Case Presentations The Child with a Limp
|
|
|
- Tyrone Wilkerson
- 5 years ago
- Views:
Transcription
1 Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState Hershey Medical Center
2 Case 1: 11 year old girl Limping intermittently for 9 weeks c/o Right knee pain for 3 weeks



3
4 What s the most likely diagnosis? What s the next step?
5 Slipped Capital Femoral Epiphysis The most common hip disorder in adolescence incidence is increasing Proximal femoral physis weakens: epiphysis glides posteriorly & inferiorly, femoral neck rotates externally, glides upward Griffith M.J.: Ann R Coll Surg Engl 58:34, 1976


6 Anatomy of SCFE Anterior Posterior Axial
7 Slipped Capital Femoral Epiphysis Incidence: ~ 1 per 10,000 in North East U.S. Mean age: Boys 13 yrs; Girls 11 ½ yrs now trending to younger age Weight: 60% are >90th percentile Relative racial frequency: Polynesian 4.5 > Black 2.2 > White 1.0 > Indonesian-Malay 0.5 > Indo-Mediterranean 0.1 Seasonal variation: north of 40 N, more frequent in summer Loder RT, et al. Clin Orthop
8 Can you name 3 conditions for which you should have increased vigilance for SCFE? Hypothyroidism Renal failure Patient treated with HGH
9 Clinical Presentation Misdiagnosis is frequent: muscle strain Limping, often painless initially Pain in groin area with activity Pain at the Knee or Lower Thigh 23% Matava et al. J Pediatr Orthop 1999 Clinical examination is key: Observe the child s gait Check hip rotation in extension & flexion on exam table


10 Rules are meant to be broken 13 yo boy, Left Hip pain
11 SCFE Radiograms Mild slips can be missed Need a good Lateral XRay, frogleg view preferable AP: look for physeal widening & irregularity, Klein s line, remodelling of femoral neck inferiorly


12 Pinkowsky G, Hennrikus W. J Pediatr Orthop 2013


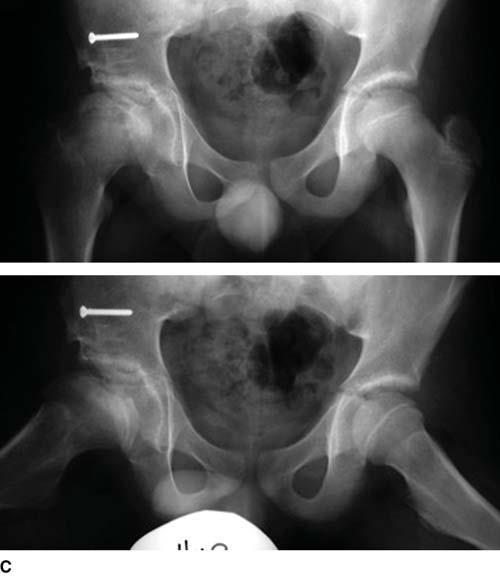
13 AP & Frogleg Bilateral Hips / Pelvis PW, male age 12y; c/o left hip pain

14 Bilateral SCFE Incidence varies by study, age, race, severity, measurement: 18% - 63% Sequential: mean is 1 yr after 1 st slip, up to 56 mos later More frequently Asymptomatic Increased Risk: Age at initial presentation 10 yrs or younger endocrine abnormality unstable SCFE
15 Natural History of Untreated SCFE 108 pts at average 41 yrs (r yr): 1/5 had good function, 2/5 poor, 2/5 moderate results declined with age Parsch K. J Pediatr Orthop(B) 1999
16 Natural History of Untreated SCFE is Poor Carney & Weinstein 1996 At least 17% displace All moderate & severe slips had developed degenerative joint disease; 5 of 14 had poor function Ordeberg G et al CORR 191: Severe slips: 28 of 35 had arthrosis
17 Natural History of Treated SCFE 41 yr follow-up: various treatments for 124 pts Acute slips: fair to poor outcomes Moderate & severe slips deteriorated In situ pinning: good to excellent 39 yr follow-up: 51 patients / 60 chronic SCFEs treated w. in situ fixation: 20 hips poor, 40 hips good Carney BT et al JBJS(A) Terjesen 2017 J Child Orthop


18


19 J.G., male, 14 yo


20 21 yr o male 8 years post pinning
21 Acute / Unstable SCFE Abrupt onset of severe pain, inability to weight bear, usually arrive by ambulance Epiphysis is mobile Exam: typical position, hip external rotation, abduction Plain Radiograms: usually gross displacement Treatment: controversial Osteonecrosis is common Outcomes: generally poor medium to long-term
 Kallio et al")
 Armstrong, Schwend 2000: 43%")
22 Acute / Unstable SCFE Rate of AVN when reduction occurred Loder et al 1993: 47% (14/30) Kallio et al 1995: 3% (1/34) Kennedy et al 2001: 15% (4/27) Rattey et al 1996: 15% (4/26) Armstrong, Schwend 2000: 43% (13/30)
23 SCFE Summary Stable slips typically present to Pediatrician first Occur during pubertal growth spurt Beware of predisposing conditions, atypical age / weight / gender Limp with or without pain at hip / groin, knee or thigh Diagnosis: history, simple physical exam Xrays: AP & Frogleg bilateral hips MRI not necessary
24 Case 2 6 ½ year old boy limping for 6 weeks Limp is intermittent, worse with activity No history of trauma ADHD Pain at inner aspect of thigh / knee
25
26 Physical Examination Short statured Walks with a lurching gait to the right Right hip is stiff, some pain with internal rotation

27 XRay
28 Legg-Calve Perthes Disease Incidence Ranges from 1:1200 to 1:12,500 Usually presents between 4 and 8 years, however reported in ages 2 to 12 years Boys: Girls = 4 to 5: 1 More common in Caucasians, Asians Bilateral in 10% of cases Can be familial May be related to disorders of thrombophilia


29
30 Disease Course Initially, avascular episodes are silent As bone of femoral epiphysis dies, it is revascularized, Osteoclasts remove dead bone while osteoblasts lay down new bone on dead trabeculae (creeping substitution). During this phase, femoral epiphysis is weak Fragmentation and collapse may occur causing geometric flattening and deformity
31 Legg Calve Perthes Disease: a long disease course Fragmentation: 1 year Reossification: 3 to 5 years remodeling and improvement of femoral head shape may occur until maturity Long term prognosis depends on shape of head at maturity


32 Radiographic Progression
33 LCPD: Clinical Presentation - History Usually between ages 4 and 8 years Boys >> Girls ADHD Small stature c/o limp - varying duration Pain usually activity related and localized to groin, anterior thigh, or knee at-risk factors age > 6 yrs; obesity; female; marked stiffness
34 Clinical Presentation Physical Exam Antalgic or Trendelenburg gait May have hip flexion contracture of degrees Limited motion, notably decreased Internal Rotation and Abduction May have leg length inequality Atrophy of thigh, calf, or buttock musculature
35 Differential Diagnosis Toxic synovitis Infection / septic arthritis Juvenile rheumatoid arthritis Tumor Sickle cell, thalassemia, hemophilia, ITP, etc. Leukemia In bilateral cases: skeletal dysplasia (spondyloepiphyseal dysplasia), endocrinopathies, some genetic syndromes.

36 LCPD: Diagnosis height, weight (typically short-statured) Gait Hip ROM Trendelenburg test; measure limb lengths Laboratory studies usually not needed
37 LCPD: Imaging AP and frog-lateral views both are necessary Determine extent of femoral epiphysis involvement Femoral epiphysis may collapse and extrude from the acetabulum Determine femoral head coverage & containment on frogleg view MRI may be useful in select cases, not typically the first step


38 AP and Frog-Lateral

39 LCPD Imaging MRI may be useful for diagnosis in difficult cases As a prognostic tool - not clear

40 Lateral Pillar Classification Femoral head can collapse over time Extent of collapse varies with severity of osteonecrosis Shape of the femoral head at maturity determines outcome, longevity of the hip A B C
41 Prognosis & Treatment Age at onset is a main determinant of outome < 6 yrs: 80 % do well Age 6 to 8: surgery may help some Age > 8 yrs: surgery often helpful Physical Therapy: not helpful Bracing: in selected patients Surgery: In selected children Soft tissue releases to improve Range of motion, Bone operations to improve coverage

42
43 Case 3 1 yr 5 month old girl Just started walking Walking on tiptoe on right No pain No h/o trauma No fever
44 Physical Examination

45
46 Developmental Dysplasia of the Hip Is this the Pediatrician s fault?
47 Developmental Dysplasia of the Hip (DDH) A Group of disorders of the hip in which the head of the femur is unstable or incongruous in relation to the acetabulum. Untreated hip dysplasia results in degenerative arthrosis; age at onset varies: subluxated hips develop rapid, severe OA in young adulthood
48 Developmental Dysplasia of the Hip Acetabular dysplasia is characterized by an immature, shallow acetabulum. Normal acetabular development is dependent upon concentric reduction of the femoral head But - Dysplasia may sometimes exist without associated instability: primary acetabular dysplasia may present later, even in adulthood Severity of dysplasia correlates with age of onset of symptoms and disability
49 Screening for DDH Typically performed by primary care providers Primary screening tool is physical exam & history The screening tool is relatively reliable, and is cost effective Early treatment can prevent disability and degenerative arthrosis of the hip, i.e., prevents significant disease burden
50 Epidemiology Incidence: 1 in 100 live births have hip instability, 1 per 1000 have a dislocation Left 3 X > Right (?) due to fetal position Females : males = 4.6:1 Family History: If 1 parent & 1 sib have DDH then 36% will have it Race: Native American > White > Black However, The Majority of DDH patients Have No Risk Factors 1 in 5,000 children have DDH that presents late, like this one
51 Etiology Mechanical: Breech Maternal hormone-induced ligamentous laxity Genetics role remains unclear
52 Risk factors for DDH Vertex: Girls: 2/1000; Boys 0.5/ 1000 First born: effect is small Positive family history: RR = 1.7; 3.2 % girls Breech especially Frank breech Female Breech: 12 % have DDH Associated packaging disorders
53 What to do Screening at Newborn and at Periodic examinations until age 1 year After age 1, if clinically indicated Refer to Orthopedic surgery if exam positive 2 week exam suspicious : U/S at 1 month or referral Breech: U/S at 6 weeks or Radiogram at 4-6 months Suspicious, up to 12 mos: refer, U/S or XRay
54 Diagnosis: age 3 months or less Ortolani test Elevation/abduction produces relocation clunk of a dislocated hip (not a click) Barlow test: (no longer considered reliable) Adduction/depression dislocates or subluxates a dislocatable or subluxable hip Ultrasound : sensitivity / specificity better at 1 month of age than as newborn; not recommended if patient > 5 months old; controversial HIP XRAY
55 Ortolani

56 Barlow
57 Diagnosis: age 3 to 12 months Ortolani/Barlow become unreliable ** Limitation of Abduction ** Foreshortening of femur (Galeazzi sign) Beware bilateral DDH

58 Clinical Signs Assymmetric skin folds: not always reliable Hip abduction can be close to symmetric Worst case scenario: bilateral DDH & loose ligaments: present with waddling gait & hyperlordosis
59 Age 12 months and older Delayed walking Toe walking if unilateral Limping Limb length discrepancy
 and lateral to perpendicular")
60 AP Pelvis Dislocated head above horizontal line (Hilgenreiner) and lateral to perpendicular (Perkins)
61 Treatment: 6 to 18 months or if failed nonoperative measures Closed reduction & Spica casting Arthrography is often useful Adductor tenotomy Open reduction as necessary Spica for 4 months with cast changes X-rays or CT scans or MRI to check reduction

62 Open Reduction & Salter Osteotomy: one of the most successful operations: % good to excellent results at 45 years follow up!
63 DDH follow-up There is a wide spectrum of disease Prognosis is good for hips treated early but Many patients can develop abnormal hips during late childhood or adolescence Contralateral normal hip can develop dysplasia up to age 12 years old Orthopedic follow-up throughout growing years is recommended

64 Summary DDH Routine physical examination by pediatrician will find many but not all cases 1 in 5000 present at 12 mos or older Shaw B, Segal L. Clinical Report: Evaluation and Referral for DDH in Infants. Pediatrics Dec Best Practices Examine the hips at periodic visits up to 6 9 months of age Consider ultrasound to clarify suspicious findings on physical examination after 3 to 4 weeks of age or to detect clinically silent DDH in the high-risk infant from 6 weeks to 4 to 6 months of age
65 Thank You 65
Childhood hip conditions. Belen Carsi Paediatric Orthopaedic Consultant
 Childhood hip conditions Belen Carsi Paediatric Orthopaedic Consultant Developmental Dysplasia of the Hip Legg-Calve-Perthes disease Slipped Capital femoral epiphysis Limp Arthritis Developmental Dysplasia
Childhood hip conditions Belen Carsi Paediatric Orthopaedic Consultant Developmental Dysplasia of the Hip Legg-Calve-Perthes disease Slipped Capital femoral epiphysis Limp Arthritis Developmental Dysplasia
Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip
 Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip *This guideline was developed from the American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental
Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip *This guideline was developed from the American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental
Hip Dysplasia David S. Feldman, MD
 Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
I have no financial relationships related to disclose
 Evaluation of a child with a limp / Slipped Capital Femoral Epiphysis (SCFE) Lee S. Segal, MD Chief, Division of Pediatric Orthopedics American Family Children s Hospital Department of Orthopedics and
Evaluation of a child with a limp / Slipped Capital Femoral Epiphysis (SCFE) Lee S. Segal, MD Chief, Division of Pediatric Orthopedics American Family Children s Hospital Department of Orthopedics and
Non-inflammatory joint pain
 Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD. November 4, 2017
 Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Friday Teaching. Bones
 Friday Teaching Bones Regarding slipped femoral capital epiphysis It represents Salter Harris type V injury 20% are bilateral There is slight widening of the joint space Slip is typically posteromedial
Friday Teaching Bones Regarding slipped femoral capital epiphysis It represents Salter Harris type V injury 20% are bilateral There is slight widening of the joint space Slip is typically posteromedial
DDH. Abnormal hip development Traditionally CDH (congenital dysplasia of the hip) Today DDH(developmental dysplasia of the hip)
 Today DDH(developmental dysplasia of the hip)") DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
Slipped Capital Femoral Epiphysis
 Slipped Capital Femoral Epiphysis Nicholas D. Fletcher, MD Assistant Professor of Orthopaedics and Scoliosis Emory University Orthopaedics Emory Orthopaedics Center for Hip Preservation What is it? Misnomer
Slipped Capital Femoral Epiphysis Nicholas D. Fletcher, MD Assistant Professor of Orthopaedics and Scoliosis Emory University Orthopaedics Emory Orthopaedics Center for Hip Preservation What is it? Misnomer
The Limping Child: Differential Diagnosis
 The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
Bilateral hip pain with right proximal femoral lesion
 Bilateral hip pain with right proximal femoral lesion Legg-Calve-Perthes Idiopathic osteonecrosis of the femoral head epiphysis during childhood First described by Arthur Thorton Legg in 1909 and published
Bilateral hip pain with right proximal femoral lesion Legg-Calve-Perthes Idiopathic osteonecrosis of the femoral head epiphysis during childhood First described by Arthur Thorton Legg in 1909 and published
Hip Biomechanics and Osteotomies
 Hip Biomechanics and Osteotomies Organization Introduction Hip Biomechanics Principles of Osteotomy Femoral Osteotomies Pelvic Osteotomies Summary Inroduction Osteoarthritis is very prevalent Primary OA
Hip Biomechanics and Osteotomies Organization Introduction Hip Biomechanics Principles of Osteotomy Femoral Osteotomies Pelvic Osteotomies Summary Inroduction Osteoarthritis is very prevalent Primary OA
Case Developmental dysplasia of hip
 Case 13303 Developmental dysplasia of hip Hidayatullah Hamidi, Sahar Maroof French medical institute for children, Kabul, Afghanistan Email: Hedayatullah.hamidi@gmail.com Maroofsahar1@gmail.com French
Case 13303 Developmental dysplasia of hip Hidayatullah Hamidi, Sahar Maroof French medical institute for children, Kabul, Afghanistan Email: Hedayatullah.hamidi@gmail.com Maroofsahar1@gmail.com French
A 4 year old with hip pain: Legg-Calvé-Perthes Disease
 A 4 year old with hip pain: Legg-Calvé-Perthes Disease Cyndie Seraphin Harvard Medical School Year III Our Patient A 4 year-old boy is complaining of severe L hip pain. The differential diagnosis of acute
A 4 year old with hip pain: Legg-Calvé-Perthes Disease Cyndie Seraphin Harvard Medical School Year III Our Patient A 4 year-old boy is complaining of severe L hip pain. The differential diagnosis of acute
Society for Pediatric Radiology 2015 Hands on Session. DDH: Pitfalls and Practical Tips
 Society for Pediatric Radiology 2015 Hands on Session DDH: Pitfalls and Practical Tips Michael A. DiPietro, M.D. John F. Holt Collegiate Professor of Radiology Professor of Pediatrics and Communicable
Society for Pediatric Radiology 2015 Hands on Session DDH: Pitfalls and Practical Tips Michael A. DiPietro, M.D. John F. Holt Collegiate Professor of Radiology Professor of Pediatrics and Communicable
The Hip from Cradle to Grave. Haemish Crawford Ascot Hospital Starship Children s Hospital
 The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
DDH: Pathology Diagnosis, and Treatment before Walking Age
 DDH: Pathology Diagnosis, and Treatment before Walking Age 영남의대 김세동 Ⅰ. Terminology of hip dysplasia a. Congenital dysplasia or dislocation of the hip(cdh): Hippocrates Congenital -Existing at Birth but
DDH: Pathology Diagnosis, and Treatment before Walking Age 영남의대 김세동 Ⅰ. Terminology of hip dysplasia a. Congenital dysplasia or dislocation of the hip(cdh): Hippocrates Congenital -Existing at Birth but
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
Peggers Super Summaries: Paediatric Hip
 EMBRYOLOGY Development o Mesenchymal stem cells cartilage blood supply bone Dates o 6/40 Limb development o 8-11/40 hip development (acetabulum and hip formed from one bone splitting by apoptosis) o 16/40
EMBRYOLOGY Development o Mesenchymal stem cells cartilage blood supply bone Dates o 6/40 Limb development o 8-11/40 hip development (acetabulum and hip formed from one bone splitting by apoptosis) o 16/40
The Hip Baby?? Baby Hippie??
 In Need of a Title? The Hip Baby?? Baby Hippie?? Review of Developmental Dysplasia of the Hip in the Newborn OCR Symposium 2018 Ryan L. Hartman, MD Specialty: Pediatric and Sports Orthopaedics 23 month
In Need of a Title? The Hip Baby?? Baby Hippie?? Review of Developmental Dysplasia of the Hip in the Newborn OCR Symposium 2018 Ryan L. Hartman, MD Specialty: Pediatric and Sports Orthopaedics 23 month
Slipped Capital Femoral Epiphysis (SCFE)
") Slipped Capital Femoral Epiphysis (SCFE) DR MUMTAZ HUSSAIN Senior Registrar DR ABDUL LATIF SAMI (Associate Professor) Head of Department Pediatric Orthopedics Introduction and Definition Epidemiology and
Slipped Capital Femoral Epiphysis (SCFE) DR MUMTAZ HUSSAIN Senior Registrar DR ABDUL LATIF SAMI (Associate Professor) Head of Department Pediatric Orthopedics Introduction and Definition Epidemiology and
What is a Hip Dysplasia?
 What is a Hip Dysplasia? Hip dysplasia, developmental dysplasia of the hip (DDH)[1] or congenital dysplasia of the hip (CDH)[2] is a congenital or acquired deformation or misalignment of the hip joint.
What is a Hip Dysplasia? Hip dysplasia, developmental dysplasia of the hip (DDH)[1] or congenital dysplasia of the hip (CDH)[2] is a congenital or acquired deformation or misalignment of the hip joint.
Developmental Dysplasia of the Hip
 1 Developmental Dysplasia of the Hip Developmental dysplasia of the hip (DDH) or otherwise known as congenital dislocation of the hip (CDH) is a developmental (ongoing) process, which can often go undetected
1 Developmental Dysplasia of the Hip Developmental dysplasia of the hip (DDH) or otherwise known as congenital dislocation of the hip (CDH) is a developmental (ongoing) process, which can often go undetected
Pediatric Orthopedics: ``To Refer or Not to Refer``
 Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
SC FE. Slipped Capital Femoral Epiphysis SPR
 SC FE Slipped Capital Femoral Epiphysis SPR Disclosures Lecture specific-nothing to disclose. Dr. Taragin is a member of the medical advisory board of Carestream Health. SAM Goal SCFE = SCIFI PRESENTATION
SC FE Slipped Capital Femoral Epiphysis SPR Disclosures Lecture specific-nothing to disclose. Dr. Taragin is a member of the medical advisory board of Carestream Health. SAM Goal SCFE = SCIFI PRESENTATION
Stephanie W. Mayer, MD. Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado
 Stephanie W. Mayer, MD Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado University of Colorado Sports Medicine Assistant Team Physician, Colorado Avalanche
Stephanie W. Mayer, MD Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado University of Colorado Sports Medicine Assistant Team Physician, Colorado Avalanche
The Limping Child. Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester
 The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
Successful Pavlik treatment in late-diagnosed developmental dysplasia of the hip
 International Orthopaedics (SICOT) (2012) 36:1661 1668 DOI 10.1007/s00264-012-1587-5 ORIGINAL PAPER Successful Pavlik treatment in late-diagnosed developmental dysplasia of the hip Michiel A. J. van de
International Orthopaedics (SICOT) (2012) 36:1661 1668 DOI 10.1007/s00264-012-1587-5 ORIGINAL PAPER Successful Pavlik treatment in late-diagnosed developmental dysplasia of the hip Michiel A. J. van de
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016
 Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌
 & Idiopathic 이대목동병원 윤여헌") Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌 Children s hip disorders Congenital & developmental disorders Developmental hip dysplasia (dislocation) of the hip Developmental
Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌 Children s hip disorders Congenital & developmental disorders Developmental hip dysplasia (dislocation) of the hip Developmental
Effects of Immobilization. N24 Pedi Musculoskeletal Spring 2012, Week 14. Cabrillo ADN/C. Madsen RN, MSN 1. Physical effects on other systems
 Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
Slipped capital femoral epiphysis
 : Diagnosis and Management DAVID PECK, MD, Providence Athletic Medicine, Novi, Michigan Slipped capital femoral epiphysis is the most common hip disorder in adolescents, and it has a prevalence of 10.8
: Diagnosis and Management DAVID PECK, MD, Providence Athletic Medicine, Novi, Michigan Slipped capital femoral epiphysis is the most common hip disorder in adolescents, and it has a prevalence of 10.8
Adult Hip Dysplasia David S. Feldman, MD
 Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort
 Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort Disclosures No disclosures relevant to this topic Objectives Evaluate and recognize common hip pathology
Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort Disclosures No disclosures relevant to this topic Objectives Evaluate and recognize common hip pathology
Four weeks of Intrauterine life
 Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
The Child With a Limp
 KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
Acquired Hip Disorders in Children and Adolescents. Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA
 Acquired Hip Disorders in Children and Adolescents Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA Don t Miss Acquired Hip Disorders SCFE Posterior Hip Dislocation Osteoid
Acquired Hip Disorders in Children and Adolescents Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA Don t Miss Acquired Hip Disorders SCFE Posterior Hip Dislocation Osteoid
Lower Extremity Alignment: Genu Varum / Valgum
 Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
1. Discuss some common pediatric problems seen in the clinic. Diagnosis Clinical examination (at birth and subsequent well-baby examinations)
") 1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
Developmental Dysplasia of the Hip
 Developmental Dysplasia of the Hip Abnormal relationship of femoral head to the acetabulum Formerly known as congenital hip dislocation Believed to be developmental Most dislocations are evident at births
Developmental Dysplasia of the Hip Abnormal relationship of femoral head to the acetabulum Formerly known as congenital hip dislocation Believed to be developmental Most dislocations are evident at births
Femoroacetabular impingement in adolescents and young adults an update
 U N I V E R S I T E T E T I B E R G E N Femoroacetabular impingement in adolescents and young adults an update Lene Bjerke Laborie, MD, PhD Paediatric Radiology Department, Haukeland University Hospital
U N I V E R S I T E T E T I B E R G E N Femoroacetabular impingement in adolescents and young adults an update Lene Bjerke Laborie, MD, PhD Paediatric Radiology Department, Haukeland University Hospital
Treatment of DDH before Walking Age 고려대학안암병원
 Treatment of DDH before Walking Age 이 순혁 고려대학안암병원 Subluxated Hip Always to deg. hip The more, the earlier Even in 2nd Decade Dysplastic Hip Eventually to osteoarthritis but later Etiology of end-stage
Treatment of DDH before Walking Age 이 순혁 고려대학안암병원 Subluxated Hip Always to deg. hip The more, the earlier Even in 2nd Decade Dysplastic Hip Eventually to osteoarthritis but later Etiology of end-stage
7/1/2012. Repetitive valgus stresses cause microfractures in the apophyseal cartilage (weak link) Common in year olds
 Common in year olds") 1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
A Patient s Guide to Perthes Disease of the Hip
 A Patient s Guide to Perthes Disease of the Hip 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Perthes Disease of the Hip 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Transient Synovitis of the Hip in Children
 A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
Ultrasound Evaluation of Pavlik Harness in Treatment of Infants with Developmental Dysplasia of the Hip: Prone Axial Approach to Harness in Situ
 Ultrasound Evaluation of Pavlik Harness in Treatment of Infants with Developmental Dysplasia of the Hip: Prone Axial Approach to Harness in Situ C Fernández, MD; M Guasp, MD; J Gómez Fernández-Montes,
Ultrasound Evaluation of Pavlik Harness in Treatment of Infants with Developmental Dysplasia of the Hip: Prone Axial Approach to Harness in Situ C Fernández, MD; M Guasp, MD; J Gómez Fernández-Montes,
COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL
 COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL Clifford L. Craig, M.D. M2 Musculoskeletal Fall 2008 I. ANGULAR AND TORSIONAL DEFORMITIES OF THE LOWER LIMBS Examination Relaxed,
COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL Clifford L. Craig, M.D. M2 Musculoskeletal Fall 2008 I. ANGULAR AND TORSIONAL DEFORMITIES OF THE LOWER LIMBS Examination Relaxed,
Combined Pelvic Osteotomy in the Treatment of Both Deformed and Dysplastic Acetabulum Three Years Prospective Study
 Prague Medical Report / Vol. 106 (2005) No. 2, p. 159 166 159) Combined Pelvic Osteotomy in the Treatment of Both Deformed and Dysplastic Acetabulum Three Years Prospective Study Al Razi Orthopedic Hospital,
Prague Medical Report / Vol. 106 (2005) No. 2, p. 159 166 159) Combined Pelvic Osteotomy in the Treatment of Both Deformed and Dysplastic Acetabulum Three Years Prospective Study Al Razi Orthopedic Hospital,
Subluxation of the hip presenting for the first time
 The treatment of subluxation of the hip in children over the age of four years John A. Fixsen, Patrick L. S. Li From the Hospitals for Sick Children, Great Ormond Street, London, England Subluxation of
The treatment of subluxation of the hip in children over the age of four years John A. Fixsen, Patrick L. S. Li From the Hospitals for Sick Children, Great Ormond Street, London, England Subluxation of
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty. Faculty Disclosures. Objectives 11/17/2017
 Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
PEDIATRIC HIP DISORDERS VINAY NAROTAM, MD ASSISTANT PROFESSOR UNIVERSITY OF NORTH CAROLINA SCHOOL OF MEDICINE DEPARTMENT OF ORTHOPAEDICS
 1 PEDIATRIC HIP DISORDERS VINAY NAROTAM, MD ASSISTANT PROFESSOR UNIVERSITY OF NORTH CAROLINA SCHOOL OF MEDICINE DEPARTMENT OF ORTHOPAEDICS Disclosures 2 I have no relevant financial relationships with
1 PEDIATRIC HIP DISORDERS VINAY NAROTAM, MD ASSISTANT PROFESSOR UNIVERSITY OF NORTH CAROLINA SCHOOL OF MEDICINE DEPARTMENT OF ORTHOPAEDICS Disclosures 2 I have no relevant financial relationships with
ORDER OF VERBAL EXAMS
 ORDER OF VERBAL EXAMS The students are able to register for the exam on the NEPTUN system. The students pick two titles, from the title list available at the beginning of the Semester. This list can be
ORDER OF VERBAL EXAMS The students are able to register for the exam on the NEPTUN system. The students pick two titles, from the title list available at the beginning of the Semester. This list can be
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh
 Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
A Patient s Guide to Limping in Children
 A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
Hip Joint DX 612 Orthopedics and Neurology
 Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Anatomy. Hip Joint DX 612 Orthopedics and Neurology. Hip ROM. Palpation
 Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Radiological Sequelae of developmental dysplasia of the hip: a Review
 Radiological Sequelae of developmental dysplasia of the hip: a Review Poster No.: P-0037 Congress: ESSR 2012 Type: Scientific Exhibit Authors: S. G. Flanagan, J. Sarkodieh, K. Mcdonald, M. Ramachandran,
Radiological Sequelae of developmental dysplasia of the hip: a Review Poster No.: P-0037 Congress: ESSR 2012 Type: Scientific Exhibit Authors: S. G. Flanagan, J. Sarkodieh, K. Mcdonald, M. Ramachandran,
Case series - Slipped capital femoral epiphysis in three members of same family as an unusual presentationn
 Slipped capital femoral epiphysis in three members of same family Case Series ISSN: 2394-0026 (P) Case series - Slipped capital femoral epiphysis in three members of same family as an unusual presentationn
Slipped capital femoral epiphysis in three members of same family Case Series ISSN: 2394-0026 (P) Case series - Slipped capital femoral epiphysis in three members of same family as an unusual presentationn
Femoral Acetabular Impingement 10/22/2016
 Femoral Acetabular Impingement 10/22/2016 Disclosures No Disclosures to report Questions Does FAI lead to early development of osteoarthritis? Is surgical correction an effective treatment for FAI? Who
Femoral Acetabular Impingement 10/22/2016 Disclosures No Disclosures to report Questions Does FAI lead to early development of osteoarthritis? Is surgical correction an effective treatment for FAI? Who
GET HIP! CAPA 2015 Annual Conference WHAT IS HIP? HIP JOINT. Bradford H. Stiles, M.D., FAAFP
 GET HIP! Bradford H. Stiles, M.D., FAAFP WHAT IS HIP? HIP JOINT Synovial ball-and-socket joint Articulation between femoral head and acetabulum Acetabulum formed by the confluence of pelvis bones (ilium,
GET HIP! Bradford H. Stiles, M.D., FAAFP WHAT IS HIP? HIP JOINT Synovial ball-and-socket joint Articulation between femoral head and acetabulum Acetabulum formed by the confluence of pelvis bones (ilium,
Evaluation of Hip Pain in Adults. Jerry Ahluwalia, M.D. November 13, 2015
 Evaluation of Hip Pain in Adults Jerry Ahluwalia, M.D. November 13, 2015 Objectives Develop a better understanding of the differential diagnosis of hip pain in active young adults Appreciate key points
Evaluation of Hip Pain in Adults Jerry Ahluwalia, M.D. November 13, 2015 Objectives Develop a better understanding of the differential diagnosis of hip pain in active young adults Appreciate key points
FAI syndrome with or without labral tear.
 Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
A free online interactive information resource for clinicians.
 A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
DDH New Developments and Timeless Classics. DDH Define Treatment Group. (by age) DDH Imaging Choice in 6wk old Infant?
 DDH Imaging Choice in 6wk old Infant?") The 59 th Annual Edward T. Smith Orthopaedic Lectureship Emerging Concepts in the Surgical Management of the Hip: Deformity, Impingement and Fracture DDH New Developments and Timeless Classics Perry L.
The 59 th Annual Edward T. Smith Orthopaedic Lectureship Emerging Concepts in the Surgical Management of the Hip: Deformity, Impingement and Fracture DDH New Developments and Timeless Classics Perry L.
SCREENING THE NEWBORN FOR DEVELOPMENTAL DYSPLASIA OF THE HIP: REVIEW
 SCREENING THE NEWBORN FOR DEVELOPMENTAL DYSPLASIA OF THE HIP: REVIEW Dr. Upendra Yadav *1, 3, Dr. Zhu Xiao Fang 3, Dr. Ajit Kumar Yadav 1, 2, Dr. Sudhir Kumar Yadav 4 and Dr. Jeetendra Yadav 4 1 Yangtze
SCREENING THE NEWBORN FOR DEVELOPMENTAL DYSPLASIA OF THE HIP: REVIEW Dr. Upendra Yadav *1, 3, Dr. Zhu Xiao Fang 3, Dr. Ajit Kumar Yadav 1, 2, Dr. Sudhir Kumar Yadav 4 and Dr. Jeetendra Yadav 4 1 Yangtze
Lower Extremity Sports Injuries
 Lower Extremity Sports Injuries AAP Musculoskeletal Boot Camp Sigrid F. Wolf, MD Pediatric Sports Medicine Fellow Northwestern University Lurie Children s Hospital Disclosure I have no relevant financial
Lower Extremity Sports Injuries AAP Musculoskeletal Boot Camp Sigrid F. Wolf, MD Pediatric Sports Medicine Fellow Northwestern University Lurie Children s Hospital Disclosure I have no relevant financial
A comparison of varus and valgus slipped capital femoral epiphysis: A case series
 case Case report Series Meiling et al. 1 peer Reviewed open OPEN ACCESS A comparison of varus and valgus slipped capital femoral epiphysis: A case series James B. Meiling, W. Paul Bowman, Matthew E. Mayfield
case Case report Series Meiling et al. 1 peer Reviewed open OPEN ACCESS A comparison of varus and valgus slipped capital femoral epiphysis: A case series James B. Meiling, W. Paul Bowman, Matthew E. Mayfield
Evaluation of the Hip and Knee
 Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Pediatric Orthopedics in Your Office. Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care
 Pediatric Orthopedics in Your Office Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care Overview for 20 minute whirlwind Clavicle Distal radius fractures Finger fractures
Pediatric Orthopedics in Your Office Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care Overview for 20 minute whirlwind Clavicle Distal radius fractures Finger fractures
Treatment of congenital subluxation and dislocation of the hip by knee splint harness
 Prosthetics and Orthotics International, 1994,18, 34-39 Treatment of congenital subluxation and dislocation of the hip by knee splint harness M. FUKUSHIMA Fukushima Orthopaedic Clinic, Hiroshima City,
Prosthetics and Orthotics International, 1994,18, 34-39 Treatment of congenital subluxation and dislocation of the hip by knee splint harness M. FUKUSHIMA Fukushima Orthopaedic Clinic, Hiroshima City,
CLINICS IN SPORTS MEDICINE
 Clin Sports Med 25 (2006) 365 369 CLINICS IN SPORTS MEDICINE A Acetabular labrum, tears of, hip arthroscopy in, 264 Acetabular rim, trimming of, and labral repair, new method for, 293 297 Acetabulum, femoral
Clin Sports Med 25 (2006) 365 369 CLINICS IN SPORTS MEDICINE A Acetabular labrum, tears of, hip arthroscopy in, 264 Acetabular rim, trimming of, and labral repair, new method for, 293 297 Acetabulum, femoral
A Patient s Guide to Labral Tears of the Hip
 A Patient s Guide to Labral Tears of the Hip 15195 Heathcote Blvd Suite 334 Haymarket, VA 20169 Phone: 703-369-9070 Fax: 703-369-9240 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Labral Tears of the Hip 15195 Heathcote Blvd Suite 334 Haymarket, VA 20169 Phone: 703-369-9070 Fax: 703-369-9240 DISCLAIMER: The information in this booklet is compiled from a variety
An understanding of the components of the normal gait cycle will aid in describing abnormalities of gait.
 Approach to the Child with a Limp: Student writer: Brian Mayson Resident editor: Elmine Statham Background The child with a limp is a common problem seen in pediatrics. A limp is defined as any deviation
Approach to the Child with a Limp: Student writer: Brian Mayson Resident editor: Elmine Statham Background The child with a limp is a common problem seen in pediatrics. A limp is defined as any deviation
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
Developmental Dysplasia of the Hip, (DDH) including Femoral and Pelvic Osteotomy
 including Femoral and Pelvic Osteotomy") Developmental Dysplasia of the Hip, (DDH) including Femoral and Pelvic Osteotomy Leicester Children s Hospital Information for Patients, Parents and Carers DRAFT What is developmental dysplasia of the
Developmental Dysplasia of the Hip, (DDH) including Femoral and Pelvic Osteotomy Leicester Children s Hospital Information for Patients, Parents and Carers DRAFT What is developmental dysplasia of the
Original Article Results of simultaneous open reduction and Salter innominate osteotomy for developmental dysplasia of the hip
 Kathmandu University Medical Journal (2005) Vol. 3, No. 1, Issue 9, 6-10 Original Article Results of simultaneous open reduction and Salter innominate osteotomy for developmental dysplasia of the hip Banskota
Kathmandu University Medical Journal (2005) Vol. 3, No. 1, Issue 9, 6-10 Original Article Results of simultaneous open reduction and Salter innominate osteotomy for developmental dysplasia of the hip Banskota
Outcome of surgical management of late presenting developmental dysplasia of hip with pelvic and femoral osteotomies
 Original Research Article DOI: 10.18231/2395-1362.2018.0012 Outcome of surgical management of late presenting developmental dysplasia of hip with pelvic and femoral osteotomies G. Jagadesh 1, Venugopal
Original Research Article DOI: 10.18231/2395-1362.2018.0012 Outcome of surgical management of late presenting developmental dysplasia of hip with pelvic and femoral osteotomies G. Jagadesh 1, Venugopal
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE
 PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
CHAPTER 9. Summary and general discussion.
 CHAPTER 9 Summary and general discussion. Chapter 9 Chapter 1 This thesis describes different aspects of slipped capital femoral epiphysis (SCFE). Although rare, SCFE is the most common adolescent hip
CHAPTER 9 Summary and general discussion. Chapter 9 Chapter 1 This thesis describes different aspects of slipped capital femoral epiphysis (SCFE). Although rare, SCFE is the most common adolescent hip
Delayed fixation of an unstable Slipped capital femoral epiphysis: A case report and review of literature
 ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 14 Number 1 Delayed fixation of an unstable Slipped capital femoral epiphysis: A case report and review of literature S Lowndes, A Khanna, D
ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 14 Number 1 Delayed fixation of an unstable Slipped capital femoral epiphysis: A case report and review of literature S Lowndes, A Khanna, D
AND PARACLINICAL INVESTIGATIONS
 Jurnal Medical Aradean (Arad Medical Journal) CONGENITAL DISLOCATION OF THE HIP: CLINICAL AND PARACLINICAL INVESTIGATIONS Violeta Oriţă, Marius Bucur Constantinescu, Beatrice Frumuşeanu, Mihaela Golumbeanu
Jurnal Medical Aradean (Arad Medical Journal) CONGENITAL DISLOCATION OF THE HIP: CLINICAL AND PARACLINICAL INVESTIGATIONS Violeta Oriţă, Marius Bucur Constantinescu, Beatrice Frumuşeanu, Mihaela Golumbeanu
Developmental dysplasia of the hip: What has changed in the last 20 years?
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5312/wjo.v6.i11.886 World J Orthop 2015 December 18; 6(11): 886-901 ISSN 2218-5836 (online)
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5312/wjo.v6.i11.886 World J Orthop 2015 December 18; 6(11): 886-901 ISSN 2218-5836 (online)
Developmental Dysplasia of the Hip From Birth to Six Months
 From Birth to Six Months James T. Guille, MD, Peter D. Pizzutillo, MD, and G. Dean MacEwen, MD Abstract The term developmental dysplasia or dislocation of the hip (DDH) refers to the complete spectrum
From Birth to Six Months James T. Guille, MD, Peter D. Pizzutillo, MD, and G. Dean MacEwen, MD Abstract The term developmental dysplasia or dislocation of the hip (DDH) refers to the complete spectrum
ONE STAGE COMBINED SURGICAL TREATMENT FOR DEVELOPMENTAL DISLOCATION OF THE HIP IN OLDER CHILDREN INCLUDING FEMORAL SHORTENING
 Basrah Journal Original Article Of Surgery Bas J Surg, March, 17, 2011 ONE STAGE COMBINED SURGICAL TREATMENT FOR DEVELOPMENTAL DISLOCATION OF THE HIP IN OLDER CHILDREN INCLUDING FEMORAL SHORTENING MBChB,
Basrah Journal Original Article Of Surgery Bas J Surg, March, 17, 2011 ONE STAGE COMBINED SURGICAL TREATMENT FOR DEVELOPMENTAL DISLOCATION OF THE HIP IN OLDER CHILDREN INCLUDING FEMORAL SHORTENING MBChB,
Perthes disease in a child with Silver-Russell syndrome
 ISPUB.COM The Internet Journal of Pediatrics and Neonatology Volume 7 Number 1 Perthes disease in a child with Silver-Russell syndrome V Kakar, R Botchu, M Katchburian Citation V Kakar, R Botchu, M Katchburian.
ISPUB.COM The Internet Journal of Pediatrics and Neonatology Volume 7 Number 1 Perthes disease in a child with Silver-Russell syndrome V Kakar, R Botchu, M Katchburian Citation V Kakar, R Botchu, M Katchburian.
Speaker s Disclosure Statement. Starvation, Death and Destruction: The Battlefield of AVN. Objectives. Risk Factors
 Starvation, Death and Destruction: The Battlefield of AVN Speaker s Disclosure Statement I have no industry relationships to disclose I will discuss off-label use of medications Dana-Farber/Boston Children
Starvation, Death and Destruction: The Battlefield of AVN Speaker s Disclosure Statement I have no industry relationships to disclose I will discuss off-label use of medications Dana-Farber/Boston Children
The Painful Hip. Jennifer R Marks, MD
 The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
Musculoskeletal Management of A Limping Child
 Musculoskeletal Management of A Limping Child Julieanne P. Sees, DO, FAOAO Pediatric Neuro-Orthopaedic Surgeon Medical Director, Neuro-Orthopaedic Rehabilitation Unit Wilmington, DE Objectives Identify
Musculoskeletal Management of A Limping Child Julieanne P. Sees, DO, FAOAO Pediatric Neuro-Orthopaedic Surgeon Medical Director, Neuro-Orthopaedic Rehabilitation Unit Wilmington, DE Objectives Identify
THE HIP JOINT IN CEREBRAL PALSY
 HOSPITAL FOR JOINT DISEASES THE HIP JOINT IN CEREBRAL PALSY David S. Feldman, MD Professor of Orthopedic Surgery and Pediatrics Chief, Pediatric Orthopedic Surgery NYU/Hospital for Joint Diseases Define
HOSPITAL FOR JOINT DISEASES THE HIP JOINT IN CEREBRAL PALSY David S. Feldman, MD Professor of Orthopedic Surgery and Pediatrics Chief, Pediatric Orthopedic Surgery NYU/Hospital for Joint Diseases Define
Total Hip Arthroplasty Performed Using Conventional and Computer-Assisted, Tissue- Preserving Techniques 6
 Total Hip Arthroplasty Performed Using Conventional and Computer-Assisted, Tissue- Preserving Techniques 6 Stephen B. Murphy, MD, Timo M. Ecker, MD and Moritz Tannast, MD Introduction Less invasive techniques
Total Hip Arthroplasty Performed Using Conventional and Computer-Assisted, Tissue- Preserving Techniques 6 Stephen B. Murphy, MD, Timo M. Ecker, MD and Moritz Tannast, MD Introduction Less invasive techniques
Osteoarthritis of the Hip
 Osteoarthritis of the Hip Sometimes called "wear-and-tear" arthritis, osteoarthritis is a common condition that many people develop during middle age or older. Osteoarthritis of the hip causes pain and
Osteoarthritis of the Hip Sometimes called "wear-and-tear" arthritis, osteoarthritis is a common condition that many people develop during middle age or older. Osteoarthritis of the hip causes pain and
Lower Extremity Fracture Management. Fractures of the Hip. Lower Extremity Fractures. Vascular Anatomy. Lower Extremity Fractures in Children
 Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Ankle Sprains and Their Imitators
 Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip
 of the Hip") A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
PEDIATRIC AND CONGENITAL IMAGING GUIDELINES: MUSCULOSKELETAL 2011 MedSolutions, Inc
 MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not
MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not
Case Study: Nadine. Conditions Treated Hip Dysplasia. Age Range During Treatment 39 years
 Case Study: Nadine Conditions Treated Hip Dysplasia Age Range During Treatment 39 years David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone
Case Study: Nadine Conditions Treated Hip Dysplasia Age Range During Treatment 39 years David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone
Ultrasound Scanning of Neonatal Hips
 Ultrasound Scanning of Neonatal Hips Dr. Dickson S F Tsang Associate Consultant Queen Mary Hospital Why? How? What? Outline IAAHS 2nd April, 2011 Outline Why? Why performing hip ultrasound (USG)? Why USG?
Ultrasound Scanning of Neonatal Hips Dr. Dickson S F Tsang Associate Consultant Queen Mary Hospital Why? How? What? Outline IAAHS 2nd April, 2011 Outline Why? Why performing hip ultrasound (USG)? Why USG?
Degenerative arthritis of Hip Bone Bangalore. Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal
 Degenerative arthritis of Hip Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal Hip joint Classical Synovial joint Biomechanics of hip Force coincides with trabecular pattern Hip joint Acetabulum
Degenerative arthritis of Hip Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal Hip joint Classical Synovial joint Biomechanics of hip Force coincides with trabecular pattern Hip joint Acetabulum
A novel method for assessing postoperative femoral head reduction in developmental dysplasia of the hip
 J Child Orthop (2014) 8:319 324 DOI 10.1007/s11832-014-0600-5 ORIGINAL CLINICAL ARTICLE A novel method for assessing postoperative femoral head reduction in developmental dysplasia of the hip Anthony Cooper
J Child Orthop (2014) 8:319 324 DOI 10.1007/s11832-014-0600-5 ORIGINAL CLINICAL ARTICLE A novel method for assessing postoperative femoral head reduction in developmental dysplasia of the hip Anthony Cooper
3/18/18. Adolescent Hip Injuries. Adolescents with Hip Injuries DISCLOSURES
 Adolescent Hip Injuries Henry Bone Ellis, Jr., MD DFW Sports Medicine Symposium March 24, 2018 DISCLOSURES Royalties and stock options Consulting income Smith and Nephew Other support Research on Osteochondritis
Adolescent Hip Injuries Henry Bone Ellis, Jr., MD DFW Sports Medicine Symposium March 24, 2018 DISCLOSURES Royalties and stock options Consulting income Smith and Nephew Other support Research on Osteochondritis