Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
|
|
|
- Marianna Gallagher
- 5 years ago
- Views:
Transcription

1 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014

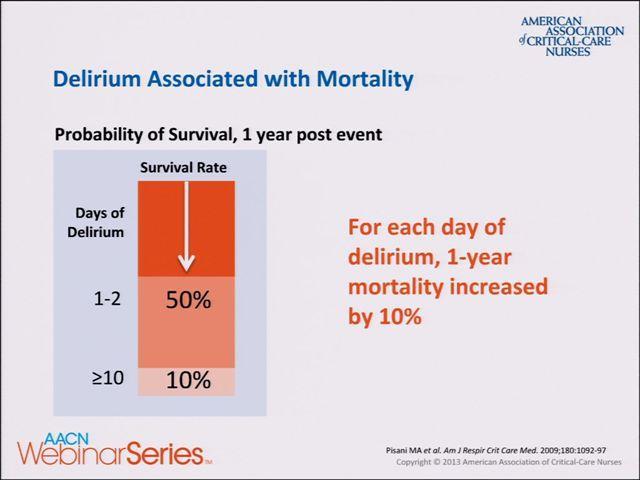
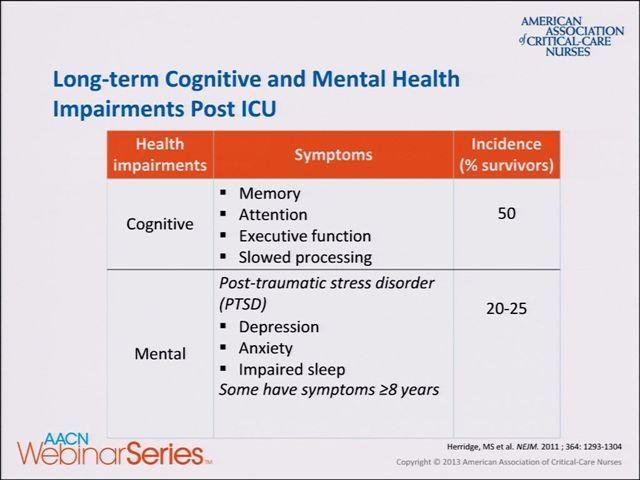
2 Delirium Delirium is an acute change in LOC accompanied by inattention and either a change in cognition or perceptual disturbance Hyperactive vs Hypoactive Affects up to 80% of ICU patients with increased length of ICU/hospital stay, time on ventilator, mortality, and long term neuropsychological deficits (Ely et al, JAMA, 2004)
3
4

5 Yasuda M et al. Neurology 2000;55: American Academy of Neurology
")
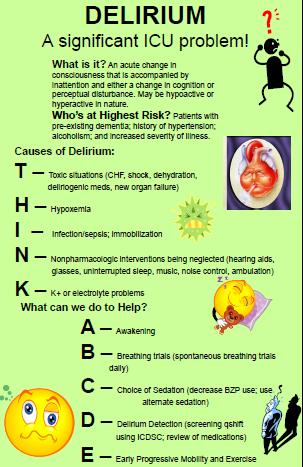
6 Delirium Risk Factors Pre-existing dementia History of hypertension Alcoholism High severity of illness at admission (ie. APACHE score)
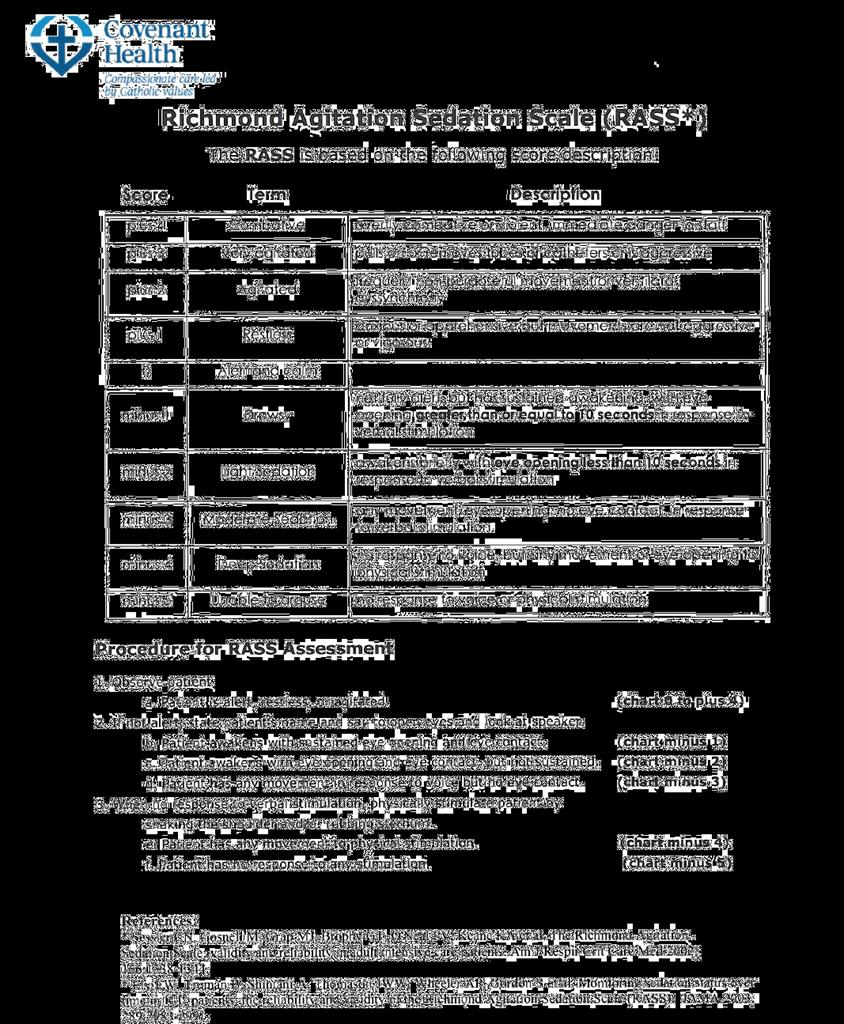
7 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the ICU (SCCM, 2012) Maintain light levels of sedation Utilize a reliable sedation assessment tool (RASS/SAS) Utilize a non-bzp sedation strategy (ie. Propofol/Dexmedetomidine) Monitor delirium scores routinely (CAM-ICU or ICDSC) BZP use may be a risk factor for the development of delirium Dexmedetomidine may be useful in decreasing delirium in ventilated patients Mobilize patients early
8 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the ICU (SCCM, 2012) No evidence to support use of haloperidol or atypical antipsychotics to prevent delirium Atypical antipsychotics may reduce the duration of delirium; no evidence for haloperidol Do not suggest using antipsychotics in patients at significant risk for torsades Dexmedetomidine rather than BZP infusions should be considered for sedation to reduce duration of delirium in non ETOH withdrawal patients Target light levels of sedation or daily sedation interruption Promote sleep No recommendation for specific modes of ventilation to promote sleep Recommend interdisciplinary team approach to facilitate use of guidelines

9 Collaborative Approach to Decreasing ICU Delirium Misericordia Hospital Strategy Aim and Objectives : Develop and deliver education and support for staff regarding delirium awareness, prevention, and management within 12 months. Determine baseline incidence of delirium within 3-4 months. Implement processes to screen 100% of all ICU patients for delirium within 6 months or less. Identify and implement standardized delirium prevention interventions in all ICU patients within 12 months or less. Implement standardized interventions for the management of delirium within 12 months or less. Implement strategies to support families of patients with delirium within 18 months or less. Establish ongoing education parameters.
10 Goals To decrease the incidence of delirium in the Misericordia ICU by: a) Reducing the utilization of analgesic and sedation infusions b) Reducing the utilization of restraints c) Decreasing ventilation days of ICU patients d) Improving mobilization of ICU patients e) Improving consecutive hours of sleep for patients and noise reduction
11
12
13
14 ICU Delirium Outcomes Percent of ICU Patients Screened % 80.00% 60.00% 40.00% 20.00% 0.00%
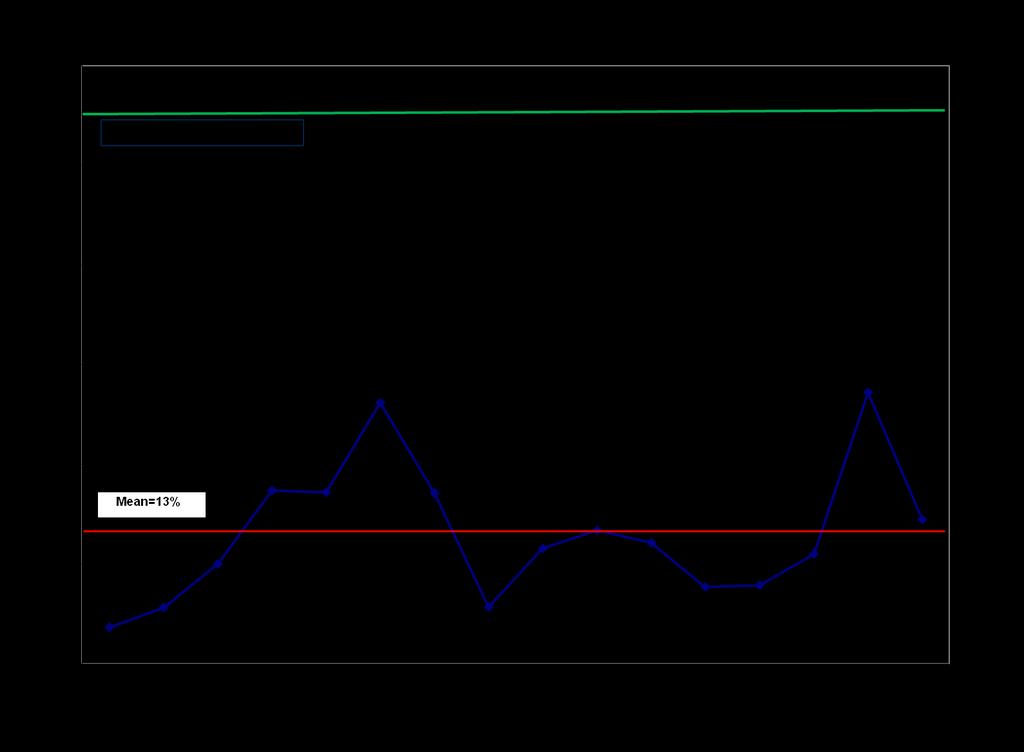
15 Delirium Incidence Misericordia ICU 70.00% Peak Incidence of H1N % 50.00% 40.00% 30.00% Mean = 34.92% 20.00% 10.00% 0.00%
16 ICU Sedation Usage By Year Number of Patients MORPHINE HYDROMORPHONE FENTANYL MIDAZOLAM PROPOFOL DEXMEDETOMIDINE
17
18
19 Average Number of Mobilizations per patient per 24 hours 3 Goal Early Mobilization Education Blitz Aug 15/12 Aug 24/12 Oct 19/12 Oct 26/12 Feb 15/13 Aug 23/13 Jan 17/14

20
21 ICU Ventilator Days Number of Patient Self extubations Average Number of Ventilator Days Peak Incident H1N
22 Number of Days ICU Length of Stay
23 ICU Admission Orders

24 ICU: Visual Analog Scale Aim for total score of 0 3 If total score > 3, treat with analgesic as ordered Adapted with approval from Wong-Baker Faces, Pain Rating Scale, 1983
25
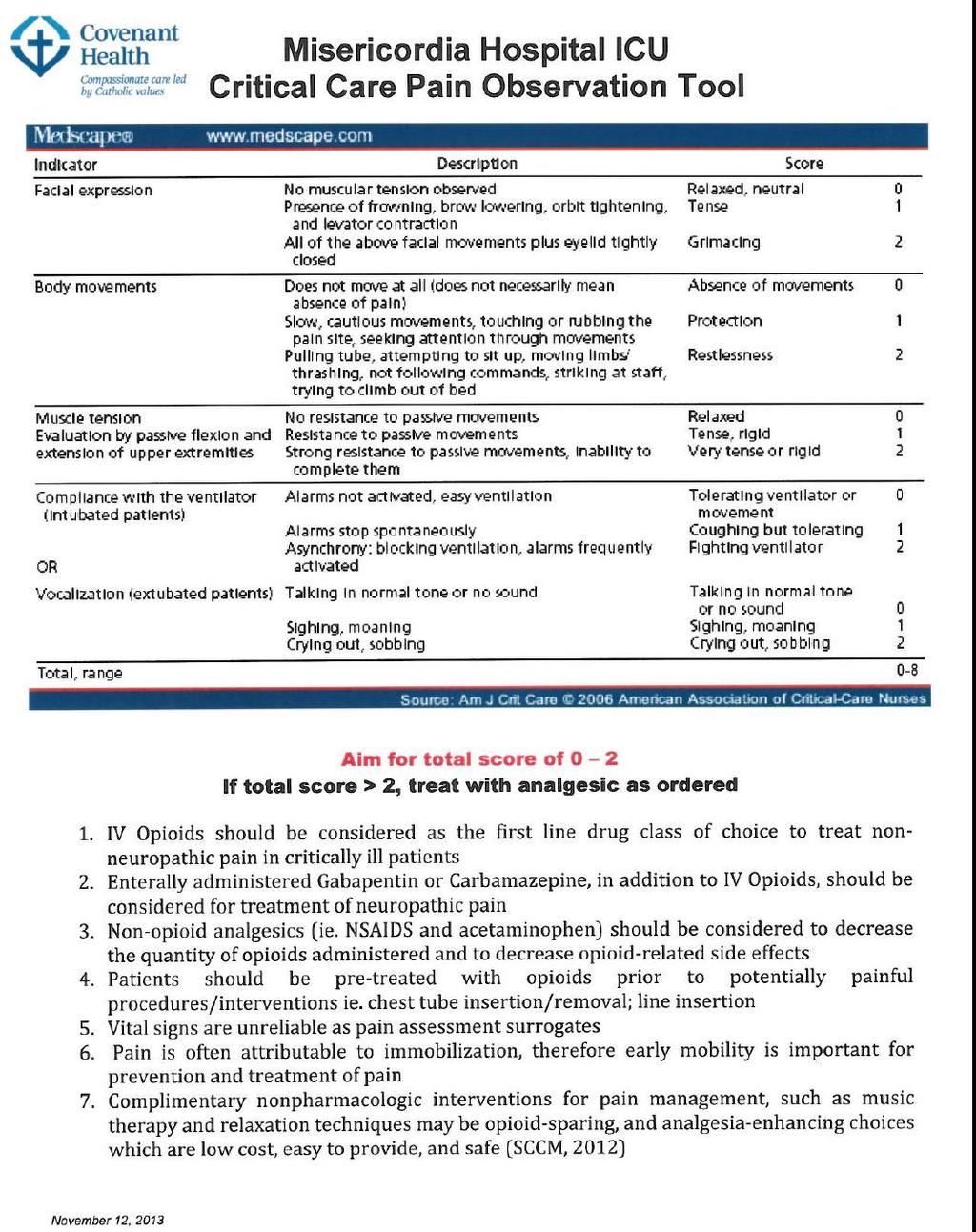
26 Treatment Approach to Agitated/ Delirious Patient Prevention is the KEY!!!!! Utilize narcotics as first option (IV Opioids) for non-neuropathic pain; add Gabapentin/Carbamazapine for neuropathic pain Pre-treat procedural pain
.")
27 Treatment Approach to Agitated/ Delirious Patient Clinical Pearls Atypical anti-psychotics (quetiapine, olanzapine, risperadone) Haloperidol no evidence to suggest that haloperidol decreases length of delirium Dexmedetomidine infusion (bolus 1mcg/kg or 0.5mcg/kg/hr; range mcg/kg/hr). For delirium unrelated to ETOH/BZP withdrawal, dexmedetomidine infusion should be considered for sedation to reduce the duration of delirium Propofol
:S494-501) -Infusions of BZPs associated with increased drug dosage, increased LOS, and increase in incidence of VAP GABA A receptors may")
 Dexmedetomidine - α2 agonist (IV bolus 1mcg/kg then infusion at 0.2-1.")
28 Treatment Approach to Agitated/ Delirious Patient the Patient with ETOH Withdrawal Benzodiazepines (ATC prn dosing) Symptom triggered therapy vs scheduled therapy associated with shorter duration of treatment, decreased BZP dose (Crit Care Med, 2010,38(9 Suppl):S ) -Infusions of BZPs associated with increased drug dosage, increased LOS, and increase in incidence of VAP GABA A receptors may become saturated with high dose BZPs therefore increasing doses will be ineffective Propofol/Barbiturates may modify withdrawal by an alternative pathway Clonidine α2 agonist ( mg po/ng BID) Dexmedetomidine - α2 agonist (IV bolus 1mcg/kg then infusion at mcg/kg/hr) may be utilized as an adjunct to BZPs Baclofen GABA B agonist (20mg po/ng BID-TID Ethanol (from the intensivist s office )
29 Accomplishments We have developed and implemented a delirium screening tool in our ICU with > 90% compliance with screening. Our delirium incidence is 15-40% with a goal of < 20%. We have significantly reduced our utilization of narcotic and benzodiazepine infusions, while increasing our use of dexmedetomine. We have significantly reduced the use of restraints. Mobility has improved from an average of 1.2 to 2.3 mobilization episodes per patient/day. We have developed a current set of ICU Admission Orders which reflect our ICU delirium strategy. We have implemented a pain assessment and treatment strategy.


30 Next Steps Development and implementation of a Family Centered Care strategy including: Distribution of ICU Family Satisfaction Survey to all patients/families Use of All About Me tool to learn more about each individual s unique needs Development and implementation of a Noise Reduction and Sleep Promotion Strategy

31 ALL ABOUT ME My Name is: You should also know: I Like To be Called: My favorite things: My Family and Friends are: My work before I got sick was: Pets: Music: Song: Books: Sports: T.V. show: Channels: I am stressed when: Glasses At home use: Hearing Aides Other Dentures Contact Lens Adapted from MGH presentation 2009
32
33
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline
 Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment
 Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES
 WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Interprofessional Trauma Conference September 28th 2018 Montreal
 Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION
 ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Delirium Screening and Prevention Faculty Disclosures
 Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium Screening and Prevention. Faculty Disclosures. Objectives 5/13/2014. I have nothing to disclose
 Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
The Difficult to Sedate ICU Patient
 The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Implementing the 2013 PAD Guidelines
 1 of 20 8/11/2013 10:25 PM www.medscape.com Implementing the 2013 PAD Guidelines Top Ten Points to Consider Brenda T. Pun, MSN, RN, ACNP, Michele C. Balas, PhD, RN, APRN-NP, CCRN, Judy Davidson, DNP, RN,
1 of 20 8/11/2013 10:25 PM www.medscape.com Implementing the 2013 PAD Guidelines Top Ten Points to Consider Brenda T. Pun, MSN, RN, ACNP, Michele C. Balas, PhD, RN, APRN-NP, CCRN, Judy Davidson, DNP, RN,
Approach to agitated patient in ICU
 Approach to agitated patient in ICU 12-2-2016 Kodati Rakesh Senior resident Pulmonary medicine Agitation Psychomotor disturbance characterized by a marked increase in both motor and psychological activities,
Approach to agitated patient in ICU 12-2-2016 Kodati Rakesh Senior resident Pulmonary medicine Agitation Psychomotor disturbance characterized by a marked increase in both motor and psychological activities,
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD
 SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD OVERVIEW Correctable causes of agitation Pain assessment opioids Agitation assessment BZNs, propofol, precedex comparisons Delirium haldol, antipsychotics
SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD OVERVIEW Correctable causes of agitation Pain assessment opioids Agitation assessment BZNs, propofol, precedex comparisons Delirium haldol, antipsychotics
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER
 Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Delirium is a frequent complication in the ICU setting.
 Clinical Investigations Dexmedetomidine for the Treatment of Hyperactive Delirium Refractory to Haloperidol in Nonintubated ICU Patients: A Nonrandomized Controlled Trial* Genís Carrasco, PhD, MD; Nacho
Clinical Investigations Dexmedetomidine for the Treatment of Hyperactive Delirium Refractory to Haloperidol in Nonintubated ICU Patients: A Nonrandomized Controlled Trial* Genís Carrasco, PhD, MD; Nacho
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Delirium: Prevention with Melatonin
 Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Juliana Barr, MD, FCCM
 Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim
Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim
Delirium in the ICU Pamela L. Smithburger, PharmD, MS, BCPS, BCCCP, FCCP Associate Professor, University of School of Pharmacy
 Delirium in the ICU Pamela L. Smithburger, PharmD, MS, BCPS, BCCCP, FCCP Associate Professor, University of Pi@sburgh School of Pharmacy Pa2ent Case JJ is 75 Yo male admi@ed to the MICU on 12/10 with acute
Delirium in the ICU Pamela L. Smithburger, PharmD, MS, BCPS, BCCCP, FCCP Associate Professor, University of Pi@sburgh School of Pharmacy Pa2ent Case JJ is 75 Yo male admi@ed to the MICU on 12/10 with acute
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit
 Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Addressing Emergency Neuro- Pharmacologic Controversies Head-On. What dose of IV benzodiazepine makes you uncomfortable?
 Addressing Emergency Neuro- Pharmacologic Controversies Head-On 38 y/o 136 bpm Bryan D. Hayes @PharmERToxGuy Sz, tremor, hallucinations Which benzodiazepine would you administer first? Why? Diazepam Lorazepam
Addressing Emergency Neuro- Pharmacologic Controversies Head-On 38 y/o 136 bpm Bryan D. Hayes @PharmERToxGuy Sz, tremor, hallucinations Which benzodiazepine would you administer first? Why? Diazepam Lorazepam
Top 5 things you need to know about pediatric procedural sedation
 Top 5 things you need to know about pediatric procedural sedation Dr. Marc N. Francis MD, FRCPC ACH/FMC Emergency Physician Clinical Lecturer University of Calgary Assistant Program Director FRCPC-EM STARS
Top 5 things you need to know about pediatric procedural sedation Dr. Marc N. Francis MD, FRCPC ACH/FMC Emergency Physician Clinical Lecturer University of Calgary Assistant Program Director FRCPC-EM STARS
Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes
 The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
From the Department of Pharmacy (JM, CAF) and Department of Pulmonary and Critical
 and Department of Pulmonary and Critical") PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
ICU Delirium: Recognition, Management and Long-Term Outcomes
 ICU Delirium: Recognition, Management and Long-Term Outcomes Sandy Staveski RN, PhD, CPNP-AC/PC, CNS Assistant Professor, Nurse Scientist Cincinnati Children s Hospital Medical Center Research in Patient
ICU Delirium: Recognition, Management and Long-Term Outcomes Sandy Staveski RN, PhD, CPNP-AC/PC, CNS Assistant Professor, Nurse Scientist Cincinnati Children s Hospital Medical Center Research in Patient
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium in Cancer: Psychopharmacologic Management
 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Vanderbilt University Medical Center Multidisciplinary Surgical Critical Care
 Vanderbilt University Medical Center Multidisciplinary Surgical Critical Care PROTOCOLIZING AND MONITORING SEDATION, ANALGESIA AND DELIRIUM IN THE CRITICALLY ILL Introduction Critically ill patients are
Vanderbilt University Medical Center Multidisciplinary Surgical Critical Care PROTOCOLIZING AND MONITORING SEDATION, ANALGESIA AND DELIRIUM IN THE CRITICALLY ILL Introduction Critically ill patients are