Cosa chiedo all autoregolazione cerebrale?
|
|
|
- April Hudson
- 5 years ago
- Views:
Transcription




1 Frank Update in Traumatologia Cranica FRANK A. RASULO ANESTHESIOLOGY, INTENSIVE CARE, PERIOPERATIVE CARE and PAIN MEDICINE Spedali Civili University Hospital Brescia, Italy Cosa chiedo all autoregolazione cerebrale?
2 INTRODUCTION NO CONFLICTS Che cos è l autoregolazione cerebrale?

3 INTRODUCTION On Intra-Cranial Pressure and the Cerebral Circulation: part I. Physiological; Part II. Histological. Bayliss WM et al. J Physiol 1895;18(4): Sir William Maddock Bayliss
4 Press / Flusso Il flusso di un liquido all interno di un tubo rigido Pressione Resistenza Flusso
5 CBF/MABP

6 GRAVITY
7


8 ACTION VESSELS et al.
9 PRESSURE AUTOREGULATION CURVE Crit Care Clin 23 (2007)

10 CVA AND TBI WHY IS AUTOREGULATION IMPORTANT IN BRAIN INJURY?
11 CVA and TBI

12 CVA and TBI
13 TBI, CBF, CVA, CVR Crit Care Clin 23 (2007) KE Wartenberg et al.
14 TBI, CBF, CVA, CVR Crit Care Clin 23 (2007) KE Wartenberg et al.

15 CVA and TBI Your Brain after you bump your head Drawing of her daughter (age 7)

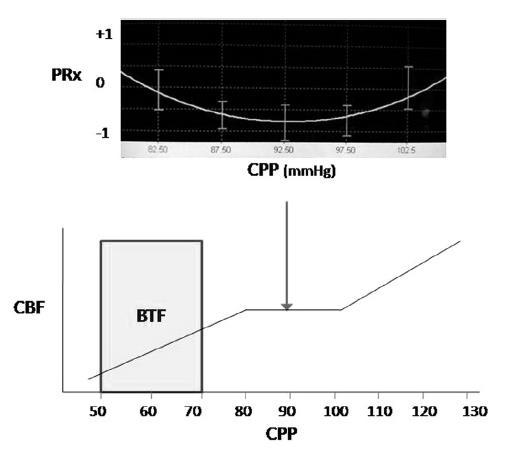
16 BTF Guidelines 4 th Edition 10mmHg

17 How we look at a CVA curve in TBI Secondary Injury PULMONARY EDEMA ARDS Modified from A. Lavinio
 507")
18 CVA and TBI Crit Care Clin 23 (2007)



19 CSS on MMM in NCC Intensive Care Med Sep;40(9):
20 Measuring CVA in TBI Testing * Clear stimulation: -drug to rise ABP -leg cuff release -head down tilt -lower body pressure -slow respiration -transient compression Assessment of Cerebral Pressure Autoregulation Frank A Rasulo, Marcella Balestreri, Basil Matta. Current Opinion in Anesthesiology. October 2002 HOW TO MEASURE CEREBROVASCULAR AUTOREGULATION Monitoring *No stimulation; spontaneaous waves of ABP or CPP

21 TESTING CVA in TBI CUFF TEST Testing * Clear stimulation: -drug to rise ABP -leg cuff release -head down tilt -lower body pressure -slow respiration -transient compression Monitoring *No stimulation; spontaneaous waves of ABP or CPP Autoregulatory is seen from the blood velocity returning to pretest values after 4 seconds.
22 TESTING CVA in TBI THRT Testing * Clear stimulation: -drug to rise ABP -leg cuff release -head down tilt -lower body pressure -slow respiration -transient compression Monitoring *No stimulation; spontaneaous waves of ABP or CPP circa 5 secondi Better accuracy One-off measurement

23 MONITORING CVA in TBI INDEX Testing * Clear stimulation: -drug to rise ABP -leg cuff release -head down tilt -lower body pressure -slow respiration -transient compression Monitoring *No stimulation; spontaneaous waves of ABP or CPP circa 5 secondi Better accuracy One-off measurement

24 Crit Care Clin 23 (2007) KE Wartenberg et al.
25
26 - ICP - ABP PRx = ICP/ABP
27 MONITORING CVA in TBI PRx CEREBROVASCULAR AUTOREGULATION PARAMETER 1 ABP PARAMETER 2 ICP Negative Correlation Autoregulation PRESERVED < 0.2 PARAMETER 1 PARAMETER 2 PRESSURE PASSIVE PARAMETER 1 PARAMETER 2 Positive Correlation Autoregulation DISTURBED

28 MONITORING CVA in TBI PRx CEREBROVASCULAR AUTOREGULATION EVD Placement PARAMETE R 1 PARAMETE R 2 PARAMETER 1 PARAMETER 2

29 MONITORING CVA in TBI PRx

30 MONITORING CVA in TBI PRx

31 MONITORING CVA in TBI PRx Cerebrovascular reactivity during hypothermia and rewarming. Lavinio A et al. Br J Anaesth. 2007;99:237 44

32 MONITORING CVA in TBI PRx

33 CVA in TBI Non-invasive PRx? Conclusions: This study provides preliminary evidence that ICPtcd may accurately exclude intracranial hypertension in patients with acute brain injury. FUTURE PRx ICPnon-invasive /ABP
34 - TCD - ABP Mx = FVm/CPP


35 MONITORING CVA in TBI Mx Consequence of disturbed CVA and hypotension Mx

36 MONITORING CVA in TBI Mx AutoregulazioneCompromessa
37 MONITORING CVA in TBI Mx CEREBROVASCULAR AUTOREGULATION Administration of hypertonic Saline PARAMETER 1 PARAMETER 2 PARAMETER 1 PARAMETER 2
38 MONITORING CVA in TBI Mx Mx Autoregulation and Cerebral Perfusion Pressure CzosnykaM.,et al. J Neurosurg 2001
39 MONITORING CVA in TBI Mx Mx Autoregulation and Cerebral Perfusion Pressure CzosnykaM.,et al. J Neurosurg 2001 Altered CVA Normal CVA
40 MONITORING CVA in TBI Mx CEREBROVASCULAR AUTOREGULATION ABP ICP CPP FV ABP ICP CPP FV ABP ICP CPP FV

41 MONITORING CVA in TBI Mx
42 MONITORING CVA in TBI Monitoring of Autoregulation Without Measurement of CBF?
43 - NIRS - ABP TOx = TOI/CPP

44 - Pbr02 - ABP ORx = PbtO2/CPP



45 MONITORING CVA in TBI TOx, ORx Continuous assessment of cerebrovascular autoregulation after traumatic brain injury using brain tissue oxygen pressure reactivity. Jaeger M., et al Crit Care Med Jun;34(6):1783-8
46 - PI - ABP
47 MONITORING CVA in TBI Continuous Measurement of Autoregulation by Spontaneous Fluctuations in Cerebral Perfusion Pressure Ken M. Brady et al. Stroke Volume 39(9): September 1, 2008 Piglets 5 to10 days old with intracranial pressure (ICP) at naïve or elevated (20 mm Hg) levels had gradual arterial hypotension induced by a balloon catheter in the inferior vena cava. Three indices of autoregulation were simultaneously and continuously calculated.

48 INDIVIDUALIZATION/OPTIMIZATION INDIVIDUALIZATION OPTIMIZATION

49 INDIVIDUALIZATION

50 INDIVIDUALIZATION the strongest clinical implication of the results is that we shouldn t abandon ICP monitoring but to refine its role in TBI management clinical methods for interpreting ICP in the setting of individual patient care. Cerebral autoregulation, cerebral perfusion pressure, cerebral blood flow, metabolic coupling etc., should allow us to recognize when ICP of 25 or 30mmHg might be cautiously accepted rather than lead to second-tier interventions analytic approaches allowing protocolizing decision making for more meaningful subclassification of injury types, would highlight the true value of ICP monitoring as part of a multimodality approach to targeted therapy. As intensivists, we probably should be embarrassed that we are not at such a point in TBI management already.
51
52 INDIVIDUALIZATION



53 INDIVIDUALIZATION Retrospective analysis of prospectively collected data from 327 patients TBI pts. ICP doses derived by the recommended BTF threshold of 20 mm Hg. VS ICP dose based on individually assessed ICP thresholds Based on PRx-CVA 6-month outcome Individualized doses of intracranial hypertension were stronger predictors of death than doses derived from the universal threshold of 20mm Hg. PRx can individualize the ICP threshold
54 INDIVIDUALIZATION Can monitoring CVA be a clinically useful therapeutic target in TBI? We must adjust the contributors to the complex cerebral autoregulation process. Several potential methods for adjusting cerebral autoregulation include: Optimization of CPP, Optimization of ventilation, Optimization of head-of-bed positioning, Optimization of pharmacologic manipulation.

55 OPTIMIZING CPP Conitinuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury Steiner L et al., Crit Care Med 2002 vol 30, No 4 We must adjust the contributors to the complex cerebral autoregulation process. Several potential methods for adjusting cerebral autoregulation include: Optimization of CPP: FRANK A. RASULO Institute of Anesthesiology & Intensive Care Neuro-critical Care Unit, Spedali Civili University Hospital of Brescia, ITALY

56 OPTIMIZING CPP Donnelly J Expert Rev. Neurother. 15(2), (2015)

57 OPTIMIZING CPP Donnelly J Expert Rev. Neurother. 15(2), (2015)
 CPPopt =")

58 OPTIMIZING CPP Continuous Assessment of Autoregulation (CPPopt) CPPopt = CPP where PRx reaches its minimum value when plotted against CPP. CPP opt? 65 mmhg!




59 OPTIMIZING CPP We aim to improve the CPPopt methodology by introducing a new visualization method that may provide insight into the complete characteristics of the CPP-PRx relationship and its temporal evolution.
60 OPTIMIZING VENTILATION Can monitoring CVA be a clinically useful therapeutic target in TBI? Several potential methods for adjusting cerebral autoregulation include: Optimization of CPP Optimization of ventilation Cerebral autoregulation dynamics in humans. Aaslid R et al. Stroke 1989;20(1):45-52 Adverse effects of prolonged hyperventilation in patients with severe head injury: a randomized clinical trial. J Muizelaar JP et al. Neurosurg 1991;75:731-9

61 OPTIMIZING VENTILATION Autoregulation and arterial CO 2 Lingzhong Meng, Adrian W. Gelb. Anesthesiology , Vol.122,
62 OPTIMIZING VENTILATION Autoregulation and arterial CO 2 Mx responds to PaCO 2 during routine CO 2 -reactivity testing.
63 OPTIMIZING POSITIONING Can monitoring CVA be a clinically useful therapeutic target in TBI? Several potential methods for adjusting cerebral autoregulation include: Optimization of CPP Optimization of ventilation Optimization of head-of-bed positioning Intracranial pressure pulse amplitude during changes in head elevation: a new parameter for determining optimum cerebral perfusion pressure? Mahfoud F, et al. Acta Neurochir (Wien) 2010; 152(3): Effect of head elevation on intracranial pressure, cerebral perfusion pressure, and cerebral blood flow in head-injured patients. Feldman Z et al. J Neurosurg 1992;76:207-11
64 OPTIMIZING DRUGS Can monitoring CVA be a clinically useful therapeutic target in TBI? Optimization of CPP Optimization of ventilation Optimization of head-of-bed positioning Optimization of pharmacologic manipulation Simvastatin. Kirkpatrick PJ Lancet Neurol 2014;13(7): EPO. Rasmussen P FASEB J 2012;26(3): Recombinant human erythropoietin. Ehrenreich H Stroke 2009;40:e B-Blockers. Strandgaard S Eur J Clin Invest 1996;26(8) Valsartan. Takada J Hypertens Res 2006;29(8):621-6 Angiotensin II AT2 receptor stimulation. Na veri L, Regul Pept 1994;52:21-9 Angiotensin converting enzyme. Waldemar G J Hypertens 1989;7:
65 CVA TBI - OUTCOME Links Between CVA and TBI Outcome Impact of intracranial pressure and cerebral perfusion pressure on severe disability and mortality after head injury. Balestreri M et al.neurocrit Care Association between dynamic cerebral autoregulation and mortality in severe head injury. Panerai RB et al. Br J Neurosurg 2004 In a multivariate analysis, age, mean ICP, initial CT, and the CVA are all independent factors OF outcome Both intermittently monitored TCD-based indices, the Mx and ARI, and continuous PRx have proven to be strongly and independently correlated with outcome Plotting mortality rate versus averaged PRx allows detection of critical value for PRx. When the PRx increases above 0.3, mortality rate abruptly increases from 20% to 70%
66 CVA - TBI - OUTCOME THRT e Outcome TCG THRR Fav orable Outcome Unf av orable
67 CVA - TBI - OUTCOME AUTOREGULATION IS SIGNIFICANTLY WORSE IN PATIENTS WITH UNFAVOURABLE OUTCOME MX Czosnyka M, Smielewski P, Piechnik S, Steiner LA, Pickard JD: Cerebral autoregulation following head injury. J Neurosurg 2001, 95 (5),
68 CVA - TBI - OUTCOME Autoregulation: Asymmetry and Mortality
69 CVA - TBI - OUTCOME Cerebrovascular Autoregulation (CVA) and Outcome Author Paper Pathology N pts. Bad outcome Overgaard J. et al. J.Neurosurg Head Trauma 43 68% Czosnyka M. et al. Stroke 1996 Head Trauma 82 70% Lam JM. Et al. Ratsep et al J.Neurosurg J.Neurosurg Head Trauma 31 65% SAH 76 68% Lang E.W. Crit. care med.2001 SAH 12 82% Steiner L. et al. JNNP 2003 Head Trauma 82 67%
70 CVA - TBI - OUTCOME Dose effect: patients with more severe impairment of cerbral autoregulation do have worse outcome Time effect: the state of autoregulation change in time Autoulation is worse first two days following trauma but only in patients who died (red line) J Neurosurg 2001, 95 (5),
71 CVA - SAH - OUTCOME



72 CVA - TBI - OUTCOME et al.
73 CVA - TBI - OUTCOME Patients with larger discrepancy (>10 mm Hg) between real CPP and CPPopt more likely have adverse outcome. This finding stresses the importance of guiding TBI treatment using CVA indices in clinical practice.

74 ALL OBVIOUS???


75 PROTOCOL INTEGRATION TBI

76 LITERATURE CVA BRAIN INJURY CVA monitoring in TBI passes from a level III to a level IIB recommendation in the new BTF guidelines.

77 PROTOCOL INTEGRATION
78 PROTOCOL INTEGRATION
79 CONCLUSION Facts: Poor autoregulation and loss of pressure-reactivity, as measured by PRx and Mx, are independent predictors of fatal outcome following head injury; Continuous monitoring with the PRx can be used to direct CPP-oriented therapy by determining the optimal CPP for pressure-reactivity. Monitoring of continuous cerebrovascular autoregulation is now possible and systems have become, and are becoming, more user-friendly; Missing Links: Despite the fact that monitoring CVA can be used in a variety of clinical scenarios and may be helpful in delineating optimal therapeutic strategies, the integration of CVA based protocols, to obtain a more individualized therapeutic strategy, is still lagging, do to lack of adequate trials.


80 GRAZIE
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples.
. Pressure-reactivity index, computational methods. Clinical examples.") Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
19. Monitoring of CA using TCD- Mx and Sx
 19. Monitoring of CA using TCD- Mx and Sx Drawing the autoregulatory curve: in clinical practice such dramatic changes in CPP are not permissible Monitoring cerebral autoregulation - certainly not a new
19. Monitoring of CA using TCD- Mx and Sx Drawing the autoregulatory curve: in clinical practice such dramatic changes in CPP are not permissible Monitoring cerebral autoregulation - certainly not a new
Regulation of Cerebral Blood Flow. Myogenic- pressure autoregulation Chemical: PaCO2, PaO2 Metabolic Neuronal
 Regulation of Cerebral Blood Flow Myogenic- pressure autoregulation Chemical: PaCO2, PaO2 Metabolic Neuronal The Autoregulation, Stupid! Drawing of her daughter (age 7) Flow through rigid tube Mogens Fog
Regulation of Cerebral Blood Flow Myogenic- pressure autoregulation Chemical: PaCO2, PaO2 Metabolic Neuronal The Autoregulation, Stupid! Drawing of her daughter (age 7) Flow through rigid tube Mogens Fog
perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP?
 7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome?
 11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
13. Volume-pressure infusion tests: Typical patterns of infusion studies in different forms of CSF circulatory disorders.
 13. Volume-pressure infusion tests: Typical patterns of infusion studies in different forms of CSF circulatory disorders. Hydrocephalus is far more complex than disorder of CSF circulation CSF circulation
13. Volume-pressure infusion tests: Typical patterns of infusion studies in different forms of CSF circulatory disorders. Hydrocephalus is far more complex than disorder of CSF circulation CSF circulation
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Current bedside monitors of brain blood flow and oxygen delivery
 24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Cosa chiedo alla PtO 2
 Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cerebral autoregulation is a complex intrinsic control. Time course for autoregulation recovery following severe traumatic brain injury
 J Neurosurg 111:695 700, 2009 Time course for autoregulation recovery following severe traumatic brain injury Clinical article Gi l l E. Sv i r i, M.D., M.Sc., 1 Ru n e Aa s l i d, Ph.D., 2 Co l l e e
J Neurosurg 111:695 700, 2009 Time course for autoregulation recovery following severe traumatic brain injury Clinical article Gi l l E. Sv i r i, M.D., M.Sc., 1 Ru n e Aa s l i d, Ph.D., 2 Co l l e e
Neurosurg Focus 25 (10):
:") Neurosurg Focus 25 (10):E2, 2008 Continuous monitoring of cerebrovascular pressure reactivity in patients with head injury Ch r i s t i a n Zw e i f e l, M.D., 1 And r e a Lav i n i o, M.D., 1 Lu z i u
Neurosurg Focus 25 (10):E2, 2008 Continuous monitoring of cerebrovascular pressure reactivity in patients with head injury Ch r i s t i a n Zw e i f e l, M.D., 1 And r e a Lav i n i o, M.D., 1 Lu z i u
Patients with aneurysmal subarachnoid hemorrhage
 CLINICAL INVESTIGATION Are Optimal Cerebral Perfusion Pressure and Cerebrovascular Autoregulation Related to Long-term Outcome in Patients With Aneurysmal Subarachnoid Hemorrhage? Frank Anthony Rasulo,
CLINICAL INVESTIGATION Are Optimal Cerebral Perfusion Pressure and Cerebrovascular Autoregulation Related to Long-term Outcome in Patients With Aneurysmal Subarachnoid Hemorrhage? Frank Anthony Rasulo,
The resistance to CSF outflow in hydrocephalus what it is and what it isn t.
 The resistance to CSF outflow in hydrocephalus what it is and what it isn t. Davson et al 1970, The mechanism of drainage of CSF. Brain 93:665-8 1989, Copenhagen, Alfred Benzon Foundation CSf outflow is
The resistance to CSF outflow in hydrocephalus what it is and what it isn t. Davson et al 1970, The mechanism of drainage of CSF. Brain 93:665-8 1989, Copenhagen, Alfred Benzon Foundation CSf outflow is
CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium
 CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium Financial disclosures Research Foundation, Flanders (senior clinical
CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium Financial disclosures Research Foundation, Flanders (senior clinical
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Multimodal monitoring to individualize care in TBI
 Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Dynamic autoregulatory response after severe head injury
 J Neurosurg 97:1054 1061, 2002 Dynamic autoregulatory response after severe head injury ROMAN HLATKY, M.D., YU FURUYA, M.D., PH.D., ALEX B. VALADKA, M.D., JORGE GONZALEZ, M.D., ARI CHACKO, M.D., YASU MIZUTANI,
J Neurosurg 97:1054 1061, 2002 Dynamic autoregulatory response after severe head injury ROMAN HLATKY, M.D., YU FURUYA, M.D., PH.D., ALEX B. VALADKA, M.D., JORGE GONZALEZ, M.D., ARI CHACKO, M.D., YASU MIZUTANI,
Cerebrovascular Reactivity Measured by Near-Infrared Spectroscopy
 Cerebrovascular Reactivity Measured by Near-Infrared Spectroscopy Jennifer K. Lee, MD; Kathleen K. Kibler, BS; Paul B. Benni, PhD; R. Blaine Easley, MD; Marek Czosnyka, PhD; Peter Smielewski, PhD; Raymond
Cerebrovascular Reactivity Measured by Near-Infrared Spectroscopy Jennifer K. Lee, MD; Kathleen K. Kibler, BS; Paul B. Benni, PhD; R. Blaine Easley, MD; Marek Czosnyka, PhD; Peter Smielewski, PhD; Raymond
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Impaired Cerebral Autoregulation in a Case of Severe Acute Encephalitis
 CASE REPORT Impaired Cerebral Autoregulation in a Case of Severe Acute Encephalitis Sung-Chun Tang, Sheng-Jean Huang, 1 Ming-Jang Chiu,* Ping-Keung Yip The status of cerebral autoregulation (CA) is an
CASE REPORT Impaired Cerebral Autoregulation in a Case of Severe Acute Encephalitis Sung-Chun Tang, Sheng-Jean Huang, 1 Ming-Jang Chiu,* Ping-Keung Yip The status of cerebral autoregulation (CA) is an
Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality
 Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
The management of severe traumatic brain injury
 J Neurosurg 120:1451 1457, 2014 AANS, 2014 Pressure autoregulation monitoring and cerebral perfusion pressure target recommendation in patients with severe traumatic brain injury based on minute-by-minute
J Neurosurg 120:1451 1457, 2014 AANS, 2014 Pressure autoregulation monitoring and cerebral perfusion pressure target recommendation in patients with severe traumatic brain injury based on minute-by-minute
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Per Kvandal Lawrence Sheppard Svein A. Landsverk Aneta Stefanovska Knut A. Kirkeboen
 J Clin Monit Comput (2013) 27:375 383 DOI 10.1007/s10877-013-9484-z ORIGINAL RESEARCH Impaired cerebrovascular reactivity after acute traumatic brain injury can be detected by wavelet phase coherence analysis
J Clin Monit Comput (2013) 27:375 383 DOI 10.1007/s10877-013-9484-z ORIGINAL RESEARCH Impaired cerebrovascular reactivity after acute traumatic brain injury can be detected by wavelet phase coherence analysis
Changes in Linear Dynamics of Cerebrovascular System After Severe Traumatic Brain Injury
 Changes in Linear Dynamics of Cerebrovascular System After Severe Traumatic Brain Injury M. Müller, MD; O. Bianchi; S. Erülkü; C. Stock; K. Schwerdtfeger, MD; for the Homburg Traumatic Brain Injury Group
Changes in Linear Dynamics of Cerebrovascular System After Severe Traumatic Brain Injury M. Müller, MD; O. Bianchi; S. Erülkü; C. Stock; K. Schwerdtfeger, MD; for the Homburg Traumatic Brain Injury Group
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Regulation of the cerebral circulation: bedside assessment and clinical implications
 Donnelly et al. Critical Care 2016, 18: REVIEW Regulation of the cerebral circulation: bedside assessment and clinical implications Joseph Donnelly 1, Karol P. Budohoski 1, Peter Smielewski 1 and Marek
Donnelly et al. Critical Care 2016, 18: REVIEW Regulation of the cerebral circulation: bedside assessment and clinical implications Joseph Donnelly 1, Karol P. Budohoski 1, Peter Smielewski 1 and Marek
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Positive end-expiratory pressure oscillation facilitates brain vascular reactivity monitoring
 J Appl Physiol 113: 1362 1368, 212. First published September 13, 212; doi:1.1152/japplphysiol.853.212. Positive end-expiratory pressure oscillation facilitates brain vascular reactivity monitoring Ken
J Appl Physiol 113: 1362 1368, 212. First published September 13, 212; doi:1.1152/japplphysiol.853.212. Positive end-expiratory pressure oscillation facilitates brain vascular reactivity monitoring Ken
Intracranial volume-pressure relationships during
 Journial of Neurology, Neurosurgery, and Psychiatry, 1974, 37, 115-1111 Intracranial volume-pressure relationships during experimental brain compression in primates 3. Effect of mannitol and hyperventilation
Journial of Neurology, Neurosurgery, and Psychiatry, 1974, 37, 115-1111 Intracranial volume-pressure relationships during experimental brain compression in primates 3. Effect of mannitol and hyperventilation
Cerebral Blood Flow Thresholds for Cerebral Ischemia in. Traumatic Brain Injury. A Systematic Review.
 Cerebral Blood Flow Thresholds for Cerebral Ischemia in Traumatic Brain Injury. A Systematic Review. Marco Botteri, MD, Elisabetta Bandera, MD, Cosetta Minelli, MD, PhD, Nicola Latronico, MD Neuroanesthesia
Cerebral Blood Flow Thresholds for Cerebral Ischemia in Traumatic Brain Injury. A Systematic Review. Marco Botteri, MD, Elisabetta Bandera, MD, Cosetta Minelli, MD, PhD, Nicola Latronico, MD Neuroanesthesia
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
The circulation of cerebral blood flow (CBF) is driven. A noninvasive estimation of cerebral perfusion pressure using critical closing pressure
 is driven. A noninvasive estimation of cerebral perfusion pressure using critical closing pressure") clinical article J Neurosurg 123:638 648, 2015 A noninvasive estimation of cerebral perfusion pressure using critical closing pressure Georgios V. Varsos, MSc, 1 Angelos G. Kolias, MSc, MRCS, 1 Peter Smielewski,
clinical article J Neurosurg 123:638 648, 2015 A noninvasive estimation of cerebral perfusion pressure using critical closing pressure Georgios V. Varsos, MSc, 1 Angelos G. Kolias, MSc, MRCS, 1 Peter Smielewski,
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Intracranial pressure pulse amplitude during changes in head elevation: a new parameter for determining optimum cerebral perfusion pressure?
 Acta Neurochir (2010) 152:443 450 DOI 10.1007/s00701-009-0520-1 CLINICAL ARTICLE Intracranial pressure pulse amplitude during changes in head elevation: a new parameter for determining optimum cerebral
Acta Neurochir (2010) 152:443 450 DOI 10.1007/s00701-009-0520-1 CLINICAL ARTICLE Intracranial pressure pulse amplitude during changes in head elevation: a new parameter for determining optimum cerebral
DISCLOSURES. Specific TCD clinical applications for patients with traumatic brain injury 1/10/2015. FTE, Private Practice for profit TBI TBI: SCOPE
 DISCLOSURES Specific TCD clinical applications for patients with traumatic brain injury FTE, Private Practice for profit Alexander Razumovsky, PhD, FAHA 38 35 th Annual Meeting 38 35 th Annual Meeting
DISCLOSURES Specific TCD clinical applications for patients with traumatic brain injury FTE, Private Practice for profit Alexander Razumovsky, PhD, FAHA 38 35 th Annual Meeting 38 35 th Annual Meeting
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
TCD and cardiac arrest
 TCD and cardiac arrest Background: An effective tissue perfusion has decisive influence on the final prognosis both during cardiopulmonary resuscitation (CPR) and after recovery of spontaneous circulation
TCD and cardiac arrest Background: An effective tissue perfusion has decisive influence on the final prognosis both during cardiopulmonary resuscitation (CPR) and after recovery of spontaneous circulation
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
NEWROSIM. Traumatic Brain Injury & Stroke Care Training Solution
 NEWROSIM Traumatic Brain Injury & Stroke Care Training Solution 10 Preprogrammed TBI and Stroke Scenarios NewroSim Scenario Guidebook Powerful computer-based hemodynamic model Interactive transcranial
NEWROSIM Traumatic Brain Injury & Stroke Care Training Solution 10 Preprogrammed TBI and Stroke Scenarios NewroSim Scenario Guidebook Powerful computer-based hemodynamic model Interactive transcranial
Effect of decompressive craniectomy on intracranial pressure and cerebrospinal compensation following traumatic brain injury
 J Neurosurg 108:66 73, 2008 Effect of decompressive craniectomy on intracranial pressure and cerebrospinal compensation following traumatic brain injury IVAN TIMOFEEV, M.R.C.S., 1 MAREK CZOSNYKA, PH.D.,
J Neurosurg 108:66 73, 2008 Effect of decompressive craniectomy on intracranial pressure and cerebrospinal compensation following traumatic brain injury IVAN TIMOFEEV, M.R.C.S., 1 MAREK CZOSNYKA, PH.D.,
NO CONFLICTS NO CONFLICTS
 Anesthesia and Critical Care Medicine Department of Surgical Specialties, Radiological Sciences and Public Health, University of Brescia; Department of Anesthesia, Critical Care and Emergency, Spedali
Anesthesia and Critical Care Medicine Department of Surgical Specialties, Radiological Sciences and Public Health, University of Brescia; Department of Anesthesia, Critical Care and Emergency, Spedali
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Cerebral autoregulation refers
 Cerebral autoregulation in pediatric traumatic brain injury* Monica S. Vavilala, MD; Lorri A. Lee, MD; Krishna Boddu, MD, FANZCA; Elizabeth Visco, CRNA; David W. Newell, MD; Jerry J. Zimmerman, PhD, MD;
Cerebral autoregulation in pediatric traumatic brain injury* Monica S. Vavilala, MD; Lorri A. Lee, MD; Krishna Boddu, MD, FANZCA; Elizabeth Visco, CRNA; David W. Newell, MD; Jerry J. Zimmerman, PhD, MD;
11 th Annual Cerebrovascular Symposium 5/11-12/2017. Hypertonic Use D E R E K C L A R K
 Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Severe Traumatic Brain Injury Protocol
 Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Comparison of frequency and time domain methods of assessment of cerebral. autoregulation in traumatic brain injury
 Comparison of frequency and time domain methods of assessment of cerebral autoregulation in traumatic brain injury Xiuyun Liu 1, MSc, Marek Czosnyka 1,5, PhD, Joseph Donnelly 1, MB ChB, Karol P. Budohoski
Comparison of frequency and time domain methods of assessment of cerebral autoregulation in traumatic brain injury Xiuyun Liu 1, MSc, Marek Czosnyka 1,5, PhD, Joseph Donnelly 1, MB ChB, Karol P. Budohoski
Functional cerebral monitoring in patients with critically illness
 Functional cerebral monitoring in patients with critically illness Anne-Marie Guerguerian MD PhD Assistant Professor of Critical Care Medicine & Pediatrics Scientist in Neurosciences & Mental Health, Research
Functional cerebral monitoring in patients with critically illness Anne-Marie Guerguerian MD PhD Assistant Professor of Critical Care Medicine & Pediatrics Scientist in Neurosciences & Mental Health, Research
Non-invasive assessment of intracranial pressure - a plugin function of ICM+ system
 Non-invasive assessment of intracranial pressure - a plugin function of ICM+ system B. Schmidt, M. Czosnyka *, P. Smielewski *, R. Plontke, J. Schwarze, J. Klingelhöfer Dept. of Neurology, Medical Centre
Non-invasive assessment of intracranial pressure - a plugin function of ICM+ system B. Schmidt, M. Czosnyka *, P. Smielewski *, R. Plontke, J. Schwarze, J. Klingelhöfer Dept. of Neurology, Medical Centre
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Increased risk of critical CBF levels in SAH patients with actual CPP below calculated optimal CPP
 Acta Neurochir (2017) 159:1065 1071 DOI 10.1007/s00701-017-3139-7 ORIGINAL ARTICLE - VASCULAR Increased risk of critical CBF levels in SAH patients with actual CPP below calculated optimal CPP Ulf Johnson
Acta Neurochir (2017) 159:1065 1071 DOI 10.1007/s00701-017-3139-7 ORIGINAL ARTICLE - VASCULAR Increased risk of critical CBF levels in SAH patients with actual CPP below calculated optimal CPP Ulf Johnson
12. Modelling of CSF compensation: Mathematical model (Marmarou). Mathematical modelling of pulsatile aqueductal CSF flow
. Mathematical modelling of pulsatile aqueductal CSF flow") 12. Modelling of CSF compensation: Mathematical model (Marmarou). Mathematical modelling of pulsatile aqueductal CSF flow Hydrocephalus Enlargement of CSF space Shunting? Revision? When? CSF dynamics Prof.
12. Modelling of CSF compensation: Mathematical model (Marmarou). Mathematical modelling of pulsatile aqueductal CSF flow Hydrocephalus Enlargement of CSF space Shunting? Revision? When? CSF dynamics Prof.
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY. Dr Nick Taylor MBBS FACEM
 PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
Assessment of Cerebrovascular Autoregulation in Head-Injured Patients. A Validation Study
 Assessment of Cerebrovascular Autoregulation in Head-Injured Patients A Validation Study Luzius A. Steiner, MD; Jonathan P. Coles, FRCA; Andrew J. Johnston, FRCA; Doris A. Chatfield, BSc; Peter Smielewski,
Assessment of Cerebrovascular Autoregulation in Head-Injured Patients A Validation Study Luzius A. Steiner, MD; Jonathan P. Coles, FRCA; Andrew J. Johnston, FRCA; Doris A. Chatfield, BSc; Peter Smielewski,
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Cerebral perfusion pressure management of severe diffuse head injury: Effect on brain compliance and intracranial pressure
 Original Article Cerebral perfusion pressure management of severe diffuse head injury: Effect on brain compliance and intracranial pressure S. Pillai, S. S. Praharaj, G. S. U. Rao,* V. R. S. Kolluri Departments
Original Article Cerebral perfusion pressure management of severe diffuse head injury: Effect on brain compliance and intracranial pressure S. Pillai, S. S. Praharaj, G. S. U. Rao,* V. R. S. Kolluri Departments
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases
 31 Original Article Indian Journal of Neurotrauma (IJNT) 2006, Vol. 3, No. 1, pp. 31-36 Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases Deepak Kumar Gupta
31 Original Article Indian Journal of Neurotrauma (IJNT) 2006, Vol. 3, No. 1, pp. 31-36 Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases Deepak Kumar Gupta
Cerebral hemodynamic effects of Cheyne-Stokes respiration in a patient with stroke.
 *Marked Revision Click here to download Marked Revision: manuscript_marked changes_final.docx Cerebral hemodynamic effects of Cheyne-Stokes respiration in a patient with stroke. Nogueira RC 1, Panerai
*Marked Revision Click here to download Marked Revision: manuscript_marked changes_final.docx Cerebral hemodynamic effects of Cheyne-Stokes respiration in a patient with stroke. Nogueira RC 1, Panerai
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS
 GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Transcranial Doppler Monitoring of Intracranial Pressure Plateau Waves
 Neurocrit Care (2017) 26:330 338 DOI 10.1007/s12028-016-0356-5 ORIGINAL ARTICLE Transcranial Doppler Monitoring of Intracranial Pressure Plateau Waves Danilo Cardim 1 Bernhard Schmidt 2 Chiara Robba 1,3
Neurocrit Care (2017) 26:330 338 DOI 10.1007/s12028-016-0356-5 ORIGINAL ARTICLE Transcranial Doppler Monitoring of Intracranial Pressure Plateau Waves Danilo Cardim 1 Bernhard Schmidt 2 Chiara Robba 1,3
Disclosures. Set up audience participation. Test question. Outline. Neuromonitoring What and When? IP for monitoring technology licensed to Medtronic
 Neuromonitoring What and When? Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set
Neuromonitoring What and When? Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set
Early abnormal transient hyperemic response test can predict delayed ischemic neurologic deficit in subarachnoid hemorrhage
 https://doi.org/10.1186/s13089-017-0079-7 ORIGINAL ARTICLE Open Access Early abnormal transient hyperemic response test can predict delayed ischemic neurologic deficit in subarachnoid hemorrhage Hosam
https://doi.org/10.1186/s13089-017-0079-7 ORIGINAL ARTICLE Open Access Early abnormal transient hyperemic response test can predict delayed ischemic neurologic deficit in subarachnoid hemorrhage Hosam
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
A comparison between the transfer function of ABP to ICP and compensatory reserve index in TBI
 Acta Neurochir Suppl (28) 12: 9 13 # Springer-Verlag 28 A comparison between the transfer function of AB to IC and compensatory reserve index in TBI Sima Shahsavari & Tomas McKelvey & Thomas Skoglund &
Acta Neurochir Suppl (28) 12: 9 13 # Springer-Verlag 28 A comparison between the transfer function of AB to IC and compensatory reserve index in TBI Sima Shahsavari & Tomas McKelvey & Thomas Skoglund &
Amethod is needed to continuously evaluate the state of
 Assessment of Cerebrovascular Autoregulation Changes of Highest Modal Frequency of Cerebrovascular Pressure Transmission With Cerebral Perfusion Pressure Michael L. Daley, PhD; Massroor Pourcyrous, MD;
Assessment of Cerebrovascular Autoregulation Changes of Highest Modal Frequency of Cerebrovascular Pressure Transmission With Cerebral Perfusion Pressure Michael L. Daley, PhD; Massroor Pourcyrous, MD;
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
The classic concept defining cerebrovascular tone is cerebral
 Dynamic Pressure Flow Velocity Relationships in the Human Cerebral Circulation Rune Aaslid, PhD; Stephanie R. Lash, MD; Gust H. Bardy, MD; William H. Gild, MD; David W. Newell, MD Background and Purpose
Dynamic Pressure Flow Velocity Relationships in the Human Cerebral Circulation Rune Aaslid, PhD; Stephanie R. Lash, MD; Gust H. Bardy, MD; William H. Gild, MD; David W. Newell, MD Background and Purpose
Plenary Address: Medico-Legal Issues in Neuro-intensive Care
 Plenary Address: Medico-Legal Issues in Neuro-intensive Care Dr Basil Matta Divisional Director, Emergency and Perioperative Care Cambridge University Hospitals NHS Foundation Trust Medico-Legal Issues
Plenary Address: Medico-Legal Issues in Neuro-intensive Care Dr Basil Matta Divisional Director, Emergency and Perioperative Care Cambridge University Hospitals NHS Foundation Trust Medico-Legal Issues
ICP (Intracranial Pressure) Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry
 Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry") ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
A Computer Model of Intracranial Pressure Dynamics during Traumatic Brain Injury that Explicitly Models Fluid Flows and Volumes
 Portland State University PDXScholar Systems Science Faculty Publications and Presentations Systems Science 2004 A Computer Model of Intracranial Pressure Dynamics during Traumatic Brain Injury that Explicitly
Portland State University PDXScholar Systems Science Faculty Publications and Presentations Systems Science 2004 A Computer Model of Intracranial Pressure Dynamics during Traumatic Brain Injury that Explicitly
TCD evaluation is used in several countries as a confirmatory test to assess CBF arrest
 ! BRAIN DEATH IS THE IRREVERSIBLE LOSS OF FUNCTION OF THE ENTIRE BRAIN INCLUDING THE BRAIN STEM Conventional Confirmatory Tests: EEG, CEREBRAL AGF, BRAIN SCINTIGRAPHY LOGISTICAL PROBLEMS TCD evaluation
! BRAIN DEATH IS THE IRREVERSIBLE LOSS OF FUNCTION OF THE ENTIRE BRAIN INCLUDING THE BRAIN STEM Conventional Confirmatory Tests: EEG, CEREBRAL AGF, BRAIN SCINTIGRAPHY LOGISTICAL PROBLEMS TCD evaluation
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Influence of general anaesthesia on slow waves of intracranial pressure
 Influence of general anaesthesia on slow waves of intracranial pressure Despina Aphrodite Lalou 1,2 Marek Czosnyka 1 Joseph Donnelly 1 Andrea Lavinio 3 John D. Pickard 1 Matthew Garnett 1 Zofia Czosnyka
Influence of general anaesthesia on slow waves of intracranial pressure Despina Aphrodite Lalou 1,2 Marek Czosnyka 1 Joseph Donnelly 1 Andrea Lavinio 3 John D. Pickard 1 Matthew Garnett 1 Zofia Czosnyka
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2): Oxford University Press
: Oxford University Press") Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized