Palliative care in long-term conditions Scottish Palliative Care Pharmacists Association
|
|
|
- Nancy Hall
- 5 years ago
- Views:
Transcription
1 Palliative care in long-term conditions Scottish Palliative Care Pharmacists Association
2 Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment of conditions at the end of life and related problems which are commonly presented in a community pharmacy or hospital in-patient setting. Learning Outcomes Be aware of prognostic factors associated with conditions receiving palliative care Develop a knowledge of the typical physical symptoms associated with conditions requiring pall care management Describe the main pharmacological and nonpharmacological treatments for symptom management of the condition Increase staff awareness and sensitivity to potential social/psychological/spiritual support needs of patients or their carers and to know where to direct them for support Describe ways in which the clinical pharmacist (community or hospital) can impact on conditions including anticipatory prescribing and stopping medicines towards the end of life
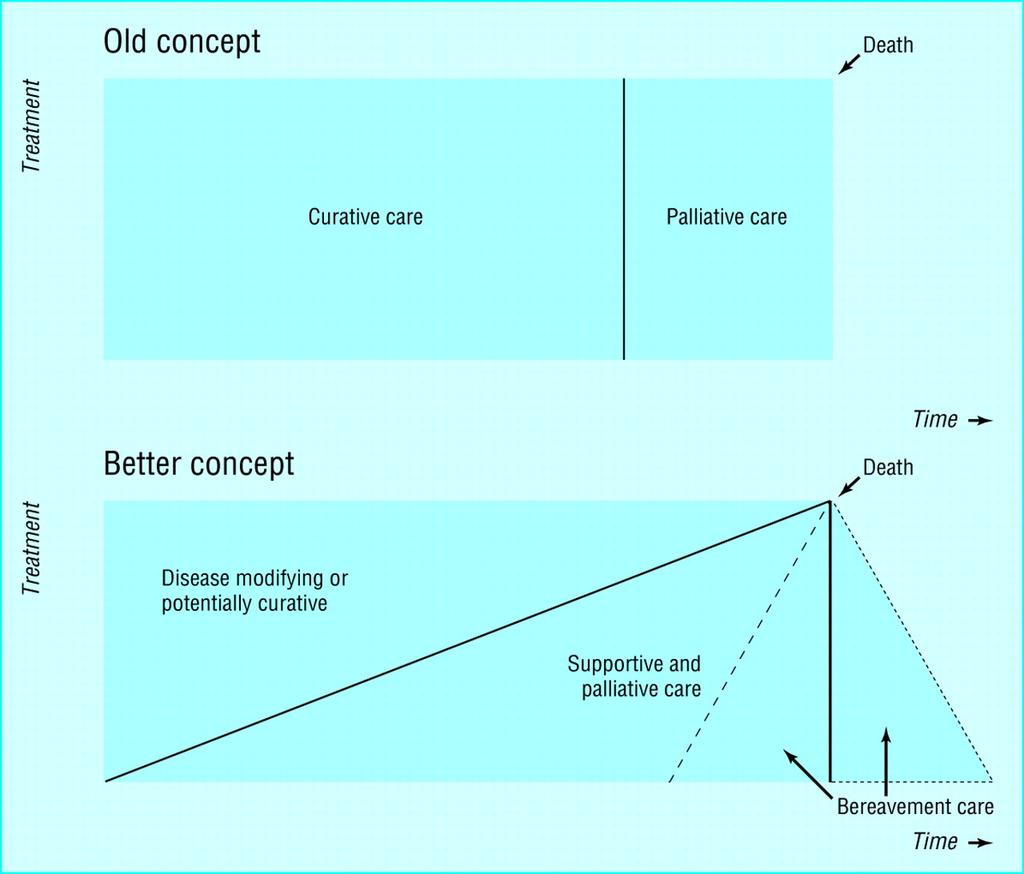
3 What is Palliative Care? Improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems physical, psychosocial and spiritual. WHO, 2004

4 LIVING and DYING WELL
5 Raising Awareness 1% population die each year 55,000 deaths in Scotland Ageing population Increasing technologies Greater expectations Reducing resources Societal changes



6 Policy and Strategies etc- Palliative Care in Scotland
7 Community pharmacy statistics Prescriptions dispensed No. of prescription items No. of instalment fees Minor ailments service No. of items dispensed Patients registered Most prescribed item: paracetamol Chronic medication service Patient registration epharmaceutical Care Risk Assessments Public health service Smoking cessation 63% of primary care quit attempts Supply of Levonelle via CPUS Rx Scotland 87.6m 22.1m 1.7m 790,509 75,000 30,000 50,194 82,000 Average per pharmacy 71,046 17, People with palliative care needs (estimate from Audit Scotland report) 41,670 34
8 Hospital Statistics Acute sector output of Living & Dying Well Short Life Working Group 5 An Evolving Process: Snapshots of palliative and end of life care in acute care settings in hospitals is now available on NES website 58% of people die in hospital 30% of all acute bed days are used by patients in their last year of life 75% of people are admitted to hospital during their last year of life
9 Prognostication Tools Prognostication Indicator Guidance PIG Supportive and Palliative Care Indicators Tool SPICT Scott Murray (Lothian)
10 What conditions are we talking about? 1. The surprise question Would you be surprised if this patient were to die in the next 6-12months 2. Choice/ Need - The patient with advanced disease makes a choice for comfort care only, not curative treatment, or is in special need of supportive / palliative care eg refusing renal transplant 3. Clinical indicators - Specific indicators of advanced disease for three main end of life patient groups - cancer, organ failure, elderly frail/ dementia

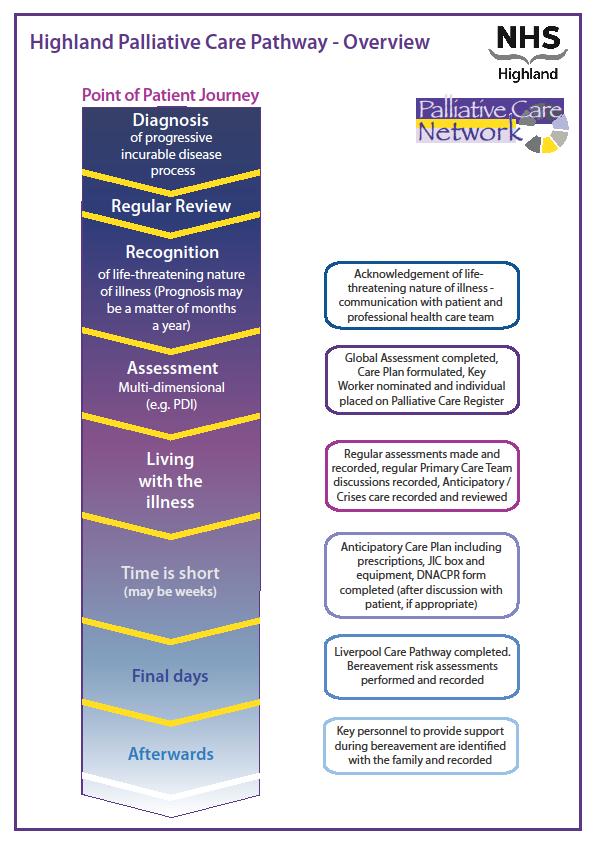
11 Trajectories diagnosis of a progressive or life-limiting illness the surprise question (clinicians would not be surprised if the patient were to die within the next 6-12 months) critical events or significant deterioration during the disease trajectory indicating the need for a change in care and management significant changes in patient or carer ability to cope indicating the need for additional support onset of the end of life phase diagnosing dying

12 Functional Status v Age
13 Symptom prevalence at end of life Cancer HF RF COPD Pain 75% 68% 49% 68% Anorexia 75% 43% 48% 64% Fatigue % 70% 80% 68% Dyspnoea 40% 61% 52% 94% N & V 45% 32% 39% 4% CNS 45% 59% 26% 22% Anxiety % 30% 27% 53% Constipation 80% 37% 28% 36%
14 Poorly relieved suffering even in the final week of life Aesthenia and weakness... 85% Pain 75 % Constipation..75 % Anorexia.. 75 % Dyspnoea % Nausea and / or vomiting.. 40% Confusion.40 % Convulsions.10% ack. D. Doyle
15 Symptom Management Local guidelines National guidelines
16 Aesthenia, fatigue & anorexia (anorexia-cachexia syndrome) Prevalence: COPD>HF>cancer> RF> CF, RA, Alzheimers, HIV/AIDs NOT reversible with nutrition Inflammatory cells produce cytokines -> increase metabolic rate and muscle and fat breakdown Energy conservation techniques keep energy for what is important to the patient, adds value and meaning Signpost to resources for assistance Pressure relieving techniques Increased concentration for unfinished business such as wills may see methylphenidate prescribed
17 Pain Pain assessment tools WHO analgesic ladder Opioids Scottish Patient Safety Programme and National Patient Safety Agency target strong opioids Titration: increments of 30 to 50% Breakthrough doses: 1/10 th to 1/6 th, may require titration Incident pain End of dose effects Toxicity Unrecognised pain in dementia
18 Constipation Causes drugs (opioids, anticholinergics) lack of mobility lack of fluid intake lack of food intake disease Prevention better than cure Stimulant /softener combination Place of methylnaltrexone?
19 Dyspnoea(breathlessness) Assessment Non-drug measures air flow, space, open window Reversible Irreversible Anxiety distraction, relaxation, benzodiazepine Role of oxygen unproven, psychological dependence, barrier between patient and family, burden of supplies and equipment, isolating Diuretics (furosemide) in heart failure to relieve fluid overload Opioids
20 Nausea and Vomiting Symptom assessment - triggers Receptor activation CTZ (drugs, toxins, biochemistry), vomiting centre (vestibular stimulus, central stimulus), mechano and chemoreceptors in gut Appropriate route of administration Avoid cyclizine in heart failure? Avoid anti-dopaminergics in Parkinson s disease Non-drug CBT, acupressure/acupuncture
21 Anxiety/ agitation & Delirium Assessment check hydration, drugs (steroids, opioid toxicity), pain, urine retention (anticholinergics), unresolved issues Anxiety non-drug measures relaxation & CBT, benzodiazepines Delirium hypo and hyperactive Remember environment to orientate and avoid excess stimulus; relaxation; antipsychotics
22
23 Anticipatory care planning GP Palliative Care registers epcs DNA CPR Living Wills & Advance directives Powers of attorney financial and welfare Capacity
24 Anticipatory Care Planning - Pharmacy issues What is likely pattern of the disease/ complications/ issues for e.g. MND, HF, dementia, Parkinson s? and therefore: What do you need to think about in terms of prescribing/ medicines? concordance... changing routes drug formulations equivalences where do you get information? off label prescribing specials accessibility/continuity of supply stopping medicines... place of care supply issues/communications across care settings
25 Concordance Choice Tablet or medicines burden Knowing what the drug is for and how to use e.g. short/ long acting opioids Appropriate route as symptoms change e.g. can no longer swallow Continuity of supplies community network Aids medication charts, non-click lok tops etc
26 Stopping medicines 1. Does the drug have a valid and current Formulary indication. Take particular regard of drugs that are tolerated poorly in frail patients 2. Is the drug expected to give day to day symptomatic benefit? Or is important in preventing rapid symptomatic deterioration 3. Is the drug replacing a vital hormone? 4. Is the drug in a form the patient can take, supplied in the most appropriate way and the least burdensome dosing strategy 5. Is the drug contraindicated or one of the High Risk Drugs Group? 6. For secondary prevention is life expectancy long enough to benefit?
27 Anticipatory prescribing ( Just in case ) Opioid pain, breathlessness Levomepromazine nausea, vomiting, delirium Midazolam anxiety & agitation, anticonvulsant Lorazepam (for sublingual use) Hyoscine butylbromide (Buscopan ) colic, secretions Diluent
28 Information sources and resources Pathway-Final.aspx
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital
 - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital") Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Palliative Emergencies. Ken Stakiw
 Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
 The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
End Stage Liver Disease Regional Audit Casenote Survey
 1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Implementing the recommendation on medication management and symptom control
 Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Palliative Care. Anticipatory Prescribing Guidelines & June Gippsland Region Palliative Care Consortium Clinical Practice Group
 Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Definitions in Palliative Care
 Definitions in Palliative Care Palliative care is specialist care provided for all people living with, and dying from a terminal condition and for whom the primary goal is quality of life. Palliative Care
Definitions in Palliative Care Palliative care is specialist care provided for all people living with, and dying from a terminal condition and for whom the primary goal is quality of life. Palliative Care
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
Dementia & Palliative Care
 Dementia & Palliative Care Aspiration, Myth or Reality? A Clinicians Perspective... Lesley Jones Advanced Practitioner Dementia Care Dementia Dementia is a chronic progressive mental disorder that adversely
Dementia & Palliative Care Aspiration, Myth or Reality? A Clinicians Perspective... Lesley Jones Advanced Practitioner Dementia Care Dementia Dementia is a chronic progressive mental disorder that adversely
Three triggers that suggest that patients could benefit from a hospice palliative care approach
 Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
SYMPTOM CONTROL IN THE LAST DAYS OF LIFE. Bradford, Airedale, Wharfedale & Craven
 Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC
 CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
Symptom Control in the Community Setting. Dr Andrew Tysoe-Calnon
 Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Approach to symptom control near the end-of-life
 Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Palliative Care Research: leading internationally and making a difference in Scotland
 Palliative Care Research: leading internationally and making a difference in Scotland Scottish Cross Party Group, June, 2011 Scott A Murray St Columba s Hospice Chair of Primary Palliative Care Primary
Palliative Care Research: leading internationally and making a difference in Scotland Scottish Cross Party Group, June, 2011 Scott A Murray St Columba s Hospice Chair of Primary Palliative Care Primary
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Palliative Care Out-of-hours. A resource pack for West Dorset. Contents:
 Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
MND Just in Case kit Information for GPs
 MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
PALLIATIVE CARE. A Brief Intervention. Euan Paterson Macmillan GP Facilitator (Glasgow)
") PALLIATIVE CARE A Brief Intervention Euan Paterson Macmillan GP Facilitator (Glasgow) euan.paterson@ntlworld.com 07792120108 1 or How to deal with ACP, epcs and the Palliative Care DES http://www.palliativecareggc.org.uk/
PALLIATIVE CARE A Brief Intervention Euan Paterson Macmillan GP Facilitator (Glasgow) euan.paterson@ntlworld.com 07792120108 1 or How to deal with ACP, epcs and the Palliative Care DES http://www.palliativecareggc.org.uk/
BREATHLESSNESS MANAGEMENT
 Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Palliative Care Management Diploma
 Palliative Care Management Diploma Introduction Palliative care (WHO, 2002) is an approach that improves the quality of life of patients and their families facing the problems associated with lifethreatening
Palliative Care Management Diploma Introduction Palliative care (WHO, 2002) is an approach that improves the quality of life of patients and their families facing the problems associated with lifethreatening
Diamorphine 4 hour. alfentanil (500microgram/mL) Calculated by dividing 24 hour oral morphine dose by 30
 Calculated by dividing 24 hour oral morphine dose by 30") If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
What is Palliative Care? DEFINITIONS PALLIATIVE CARE. Palliative & End of Life Care Services N E Lincs 28/09/2017 1
 What is Palliative Care? 1 DEFINITIONS Palliative Care: is the active holistic care of patients with advanced progressive illness. The goal of palliative care is achievement of the best quality of life
What is Palliative Care? 1 DEFINITIONS Palliative Care: is the active holistic care of patients with advanced progressive illness. The goal of palliative care is achievement of the best quality of life
NHS Grampian. Care Plan Palliative & Supportive. Acute Care Settings
 NHS Grampian Palliative & Supportive Care Plan 2013 Acute Care Settings Contents Page 1. Introduction 2. Standards 3. The identification of the palliative patient 4. Assessment of the palliative patient
NHS Grampian Palliative & Supportive Care Plan 2013 Acute Care Settings Contents Page 1. Introduction 2. Standards 3. The identification of the palliative patient 4. Assessment of the palliative patient
Palliative Medicine Overview. Francine Arneson, MD Palliative Medicine
 Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
Palliative Medicine in Critical Care Not Just Hospice. Robin. Truth or Myth 6/11/2015. Francine Arneson, MD Palliative Medicine
 Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
PALLIATIVE CARE. A Brief Intervention. Euan Paterson Macmillan GP Facilitator (Glasgow)
") PALLIATIVE CARE A Brief Intervention Euan Paterson Macmillan GP Facilitator (Glasgow) euan.paterson@ntlworld.com 07792120108 or How to deal with ACP, epcs and the Palliative Care DES http://www.palliativecareggc.org.uk/
PALLIATIVE CARE A Brief Intervention Euan Paterson Macmillan GP Facilitator (Glasgow) euan.paterson@ntlworld.com 07792120108 or How to deal with ACP, epcs and the Palliative Care DES http://www.palliativecareggc.org.uk/
Ventilation/End of Life Neuromuscular Disorders. Dr Emma Husbands Consultant Palliative Medicine
 Ventilation/End of Life Neuromuscular Disorders Dr Emma Husbands Consultant Palliative Medicine Emma.Husbands@glos.nhs.uk Contents Cases NIV and palliation and ethical bits APM guidelines Important bits
Ventilation/End of Life Neuromuscular Disorders Dr Emma Husbands Consultant Palliative Medicine Emma.Husbands@glos.nhs.uk Contents Cases NIV and palliation and ethical bits APM guidelines Important bits
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
Heart Failure (HF) - Primary Care Flow Charts. Pre diagnosis Symptoms or signs suggestive of HF
 - Primary Care Flow Charts. Pre diagnosis Symptoms or signs suggestive of HF") Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts. Symptoms or signs suggestive of HF. Pre diagnosis. Refer to the Heart Failure Clinic at VHK for
 - Primary Care Flow Charts. Symptoms or signs suggestive of HF. Pre diagnosis. Refer to the Heart Failure Clinic at VHK for") Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
This survey aims to look at individual practice and can be completed by any healthcare professional.
 This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
End of Life Care. Dr Anne Garry Consultant in Palliative Medicine
 End of Life Care Dr Anne Garry Consultant in Palliative Medicine Concerns voiced both by public and professionals.. Implementation and on-going training highly variable across country Decisions made by
End of Life Care Dr Anne Garry Consultant in Palliative Medicine Concerns voiced both by public and professionals.. Implementation and on-going training highly variable across country Decisions made by
PALLIATIVE CARE. A Brief Intervention. Euan Paterson Macmillan GP Facilitator (Glasgow)
") PALLIATIVE CARE A Brief Intervention Euan Paterson Macmillan GP Facilitator (Glasgow) euan.paterson@ntlworld.com 07792120108 1 or How to deal with ACP, epcs and the Palliative Care DES http://www.palliativecareggc.org.uk/
PALLIATIVE CARE A Brief Intervention Euan Paterson Macmillan GP Facilitator (Glasgow) euan.paterson@ntlworld.com 07792120108 1 or How to deal with ACP, epcs and the Palliative Care DES http://www.palliativecareggc.org.uk/
Training in palliative and end-of-life care: Guidance for trainees (and their trainers) in non-palliative medicine training posts
 in non-palliative medicine training posts") Training in palliative and end-of-life care: Guidance for trainees (and their trainers) in non-palliative medicine training posts August 204 Produced by Dr Fiona Hicks onsultant in Palliative Medicine
Training in palliative and end-of-life care: Guidance for trainees (and their trainers) in non-palliative medicine training posts August 204 Produced by Dr Fiona Hicks onsultant in Palliative Medicine
Anticipatory Medications for End of Life Patients. Doses must be proportional to the current analgesic medication YES NO YES NO
 Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Target audience: The target audience for this guidance are: GPs Care home managers and nurses, District nurses, and Specialist Palliative Care teams.
 Anticipatory medication guidance for the last days of life for frail older people being care for in care homes who do not have Specialist Palliative Care needs Purpose of guidance: The purpose of this
Anticipatory medication guidance for the last days of life for frail older people being care for in care homes who do not have Specialist Palliative Care needs Purpose of guidance: The purpose of this
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital.
 Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol
 Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol") 483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
TRAJECTORY OF ILLNESS IN END OF LIFE CARE
 TRAJECTORY OF ILLNESS IN END OF LIFE CARE By Dr Helen Fryer OBJECTIVES To be aware of the three commonest trajectories of decline in the UK To understand the challenges faced in delivering effective Palliative
TRAJECTORY OF ILLNESS IN END OF LIFE CARE By Dr Helen Fryer OBJECTIVES To be aware of the three commonest trajectories of decline in the UK To understand the challenges faced in delivering effective Palliative
Heart Failure Vital steps for palliative care. Dr Karen J Hogg Glasgow Royal Infirmary
 Heart Failure Vital steps for palliative care Dr Karen J Hogg Glasgow Royal Infirmary Overview Why is heart failure a problem? Why do we need integrated cardiology and palliative care services? Cardiology
Heart Failure Vital steps for palliative care Dr Karen J Hogg Glasgow Royal Infirmary Overview Why is heart failure a problem? Why do we need integrated cardiology and palliative care services? Cardiology
Palliative care competencies: is it for all? Khon Kaen International Conference in Palliative Care 2018
 Palliative care competencies: is it for all? Khon Kaen International Conference in Palliative Care 2018 Definition Competence The ability to do something successfully or efficiently For us it means reaching
Palliative care competencies: is it for all? Khon Kaen International Conference in Palliative Care 2018 Definition Competence The ability to do something successfully or efficiently For us it means reaching
Palliative Care and the Critical Role of the Pharmacist. Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre
 Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
Symptom Control in Heart Failure. Dr Claire L Hookey
 Symptom Control in Heart Failure Dr Claire L Hookey Heart Failure symptoms Class III/IV CHF, mean 67.1 years, mean EF 22.3% Most prevalent symptoms:- lack of energy (66%) dry mouth (62%) shortness of breath
Symptom Control in Heart Failure Dr Claire L Hookey Heart Failure symptoms Class III/IV CHF, mean 67.1 years, mean EF 22.3% Most prevalent symptoms:- lack of energy (66%) dry mouth (62%) shortness of breath
To Cover or Not To Cover? A Review of Medication Coverage Guidelines. Dr. Sherita D. Castille, Pharm D Clinical Pharmacist. Agenda.
 To Cover or t To Cover? A Review of Medication Coverage Guidelines Dr. Sherita D. Castille, Pharm D Clinical Pharmacist Agenda 2 Overview Define key Medicare terms Determine relatedness to terminal prognosis
To Cover or t To Cover? A Review of Medication Coverage Guidelines Dr. Sherita D. Castille, Pharm D Clinical Pharmacist Agenda 2 Overview Define key Medicare terms Determine relatedness to terminal prognosis
Care of dying adults in the last days of life. Improving care at the very end of life.
 Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Annette Edwards Consultant in Palliative Medicine
 Annette Edwards Consultant in Palliative Medicine Learning about core palliative care principles from the experience of managing patients with Motor Neurone Disease Dr Annette Edwards Consultant in Palliative
Annette Edwards Consultant in Palliative Medicine Learning about core palliative care principles from the experience of managing patients with Motor Neurone Disease Dr Annette Edwards Consultant in Palliative
Managing Symptoms in End of Life Care
 Unit Code: PT2/3/EA/004 This unit has 4 learning outcomes. LEARNING OUTCOMES The learner will: 1. Understand the effects of symptoms in relation to end of life care 2. Be able to manage symptoms of end
Unit Code: PT2/3/EA/004 This unit has 4 learning outcomes. LEARNING OUTCOMES The learner will: 1. Understand the effects of symptoms in relation to end of life care 2. Be able to manage symptoms of end
abcdefghijklmnopqrstu
 NHS Circular: PCA(M)(2012) 6 Health and Social Care Integration Directorate Primary Care Division abcdefghijklmnopqrstu Dear Colleague THE PRIMARY MEDICAL SERVICES DIRECTED ENHANCED SERVICES (SCOTLAND)
NHS Circular: PCA(M)(2012) 6 Health and Social Care Integration Directorate Primary Care Division abcdefghijklmnopqrstu Dear Colleague THE PRIMARY MEDICAL SERVICES DIRECTED ENHANCED SERVICES (SCOTLAND)
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Breathlessness in advanced disease. February 2017
 Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
ALLERGIES/ SENSITIVITIES This section must be completed before prescribing/administering any drug
 COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
Specialist Palliative Care Audit and Guidelines Group (SPAGG)
") Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
End of Life Care in Dementia. Sue Atkins Dignity in Care/Dementia/Learning Disabilities Clinical Nurse Specialist
 End of Life Care in Dementia Sue Atkins Dignity in Care/Dementia/Learning Disabilities Clinical Nurse Specialist Objectives Understanding the decline in people with dementia To recognise when patients
End of Life Care in Dementia Sue Atkins Dignity in Care/Dementia/Learning Disabilities Clinical Nurse Specialist Objectives Understanding the decline in people with dementia To recognise when patients
PALLIATIVE CARE NEEDS OF PEOPLE WITH DEMENTIA AT END OF LIFE
 PALLIATIVE CARE NEEDS OF PEOPLE WITH DEMENTIA AT END OF LIFE DR. CIARA MCGLADE CONSULTANT GERIATRICIAN MALLOW GENERAL HOSPITAL APRIL 2016 DEMENTIA IN IRELAND 160000 140000 120000 100000 80000 60000 40000
PALLIATIVE CARE NEEDS OF PEOPLE WITH DEMENTIA AT END OF LIFE DR. CIARA MCGLADE CONSULTANT GERIATRICIAN MALLOW GENERAL HOSPITAL APRIL 2016 DEMENTIA IN IRELAND 160000 140000 120000 100000 80000 60000 40000
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Health Learning Partnership End of Life Care 29 th June 2016
 Health Learning Partnership End of Life Care 29 th June 2016 Beth Wright Consultant in Palliative Medicine Case 1 Malignant bowel obstruction Sarah is a 43 year old woman colon cancer, diagnosed in 2014.
Health Learning Partnership End of Life Care 29 th June 2016 Beth Wright Consultant in Palliative Medicine Case 1 Malignant bowel obstruction Sarah is a 43 year old woman colon cancer, diagnosed in 2014.
Polypharmacy: Guidance for Prescribing in Frail Adults
 Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
describe the epidemiological and clinical features along the illness trajectories of specific lifelimiting
 MODULE 3 Palliative assessment and intervention To understand a person's symptoms and identify appropriate intervention strategies, a comprehensive, multidimensional approach to assessment is needed. OVERVIEW
MODULE 3 Palliative assessment and intervention To understand a person's symptoms and identify appropriate intervention strategies, a comprehensive, multidimensional approach to assessment is needed. OVERVIEW
Primary Diagnosis YES NO ICD - Code Cancer Cognitive impairment Cardiac Respiratory Neurological Musculoskeletal Respiratory Other
 Chart review date: / / Reviewer: Centre Name: Hospital Home RACF DOB: / / AGE: GENDER: Male Female Admission Date: / / Death Date: / / 1. DIAGNOSIS Primary Diagnosis YES NO ICD - Code Cancer Cognitive
Chart review date: / / Reviewer: Centre Name: Hospital Home RACF DOB: / / AGE: GENDER: Male Female Admission Date: / / Death Date: / / 1. DIAGNOSIS Primary Diagnosis YES NO ICD - Code Cancer Cognitive
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Foundations of Palliative Care Series
 Foundations of Palliative Care Series Developed by: Tim Sakaluk MD, Ingrid See CPL, Tammy Dyson SW, Sharon Salomons SCP!!!!!! This course was developed in collaboration with the UBC Learning Circle to
Foundations of Palliative Care Series Developed by: Tim Sakaluk MD, Ingrid See CPL, Tammy Dyson SW, Sharon Salomons SCP!!!!!! This course was developed in collaboration with the UBC Learning Circle to
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kelley AS, Morrison RS. Palliative care for the seriously ill.
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kelley AS, Morrison RS. Palliative care for the seriously ill.
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care
 SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
The Role of Palliative Care in Advanced Lung Disease
 The Role of Palliative Care in Advanced Lung Disease Timothy B. Short, MD, FAAFP, FAAHPM Associate Professor, Palliative Medicine University of Virginia Learning Objectives Describe palliative care s approach
The Role of Palliative Care in Advanced Lung Disease Timothy B. Short, MD, FAAFP, FAAHPM Associate Professor, Palliative Medicine University of Virginia Learning Objectives Describe palliative care s approach