Promoting Functional Independence in the Context of an Acute Illness
|
|
|
- Marybeth Eaton
- 5 years ago
- Views:
Transcription
1 Promoting Functional Independence in the Context of an Acute Illness Cynthia J. Brown, MD, MSPH Associate Professor of Medicine, Director, Geriatric Medicine Section University of Alabama at Birmingham Birmingham/Atlanta VA GRECC
2 Objectives 1. Describe the prevalence of risk factors for functional decline among older persons who become acutely ill. 2. Explain potential barriers to hospital mobility for older adults. 3. Describe interventions to promote mobility among hospitalized elders.
3 Delirium Present on admission in 10-15% of older patients Occurs during admission for additional 10-30% of patients Predictor of prolonged hospital stay Associated with increased rates of hospital death and nursing home placement Demonstrated prevention measure: Avoidance of low mobility (bed rest or bed to chair transfers) Inouye SK, et al. N Engl J Med, 2006
4 Falls Average of falls per1000 bed days After controlling for age, rates vary depending on hospital service Major Risk factor: Muscle weakness/ Deconditioning Schwendimann R, et al. BMC Nursing 2005
5 Pressure Ulcers Annual incidence of hospital-acquired pressure ulcers 2.9 to 29%. ICUs; 33% incidence and 41% prevalence. Older patients admitted for non-elective orthopedic procedures, 66% incidence. Stage III-IV pressure ulcers considered a never event by CMS. Primary risk factor: bed rest/low mobility Salcido R, Popescu A. Pressure Ulcers and Wound Care. 2012
6 Functional Decline Decline in ability to perform one or more basic Activities of Daily Living (ADL). Rates range from 15-35% during hospitalization. Only 10% recover prior to discharge. 15% not at pre-hospital level at 3 months. Major risk factor is bed rest/ low mobility Boyd CM, J Am Geriatr Soc, 2009

7 Brown CJ, Roth DL, Allman RM, Sawyer P, Ritchie CS, Roseman JM. Trajectories of Life-Space Mobility after Hospitalization. Ann Intern Med 150(6): , 2009.
8 Measuring Life-Space Life-Space 0 Bedroom Life-Space 1 Home Life-Space 2 Outside House Unrestricted Restricted Life-Space 3 Neighborhood Life-Space 4 Life-Space 5 Town Unlimited Scores range from with higher scores reflecting greater mobility
9 Escambia Mobile Baldwin ALABAMA Lauderdale Limestone Madison Jackson Colbert Franklin Lawrence Morgan Marshall De Kalb Marion Cullman Cherokee Winston Etowah Blount Walker Lamar Fayette Saint Clair Calhoun Jefferson Cleburne Talladega Tuscaloosa Shelby Clay Pickens Randolph Bibb Greene Chilton Hale Perry Sumter Autauga Coosa Tallapoosa Chambers Elmore Lee Macon Marengo Dallas Montgomery Russell Lowndes Choctaw Bullock Wilcox Clarke Pike Monroe Butler Crenshaw Washington Conecuh Coffee Covington Geneva Barbour Henry Dale Urban Counties Rural Counties Houston UAB Study of Aging Subjects stratified, random sample of Medicare beneficiaries living in 5 counties in central Alabama. Study over-sampled males, African Americans, and rural residents.
10 Methods 211 hospitalizations among 687 participants over 4 years Surgical admissions = 44; Non-surgical admissions = 167 Life-Space Assessment every 6 months Using multilevel change model to determined trajectory of Life-Space before and after hospitalization.
11 Life-Space Trajectories after Hospitalization = Surgical admissions = Non-surgical admissions
12 Key Point Regarding Hospital Hazards Many hospital hazards described share two predisposing factors: Older age Low mobility, defined as being limited to bed or chair
13 Creditor MC Ann Intern Med 1995


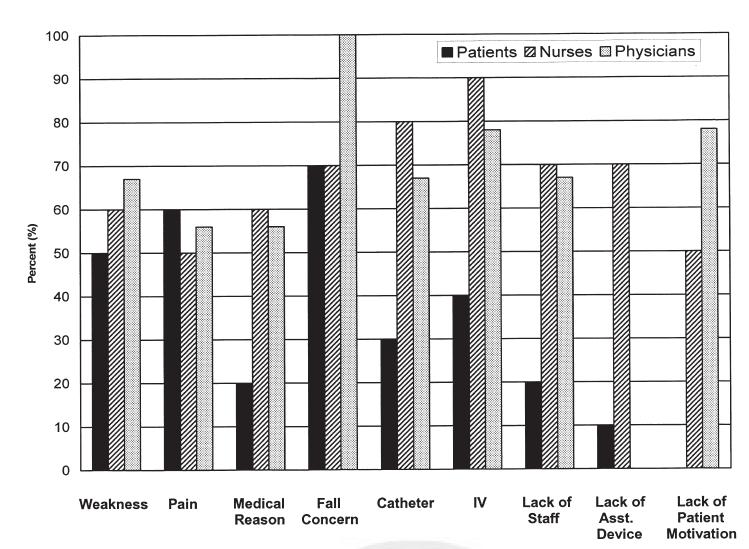
14 Brown CJ, Williams BR, Woodby LL, Davis LL, Allman RM. Barriers to mobility during hospitalization from the perspective of older patients, their nurses and physicians. J Hosp Med 2(5): , 2007.
15 Potential Barriers to Hospital Mobility Patient-related factors Illness severity Comorbid conditions Altered mental status Patients symptoms Treatment-related factors Hospital devices Admitting diagnosis Side effects of medications PATIENT Institution-related factors Staffing patterns Environment encourages bed rest Lack of ambulatory devices Attitudinal factors Attitude toward mobility Expectation of hospital stay Concern about falls
16 Participants: Methods 10 patients, age > 75 years admitted to medical wards at UAB Hospital Patient s nurse & physician also recruited (n=29) Questionnaire Development: Semi-structured interview guide New themes incorporated into interview Interviews audiotaped, transcribed and examined for common themes
17
18 Barrier: Lack of Importance "I think nurses in general would prefer the patient to stay in bed. I believe they perceive it as a risk for falls and a risk for pulling out their IVs or any other medical device and it is probably not viewed as an important factor in someone who is recovering from an illness."
19 Barrier: Environment I think it is just that patients, when they are in the hospital, they feel they are supposed to be in bed. And they are more comfortable there and a lot of times they can see the TV better.
20 Implications Study an important step in development of successful interventions to minimize low mobility. Suggests there are modifiable and non- modifiable reasons for low mobility. Does not address the potential that illness severity and comorbid illness are key reasons for low mobility.

21 Brown CJ, Friedkin RJ, Inouye SK. Prevalence and Outcomes of Low Mobility in Hospitalized Older Patients. J Am Geriatr Soc 52: , 2004.
22 Prevalence and Outcomes of Low Mobility in Hospitalized Older Patients 498 hospitalized medical patients, age 70 years Mobility scale based on nurse report: degree of assistance needed number of times transferred and ambulated Average of all mobility observations for each patient, scores trichotomized. 0-4: low mobility 4.1-8: intermediate mobility : high mobility
23 Prevalence of Low Mobility Bed rest present at some point during hospitalization for 33% of older patients 16% patients experienced low mobility, defined as bed or bed to chair activity, throughout hospitalization
24 Increased Risk of Adverse Outcomes by Mobility Outcomes Low Mobility Intermediate Mobility Any decline in ADLs New Institutionalization at Discharge Death Death or New Institutionalization Adjusted for ADLs, Demographics, APACHE II, Charlson and ICU/CCU stay; Odds Ratio compared to High mobility group (P <.006)
25 Graded Relationship Between Mobility Level and Adverse Outcome % with Outcome Low Intrm High Functional New In-Hospital Death or Decline Institutionalization Death Institutionalization
26 Documented Reasons for Bed Rest in Low Mobility Patients (176 obs in 66 pts) Diagnosis or Procedure N (%) No indication documented 102 (58) Imminently terminal condition 18 (10.2) Rule-out myocardial infarction 17 (9.7) Hypoxemia with exertion 8 (4.5) Acute post-operative period 6 (3.4) Acute deep vein thrombosis 5 (2.8)
27 Conclusions Low mobility was associated with adverse outcomes after controlling for illness severity and comorbidities. Reasons for bed rest were frequently not documented. However, still lack a validated measure of mobility.


28 Brown CJ, Redden DT, Flood KL, Allman RM.The underrecognized epidemic of low mobility during hospitalization of older adults. J Am Geriatr Soc 57(9): , 2009
29 Epidemic of Low Mobility 45 hospitalized VA medical patients age 65 years not delirious or demented able to walk in the 2 weeks prior to admission Mean proportion of time spent lying, sitting, and standing/walking determined for each hour after hospital admission using wireless monitors and previously validated algorithm.


30
31 Results Mean length of stay 5.1 days Generated 2592 one-hour periods of data No patient remained in bed entire measured hospital stay 83% of measured hospital stay spent lying in bed. Time spent standing/walking Ranged from 0.2% to 21% Median time was 3% or 43 minutes/day.
32 100 Lying Sitting Standing/Walking Mean Percent of Time Day 1 Day 2 Day 2 Day 3 Day 3 Day 4 Day 4 12pm 12am 12pm 12am 12pm 12am 12pm Admission Day and Time
33 Conclusions Wireless monitors are a valid method of measuring mobility. Hospital patients are spending at least 80% of their time in bed. On average, less than 5% of time spent standing or walking.
34 Potential Interventions to Improve Mobility During Hospitalization Consult Physical Therapy Hospital Elder Life Program (HELP) Graduated Walking Programs Specially trained transporters Enhanced mobility program
35 Solution: Consult Physical Therapy In one 1000 bed hospital, PT receives new referrals daily Patients seen once a day Average missed visit rate: 22% 8% patients referred day of discharge 10-12% of new PT referrals, no skilled need (i.e. inappropriate referrals)
36 Solution: Hospital Elder Life Program (HELP) Target six risk factors for delirium: Cognitive Impairment Sleep deprivation Visual impairment Hearing Impairment Dehydration Immobility Early mobilization protocol; ambulation or ROM Minimize use of immobilizing equipment
37 Solution: Early Ambulation with Trained Transporters Pilot study in community-based hospital using specially trained transporters to walk ward patients during slow periods. Included nights and week-ends Participants spent 2.4 days in program, with average of 5.6 walks per patient. Program feasible, but too small to demonstrate changes in outcomes. Tucker D, Geriatr Nursing 2004
38 Safety and Efficacy of a Hospital Mobility Program
39 Specific Aim To examine the impact of a hospital mobility program on activities of daily living (ADL) and community mobility as measured by the Life-Space Assessment (LSA) compared to usual care.
40 Methods 100 patients from Birmingham VAMC Not delirious or demented, walking 2 weeks PTA Randomly assigned to Mobility Program (MP) or Usual Care (UC). Daily assessments by blinded assessors. One month telephone follow-up. Physicians blinded to assure no change in usual care (e.g. activity orders, PT consults).
41 Daily motivational interviewing. Provision of folder; document goals, barriers. Methods (cont.) Mobility Program (MP) Usual Care (UC) Twice daily walks with Twice daily friendly assistance. visits. Provision of rolling Provision of folders walker, if safe. with friendly messages.
42 Assessments In-Hospital ADL ability Baseline LSA Depression APACHE II Charlson Comorbidity index Chart review for LOS, PT consults One month follow-up ADL ability Post-hospital LSA
43 Baseline Characteristics (N = 100) Usual Care Walking Program P value Age 73.4 ± ± Gender, male 49 (98%) 48 (96%) 0.56 Race, black 8 (16%) 11 (22%) 0.44 LOS, mean 3.6 ± ± median GDS 5.0 ± ± Charleson Comorbidity 4.1 ± ± APACHE 15.3 ± ± PT Ordered 17 (34%) 24 (48%) 0.15
44 Results In-hospital, 3 falls in 2 patients reported all in UC group 8 participants did not complete study; 2 UC and 6 WP Death (n=3; 2WP, 1UC) Medical complications (n=4, 4WP) Patient refusal (n=1, 1UC) Missing ADL and LSA scores imputed
45 Pre-Post Hospital Function Mobility Usual Care Program P value Baseline ADL 8.8 ± ± Post-Hospital ADL 8.2 ± ± P-values for group differences between pre and post hospital outcomes adjusted for baseline, age, gender, race
46 Pre-Post Life-Space Assessment Mobility Usual Care Program P value Baseline LSA 51.5 (21.1) 53.9 (29.4) 0.4 Post-Hospital LSA 41.6 (21.5) 52.5 (29.0).0096 P-values for group differences between pre and post hospital outcomes adjusted for baseline, age, gender, race
47 Independent Predictors of Post-Hospital LSA Independent predictors of post-hospital LSA using linear regression: Baseline LSA (p<.0001) Length of stay (p=.012) Group assignment; MP or UC (p=.017) Model controlled for: Demographics, Depression, Illness Severity, Comorbidy score, LOS, Group Assignment (WP or UC) and baseline LSA.
48 Conclusions Participants in UC group experienced a mean 10-point decline in LSA scores, while those in MP group experienced a 1-point decline. Among survivors, being assigned to MP group was independently associated with a higher one-month post-hospitalization LSA.
49 Take Home Points Interventions designed to address modifiable barriers and provide a safe environment can increase mobility. Adverse outcomes (i.e. delirium, pressure ulcers, falls, and functional decline) probably can be prevented with increased mobility.

50 Exercising in the Park Beijing, China 2007
RD INSTRUCTION 1980-D, EXHIBIT C PAGE 1 GUARANTEED HOUSING PROGRAM INCOME LIMITS
 RD INSTRUCTION 1980-D, EXHIBIT C PAGE 1 Anniston-Oxford, AL MSA VERY LOW INCOME 18600 21250 23900 26550 28700 30800 32950 35050 LOW INCOME 29750 34000 38250 42500 45900 49300 52700 56100 Auburn-Opelika,
RD INSTRUCTION 1980-D, EXHIBIT C PAGE 1 Anniston-Oxford, AL MSA VERY LOW INCOME 18600 21250 23900 26550 28700 30800 32950 35050 LOW INCOME 29750 34000 38250 42500 45900 49300 52700 56100 Auburn-Opelika,
CEREBROVASCULAR DISEASES (STROKE) MORTALITY
 MORTALITY") Indicators of Health Status in CEREBROVASCULAR DISEASES (STROKE) MORTALITY Jointly produced to assist those seeking to improve health care in rural by The Office of Primary Care and Rural Health, Department
Indicators of Health Status in CEREBROVASCULAR DISEASES (STROKE) MORTALITY Jointly produced to assist those seeking to improve health care in rural by The Office of Primary Care and Rural Health, Department
Indicators of Health Status in Alabama DIABETES MORTALITY. Jointly produced to assist those seeking to improve health care in rural Alabama
 Indicators of Health Status in DIABETES MORTALITY Jointly produced to assist those seeking to improve health care in rural by The Office of Primary Care and Rural Health, Department of Public Health and
Indicators of Health Status in DIABETES MORTALITY Jointly produced to assist those seeking to improve health care in rural by The Office of Primary Care and Rural Health, Department of Public Health and
Indicators of Health Status in Alabama CANCER MORTALITY. Jointly produced to assist those seeking to improve health care in rural Alabama
 Indicators of Health Status in CANCER MORTALITY Jointly produced to assist those seeking to improve health care in rural by The Office of Primary Care and Rural Health, Department of Public Health and
Indicators of Health Status in CANCER MORTALITY Jointly produced to assist those seeking to improve health care in rural by The Office of Primary Care and Rural Health, Department of Public Health and
Directory of Public Transportation in Alabama
 Directory of Public in Alabama 2016 Compiled by the Regional Planning of Greater Birmingham for the Alabama Council on Developmental Disabilities County Service Area Autauga Autauga County Autauga County
Directory of Public in Alabama 2016 Compiled by the Regional Planning of Greater Birmingham for the Alabama Council on Developmental Disabilities County Service Area Autauga Autauga County Autauga County
Table of Contents. 2 P age. Susan G. Komen
 ALABAMA Table of Contents Table of Contents... 2 Introduction... 3 About... 3 Susan G. Komen Affiliate Network... 3 Purpose of the State Community Profile Report... 4 Quantitative Data: Measuring Breast
ALABAMA Table of Contents Table of Contents... 2 Introduction... 3 About... 3 Susan G. Komen Affiliate Network... 3 Purpose of the State Community Profile Report... 4 Quantitative Data: Measuring Breast
ACEA 2013 CONFERENCE REGISTRATION SYSTEM NAME TITLE PHONE # PAID RECEIPT
 Alabama State Dept. Sallye Longshore Federal Programs 334-242-8199 Mark Ward Federal Programs 334-242-8199 ALBERTVILLE CITY ALEXANDER CITY ANDALUSIA CITY ANNISTON CITY ARAB CITY ATHENS CITY ATTALLA CITY
Alabama State Dept. Sallye Longshore Federal Programs 334-242-8199 Mark Ward Federal Programs 334-242-8199 ALBERTVILLE CITY ALEXANDER CITY ANDALUSIA CITY ANNISTON CITY ARAB CITY ATHENS CITY ATTALLA CITY
2017 County Health Rankings. Alabama
 2017 County Health Rankings Alabama INTRODUCTION The County Health Rankings & Roadmaps program brings actionable data and strategies to communities to make it easier for people to be healthy in their homes,
2017 County Health Rankings Alabama INTRODUCTION The County Health Rankings & Roadmaps program brings actionable data and strategies to communities to make it easier for people to be healthy in their homes,
the risk of heart disease and stroke in alabama: burden document
 te risk of eart disease and stroke in alabama: burden document finding te Pat to CardioVasCUlar ealt 21 table of Contents executive Summary... 1 demograpic caracteristics of Alabama... 2 Leading causes
te risk of eart disease and stroke in alabama: burden document finding te Pat to CardioVasCUlar ealt 21 table of Contents executive Summary... 1 demograpic caracteristics of Alabama... 2 Leading causes
EBSCO August 2018 Client Name Sessions Searches Full-Text Requests Abstract Requests ADELIA MCCONNELL RUSSELL LIBRARY AKRON PUBLIC LIBRARY 0
 EBSCO August 2018 Client Name Sessions Searches Full-Text Requests Abstract Requests ADELIA MCCONNELL RUSSELL LIBRARY 3 0 0 0 AKRON PUBLIC LIBRARY 0 0 2 0 ALABAMA AGRICULTURAL & MECHANICAL UNIV 437 1,096
EBSCO August 2018 Client Name Sessions Searches Full-Text Requests Abstract Requests ADELIA MCCONNELL RUSSELL LIBRARY 3 0 0 0 AKRON PUBLIC LIBRARY 0 0 2 0 ALABAMA AGRICULTURAL & MECHANICAL UNIV 437 1,096
Alabama Department of Public Health. Donald E. Williamson, M.D. State Health Officer
 the chronic disease that affects nearly one in ten people A report from the ALABAMA DEPARTMENT OF PUBLIC HEALTH March 2007 Alabama Department of Public Health Donald E. Williamson, M.D. State Health Officer
the chronic disease that affects nearly one in ten people A report from the ALABAMA DEPARTMENT OF PUBLIC HEALTH March 2007 Alabama Department of Public Health Donald E. Williamson, M.D. State Health Officer
ST. VINCENT S BIRMINGHAM BRUNO CANCER CENTER CANCER PROGRAM 2017 ANNUAL REPORT & 2016 STATISTICAL REVIEW
 ST. VINCENT S BIRMINGHAM BRUNO CANCER CENTER CANCER PROGRAM 27 ANNUAL REPORT & 26 STATISTICAL REVIEW 2 CALL TO ACTION CORE VALUES Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No
ST. VINCENT S BIRMINGHAM BRUNO CANCER CENTER CANCER PROGRAM 27 ANNUAL REPORT & 26 STATISTICAL REVIEW 2 CALL TO ACTION CORE VALUES Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No
Every October, Medicare Advantage plans like
 A Newsletter For Members of Vi va Medicare Plus Volume 8 Issue 14 www.vivamedicaremember.com Fall 2009 Changes for the 2010 Plan Year Every October, Medicare Advantage plans like Vi va Medicare Plus announce
A Newsletter For Members of Vi va Medicare Plus Volume 8 Issue 14 www.vivamedicaremember.com Fall 2009 Changes for the 2010 Plan Year Every October, Medicare Advantage plans like Vi va Medicare Plus announce
~ Represents a count of 10 or lower AND its associated percent field * Greater than or equal to 99%
 1 of 11 Alabama State Department of Education Code Name Graduation Rate State of Alabama 0000 State Of Alabama 80% Autauga County 0000 Autauga County 83% Autauga County 0015 Autaugaville 83% Autauga County
1 of 11 Alabama State Department of Education Code Name Graduation Rate State of Alabama 0000 State Of Alabama 80% Autauga County 0000 Autauga County 83% Autauga County 0015 Autaugaville 83% Autauga County
2015 Annual Report and 2014 Statistical Review Inspired by
 05 Annual Report and 0 Statistical Review Inspired by BRUNO CANCER CENTER CANCER PROGRAM Call to Action Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No One Behind For Life Core
05 Annual Report and 0 Statistical Review Inspired by BRUNO CANCER CENTER CANCER PROGRAM Call to Action Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No One Behind For Life Core
ST. VINCENT S BIRMINGHAM BRUNO CANCER CENTER CANCER PROGRAM
 BRUNO CANCER CENTER CANCER PROGRAM 8 ANNUAL REPORT & 7 STATISTICAL REVIEW CALL TO ACTION CORE VALUES Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No One Behind For Life Service
BRUNO CANCER CENTER CANCER PROGRAM 8 ANNUAL REPORT & 7 STATISTICAL REVIEW CALL TO ACTION CORE VALUES Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No One Behind For Life Service
The Oral Health of Alabama s Children,
 Table 1: Demographic characteristics of children surveyed compared to participating schools, schools in the original sample and schools in the sampling frame (based on 2010-2011 enrollment data & children
Table 1: Demographic characteristics of children surveyed compared to participating schools, schools in the original sample and schools in the sampling frame (based on 2010-2011 enrollment data & children
2012 Annual Report & 2011 Statistical Review WHERE HOPE & MEDICINE MEET BRUNO CANCER CENTER CANCER PROGRAM
 0 Annual Report & 0 Statistical Review WHERE HOPE & MEDICINE MEET BRUNO CANCER CENTER CANCER PROGRAM CALL TO ACTION A Healthcare That Works A Healthcare That Is Safe A Healthcare That Leaves No One Behind
0 Annual Report & 0 Statistical Review WHERE HOPE & MEDICINE MEET BRUNO CANCER CENTER CANCER PROGRAM CALL TO ACTION A Healthcare That Works A Healthcare That Is Safe A Healthcare That Leaves No One Behind
Bruno Cancer Center Cancer Program
 Bruno Cancer Center Cancer Program 29 Annual Report & 28 Statistical Review CALL TO ACTION Healthcare That Works Healthcare That is Safe Healthcare That Leaves No One Behind For Life CORE VALUES We are
Bruno Cancer Center Cancer Program 29 Annual Report & 28 Statistical Review CALL TO ACTION Healthcare That Works Healthcare That is Safe Healthcare That Leaves No One Behind For Life CORE VALUES We are
HOSPICES JANUARY 20, 2017
 ABC HOSPICE, INC 266 INDUSTRIAL DRIVE P O BOX 1486 RAINSVILLE AL 35986 (256) 638-3491 DEKALB AFFINITY HOSPICE 216 AQUARIUS DRIVE, STE 309 P O BOX 190125 BIRMINGHAM AL 35209 (205) 949-0400 (205) 949-0405
ABC HOSPICE, INC 266 INDUSTRIAL DRIVE P O BOX 1486 RAINSVILLE AL 35986 (256) 638-3491 DEKALB AFFINITY HOSPICE 216 AQUARIUS DRIVE, STE 309 P O BOX 190125 BIRMINGHAM AL 35209 (205) 949-0400 (205) 949-0405
CANCER ANNUAL REPORT. Baptist Health Cancer Program
 20 16 CANCER ANNUAL REPORT Baptist Health Cancer Program Tiles made by patients and caregivers hang in Montgomery Cancer Center to encourage others on their journey. A BAPTIST HEALTH FACILITY TABLE OF
20 16 CANCER ANNUAL REPORT Baptist Health Cancer Program Tiles made by patients and caregivers hang in Montgomery Cancer Center to encourage others on their journey. A BAPTIST HEALTH FACILITY TABLE OF
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Call to Action. Core Values. Enabling Strengths. Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No One Behind for Life
 Call to Action Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No One Behind for Life Core Values We are called to: Service of the Poor Reverence Integrity Wisdom Creativity Dedication
Call to Action Healthcare That Works Healthcare That Is Safe Healthcare That Leaves No One Behind for Life Core Values We are called to: Service of the Poor Reverence Integrity Wisdom Creativity Dedication
Volunteers Improving Mobility and Ambulation
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Volunteers Improving Mobility and Ambulation Amber Healy BSN, RN Lehigh Valley Health Network Michelle Wolfe BSN, RN Lehigh
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Volunteers Improving Mobility and Ambulation Amber Healy BSN, RN Lehigh Valley Health Network Michelle Wolfe BSN, RN Lehigh
Comprehensive Cancer Control
 Comprehensive Cancer Control 2006-2010 Plan MISSION STATEMENT The mission of the Alabama Comprehensive Cancer Control Coalition (ACCCC) is to develop and sustain an integrated and coordinated approach
Comprehensive Cancer Control 2006-2010 Plan MISSION STATEMENT The mission of the Alabama Comprehensive Cancer Control Coalition (ACCCC) is to develop and sustain an integrated and coordinated approach
Creating a Hospital Nurse-Driven Mobility Program - Why and How Physical Therapist Should Lead the Way
 Creating a Hospital Nurse-Driven Mobility Program - Why and How Physical Therapist Should Lead the Way, GCS University of North Georgia Grady Health System The Problem The Solution The How To F u n c t
Creating a Hospital Nurse-Driven Mobility Program - Why and How Physical Therapist Should Lead the Way, GCS University of North Georgia Grady Health System The Problem The Solution The How To F u n c t
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
State of Alabama HIV Surveillance 2012 Annual Report Finalized
 State of Alabama HIV Surveillance 2012 Annual Report Finalized Prepared by: Division of HIV/AIDS Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
State of Alabama HIV Surveillance 2012 Annual Report Finalized Prepared by: Division of HIV/AIDS Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
State of Alabama HIV Surveillance 2013 Annual Report Finalized
 State of Alabama HIV Surveillance 2013 Annual Report Finalized Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
State of Alabama HIV Surveillance 2013 Annual Report Finalized Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
Alabama. Cancer Facts & Figures 2014
 Alabama Cancer Facts & Figures 2014 Alabama Department of Public Health Letter American Cancer Society Letter Dear Alabamians, I am pleased to present Alabama Cancer Facts & Figures 2014. The American
Alabama Cancer Facts & Figures 2014 Alabama Department of Public Health Letter American Cancer Society Letter Dear Alabamians, I am pleased to present Alabama Cancer Facts & Figures 2014. The American
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Aging Research Day March 8, 2012
 Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
HOW THE POLL WAS CONDUCTED
 HOW THE POLL WAS CONDUCTED This poll was conducted by Mason-Dixon Polling & Research, Inc. of Jacksonville, Florida from April 17 through April 19, 2018. A total of 625 registered Tennessee voters were
HOW THE POLL WAS CONDUCTED This poll was conducted by Mason-Dixon Polling & Research, Inc. of Jacksonville, Florida from April 17 through April 19, 2018. A total of 625 registered Tennessee voters were
Alabama Department of Public Health. Sexually Transmitted Diseases
 Alabama Department of Public Health Sexually Transmitted Diseases Annual Report 29 August 16, 21 Dear Alabama Stakeholder: The Division of Sexually Transmitted Disease Prevention and Control of the Alabama
Alabama Department of Public Health Sexually Transmitted Diseases Annual Report 29 August 16, 21 Dear Alabama Stakeholder: The Division of Sexually Transmitted Disease Prevention and Control of the Alabama
Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University
 Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University Considerations What is the problem? What is the current evidence
Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University Considerations What is the problem? What is the current evidence
Cancer Health Disparities Research Leading to Elimination
 COMPREHENSIVE CANCER CENTER Cancer Health Disparities Research Leading to Elimination Edward E. Partridge, MD, Director Comprehensive Cancer Center Professor of Gynecologic Oncology Evalina B. Spencer
COMPREHENSIVE CANCER CENTER Cancer Health Disparities Research Leading to Elimination Edward E. Partridge, MD, Director Comprehensive Cancer Center Professor of Gynecologic Oncology Evalina B. Spencer
Surgery in Frail Elders. Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011
 Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
This dynamic document will be reviewed and updated on a periodic basis. Each change will be recorded in the Revision History section.
 lll ARKANSAS MEDICARE HbA1c UTILIZATION REPORT November 20, 2015 T. Mac Bird Ph.D., APCD Analytic Lead Kenley Money, APCD Director Version 1.0.2015 ACHI is a nonpartisan, independent, health policy center
lll ARKANSAS MEDICARE HbA1c UTILIZATION REPORT November 20, 2015 T. Mac Bird Ph.D., APCD Analytic Lead Kenley Money, APCD Director Version 1.0.2015 ACHI is a nonpartisan, independent, health policy center
N E W S F O R A L A B A M A N E U T R A L S
 N E W S F O R A L A B A M A N E U T R A L S From the Director Spring 2017 E News A Personal Note From the Director One More Issue! I get to write one more e news before I leave the Center and head out
N E W S F O R A L A B A M A N E U T R A L S From the Director Spring 2017 E News A Personal Note From the Director One More Issue! I get to write one more e news before I leave the Center and head out
HIV Integrated Epidemiological Profile December 2011 State of Alabama
 HIV Integrated Epidemiological Profile December 2011 State of Alabama 12/31/2011 Alabama Department of Public Health Division of HIV/AIDS Prevention and Control TABLE OF CONTENTS List of Figures 3 List
HIV Integrated Epidemiological Profile December 2011 State of Alabama 12/31/2011 Alabama Department of Public Health Division of HIV/AIDS Prevention and Control TABLE OF CONTENTS List of Figures 3 List
State of Alabama HIV Surveillance 2014 Annual Report
 State of Alabama HIV Surveillance 2014 Annual Report Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Richard P. Rogers, MS, MPH richard.rogers@adph.state.al.us
State of Alabama HIV Surveillance 2014 Annual Report Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Richard P. Rogers, MS, MPH richard.rogers@adph.state.al.us
Death by Bedrest: The Perils of The Hospital
 Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Early and Structured Rehabilitation Team Collaboration. David McWilliams Clinical Specialist Physiotherapist - UHB
 Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Monthly Market Data Report
 670 - h t t p : / / www. H i MARKET DATA REPORT Monthly Market Data Report Report Characteristics Report Name: Monthly Market Data Report Report Date Range: 10/2017 10/2018 Filters Used: Location Avg/Med:
670 - h t t p : / / www. H i MARKET DATA REPORT Monthly Market Data Report Report Characteristics Report Name: Monthly Market Data Report Report Date Range: 10/2017 10/2018 Filters Used: Location Avg/Med:
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Monthly Market Data Report
 495 - h t t p : / / www. MARKET DATA REPORT Monthly Market Data Report Report Characteristics Report Name: Monthly Market Data Report Report Date Range: 6/2017 6/2018 Filters Used: Location Avg/Med: Avg
495 - h t t p : / / www. MARKET DATA REPORT Monthly Market Data Report Report Characteristics Report Name: Monthly Market Data Report Report Date Range: 6/2017 6/2018 Filters Used: Location Avg/Med: Avg
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum
 Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Comparison of 3-Year Average and ILI Rates Statewide
 For week 42 (10/18/09-10/24/09), the overall state ILI rate (7.4%) decreased from last week (8.1%), but was still higher than this time last year (6.4%). Statewide ILI Data, Week 42 ending ober 24, 2009
For week 42 (10/18/09-10/24/09), the overall state ILI rate (7.4%) decreased from last week (8.1%), but was still higher than this time last year (6.4%). Statewide ILI Data, Week 42 ending ober 24, 2009
Executive Summary Composite Prevention Profile: Rural, Illinois
 Executive Summary : Rural, Illinois 2008 Adams County Alexander County Brown County Bureau County Carroll County Cass County Christian County Clark County Clay County Coles County Crawford County Cumberland
Executive Summary : Rural, Illinois 2008 Adams County Alexander County Brown County Bureau County Carroll County Cass County Christian County Clark County Clay County Coles County Crawford County Cumberland
Executive Summary Composite Prevention Profile: City of Chicago, Illinois
 Executive Summary :, Illinois 2008 Prepared by Published by the Center for Prevention Research and Development, within the Institute of Government and Public Affairs at the University of Illinois, based
Executive Summary :, Illinois 2008 Prepared by Published by the Center for Prevention Research and Development, within the Institute of Government and Public Affairs at the University of Illinois, based
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Syringe Exchange: Indicators of Need & Success March 2015
 Syringe Exchange: Indicators of Need & Success March 2015 The recent outbreak of HIV in southern Indiana among injection drug users brings attention to the lack of a strong public health system in these
Syringe Exchange: Indicators of Need & Success March 2015 The recent outbreak of HIV in southern Indiana among injection drug users brings attention to the lack of a strong public health system in these
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Addressing Colorectal Cancer Disparities in Arkansas
 Addressing Colorectal Cancer Disparities in Arkansas Collaborating Institutions Winthrop P. Rockefeller Cancer Institute Fay W. Boozman College of Public Health Arkansas Department of Public Health Arkansas
Addressing Colorectal Cancer Disparities in Arkansas Collaborating Institutions Winthrop P. Rockefeller Cancer Institute Fay W. Boozman College of Public Health Arkansas Department of Public Health Arkansas
Executive Summary Composite Prevention Profile: Urban/Suburban, Illinois (excluding Chicago Metro Area)
") Executive Summary Composite Prevention Profile: Urban/Suburban, Illinois (excluding Chicago Metro Area) 2008 Bond County Calhoun County Clinton County Henry County Kankakee County Macoupin County Marshall
Executive Summary Composite Prevention Profile: Urban/Suburban, Illinois (excluding Chicago Metro Area) 2008 Bond County Calhoun County Clinton County Henry County Kankakee County Macoupin County Marshall
Evaluating Functional Status in Hospitalized Geriatric Patients. UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series
 Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Functional Activity and Mobility
 Functional Activity and Mobility Documentation for Hospitalized Adult The Johns Hopkins University and The Johns Hopkins Health System Corporation Goals for Documentation of Activity and Mobility To develop
Functional Activity and Mobility Documentation for Hospitalized Adult The Johns Hopkins University and The Johns Hopkins Health System Corporation Goals for Documentation of Activity and Mobility To develop
UND GERIATRIC MEDICINE FELLOWSHIP CURRICULUM ACUTE CARE
 LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
CHILDHOOD HEALTH. Key findings
 Key findings Prenatal care 85.5 percent of Illinois women received prenatal care in the first trimester in 2004. That s up from 82.4 percent in 2000 but short of the national Healthy People 2010 goal of
Key findings Prenatal care 85.5 percent of Illinois women received prenatal care in the first trimester in 2004. That s up from 82.4 percent in 2000 but short of the national Healthy People 2010 goal of
Jacqueline Trask, PhD, MSW Curriculum Vitae
 Jacqueline Trask, PhD, MSW Curriculum Vitae CONTACT INFORMATION Title: Address: Assistant Professor 700 Pelham Road North 310 Brewer Hall Jacksonville, AL 35265-1602 Office: (256) 782-5621 Fax: (256) 782-5168
Jacqueline Trask, PhD, MSW Curriculum Vitae CONTACT INFORMATION Title: Address: Assistant Professor 700 Pelham Road North 310 Brewer Hall Jacksonville, AL 35265-1602 Office: (256) 782-5621 Fax: (256) 782-5168
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
In each hospital-year, we calculated a 30-day unplanned. readmission rate among patients who survived at least 30 days
 Romley JA, Goldman DP, Sood N. US hospitals experienced substantial productivity growth during 2002 11. Health Aff (Millwood). 2015;34(3). Published online February 11, 2015. Appendix Adjusting hospital
Romley JA, Goldman DP, Sood N. US hospitals experienced substantial productivity growth during 2002 11. Health Aff (Millwood). 2015;34(3). Published online February 11, 2015. Appendix Adjusting hospital
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
UNTHSC TCOM Geriatric Competencies Curriculum Mapping Document
 INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
ARKANSAS DEPARTMENT OF HEALTH
 Thank you for taking an interest in the Arkansas Prescription Monitoring Program (PMP). The goal of the PMP is to enhance patient care by ensuring the legitimate use of controlled substances. The following
Thank you for taking an interest in the Arkansas Prescription Monitoring Program (PMP). The goal of the PMP is to enhance patient care by ensuring the legitimate use of controlled substances. The following
H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline
 H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline Montreal ITC 2014 Sept. 26 Joann Creager, CNS Geriatrics, Manager, MUHC Elder Friendly Hospital Presentation Overview 1. Elder patient
H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline Montreal ITC 2014 Sept. 26 Joann Creager, CNS Geriatrics, Manager, MUHC Elder Friendly Hospital Presentation Overview 1. Elder patient
Mississippi Newborn Screening Report
 Mississippi Newborn Screening Report 2011-2016 Introduction The primary goal of the Newborn Screening Program is to screen every infant born in the state and refer infants with abnormal results to appropriate
Mississippi Newborn Screening Report 2011-2016 Introduction The primary goal of the Newborn Screening Program is to screen every infant born in the state and refer infants with abnormal results to appropriate
Governor s Commission for a Drug-Free Indiana. Commission s Purpose. Local Coordinating Councils 10/18/2013
 Governor s Commission for a Drug-Free Indiana Presented By: Indiana Criminal Justice Institute Substance Abuse Services Division Commission s Purpose Strengthen Local Coordinating Councils (LCCs) and assist
Governor s Commission for a Drug-Free Indiana Presented By: Indiana Criminal Justice Institute Substance Abuse Services Division Commission s Purpose Strengthen Local Coordinating Councils (LCCs) and assist
A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come
: What we know, what we think and what s to come") A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come The AVERT Trial Collaboration group Joshua Kwant, Blinded Assessor 17 th May 2016 NIMAST Nothing to disclose Disclosure
A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come The AVERT Trial Collaboration group Joshua Kwant, Blinded Assessor 17 th May 2016 NIMAST Nothing to disclose Disclosure
How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit
 model of care beyond one unit") How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit Roger Wong, BMSc, MD, FRCPC, FACP Clinical Professor, Division of Geriatric Medicine Associate Dean, Postgraduate Medical
How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit Roger Wong, BMSc, MD, FRCPC, FACP Clinical Professor, Division of Geriatric Medicine Associate Dean, Postgraduate Medical
THE relationship between body mass index (BMI),
,") Journal of Gerontology: MEDICAL SCIENCES 2008, Vol. 63A, No. 1, 67 75 Copyright 2008 by The Gerontological Society of America Unintentional Weight Loss Predicts Decline in Activities of Daily Living Function
Journal of Gerontology: MEDICAL SCIENCES 2008, Vol. 63A, No. 1, 67 75 Copyright 2008 by The Gerontological Society of America Unintentional Weight Loss Predicts Decline in Activities of Daily Living Function
Executive Summary Composite Prevention Profile: Suburban Chicago Metro Area, Illinois
 Executive Summary : Suburban Chicago Metro Area, Illinois 2008 Cook County (excluding the city of Chicago) DeKalb County DuPage County Grundy County Kane County Kendall County Lake County McHenry County
Executive Summary : Suburban Chicago Metro Area, Illinois 2008 Cook County (excluding the city of Chicago) DeKalb County DuPage County Grundy County Kane County Kendall County Lake County McHenry County
How to prevent early & unplanned hospital readmission?
 How to prevent early & unplanned hospital readmission? - after subacute care K. Singler 21th September 2017 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report. K. Singler
How to prevent early & unplanned hospital readmission? - after subacute care K. Singler 21th September 2017 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report. K. Singler
The Gift of Growing Up
 The Gift of Growing Up Thank you all for supporting Children s of Alabama through your Children s Miracle Network Hospitals campaign, event or signature day! We are so grateful for you! In 2017, more than
The Gift of Growing Up Thank you all for supporting Children s of Alabama through your Children s Miracle Network Hospitals campaign, event or signature day! We are so grateful for you! In 2017, more than
Illinois Stroke Data Report
 Illinois Stroke Data Report Robynn Cheng Leidig, MPH CDC Public Health Prevention Service Fellow Division of Patient Safety and Quality Illinois Department of Public Health September 2015 Illinois Stroke
Illinois Stroke Data Report Robynn Cheng Leidig, MPH CDC Public Health Prevention Service Fellow Division of Patient Safety and Quality Illinois Department of Public Health September 2015 Illinois Stroke
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
CHAPTER 2: HEALTH CARE ACCESS
 CHAPTER 2: HEALTH CARE ACCESS No Health Care Coverage (among Adults 18 to 64) in 2006 Definition Responding No to the following question: Do you have any kind of health care coverage, including health
CHAPTER 2: HEALTH CARE ACCESS No Health Care Coverage (among Adults 18 to 64) in 2006 Definition Responding No to the following question: Do you have any kind of health care coverage, including health
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Geriatric Hip Fracture Co-Management. Pannida Wattanapanom, M.D., FACP.
 Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Bartow county georgia school calendar
 Bartow county georgia 2017-2018 school calendar 09/26/2018 Cdg games sonic 09/27/2018 More than just a movie night mobius unleashed 09/28/2018 -PARA QUE SIRVE LAS PASTILLAS GRAMAXIN -Mami ko mene bhut
Bartow county georgia 2017-2018 school calendar 09/26/2018 Cdg games sonic 09/27/2018 More than just a movie night mobius unleashed 09/28/2018 -PARA QUE SIRVE LAS PASTILLAS GRAMAXIN -Mami ko mene bhut
Improving Ohio s Health: Controlling Diabetes and Hypertension
 Improving Ohio s Health: Controlling Diabetes and Ohio Hospital for Diabetes and 1 By Cathy Costello, JD, Director of CliniSyncPLUS Services This article is the first in a series devoted to diabetes and
Improving Ohio s Health: Controlling Diabetes and Ohio Hospital for Diabetes and 1 By Cathy Costello, JD, Director of CliniSyncPLUS Services This article is the first in a series devoted to diabetes and
KASPER QUARTERLY THRESHOLD ANALYSIS REPORT THIRD QUARTER 2017
 DECEMBER 1, KASPER QUARTERLY THRESHOLD ANALYSIS REPORT THIRD QUARTER Prepared by Dana Quesinberry, JD KASPER Quarterly Threshold Analysis Report, Third Quarter The Kentucky Injury Prevention and Research
DECEMBER 1, KASPER QUARTERLY THRESHOLD ANALYSIS REPORT THIRD QUARTER Prepared by Dana Quesinberry, JD KASPER Quarterly Threshold Analysis Report, Third Quarter The Kentucky Injury Prevention and Research
ACEing Age Old Issues in the Care of Older Canadians
 ACEing Age Old Issues in the Care of Older Canadians Dr. Samir K. Sinha MD, DPhil, FRCPC Peter and Shelagh Godsoe Chair in Geriatrics and Director of Geriatrics Sinai Health System and the University Health
ACEing Age Old Issues in the Care of Older Canadians Dr. Samir K. Sinha MD, DPhil, FRCPC Peter and Shelagh Godsoe Chair in Geriatrics and Director of Geriatrics Sinai Health System and the University Health
ORIGINAL INVESTIGATION. Effects of an Acute Care for Elders Unit on Costs and 30-Day Readmissions
 ORIGINAL INVESTIGATION Effects of an Acute Care for Elders Unit on Costs and 30-Day Readmissions Kellie L. Flood, MD; Paul A. MacLennan, PhD; Deborah McGrew, MHA; Darlene Green, DSN; Cindy Dodd, BSN; Cynthia
ORIGINAL INVESTIGATION Effects of an Acute Care for Elders Unit on Costs and 30-Day Readmissions Kellie L. Flood, MD; Paul A. MacLennan, PhD; Deborah McGrew, MHA; Darlene Green, DSN; Cindy Dodd, BSN; Cynthia
Preventing Hospital Acquired Debility
 Preventing Hospital Acquired Debility IATROGENIC DISABILITY PARTIALLY AVOIDABLE PHYSICAL DEPENDENCE MEDICAL DECONDITIONING HOSPITAL ACQUIRED DECONDITIONING POST HOSPITAL SYNDROME Objectives 1. Identify
Preventing Hospital Acquired Debility IATROGENIC DISABILITY PARTIALLY AVOIDABLE PHYSICAL DEPENDENCE MEDICAL DECONDITIONING HOSPITAL ACQUIRED DECONDITIONING POST HOSPITAL SYNDROME Objectives 1. Identify
PROVIDING BETTER CARE FOR OLDER CANADIANS OBJECTIVES
 PROVIDING BETTER CARE FOR OLDER CANADIANS CGS/ SQG SYMPOSIUM MARIE-JEANNE KERGOAT MD, FRCPC,TORONTO, APRIL 19TH 2013 OBJECTIVES Debate with other clinicians responsible for delivering care to vulnerable
PROVIDING BETTER CARE FOR OLDER CANADIANS CGS/ SQG SYMPOSIUM MARIE-JEANNE KERGOAT MD, FRCPC,TORONTO, APRIL 19TH 2013 OBJECTIVES Debate with other clinicians responsible for delivering care to vulnerable
Delirium and Falls. Julia Poole CNC Aged Care RNSH
 Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
New York City Development of the Geriatric Collaborative
 New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
The Burden of Cardiovascular Disease in Illinois. Mortality, Morbidity and Risk Factors 2013
 The Burden of Cardiovascular Disease in Illinois Mortality, Morbidity and Risk Factors 2013 Table of Contents Executive Summary... iii Introduction... 1 Cardiovascular Disease Mortality... 2 Heart Disease
The Burden of Cardiovascular Disease in Illinois Mortality, Morbidity and Risk Factors 2013 Table of Contents Executive Summary... iii Introduction... 1 Cardiovascular Disease Mortality... 2 Heart Disease
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Flu season is quickly approaching and your friends
 A Newsletter For Members of Vi va Medicare Plus www.vivamedicaremember.com Fall 2010 Make Plans to get a Flu Shot this Year! Flu season is quickly approaching and your friends at Vi va Medicare Plus want
A Newsletter For Members of Vi va Medicare Plus www.vivamedicaremember.com Fall 2010 Make Plans to get a Flu Shot this Year! Flu season is quickly approaching and your friends at Vi va Medicare Plus want
Quality Care for the Hospitalized Older Adult
 Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
President s Challenge Karen Bixler
 ESPA 2018 Summer Newsletter 2018-2019 President s Challenge Karen Bixler Thanks so much for entrusting me as your incoming President for the 2018-2019 year. I m super excited to be hosting the upcoming
ESPA 2018 Summer Newsletter 2018-2019 President s Challenge Karen Bixler Thanks so much for entrusting me as your incoming President for the 2018-2019 year. I m super excited to be hosting the upcoming
Hospitalization- Associated Disability
 Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
2007 Open Heart Surgery Survey
 Part A : General Information 2007 Open Heart Surgery Survey 1. Identification UID: Facility Name: County: Street Address: City: Zip: Mailing Address: Mailing City: Mailing Zip: Medicare Provider Number:
Part A : General Information 2007 Open Heart Surgery Survey 1. Identification UID: Facility Name: County: Street Address: City: Zip: Mailing Address: Mailing City: Mailing Zip: Medicare Provider Number: