Parkinson s Disease. Sirilak yimcharoen
|
|
|
- Darleen Nichols
- 5 years ago
- Views:
Transcription
1 Parkinson s Disease Sirilak yimcharoen
2 EPIDEMIOLOGY ~1% of people over 55 years Age range years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically before age 45 years)

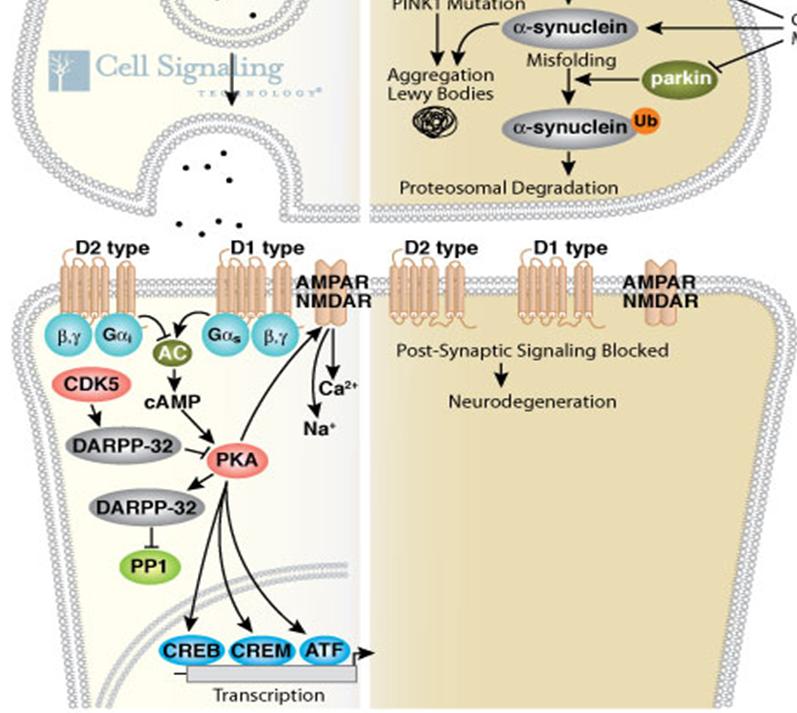
3 PATHOGENESIS Microscopic presence of Lewy bodies in the remaining neurons Genetic :earlier age onset


4 Etiology Degradation of dopaminergic neurons in the substantia nigra
5
6 CLINICAL FEATURES Symptoms Motor symptoms Non motor symptoms cardinal signs rest tremor rigidity bradykinesia
7 Motor symptoms Tremor, bradykinesia, rigidity, postural instability Hypominia, dysarthria, dysphagia, Decreased arm swing, difficult arising from chair micrographia Glabellar reflex, blebphalospasm, dystonia, camptocormia, scoliosis
8 Bradykinesia most characteristic clinical feature manifestations of bradykinesia slowness of movement loss of spontaneous movements and gesturing drooling monotonic and hypophonic dysarthria loss of facial expression Freezing(motor blocks) is a form of akinesia
9 Bradykinesia correlate best with degree of dopamine deficiency Assessment of bradykinesia rapid, repetitive, alternating movements of the hand observing not only slowness but also decrementing amplitude
10 Tremor Rest tremor is the most common unilateral, frequency between 4 and 6 Hz Hand tremors are described as supination pronation ( pill-rolling ) involve :lips, chin, jaw and legs rarely involve: the neck/head responsive to dopaminergic therapy

11 Rigidity increased resistance cogwheel Postural deformities Camptocormia
12 Non-motor symptoms Mental problem : dementia, depression, apathy Autonomic disturbance : postural hypotension, constipation, bladder dysfunction Sensory symptom : anosmia, ageusia, paresthesia Sleep disturbance
13 Diagnostic criteria UK Parkinson s Disease Society Brain Bank s clinical criteria for the diagnosis of probable Parkinson s disease Step 1 Bradykinesia At least one of the following criteria: Rigidity 4 6 Hz rest tremor Postural instability not caused by primary visual, vestibular, cerebellar or proprioceptive dysfunction Step 2 Exclude other causes of parkinsonism Step 3 At least three of the following supportive (prospective) criteria: Unilateral onset Rest tremor Progressive disorder Persistent asymmetry primarily affecting side of onset Excellent response (70 100%) to levodopa Severe levodopa induced chorea (dyskinesia) Levodopa response for 5 years or more Clinical course of 10 years or more
14 National Institute of Neurological Disorders and Stroke (NINDS) diagnostic criteria for Parkinson s disease Group A features (characteristic of PD) Resting tremor Bradykinesia Rigidity Asymmetric onset Group B features (suggestive of alternative diagnoses) Features unusual early in the clinical course Prominent postural instability in the first 3 years after symptom onset Freezing phenomenon in the first 3 years Hallucinations unrelated to medications in the first 3 years Dementia preceding motor symptoms or in the first year Supranuclear gaze palsy (other than restriction of upward gaze) or slowing of vertical saccades Severe, symptomatic dysautonomia unrelated to medications Documentation of condition known to produce parkinsonism and plausibly connected to the patient s symptoms (such as suitably located focal brain lesions or neuroleptic use within the past 6 months)
15 National Institute of Neurological Disorders and Stroke (NINDS) diagnostic criteria for Parkinson s disease Criteria for definite PD All criteria for probable Parkinson s are met and Histopathological confirmation of the diagnosis is obtained at autopsy Criteria for probable PD At least three of the four features in group A are present and None of the features in group B is present (note: symptom duration 3 years is necessary to meet this requirement) and Substantial and sustained response to levodopa or a dopamine agonist has been documented Criteria for possible PD At least two of the four features in group A are present; at least one of these is tremor or bradykinesia and Either none of the features in group B is present or symptoms have been present 3 years and none of the features in group B is present and Either substantial and sustained response to levodopa or a dopamine agonist has been documented or the patient has not had an adequate trial of levodopa or a dopamine agonist
16 Disease staging and assessment Hoehn and Yahr Staging UPDRS 0 No signs of disease. There are 6 major parts; 1 Unilateral disease. 1. Mentation, behavior and mood Bilateral disease, without impairment 2 2. Activities of daily living of balance. 3. Motor examination 3 Mild to moderate bilateral disease; some postural instability; physically independent. 4. Complication of therapy 5. Modified Hoehn and Yahr staging 6. Schwab and England Severe disability; still able to walk or 4 activites of daily living scale stand unassisted. 5 Wheelchair bound or bedridden unless aided.
17 Differential diagnosis of parkinsonism 1. Primary parkinsonism parkinson s disease Juvenile parkinsonism 3. Parkinson plus disorder Multiple system atrophy Cortico-basal ganglionic degeneration Progressive supranuclear palsy 5. Secondary parkinsonism Drug-induced Vascular parkinsonism
18 Differential diagnosis of parkinsonism 3. Secondary parkinsonism Normal pressure hydrocephalus Toxin-induced Infectious 4. Heredodegenerative parkinsonism Dementia with Lewy Bodies Huntington disease Wilson disease

19 Treatment Algorithm
20 Treatment Algorithm Anticholinergics (Tremor) Dopamine agonists Pharmacologic 65 yrs >65 yrs Add COMT inh., MAO-B inh., or others Dopamine replacement Clinical pearls in drug selection Age Cognitive function Severity of motor features Response to previous PD treatment
21 3OMD Peripheral organ COM T 3OMD Alphasynuclein COM T NMDA R

22 Peripheral organ 3OMD COM T Entacapon e Tolcapone Benserazid e Carbidopa 3OMD Alphasynuclein COM T Amantadin e NMDA R Selegiline Rasagiline Dopamin e agonists
 Start with low dose")

23 Dopamine Replacement L-dopa/Benserazide (4:1), L-dopa/Carbidopa (10:1) Start with low dose (prefer regular release) Select appropriate preparation Beware of motor complications (later disease)
24 Complications from levodopa Motor complications Wearing off effect On-off effect Peak-dose dyskinesia Non-motor complications Psychosis Hallucination Autonomic symptoms e.g. constipation

25 Motor Complications from Levodopa Level of levodopa in the body Wearing off Time Peak dose dyskinesia On 3me Off 3me Dose Dose Dose Dose Dose treating_pd_with_medications/what_is_wearing_off/
26 Management of Motor Wearing off Complications On-off Peak dose Symptom deterioration Random deterioration Too much movement Predictable Unpredictable dose ± frequency, add an3dykine3cs frequency, controlled release DT, add other drugs
 Fibrosis:")

 Caution: Sleep attack was")

27 CNS Drugs 2010; 24 (11): Ergot Dopamine agonists e.g. Caution: Fibrosis e.g. heart valve, lung (dose and time of exposure related) Fibrosis: stimulation of 5- HT2B that may potentiate inflammation Nonergot e.g. pramiprexol, ropinirole Benefit when use in early disease Bromocriptine (delays the use of levodopa) Start low, go slow (better tolerate with evening dose) Caution: Sleep attack was first reported in pt treated with ropinirole and pramiprexol Use in management of motor complications e.g. dyskinesia esp. long acting

28 COMT Inhibitors Entacapone and Tolcapone (not available in Thailand) Benefit Reduce dose of levodopa Use to treat motor complications Cautions Autonomic symptoms e.g. diarrhea levodopa Hepatotoxic esp. tolcapone Monitor liver function closely in first 6 mons. European Handbook of Neurological Management (2 nd Ed), 2011
, 2011")
29 MAO-B Inhibitors Selegiline and Rasagiline Benefit Neuroprotective Cautions Drug interaction CYP2B6, CYP2C19 SSRI, lithium, imipramine à risk of serotonin syndrome Selegiline metabolite is amphetamine derivatives Minimal effects e.g. insomnia, hallucination European Handbook of Neurological Management (2 nd Ed), 2011
 Cognitive impairment (due to")
30 Brain and Cogni3on 68 (2008) , Pharmacology & Therapeu3cs 117 (2008) Anticholinergics Trihexylphenidyl, benztropine Benefit Tremor predominant Cautions Anticholinergic side effects (start low, go slow) Cognitive impairment (due to M1 machr)
31 NMDA-receptor antagonist
 Management of motor complication esp.")
32 European Handbook of Neurological Management (2 nd Ed), 2011 NMDA-receptor antagonist Amantadine Benefit Inhibit excitatory pathway (glutamic pathway) Management of motor complication esp. dyskinesia Caution Dose adjustment in renal impairment
33 The end
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
MAXIMIZING FUNCTION IN PARKINSON S DISEASE
 1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
2-The age at onset of PD is variable, usually between 50 and 80 years, with a mean onset of 55 years (1).
.") Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
2/20/18. History of Parkinson s. What is happening in the brain? DOPAMINE! Epidemiology. Parkinson s Disease. It s much more than tremor
 Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Parkinson s Disease. Patients will ask you. 8/14/2015. Objectives
 Parkinson s Disease Jean Van Kingsley MS, FNP-BC Objectives Describe the pathophysiolgy of PD. Review clinical charachteristics of PD. Identify management strategies, to maximize functional status. Recognize
Parkinson s Disease Jean Van Kingsley MS, FNP-BC Objectives Describe the pathophysiolgy of PD. Review clinical charachteristics of PD. Identify management strategies, to maximize functional status. Recognize
Movement Disorders. Eric Kraus, MD! Neurology!
 Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to
 parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz. Parkinson s Disease. A Guide to Medical Treatment
 M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Parts of the motor circuits
 MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
8/28/2017. Behind the Scenes of Parkinson s Disease
 BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1)
") 475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Form B3L: UPDRS Part III Motor Examination 1
 Initial Visit Packet NACC Uniform Data Set (UDS) LBD MODULE Form B3L: UPDRS Part III Motor Examination 1 ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to
Initial Visit Packet NACC Uniform Data Set (UDS) LBD MODULE Form B3L: UPDRS Part III Motor Examination 1 ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
Parkinson s Disease Update. Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015
 Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Drugs for Neurodegenerative Diseases 2 Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 DRUGS USED IN PARKINSON S DISEASE/ B. Selegiline and rasagiline Selegiline, also called
DRUGS THAT ACT IN THE CNS Drugs for Neurodegenerative Diseases 2 Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 DRUGS USED IN PARKINSON S DISEASE/ B. Selegiline and rasagiline Selegiline, also called
Margo J Nell Dept Pharmacology
 Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Drugs Affecting the Central Nervous System
 Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Alison Charleston 1 st September 2016
 Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
PARKINSON S MEDICATION
 PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
Objectives. Distinguishing Parkinson s disease from other parkinsonian and tremor syndromes. Characteristics. Basal Ganglia Structures
 12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
Re-Submission. Scottish Medicines Consortium. rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.
 (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.") Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
Medications used to treat Parkinson s disease
 Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
UNDERSTANDING PARKINSON S DISEASE
 UNDERSTANDING PARKINSON S DISEASE WHAT IS PARKINSON S DISEASE? A progressive disease of the nervous system marked by tremor, muscular rigidity, and slow, imprecise movement, chiefly affecting middleaged
UNDERSTANDING PARKINSON S DISEASE WHAT IS PARKINSON S DISEASE? A progressive disease of the nervous system marked by tremor, muscular rigidity, and slow, imprecise movement, chiefly affecting middleaged
Understanding Parkinson s Disease Important information for you and your loved ones
 Patient Education Understanding Parkinson s Disease Important information for you and your loved ones This handout explains the signs, symptoms, and possible treatments of Parkinson s disease. Parkinson
Patient Education Understanding Parkinson s Disease Important information for you and your loved ones This handout explains the signs, symptoms, and possible treatments of Parkinson s disease. Parkinson
Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn
 Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn Objectives What agents do we currently have available and what do we ideally need? What biomarkers exist for
Presented by Meagan Koepnick, Josh McDonald, Abby Narayan, Jared Szabo Mentored by Dr. Doorn Objectives What agents do we currently have available and what do we ideally need? What biomarkers exist for
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Pal Riba, M.D., Ph.D. Department of Pharmacology and Pharmacotherapy Semmelweis University, Budapest, Hungary November 7, 2017
 Pal Riba, M.D., Ph.D. Department of Pharmacology and Pharmacotherapy Semmelweis University, Budapest, Hungary November 7, 2017 Definition of neurodegeneration Irreversible death of neurons resulting in
Pal Riba, M.D., Ph.D. Department of Pharmacology and Pharmacotherapy Semmelweis University, Budapest, Hungary November 7, 2017 Definition of neurodegeneration Irreversible death of neurons resulting in
9/26/18. Objectives. Disclosures. Parkinson s Disease Update Clinical and Operational Considerations
 Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Moving fast or moving slow: an overview of Movement Disorders
 Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
DRUG TREATMENT OF PARKINSON S DISEASE. Mr. D.Raju, M.pharm, Lecturer
 DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
EBM Parkinson s Diseases
 Parkinson s Diseases Version 1 Final Page 1 Document control Version history Version Date Comments 1e (draft) 30 March 2007 Comments from customer incorporated 1d (draft) 22 January 2007 Formatting 1c
Parkinson s Diseases Version 1 Final Page 1 Document control Version history Version Date Comments 1e (draft) 30 March 2007 Comments from customer incorporated 1d (draft) 22 January 2007 Formatting 1c
Cardinal Features of Parkinson s. Management of Parkinson s Disease. Drug Induced Parkinson s. Other Parkinson s Symptoms.
 Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Motor Fluctuations in Parkinson s Disease
 Motor Fluctuations in Parkinson s Disease Saeed Bohlega, MD, FRCPC Senior Distinguished Consultant Department of Neurosciences King Faisal Specialist Hospital & Research Centre Outline Type of fluctuations
Motor Fluctuations in Parkinson s Disease Saeed Bohlega, MD, FRCPC Senior Distinguished Consultant Department of Neurosciences King Faisal Specialist Hospital & Research Centre Outline Type of fluctuations
Update on Parkinson s disease and other Movement Disorders October 2018
 Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Making Every Little Bit Count: Parkinson s Disease. SHP Neurobiology of Development and Disease
 Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
U n i f i e d P a r k i n s o n s D i s e a s e R a t i n g S c a l e ( U P D R S )
") Patient last name:................................. Date of birth:.... /.... /........ Patient first name:................................. Date:.... /.... /........ U n i f i e d P a r k i n s o n s D
Patient last name:................................. Date of birth:.... /.... /........ Patient first name:................................. Date:.... /.... /........ U n i f i e d P a r k i n s o n s D
Objectives. Emerging Treatments in Parkinson s s Disease. Pathology. As Parkinson s progresses it eventually affects large portions of the brain.
 Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
With Time, The Pathology of PD Spreads Throughout the Brain
 With Time, The Pathology of PD Spreads Throughout the Brain Braak s staging of Parkinson s disease pathology dm co sn mc hc fc 1 Hubert H. Fernandez, MD, FAAN Professor of Medicine (Neurology) Cleveland
With Time, The Pathology of PD Spreads Throughout the Brain Braak s staging of Parkinson s disease pathology dm co sn mc hc fc 1 Hubert H. Fernandez, MD, FAAN Professor of Medicine (Neurology) Cleveland
Chapter 20. Media Directory. Amyotrophic Lateral Sclerosis. Alzheimer s Disease. Huntington s Chorea. Multiple Sclerosis
 Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Rasagiline and Rapid Symptomatic Motor Effect in Parkinson s Disease: Review of Literature
 Neurol Ther (2014) 3:41 66 DOI 10.1007/s40120-013-0014-1 REVIEW Rasagiline and Rapid Symptomatic Motor Effect in Parkinson s Disease: Review of Literature Michele Pistacchi Francesco Martinello Manuela
Neurol Ther (2014) 3:41 66 DOI 10.1007/s40120-013-0014-1 REVIEW Rasagiline and Rapid Symptomatic Motor Effect in Parkinson s Disease: Review of Literature Michele Pistacchi Francesco Martinello Manuela
Parkinson s Disease and other related movement disorders a video guide to diagnosis
 Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Joint Session with ACOFP and Mayo Clinic. Parkinson's Disease: 5 Pearls. Jay Van Gerpen, MD
 Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
Drugs used in Parkinsonism
 Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
CE on SUNDAY Newark, NJ October 18, 2009
 CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 10:30 AM 11:45 AM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Treating Parkinson s Disease: A Pharmacist s Overview
CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 10:30 AM 11:45 AM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Treating Parkinson s Disease: A Pharmacist s Overview
05-Nov-15. Impact of Parkinson s Disease in Australia. The Nature of Parkinson s disease 21st Century
 Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
The Shaking Palsy of 1817
 The Shaking Palsy of 1817 A Treatment Update on Parkinson s Disease Dr Eitzaz Sadiq Neurologist CH Baragwanath Acadamic Hospital Parkinson s Disease O Premature death of dopaminergic neurons O Symptoms
The Shaking Palsy of 1817 A Treatment Update on Parkinson s Disease Dr Eitzaz Sadiq Neurologist CH Baragwanath Acadamic Hospital Parkinson s Disease O Premature death of dopaminergic neurons O Symptoms
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
XADAGO (safinamide) oral tablet
 oral tablet") XADAGO (safinamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
XADAGO (safinamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Learning Objectives. Parkinson s Disease: Choices and Challenges. Parkinson Disease: More Than Meets the Eye. Hallmark Symptoms in PD
 Parkinson s Disease: Choices and Challenges Susan C. Imke FNP, GNP-C Fort Worth, Texas Learning Objectives List four hallmark features of Idiopathic Parkinson Disease, and identify distinguishing features
Parkinson s Disease: Choices and Challenges Susan C. Imke FNP, GNP-C Fort Worth, Texas Learning Objectives List four hallmark features of Idiopathic Parkinson Disease, and identify distinguishing features
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Basal ganglia motor circuit
 Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
Movement Disorders- Parkinson s Disease. Fahed Saada, MD March 8 th, th Family Medicine Refresher Course St.
 Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Parkinson s Disease: the ABC s of PD Drug Therapy
 Parkinson s Disease: the ABC s of PD Drug Therapy Kimberly Mulcahy, PharmD, BCPS Clinical Pharmacist Buffalo Psychiatric Center NYSOMH Adjunct Faculty University at Buffalo SoPPS Disclosure No financial
Parkinson s Disease: the ABC s of PD Drug Therapy Kimberly Mulcahy, PharmD, BCPS Clinical Pharmacist Buffalo Psychiatric Center NYSOMH Adjunct Faculty University at Buffalo SoPPS Disclosure No financial
An Approach to Patients with Movement Disorders
 An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016
 Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016") Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016 What is Parkinson s? Parkinson's is a progressive neurological condition. People
Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016 What is Parkinson s? Parkinson's is a progressive neurological condition. People
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N.
 PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
Is Safinamide Effective as an Add-on Medication in Treating Parkinson's Disease Motor Symptoms?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2016 Is Safinamide Effective as an Add-on
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2016 Is Safinamide Effective as an Add-on
Parkinson s Pharmacology
 PHPP 517 (IT-III) Fall 2011 JACOBS Wed 10/12 8:00 8:50 AM 1 Learning objectives 1. Describe the direct and indirect pathways of the extrapyramidal system and its modulation by ACh and DA. 2. Contrast the
PHPP 517 (IT-III) Fall 2011 JACOBS Wed 10/12 8:00 8:50 AM 1 Learning objectives 1. Describe the direct and indirect pathways of the extrapyramidal system and its modulation by ACh and DA. 2. Contrast the
Date of Referral: Enhanced Primary Care Pathway: Parkinson s Disease
 Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification