Spinal Trauma. Dr T G Kruger
|
|
|
- Elfreda Watkins
- 5 years ago
- Views:
Transcription



1 Spinal Trauma Dr T G Kruger
2 Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have head injuries South Africa high incidence of gunshot injuries to the spine
3 Location Most commonly cervical - 60% 6% of all blunt trauma injuries have associated cervical injuries Lumbar up to 25% of spinal injuries 50% of patients have complete fallout
4 Neural injury primary injury - tissue disruption by mechanical forces secondary injury - biologic response initiated by the trauma
5 Primary injury Concussion - physiologic disruption without anatomic changes Contusion - tissue haemorrhage and swelling Laceration - loss of continuity of structural elements Most cord injuries are crushing injuries

6 Biological response
7 Secondary injury Ischemia contributes to delayed secondary injury Severity of neurological injury is proportional to the duration of cord deformation Reversible injury may become irreversible from local ischemia and inflammation.
8 Goal of treatment Restoration of the patient to maximal possible function Protect all patients until a spinal injury is definitively excluded or identified Identify associated injuries Protecting uninjured neural tissues Maximize recovery of injured neural tissues Optimize musculoskeletal portions of the spinal column

9 Initial management All trauma patients are at risk for spinal injury ABC ATLS maximize O 2 to the cord Securing the airway In line stabilization Head and neck - aligned with the long axis of the trunk Immobilized in this position Cervical collar, sandbags, tape, and spine board Remember the anatomic differences of children Steroid should be administered as soon as Dx of cord pathology is made Transport as soon as stable time is NB
 Diagnosis of severely unstable injuries Analysis of hemodynamic parameters Hemodinamic shock Neurogenic")
10 Casualty Continue resuscitation Urinary catheter Peripheral lines Nasogastric tube Spine evaluation(primary): Neurological evaluation (Gross) Diagnosis of severely unstable injuries Analysis of hemodynamic parameters Hemodinamic shock Neurogenic shock

11 Casualty Complete spine examination follows resuscitation Inspection and palpation Log Roll 4 assistants necessary Haemorrhage, abrasion, laceration, malalignment, or palpable gap Perineal reflex and rectal examination

12 Casualty Complete neurological examination Complete Frankel scale A Total loss of function B Sensation sparing C Motor sparing not useful D Motor sparing useful E Normal Neurological level is the most caudal level with intact motor and sensory function
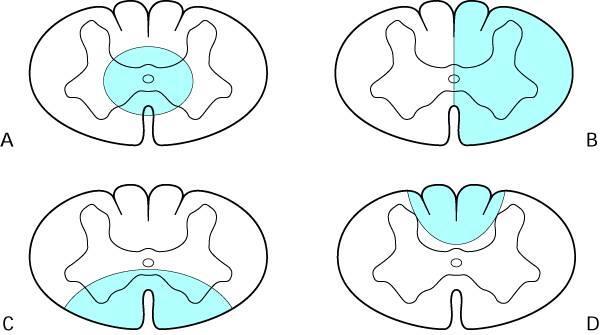
13 Neurological assessment Power is graded from 1 to 5 Incomplete lesions Sentral Cord Brown Sequard Anterior Cord syndrome Posterior Cord syndrome Sacral sparing

14
15 Unresponsive patient Spontaneous extremity motion Response to noxious stimuli Reflexes Rectal tone Spontaneous respiration Elevation and separation of the costal margins
16 NO FINAL NEUROLOGICAL LEVEL UNTIL SPINAL SHOCK IS OVER
17 Spinal shock Over when primitive reflexes return Bulbocavernosis reflex Anal wink Absence of the bulbocavernosus reflex and the anal wink Spinal shock, damage to the sacral segments of the cord, or injury to the sacral roots.



18 Radiographic evaluation Cervical X-rays See C7 T1 junction If not possible do swimmers view
19 Cervical XR





20 Radiographic evaluation Cervical XR Soft tissue injury flexion extension views Dangerous in acute setting Thoracolumbar X-rays Often difficult to interpret Have to make accurate diagnosis Ct scan MRI Determine the mechanism of injury Compression versus distraction

21 Immobilization Cervical injuries Distraction injuries Halo thoracic jacket Sandbags and tape Watch out for pressure sores All other injuries Gardner Well s skull tongs A neck collar alone is not sufficient immobilization for a cervical injury
22 C spine injury Incomplete and complete neurology Immediate closed reduction Up to 70% of body weight is safe MRI should not delay reduction Post reduction MRI Awake patient!!!!! Intact/obtunded patients MRI before reduction Surgery
23 Traction Technique Arbitrary starting weight of 3 pounds per injury level Caveat fracture dislocation C2 Levine + Edwards Type IIA Ankylosing spondilitis Added every min Monitoring No upper weight limit
24 Traction Technique Stop adding weights: Reduction Intractable pain Worsening neurology Over distraction on XR Impractical to add weight Pt sliding up in the bed Decision that reduction has failed
25 Thoracolumbar Positional immobilization Reduction and decompression can not be performed closed Surgery usually necessary in cases of neurological compromise Instability is already implied
26 Special cases Significant spinal cord injury trauma without any fractures or ligamentous ruptures SCIWORA Commonly children <10 years of age Patients > 50yrs Bulging of ligamentum flavum Gunshot Injuries Rarely cause spine instability Decompression does not improve recovery Traversed the oropharynx or colon intravenous antibiotics 3 days for infection prophylaxis
27 Checklist spinal cord injury IV line Nasogastric tube Bladder catherization CVP O2 DVT Prevention of gastric ulcers
28 Complications Skin and pressure sores Bladder and bowel Muscle and joints Hyper-reflexia syndrome Heterotopic ossification Physiological set-up
29 Prognosis Initial management Age Severity of spinal injury General condition of patient Associated injuries Definitive management Rehabilitation
30 Spinal Trauma Dr T G Kruger

31
32 Cervical fractures
33 Cervical spine injuries Whiplash C1 (Jefferson fracture) C1 / C2 rotatory subluxation C2 odontoid fracture or dislocation Hangmans C2 fracture C3 to C7 fracture and dislocations Facet dislocations

34 Whiplash

35 Whiplash

36 Whiplash
37 Whiplash Purely soft tissue injury Can lead to neurological compromise in severe cases Most cases need only conservative treatment Important to exclude serious injury with flexion extension views Before discharge 85% of fatalities associated with blunt trauma to the craniocervical spine are purely ligamentous injuries


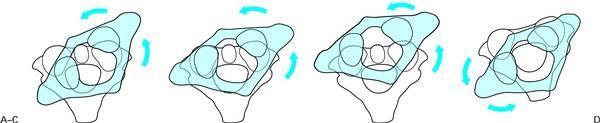
38 Mechanism of injury Mechanism of Injury Axial Force: Distraction Force



39 Cervical Trauma Mechanism of Injury Flexion: Extension:




40 Cervical Trauma Mechanism of Injury Shear: A force parallel to the surface on which it acts Rotational A torsional force that rotates tissue fibers

41

42




43 Functional units Cervical vertebrae divided into 2 functional units Upper cervical region C1 C2 Lower cervical region C3 T1
44 Upper cervical spine Neurological symptoms vary Locked in syndrome Brown Sequart syndrome Most used to be incompatible with life No neurology due to large empty space Clinical - look for haematoma and swelling
45 Radiology Lateral C-spine not enough for upper cervical injuries Open mouth view is essential If still uncertain do tomograms

46


47 Open mouth view Normal AP cannot see upper cervical area
48 Fractures of the Atlas Usually due to axial compression Can be stable or unstable Combined overhang >6.9mm = unstable All depends on the integrity of the transverse ligament Can be diagnosed with MRI Stable = conservative treatment
49 Fractures of the Atlas A + B > 6.9mm A B Jefferson Fracture

50 Atlantoaxial Rotary subluxation



51 Odontoid Fractures Most common C2 fracture Usually unstable Treatment depends on type of fracture and displacement Treatment either Halo-thoracic jacket or surgery


52 Hangman s fracture Traumatic Spondylolisthesis of the Axis

53 Lower cervical spine Stability easiest to gage using the 3 column model Anterior column anterior half of the vertebral body and the anterior ligamentous complex Middle column dorsal half of the vertebral body and the middle ligamentous complex Posterior column everything posterior to the middle column
54 COMPRESSION FLEXION Allen and Fergusson


55

56

57 Vertical compression



58
59 Distraction-flexion Perched facets<25% Unifacet



60 Distraction flexion Reduction ASAP



61 Distraction flexion Reduction ASAP
62 Compression extension Unilateral lamina Bilateral lamina Bilateral Arch Partially displaced

63 Distraction extension

64 Lateral flexion
65 Thoracolumbar fractures
66 Physical Examination Log-rolled to the side + cervical spine immobilized Entire length of the spine should be inspected Abrasions, ecchymoses, deformity Spinous processes should be palpated for step-offs or interspinous widening Backboard in lateral turning is recommended

67 Classification No ideal system available Denis 3 column system


68 Fractures Compression fractures Most common Usually throracolumbar junction Middle column remains intact Usually stable Treated conservatively




69 Burst fractures Failure of anterior and middle columns Often retropulsion of fragments into canal
70 Burst fractures Radiological signs More than 50% compression Retropulsion of fagments Widening of interpendicular distance on AP view Usually unstable Brace or operative treatment


 of intraabdominal damage")
71 Flexion-distraction Seat Belt injuries Chance fractures Can be only ligamentous injury Can be missed Rarely neurological compromize High incidence (50% to 67%) of intraabdominal damage Unstable fractures
72 Fracture-Dislocations Failure of all 3 columns Very unstable High incidence of neurological damage Usually needs surgery
73 Sacral fractures Difficult to diagnose Frequently associated with pelvis fractures Treatment difficult Associated with damage to sacral nerve plexus Retro peritoneal bleeding can be a problem Usually treated conservatively

74
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D.
 Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Acute spinal cord injury
 Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Wounds and Injuries of the Spinal Column and Cord
 Wounds and Injuries of the Spinal Column and Cord Chapter 20 Wounds and Injuries of the Spinal Column and Cord Introduction Combat injuries of the spinal column, with or without associated spinal cord
Wounds and Injuries of the Spinal Column and Cord Chapter 20 Wounds and Injuries of the Spinal Column and Cord Introduction Combat injuries of the spinal column, with or without associated spinal cord
Spine Trauma- Part B
 Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
Fractures of the thoracic and lumbar spine and thoracolumbar transition
 Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Outline. Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures
 C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Subaxial Cervical Spine Trauma
 Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Subaxial Cervical Spine Trauma Dr Hesarikia BUMS
 Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Thorasic and lumbar spinal injury. Dr.Abrisham
 Thorasic and lumbar spinal injury Dr.Abrisham Goal : alignment Stability Preserve neuologic function early mobilization Incidence: most site is thoraco lumbar 50% T 11 to L 1 30% L 2 to L 5 Motor vehicle
Thorasic and lumbar spinal injury Dr.Abrisham Goal : alignment Stability Preserve neuologic function early mobilization Incidence: most site is thoraco lumbar 50% T 11 to L 1 30% L 2 to L 5 Motor vehicle
102 Results RESULTS. Age Mean=S.D Range 42= years -84 years Number % <30 years years >50 years
 102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
Cervical Spine Injury Guidelines
 6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question.
 EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
The craniocervical junction
 Anver Jameel, MD The craniocervical junction A biomechanical and anatomical unit that extends from the skull base to C2 Includes the clivus, foramen magnum and contiguous occipital bone, the occipital
Anver Jameel, MD The craniocervical junction A biomechanical and anatomical unit that extends from the skull base to C2 Includes the clivus, foramen magnum and contiguous occipital bone, the occipital
Thoracic and Lumbar Spine Fractures and Dislocations: Assessment and Classification
 Thoracic and Lumbar Spine Fractures and Dislocations: Assessment and Classification Mark L Prasarn MD University of Texas Dept of Orthopaedic Surgery Houston, Texas Updated 7/2016 Anatomy of the Spine
Thoracic and Lumbar Spine Fractures and Dislocations: Assessment and Classification Mark L Prasarn MD University of Texas Dept of Orthopaedic Surgery Houston, Texas Updated 7/2016 Anatomy of the Spine
Thoracolumbar Spine Fractures
 Thoracolumbar Spine Fractures C. Craig Blackmore, MD, MPH Professor of Radiology Adjunct Professor of Health Services Harborview Injury Prevention and Research Center University of Washington Outline Who
Thoracolumbar Spine Fractures C. Craig Blackmore, MD, MPH Professor of Radiology Adjunct Professor of Health Services Harborview Injury Prevention and Research Center University of Washington Outline Who
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Classification of Thoracolumbar Spine Injuries
 Classification of Thoracolumbar Spine Injuries Guillem Saló Bru 1 IMAS. Hospitals del Mar i de l Esperança. ICATME. Institut Universitari Dexeus USP. UNIVERSITAT AUTÒNOMA DE BARCELONA Objectives of classification
Classification of Thoracolumbar Spine Injuries Guillem Saló Bru 1 IMAS. Hospitals del Mar i de l Esperança. ICATME. Institut Universitari Dexeus USP. UNIVERSITAT AUTÒNOMA DE BARCELONA Objectives of classification
SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012
 SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012 INTRODUCTION Mortal condition recognised since antiquity First described in the Edwin Smith papyrus 2500BC An ailment not
SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012 INTRODUCTION Mortal condition recognised since antiquity First described in the Edwin Smith papyrus 2500BC An ailment not
VERTEBRAL COLUMN ANATOMY IN CNS COURSE
 VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES
 AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES T H E A O / A S I F ( A R B E I T S G E M E I N S C H A F T F Ü R O S T E O S Y N T H E S E F R A G E N / A S S O C I A T I O N F O R T H E S T U D Y O
AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES T H E A O / A S I F ( A R B E I T S G E M E I N S C H A F T F Ü R O S T E O S Y N T H E S E F R A G E N / A S S O C I A T I O N F O R T H E S T U D Y O
Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men years old
 Annually 15,000 permanent spinal cord injuries Commonly men years old") 1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
factor for identifying unstable thoracolumbar fractures. There are clinical and radiological criteria
 NMJ-Vol :2/ Issue:1/ Jan June 2013 Case Report Medical Sciences Progressive subluxation of thoracic wedge compression fracture with unidentified PLC injury Dr.Thalluri.Gopala krishnaiah* Dr.Voleti.Surya
NMJ-Vol :2/ Issue:1/ Jan June 2013 Case Report Medical Sciences Progressive subluxation of thoracic wedge compression fracture with unidentified PLC injury Dr.Thalluri.Gopala krishnaiah* Dr.Voleti.Surya
Imaging of Cervical Spine Trauma
 Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Upper Cervical Spine - Occult Injury and Trigger for CT Exam
 Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
11. Spinal cord injury
 11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
SPECIFIC CATEGORIES OF INJURIES
 Página 1 de 20 Copyright 2003 Lippincott Williams & Wilkins Hickey, Joanne V. Clinical Practice of Neurological & Neurosurgical Nursing, 5th Edition SPECIFIC CATEGORIES OF INJURIES Part of "Chapter 19
Página 1 de 20 Copyright 2003 Lippincott Williams & Wilkins Hickey, Joanne V. Clinical Practice of Neurological & Neurosurgical Nursing, 5th Edition SPECIFIC CATEGORIES OF INJURIES Part of "Chapter 19
It consist of two components: the outer, laminar fibrous container (or annulus), and the inner, semifluid mass (the nucleus pulposus).
, and the inner, semifluid mass (the nucleus pulposus).") Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Imaging of Trauma to the Spine. Orthopedic Diplomate Program University of Bridgeport College of Chiropractic
 Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Ligaments of the vertebral column:
 In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
RETROLISTHESIS. Retrolisthesis. is found mainly in the cervical spine and lumbar region but can also be often seen in the thoracic spine
 RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Physical and Radiographic Examination of the Spine
 Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms.
 RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
MDCT and MRI evaluation of cervical spine trauma
 Insights Imaging (2014) 5:67 75 DOI 10.1007/s13244-013-0304-2 PICTORIAL REVIEW MDCT and MRI evaluation of cervical spine trauma Michael Utz & Shadab Khan & Daniel O Connor & Stephen Meyers Received: 10
Insights Imaging (2014) 5:67 75 DOI 10.1007/s13244-013-0304-2 PICTORIAL REVIEW MDCT and MRI evaluation of cervical spine trauma Michael Utz & Shadab Khan & Daniel O Connor & Stephen Meyers Received: 10
Thoracolumbar spine trauma classifications: evolution or more confusion
 Thoracolumbar spine trauma classifications: evolution or more confusion Poster No.: C-1713 Congress: ECR 2012 Type: Educational Exhibit Authors: J. P. Salazar, J. Halaburda Berni, C. Torrents, L. Casas;
Thoracolumbar spine trauma classifications: evolution or more confusion Poster No.: C-1713 Congress: ECR 2012 Type: Educational Exhibit Authors: J. P. Salazar, J. Halaburda Berni, C. Torrents, L. Casas;
2. The vertebral arch is composed of pedicles (projecting from the body) and laminae (uniting arch posteriorly).
 and laminae (uniting arch posteriorly).") VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Spinal Column. Anatomy Of The Spine
 Anatomy Of The Spine The spine is a flexible column, composed of a stack of individual bones. Each bone is called a vertebra. There are seven vertebrae in the neck (cervical vertebrae) twelve in the thoracic
Anatomy Of The Spine The spine is a flexible column, composed of a stack of individual bones. Each bone is called a vertebra. There are seven vertebrae in the neck (cervical vertebrae) twelve in the thoracic
Spine. Neuroradiology. Spine. Spine Pathology. Distribution of fractures. Radiological algorithm. Role of radiology 18/11/2015
 Spine Neuroradiology Spine Prof.Dr.Nail Bulakbaşı X Ray: AP/L/Oblique Vertebra & disc spaces CT & CTA Vertebra, discs, vessels MRI & MRA Vertebra, disc, vessels, meninges Spinal cord & nerves Myelography
Spine Neuroradiology Spine Prof.Dr.Nail Bulakbaşı X Ray: AP/L/Oblique Vertebra & disc spaces CT & CTA Vertebra, discs, vessels MRI & MRA Vertebra, disc, vessels, meninges Spinal cord & nerves Myelography
THORACO-LUMBAR SPINE TRAUMA NORDIC TRAUMA COURSE 2016, AARHUS
 THORACO-LUMBAR SPINE TRAUMA NORDIC TRAUMA COURSE 2016, AARHUS Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Quynh T. Nguyen, MHS, PA-C
THORACO-LUMBAR SPINE TRAUMA NORDIC TRAUMA COURSE 2016, AARHUS Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Quynh T. Nguyen, MHS, PA-C
Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar
 BIOMECHANICS OF SPINE Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar What is biomechanics? Biomechanics is the study of the consequences of application of external force on the spine Primary
BIOMECHANICS OF SPINE Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar What is biomechanics? Biomechanics is the study of the consequences of application of external force on the spine Primary
THE VERTEBRAL COLUMN. Average adult length: In male: about 70 cms. In female: about 65 cms.
 THE VERTEBRAL COLUMN Average adult length: In male: about 70 cms. In female: about 65 cms. 1 Vertebral Column (Regions and Curvatures) Curvatures of the vertebral column: A. Primary curvature: C-shaped;
THE VERTEBRAL COLUMN Average adult length: In male: about 70 cms. In female: about 65 cms. 1 Vertebral Column (Regions and Curvatures) Curvatures of the vertebral column: A. Primary curvature: C-shaped;
Spinal Trauma at the Pediatric Age
 Spinal Trauma at the Pediatric Age Burçak B LG NER Nejat AKALAN ABSTRACT Spinal trauma is relatively rare in pediatric patients. The anatomy and biomechanics of the growing spine produce failure patterns
Spinal Trauma at the Pediatric Age Burçak B LG NER Nejat AKALAN ABSTRACT Spinal trauma is relatively rare in pediatric patients. The anatomy and biomechanics of the growing spine produce failure patterns
The Spine.
 The Spine www.fisiokinesiterapia.biz Characteristics of Vertebrae Cervical Spine 1 and 2 Sacrum and Coccyx Curves Lordotic in the Spine Kyphotic Lordotic Ligamentous Support Muscles of the Spine Spinal
The Spine www.fisiokinesiterapia.biz Characteristics of Vertebrae Cervical Spine 1 and 2 Sacrum and Coccyx Curves Lordotic in the Spine Kyphotic Lordotic Ligamentous Support Muscles of the Spine Spinal
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc. Copyright 2014, 2011, 2006 by Saunders, an imprint of Elsevier, Inc.
 Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Sir William Asher ANATOMY
 SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
Selective Spine Assessment & Spinal Motion Restriction
 Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
VERTEBRAL COLUMN VERTEBRAL COLUMN
 VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
Cervical Spine Trauma 2016 Nordic Trauma Society
 Cervical Spine Trauma 2016 Nordic Trauma Society Stuart E. Mirvis. M.D., FACR Department of Radiology and Maryland Shock-Trauma Center University of Maryland School of Medicine Topics to Review Definition
Cervical Spine Trauma 2016 Nordic Trauma Society Stuart E. Mirvis. M.D., FACR Department of Radiology and Maryland Shock-Trauma Center University of Maryland School of Medicine Topics to Review Definition
Spinal Trauma. General Rehabilitation of Patient with Spinal Trauma. Common Spinal Injuries. Important Anatomical Structures at each Vertebral Level
 Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
No greater tragedy can befall on a young adult in this most
 SUPPLEMENT TO JAPI may 2012 VOL. 60 19 Operative Management of Spinal Injuries Sajan Hegde * Introduction No greater tragedy can befall on a young adult in this most active period of life than a spinal
SUPPLEMENT TO JAPI may 2012 VOL. 60 19 Operative Management of Spinal Injuries Sajan Hegde * Introduction No greater tragedy can befall on a young adult in this most active period of life than a spinal
Key Primary CPT Codes: Refer to pages: 7-9 Last Review Date: October 2016 Medical Coverage Guideline Number:
 National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
VAriation. Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon. Orthopaedic & Neurosurgery backgrounds. Subspeciality training
 Greg Etherington Spine Surgeon. Orthopaedic & Neurosurgery backgrounds. Subspeciality training") Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon Orthopaedic & Neurosurgery backgrounds Subspeciality training spine, upper limb, trauma, pelvis. What do you do in spine? Lumbar Cervical Trauma
Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon Orthopaedic & Neurosurgery backgrounds Subspeciality training spine, upper limb, trauma, pelvis. What do you do in spine? Lumbar Cervical Trauma
A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries
 A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries Award: Certificate of Merit Poster No.: C-1741 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Adams, A.
A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries Award: Certificate of Merit Poster No.: C-1741 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Adams, A.
 Introduction Posterior cervical fusion is done through the back posterior of the neck. The surgery joins two or more neck vertebrae into one solid section of bone. The medical term for fusion is arthrodesis.
Introduction Posterior cervical fusion is done through the back posterior of the neck. The surgery joins two or more neck vertebrae into one solid section of bone. The medical term for fusion is arthrodesis.
Evaluation for spinal injuries among unconscious victims of blunt polytrauma: a management guideline for intensive care
 Evaluation for spinal injuries among unconscious victims of blunt polytrauma: a management guideline for intensive care Background 1.0 There is lack of consistency among clinicians when managing critically
Evaluation for spinal injuries among unconscious victims of blunt polytrauma: a management guideline for intensive care Background 1.0 There is lack of consistency among clinicians when managing critically
Chapter 20: The Spine The McGraw-Hill Companies, Inc. All rights reserved.
 Chapter 20: The Spine Anatomy of the Spine Prevention of Injuries to the Spine Cervical Spine Muscle Strengthening Muscles of the neck resist hyperflexion, hyperextension and rotational forces Prior
Chapter 20: The Spine Anatomy of the Spine Prevention of Injuries to the Spine Cervical Spine Muscle Strengthening Muscles of the neck resist hyperflexion, hyperextension and rotational forces Prior
Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series
: Case Series") Romanian Neurosurgery (2015) XXIX 3: 335-341 335 Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series Guru Dutta Satyarthee, Gaurang Vaghani,
Romanian Neurosurgery (2015) XXIX 3: 335-341 335 Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series Guru Dutta Satyarthee, Gaurang Vaghani,
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Anterior Cervical Subluxation: An Unstable Position
 275 Anterior Cervical Subluxation: An Unstable Position, 1 A. T. Scher1 The radioiogic signs of cervical anterior subluxation are subtle. Even when recognized, the injury may not be considered significant.
275 Anterior Cervical Subluxation: An Unstable Position, 1 A. T. Scher1 The radioiogic signs of cervical anterior subluxation are subtle. Even when recognized, the injury may not be considered significant.
Traumatic Spinal Cord Injury. 39 th CANP Annual Educational Conference March 18 th, :00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc
 Traumatic Spinal Cord Injury 39 th CANP Annual Educational Conference March 18 th, 2016 5:00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc Disclosures No conflicts of interest to disclose. Introduction
Traumatic Spinal Cord Injury 39 th CANP Annual Educational Conference March 18 th, 2016 5:00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc Disclosures No conflicts of interest to disclose. Introduction
Injuries to the Head and Spine
 Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Spontaneous Resolution of Spinal Canal Deformity After Burst Dispersion Fracture
 779 Spontaneous Resolution of Spinal Canal Deformity After Burst Dispersion Fracture T. M. H. Chakera 1 George Bedbrook C. M. Bradley3 We reviewed the records of 8 patients with 30 burst-dispersion spinal
779 Spontaneous Resolution of Spinal Canal Deformity After Burst Dispersion Fracture T. M. H. Chakera 1 George Bedbrook C. M. Bradley3 We reviewed the records of 8 patients with 30 burst-dispersion spinal
How to Determine the Severity of a Spinal Sprain Outline
 Spinal Trauma How to Determine the Severity of a Spinal Sprain Outline Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners.
Spinal Trauma How to Determine the Severity of a Spinal Sprain Outline Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners.
1/15/2012. Cervical Spine Trauma. Who to Image. Who to Image. Who to Image. Who to Image. Trauma Cx Spine Protocols NEXUS. CCR and Nexus CCR CCR
 Trauma Cx Spine Protocols Cervical Spine Trauma Issues The clinically negative Cx-spine Does everyone need a CT Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of
Trauma Cx Spine Protocols Cervical Spine Trauma Issues The clinically negative Cx-spine Does everyone need a CT Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director
 Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Introduction. Objectives C-Spine: Where Are We Now? NAEMSP Medical Director Course 1/9/2013
 NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
ISPUB.COM. Fracture Through the Body of the Axis. B Johnson, N Jayasekera CASE REPORT
 ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 8 Number 1 B Johnson, N Jayasekera Citation B Johnson, N Jayasekera.. The Internet Journal of Orthopedic Surgery. 2007 Volume 8 Number 1. Abstract
ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 8 Number 1 B Johnson, N Jayasekera Citation B Johnson, N Jayasekera.. The Internet Journal of Orthopedic Surgery. 2007 Volume 8 Number 1. Abstract
A CASE OF MISMANAGED CERVICAL FRACTURE IN A PATIENT OF ANKYLOSING SPONDYLITIS
 A CASE OF MISMANAGED CERVICAL FRACTURE IN A PATIENT OF ANKYLOSING SPONDYLITIS INTRODUCTION Spine fractures occur with minor trauma in patients with ankylosing Spondylitis. They are highly unstable with
A CASE OF MISMANAGED CERVICAL FRACTURE IN A PATIENT OF ANKYLOSING SPONDYLITIS INTRODUCTION Spine fractures occur with minor trauma in patients with ankylosing Spondylitis. They are highly unstable with
SpineFAQs. Lumbar Spondylolisthesis
 SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
LUMBAR SPINAL STENOSIS
 LUMBAR SPINAL STENOSIS Always occurs in the mobile segment. Factors play role in Stenosis Pre existing congenital or developmental narrowing of the lumbar spinal canal Translation of one anatomic segment
LUMBAR SPINAL STENOSIS Always occurs in the mobile segment. Factors play role in Stenosis Pre existing congenital or developmental narrowing of the lumbar spinal canal Translation of one anatomic segment
AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM
 AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM APPENDICULAR SKELETON BONES OF THE FREE APPENDAGES & THEIR POINTS OF ATTACHMENTS
AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM APPENDICULAR SKELETON BONES OF THE FREE APPENDAGES & THEIR POINTS OF ATTACHMENTS
Diagnostic accuracy of MRI in detecting posterior ligamentous complex injury in thoracolumbar vertebral fractures
 Diagnostic accuracy of MRI in detecting posterior ligamentous complex injury in thoracolumbar vertebral fractures Poster No.: C-1726 Congress: ECR 2011 Type: Scientific Exhibit Authors: E. Aguirre, P.
Diagnostic accuracy of MRI in detecting posterior ligamentous complex injury in thoracolumbar vertebral fractures Poster No.: C-1726 Congress: ECR 2011 Type: Scientific Exhibit Authors: E. Aguirre, P.
Pediatric Trauma Karim Rafaat, MD
 Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Airway Management in Adults after Cervical Spine Trauma Edward T. Crosby, M.D., F.R.C.P.C.*
 REVIEW ARTICLE David C. Warltier, M.D., Ph.D., Editor Anesthesiology 2006; 104:1293 318 2006 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Airway Management in Adults
REVIEW ARTICLE David C. Warltier, M.D., Ph.D., Editor Anesthesiology 2006; 104:1293 318 2006 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Airway Management in Adults
ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN
 ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN Consultant Musculoskeletal Radiologist Royal National Orthopaedic Hospital Stanmore,UK. INTRODUCTION 2 INTRODUCTION 3 INTRODUCTION Spinal
ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN Consultant Musculoskeletal Radiologist Royal National Orthopaedic Hospital Stanmore,UK. INTRODUCTION 2 INTRODUCTION 3 INTRODUCTION Spinal
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Prognosis of neurological deficits associated with upper cervical spine injuries
 Paraplegia (1995) 33, 195-202 1995 International Medical Society of Paraplegia All rights reserved 0031-1758/95 $9.00 Prognosis of neurological deficits associated with upper cervical spine injuries Y
Paraplegia (1995) 33, 195-202 1995 International Medical Society of Paraplegia All rights reserved 0031-1758/95 $9.00 Prognosis of neurological deficits associated with upper cervical spine injuries Y
Thoracic and Lumbar Spine Anatomy.
 Thoracic and Lumbar Spine Anatomy www.fisiokinesiterapia.biz Thoracic Vertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature Costal Fovea
Thoracic and Lumbar Spine Anatomy www.fisiokinesiterapia.biz Thoracic Vertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature Costal Fovea
POSTERIOR CERVICAL FUSION
 AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
Indications for cervical spine immobilisation: -
 Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic)
") Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic) Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete
Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic) Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete
Thoracolumbar Spinal Injuries
 31 Thoracolumbar Spinal Injuries Michael Heinzelmann, Guido A. Wanner Fractures Section 883 Core Messages Spinal fractures are frequently located at the thoracolumbar junction for biomechanical reasons
31 Thoracolumbar Spinal Injuries Michael Heinzelmann, Guido A. Wanner Fractures Section 883 Core Messages Spinal fractures are frequently located at the thoracolumbar junction for biomechanical reasons
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW
 INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
The Positive Findings In Neck Injuries. American Journal of Orthopedics. August-September, 1964, pp
 The Positive Findings In Neck Injuries 1 American Journal of Orthopedics August-September, 1964, pp. 178-187 Ruth Jackson, MD This author analyzed 5,000 patients with disorders and found the following:
The Positive Findings In Neck Injuries 1 American Journal of Orthopedics August-September, 1964, pp. 178-187 Ruth Jackson, MD This author analyzed 5,000 patients with disorders and found the following:
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018
 EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management.
 River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#