12; WBAT/ROMAT
Rehabilitation Guidelines for Meniscal Repair
 Rehabilitation Guidelines for Meniscal Repair The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These bones are supported by a large
Rehabilitation Guidelines for Meniscal Repair The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These bones are supported by a large
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas Phone: Fax:
 Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 MENISCAL REPAIR PROTOCOL Longitudinal Meniscal Repair This rehabilitation
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 MENISCAL REPAIR PROTOCOL Longitudinal Meniscal Repair This rehabilitation
7/20/14. Patella Instability. Alignment. PF contact areas. Tissue Restraints. Pain. Acute Blunt force trauma Disorders of the Patellafemoral Joint
 Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
Knee PCL Reconstruction Rehabilitation Program
 The Gundersen Health System Sports Medicine PCL Reconstruction Rehabilitation Program is an evidencebased and soft tissue healing dependent program allowing patients to progress to vocational and sports-related
The Gundersen Health System Sports Medicine PCL Reconstruction Rehabilitation Program is an evidencebased and soft tissue healing dependent program allowing patients to progress to vocational and sports-related
What to Expect from your Anterior Cruciate Ligament (ACL) Reconstruction Surgery A Guide for Patients
 Reconstruction Surgery A Guide for Patients") What to Expect from your Anterior Cruciate Ligament (ACL) Reconstruction Surgery A Guide for Patients Sources of Information: http://orthoinfo.aaos.org http://www.orthoinfo.org/informedpatient.cfm http://www.sportsmed.org/patient/
What to Expect from your Anterior Cruciate Ligament (ACL) Reconstruction Surgery A Guide for Patients Sources of Information: http://orthoinfo.aaos.org http://www.orthoinfo.org/informedpatient.cfm http://www.sportsmed.org/patient/
Accelerated Rehabilitation Following ACL Allograft Reconstruction
 Page 1 of 7 Accelerated Rehabilitation Following ACL Allograft Reconstruction PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore normal range of motion (especially knee extension)
Page 1 of 7 Accelerated Rehabilitation Following ACL Allograft Reconstruction PREOPERATIVE PHASE Goals: Diminish inflammation, swelling, and pain Restore normal range of motion (especially knee extension)
Medical Practice for Sports Injuries and Disorders of the Knee
 Sports-Related Injuries and Disorders Medical Practice for Sports Injuries and Disorders of the Knee JMAJ 48(1): 20 24, 2005 Hirotsugu MURATSU*, Masahiro KUROSAKA**, Tetsuji YAMAMOTO***, and Shinichi YOSHIDA****
Sports-Related Injuries and Disorders Medical Practice for Sports Injuries and Disorders of the Knee JMAJ 48(1): 20 24, 2005 Hirotsugu MURATSU*, Masahiro KUROSAKA**, Tetsuji YAMAMOTO***, and Shinichi YOSHIDA****