REDEFINING PARKINSON S DISEASE
|
|
|
- Dominick Lloyd
- 5 years ago
- Views:
Transcription
1 REDEFINING PARKINSON S DISEASE Did James Parkinson Get It Right? Matthew B. Stern, M.D. University of Pennsylvania USA

2 1 Hoxton Square

3 W. Poewe, Austria J. Obeso, Spain E. Tolosa, Spain M. Stern, USA

4 To delay their publication did not, indeed appear to be warrantable. The disease had escaped particular notice; and the task of ascertaining its nature and cause by anatomical investigation, did not seem likely to be taken up by those who, from their abilities and opportunities, were most likely to accomplish it.




5 James Parkinson s Shaking Palsy Involuntary tremulous motion with lessened muscular power, in parts not in action and even when supported: with a propensity to bend the trunk forwards and to pass from a walking to a running pace: the senses and intellects being uninjured. An Essay on the Shaking Palsy 1817 The shaking palsy had not yet obtained a place in the classification of nosologists.

ID l'.r.us, LU.OUUUJ,l.-S1'Z.&T; A1fD ca&cjilaiid A.")
6 OBG.4NIC BEM.41NS OF.4 FOIIJIEB WORLD EXAMINATION OF THE MINERALIZED RE_MAINS VEGETABLES AND AN IM ALS A N TE D ILU V IA_- W OR L D ; \..,.._. TJ'.U.,... EXTRANEOUS FOSSU.S. By J,tMES f:!rk[ns ON_, Ho.rtou. le. PLATE XIII. THB PfRST VOLUME.; THE VEGETABLE KINGDOM,. LONDON : rw...u l1'c,...nn,l<;iu,.. 4"1u.;TI u:u;::i: 01: =,:: 1:. :: 7,':;::. J./ :, =: l'ID I, UCN, CUC&CIIUIICH ffl.ct; 11.AClt..)ID l'.r.us, LU.OUUUJ,l.-S1'Z.&T; A1fD ca&cjilaiid A.HD,iouu, rljcjiuiy4q.u,uii, e. \.
7 Factoid



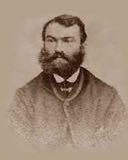
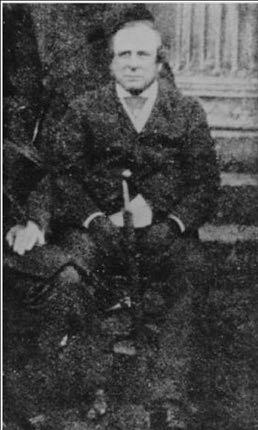
8 James Parkinson The Ale-House Sermon He was rather below the middle stature with an energetic intelligent expression of countenance and of mild and courteous manners. He was always ready to impart information on the subject of medicine and geology. Gideon Mantell




9 Charcot on Parkinson It will provide you with the satisfaction and knowledge that one always gleans from a direct clinical description made by an honest and careful observer. Charcot talking about An Essay on the Shaking Palsy I have seen such patients everywhere on the streets of Rome, of Amsterdam in Spain it is always the same picture they can be identified from afar you do not need a medical history. Charcot Leçons du Mardi 1888
10 So slight and nearly imperceptible are the first inroads of this malady, and so extremely slow its progress, that it rarely happens, that the patient can form any recollection of the precise period of its commencement. The first symptoms... are a slight sense of weakness, with a proneness to trembling in some particular part; sometimes in the head, but most commonly in one of the hands and arms. James Parkinson: An Essay on the Shaking Palsy. London 1817
11 But as the disease proceeds, the hand fails to answer with exactness to the dictates of the will. The legs are not raised to that height, or promptitude which the will directs, so that the utmost care is necessary to prevent frequent falls. Hitherto the patient will have experienced but little inconvenience; and befriended by the strong influence of habitual endurance, would perhaps seldom think of his being the subject of disease, except when reminded of it by the unsteadiness of his hand, whilst writing or employing himself in any nicer kind of manipulation. James Parkinson: An Essay on the Shaking Palsy. 1817
12 The submission of the limbs to the directions of the will can hardly ever be obtained in the performance of the most ordinary offices of life. The fingers cannot be disposed of in the proposed directions, and applied with certainty to any proposed point. The dictates of the will, are even, in the last stages of the disease, conveyed to the muscles but their actions are perverted. James Parkinson: An Essay on the Shaking Palsy. London 1817
 of a number of clinical events.")
13 One of the major developments in our attitude towards Parkinson s disease has been the growth of a concept of Parkinsonism as a syndrome- a symptom- complex which may emanate from various causations. The shaking palsy of James Parkinson is now looked upon as merely one representative (though still the most important) of a number of clinical events. Critchley 1955
14 UK Brain Bank Criteria 175 Years Later Diagnosis of Parkinsonian Syndrome Bradykinesia and at least one of the following: Muscular Rigidity 4-6 Hz rest tremor Postural instability not caused by primary visual, vestibular, cerebellar or proprioceptive dysfunction
15 UK Brain Bank Criteria (Cont.) Supportive prospective positive criteria for Parkinson s disease Three or more required for diagnosis of definite Parkinson s disease in combination with step one. Unilateral onset Rest tremor present Progressive disorder Persistent asymmetry affecting side of onset most Excellent response (70-100%) to levodopa Severe levodopa-induced chorea Levodopa response for 5 years or more Clinical course of ten years or more *From: Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson s disease. A clinico-pathological study of 100 cases. JNNP 1992;55:
16 The Last 25 years: Non-motor Symptoms in PD Prodromal Features? Major features of prodromal PD include the following with various combinations: Olfactory dysfunction Autonomic dysfunction (Orthostatic hypotension, constipation, urinary and erectile dysfunctions) Sleep and wake disorders (Insomnia, excessive daytime sleepiness, Rem Sleep Behavior Disorder (RBD)) Psychiatric (depression and anxiety) and cognitive impairments (MCI, dementia) Subtle motor dysfunctions Chaudhuri and Schapira, Lancet Neurol 2009, Berg et al, Mov Disord 2015, Sauerbier et al Park Rel Disorders 2015,

17 Natural History of Parkinson s Disease Premanifest Phase Clinical PD Dopamine (and other) neurons Symptom severity BIOMARKER Diagnosis Braak H, et al. Neurobiol Aging, 2003;24:

18 Movement Disorders 27:54-60, 2012
19 PD: A NEW DIAGNOSTIC APPROACH PHASE 1 PHASE 2 PHASE 3 Preclinical PD (molecular markers of PD) Non-Motor PD (hyposmia, Cardiac, GI, RBD, etc) Motor PD (Early Motor, Monosymptomatic) (Classic Neurologic Manifestations)
20 The International Parkinson and Movement Disorder Society Task Force The Definition of Parkinson s Disease Dr. Ron Postuma (Co-Chair) Dr. Daniela Berg (Co-Chair)
, the International Parkinson and Movement Disorders Society (MDS) commissioned a task force to consider")
21 Mov Disord 2014 With advances in knowledge disease boundaries may change. Occasionally, these changes are of such a magnitude that they require redefinition of the disease. In recognition of the profound changes in our understanding of Parkinson s disease (PD), the International Parkinson and Movement Disorders Society (MDS) commissioned a task force to consider a redefinition of PD.
22 Major Issues in Redefining PD The Clinical vs. Pathologic Gold Standard Is PD a syndrome with many causes (genetic, etc)? PD versus LBD (cognitive >>motor) PD subtypes
23 Issue 1: What is the Gold Standard? Current Thinking A motor syndrome with levodopa responsive Parkinsonism Pathologic confirmation of alpha-synuclein deposition and neuronal loss in the substantia nigra pars compacta If the pathology is not found, the clinical diagnosis is incorrect. Similarly, the pathology is incidental in the absence of a clinical syndrome
24 Alternative Gold Standards Should we remain true to James Parkinson and define PD as only a clinical syndrome? Should genetics be the ultimate standard since pathology can vary among the different genetic causes? Problems: Genetics accounts for a small proportion of all PD cases
25 Moving Forward: The MDS Task Force The core criteria of a clinical syndrome accompanied by SN degeneration and synuclein pathology remain a gold standard until reliable biomarkers of CNS pathology are developed. A separate clinicogenetic category be established to include those patients with the classic clinical syndrome regardless of synuclein deposition. A new approach to genetic classification which differentiates between causative and risk factor genes
26 Issue #2: What Fits Under the PD Umbrella? The issue: A patient developed cognitive impairment 18 months after PD diagnosis; he has PD dementia (PDD). Another developed cognitive impairment 10 months after PD diagnosis; according to current definitions, the initial diagnosis was wrong, and she has DLB. Does this make sense? (i.e. is the 1 year rule valid?)
.")
27 Simplified model of how the type of cortical pathology and clinical presentation of PDD and DLB might interact. Dementia in DLB/PD is associated with two major pathologies: synucleinopathy (i.e., Parkinson pathology) and neuritic amyloidopathy (i.e., Alzheimer pathology). In PD patients who develop dementia very late in their illness, or not at all (far left), neuritic amyloid deposition is minimal (or absent), and cortical pathology is mainly that of a-syn deposition. At the other extreme, DLB patients with predominant neuritic amyloid deposition and very minimal a-syn deposition would usually be diagnosed as AD during life, developing clinical DLB hallmarks late (if at all). Between these two extremes of the spectrum lie the most patients with PD and DLB.
28 Issue #3: PD Subtypes The issue: A patient had unilateral tremor onset at age 40, robust L-dopa response with fluctuations and, 20 years later, has few nonmotor features. A second developed bilateral bradykinesia and rigidity at age 80 and had no fluctuations, but had severe constipation, urinary dysfunction, sleep disturbance, and depression, eventually dying with dementia. Do these patients have the same disease?
29 Moving Forward: the MDS Task Force Clinical subtypes should only be delineated if there are clear data that demonstrate consistent, large differences in prognosis, predicted disease manifestations, or treatment. Currently, it is unclear whether any of the current subtype classifications qualify. The search for subtypes should not be restricted to clinical features, but should include subtypes of molecular pathogenesis.
30 Issue #4: The Beginning of PD The issue: A patient has RBD, olfactory loss, constipation, and depression, but no parkinsonism. Dopaminergic neuroimaging and SN ultrasound are abnormal. Doesn t this patient have PD?
31 Issue #5: Developing New Diagnostic Criteria No standard clinical criteria exist. Many criteria have been proposed for PD, but none have been developed or adopted by an international organization such as the MDS. New knowledge: Diagnostic criteria must accommodate new findings. The systemic character of the disease needs to be acknowledged, especially incorporating nonmotor symptoms. Ancillary testing: Currently, PD diagnoses are generally made clinically, without requiring additional diagnostic tests. Moreover, as knowledge advances, diagnostic biochemical markers, neuroimaging, or means to document a-syn deposition may become clinically available..
 3. No red flags CLINICALLY PROBABLE PD 1.")
32 2015 DIAGNOSIS OF PD Parkinsonism (Bradykinesia with either rigidity, tremor or both) PLUS: CLINICALLY ESTABLISHED PD: 1. Absence of absolute exclusion criteria 2. Atleast two supportive criteria (levodopa response, dyskinesia, hyposmia, positive DAT, cardiac sympathetic denervation by SPECT) 3. No red flags CLINICALLY PROBABLE PD 1. Absence of absolute exclusion criteria (cerebellar signs, vertical gaze abn) 2. Presence of red flags (rapid progression, no progression, falls, autonomic failure counterbalanced by supportive criteria
33 The Next Step in Redefining PD: CASE: A 55 year old man consults a sleep specialist for treatment of REM Sleep Behavior Disorder. Additional studies by a forward thinking Neurologist reveal severe hyposmia and significantly reduced dopamine transporter binding (<65% of normal) bilaterally. He has misfolded alpha synuclein aggregates detected in the CSF. He has never had neurologic symptoms although has had periods of depression and constipation. QUESTION: Does this patient have Parkinson s Disease? ANSWER: YES!!!!
34 The year is The patient is now 65 and has been treated with anti-synuclein agents, antioxidants and mitochondrial membrane stabilizers combined into 1 capsule. He has been advised to drink coffee (and start smoking). He rides his bike 10 miles every day. He has never developed neurologic symptoms... But he still has Parkinson s disease
35 Did James Parkinson Get It Right? Not exactly, but regardless of our refinements in definition, he came pretty close!!!!
36 "Progress is impossible without change, and those who cannot change their minds cannot change anything." -- George Bernard Shaw
37
38
 Peripheral Autonomic Nervous System (heart, intestinal tract, bladder) Neocortex Olfactory Cortex Temporal Cortex Langston, Ann.Neurol.")
39 The Parkinson s Complex Parkinsonism Substantia Nigra Medulla Pons Amygdala Basal Forebrain Hypothalamus Olfactory bulb Spinal Cord (intermediolateral column) Peripheral Autonomic Nervous System (heart, intestinal tract, bladder) Neocortex Olfactory Cortex Temporal Cortex Langston, Ann.Neurol. 2006;59(4):
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
The Parkinson s You Can t See
 The Parkinson s You Can t See We principally see the motor phenomena of Parkinson's disease, but is there an early stage without visible features? Might this provide a window for disease-modifying therapy?
The Parkinson s You Can t See We principally see the motor phenomena of Parkinson's disease, but is there an early stage without visible features? Might this provide a window for disease-modifying therapy?
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
How to Diagnose Early (Prodromal) Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.
 Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.") How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Early Clinical Features of Parkinson s Disease and Related Disorders. Dr. Alastair Noyce
 1 Specialist Registrar in Neurology, London Deanery Parkinson s UK Doctoral Research Fellow Project lead for PREDICT-PD Declarations Salary: Parkinson's UK, Barts and the London NHS Trust Grants: Parkinson's
1 Specialist Registrar in Neurology, London Deanery Parkinson s UK Doctoral Research Fellow Project lead for PREDICT-PD Declarations Salary: Parkinson's UK, Barts and the London NHS Trust Grants: Parkinson's
Parkinson's Disease KP Update
 Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn
 Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn Objectives What agents do we currently have available and what do we ideally need? What biomarkers exist for
Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn Objectives What agents do we currently have available and what do we ideally need? What biomarkers exist for
The Latest Research in Parkinson s Disease. Lawrence Elmer, MD, PhD Professor, Dept. of Neurology University of Toledo
 The Latest Research in Parkinson s Disease Lawrence Elmer, MD, PhD Professor, Dept. of Neurology University of Toledo OR.. Rethinking Parkinson s Disease Lawrence Elmer, MD, PhD Professor, Dept. of Neurology
The Latest Research in Parkinson s Disease Lawrence Elmer, MD, PhD Professor, Dept. of Neurology University of Toledo OR.. Rethinking Parkinson s Disease Lawrence Elmer, MD, PhD Professor, Dept. of Neurology
Origins. Update on Parkinson s Disease
 Update on Parkinson s Disease Melinda Burnett, MD Origins First described in 1817 by James Parkinson: Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported;
Update on Parkinson s Disease Melinda Burnett, MD Origins First described in 1817 by James Parkinson: Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported;
DEMENTIA IN PARKINSON`S DISEASE. DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD
 Director-Parkinson`s Disease Service for the Older Person HNELHD") DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s
DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE
 FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE DEE SILVER M.D MOVEMENT DISORDER SPECIALIST MEDICAL DIRECTOR -- PARKINSON ASSOCIATION OF SAN DIEGO 1980 TO PRESENT SCRIPPS MEMORIAL HOSPITAL, LA JOLLA CA.
FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE DEE SILVER M.D MOVEMENT DISORDER SPECIALIST MEDICAL DIRECTOR -- PARKINSON ASSOCIATION OF SAN DIEGO 1980 TO PRESENT SCRIPPS MEMORIAL HOSPITAL, LA JOLLA CA.
Moving fast or moving slow: an overview of Movement Disorders
 Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Learnings from Parkinson s disease: Critical role of Biomarkers in successful drug development
 Learnings from Parkinson s disease: Critical role of Biomarkers in successful drug development Ken Marek Coalition Against Major Diseases and FDA 2014 Annual Scientific Workshop Oct 2014 Disclosure Co-founder
Learnings from Parkinson s disease: Critical role of Biomarkers in successful drug development Ken Marek Coalition Against Major Diseases and FDA 2014 Annual Scientific Workshop Oct 2014 Disclosure Co-founder
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Moving Treatment Earlier Disease Modification in Early PD
 Moving Treatment Earlier Disease Modification in Early PD Ron Postuma Montreal General Hospital McGill University Disclosures: - Grants: Fonds de la Recherche en Sante Quebec, Canadian Institute of Health
Moving Treatment Earlier Disease Modification in Early PD Ron Postuma Montreal General Hospital McGill University Disclosures: - Grants: Fonds de la Recherche en Sante Quebec, Canadian Institute of Health
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Non-motor subtypes of Early Parkinson Disease in the Parkinson s Progression Markers Initiative
 Non-motor subtypes of Early Parkinson Disease in the Parkinson s Progression Markers Initiative Samay Jain, MD MSc Seo Young Park, PhD University of Pittsburgh Department of Neurology and Center for Research
Non-motor subtypes of Early Parkinson Disease in the Parkinson s Progression Markers Initiative Samay Jain, MD MSc Seo Young Park, PhD University of Pittsburgh Department of Neurology and Center for Research
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
La neurosonologia. Ecografia cerebrale e nuove applicazioni nelle malattie neurodegenerative. Nelle patologie degenerative e vascolari cerebrali
 La neurosonologia Nelle patologie degenerative e vascolari cerebrali Andrea Pilotto Ecografia cerebrale e nuove applicazioni nelle malattie neurodegenerative Prof. Daniela Berg Department of Neurodegeneration
La neurosonologia Nelle patologie degenerative e vascolari cerebrali Andrea Pilotto Ecografia cerebrale e nuove applicazioni nelle malattie neurodegenerative Prof. Daniela Berg Department of Neurodegeneration
Non-motor symptoms as a marker of. Michael Samuel
 Non-motor symptoms as a marker of progression in Parkinson s s disease Michael Samuel London, UK 1 Definitions and their problems Non-motor symptoms as a marker of progression Non-motor symptoms (NMS)
Non-motor symptoms as a marker of progression in Parkinson s s disease Michael Samuel London, UK 1 Definitions and their problems Non-motor symptoms as a marker of progression Non-motor symptoms (NMS)
Making Every Little Bit Count: Parkinson s Disease. SHP Neurobiology of Development and Disease
 Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Welcome and Introductions
 Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
UNDERSTANDING PARKINSON S AND THE POWER OF INTENT. Samantha Elandary, MA, CCC-SLP Founder & Chief Executive Officer Parkinson Voice Project
 UNDERSTANDING PARKINSON S AND THE POWER OF INTENT Samantha Elandary, MA, CCC-SLP Founder & Chief Executive Officer Parkinson Voice Project What is Parkinson s? TOOLS FOR MANAGING PARKINSON S! Medications!
UNDERSTANDING PARKINSON S AND THE POWER OF INTENT Samantha Elandary, MA, CCC-SLP Founder & Chief Executive Officer Parkinson Voice Project What is Parkinson s? TOOLS FOR MANAGING PARKINSON S! Medications!
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
Movement Disorders- Parkinson s Disease. Fahed Saada, MD March 8 th, th Family Medicine Refresher Course St.
 Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz. Parkinson s Disease. A Guide to Medical Treatment
 M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
Comprehensive Approach to DLB Management
 Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinsons Disease & Movement Disorder Aug 11-13, Frankfurt l Dr. Geeta Shroff
 USE OF HUMAN EMBRYONIC STEM CELLS IN THE TREATMENT OF PARKINSON S DISEASE Dr. Geeta Shroff Founder and Medical Director, Nutech Mediworld CONDITIONS TREATED Spinal Cord Injury Cell Culture Technology Diabetes
USE OF HUMAN EMBRYONIC STEM CELLS IN THE TREATMENT OF PARKINSON S DISEASE Dr. Geeta Shroff Founder and Medical Director, Nutech Mediworld CONDITIONS TREATED Spinal Cord Injury Cell Culture Technology Diabetes
MAXIMIZING FUNCTION IN PARKINSON S DISEASE
 1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
Welcome and Introductions
 Parkinson s Disease Spotlight on Addressing Motor and Non-Motor Symptoms The Changing Landscape Wednesday, March 8, 2017 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Parkinson s Disease Spotlight on Addressing Motor and Non-Motor Symptoms The Changing Landscape Wednesday, March 8, 2017 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Part I Parkinson Disease Diagnosis and Treatment
 Part I Parkinson Disease Diagnosis and Treatment Parkinson Disease A Health Policy Perspective. Edited by Wayne Martin, Oksana Suchowersky, Katharina Kovacs Burns, and Egon Jonsson Copyright 2010 WILEY-VCH
Part I Parkinson Disease Diagnosis and Treatment Parkinson Disease A Health Policy Perspective. Edited by Wayne Martin, Oksana Suchowersky, Katharina Kovacs Burns, and Egon Jonsson Copyright 2010 WILEY-VCH
IMPAIRMENT OF THE NERVOUS SYSTEM
 IMPAIRMENT OF THE NERVOUS SYSTEM The following information provides criteria for the evaluation of permanent impairment resulting from dysfunction brain, spinal cord and cranial nerves and certain peripheral
IMPAIRMENT OF THE NERVOUS SYSTEM The following information provides criteria for the evaluation of permanent impairment resulting from dysfunction brain, spinal cord and cranial nerves and certain peripheral
Issues for Patient Discussion
 onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
USING PRECISION MEDICINE TO HELP PATIENTS WITH PARKINSON S DISEASE. The Michael J. Fox Foundation for Parkinson s Research
 USING PRECISION MEDICINE TO HELP PATIENTS WITH PARKINSON S DISEASE The Michael J. Fox Foundation for Parkinson s Research MJFF IS THE WORLD S LARGEST NONPROFIT FUNDER OF PD RESEARCH Our Mission We are
USING PRECISION MEDICINE TO HELP PATIENTS WITH PARKINSON S DISEASE The Michael J. Fox Foundation for Parkinson s Research MJFF IS THE WORLD S LARGEST NONPROFIT FUNDER OF PD RESEARCH Our Mission We are
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
14 - Central Nervous System. The Brain Taft College Human Physiology
 14 - Central Nervous System The Brain Taft College Human Physiology Development of the Brain The brain begins as a simple tube, a neural tube. The tube or chamber (ventricle) is filled with cerebrospinal
14 - Central Nervous System The Brain Taft College Human Physiology Development of the Brain The brain begins as a simple tube, a neural tube. The tube or chamber (ventricle) is filled with cerebrospinal
Pietro Cortelli. IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna
 Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna HYSTORY 1900 description of OPCA (Dejerine, Thomas) 1960 description of Shy-Drager
Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna HYSTORY 1900 description of OPCA (Dejerine, Thomas) 1960 description of Shy-Drager
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Lecture XIII. Brain Diseases I - Parkinsonism! Brain Diseases I!
 Lecture XIII. Brain Diseases I - Parkinsonism! Bio 3411! Wednesday!! Lecture XIII. Brain Diseases - I.! 1! Brain Diseases I! NEUROSCIENCE 5 th ed! Page!!Figure!!Feature! 408 18.9 A!!Substantia Nigra in
Lecture XIII. Brain Diseases I - Parkinsonism! Bio 3411! Wednesday!! Lecture XIII. Brain Diseases - I.! 1! Brain Diseases I! NEUROSCIENCE 5 th ed! Page!!Figure!!Feature! 408 18.9 A!!Substantia Nigra in
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Motor Fluctuations in Parkinson s Disease
 Motor Fluctuations in Parkinson s Disease Saeed Bohlega, MD, FRCPC Senior Distinguished Consultant Department of Neurosciences King Faisal Specialist Hospital & Research Centre Outline Type of fluctuations
Motor Fluctuations in Parkinson s Disease Saeed Bohlega, MD, FRCPC Senior Distinguished Consultant Department of Neurosciences King Faisal Specialist Hospital & Research Centre Outline Type of fluctuations
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Headway Victoria Epilepsy and Parkinson s Centre
 Headway Victoria Epilepsy and Parkinson s Centre Parkinson s Overview and Medication Shannon Oatway Community Education/ Awareness Coordinator What is Parkinson s Disease? The basics It is a chronic and
Headway Victoria Epilepsy and Parkinson s Centre Parkinson s Overview and Medication Shannon Oatway Community Education/ Awareness Coordinator What is Parkinson s Disease? The basics It is a chronic and
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
Atypical parkinsonism
 Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
The Marmoset Monkey as Model for Neurological Disorders
 The Marmoset Monkey as Model for Neurological Disorders Jan Langermans and Ingrid Philippens From Laboratory to Clinic Disease models neuroscience: Parkinson, Sleep, Stress, Alzheimer, MS MS Models: rhmog
The Marmoset Monkey as Model for Neurological Disorders Jan Langermans and Ingrid Philippens From Laboratory to Clinic Disease models neuroscience: Parkinson, Sleep, Stress, Alzheimer, MS MS Models: rhmog
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Cheyenne 11/28 Neurological Disorders II. Transmissible Spongiform Encephalopathy
 Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
FDG-PET e parkinsonismi
 Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Multiple System Atrophy
 Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Prion-like propagation of alpha-synuclein aggregates in the brain of wild-type mice
 Prion-like propagation of alpha-synuclein aggregates in the brain of wild-type mice Nolwen L. Rey, PhD Patrik Brundin s Laboratory, Van Andel Research Institute Grand Rapids, Michigan, USA 15th Annual
Prion-like propagation of alpha-synuclein aggregates in the brain of wild-type mice Nolwen L. Rey, PhD Patrik Brundin s Laboratory, Van Andel Research Institute Grand Rapids, Michigan, USA 15th Annual
Managing Movement Disorders in the older patient
 Managing Movement Disorders in the older patient Dr Jan Gregson 24 November 2017 With thanks to Dr Kirsten Holst, Physician and Geriatrician, MidCentral DHB I guess I am not an expert in the area of prescribing
Managing Movement Disorders in the older patient Dr Jan Gregson 24 November 2017 With thanks to Dr Kirsten Holst, Physician and Geriatrician, MidCentral DHB I guess I am not an expert in the area of prescribing
Basal ganglia motor circuit
 Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
UPDATE ON RESEARCH IN PARKINSON S DISEASE
 UPDATE ON RESEARCH IN PARKINSON S DISEASE Charles H. Adler, M.D., Ph.D. Professor of Neurology Mayo Clinic College of Medicine Co-Principal Investigator Arizona Parkinson s Disease Consortium Arizona Study
UPDATE ON RESEARCH IN PARKINSON S DISEASE Charles H. Adler, M.D., Ph.D. Professor of Neurology Mayo Clinic College of Medicine Co-Principal Investigator Arizona Parkinson s Disease Consortium Arizona Study
Malattia di Parkinson: patogenesi molecolare e nuove strategie terapeutiche
 LA NEUROSONOLOGIA NELLE PATOLOGIE DEGENERATIVE E VASCOLARI CEREBRALI San Benedetto del Tronto 6-8 novembre 2017 Malattia di Parkinson: patogenesi molecolare e nuove strategie terapeutiche Giuseppe De Michele
LA NEUROSONOLOGIA NELLE PATOLOGIE DEGENERATIVE E VASCOLARI CEREBRALI San Benedetto del Tronto 6-8 novembre 2017 Malattia di Parkinson: patogenesi molecolare e nuove strategie terapeutiche Giuseppe De Michele
PSYCHOSIS IN PARKINSON'S DISEASE
 PSYCHOSIS IN PARKINSON'S DISEASE Objectives Identify neurobiological substrates associated with Parkinson s disease psychosis Describe the differences between older antipsychotics and novel therapies for
PSYCHOSIS IN PARKINSON'S DISEASE Objectives Identify neurobiological substrates associated with Parkinson s disease psychosis Describe the differences between older antipsychotics and novel therapies for
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
WELCOME. Parkinson s 101 for the Newly Diagnosed. Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW
 WELCOME Parkinson s 101 for the Newly Diagnosed Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW Parkinson s Disease 101 Presenter for Today Cari Friedman, LCSW Patient and Family Service
WELCOME Parkinson s 101 for the Newly Diagnosed Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW Parkinson s Disease 101 Presenter for Today Cari Friedman, LCSW Patient and Family Service
Update on Parkinson s disease and other Movement Disorders October 2018
 Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Date of Referral: Enhanced Primary Care Pathway: Parkinson s Disease
 Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
ASSFN Clinical Case: Bilateral STN DBS Implant for Parkinson s Disease
 ASSFN Clinical Case: Bilateral STN DBS Implant for Parkinson s Disease Parkinson s Disease Cardinal Signs: Resting tremor Rigidity Bradykinesia Postural instability Other Symptoms Dystonia Dysphagia Autonomic
ASSFN Clinical Case: Bilateral STN DBS Implant for Parkinson s Disease Parkinson s Disease Cardinal Signs: Resting tremor Rigidity Bradykinesia Postural instability Other Symptoms Dystonia Dysphagia Autonomic
17 th WORKSHOP ON NEUROOTOLOGY. Dementia & Imbalance. DR. ATRI CHATTERJEE Assistant Professor. Neurology VMMC & SafdarJung Hospital New Delhi
 17 th WORKSHOP ON NEUROOTOLOGY Dementia & Imbalance DR. ATRI CHATTERJEE Assistant Professor. Neurology VMMC & SafdarJung Hospital New Delhi ?Association Dementia Imbalance?Causation balance: An even distribution
17 th WORKSHOP ON NEUROOTOLOGY Dementia & Imbalance DR. ATRI CHATTERJEE Assistant Professor. Neurology VMMC & SafdarJung Hospital New Delhi ?Association Dementia Imbalance?Causation balance: An even distribution
Part I: 2017 UPDATE ON OUR CURRENT UNDERSTANDING OF PARKINSON DISEASE
 Part I: 2017 UPDATE ON OUR CURRENT UNDERSTANDING OF PARKINSON DISEASE Hubert H. Fernandez, MD, FAAN Cleveland Clinic Cleveland, OH In the last decade, advancements in pathology, genetics, biomarkers, and
Part I: 2017 UPDATE ON OUR CURRENT UNDERSTANDING OF PARKINSON DISEASE Hubert H. Fernandez, MD, FAAN Cleveland Clinic Cleveland, OH In the last decade, advancements in pathology, genetics, biomarkers, and
Imaging biomarkers for Parkinson s disease
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 6 MDS-ES/EAN: Neuroimaging in movement disorders - Level 2 Imaging biomarkers for Parkinson
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 6 MDS-ES/EAN: Neuroimaging in movement disorders - Level 2 Imaging biomarkers for Parkinson