2016 Top Papers in Critical Care
|
|
|
- Sybil Newman
- 5 years ago
- Views:
Transcription
1 2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience Critical Care Nurse Practitioner
2 Objectives Examine four studies that have been published in a highly reputable, peer reviewed journal within the last months Identify and discuss the background, objective, methods, results, and limitations of each study Confirm current practice or encourage an evidence based change to current practice

3
4 Background Brain injury is the primary cause of death in patients treated in an ICU after out-of-hospital cardiac arrest Severe neurologic impairment in long-term survivors is rare, with most having little to no disability

5 Objective To compare the effects of two target temperature regimens on long term cognitive function and quality of life after cardiac arrest
6 Trial design Methods Parallel group of randomized clinical trials performed in 36 ICUs in Europe and Australia Patients Inclusion Criteria Adult GCS 8 Out- of hospital CA with ROSC Exclusion Criteria 240 minutes ROSC Unwitnessed CA with asystole Suspected/known CVA Temp < 30 o C

7 Methods Randomization and Masking Eligible patients were randomly assigned 1:1 to TTM at either 33 o C or 36 o C Clinicians were not masked to the interventions, but were instructed not to discuss allocation temperature with the patients relatives
8 Methods Clinical Outcome Assessment 6 months after CA patients and their families were asked to participate in a follow up assessment via phone or in-person Outcomes were assessed from 4 perspectives: clinician-reported measures performance measures observer-reported measures patient reported measures
9 Methods Clinician reported measures Performancemeasures Observer-reported measures Patient-reported measures Cerebral Performance Categories (CPC) scale Modified Rankin Scale (mrs) Mini-Mental State Examination (MMSE) MMSE Adult Lifestyles and Function Interview (ALFI) for phone interviews Informant Questionnaire of Cognitive Decline in the Elderly (IQCODE) Two-Simple Questions Medical Outcomes Study Short Form Health Survey (SF-36v2) *MMSE and the IQCODE have not been validated in this specific population
10 Results Patients were enrolled from November 2011 January 2013 Total sample size of 939 patients 473 assigned to 33 o C and 466 assigned to 36 o C At follow up 245 were alive in the 33 o C group and 246 in the 36 o C group Median time from CA to follow up was 186 days

11

12
13 Limitations More patients in the 33 o C group have <12 years of education The optimum timing of patient assessment post CA remains to be determined Risk of bias if informants noted allocated temperature at the bedside during the intervention
14 Conclusion Both quality of life and cognitive function was similar in patients with cardiac arrest receiving targeted temperature management at 33 o C or 36 o C

15
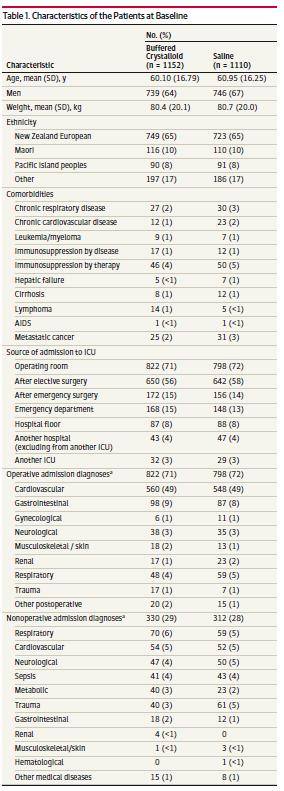
16 Background The administration of IV fluids to increase intravascular volume or maintain hydration is a common intervention in the ICU 0.9% saline (NS) is the most commonly used resuscitation fluid Does the high chloride content of saline contribute to the development of AKI?
17 Objective To determine the effect of a buffered crystalloid compared with saline on renal complications in patients admitted to the ICU
18 Study Design prospective investigator initiated multicenter blinded cluster-randomized double crossover Methods Conducted in 4 tertiary ICUs in New Zealand A predefined statistical analysis plan was reported and published prior to recruitment
19 Patients Methods All patients receiving crystalloid fluid therapy as clinically indicated were eligible Exclusions: patients on RRT or expected to require RRT within 6 hours, donor patients, palliative care patients, and patients previously enrolled in the study

20 Methods Study Randomization and Treatment ICUs were assigned to use blinded study fluids for alternating treatment blocks of 7 weeks Investigators and clinicians were blind to the study fluid allocation for the duration of the study The treating clinician determined the rate and frequency of fluid administration. FLUID A FLUID B
21 Primary outcome the proportion of patients with AKI, defined as a degree of renal dysfunction or injury or greater based on creatinine Methods Secondary outcomes Difference in creatinine pre/post ICU Use of RRT in the ICU and the requirements for RRT after discharge The proportion of patients requiring mechanical ventilation The proportion of patients requiring ICU readmission during their hospital stay ICU and hospital LOS ICU and hospital mortality


22
23 Results 9.6% vs 9.2 % of patients developed AKI within 90 days No significant difference in: the probability of requiring RRT service utilization use or duration of mechanical ventilation rates of death in the ICU or hospital cause specific mortality at 90 days
24 Limitations No sample size calculations > 90% of patients were exposed to IV fluids before enrollment Heterogeneous population of patients who were critically ill with low overall mortality
25 Conclusion This study found that there was no significant difference in rate of AKI in critically ill patients who received normal saline vs. plasmalyte
26
27 Background Limited data available on the target blood pressure range when treating acute hypertensive response in patients with ICH INTERACT2 trial found no significant difference in death or disability among patients in the intensive BP reduction arm vs. the guideline recommended treatment arm

28 Objective To determine the efficacy of rapidly lowering the SBP level in patients in an earlier time window after symptom onset than that evaluated in previous trials
29 Trial Design randomized multicenter open-label trial Methods evaluating the efficacy of intensive versus standard antihypertensive treatment that was initiated within 4.5 hours after symptom onset and continued for the next 24 hours at least one SBP reading of 180mm Hg between symptom onset and treatment was required
30 Methods Treatment for SBP 180 could be initiated before randomization to lower than 180mm Hg as per guidelines, patients were not eligible if SBP 140 mmhg prior to randomization Trial initially recruited patients within 3 hours of symptom onset, but window was extended to 4.5 hours based on new data
31 Methods Inclusion Criteria 18 years of age or older GCS score 5 Initial CTH with IPH < 60 cm 3 Treatment initiated within 4.5 hours of symptom onset Randomization performed centrally through the trial website using a minimization algorithm combined with the biased-coin method Trial Oversight an independent oversight committee evaluated adherence to protocols
32 Trial Interventions Methods Goal of treatment was to reduce and maintain the hourly minimum SBP in the mmhg range in the standard group and in the mmHg range in the intensive treatment group throughout the 24h time period after randomization Nicardipine was the first line antihypertensive agent Labetalol * was used as second agent

33 Trial Interventions Methods Primary treatment failure: not reaching the target SBP within 2 hours of randomization Secondary treatment failure: the hourly minimum SBP remaining higher than the upper limit of the target range for 2 consecutive hours during the initial 24h period
34 Trial Assessments Methods A non-contrast CTH was obtained 24 hours after the initiation of treatment, and both the baseline and 24h scan were forwarded The reader determined the site of hemorrhage, the presence/absence of blood, and the volume of the hematoma
35 Trial Assessments Methods Follow up via telephone interview at 1 month Follow up in clinic at 3 months Outcome Measures Primary outcome: proportion of patients who had moderately severe - severe disability or died at 3 months Secondary outcomes: scores on the EQ-5D utility index and VAS at 3 months, and the proportion of participants with 33% or greater volume expansion of their hematoma
36 Statistical Analysis Methods Primary hypothesis: Intensive treatment would be associated with a likelihood of death and disability at 3 months after ICH that was at least 10 percentage points lower than the likelihood associated with standard treatment Required sample size of 1042 patients Enrollment was stopped because of futility after the pre-specified second interim analysis
37 Results Enrollment period: May 2011 September sites in the U.S., Japan, China, Taiwan, South Korea, and Germany 1000 patients were randomized

38
39 Results Primary treatment failure occurred in 12.2 % of in the intensive treatment group and 0.8% in the standard group Secondary treatment failure occurred in 15.6% of the intensive treatment group and 1.4 % in the standard group Death or disability was observed in 38.7% in the intensive group and 37.7% in the standard group
40 Results No significant difference noted between the 2 groups: Modified Rankin score at 3 months EQ-5D measure Percentage of patient with hematoma expansion Rate of death at 3 months Neurological deterioration at 24 hours
41 Limitations Trial incorporated the pre-randomization use of IV antihypertensive medications A high percentage of patients with favorable characteristics may have conferred a predisposition to a favorable outcome in the trial s sample regardless of treatment
42 Conclusion Results suggest that aggressive reduction of SBP to mmhg does not provide any clinical benefit

43
44 Background Chest compressions are frequently interrupted by ventilations during out-of-hospital CA One strategy to reduce the interruption of compressions is to provide asynchronous PPV Observational studies have suggested that continuous compressions are associated with higher survival rates
45 Objective Compare whether continuous chest compressions vs. chest compressions interrupted for ventilation during CPR affected the rate of survival, neurological function, or rate of adverse events
46 Study design Methods Included 8 ROC site and 114 EMS agencies Informed consent was waived given the study involved research in emergency medicine Patient population Inclusion criteria Adults with non-trauma related out-ofhospital CA Exclusion criteria EMS witnessed arrest Advance directive with DNR Traumatic injury Asphyxial cause of arrest Exsanguination Known pregnancy Preexisting trach Known prisoners Had CPR performed by non ROC EMS providers or a mechanical device
47 Methods Study interventions 114 participating EMS agencies were grouped into 47 clusters Twice a year each cluster was crossed over Control group: 30 compressions:2 ventilations Intervention group: 100 compressions: 10 ventilations Outcomes Primary outcome: rate of survival to hospital discharge

48

49
50 Limitations Mean difference in the chest compression fraction was small There was an imbalance in the number of patients assigned to each group The quality of post resuscitation care is associated with outcomes, but was not mandated in the study Oxygenation or minutes of ventilation delivered were not measured
51 Conclusion Continuous chest compressions with PPV did not result in significantly higher rates of survival or favorable neurologic status than the rates with interrupted chest compressions
52 References Anderson C, et al. Rapid blood pressure lowering in patients with acute intracerebral hemorrhage. NEJM. 2013;368(25): Cronberg T, et al. Neurologic function and health-related quality of life in patients following targeted temperature management at 33 o C vs 36 o C after out-of-hospital cardiac arrest. JAMA Neurol. 2015;133(6): Nichol G, et al. Trial of continuous or interrupted chest compressions during CPR. NEJM. 2015; 373(23): Qureshi A, et al. Intensive blood pressure lowering in patient with acute cerebral hemorrhage. NEJM. June 2016; doi: /nejmoa Young P, et al. Effect of a buffered crystalloid solution vs saline on acute kidney injury among patients in the intensive care unit. JAMA. 2015;314(16):

53 Questions
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital
 Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Science Behind Resuscitation. Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013
 Science Behind Resuscitation Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013 Conflict of Interest No Financial or Industrial Conflicts Slides: Drs. Nelson, Cole and Larabee
Science Behind Resuscitation Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013 Conflict of Interest No Financial or Industrial Conflicts Slides: Drs. Nelson, Cole and Larabee
Lesson learnt from big trials. Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ.
 Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Resuscitation Science : Advancing Care for the Sickest Patients
 Resuscitation Science : Advancing Care for the Sickest Patients William Hallinan University of Rochester What is resuscitation science? Simply the science of resuscitation : Pre arrest Arrest care Medical
Resuscitation Science : Advancing Care for the Sickest Patients William Hallinan University of Rochester What is resuscitation science? Simply the science of resuscitation : Pre arrest Arrest care Medical
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Most Important EMS Articles EAGLES 2017
 Most Important EMS Articles EAGLES 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Overview Best antiarrhythmic
Most Important EMS Articles EAGLES 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Overview Best antiarrhythmic
Updates in Critical Care Sepsis, Fluids, Epi and Long-Term Outcomes
 Updates in Critical Care Sepsis, Fluids, Epi and Long-Term Outcomes Matt Anderson, MD USD SSOM, Clinical Assistant Professor Regional Health, Critical Care Medicine mjanderson972@gmail.com Disclosure(s)
Updates in Critical Care Sepsis, Fluids, Epi and Long-Term Outcomes Matt Anderson, MD USD SSOM, Clinical Assistant Professor Regional Health, Critical Care Medicine mjanderson972@gmail.com Disclosure(s)
Most Important EMS Articles EAGLES 2017
 Most Important EMS Articles EAGLES 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Overview Best antiarrhythmic
Most Important EMS Articles EAGLES 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Overview Best antiarrhythmic
Hypothermia After Cardiac Arrest: Where Are We Now?
 Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Follow-up GISELA LILJA
 Follow-up GISELA LILJA Outcome in the TTM 2 trial Primary outcome Survival Secondary outcome Overall social functioning Patient-reported health (quality of life) Tertiary outcome Detailed information on
Follow-up GISELA LILJA Outcome in the TTM 2 trial Primary outcome Survival Secondary outcome Overall social functioning Patient-reported health (quality of life) Tertiary outcome Detailed information on
Klinikum Frankfurt Höchst
 Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
5 Key EMS Articles for 2012
 5 Key EMS Articles for 2012 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN 5 Key Topics Cardiac Arrest Trauma
5 Key EMS Articles for 2012 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN 5 Key Topics Cardiac Arrest Trauma
Cardiac Arrest January 2017 CPR /3/ Day to Survival Propensity Matched
 Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
ECLS: A new frontier for refractory V.Fib and pulseless VT
 ECLS: A new frontier for refractory V.Fib and pulseless VT Ernest L. Mazzaferri, Jr. MD, FACC September 15, 2017 Cardiovascular Emergencies: An exploration into the expansion of time-critical diagnosis
ECLS: A new frontier for refractory V.Fib and pulseless VT Ernest L. Mazzaferri, Jr. MD, FACC September 15, 2017 Cardiovascular Emergencies: An exploration into the expansion of time-critical diagnosis
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Kiehl EL, 1,2 Parker AM, 1 Matar RM, 2 Gottbrecht M, 1 Johansen MC, 1 Adams MP, 1 Griffiths LA, 2 Bidwell KL, 1 Menon V, 2 Enfield KB, 1 Gimple LW 1
 C-GRApH: A Validated Scoring System For The Early Risk Stratification Of Neurologic Outcomes After Out-of-hospital Cardiac Arrest Treated With Therapeutic Hypothermia Kiehl EL, 1,2 Parker AM, 1 Matar RM,
C-GRApH: A Validated Scoring System For The Early Risk Stratification Of Neurologic Outcomes After Out-of-hospital Cardiac Arrest Treated With Therapeutic Hypothermia Kiehl EL, 1,2 Parker AM, 1 Matar RM,
ROC PRIMED Questions and Answers
 ROC PRIMED Questions and Answers 1) What is the ROC PRIMED study? ROC PRIMED stands for the Resuscitation Outcomes Consortium Prehospital Resuscitation using an IMpedance valve and Early versus Delayed
ROC PRIMED Questions and Answers 1) What is the ROC PRIMED study? ROC PRIMED stands for the Resuscitation Outcomes Consortium Prehospital Resuscitation using an IMpedance valve and Early versus Delayed
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD
 Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD") FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
in Cardiac Arrest Management Sean Kivlehan, MD, MPH May 2014
 in Cardiac Arrest Management Sean Kivlehan, MD, MPH May 2014 1. Capnography 2. Compressions 3. CPR Devices 4. Hypothermia 5. Access 6. Medications Outline Capnography & Termination Significantly Associated
in Cardiac Arrest Management Sean Kivlehan, MD, MPH May 2014 1. Capnography 2. Compressions 3. CPR Devices 4. Hypothermia 5. Access 6. Medications Outline Capnography & Termination Significantly Associated
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Epinephrine Cardiovascular Emergencies Symposium 2018
 Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Science Behind CPR Update from Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 Science Behind CPR Update from 2010 Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences FRAMING THE DISCUSSION NO ONE SURVIVES CARDIAC ARREST, EXCEPT ON TV Conflicts of
Science Behind CPR Update from 2010 Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences FRAMING THE DISCUSSION NO ONE SURVIVES CARDIAC ARREST, EXCEPT ON TV Conflicts of
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Refractory cardiac arrest
 Refractory cardiac arrest Claudio Sandroni Dept. of Anaesthesiology and Intensive Care Catholic University School of Medicine Rome Italy IRC Scientific Committee Conflicts of interest None Cardiac arrest:
Refractory cardiac arrest Claudio Sandroni Dept. of Anaesthesiology and Intensive Care Catholic University School of Medicine Rome Italy IRC Scientific Committee Conflicts of interest None Cardiac arrest:
2015 AHA Guidelines: Pediatric Updates
 2015 AHA Guidelines: Pediatric Updates Advances in Pediatric Emergency Medicine December 9, 2016 Karen O Connell, MD, MEd Associate Professor of Pediatrics and Emergency Medicine Emergency Medicine and
2015 AHA Guidelines: Pediatric Updates Advances in Pediatric Emergency Medicine December 9, 2016 Karen O Connell, MD, MEd Associate Professor of Pediatrics and Emergency Medicine Emergency Medicine and
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
2015 Interim Training Materials
 2015 Interim Training Materials ACLS Manual and ACLS EP Manual Comparison Chart Assessment sequence Manual, Part 2: The Systematic Approach, and Part BLS Changes The HCP should check for response while
2015 Interim Training Materials ACLS Manual and ACLS EP Manual Comparison Chart Assessment sequence Manual, Part 2: The Systematic Approach, and Part BLS Changes The HCP should check for response while
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Enhancing 5 th Chain TTM after Cardiac Arrest
 Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Emergency Cardiac Care Guidelines 2015
 Emergency Cardiac Care Guidelines 2015 VACEP 2016 William Brady, MD University of Virginia Guidelines 2015 Basic Life Support & Advanced Cardiac Life Support Acute Coronary Syndrome Pediatric Advanced
Emergency Cardiac Care Guidelines 2015 VACEP 2016 William Brady, MD University of Virginia Guidelines 2015 Basic Life Support & Advanced Cardiac Life Support Acute Coronary Syndrome Pediatric Advanced
GETTING TO THE HEART OF THE MATTER. Ritu Sahni, MD, MPH Lake Oswego Fire Department Washington County EMS Clackamas County EMS
 GETTING TO THE HEART OF THE MATTER Ritu Sahni, MD, MPH Lake Oswego Fire Department Washington County EMS Clackamas County EMS TAKE HOME POINTS CPR is the most important thing Train like we fight Measure
GETTING TO THE HEART OF THE MATTER Ritu Sahni, MD, MPH Lake Oswego Fire Department Washington County EMS Clackamas County EMS TAKE HOME POINTS CPR is the most important thing Train like we fight Measure
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Top Papers in Critical Care Janna Landsperger, ACNP-BC
 Top Papers in Critical Care 2014 Janna Landsperger, ACNP-BC Objectives Review journal articles regarding delivery of critical care published over the past twelve months Provide evidence in support of current
Top Papers in Critical Care 2014 Janna Landsperger, ACNP-BC Objectives Review journal articles regarding delivery of critical care published over the past twelve months Provide evidence in support of current
Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity
 Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity Hannah Jordan A. Study Purpose and Rationale Pulseless electrical activity during cardiac arrest carries a
Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity Hannah Jordan A. Study Purpose and Rationale Pulseless electrical activity during cardiac arrest carries a
New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto
 New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto COI Declaration Industry and ROC ALS Taskforce ILCOR Author
New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto COI Declaration Industry and ROC ALS Taskforce ILCOR Author
Developments in Cardiopulmonary Resuscitation Guidelines
 Developments in Cardiopulmonary Resuscitation Guidelines Bernd W. Böttiger Seite 1 To preserve human life by making high quality resuscitation available to all Outcome after CPR in Germany ROSC ( Return
Developments in Cardiopulmonary Resuscitation Guidelines Bernd W. Böttiger Seite 1 To preserve human life by making high quality resuscitation available to all Outcome after CPR in Germany ROSC ( Return
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Advanced Resuscitation - Adolescent
 C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
JUST SAY NO TO DRUGS?
 JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines
 Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Key statistics from the National Cardiac Arrest Audit: Paediatric arrests April 2012 to March 2017
 Key statistics from the National Cardiac Arrest Audit: Paediatric arrests April 12 to March 17 Supported by Resuscitation Council (UK) and Intensive Care National Audit & Research Centre (ICNARC) Data
Key statistics from the National Cardiac Arrest Audit: Paediatric arrests April 12 to March 17 Supported by Resuscitation Council (UK) and Intensive Care National Audit & Research Centre (ICNARC) Data
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
Introduction. Introduction. Introduction. Results. Method
 Standard cardiopulmonary resuscitation versus active compression-decompression cardiopulmonary resuscitation with augmentation of negative intrathoracic pressure for out-of-hospital cardiac arrest: a randomized
Standard cardiopulmonary resuscitation versus active compression-decompression cardiopulmonary resuscitation with augmentation of negative intrathoracic pressure for out-of-hospital cardiac arrest: a randomized
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Manual Defibrillation. CPR AGE: 18 years LOA: Altered HR: N/A RR: N/A SBP: N/A Other: N/A
 ROC AMIODARONE, LIDOCAINE OR PLACEBO FOR OUT OF HOSPITAL CARDIAC ARREST DUE TO VENTRICULAR FIBRILLATION OR TACHYCARDIA (ALPS) STUDY: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic
ROC AMIODARONE, LIDOCAINE OR PLACEBO FOR OUT OF HOSPITAL CARDIAC ARREST DUE TO VENTRICULAR FIBRILLATION OR TACHYCARDIA (ALPS) STUDY: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic
Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti
 Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti U.O.C Anestesia e Terapia Intensiva Policlinico San Martino - GENOVA Natural Course of Neurological Recovery Following Cardiac Arrest Cardiac
Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti U.O.C Anestesia e Terapia Intensiva Policlinico San Martino - GENOVA Natural Course of Neurological Recovery Following Cardiac Arrest Cardiac
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage
 Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage John J. Lewin III, PharmD, MBA, BCCCP, FASHP, FCCM, FNCS Division Director, Critical Care & Surgery Pharmacy Services, The Johns
Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage John J. Lewin III, PharmD, MBA, BCCCP, FASHP, FCCM, FNCS Division Director, Critical Care & Surgery Pharmacy Services, The Johns
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Supplementary Online Content
 Supplementary Online Content Hasegawa K, Hiraide A, Chang Y, Brown DFM. Association of prehospital advancied airway management with neurologic outcome and survival in patients with out-of-hospital cardiac
Supplementary Online Content Hasegawa K, Hiraide A, Chang Y, Brown DFM. Association of prehospital advancied airway management with neurologic outcome and survival in patients with out-of-hospital cardiac
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Objectives. Trends in Resuscitation POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE?
 POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
Management of Post Cardiac Arrest Syndrome
 Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
A protocol for the 0.9% saline versus Plasma-Lyte 148 for intensive care fluid therapy (SPLIT) study
 study") A protocol for the 0.9% saline versus Plasma-Lyte 148 for intensive care fluid therapy (SPLIT) study Sumeet K Reddy, Michael J Bailey, Richard W Beasley, Rinaldo Bellomo, Seton J Henderson, Diane M Mackle,
A protocol for the 0.9% saline versus Plasma-Lyte 148 for intensive care fluid therapy (SPLIT) study Sumeet K Reddy, Michael J Bailey, Richard W Beasley, Rinaldo Bellomo, Seton J Henderson, Diane M Mackle,
Top Sepsis Studies
 A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Critical Review Form Therapy Objectives: Methods:
 Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
There Is Something More We Can Do: An Introduction to Hospice and Palliative Care
 There Is Something More We Can Do: An Introduction to Hospice and Palliative Care presented to the Washington Patient Safety Coalition July 28, 2010 Hope Wechkin, MD Medical Director Evergreen Hospice
There Is Something More We Can Do: An Introduction to Hospice and Palliative Care presented to the Washington Patient Safety Coalition July 28, 2010 Hope Wechkin, MD Medical Director Evergreen Hospice
Out-of-hospital Cardiac Arrest. Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland
 Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Supplementary Online Content
 Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Improving Outcome from In-Hospital Cardiac Arrest
 Improving Outcome from In-Hospital Cardiac Arrest National Teaching Institute San Diego, CA Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Independent CNS/Staff Nurse Objectives 1. Discuss the AHA in-hospital
Improving Outcome from In-Hospital Cardiac Arrest National Teaching Institute San Diego, CA Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Independent CNS/Staff Nurse Objectives 1. Discuss the AHA in-hospital
Top 10 Articles in 2016 in Emergency Medicine N.JERBI, W.KERKENI, C. BOUHAMED, R.BOUKEF, S.NOUIRA,
 Top 10 Articles in 2016 in Emergency Medicine N.JERBI, W.KERKENI, C. BOUHAMED, R.BOUKEF, S.NOUIRA, Manual Cardiopulmonary Resuscitation Versus CPR Including a Mechanical Chest Compression Device in Out-of-Hospital
Top 10 Articles in 2016 in Emergency Medicine N.JERBI, W.KERKENI, C. BOUHAMED, R.BOUKEF, S.NOUIRA, Manual Cardiopulmonary Resuscitation Versus CPR Including a Mechanical Chest Compression Device in Out-of-Hospital
Prof Gavin Perkins Co-Chair ILCOR
 Epidemiology of out of hospital cardiac arrest how to improve survival Prof Gavin Perkins Co-Chair ILCOR Chair, Community Resuscitation Committee, Resuscitation Council (UK) Conflict of interest Commercial
Epidemiology of out of hospital cardiac arrest how to improve survival Prof Gavin Perkins Co-Chair ILCOR Chair, Community Resuscitation Committee, Resuscitation Council (UK) Conflict of interest Commercial
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Blood Pressure Management in Acute Stroke. Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh
 Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Pediatric CPR. Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY
 Pediatric CPR Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY What are the differences? Normal limits ADULT CARDIOPULMONARY ARREST CAUSES INFANTS AND CHILDREN İschemic
Pediatric CPR Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY What are the differences? Normal limits ADULT CARDIOPULMONARY ARREST CAUSES INFANTS AND CHILDREN İschemic
Donation After Cardiac Death
 Donation After Cardiac Death Barriers to increasing organ donations after cardiac death Key lessons learned from previous and ongoing efforts/next steps Uncontrolled Category II DCD Kenneth E. Wood, DO
Donation After Cardiac Death Barriers to increasing organ donations after cardiac death Key lessons learned from previous and ongoing efforts/next steps Uncontrolled Category II DCD Kenneth E. Wood, DO
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Strategies for Enhancing Sepsis Survivorship
 Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
Advanced airway placement (ETT vs SGA)
") Advanced airway placement (ETT vs SGA) Among adults who are in cardiac arrest in any setting (P), does tracheal tube insertion as first advanced airway (I), compared with insertion of a supraglottic airway
Advanced airway placement (ETT vs SGA) Among adults who are in cardiac arrest in any setting (P), does tracheal tube insertion as first advanced airway (I), compared with insertion of a supraglottic airway
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
Cardiac Arrest Registry Database Office of the Medical Director
 Cardiac Arrest Registry Database 2010 Office of the Medical Director 1 Monthly Statistical Summary Cardiac Arrest, September 2010 Western Western Description Division Division % Totals Eastern Division
Cardiac Arrest Registry Database 2010 Office of the Medical Director 1 Monthly Statistical Summary Cardiac Arrest, September 2010 Western Western Description Division Division % Totals Eastern Division
Post-Resuscitation Care. Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena
 Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Cardiac Arrest Registry Database Office of the Medical Director
 Cardiac Arrest Registry Database 2010 Office of the Medical Director 1 Monthly Statistical Summary Cardiac Arrest, December 2010 Western Western Description Division Division % Totals Eastern Division
Cardiac Arrest Registry Database 2010 Office of the Medical Director 1 Monthly Statistical Summary Cardiac Arrest, December 2010 Western Western Description Division Division % Totals Eastern Division
18% Survival from In-Hospital Cardiac Arrest Ways we can do better! National Teaching Institute Denver, CO Class Code: 149 A
 18% Survival from In-Hospital Cardiac Arrest Ways we can do better! National Teaching Institute Denver, CO Class Code: 149 A Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Independent CNS/Staff Nurse Objectives
18% Survival from In-Hospital Cardiac Arrest Ways we can do better! National Teaching Institute Denver, CO Class Code: 149 A Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Independent CNS/Staff Nurse Objectives
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Victorian Ambulance Cardiac Arrest Registry (VACAR)
") Victorian Ambulance Cardiac Arrest Registry (VACAR) Dr Karen Smith (PhD) VACAR Chair Manager Research and Evaluation Ambulance Victoria Smith K, Bray J, Barnes V, Lodder M, Cameron P, Bernard S and Currell
Victorian Ambulance Cardiac Arrest Registry (VACAR) Dr Karen Smith (PhD) VACAR Chair Manager Research and Evaluation Ambulance Victoria Smith K, Bray J, Barnes V, Lodder M, Cameron P, Bernard S and Currell
When to think about palliation
 When to think about palliation Hannah Wunsch, MD MSc Department of Critical Care Medicine, Sunnybrook Health Sciences Centre Associate Professor of Anesthesiology, University of Toronto Visiting Assistant
When to think about palliation Hannah Wunsch, MD MSc Department of Critical Care Medicine, Sunnybrook Health Sciences Centre Associate Professor of Anesthesiology, University of Toronto Visiting Assistant
Department of Surgery, Division of Cardiothoracic Surgery
 Review of In-Hospital and Out-of-Hospital Cardiac Arrests at a Tertiary Community Hospital for Potential ECPR Rescue Amanda Broderick 1, Jordan Williams 1, Alexandra Maryashina 1, & James Wu, MD 1 1 Department
Review of In-Hospital and Out-of-Hospital Cardiac Arrests at a Tertiary Community Hospital for Potential ECPR Rescue Amanda Broderick 1, Jordan Williams 1, Alexandra Maryashina 1, & James Wu, MD 1 1 Department
What is the right fluid to use?
 What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Therapeutic hypothermia following cardiac arrest
 TITLE: Therapeutic hypothermia following cardiac arrest AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
TITLE: Therapeutic hypothermia following cardiac arrest AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
Contents. Version 1.0: 01/02/2010 Protocol# ISRCTN Page 1 of 7
 Contents 1. INTRODUCTION... 2 2. STUDY SYNOPSIS... 2 3. STUDY OBJECTIVES... 2 3.1. Primary Objective... 2 3.2. Secondary Objectives... 2 3.3. Assessment of Objectives... 3 3.4. Change the Primary Objective
Contents 1. INTRODUCTION... 2 2. STUDY SYNOPSIS... 2 3. STUDY OBJECTIVES... 2 3.1. Primary Objective... 2 3.2. Secondary Objectives... 2 3.3. Assessment of Objectives... 3 3.4. Change the Primary Objective
Hypothermia: The Science and Recommendations (In-hospital and Out)
") Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society