Heavy Menstrual Bleeding. Mr Nick Nicholas MD FRCOG Grad Dip Law. Consultant Gynaecologist
|
|
|
- Iris Snow
- 5 years ago
- Views:
Transcription
1 Heavy Menstrual Bleeding Mr Nick Nicholas MD FRCOG Grad Dip Law. Consultant Gynaecologist
2 Why is HMB so important? 1:20 women aged consult their GP with HMB Once referred to gynaecologist, surgical intervention is highly likely 1in 5 women in UK will have hysterectomy before 60 In at least 50% of these,hmb will be the main problem In about 50% of all women who have a TAH for HMB they have a normal size uterus Only about 58% of women with HMB receive medical treatment prior to referral to a specialist NICE issued new guidelines in 2007
3 Incidence and Prevalence Affects approximately 880,000 women in England Annual rate of women with heavy menstrual bleeding presenting to services 6.00% 5.40% Rate of presentation 5.00% 4.00% 3.00% 2.00% 1.00% 0.67% 2.58% 1.94% 1.73% 2.10% 2.96% 4.47% 4.64% 0.00% 12 to to to to to to to to to 51 Age range
4 National RCOG Audit of HMB (2010) an Organisational audit of acute NHS trusts in England and Wales to describe the organisation of hospital gynaecological services, current referral patterns and local protocols with reference to the management of HMB a Prospective audit of patient-reported outcomes of women with HMB symptoms who attend outpatient gynaecology clinics between 1 February 2011 and 31 January 2012.


5 Relative rates of surgery for women with HMB in English PCTs between April 2006 and December 2009
6 Organisational audit of HMB n=221 NHS Hospitals 38.4% of responding hospitals reported that they had a dedicated menstrual bleeding clinic. The majority of hospitals reported the availability of ultrasound (80.0%), hysteroscopy (87.3%) and endometrial biopsy (97.7%) as well as a wide variety of surgical procedures and appropriate levels of investigations at the initial consultation.
7 Organisational audit of HMB 76.0% of hospitals provided an HMBspecific information leaflet for women, 8.3% referred women to a website for information and 19.8% did not provide written information. Only 29.9% of hospitals reported that they had a local, written protocol regarding the care and management of women with HMB.
8 Description of local HMB protocols Local HMB Guideline No of hospitals (214) % RCOG Standards NICE Care pathway protocol Locally developed protocol Reported having one but no proof No protocol
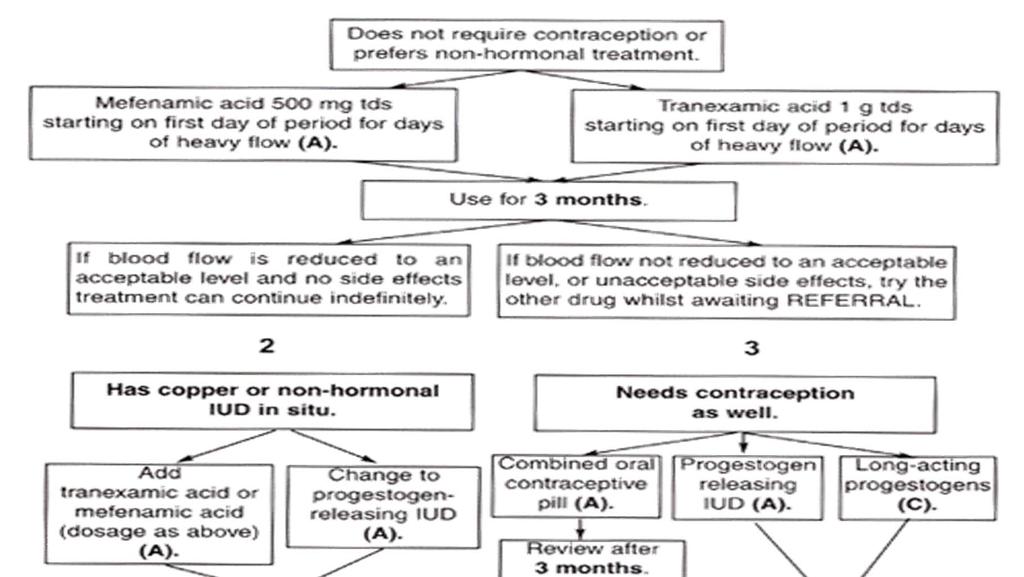
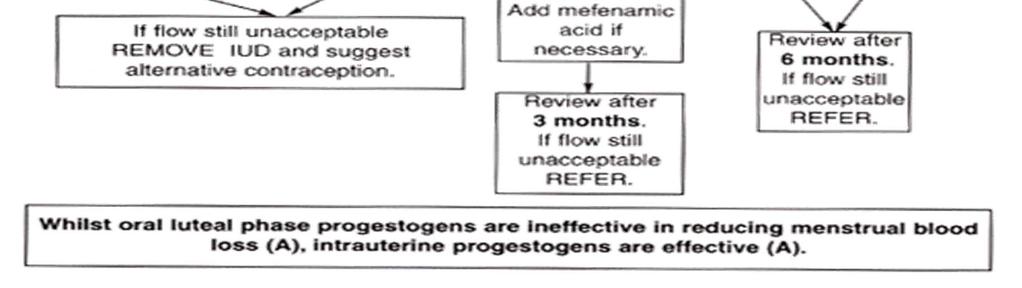
9 Management of HMB in Primary Care Taken from NICE Guideline Heavy Menstrual Bleeding January 2007
10 Risk factors for HMB Fibroids Polyps-do NOT cause HMB Blood Disorders Von Willebrands Disease Thyroid Disorders-NOT associated with HMB Endometriosis-usually causes pain but ALSO HMB
11 Risk factors for HMB Gynaecological conditions such as: uterine fibroids adenomyosis or endometriosis endometrial cancer unopposed oestrogen use Increase in age Ethnic group Sociocultural factors
12 Recommendations on definition of HMB For clinical purposes, HMB should be defined as excessive menstrual blood loss which interferes with the woman s physical, emotional, social and material quality of life, and which can occur alone or in combination with other symptoms. Any interventions should aim to improve quality of life measures. [D]
13 History taking for HMB Nature of bleeding Symptoms suggesting possible significant pathology ie pelvic pain and pressure symptoms To identify women s ideas, concerns, expectations and needs
14 Physical examination for HMB Physical examination of the woman by observation, abdominal palpation, visualisation of the cervix and bimanual (internal) examination has the purpose of detecting underlying pathology to inform treatment and the need for investigations
15 Recommendations on physical examination for HMB A physical examination should be carried out before all: LNG-IUS fittings investigations for structural abnormalities investigations for histological abnormalities. [D] Women with fibroids that are palpable abdominally or who have intra-cavity fibroids and/or whose uterine length as measured at ultrasound or hysteroscopy is greater than 12 cm should be offered immediate referral to a specialist.
16 Recommendations on laboratory tests for HMB A full blood count test should be carried out on all women with HMB. This should be done in parallel with any HMB treatment offered. [C] Testing for coagulation disorders (for example, von Willebrand disease) should be considered in women who have had HMB since menarche and have personal or family history suggesting a coagulation disorder. [C] A serum ferritin test should not routinely be carried out on women with HMB. [B] Female hormone testing should not be carried out on women with HMB. [C] Thyroid testing should only be carried out when other signs and symptoms of thyroid disease are present, otherwise DON T DO IT.[C]
17 Recommendations on investigations for HMB If appropriate, a biopsy should be taken to exclude endometrial cancer or atypical hyperplasia. Indications for a biopsy include, for example, persistent intermenstrual bleeding, and in women aged 45 and over treatment failure or ineffective treatment. [D] Imaging should be undertaken in the following circumstances: the uterus is palpable abdominally vaginal examination reveals a pelvic mass of uncertain origin pharmaceutical treatment fails. [D] Ultrasound is the first-line diagnostic tool for identifying structural abnormalities. [A]
18 Recommendations on investigations for HMB Hysteroscopy should be used as a diagnostic tool only when ultrasound results are inconclusive, for example, to determine the exact location of a fibroid or the exact nature of the abnormality. [A] If imaging shows the presence of uterine fibroids then appropriate treatment should be planned based on size, number and location of the fibroids. [D] Saline infusion sonography should not be used as a first-line diagnostic tool. [A] Magnetic resonance imaging (MRI) should not be used as a first-line diagnostic tool. [B] Dilatation and curettage alone should not be used as a diagnostic tool. [B] Where dilatation is required for non-hysteroscopic ablative procedures, hysteroscopy should be used immediately prior to the procedure to ensure correct placement of the device. [D]
19 Recommendations on education for women with HMB A woman with HMB referred to specialist care should be given information before her outpatient appointment. The Institute s information for patients ( Understanding NICE guidance Women should be made aware of the impact on fertility that any planned surgery or uterine artery embolisation (UAE) may have, and if a potential treatment (hysterectomy or ablation) involves the loss of fertility then opportunities for discussion should be made available. [D]
20 Intervention (LNG-IUS) Potential unwanted outcomes of interventions for HMB common = 1 in 100 chance, less common = 1 in 1000 chance, rare = 1 in chance, very rare = 1 in chance) Potential unwanted outcomes. Common: irregular bleeding that may last for over 6 months; hormone-related problems such as breast tenderness, acne or headaches, which, if present, are generally minor and transient Less common: amenorrhoea Rare: uterine perforation at the time of IUS insertion
21 Potential unwanted outcomes of interventions for HMB Intervention Tranexamic acid (NSAIDs) COCP Potential unwanted outcomes Less common: indigestion; diarrhoea; headaches Common: indigestion; diarrhoea Rare: worsening of asthma in sensitive individuals; peptic ulcers with possible bleeding and Peritonitis Common: mood changes; headaches; nausea; fluid retention; breast tenderness Rare: deep vein thrombosis; stroke; heart attacks
22 Potential unwanted outcomes of interventions for HMB Intervention Oral progestogen Injected progestogen Potential outcomes Common: weight gain; bloating; breast tenderness; headaches; acne (but all are usually minor and transient) Rare: depression Common: weight gain; irregular bleeding; amenorrhoea; premenstruallike syndrome (including bloating, fluid retention, breast tenderness)
23 Potential unwanted outcomes of interventions for HMB Intervention (GnRH-a Potential Outcomes Common: menopausal-like symptoms Less common: osteoporosis, with longer than 6 months use Endometrial ablation Common: vaginal discharge; increased period pain or cramping (even if no further bleeding); need for additional surgery Less common: infection Rare: perforation
24 Potential unwanted outcomes of interventions for HMB Intervention Uterine artery embolisation Common: persistent vaginal discharge; post embolisation syndrome pain, nausea, vomiting and fever (not involving hospitalisation) Less common: need for additional surgery; premature ovarian failure, particularly in women over 45 years old; haematoma Rare: haemorrhage; non-target embolisation causing tissue necrosis; infection causing septicaemia
25 Potential unwanted outcomes of interventions for HMB Intervention Myomectomy Possible Outcomes Less common: adhesions (which may lead to pain and/or impaired fertility); need for additional surgery; recurrence of fibroids; perforation (hysteroscopic route); infection Rare: haemorrhage
26 Potential unwanted outcomes of interventions for HMB Intervention Hysterectomy Possible Outcomes Less common: intra-operative haemorrhage; damage to other abdominal organs, such as the urinary tract or bowel; urinary dysfunction frequent passing of urine and incontinence Rare: thrombosis (DVT and clot on the lung) Very rare: death (Complications are more likely when hysterectomy is performed in the presence of fibroids)
27 Pharmacological Treatments Mirena IUCD Tranexamic Acid 1gm qds NSAIDs (mefanamic acid 500mgs tds) COCP Norethisterone (15 mg) daily from days 5 to 26
28 Pharmacological Treatments Injected long-acting progestogens.?gnrh analogues for fibroids DO NOT USE Danazol for HMB Oral progestogens given during the luteal phase only should not be used for the treatment of HMB Etamsylate should not be used for the treatment of HMB

29 Available surgical options for women with HMB at NHS hospitals in England and Wales
30 Surgical Options Endometrial ablative techniques (where fertility is not necessary, but contraception still necessary) Thermachoice Novasure MEA TCRE Dilatation and curettage should not be used as a therapeutic treatment
31 Surgical Options UAE, myomectomy or hysterectomy should be considered in cases of HMB where large fibroids ( > 3 cm in diameter) May need GNRH analogue
32 Surgical Options Hysterectomy NOT first line treatment solely for HMB should be considered only when: other treatment options have failed, are contraindicated or are declined by the woman there is a wish for amenorrhoea the woman (who has been fully informed) requests it the woman no longer wishes to retain her uterus and fertility.


33 Number of surgical operations for women with HMB in English NHS trusts between 1 April 1997 and 31 December 2009
34 When to refer? Palpable abdominal fibroids Intracavity fibroids Bulky uterus Uterine length at USS or hysteroscopy >12cm Failed medical treatment for?3/12 If no response to drugs Pt requesting surgical Rx Severe anaemia Drugs contraindicated/not tolerated Diagnosis uncertain
35 Costs and savings Recommendations with significant resource impact Annual cost millions full blood count investigations 0.9 transvaginal ultrasound investigations 10.4 endometrial biopsy for suspected endometrial cancer -0.9 pharmaceutical treatments levonorgestrelreleasing intrauterine system -0.6 substitution of hysterectomy with endometrial ablation -1.2 Total net cost of implementing the HMB guideline 8.7
36 Implementation advice on improving education and information provision for women with HMB Choice of treatment Women s preferences and choices and individualised options Shared decision making when uncertain Allow time to decide Opportunity to reconsider Opportunity for second opinion Woman s right to chose which option
37
38
39 Thank You
40 What this talk is about? National HMB Audit 2010 Organisational Management of HMB in Primary Care What to give? When to refer? Some Secondary Care considerations
41 Between 1997 and 2009, the rate of surgery decreased in women under 40 years of age, falling by around 50% in women under 35 years of age. By contrast, rates of surgery among older women have been increasing
Menstrual Disorders & Ambulatory Gynaecology
 Menstrual Disorders & Ambulatory Gynaecology Mr. Nagui Lewis Aziz M B, CH B, FRCOG Consultant Gynaecologist The Royal Oldham Hospital 01/09/2018 Heavy menstrual bleeding (HMB ) is a common problem responsible
Menstrual Disorders & Ambulatory Gynaecology Mr. Nagui Lewis Aziz M B, CH B, FRCOG Consultant Gynaecologist The Royal Oldham Hospital 01/09/2018 Heavy menstrual bleeding (HMB ) is a common problem responsible
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health and social care directorate. Quality standards and indicators.
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health and social care directorate Quality standards and indicators Briefing paper Quality standard topic: Heavy menstrual bleeding Output: Prioritised
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health and social care directorate Quality standards and indicators Briefing paper Quality standard topic: Heavy menstrual bleeding Output: Prioritised
Heavy menstrual bleeding: assessment and management
 Heavy menstrual bleeding: assessment and management NICE guideline Draft for consultation, August 0 This guideline covers assessing and treating heavy menstrual bleeding. It aims to help healthcare professionals
Heavy menstrual bleeding: assessment and management NICE guideline Draft for consultation, August 0 This guideline covers assessing and treating heavy menstrual bleeding. It aims to help healthcare professionals
Excessive menstrual blood loss
 Ian Chilcott Excessive menstrual blood loss >80mls - That interferes with physical, emotional, social and material quality of life 1 in 20 women aged 30 to 49 years consult their GP each year with menorrhagia
Ian Chilcott Excessive menstrual blood loss >80mls - That interferes with physical, emotional, social and material quality of life 1 in 20 women aged 30 to 49 years consult their GP each year with menorrhagia
NICE guideline Published: 14 March 2018 nice.org.uk/guidance/ng88
 Heavy menstrual bleeding: assessment and management NICE guideline Published: 14 March 2018 nice.org.uk/guidance/ng88 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Heavy menstrual bleeding: assessment and management NICE guideline Published: 14 March 2018 nice.org.uk/guidance/ng88 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Investigating HMB- an evidence based approach
 BSGE Meeting: Contemporary management of heavy menstrual bleeding (HMB) in primary and secondary care: (7 th December 2018, RCOG) Investigating HMB- an evidence based approach T. Justin Clark MB ChB, MD(Hons),
BSGE Meeting: Contemporary management of heavy menstrual bleeding (HMB) in primary and secondary care: (7 th December 2018, RCOG) Investigating HMB- an evidence based approach T. Justin Clark MB ChB, MD(Hons),
Abnormal uterine bleeding:
 Primary Care Women s Health Forum 16th June 2010 Abnormal uterine bleeding: The University Of Birmingham T Justin Clark MD (Hons), MRCOG Consultant Obstetrician and Gynaecologist Birmingham Women s Hospital
Primary Care Women s Health Forum 16th June 2010 Abnormal uterine bleeding: The University Of Birmingham T Justin Clark MD (Hons), MRCOG Consultant Obstetrician and Gynaecologist Birmingham Women s Hospital
Primary Care Gynaecology Guidelines: HEAVY REGULAR MENSTRUAL BLEEDING
 Primary Care Guidelines: HEAVY REGULAR MENSTRUAL BLEEDING
Primary Care Guidelines: HEAVY REGULAR MENSTRUAL BLEEDING
Dr Mary Birdsall. Fertility Associates Auckland
 Dr Mary Birdsall Fertility Associates Auckland Period Problems Mary Birdsall Medical Director Fertility Associates Auckland Period Problems Basic Physiology No Periods Irregular Periods Heavy Periods
Dr Mary Birdsall Fertility Associates Auckland Period Problems Mary Birdsall Medical Director Fertility Associates Auckland Period Problems Basic Physiology No Periods Irregular Periods Heavy Periods
Current approaches to managing heavy menstrual bleeding
 Drug review Heavy menstrual bleeding Current approaches to managing heavy menstrual bleeding Jasmine Tay BM BS, Shruti Mohan MRCOG and Jenny Higham FRCOG SPL The choice of drug treatment for heavy menstrual
Drug review Heavy menstrual bleeding Current approaches to managing heavy menstrual bleeding Jasmine Tay BM BS, Shruti Mohan MRCOG and Jenny Higham FRCOG SPL The choice of drug treatment for heavy menstrual
Medical Management of Fibroids Esmya. Dr Paula Briggs Consultant in Sexual and Reproductive Health
 Medical Management of Fibroids Esmya Dr Paula Briggs Consultant in Sexual and Reproductive Health Treatment options for Uterine Fibroids ESMYA Selective Uterine Artery Embolisation Fibroid ablation (hysteroscopic
Medical Management of Fibroids Esmya Dr Paula Briggs Consultant in Sexual and Reproductive Health Treatment options for Uterine Fibroids ESMYA Selective Uterine Artery Embolisation Fibroid ablation (hysteroscopic
Healthcare Education Research
 Healthcare Education Research Heavy menstrual bleeding: investigation, diagnosis & management An update for health professionals Assessment of heavy menstrual bleeding in primary care Dr Amanda Newman
Healthcare Education Research Heavy menstrual bleeding: investigation, diagnosis & management An update for health professionals Assessment of heavy menstrual bleeding in primary care Dr Amanda Newman
The 6 th Scientific Meeting of the Asia Pacific Menopause Federation
 Abnormal uterine bleeding in the perimenopause Perimenopausal menstrual problems are among the most common causes for family practitioner and specialist referral. Often it is due to the hormone changes
Abnormal uterine bleeding in the perimenopause Perimenopausal menstrual problems are among the most common causes for family practitioner and specialist referral. Often it is due to the hormone changes
Treatment of Heavy Menstrual Bleeding: Ludkin (Nurse Hysteroscopist, Bradford Royal Infirmary) & M Rogers (Advanced
 & M Rogers (Advanced") Treatment of Heavy Menstrual Bleeding: Nov 14 th 2013- Authors: Prof Sian Jones (Gynaecologist, Bradford Royal Infirmary, H Ludkin (Nurse Hysteroscopist, Bradford Royal Infirmary) & M Rogers (Advanced
Treatment of Heavy Menstrual Bleeding: Nov 14 th 2013- Authors: Prof Sian Jones (Gynaecologist, Bradford Royal Infirmary, H Ludkin (Nurse Hysteroscopist, Bradford Royal Infirmary) & M Rogers (Advanced
Fibroid mapping. Haitham Hamoda MD FRCOG Consultant Gynaecologist, Subspecialist in Reproductive Medicine & Surgery King s College Hospital
 Fibroid mapping Haitham Hamoda MD FRCOG Consultant Gynaecologist, Subspecialist in Reproductive Medicine & Surgery King s College Hospital Fibroids Common condition >70% of women by onset of menopause.
Fibroid mapping Haitham Hamoda MD FRCOG Consultant Gynaecologist, Subspecialist in Reproductive Medicine & Surgery King s College Hospital Fibroids Common condition >70% of women by onset of menopause.
CLEAR COVERAGE HYSTERECTOMY CHECKLISTS
 CLEAR COVERAGE HYSTERECTOMY CHECKLISTS Click on the link below to access the checklist sheet. Abnormal Uterine Bleeding Adenomyosis Chronic Abdominal or Pelvic Pain Endometriosis Fibroids General Guidelines
CLEAR COVERAGE HYSTERECTOMY CHECKLISTS Click on the link below to access the checklist sheet. Abnormal Uterine Bleeding Adenomyosis Chronic Abdominal or Pelvic Pain Endometriosis Fibroids General Guidelines
PATIENT GROUP CONDEMNS NICE REVISED HEAVY MENSTRUAL BLEEDING GUIDELINES UNSAFE FOR WOMEN MANY MORE WOMEN WILL DIE AND SUFFER SERIOUS COMPLICATIONS
 PRESS RELEASE For immediate release 20 th February 2018 PATIENT GROUP CONDEMNS NICE REVISED HEAVY MENSTRUAL BLEEDING GUIDELINES UNSAFE FOR WOMEN MANY MORE WOMEN WILL DIE AND SUFFER SERIOUS COMPLICATIONS
PRESS RELEASE For immediate release 20 th February 2018 PATIENT GROUP CONDEMNS NICE REVISED HEAVY MENSTRUAL BLEEDING GUIDELINES UNSAFE FOR WOMEN MANY MORE WOMEN WILL DIE AND SUFFER SERIOUS COMPLICATIONS
Modern Management of Fibroids
 Modern Management of Fibroids Mr Narendra Pisal The Portland Hospital Fibroids Very common 20-40% of all women Up to 80% of black women by 50y Most fibroids are asymptomatic 50% will have significant symptoms
Modern Management of Fibroids Mr Narendra Pisal The Portland Hospital Fibroids Very common 20-40% of all women Up to 80% of black women by 50y Most fibroids are asymptomatic 50% will have significant symptoms
Gynaecology Cancer Red Flags. Dr Dina Bisson Consultant Obstetrician and Gynaecologist Southmead Hospital North Bristol NHS Trust 27 April 2017
 Gynaecology Cancer Red Flags Dr Dina Bisson Consultant Obstetrician and Gynaecologist Southmead Hospital North Bristol NHS Trust 27 April 2017 Gynaecological Cancers Endometrial Cancer Ovarian Cancer Cervical
Gynaecology Cancer Red Flags Dr Dina Bisson Consultant Obstetrician and Gynaecologist Southmead Hospital North Bristol NHS Trust 27 April 2017 Gynaecological Cancers Endometrial Cancer Ovarian Cancer Cervical
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Management of Gynae Problems in Primary Care David Griffiths FRCOG The Great Western Hospital Swindon. A brief overview
 Management of Gynae Problems in Primary Care David Griffiths FRCOG The Great Western Hospital Swindon A brief overview Pelvic Pain Challenge to the physician In UK 1 Million sufferers 20% of all gynae
Management of Gynae Problems in Primary Care David Griffiths FRCOG The Great Western Hospital Swindon A brief overview Pelvic Pain Challenge to the physician In UK 1 Million sufferers 20% of all gynae
Uterine artery embolisation for treating adenomyosis
 Uterine artery embolisation for treating Issued: December 2013 guidance.nice.org.uk/ipg NICE has accredited the process used by the NICE Interventional Procedures Programme to produce interventional procedures
Uterine artery embolisation for treating Issued: December 2013 guidance.nice.org.uk/ipg NICE has accredited the process used by the NICE Interventional Procedures Programme to produce interventional procedures
An Update on the Management of Heavy Menstrual Bleeding
 An Update on the Management of Heavy Menstrual Bleeding Sonia WM LAI MBBS, MRCOG SL MOK MBBS SK LAM MBBS, FRCOG Department of Obstetrics and Gynaecology, Kwong Wah Hospital, 25 Waterloo Road, Kowloon,
An Update on the Management of Heavy Menstrual Bleeding Sonia WM LAI MBBS, MRCOG SL MOK MBBS SK LAM MBBS, FRCOG Department of Obstetrics and Gynaecology, Kwong Wah Hospital, 25 Waterloo Road, Kowloon,
Levosert levonorgestrel 20mcg/24hour intrauterine device
 Levosert levonorgestrel 20mcg/24hour intrauterine device Verdict: Formulary inclusion: Formulary category: Restrictions: Reason for inclusion: Link to formulary: Link to medicine review summary: Levosert
Levosert levonorgestrel 20mcg/24hour intrauterine device Verdict: Formulary inclusion: Formulary category: Restrictions: Reason for inclusion: Link to formulary: Link to medicine review summary: Levosert
5/5/2010 FINANCIAL DISCLOSURE. Abnormal Uterine Bleeding. Is This A Problem? About me % of visits to gynecologist
 Abnormal Uterine FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology May 5, 2010 About
Abnormal Uterine FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology May 5, 2010 About
Endometriosis factsheet
 Endometriosis factsheet Endorsed by What is endometriosis? Do you see female patients? Do they have painful periods? Pain pre or post their periods? Painful sex? Do they suffer chronic pain, which may
Endometriosis factsheet Endorsed by What is endometriosis? Do you see female patients? Do they have painful periods? Pain pre or post their periods? Painful sex? Do they suffer chronic pain, which may
Policy for Hysteroscopy Page 1 of 5. Policy for Hysteroscopy. V1.1 OPCS/ICD codes added. Version of: Version of: March 2018
 Policy for Hysteroscopy Version of: 16.03.2018 Version of: March 2018 Version Number: Changes Made: V1.1 OPCS/ICD codes added. V1 Ratified policy agreed by Healthier Lancashire and South Cumbria s Joint
Policy for Hysteroscopy Version of: 16.03.2018 Version of: March 2018 Version Number: Changes Made: V1.1 OPCS/ICD codes added. V1 Ratified policy agreed by Healthier Lancashire and South Cumbria s Joint
Conflicts 10/5/2016. Abnormal Uterine Bleeding. Objectives Review diagnosis and updated nomenclature. Management options for acute and chronic AUB.
 Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust
 Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust Endometriosis one of the most common conditions requiring treatment Growth of endometrial like tissue outside
Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust Endometriosis one of the most common conditions requiring treatment Growth of endometrial like tissue outside
Endometrial Ablation for Heavy Menstrual Bleeding. Jonathan Lord Consultant gynaecologist
 Endometrial Ablation for Heavy Menstrual Bleeding Jonathan Lord Consultant gynaecologist Affiliation: Declaration of Interests NICE HMB guideline committee member Expenses & honaria: Hologic (manufacturer
Endometrial Ablation for Heavy Menstrual Bleeding Jonathan Lord Consultant gynaecologist Affiliation: Declaration of Interests NICE HMB guideline committee member Expenses & honaria: Hologic (manufacturer
The facts about Endometriosis
 The facts about Endometriosis A specialist team of health professionals with the expertise to provide personalised and up to date treatment for women with endometriosis. Nurse Co ordinator Gynaecologists
The facts about Endometriosis A specialist team of health professionals with the expertise to provide personalised and up to date treatment for women with endometriosis. Nurse Co ordinator Gynaecologists
Hysteroscopy. Department of Gynaecology. Patient information
 Hysteroscopy Department of Gynaecology Patient information What is is a hysteroscopy? a Hysteroscopy? A hysteroscopy is a procedure during which the inside of the uterus (womb) is examined using a thin
Hysteroscopy Department of Gynaecology Patient information What is is a hysteroscopy? a Hysteroscopy? A hysteroscopy is a procedure during which the inside of the uterus (womb) is examined using a thin
Endometriosis. *Chocolate cyst in the ovary
 Endometriosis What is endometriosis? Endometriosis is a common condition in young women. It's chronic, painful, and it often progressively gets worse over the time. *Chocolate cyst in the ovary Normally,
Endometriosis What is endometriosis? Endometriosis is a common condition in young women. It's chronic, painful, and it often progressively gets worse over the time. *Chocolate cyst in the ovary Normally,
Menorrhagia Update. Simon Edmonds Middlemore Hospital Ascot Central Women s Clinic Auckland
 Menorrhagia Update Simon Edmonds Middlemore Hospital Ascot Central Women s Clinic Auckland What is it? Subjective Excessive blood loss at time of menstruation flooding heavy clots Objective > 80mls volume
Menorrhagia Update Simon Edmonds Middlemore Hospital Ascot Central Women s Clinic Auckland What is it? Subjective Excessive blood loss at time of menstruation flooding heavy clots Objective > 80mls volume
Menopause management NICE Implementation
 Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Your visit to the Outpatient Hysteroscopy Clinic
 Your visit to the Outpatient Hysteroscopy Clinic Department of Gynaecology Patient Information What What is the is an Outpatient outpatient Cystoscopy hysteroscopy? Clinic? An outpatient hysteroscopy means
Your visit to the Outpatient Hysteroscopy Clinic Department of Gynaecology Patient Information What What is the is an Outpatient outpatient Cystoscopy hysteroscopy? Clinic? An outpatient hysteroscopy means
COLLEGE OF OBSTETRICIANS AND GYNAECOLOGISTS, SINGAPORE 2006
 COLLEGE OF OBSTETRICIANS AND GYNAECOLOGISTS, SINGAPORE 2006 CONSENSUS STATEMENT ON THE MANAGEMENT AND EVALUATION OF MENORRHAGIA (INCLUDING MANAGEMENT OF FIBROIDS) Introduction Menorrhagia is defined as
COLLEGE OF OBSTETRICIANS AND GYNAECOLOGISTS, SINGAPORE 2006 CONSENSUS STATEMENT ON THE MANAGEMENT AND EVALUATION OF MENORRHAGIA (INCLUDING MANAGEMENT OF FIBROIDS) Introduction Menorrhagia is defined as
Cervical Cancer - Suspected
 Cervical Cancer - Suspected Presentation for patients Asymptomatic presentation Symptomatic presentation History and examination Consider differential diagnoses RED FLAG! Cervix appears normal after examination
Cervical Cancer - Suspected Presentation for patients Asymptomatic presentation Symptomatic presentation History and examination Consider differential diagnoses RED FLAG! Cervix appears normal after examination
Endometriosis. What you need to know. 139 Dumaresq Street Campbelltown Phone Fax
 Endometriosis What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 What is Endometriosis? Endometriosis is a condition whereby the lining
Endometriosis What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 What is Endometriosis? Endometriosis is a condition whereby the lining
Laparoscopic Hysterectomy
 Laparoscopic Hysterectomy A/Professor Alan Lam MBBS (Hons) FRCOG FRACOG Director Laparoscopic hysterectomy Laparoscopic hysterectomy hysterectomy Laparoscopic hysterectomy Laparoscopic Laparoscopic hysterectomy
Laparoscopic Hysterectomy A/Professor Alan Lam MBBS (Hons) FRCOG FRACOG Director Laparoscopic hysterectomy Laparoscopic hysterectomy hysterectomy Laparoscopic hysterectomy Laparoscopic Laparoscopic hysterectomy
Hysteroscopy. What you need to know. 139 Dumaresq Street Campbelltown Phone Fax
 Hysteroscopy What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 HYSTEROSCOPY AND DILATATION & CURETTAGE OF THE UTERUS Introduction I have
Hysteroscopy What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 HYSTEROSCOPY AND DILATATION & CURETTAGE OF THE UTERUS Introduction I have
Dysmenorrhoea Gynaecology د.شيماءعبداالميرالجميلي. Aetiology of secondary dysmenorrhea
 30-11-2014 Gynaecology Dysmenorrhoea د.شيماءعبداالميرالجميلي Dysmenorrhoea is defined as painful menstruation. It is experienced by 45 95 per cent of women of reproductive age.primary Spasmodic Dysmenorrhea
30-11-2014 Gynaecology Dysmenorrhoea د.شيماءعبداالميرالجميلي Dysmenorrhoea is defined as painful menstruation. It is experienced by 45 95 per cent of women of reproductive age.primary Spasmodic Dysmenorrhea
Pelvic Pain. What you need to know. 139 Dumaresq Street Campbelltown Phone Fax
 Pelvic Pain What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 PELVIC PAIN This is a common problem and most women experience some form
Pelvic Pain What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 PELVIC PAIN This is a common problem and most women experience some form
Saint Mary s Hospital. Gynaecology Unit. Saint Mary s Hospital. Endometriosis. Information For Patients
 Saint Mary s Hospital Gynaecology Unit Saint Mary s Hospital Endometriosis Information For Patients Contents What is endometriosis?... 3 What happens?... 3 Who is affected?... 3 Outlook... 3 What are the
Saint Mary s Hospital Gynaecology Unit Saint Mary s Hospital Endometriosis Information For Patients Contents What is endometriosis?... 3 What happens?... 3 Who is affected?... 3 Outlook... 3 What are the
PALM-COEIN: Your AUB Counseling Guide
 PALM-COEIN: Your AUB Counseling Guide 10 million+ Treat the cause, not the symptom In the U.S, more than 10 million women between the ages of 35 and 49 are affected by AUB 1 Diagnosis Cause Structural
PALM-COEIN: Your AUB Counseling Guide 10 million+ Treat the cause, not the symptom In the U.S, more than 10 million women between the ages of 35 and 49 are affected by AUB 1 Diagnosis Cause Structural
All referrals for out-patient appointments can also be discussed with the Obstetrics and Gynaecology registrar as necessary. Presence of ascites
 Gynaecology Referral Pathway for GPs to Aid Triage for Gynaecology Services in the Rotunda For acute gynaecology (suspected torsion, acute PID, etc..) or acute early pregnancy referrals please consider
Gynaecology Referral Pathway for GPs to Aid Triage for Gynaecology Services in the Rotunda For acute gynaecology (suspected torsion, acute PID, etc..) or acute early pregnancy referrals please consider
FDA-Approved Patient Labeling Patient Information Mirena (mur-ā-nah) (levonorgestrel-releasing intrauterine system)
 (levonorgestrel-releasing intrauterine system)") FDA-Approved Patient Labeling Patient Information Mirena (mur-ā-nah) (levonorgestrel-releasing intrauterine system) Mirena does not protect against HIV infection (AIDS) and other sexually transmitted infections
FDA-Approved Patient Labeling Patient Information Mirena (mur-ā-nah) (levonorgestrel-releasing intrauterine system) Mirena does not protect against HIV infection (AIDS) and other sexually transmitted infections
What is Endometriosis?
 What is Endometriosis? Obstetrics & Gynaecology Women & Children s Services This leaflet has been designed to give you important information about your condition / procedure, and to answer some common
What is Endometriosis? Obstetrics & Gynaecology Women & Children s Services This leaflet has been designed to give you important information about your condition / procedure, and to answer some common
Out Patient Hysteroscopy Unit GUIDELINES
 Out Patient Hysteroscopy Unit GUIDELINES 1 AIMS The aim of the menstrual assessment clinic [MAC] (incorporating outpatient hysteroscopy) at Queen Charlotte s and Chelsea Hospital will be to provide a one-stop
Out Patient Hysteroscopy Unit GUIDELINES 1 AIMS The aim of the menstrual assessment clinic [MAC] (incorporating outpatient hysteroscopy) at Queen Charlotte s and Chelsea Hospital will be to provide a one-stop
National Heavy Menstrual Bleeding Audit
 First Annual Report May 2011 Funding provided by: National Heavy Menstrual Bleeding Audit A national audit to assess patient outcomes and experiences of care for women with heavy menstrual bleeding in
First Annual Report May 2011 Funding provided by: National Heavy Menstrual Bleeding Audit A national audit to assess patient outcomes and experiences of care for women with heavy menstrual bleeding in
By Dr Rukhsana Hussain 5 th April 2016
 By Dr Rukhsana Hussain 5 th April 2016 1. Is it indicated? Vasomotor symptoms (flushes/sweats) Vaginal atrophy Cycle control (In perimenopause consider low dose COCP (age
By Dr Rukhsana Hussain 5 th April 2016 1. Is it indicated? Vasomotor symptoms (flushes/sweats) Vaginal atrophy Cycle control (In perimenopause consider low dose COCP (age
INTERVENTIONAL PROCEDURES PROGRAMME
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of balloon thermal endometrial ablation (Cavaterm) Introduction This overview has been prepared
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of balloon thermal endometrial ablation (Cavaterm) Introduction This overview has been prepared
University Gynecologic Oncology Associates
 University Gynecologic Oncology Associates Medical History Form Date: Name: Date of Birth: / / GYNE HISTORY Age of first period? If you no longer have periods, at what age did they stop? Are you pregnant
University Gynecologic Oncology Associates Medical History Form Date: Name: Date of Birth: / / GYNE HISTORY Age of first period? If you no longer have periods, at what age did they stop? Are you pregnant
Subject Index. Cavaterm, endometrial ablation complications 146, 150 contraindications 152 cost analysis compared with hysterectomy
 OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Abnormal uterine bleeding, see also Adenomyosis, Endometrial cancer, Menorrhagia dilatation and curettage 21, 22, 25 hysteroscopy of premenopausal women anesthesia
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Abnormal uterine bleeding, see also Adenomyosis, Endometrial cancer, Menorrhagia dilatation and curettage 21, 22, 25 hysteroscopy of premenopausal women anesthesia
GLOBAL ENDOMETRIAL ABLATION TECHNOLOGY
 GLOBAL ENDOMETRIAL ABLATION TECHNOLOGY Training: Part 1 Anatomy and Physiology Female Anatomy Normal Uterus Female Anatomy Normal Uterus Female Anatomy Uterine Positions Abnormal Uterus Retroflexed Normal
GLOBAL ENDOMETRIAL ABLATION TECHNOLOGY Training: Part 1 Anatomy and Physiology Female Anatomy Normal Uterus Female Anatomy Normal Uterus Female Anatomy Uterine Positions Abnormal Uterus Retroflexed Normal
Heavy Menstrual Bleeding (HMB) Dysmenorrhoea / Endometriosis Endometrial Hyperplasia HRT
 Dysmenorrhoea / Endometriosis Endometrial Hyperplasia HRT") Heavy Menstrual Bleeding (HMB) Dysmenorrhoea / Endometriosis Endometrial Hyperplasia HRT Janesh Gupta Professor of Obstetrics and Gynaecology Birmingham Women s Hospital Heavy Menstrual Bleeding (HMB)
Heavy Menstrual Bleeding (HMB) Dysmenorrhoea / Endometriosis Endometrial Hyperplasia HRT Janesh Gupta Professor of Obstetrics and Gynaecology Birmingham Women s Hospital Heavy Menstrual Bleeding (HMB)
Instruction for the patient
 WS 4 Case 3 STI and IUD Your situation Instruction for the patient You are 32 years old, divorced and have one child; you have just started a new relationship You underwent surgical resection of the left
WS 4 Case 3 STI and IUD Your situation Instruction for the patient You are 32 years old, divorced and have one child; you have just started a new relationship You underwent surgical resection of the left
Gynaecological Oncology Cases
 Gynaecological Oncology Cases 1. Tamoxifen and the endometrium 2. Cancer and the older woman Dr Julie M Lamont Consultant Gynaecological Oncologist Epworth Freemasons Hospital 21 st April 2015 Mrs FS 66
Gynaecological Oncology Cases 1. Tamoxifen and the endometrium 2. Cancer and the older woman Dr Julie M Lamont Consultant Gynaecological Oncologist Epworth Freemasons Hospital 21 st April 2015 Mrs FS 66
Management of Endometrial Hyperplasia
 Management of Endometrial Hyperplasia Green-top Guideline No. 67 RCOG/SGE Joint Guideline February 2016 Management of Endometrial Hyperplasia This is the first edition of this guideline.this is a joint
Management of Endometrial Hyperplasia Green-top Guideline No. 67 RCOG/SGE Joint Guideline February 2016 Management of Endometrial Hyperplasia This is the first edition of this guideline.this is a joint
Endometriosis Information Leaflet
 Endometriosis Information Leaflet What is Endometriosis? Endometriosis is a condition where tissue similar to the lining of the womb (endometrium) is found outside the womb. About 1 out of 10 women of
Endometriosis Information Leaflet What is Endometriosis? Endometriosis is a condition where tissue similar to the lining of the womb (endometrium) is found outside the womb. About 1 out of 10 women of
Menopause & HRT. Rosie & Alex. Image:
 Menopause & HRT Rosie & Alex Image: http://www.keepcalm-o-matic.co.uk/ Menopause The permanent cessation of menstruation for 12 months When does it happen? Average age 51 Image: Nature Medicine - 12, 612-613
Menopause & HRT Rosie & Alex Image: http://www.keepcalm-o-matic.co.uk/ Menopause The permanent cessation of menstruation for 12 months When does it happen? Average age 51 Image: Nature Medicine - 12, 612-613
Topics. Periods Menopause & HRT Contraception Vulva problems
 Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Frequency of menses. Duration of menses 3 days to 7 days. Flow/amount of menses Average blood loss with menstruation is 60-80cc.
 Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
Gynecologic Decision Making Based on Sonographic Findings
 Gynecologic Decision Making Based on Sonographic Findings Mindy Goldman, MD Department of Obstetrics & Gynecology & Vickie A. Feldstein, MD Department of Radiology University of California, San Francisco
Gynecologic Decision Making Based on Sonographic Findings Mindy Goldman, MD Department of Obstetrics & Gynecology & Vickie A. Feldstein, MD Department of Radiology University of California, San Francisco
Fibroids: diagnosis and management
 Link to this article online for CPD/CME credits 1 University of Glasgow, Glasgow Royal Infirmary Campus, Glasgow G31 2ER, UK 2 University of Birmingham, Birmingham Women s Hospital, Birmingham, UK 3 The
Link to this article online for CPD/CME credits 1 University of Glasgow, Glasgow Royal Infirmary Campus, Glasgow G31 2ER, UK 2 University of Birmingham, Birmingham Women s Hospital, Birmingham, UK 3 The
Perimenopausal DUB. Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario
 Perimenopausal DUB Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario Objectives Clinicians will: Make a confident diagnosis for Perimenopausal DUB (know how/when to
Perimenopausal DUB Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario Objectives Clinicians will: Make a confident diagnosis for Perimenopausal DUB (know how/when to
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE GUIDANCE EXECUTIVE (GE)
") NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE GUIDANCE EXECUTIVE (GE) Review of TA78 fluid filled thermal balloon and microwave endometrial ablation for menstrual bleeding This guidance was issued
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE GUIDANCE EXECUTIVE (GE) Review of TA78 fluid filled thermal balloon and microwave endometrial ablation for menstrual bleeding This guidance was issued
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal myomectomy in leiomyoma management, 77 Abnormal uterine bleeding (AUB) described, 103 105 normal menstrual bleeding vs., 104
Index Note: Page numbers of article titles are in boldface type. A Abdominal myomectomy in leiomyoma management, 77 Abnormal uterine bleeding (AUB) described, 103 105 normal menstrual bleeding vs., 104
Gayatrri Anipindi *, Vani I. Original Research Article. Abstract
 Original Research Article Role of levonorgestrel releasing intrauterine device in management of heavy menstrual bleeding: A safe and effective option for all PALM COEIN variants Gayatrri Anipindi *, Vani
Original Research Article Role of levonorgestrel releasing intrauterine device in management of heavy menstrual bleeding: A safe and effective option for all PALM COEIN variants Gayatrri Anipindi *, Vani
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre
 Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
Freedom of Information
 ND ref. FOI/16/309 Freedom of Information Thank you for your 19/10/16 request for the following information: Under the Freedom of Information Act, please could you fill out the following Freedom of Information
ND ref. FOI/16/309 Freedom of Information Thank you for your 19/10/16 request for the following information: Under the Freedom of Information Act, please could you fill out the following Freedom of Information
Dr Devashana Gupta. Repromed Auckland. 17:30-18:00 Fibroids, Endometriosis and DUB
 Dr Devashana Gupta Repromed Auckland 17:30-18:00 Fibroids, Endometriosis and DUB Fibroids, Endometriosis and AUB Dr Devashana Gupta 9 th June 2018 Abnormal uterine bleeding PALM-COEIN 3 What is abnormal
Dr Devashana Gupta Repromed Auckland 17:30-18:00 Fibroids, Endometriosis and DUB Fibroids, Endometriosis and AUB Dr Devashana Gupta 9 th June 2018 Abnormal uterine bleeding PALM-COEIN 3 What is abnormal
Menopause & HRT. Matt McKenna Elliot Davis
 Menopause & HRT Matt McKenna Elliot Davis Menopause Before age 40: Premature Menopause After 12 months clinical diagnosis made Depletion of Ovarian Follicles Oestrogen Progesterone LH FSH Spontaneous Amemorrhoea
Menopause & HRT Matt McKenna Elliot Davis Menopause Before age 40: Premature Menopause After 12 months clinical diagnosis made Depletion of Ovarian Follicles Oestrogen Progesterone LH FSH Spontaneous Amemorrhoea
THE EFFECTIVENESS OF THE MIRENA COIL (LEVONORGESTREL-RELEASING INTRAUTERINE SYSTEM) IN MENORRHAGIA
 IN MENORRHAGIA") THE EFFECTIVENESS OF THE MIRENA COIL (LEVONORGESTREL-RELEASING INTRAUTERINE SYSTEM) IN MENORRHAGIA A West Midlands Development and Evaluation Service Report Authors: Antony Stewart, Carole Cummins, Lisa
THE EFFECTIVENESS OF THE MIRENA COIL (LEVONORGESTREL-RELEASING INTRAUTERINE SYSTEM) IN MENORRHAGIA A West Midlands Development and Evaluation Service Report Authors: Antony Stewart, Carole Cummins, Lisa
Vani Lingam Consultant Obstetrician and Gynaecologist Queens Hospital Burton NHS Trust 13 th June
 Vani Lingam Consultant Obstetrician and Gynaecologist Queens Hospital Burton NHS Trust 13 th June Definition of normal menstruation Cycle Length Cycle predictability Duration Volume of blood flow Cycle
Vani Lingam Consultant Obstetrician and Gynaecologist Queens Hospital Burton NHS Trust 13 th June Definition of normal menstruation Cycle Length Cycle predictability Duration Volume of blood flow Cycle
Endometrial line thickness in different conditions.
 Endometrial line thickness in different conditions 1 Endometrial thickens in response to Rising estrogen levels during the menstrual cycle and then shedding endometrial at the times of menses 2 The thickens
Endometrial line thickness in different conditions 1 Endometrial thickens in response to Rising estrogen levels during the menstrual cycle and then shedding endometrial at the times of menses 2 The thickens
Laparoscopy-Hysteroscopy
 Laparoscopy-Hysteroscopy Patient Information Laparoscopy The laparoscope, a surgical instrument similar to a telescope, is inserted through a small incision (cut) in the belly button during laparoscopy.
Laparoscopy-Hysteroscopy Patient Information Laparoscopy The laparoscope, a surgical instrument similar to a telescope, is inserted through a small incision (cut) in the belly button during laparoscopy.
Endometrial Cancer Biopsy of the endometrium Evaluation of women of all ages
 Endometrial Cancer Biopsy of the endometrium Evaluation of women of all ages Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Health System Ann Arbor, Michigan Cancer of the
Endometrial Cancer Biopsy of the endometrium Evaluation of women of all ages Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Health System Ann Arbor, Michigan Cancer of the
Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts
 Benefits & Risks - The Facts") Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts HRT is a prescription only treatment that replaces some of the lost oestrogen and progesterone hormones which occur during menopause. It can
Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts HRT is a prescription only treatment that replaces some of the lost oestrogen and progesterone hormones which occur during menopause. It can
Information for you. Managing premenstrual syndrome (PMS) What is PMS?
 What is PMS?") Managing premenstrual syndrome (PMS) Information for you Published in August 2009 What is PMS? Premenstrual syndrome or PMS is the name given to a collection of physical and emotional symptoms that can
Managing premenstrual syndrome (PMS) Information for you Published in August 2009 What is PMS? Premenstrual syndrome or PMS is the name given to a collection of physical and emotional symptoms that can
The Centre for Reproductive Medicine HYSTERECTOMY
 The Centre for Reproductive Medicine PO Box 20559 Nimbin NSW 2480 Australia Maxwell Brinsmead MB BS PhD MRCOG FRANZCOG Phone + 61 409 870 346 Retired Obstetrician & Gynaecologist E-mail max@brinsmead.net.au
The Centre for Reproductive Medicine PO Box 20559 Nimbin NSW 2480 Australia Maxwell Brinsmead MB BS PhD MRCOG FRANZCOG Phone + 61 409 870 346 Retired Obstetrician & Gynaecologist E-mail max@brinsmead.net.au
Pathway Gynaecology Cancer & Diagnostic Protocol for Inter Trust transfer
 NICaN Pathway Gynaecology Cancer & Diagnostic Protocol for Inter Trust transfer Timed schedules to enable the proactive management of the patient from point of receipt of referral to first definitive treatment
NICaN Pathway Gynaecology Cancer & Diagnostic Protocol for Inter Trust transfer Timed schedules to enable the proactive management of the patient from point of receipt of referral to first definitive treatment
Mr Doug Barclay Gynaecologist Ascot Central Women s Clinic Auckland. Mr Simon Edmonds Gynaecologist Middlemore Hospital Auckland
 Mr Doug Barclay Gynaecologist Ascot Central Women s Clinic Auckland Mr Simon Edmonds Gynaecologist Middlemore Hospital Auckland 16:30-17:25 WS #69: Practical Mirena Insertion and Pipelle Endometrial Sampling
Mr Doug Barclay Gynaecologist Ascot Central Women s Clinic Auckland Mr Simon Edmonds Gynaecologist Middlemore Hospital Auckland 16:30-17:25 WS #69: Practical Mirena Insertion and Pipelle Endometrial Sampling
Information for you. Managing premenstrual syndrome (PMS) What is PMS?
 What is PMS?") Managing premenstrual syndrome (PMS) Information for you Published in August 2009 What is PMS? Premenstrual syndrome or PMS is the name given to a collection of physical and emotional symptoms that can
Managing premenstrual syndrome (PMS) Information for you Published in August 2009 What is PMS? Premenstrual syndrome or PMS is the name given to a collection of physical and emotional symptoms that can
bleeding Studies naar de diagnostiek van endom triumcarcinoom bij vrouwen met postm nopauzaal bloedverlies. Studies on the
 Studies on the diagnosis of endometria cancer in women with postmenopausal bleeding. Studies naar de diagnostiek va endometriumcarcinoom bij vrouwen m postmenopauzaal bloedverlies. Studies on the diagnosis
Studies on the diagnosis of endometria cancer in women with postmenopausal bleeding. Studies naar de diagnostiek va endometriumcarcinoom bij vrouwen m postmenopauzaal bloedverlies. Studies on the diagnosis
Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital
 Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital Touchdown to CME Eighth District Academy of Osteopathic Medicine & Surgery October 8. 2017 Goals
Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital Touchdown to CME Eighth District Academy of Osteopathic Medicine & Surgery October 8. 2017 Goals
Ovaries: In Sickness and Health. Mr N Pisal Consultant Gynaecologist The Portland Hospital
 Ovaries: In Sickness and Health Mr N Pisal Consultant Gynaecologist The Portland Hospital Topics for discussion How to assess ovarian function? AMH PCOS Ovarian pain Ovarian cysts Ovarian screening Menopause
Ovaries: In Sickness and Health Mr N Pisal Consultant Gynaecologist The Portland Hospital Topics for discussion How to assess ovarian function? AMH PCOS Ovarian pain Ovarian cysts Ovarian screening Menopause
INTERVENTIONAL PROCEDURES PROGRAMME
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of microwave endometrial ablation Introduction This overview has been prepared to assist
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of microwave endometrial ablation Introduction This overview has been prepared to assist
Hysteroscopy Clinic. Patient Information. Women and Children - Gynaecology
 8 Hysteroscopy Clinic Patient Information Women and Children - Gynaecology When a woman is first told that she has a gynaecological condition that requires further investigation at a specialised hospital
8 Hysteroscopy Clinic Patient Information Women and Children - Gynaecology When a woman is first told that she has a gynaecological condition that requires further investigation at a specialised hospital
Product Information. Confidence that lasts
 Confidence that lasts What is Mirena? Inhibition of sperm motility and function inside the uterus and the fallopian tubes, preventing fertilization (Videla-Rivero et al. 1987). Section of system Levonorgestrel
Confidence that lasts What is Mirena? Inhibition of sperm motility and function inside the uterus and the fallopian tubes, preventing fertilization (Videla-Rivero et al. 1987). Section of system Levonorgestrel
Information leaflet on. Laparoscopic Treatment of Endometriosis
 Information leaflet on Laparoscopic Treatment of Endometriosis 1 What is endometriosis? Endometriosis is a condition, which affects many women. It is defined as the presence of endometrial tissue outside
Information leaflet on Laparoscopic Treatment of Endometriosis 1 What is endometriosis? Endometriosis is a condition, which affects many women. It is defined as the presence of endometrial tissue outside
Index. Cambridge University Press Ambulatory Gynaecology: A New Concept in the Treatment of Women Edited by Kevin Jones.
 abnormal uterine bleeding 1, 36 51 accreditation and training 51 epidemiology, guidelines and national targets 36 42 organisation of service 43 primary diagnostic tool 50 accreditation 34, 51 acetic acid
abnormal uterine bleeding 1, 36 51 accreditation and training 51 epidemiology, guidelines and national targets 36 42 organisation of service 43 primary diagnostic tool 50 accreditation 34, 51 acetic acid
Minimal Access Surgery in Gynaecology
 Gynaecology & Fertility Information for GPs August 2014 Minimal Access Surgery in Gynaecology Today, laparoscopy is an alternative technique for carrying out many operations that have traditionally required
Gynaecology & Fertility Information for GPs August 2014 Minimal Access Surgery in Gynaecology Today, laparoscopy is an alternative technique for carrying out many operations that have traditionally required
Abnormal Uterine Bleeding: Evaluation of Premenopausal Women. Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF
 Abnormal Uterine Bleeding: Evaluation of Premenopausal Women Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF Objectives Define normal and abnormal uterine bleeding Review
Abnormal Uterine Bleeding: Evaluation of Premenopausal Women Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF Objectives Define normal and abnormal uterine bleeding Review
GP Guidelines for the Management of Adult Patients with Gynaecological Cancers 2012
 GP Guidelines for the Management of Adult Patients with Gynaecological Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt of a new version. Date
GP Guidelines for the Management of Adult Patients with Gynaecological Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt of a new version. Date
Medical treatment for uterine fibroids
 Medical treatment for uterine fibroids Prof Mary Ann Lumsden Prof of Gynaecology and Medical Education University of Glasgow Senior Vice President RCOG Conflict of Interest Chair, Guideline development
Medical treatment for uterine fibroids Prof Mary Ann Lumsden Prof of Gynaecology and Medical Education University of Glasgow Senior Vice President RCOG Conflict of Interest Chair, Guideline development
Laparoscopy and Hysteroscopy
 AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Laparoscopy and Hysteroscopy A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of
AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Laparoscopy and Hysteroscopy A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of
Health Board/Region: All-Wales
 Peer Review: Cancer Sub-site: Gynaecology Health Board/Region: All-Wales Cycle: Second Date of review: February 2018 This report describes the findings and themes observed by clinical review panels during
Peer Review: Cancer Sub-site: Gynaecology Health Board/Region: All-Wales Cycle: Second Date of review: February 2018 This report describes the findings and themes observed by clinical review panels during
Palm Beach Obstetrics & Gynecology, PA
 Palm Beach Obstetrics & Gynecology, PA 4671 S. Congress Avenue, Lake Worth, FL 33461 561.434.0111 4631 N. Congress Avenue, Suite 102, West Palm Beach, FL 33407 Endometriosis The lining of the uterus is
Palm Beach Obstetrics & Gynecology, PA 4671 S. Congress Avenue, Lake Worth, FL 33461 561.434.0111 4631 N. Congress Avenue, Suite 102, West Palm Beach, FL 33407 Endometriosis The lining of the uterus is