DELIRIUM. J. Sukanya 28.Jun.12
|
|
|
- Barnaby Ralf Gilbert
- 5 years ago
- Views:
Transcription

1 DELIRIUM J. Sukanya 28.Jun.12
2 Outline Why? What? How? What s next? Delirium
3 Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening, potentially preventable Acutely admitted elderly patients Nat. Rev. Neurol. 5, (2009) Vol 9 September 2010
4 Introduction Disadvantages of Delirium Increased risk of morbidity and mortality Increased health care costs New data link this syndrome to poor long-term outcome Nat. Rev. Neurol. 5, (2009) Vol 9 September 2010 Geriatr Gerontol Int.2012 Jun 7.
5 Why? Delirium
6 Epidemiology Delirium: hypoactive form More common Often unrecognized N Engl J Med 2006;354: Dtsch Arztebl Int.2012 May;109(21):
7 Epidemiology Vary depending on The patients characteristics Setting of care Sensitivity of the detection method Among general hospital populations The prevalence The incidence percent 6-56 percent N Engl J Med 2006;354: Nat. Rev. Neurol. 5, (2009)
8 Epidemiology The overall prevalence in the community 1-2 percent Up to 14 percent At the emergency departments - if more than 85 years old percent of older patients presenting with delirium Often heralds the presence of life-threatening conditions N Engl J Med 2006;354: Nat. Rev. Neurol. 5, (2009)
9 Epidemiology Postoperative In intensive care setting percent percent In nursing homes or post acute care settings Up to 60 percent At the end of life Up to 83 percent N Engl J Med 2006;354: Nat. Rev. Neurol. 5, (2009)
10 Epidemiology Incidence of post-stroke delirium and 1-year outcome N =314 Acute stroke unit 72.9 years Incidence 27.4% Higher functional impairment/nursing home placement/mortality Geriatr Gerontol Int.2012 Jun 7.
11 Epidemiology The mortality rates Range from percent As high as the rates with acute myocardial infarction or sepsis The one-year mortality rate percent N Engl J Med 2006;354: Geriatr Gerontol Int.2012 Jun 7.
12 Prevalence and incidence of delirium in Thai older patients: a study at general medical wards in Siriraj Hospital. Praditsuwan R, Limmathuroskul D, Assanasen J, Pakdeewongse S, Eiamjinnasuwat W, Sirisuwat A, Srinonprasert V. J Med Assoc Thai.2012 Feb;95 Suppl 2:S
13 OBJECTIVE To determine prevalence and incidence of delirium In older patients Admitted to general medical wards In a university hospital in Thailand J Med Assoc Thai.2012 Feb;95 Suppl 2:S
14 MATERIAL AND METHOD A prospective observational study Age 70 years or older In general medical wards during study period Delirium assessments Initially within the first 24 hours of admission And serially every 48 hours Until developed delirium or were discharged J Med Assoc Thai.2012 Feb;95 Suppl 2:S
15 MATERIAL AND METHOD Delirium was diagnosed by experienced geriatricians Based on the DSM-IV criteria Prevalence Based on delirium identified at the first assessment Incidence Based on cases developed during hospitalization J Med Assoc Thai.2012 Feb;95 Suppl 2:S
16 RESULTS N = 225 The prevalence of delirium 40.4% The incidence of delirium 8.4% The total occurrence rate of delirium 48.9% J Med Assoc Thai.2012 Feb;95 Suppl 2:S
17 RESULTS Occurrence rate of delirium significantly increased with Age (p = 0.003) Illness severity (p < 0.001) Number of impaired activities of daily living J Med Assoc Thai.2012 Feb;95 Suppl 2:S
")
18 Nat. Rev. Neurol. 5, (2009)
19 A review and meta-analysis of published studies Death 2 years Hazard ratio 1.95, Institutionalisation 15 months Odds ratio [OR] 2.41, Developing dementia 4 years OR 12.52, Vol 9 September 2010 JAMA. 2010; 304:
20 A review and meta-analysis of published studies Poor outcome independent of important confounders Age Sex Comorbid illness or illness severity Baseline dementia Vol 9 September 2010 JAMA. 2010; 304:
21 Incidence of post-stroke delirium and 1-year outcome Nursing home placement 62% vs 11.2% Mortality Inpatient mortality 18% vs 2.2% 1-year mortality 30% vs 7.4% Longer hospital stay 45 vs 22 days Geriatr Gerontol Int.2012 Jun 7.
22 Adverse Outcomes After Hospitalization and Delirium in Persons With Alzheimer Disease Death 1/16 Institutionalization 1/7 Cognitive decline 1/5 Any adverse outcome 1/8 Ann Intern Med. 2012;156:
23 What? Delirium
24 N Engl J Med 2006;354:
25 N Engl J Med 2006;354:
26 Clinical features Symptom profile of delirium In northern India Assessed 100 consecutive cases of DSM-IV delirium Mean age: 44.4 [standard deviation: 19.4] years Most frequent symptoms Attention, Orientation, Visuospatial ability, Sleep disturbance Less frequent Language, Thought-process abnormality, Motor agitation J Neuropsychiatry Clin Neurosci Dec 1;24(1):

27 Hazzard Geriatric Medicine and Gerontology 6thEd
28 N Engl J Med 2006;354:
29 N Engl J Med 2006;354:
30 Incidence of post-stroke delirium and 1-year outcome Independent risk factors of post-stroke delirium Chest infection OR = 22.0 Total anterior circulation infarct OR = 18.8 Presence of acute urinary retention OR = 7.67 posterior circulation infarct OR = 3.52 pre-existing cognitive impairment OR = 2.51 National Institutes of Health Stroke Scale OR 1.13 Age OR 1.05 Geriatr Gerontol Int.2012 Jun 7.
31 J Med Assoc Thai 2011; 94 (Suppl. 1): S99-S104 Risk Factors for Developing Delirium in Older Patients Admitted to General Medical Wards
32 Risk Factors for Developing Delirium in Older Patients Admitted to General Medical Wards A prospective observational study Risk factors Preexisting dementia (OR = 5.52, 95% CI = ), Severe illness (OR = 5.18, 95% CI = ) Presence of infection (OR = 2.54, 95% CI = ) Azothemia (OR = 2.55, 95% CI = ). J Med Assoc Thai 2011; 94 (Suppl. 1): S99-S104
33 Etiology- case report Cognitive decline in an old woman: Do not miss a rare etiology! Brussels, Belgium Report a case of a woman with neurological symptoms?dementia Final diagnosis Late-onset SLE Leads to misdiagnosis Exp Gerontol Jul;47(7):534-5.
 Critical Care 2011, 15:R78 J Am")
34 Nat. Rev. Neurol. 5, (2009) Critical Care 2011, 15:R78 J Am Geriatr Soc Apr;60(4):
35 Pathophysiology Plasma levels of procalcitonin and CRP Critically ill patients High baseline inflammatory biomarkers Predicted prolonged periods of acute brain dysfunction Critical Care 2011, 15:R78
36 Pathophysiology Plasma cholinesterase activity (acetylcholinesterase (AChE) and butyrylcholinesterase (BuChE)) Inflammatory mediators (C-reactive protein (CRP), interleukin (IL)-1 beta, tumor necrosis factor alpha, IL-6, IL-8, IL-10) Unbalanced inflammatory response Dysfunctional interaction Between the cholinergic and immune systems J Am Geriatr Soc Apr;60(4):
37 How? Delirium
38 Diagnostic Criteria: ICD-10 ICD-10 Diagnostic Criteria For a definite diagnosis, symptoms, mild or severe, should be present in each one of the following areas: A. Impairment of consciousness and attention B. Global disturbance of cognition C. Psychomotor disturbances D. Disturbance of the sleep - wake cycle E. Emotional disturbances The Supplementary Appendix of N Engl J Med 2006;354:
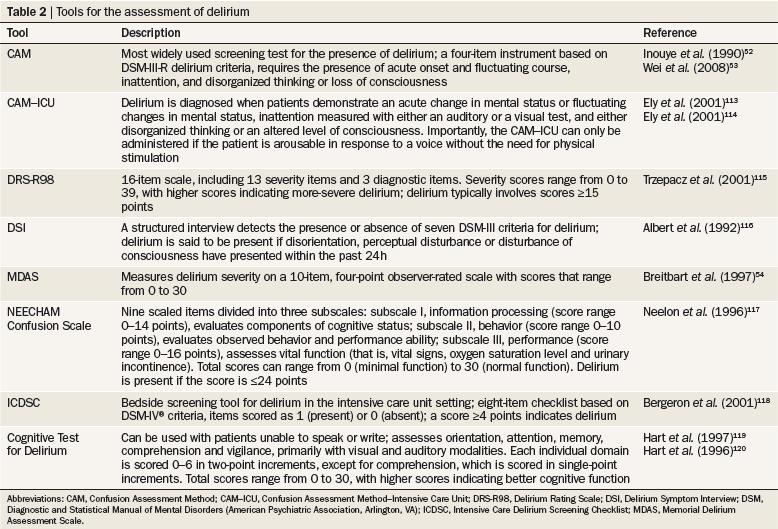
39 Diagnostic Criteria: CAM The Confusion Assessment Method (CAM) Diagnostic Algorithm Feature 1. Acute onset and fluctuating course Feature 2. Inattention Feature 3. Disorganized thinking Feature 4. Altered level of consciousness The diagnosis by CAM Requires the presence of features 1 and 2 and of either 3 or 4 The Supplementary Appendix of N Engl J Med 2006;354:
40 Diagnosing delirium in elderly Thai patients: Utilization of the CAM algorithm Sensitivity 91.9% Specificity 100.0% PPV 100.0% NPV 90.6% Wongpakaran et al. BMC Family Practice 2011,
")
41 Nat. Rev. Neurol. 5, (2009)


42 Confusion Assessment Method
43
44 CONFUSION ASSESSMENT METHOD IN THE ICU (CAM-ICU) TARGET POPULATION: Should be used on all older adults admitted to the ICU Promptly identify Any potential delirium and prevent negative outcomes
45
 www.")
46 (The Richmond Agitation-Sedation Scale)
47 Thai Delirium Rating Scale* Develop Thai Delirium Rating Scale Thai Delirium Rating Scale (TDRS) Good reliability and validity For discriminate delirium from other psychiatric patients Sensitivity: 97% Specificity: 91% TDRS is a reliable and valid instrument to diagnose delirium for medical personal and for delirium research J Psychiatr Assoc Thailand 2000; 45(4):
48 Dose the Scores of Thai Delirium Rating Scale Correlate with the Severity of Delirium? Study the correlation between total scores of TDRS VS the severity of delirium 5-item scores in Thai Delirium Rating Scale psychomotor activity, cognitive status during formal testing, sleep-wake cycle disturbance, lability of mood, and variability of symptoms The 5-item version of TDRS can be used to indicate the severity of delirium J Psychiatr Assoc Thailand 2000; 45(4):
49 Development of Thai Version of Delirium Rating Scale Develop and validate TDRS for nonpsychiatric physicians Thai version of Delirium Rating Scale appeared to be useful for detecting delirium by trained physicians with good levels of validity and reliability J Psychiatr Assoc Thailand 2000; 45(4):
50 Validity of thai delirium rating scale 6 items version The Thai Delirium Rating scale 6 items version A brief, feasible and valid instrument to diagnose delirium instead of the Thai Delirium Rating Scale 10 items version Siriraj Hospital Gazette, Vol. 53, No 9, September Page


51 Siriraj Hospital Gazette, Vol. 53, No 9, September Page
52 สถาบ นจ ตเวชศาสตร สมเด จเจ าพระยา

53 สถาบ นจ ตเวชศาสตร สมเด จเจ าพระยา
54 สถาบ นจ ตเวชศาสตร สมเด จเจ าพระยา
55 Assessment of risk factors for delirium First present to hospital or long term care Any risk factors? Keep observation Every opportunity For any changes in the risk factors for delirium BMJ 2010;341:c3704
56 Assessment of risk factors for delirium Risk factors Age 65 years or older Cognitive impairment (past or present), and/ or dementia If cognitive impairment is suspected, confirm it using a standardised and validated cognitive impairment measure (mini mental state examination ) Current hip fracture Severe illness BMJ 2010;341:c3704

57 Fong, T. G. et al. Nat. Rev. Neurol. 5, (2009)
58 What s next? Delirium
59 Prevention is the best! N Engl J Med 2006;354:
60 Prevention Non-pharmacologic approach Pharmacologic approach N Engl J Med 2006;354:
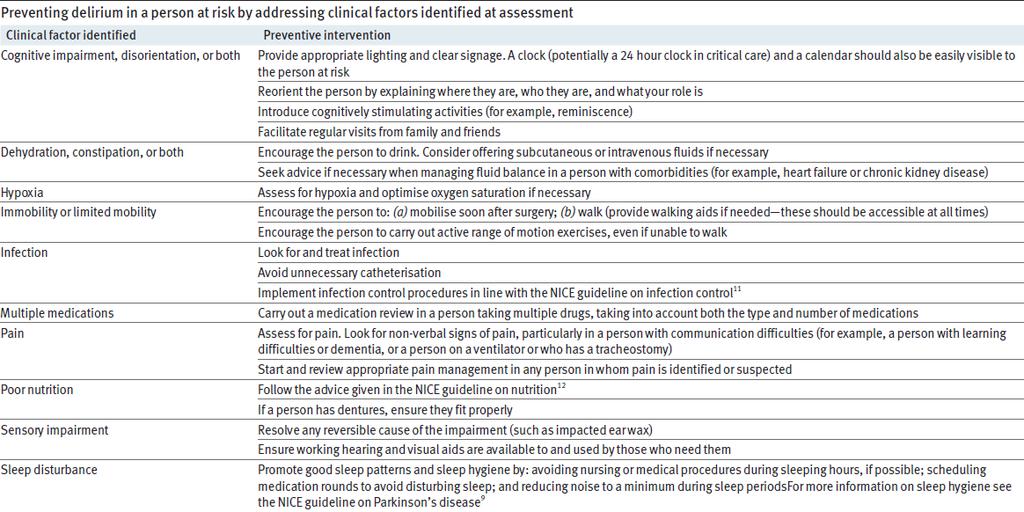
61 Interventions to prevent delirium Within 24 hours of admission, assess precipitating factors: Cognitive impairment, disorientation, or both Dehydration, constipation, or both Hypoxia Immobility or limited mobility BMJ 2010;341:c3704
62 Interventions to prevent delirium Within 24 hours of admission, assess precipitating factors: Infection Multiple medications Pain Poor nutrition Sensory impairment Sleep disturbance BMJ 2010;341:c3704
63 BMJ 2010;341:c3704
64 The Hospital Elder Life Program A model of care to prevent cognitive and functional decline in older hospitalized patients Screened on admission for six risk factors Cognitive impairment, sleep deprivation, immobility, dehydration, vision or hearing impairment Interdisciplinary team Other experts consultation twice-weekly J Am Geriatr Soc Dec;48(12):



65 Communication and Comfort Program Exercise Program Meal Program Recreation and Relaxation Program
66 Reducing delirium after hip fracture: a randomized trial Proactive geriatrics consultation One case of delirium was prevented for every 5.6 patients Reduced delirium by over one-third Reduced severe delirium by over one-half J Am Geriatr Soc May;49(5):
67 The REACH-OUT trial Homebased rehabilitation vs Inpatient hospital setting Frail older patients Lower incidence of delirium lower cost greater satisfaction Age Ageing Jan;35(1):53-60.
68 Pilot randomized trial of donepezil hydrochloride for delirium after hip fracture. N = 16, aged 70 and older with hip fracture Donepezil 5 mg or placebo Initiated within 24 hrs of surgery, pre/postoperatively Daily treatment was continued for 30 days or until side effects or the clinical situation required termination Donepezil had no significant improvement in delirium presence or severity but experienced more side effects J Am Geriatr Soc Nov;59 Suppl 2:S282-8.
69 Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: a randomized controlled trial Short-term low-dose intravenous haloperidol Prospective, randomized, double-blind, and placebocontrolled trial in two centers Crit Care Med Mar;40(3):731-9.
70 Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: a randomized controlled trial The primary end point Incidence of delirium within the first 7 days after surgery Secondary end points Time to onset of delirium Number of delirium-free days Length of intensive care unit stay Crit Care Med Mar;40(3):731-9.
71 Dexmedetomidine for postoperative sedation in elderly patients with cognitive impairment N = 10/ 70 to 90 years DEX microg /kg/ hr: 30 to 60 min before the end of the operation microg /kg/ hr: by the time of extubation, Increased 0.1 microg /kg/ hr: depend Masui Apr;61(4):
72 Dexmedetomidine for postoperative sedation in elderly patients with cognitive impairment 7/10 calm 3/10 the dose had to be increased by 0.1 microg x kg(-1) x hr(-1) No serious complication,except bradycardia (2/10) Low-dose DEX is safe and useful for postoperative sedation in elderly patients with cognitive impairment Masui Apr;61(4):
73 N Engl J Med 2006;354:
74 N Engl J Med 2006;354:
75 N Engl J Med 2006;354:
76 9 10 N Engl J Med 2006;354:
77 11 N Engl J Med 2006;354:
78 Management Indication of pharmacologic management Threaten their own safety Safety of other persons Interruption of essential therapy Mechanical ventilation or central venous catheters N Engl J Med 2006;354:
")
79 Nat. Rev. Neurol. 5, (2009)
80 Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial Higher mortality Longer median duration of delirium 3-time 5:3 days Lancet Nov 27;376(9755):
81 Summary Delirium
82 Why? Common Morbidity and mortality Poor quality of life What? Summary Identify risk group Interaction Between the cholinergic and immune systems ว รศ กด เม องไพศาล. อาการซ ม ส บสนเฉ ยบพล นในผ ส งอาย (Delirium in the Elderly) hppt:// /researchcenter/download/ /15.pdf
83 How? Summary CAM / CAM-ICU/TDRS Delirium/Dementia/Depression/Acute pshychosis What s next? Preventive measure Early diagnosis and early intervention ว รศ กด เม องไพศาล. อาการซ ม ส บสนเฉ ยบพล นในผ ส งอาย (Delirium in the Elderly) hppt:// /researchcenter/download/ /15.pdf

84
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
DELIRIUM. Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine
 DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
Why Target Delirium for Surgical Quality Improvement?
 Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Continence, falls and the frailty syndrome. Anne Foley - BGS Bladders and Bowel Health 2012
 Continence, falls and the frailty syndrome Outline Frailty Geriatric syndromes and giants Aetiology What can be done? The future Frailty Frailty Frailty (noun): The state of being weak in health or body
Continence, falls and the frailty syndrome Outline Frailty Geriatric syndromes and giants Aetiology What can be done? The future Frailty Frailty Frailty (noun): The state of being weak in health or body
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
There s No Place like Home
 THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
The role of the Geriatrician
 Post-operative management of the older adults with cancer The role of the Geriatrician Sofia Duque Hospital Beatriz Ângelo Geriatric University Unit Faculty of Medicine of Lisbon Geriatrics Study Group
Post-operative management of the older adults with cancer The role of the Geriatrician Sofia Duque Hospital Beatriz Ângelo Geriatric University Unit Faculty of Medicine of Lisbon Geriatrics Study Group
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
Geriatric Hip Fracture Co-Management. Pannida Wattanapanom, M.D., FACP.
 Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Research & Reviews: Journal of Nursing & Health Sciences
 Research & Reviews: Journal of Nursing & Health Sciences A Cohort Study on Detecting Delirium Using 4 A s Test in a London, UK, Hospital Annalisa Casarin 1,2,3, Pranev Sharma 4, Satyawan Bhat 2,3, Marcela
Research & Reviews: Journal of Nursing & Health Sciences A Cohort Study on Detecting Delirium Using 4 A s Test in a London, UK, Hospital Annalisa Casarin 1,2,3, Pranev Sharma 4, Satyawan Bhat 2,3, Marcela
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
PSYCHOSOCIAL SYMPTOMS (DELIRIUM)
") PSYCHOSOCIAL SYMPTOMS (DELIRIUM) Rut Kiman MD, MSc Head Pediatric Palliative Care Team Hospital Nacional Prof. A. Posadas Buenos Aires -Argentina Senior Lecturer. Pediatric Department School of Medicine.
PSYCHOSOCIAL SYMPTOMS (DELIRIUM) Rut Kiman MD, MSc Head Pediatric Palliative Care Team Hospital Nacional Prof. A. Posadas Buenos Aires -Argentina Senior Lecturer. Pediatric Department School of Medicine.
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Risk factors for incident delirium in acute medical in-patients. A systematic review
 Risk factors for incident delirium in acute medical in-patients. A systematic review Reviewers Emily Cull RN, BN(Hons) 1 Bridie Kent PhD, BSc(Hons), RN 2 Dr Nicole M. Phillips DipAppSc(Nsg), BN, GDipAdvNsg(Educ),
Risk factors for incident delirium in acute medical in-patients. A systematic review Reviewers Emily Cull RN, BN(Hons) 1 Bridie Kent PhD, BSc(Hons), RN 2 Dr Nicole M. Phillips DipAppSc(Nsg), BN, GDipAdvNsg(Educ),
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Delirium Assessment and management in relation to falls risk in hospital
 Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
QuickTime and a DV - NTSC decompressor are needed to see this picture.
 QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Adverse Outcomes After Hospitalization and Delirium in Persons With Alzheimer Disease
 Adverse Outcomes After Hospitalization and Delirium in Persons With Alzheimer Disease J. Sukanya 05.Jul.2012 Outline Background Methods Results Discussion Appraisal Background Common outcomes in hospitalized
Adverse Outcomes After Hospitalization and Delirium in Persons With Alzheimer Disease J. Sukanya 05.Jul.2012 Outline Background Methods Results Discussion Appraisal Background Common outcomes in hospitalized
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
DSM-5 MAJOR AND MILD NEUROCOGNITIVE DISORDERS (PAGE 602)
") SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Management of Delirium in the Elderly Patients: A Review of Evidence
 Review Article imedpub Journals http://journals.imedpub.com Journal of Drug Abuse 2471-853X DOI: 10.21767/2471-853X.10006 Abstract Management of Delirium in the Elderly Patients: A Review of Evidence Delirium
Review Article imedpub Journals http://journals.imedpub.com Journal of Drug Abuse 2471-853X DOI: 10.21767/2471-853X.10006 Abstract Management of Delirium in the Elderly Patients: A Review of Evidence Delirium
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Prevention of Delirium:! Acute Heart Failure! Bonnie L. Albert, DNP, ACNP-BC!
 Prevention of Delirium:! Acute Heart Failure! Bonnie L. Albert, DNP, ACNP-BC! Delirium: Hospital Complication! Delirium: a disturbance of consciousness characterized by acute onset and fluctuating course
Prevention of Delirium:! Acute Heart Failure! Bonnie L. Albert, DNP, ACNP-BC! Delirium: Hospital Complication! Delirium: a disturbance of consciousness characterized by acute onset and fluctuating course
Delirium and cognitive impairment in the perioperative
 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
The Long-term Prognosis of Delirium
 The Long-term Prognosis of Jane McCusker, MD, DrPH, Professor, Epidemiology and Biostatistics, McGill University; Head, Clinical Epidemiology and Community Studies, St. Mary s Hospital, Montreal, QC. Nine
The Long-term Prognosis of Jane McCusker, MD, DrPH, Professor, Epidemiology and Biostatistics, McGill University; Head, Clinical Epidemiology and Community Studies, St. Mary s Hospital, Montreal, QC. Nine
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Care of older people in surgery (COPS)
") Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Brain dysfunction in the ICU
 High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Disentangling Delirium and Dementia
 Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Quality of Acute Care for Older Persons with Dementia
 Quality of Acute Care for Older Persons with Dementia A Hospital-Based Pilot Study Chien-Liang Liu Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, Taiwan 2013/04/20 Outline Background
Quality of Acute Care for Older Persons with Dementia A Hospital-Based Pilot Study Chien-Liang Liu Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, Taiwan 2013/04/20 Outline Background
Cognitive Status. Read each question below to the patient. Score one point for each correct response.
 Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Pharmacological Treatment of Aggression in the Elderly
 Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Delirium: A Condition of All Ages. Delirium, also known as acute confusional state, Definition. Epidemiology
 Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
9/19/2018. Common Medical Issues and Management in the Geriatric Trauma Patient. Disclosures. Objectives. I have no financial disclosures
 Common Medical Issues and Management in the Geriatric Trauma Patient 2018 UW Medicine EMS & Trauma Conference September 17, 2018 Joe C. Huang, M.D. Clinical Instructor Medical Director, Geriatrics-Palliative
Common Medical Issues and Management in the Geriatric Trauma Patient 2018 UW Medicine EMS & Trauma Conference September 17, 2018 Joe C. Huang, M.D. Clinical Instructor Medical Director, Geriatrics-Palliative
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
People at the centre of health and care
 People at the centre of health and care Improving Care for Older People in Acute Care F is for Frailty F is for Frailty Identification and co-ordination of care for frail older people Starting point -
People at the centre of health and care Improving Care for Older People in Acute Care F is for Frailty F is for Frailty Identification and co-ordination of care for frail older people Starting point -
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
UNTHSC TCOM Geriatric Competencies Curriculum Mapping Document
 INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject