I have no financial relationships related to disclose
|
|
|
- Victor Morrison
- 5 years ago
- Views:
Transcription
 Lee S.")

 I have no")




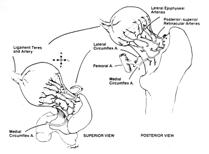
1 Evaluation of a child with a limp / Slipped Capital Femoral Epiphysis (SCFE) Lee S. Segal, MD Chief, Division of Pediatric Orthopedics American Family Children s Hospital Department of Orthopedics and Rehabilitation, University of Wisconsin School of Medicine and Public Health Madison, WI Evaluation of a child with a limp / Slipped Capital Femoral Epiphysis (SCFE) I have no financial relationships related to disclose common presentation to pediatric orthopaedic office limp can be caused by pain, weakness, or mechanical factors requires thorough history and physical examination Introduction Evaluation of the limping child narrow differential dx based upon 1. Gait 2. Location 3. Age Toddler (<4y) Child (4-10y) Adolescent (>10y) 4. Pain Normal gait Abnormal gait Trendelenburg equinus (toe- walking) circumduction/ vaulting steppage 1


 bone scan ultrasound CT MRI")


2 Non- antalgic gait Equinus: CP, congenitally tight heel cord, LLD, clubfoot Trendelenberg: LCP, DDH, SCFE, Muscular dystrophy Circumduction/Vaulting: CP, LLD, any stiffness of ankle/knee Steppage: CMT, CP, Spina Bifida History Is limp associated with or without pain? PQRST- characterize pain Provokes, Palliates Quality Radiate, Referred Severity Timing PMH Family history Physical examination gait table- top exam (supine, prone) Take age of child into consideration with exam radiographs (comparison, oblique) bone scan ultrasound CT MRI Imaging CBC with Diff ESR / CRP Lyme titer rheum (ANA, RF) joint aspiration (cell count, etc) Lab tests Critical Questions Flynn J, Widmann RF: The Limping Child: Evaluation and Diagnosis. JAAOS 2001 Is the limp due to pain? Did the pain occur suddenly or gradually, or has it always been there? Is the child systemically ill? Does the child exhibit a specific gait pattern? Can the pain be localized? 2
")

 Uterine")





")
3 Toddler s fracture DDH osteomyelitis, septic arthritis JA, Lyme tumor (benign/ malignant) Non- accidental trauma Toddler (<4y) DDH: 3+8 month old In toddler, not uncommon to present with a LLD and limp Risk Factors 4 F s : Breech, +FH, 1 st born, female (6:1) Uterine compression syndrome Associated structural abnormalities Ethnic groups * majority of infants with DDH don t have a risk factor * safe swaddling Treatment depends on age of presentation 0-6 months Pavlik harness 6-18 months Hip arthrogram, +/- adductor tenotomy, closed/open reduction and hip spica cast for weeks > 3 years late discovery DDH open reduction with femoral shortening + pelvic osteotomy Pediatric bone and joint infection / synovitis Legg- Calve- Perthes fracture OCD Foreign body Tumor Lyme disease Child (4-10y) Transient synovitis Septic arthritis Osteomyelitis 3

 Don t want to miss septic hip, severe sequelae Confirm with aspiration fluid")

 Treatment is drainage and irrigation,")

4 Transient Synovitis Hip joint most often affected Mild pain, fever, stiffness, lab abnormalities (T<101, ESR< 50, WBC< 15,000) Tolerate movement of hip if done cautiously U/S shows minimal fluid in joint TX- Rest and NSAIDS Improvement is usually within a few days to 2 wks Wax and wane, recurrence Septic arthritis hip joint commonly involved Child appears toxic, irritable Severe pain with joint ROM U/S demonstrate joint effusion Neonate often has multiple joint involvement, may not mount inflammatory response (fever, ESR, WBC) Don t want to miss septic hip, severe sequelae Confirm with aspiration fluid normal Transient synovitis vs septic arthritis of hip Prediction of septic arthritis is 93% with 3 or more of the following (Kocher criteria) Fever NWB ESR >40 WBC >12,000 * Does not replace the clinical exam Septic arthritis of the hip Infant with septic arthritis of the left hip Hip held rigidly in the classic position of flexion, abduction, and external rotation position that maximizes capsular volume Infant relatively comfortable as long as the hip remains immobile in this position Septic Arthritis Diagnosis is made via hip joint aspiration (US or in OR) Treatment is drainage and irrigation, followed by antibiotics Early treatment is important for a good result Identify the cause, determine which antibiotic, duration, route Legg Calve- Perthes Disease Most common in children 4 to 8 yrs old Males > females affected Insidious limp is most common presentation Limited hip abduction and internal rotation on exam 4

 disruption of")







, OCD Transitional: SCFE,")
5 LCP - etiology Unknown source of frustration, 2 prevailing theories Perthes Disease temporal classification - xray Initial Fragmentation Reossification Healed 9 Mo 32 Mo 10 yr (1) disruption of blood supply * disturbance clotting mechanism * hyperviscosity Factor Leiden V, Protein S and C deficiency (2) underlying systemic disorder primary disorder of epiphyseal cartilage? delayed skeletal maturation, shorter stature, ADHD Extent of involvement Catterall Lateral Pillar classification prognosis Age at presentation (<6 years) Extent of involvement Perfusion MRI Duration of disease process Clinical ROM Treatment principles goal maintain sphericity femoral head Maintain ROM (PT, NSAID, petrie casts) Containment (bracing vs surgery) If >6 yo or lateral pillar B/C, hip subluxation, other treatment may be considered (femoral or pelvic osteotomy) Long term prognosis depends on residual femoral head deformity Adolescent (>10 yrs) CITMAT Sports - related stress fractures (overuse, repetitive), OCD Transitional: SCFE, tarsal coalition, Osgood- Schlatter Inflammation: Juvenile arthritis, Infection: Osteomyelitis, Lyme disease Tumor 5


 the unsolved adolescent hip disorder Most")




6 The limping child Common musculoskeletal presentation Determine gait pattern, associated with or without pain, age of child, and localization Establish differential DX, choose appropriate studies to confirm diagnosis Be familiar with treatment with relation to condition Slipped Capital Femoral Epiphysis (SCFE) the unsolved adolescent hip disorder Most common adolescent hip disorder Missed or delay in diagnosis Asymptomatic, chronic SCFE tilt deformity Etiology remains unknown etiology remains unknown Missed or delay in diagnosis endocrine trauma mechanical genetic inflammatory Kocher et al Pediatrics 2004 Median delay 8 weeks Significant relationship: delay in dx à increase slip severity Matava JPO 1999 Isolated distal thigh or knee pain common presentation Leads to higher rates of missed dx, unnecessary x- rays, and more severe slips Silent slip Silent slip 6






 consider")


 pituitary and parathyroid")
7 Silent slip Silent slip à tilt / pistol grip deformity Clinical presentation May complain of hip, thigh, or knee pain (Hilton s Law) Extremity externally rotated + roll test +/- ability to WB ** Any older child or adolescent with knee pain has a SCFE until proven otherwise Preventing progression of the slip Promote closure of the growth plate Minimizing risks of AVN / chondrolysis Prophylactic pinning of contralateral hip controversial in NA Treatment goals Narrow age range at presentation Males yrs Females yrs Beyond this range (+/- 2 yrs) consider endocrine or systemic disorder (atypical) Atypical SCFE Below 10 th percentile for height for chronologic age Bilateral presentation Juvenile Consider associated endocrine disorder : hypothyroidism (esp. if < 10) pituitary and parathyroid abnormalities VDRR Radiation exposure GH treatment Renal osteodystrophy 7
")

 40 o Traditional (temporal) Acute, acute")





8 smooth k- wires/semitubular plate (1996) Epidemiology kidney transplant (2005) Incidence - 2/100,000 Ethnic variation Seasonal variation Geographic variation (40 o latitude) Bilateral 25% (?) 40 o Traditional (temporal) Acute, acute on chronic, chronic Physeal stability Severity of slip classification Onset < 3 weeks Epiphyseal displacement without remodeling High risk AVN >15% Acute SCFE Physeal stability pathophysiology Loder et al JBJS 75A, 1993 Clinical evaluation Unstable - patient presents with severe hip pain, and is unable to walk with or without crutches, regardless of the duration of symptoms Fluoroscopic evaluation *prognostic importance Direction of slip True posterior Hypertrophic zone of physis 8



 Prevent further slip*")

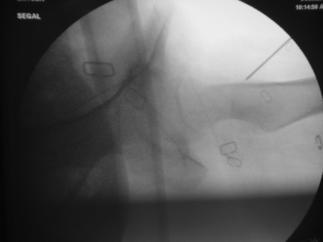
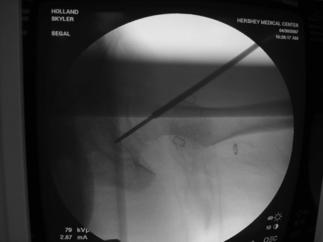
9 Torsional basis / SCFE torsional basis of SCFE Both coronal + sagittal planes of shear loading Displacement of CFE resolved by common torsional force radiographs AC ** must obtain both AP and frog- lateral x- rays of the pelvis AP radiograph - Difficult to recognize minimal slip Clues Klein s line Decreased epiphyseal height Blanch sign AC Goals of Treatment (older) Prevent further slip* Promote premature physeal closure* Minimize risks associated with SCFE Evolving concepts with SCFE FAI femoral acetabular impingement 9





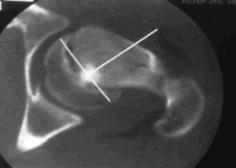






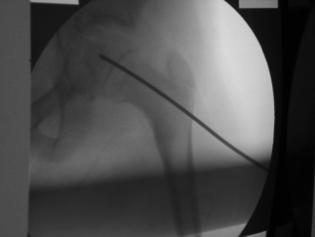
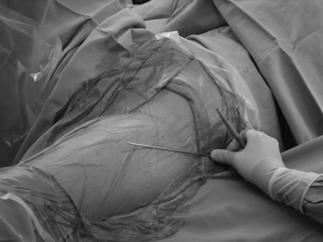

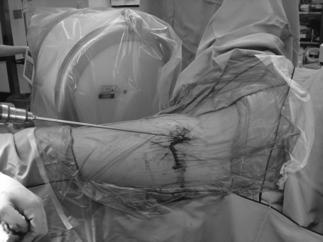
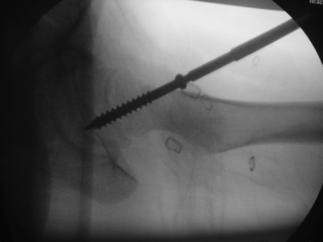
10 treatment Always consider dx Don t send home Differentiate stable vs. unstable Do not allow further ambulation Surgical urgency standard of care North America : in- situ single screw fixation NORTH AMERICA CANNULATED SCREW FIXATION/single B/L INCIDENCE 25% OBSERVE CONTRALATERAL HIP GERMANY K WIRE FIXATION B/L INCIDENCE 75% STABILIZE CONTRALATERAL HIP Entry site different than pinning hip fracture 10



















11 9/7/14 11















12 risks AVN chondrolysis Unstable Slip severity Iatrogenic Segmental vs global pitfalls c. Pin in situ for severe SCFE In past used to consider osteotomies to compensate for deformity a. b. a. Growth disturbance / premature closure b. Subtrochanteric fracture c. Strip screws upon attempt to remove C osteotomies A New concepts Contralateral hip prophylactic stabilization Femoral acetabular impingement (FAI) AVN risk higher closer to deformity Open surgical hip dislocation 12











13 Femoral Acetabular Impingement (FAI) Open surgical hip dislocation Preserve blood supply CAM FAI Surgical hip dislocation protects blood supply to femoral head summary Any adolescent with knee pain is a SCFE until proven otherwise Always obtain x- ray of pelvis Always obtain 2 views (AP/Frog) Surgical urgency don t send home Delay in Dx increases risk of slip severity Thank you 13
Case Presentations The Child with a Limp
 Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState
Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState
Childhood hip conditions. Belen Carsi Paediatric Orthopaedic Consultant
 Childhood hip conditions Belen Carsi Paediatric Orthopaedic Consultant Developmental Dysplasia of the Hip Legg-Calve-Perthes disease Slipped Capital femoral epiphysis Limp Arthritis Developmental Dysplasia
Childhood hip conditions Belen Carsi Paediatric Orthopaedic Consultant Developmental Dysplasia of the Hip Legg-Calve-Perthes disease Slipped Capital femoral epiphysis Limp Arthritis Developmental Dysplasia
Peggers Super Summaries: Paediatric Hip
 EMBRYOLOGY Development o Mesenchymal stem cells cartilage blood supply bone Dates o 6/40 Limb development o 8-11/40 hip development (acetabulum and hip formed from one bone splitting by apoptosis) o 16/40
EMBRYOLOGY Development o Mesenchymal stem cells cartilage blood supply bone Dates o 6/40 Limb development o 8-11/40 hip development (acetabulum and hip formed from one bone splitting by apoptosis) o 16/40
The Limping Child: Differential Diagnosis
 The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌
 & Idiopathic 이대목동병원 윤여헌") Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌 Children s hip disorders Congenital & developmental disorders Developmental hip dysplasia (dislocation) of the hip Developmental
Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌 Children s hip disorders Congenital & developmental disorders Developmental hip dysplasia (dislocation) of the hip Developmental
Bilateral hip pain with right proximal femoral lesion
 Bilateral hip pain with right proximal femoral lesion Legg-Calve-Perthes Idiopathic osteonecrosis of the femoral head epiphysis during childhood First described by Arthur Thorton Legg in 1909 and published
Bilateral hip pain with right proximal femoral lesion Legg-Calve-Perthes Idiopathic osteonecrosis of the femoral head epiphysis during childhood First described by Arthur Thorton Legg in 1909 and published
Slipped Capital Femoral Epiphysis (SCFE)
") Slipped Capital Femoral Epiphysis (SCFE) DR MUMTAZ HUSSAIN Senior Registrar DR ABDUL LATIF SAMI (Associate Professor) Head of Department Pediatric Orthopedics Introduction and Definition Epidemiology and
Slipped Capital Femoral Epiphysis (SCFE) DR MUMTAZ HUSSAIN Senior Registrar DR ABDUL LATIF SAMI (Associate Professor) Head of Department Pediatric Orthopedics Introduction and Definition Epidemiology and
The Limping Child. Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester
 The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
Musculoskeletal Management of A Limping Child
 Musculoskeletal Management of A Limping Child Julieanne P. Sees, DO, FAOAO Pediatric Neuro-Orthopaedic Surgeon Medical Director, Neuro-Orthopaedic Rehabilitation Unit Wilmington, DE Objectives Identify
Musculoskeletal Management of A Limping Child Julieanne P. Sees, DO, FAOAO Pediatric Neuro-Orthopaedic Surgeon Medical Director, Neuro-Orthopaedic Rehabilitation Unit Wilmington, DE Objectives Identify
The Child With a Limp
 KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
Slipped Capital Femoral Epiphysis
 Slipped Capital Femoral Epiphysis Nicholas D. Fletcher, MD Assistant Professor of Orthopaedics and Scoliosis Emory University Orthopaedics Emory Orthopaedics Center for Hip Preservation What is it? Misnomer
Slipped Capital Femoral Epiphysis Nicholas D. Fletcher, MD Assistant Professor of Orthopaedics and Scoliosis Emory University Orthopaedics Emory Orthopaedics Center for Hip Preservation What is it? Misnomer
1. Discuss some common pediatric problems seen in the clinic. Diagnosis Clinical examination (at birth and subsequent well-baby examinations)
") 1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
Non-inflammatory joint pain
 Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Hip Biomechanics and Osteotomies
 Hip Biomechanics and Osteotomies Organization Introduction Hip Biomechanics Principles of Osteotomy Femoral Osteotomies Pelvic Osteotomies Summary Inroduction Osteoarthritis is very prevalent Primary OA
Hip Biomechanics and Osteotomies Organization Introduction Hip Biomechanics Principles of Osteotomy Femoral Osteotomies Pelvic Osteotomies Summary Inroduction Osteoarthritis is very prevalent Primary OA
Lower Extremity Fracture Management. Fractures of the Hip. Lower Extremity Fractures. Vascular Anatomy. Lower Extremity Fractures in Children
 Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
Four weeks of Intrauterine life
 Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
7/1/2012. Repetitive valgus stresses cause microfractures in the apophyseal cartilage (weak link) Common in year olds
 Common in year olds") 1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
A Patient s Guide to Limping in Children
 A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
Hip Dysplasia David S. Feldman, MD
 Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016
 Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Friday Teaching. Bones
 Friday Teaching Bones Regarding slipped femoral capital epiphysis It represents Salter Harris type V injury 20% are bilateral There is slight widening of the joint space Slip is typically posteromedial
Friday Teaching Bones Regarding slipped femoral capital epiphysis It represents Salter Harris type V injury 20% are bilateral There is slight widening of the joint space Slip is typically posteromedial
Effects of Immobilization. N24 Pedi Musculoskeletal Spring 2012, Week 14. Cabrillo ADN/C. Madsen RN, MSN 1. Physical effects on other systems
 Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh
 Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Musculoskeletal Concerns in the Pediatric Athlete. John Hatzenbuehler, MD FACSM ACSM TPC Course 2015
 Musculoskeletal Concerns in the Pediatric Athlete John Hatzenbuehler, MD FACSM ACSM TPC Course 2015 Dislclosures Neither I, John Hatzenbuehler nor any family member(s), have any relevant financial relationships
Musculoskeletal Concerns in the Pediatric Athlete John Hatzenbuehler, MD FACSM ACSM TPC Course 2015 Dislclosures Neither I, John Hatzenbuehler nor any family member(s), have any relevant financial relationships
DDH. Abnormal hip development Traditionally CDH (congenital dysplasia of the hip) Today DDH(developmental dysplasia of the hip)
 Today DDH(developmental dysplasia of the hip)") DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
The Hip Baby?? Baby Hippie??
 In Need of a Title? The Hip Baby?? Baby Hippie?? Review of Developmental Dysplasia of the Hip in the Newborn OCR Symposium 2018 Ryan L. Hartman, MD Specialty: Pediatric and Sports Orthopaedics 23 month
In Need of a Title? The Hip Baby?? Baby Hippie?? Review of Developmental Dysplasia of the Hip in the Newborn OCR Symposium 2018 Ryan L. Hartman, MD Specialty: Pediatric and Sports Orthopaedics 23 month
Pediatric Orthopedics in Your Office. Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care
 Pediatric Orthopedics in Your Office Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care Overview for 20 minute whirlwind Clavicle Distal radius fractures Finger fractures
Pediatric Orthopedics in Your Office Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care Overview for 20 minute whirlwind Clavicle Distal radius fractures Finger fractures
Broadening the Differential: Spine and Lower Extremity Injuries in the Young Athlete. Disclosures. Goals. Dr. Nirav K. Pandya
 Broadening the Differential: Spine and Lower Extremity Injuries in the Young Athlete Disclosures - Consultant - Orthopediatrics - Committee Member POSNA Dr. Nirav K. Pandya Assistant Professor of Orthopaedic
Broadening the Differential: Spine and Lower Extremity Injuries in the Young Athlete Disclosures - Consultant - Orthopediatrics - Committee Member POSNA Dr. Nirav K. Pandya Assistant Professor of Orthopaedic
Disclosures Head to Toe: Common Sports Injuries in Kids
 Disclosures Head to Toe: Common Sports Injuries in Kids None R. Jay Lee MD Director Pediatric Orthopaedic Fellowship Assistant Professor Pediatric Orthopaedics Johns Hopkins / Bloomberg Children s Objectives
Disclosures Head to Toe: Common Sports Injuries in Kids None R. Jay Lee MD Director Pediatric Orthopaedic Fellowship Assistant Professor Pediatric Orthopaedics Johns Hopkins / Bloomberg Children s Objectives
Pediatric Orthopedics: ``To Refer or Not to Refer``
 Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
An understanding of the components of the normal gait cycle will aid in describing abnormalities of gait.
 Approach to the Child with a Limp: Student writer: Brian Mayson Resident editor: Elmine Statham Background The child with a limp is a common problem seen in pediatrics. A limp is defined as any deviation
Approach to the Child with a Limp: Student writer: Brian Mayson Resident editor: Elmine Statham Background The child with a limp is a common problem seen in pediatrics. A limp is defined as any deviation
SC FE. Slipped Capital Femoral Epiphysis SPR
 SC FE Slipped Capital Femoral Epiphysis SPR Disclosures Lecture specific-nothing to disclose. Dr. Taragin is a member of the medical advisory board of Carestream Health. SAM Goal SCFE = SCIFI PRESENTATION
SC FE Slipped Capital Femoral Epiphysis SPR Disclosures Lecture specific-nothing to disclose. Dr. Taragin is a member of the medical advisory board of Carestream Health. SAM Goal SCFE = SCIFI PRESENTATION
3/18/18. Adolescent Hip Injuries. Adolescents with Hip Injuries DISCLOSURES
 Adolescent Hip Injuries Henry Bone Ellis, Jr., MD DFW Sports Medicine Symposium March 24, 2018 DISCLOSURES Royalties and stock options Consulting income Smith and Nephew Other support Research on Osteochondritis
Adolescent Hip Injuries Henry Bone Ellis, Jr., MD DFW Sports Medicine Symposium March 24, 2018 DISCLOSURES Royalties and stock options Consulting income Smith and Nephew Other support Research on Osteochondritis
Acquired Hip Disorders in Children and Adolescents. Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA
 Acquired Hip Disorders in Children and Adolescents Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA Don t Miss Acquired Hip Disorders SCFE Posterior Hip Dislocation Osteoid
Acquired Hip Disorders in Children and Adolescents Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA Don t Miss Acquired Hip Disorders SCFE Posterior Hip Dislocation Osteoid
The Hip from Cradle to Grave. Haemish Crawford Ascot Hospital Starship Children s Hospital
 The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD. November 4, 2017
 Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Stephanie W. Mayer, MD. Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado
 Stephanie W. Mayer, MD Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado University of Colorado Sports Medicine Assistant Team Physician, Colorado Avalanche
Stephanie W. Mayer, MD Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado University of Colorado Sports Medicine Assistant Team Physician, Colorado Avalanche
A Patient s Guide to Transient Synovitis of the Hip in Children
 A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
Physeal Fractures and Growth Arrest
 Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort
 Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort Disclosures No disclosures relevant to this topic Objectives Evaluate and recognize common hip pathology
Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort Disclosures No disclosures relevant to this topic Objectives Evaluate and recognize common hip pathology
A 4 year old with hip pain: Legg-Calvé-Perthes Disease
 A 4 year old with hip pain: Legg-Calvé-Perthes Disease Cyndie Seraphin Harvard Medical School Year III Our Patient A 4 year-old boy is complaining of severe L hip pain. The differential diagnosis of acute
A 4 year old with hip pain: Legg-Calvé-Perthes Disease Cyndie Seraphin Harvard Medical School Year III Our Patient A 4 year-old boy is complaining of severe L hip pain. The differential diagnosis of acute
Bone and Joint Infections Oh, My
 Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Evaluation of Hip Pain in Adults. Jerry Ahluwalia, M.D. November 13, 2015
 Evaluation of Hip Pain in Adults Jerry Ahluwalia, M.D. November 13, 2015 Objectives Develop a better understanding of the differential diagnosis of hip pain in active young adults Appreciate key points
Evaluation of Hip Pain in Adults Jerry Ahluwalia, M.D. November 13, 2015 Objectives Develop a better understanding of the differential diagnosis of hip pain in active young adults Appreciate key points
Osteochondritis Dissecans of the Knee. M Lucas Murnaghan MD, MEd, FRCSC
 Osteochondritis Dissecans of the Knee M Lucas Murnaghan MD, MEd, FRCSC Outline 1. Clinical Presentation 2. Investigations 3. Classification 4. Non-operative Treatment 5. Operative Treatment 6. Treatment
Osteochondritis Dissecans of the Knee M Lucas Murnaghan MD, MEd, FRCSC Outline 1. Clinical Presentation 2. Investigations 3. Classification 4. Non-operative Treatment 5. Operative Treatment 6. Treatment
Treatment Alternatives for Pediatric Femoral Fractures
 Treatment Alternatives for Pediatric Femoral Fractures Gregory A. Schmale, MD Seattle Children's Hospital, USA, gregory.schmale@seattlechildrens.org version 2 I have no conflicts of interest to report
Treatment Alternatives for Pediatric Femoral Fractures Gregory A. Schmale, MD Seattle Children's Hospital, USA, gregory.schmale@seattlechildrens.org version 2 I have no conflicts of interest to report
Slipped capital femoral epiphysis
 : Diagnosis and Management DAVID PECK, MD, Providence Athletic Medicine, Novi, Michigan Slipped capital femoral epiphysis is the most common hip disorder in adolescents, and it has a prevalence of 10.8
: Diagnosis and Management DAVID PECK, MD, Providence Athletic Medicine, Novi, Michigan Slipped capital femoral epiphysis is the most common hip disorder in adolescents, and it has a prevalence of 10.8
Identify signs/symptoms/risk factors for: Understand issues of overtraining and signs of pediatric burnout
 Identify signs/symptoms/risk factors for: Little League Elbow Apophysitis including Osgood-Schlatter and Sever s Slipped Capital Femoral Epiphysis Understand issues of overtraining and signs of pediatric
Identify signs/symptoms/risk factors for: Little League Elbow Apophysitis including Osgood-Schlatter and Sever s Slipped Capital Femoral Epiphysis Understand issues of overtraining and signs of pediatric
Pediatric Rounds Topics and Objectives
 Pediatric Rounds Topics and Objectives Development Dysplasia Hip... 4... 4... 4... 5 Communicator... 5 Scholar... 5 Slipped Capital Femoral Epiphysis... 5... 5... 5... 6 Communicator... 6 Health Advocate...
Pediatric Rounds Topics and Objectives Development Dysplasia Hip... 4... 4... 4... 5 Communicator... 5 Scholar... 5 Slipped Capital Femoral Epiphysis... 5... 5... 5... 6 Communicator... 6 Health Advocate...
Limping Kids. SJRHEM Rounds - Dr David Lewis
 Limping Kids SJRHEM Rounds - Dr David Lewis October 11th 2014 Limping Kids A Case Base Rounds Interactive Links to further reading Posted to the website www.sjrhem.ca Case 1 - Age of Child An 18 month
Limping Kids SJRHEM Rounds - Dr David Lewis October 11th 2014 Limping Kids A Case Base Rounds Interactive Links to further reading Posted to the website www.sjrhem.ca Case 1 - Age of Child An 18 month
Will She Still Make the WNBA? Sports Injuries & Fractures
 Will She Still Make the WNBA? Sports Injuries & Fractures Aharon Z. Gladstein MD Pediatric Orthopaedic Surgery Pediatric Sports Medicine Sports Injuries Chronic (overuse) Acute Who can be treated in PCP
Will She Still Make the WNBA? Sports Injuries & Fractures Aharon Z. Gladstein MD Pediatric Orthopaedic Surgery Pediatric Sports Medicine Sports Injuries Chronic (overuse) Acute Who can be treated in PCP
The Painful Hip. Jennifer R Marks, MD
 The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011
 SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
DDH New Developments and Timeless Classics. DDH Define Treatment Group. (by age) DDH Imaging Choice in 6wk old Infant?
 DDH Imaging Choice in 6wk old Infant?") The 59 th Annual Edward T. Smith Orthopaedic Lectureship Emerging Concepts in the Surgical Management of the Hip: Deformity, Impingement and Fracture DDH New Developments and Timeless Classics Perry L.
The 59 th Annual Edward T. Smith Orthopaedic Lectureship Emerging Concepts in the Surgical Management of the Hip: Deformity, Impingement and Fracture DDH New Developments and Timeless Classics Perry L.
PEDIATRIC AND CONGENITAL IMAGING GUIDELINES MUSCULOSKELETAL 2009 MedSolutions, Inc
 MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not
MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not
LIMB LENGTH DISCREPANCIES
 LIMB LENGTH DISCREPANCIES Jill C Flanagan, MD OBJECTIVES Evaluate the patient with a possible limb length difference (LLD) Understand general treatment principles when managing limb length differences
LIMB LENGTH DISCREPANCIES Jill C Flanagan, MD OBJECTIVES Evaluate the patient with a possible limb length difference (LLD) Understand general treatment principles when managing limb length differences
OUTLINE FRACTURES OUTLINE. PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT. Mohammad Diab M.D. UCSF FRACTURE
 PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT FRACTURE Mohammad Diab M.D. UCSF FRACTURE articular displacement < 2 mm. accept FRACTURES routine imaging S-H 3 S-H 4 displacement > 2 mm. ORIF
PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT FRACTURE Mohammad Diab M.D. UCSF FRACTURE articular displacement < 2 mm. accept FRACTURES routine imaging S-H 3 S-H 4 displacement > 2 mm. ORIF
The Child with a Limp
 The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
Pediatric Orthopaedic Fellowship Curriculum
 Pediatric Orthopaedic Fellowship Curriculum The Fellowship Pediatric Orthopaedic Curriculum is designed for the fellow to spend three months each in four content areas. There are five content areas comprising
Pediatric Orthopaedic Fellowship Curriculum The Fellowship Pediatric Orthopaedic Curriculum is designed for the fellow to spend three months each in four content areas. There are five content areas comprising
Society for Pediatric Radiology 2015 Hands on Session. DDH: Pitfalls and Practical Tips
 Society for Pediatric Radiology 2015 Hands on Session DDH: Pitfalls and Practical Tips Michael A. DiPietro, M.D. John F. Holt Collegiate Professor of Radiology Professor of Pediatrics and Communicable
Society for Pediatric Radiology 2015 Hands on Session DDH: Pitfalls and Practical Tips Michael A. DiPietro, M.D. John F. Holt Collegiate Professor of Radiology Professor of Pediatrics and Communicable
Delayed fixation of an unstable Slipped capital femoral epiphysis: A case report and review of literature
 ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 14 Number 1 Delayed fixation of an unstable Slipped capital femoral epiphysis: A case report and review of literature S Lowndes, A Khanna, D
ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 14 Number 1 Delayed fixation of an unstable Slipped capital femoral epiphysis: A case report and review of literature S Lowndes, A Khanna, D
Labral Tears/FAI. Andrew Parker, MD
 Labral Tears/FAI Andrew Parker, MD Athletic Hip Injuries Incidence of hip injuries has increased dramatically over the last decade In part due to better recognition with improved imaging and arthroscopy,
Labral Tears/FAI Andrew Parker, MD Athletic Hip Injuries Incidence of hip injuries has increased dramatically over the last decade In part due to better recognition with improved imaging and arthroscopy,
Preserve or improve gait efficiency Early identification and stabilization or correction of lower extremity deformities
 ORTHOPEDICS Primary Outcomes Maintenance of a stable and balanced spine. Optimize pulmonary function. Avoid restrictive pulmonary disease. Optimize spinal growth. Avoid or facilitate healing of sacral/ischial
ORTHOPEDICS Primary Outcomes Maintenance of a stable and balanced spine. Optimize pulmonary function. Avoid restrictive pulmonary disease. Optimize spinal growth. Avoid or facilitate healing of sacral/ischial
CHAPTER 9. Summary and general discussion.
 CHAPTER 9 Summary and general discussion. Chapter 9 Chapter 1 This thesis describes different aspects of slipped capital femoral epiphysis (SCFE). Although rare, SCFE is the most common adolescent hip
CHAPTER 9 Summary and general discussion. Chapter 9 Chapter 1 This thesis describes different aspects of slipped capital femoral epiphysis (SCFE). Although rare, SCFE is the most common adolescent hip
GET HIP! CAPA 2015 Annual Conference WHAT IS HIP? HIP JOINT. Bradford H. Stiles, M.D., FAAFP
 GET HIP! Bradford H. Stiles, M.D., FAAFP WHAT IS HIP? HIP JOINT Synovial ball-and-socket joint Articulation between femoral head and acetabulum Acetabulum formed by the confluence of pelvis bones (ilium,
GET HIP! Bradford H. Stiles, M.D., FAAFP WHAT IS HIP? HIP JOINT Synovial ball-and-socket joint Articulation between femoral head and acetabulum Acetabulum formed by the confluence of pelvis bones (ilium,
No Disclosures. Topics. Pediatric ACL Tears
 Knee Injuries in Skeletally Immature Athletes No Disclosures Zachary Stinson, M.D. 2 Topics ACL Tears and Tibial Eminence Fractures Meniscus Injuries Discoid Meniscus Osteochondritis Dessicans Patellar
Knee Injuries in Skeletally Immature Athletes No Disclosures Zachary Stinson, M.D. 2 Topics ACL Tears and Tibial Eminence Fractures Meniscus Injuries Discoid Meniscus Osteochondritis Dessicans Patellar
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip
 of the Hip") A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot)
") 2015-2016 Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot) 1. Considerations in the Management of Pediatric Patients Kerry Armet 7 July 2015 Fluid
2015-2016 Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot) 1. Considerations in the Management of Pediatric Patients Kerry Armet 7 July 2015 Fluid
Degenerative arthritis of Hip Bone Bangalore. Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal
 Degenerative arthritis of Hip Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal Hip joint Classical Synovial joint Biomechanics of hip Force coincides with trabecular pattern Hip joint Acetabulum
Degenerative arthritis of Hip Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal Hip joint Classical Synovial joint Biomechanics of hip Force coincides with trabecular pattern Hip joint Acetabulum
Adult Hip Dysplasia David S. Feldman, MD
 Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Orthopaedic Hip (and Thigh) Referral Guidelines
 Referral Guidelines") Orthopaedic Hip (and Thigh) Referral Guidelines Austin Health Orthopaedic Clinic holds weekly multidisciplinary meetings to discuss and plan the treatment of patients with Orthopaedic and Fracture conditions.
Orthopaedic Hip (and Thigh) Referral Guidelines Austin Health Orthopaedic Clinic holds weekly multidisciplinary meetings to discuss and plan the treatment of patients with Orthopaedic and Fracture conditions.
PEDIATRIC AND CONGENITAL IMAGING GUIDELINES: MUSCULOSKELETAL 2011 MedSolutions, Inc
 MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not
MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital
 Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
APPROACH TO THE DIAGNOSIS OF GROIN PAIN. Alexandra Myers, D.O., M.S.H.S. February 22, 2018 OPSC Annual Convention
 APPROACH TO THE DIAGNOSIS OF GROIN PAIN Alexandra Myers, D.O., M.S.H.S. February 22, 2018 OPSC Annual Convention OVERVIEW Review the entities that may contribute to groin pain Discuss the approach to making
APPROACH TO THE DIAGNOSIS OF GROIN PAIN Alexandra Myers, D.O., M.S.H.S. February 22, 2018 OPSC Annual Convention OVERVIEW Review the entities that may contribute to groin pain Discuss the approach to making
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Sports Medicine in your office: What not to miss!
 Sports Medicine in your office: What not to miss! 2018 Primary Care Approach to Treating the Injured Athlete May 4, 2018 John H. Wilckens, MD Associate Professor, Dept of Orthopaedic Surgery Disclosures
Sports Medicine in your office: What not to miss! 2018 Primary Care Approach to Treating the Injured Athlete May 4, 2018 John H. Wilckens, MD Associate Professor, Dept of Orthopaedic Surgery Disclosures
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE
 PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
The Surgical Management of Rickets & Osteogenesis Imperfecta
 The Surgical Management of Rickets & Osteogenesis Imperfecta Dr Greg Firth Chris Hani Baragwanath Academic Hospital Department of Orthopaedics University of the Witwatersrand Rickets Inadequate mineralization
The Surgical Management of Rickets & Osteogenesis Imperfecta Dr Greg Firth Chris Hani Baragwanath Academic Hospital Department of Orthopaedics University of the Witwatersrand Rickets Inadequate mineralization
Other Upper Extremity Trauma. Inje University Sanggye Paik Hospital Yong-Woon Shin
 Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
ORTHOPEDICS AND TRAUMATOLOGY TRAINING PROGRAM
 ORTHOPEDICS AND TRAUMATOLOGY TRAINING PROGRAM (3 Weeks) YEDİTEPE UNIVERSITY HOSPITAL Head of the Department of Orthopedics and Traumatology: Faik Altıntaş, MD Prof. Uğur Şaylı, MD Prof. Turhan Özler, MD
ORTHOPEDICS AND TRAUMATOLOGY TRAINING PROGRAM (3 Weeks) YEDİTEPE UNIVERSITY HOSPITAL Head of the Department of Orthopedics and Traumatology: Faik Altıntaş, MD Prof. Uğur Şaylı, MD Prof. Turhan Özler, MD
DDH: Pathology Diagnosis, and Treatment before Walking Age
 DDH: Pathology Diagnosis, and Treatment before Walking Age 영남의대 김세동 Ⅰ. Terminology of hip dysplasia a. Congenital dysplasia or dislocation of the hip(cdh): Hippocrates Congenital -Existing at Birth but
DDH: Pathology Diagnosis, and Treatment before Walking Age 영남의대 김세동 Ⅰ. Terminology of hip dysplasia a. Congenital dysplasia or dislocation of the hip(cdh): Hippocrates Congenital -Existing at Birth but
Evaluation of the Hip and Knee
 Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Treatment of DDH before Walking Age 고려대학안암병원
 Treatment of DDH before Walking Age 이 순혁 고려대학안암병원 Subluxated Hip Always to deg. hip The more, the earlier Even in 2nd Decade Dysplastic Hip Eventually to osteoarthritis but later Etiology of end-stage
Treatment of DDH before Walking Age 이 순혁 고려대학안암병원 Subluxated Hip Always to deg. hip The more, the earlier Even in 2nd Decade Dysplastic Hip Eventually to osteoarthritis but later Etiology of end-stage
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
A free online interactive information resource for clinicians.
 A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
hip pathology w mccormick 2017 mccormickortho.com
 hip pathology w mccormick 2017 mccormickortho.com overview classification common hip pathologies FAI GT pain snapping workup treatments sample cases rehabilitation outcomes/complications hip pathology
hip pathology w mccormick 2017 mccormickortho.com overview classification common hip pathologies FAI GT pain snapping workup treatments sample cases rehabilitation outcomes/complications hip pathology
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS. Paediatric MS History o Reason for referral o Past history
 LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
A Patient s Guide to Perthes Disease of the Hip
 A Patient s Guide to Perthes Disease of the Hip 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Perthes Disease of the Hip 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety
Case Report Valgus Slipped Capital Femoral Epiphysis in Patient with Hypopituitarism
 Hindawi Case eports in Orthopedics Volume 2017, Article ID 8981250, 4 pages https://doi.org/10.1155/2017/8981250 Case eport Valgus Slipped Capital Femoral Epiphysis in Patient with Hypopituitarism Yoshihiro
Hindawi Case eports in Orthopedics Volume 2017, Article ID 8981250, 4 pages https://doi.org/10.1155/2017/8981250 Case eport Valgus Slipped Capital Femoral Epiphysis in Patient with Hypopituitarism Yoshihiro
Orthopedics. 1. GOAL: Understand the pediatrician's role in preventing and screening for
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Orthopedics 1. GOAL: Understand the pediatrician's role in preventing and screening for orthopedic injury, disease and dysfunction.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Orthopedics 1. GOAL: Understand the pediatrician's role in preventing and screening for orthopedic injury, disease and dysfunction.
Orthopedics. Michael Conklin, MD, Chair Sam Rosenfeld, MD Chanka Nanyakara, MD Shyam Kishan, MD
 Orthopedics Michael Conklin, MD, Chair Sam Rosenfeld, MD Chanka Nanyakara, MD Shyam Kishan, MD Outcomes Primary Outcomes Maintenance of a stable and balanced spine. Optimize pulmonary function. Avoid restrictive
Orthopedics Michael Conklin, MD, Chair Sam Rosenfeld, MD Chanka Nanyakara, MD Shyam Kishan, MD Outcomes Primary Outcomes Maintenance of a stable and balanced spine. Optimize pulmonary function. Avoid restrictive
Non-Arthroplasty Hip Surgery. Javad Parvizi MD FRCS Professor of Orthopaedic Surgery
 Non-Arthroplasty Hip Surgery Javad Parvizi MD FRCS Professor of Orthopaedic Surgery Subcapital reduction osteotomy Relative lengthening of femoral neck (Perthes) AVN surgery Femoral osteotomy Trap door
Non-Arthroplasty Hip Surgery Javad Parvizi MD FRCS Professor of Orthopaedic Surgery Subcapital reduction osteotomy Relative lengthening of femoral neck (Perthes) AVN surgery Femoral osteotomy Trap door
Apply this knowledge into proper management strategies and referrals
 1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
1/10/2017 PEDIATRIC LIMP: BOARD REVIEW GOALS & OBJECTIVES RELEVANCE DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017
 PEDIATRIC LIMP: BOARD REVIEW DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017 RELEVANCE AOBFP EXAM BLUEPRINT: ORTHO 5% PEDS 4% ADOLESCENTS 4% SPORTS 3 % http://static3.businessinsider.com/image/52545f89eab8ea62534aa515-1200-375/brain%20golfing.jpg
PEDIATRIC LIMP: BOARD REVIEW DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017 RELEVANCE AOBFP EXAM BLUEPRINT: ORTHO 5% PEDS 4% ADOLESCENTS 4% SPORTS 3 % http://static3.businessinsider.com/image/52545f89eab8ea62534aa515-1200-375/brain%20golfing.jpg
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA. Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009
 EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
University of South Florida
 University of South Florida Pediatric Orthopaedics PGY 4 Competency Based Goals & Objectives Competency 1- Patient Care: Provide family centered patient care that is developmentally and age appropriate,
University of South Florida Pediatric Orthopaedics PGY 4 Competency Based Goals & Objectives Competency 1- Patient Care: Provide family centered patient care that is developmentally and age appropriate,
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
PEDIATRIC HIP DISORDERS VINAY NAROTAM, MD ASSISTANT PROFESSOR UNIVERSITY OF NORTH CAROLINA SCHOOL OF MEDICINE DEPARTMENT OF ORTHOPAEDICS
 1 PEDIATRIC HIP DISORDERS VINAY NAROTAM, MD ASSISTANT PROFESSOR UNIVERSITY OF NORTH CAROLINA SCHOOL OF MEDICINE DEPARTMENT OF ORTHOPAEDICS Disclosures 2 I have no relevant financial relationships with
1 PEDIATRIC HIP DISORDERS VINAY NAROTAM, MD ASSISTANT PROFESSOR UNIVERSITY OF NORTH CAROLINA SCHOOL OF MEDICINE DEPARTMENT OF ORTHOPAEDICS Disclosures 2 I have no relevant financial relationships with