Prevalent Sleep Disordered Breathing & Obstructive Sleep Apnea in Spite of Treatment for Acromegaly
|
|
|
- Kerrie Carroll
- 5 years ago
- Views:
Transcription

1 Prevalent Sleep Disordered Breathing & Obstructive Sleep Apnea in Spite of Treatment for Acromegaly Chris Yedinak DNP,MN,FNP Assistant Professor Oregon Health & Sciences University Portland. Oregon. USA Date: July 30 th 2017 STTI -Dublin
2 DISCLOSURES No conflicts of interest with respect to this presentation
3 Objectives 1. Describe the relationship of morphologic changes associated with acromegaly and the risk of sleep disordered breathing (SDB)or obstructive sleep apnea (OSA) a.define sleep disordered breathing and OSA b.define acromegaly c.outline overall risk factors for SDB and OSA d.outline morphologic changes that affect airway function in acromegaly e.identify co-morbid risks of OSA 2. Identify populations with OSA requiring further etiologic evaluation a.outline signs and symptoms indicative of risk b.select populations with OSA at risk for acromegaly c.outline co-morbidities of OSA in acromegaly 3. Explain rationale for re-screening male and female patients cured of acromegaly for OSA a.demonstrate the use of screening tools in risk assessment for OSA/SDB b.argue for follow up sleep study for female patients cured/ of acromegaly.

4 Sleep Disordered Breathing: Episodic absence of breathing Oxygen saturation lower than 90%
5 Sleep Apnea Central- neural mediation of disordered or periodic breathing: injury, genetic autonomic dysfunction -etiology in brain stem Obstructive- repeated episodes of partial (hypopnea) or full (apnea) obstruction of the upper airway during sleep causing oxygen desaturation and brief arousal. Mixed
6




7 SDB and OSA- result in: Devita et al.,2016; Silva et al., 2016; Nutt et al.,2013; Powlson & Gurnell.,2015, Bilal 2017

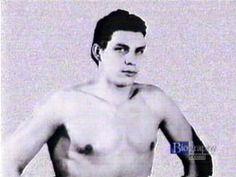
8 Acromegaly
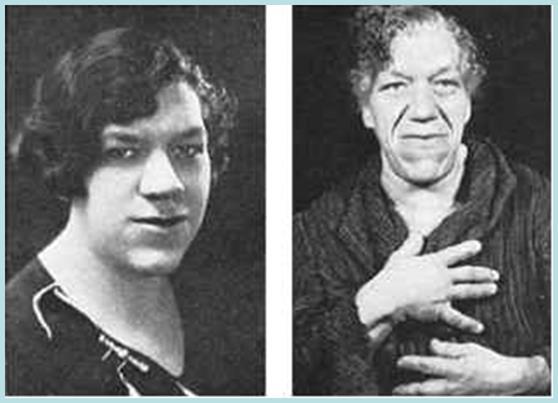
9 Acromegaly: A pituitary adenoma which secretes excess growth hormone Rare -5 cases/million/year * prevalence is 60 cases/million Insidious average of 4-10 years to diagnosis (Melmed,2009). Soft tissue and bony overgrowth. Cardiovascular mortality risk 4.6 times higher than that of the general population (Mestron et al.,2004; Sherlock et al.,2014).


10 Acromegaly & Sleep Apnea: Hypertrophy of pharyngeal soft tissue Craniofacial deformations
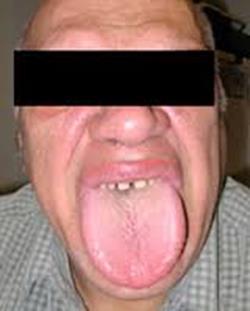
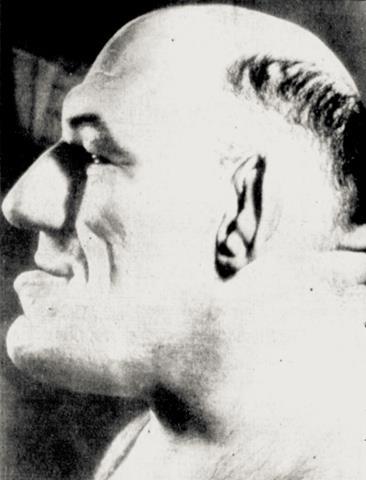

11 Macroglossia Jaw & Joint deformities
12


13


.")
14 Acromegaly & Obstructive Sleep Apnea: 40-80% Acromegaly 5% General Population (Galerneau et al.,2016). OBS/OSA = Acromegaly Acromegaly = OBS/OSA
15 Problem: Theoretically soft tissue hypertrophy is reversible post treatment (Powlson & Gurnell.,2015) Little data to support resolution of SDB/ OSA post normalization of growth hormone levels
16 AIM: To determine the prevalence of OSA by diagnosis versus those patients meeting risk criteria for SDB/OSA both pre and post treatment for acromegaly.
17 Methods: Prospective pre/post design Convenience sampling from a single institution Inclusion Criteria New diagnosis of acromegaly (biochemical + pathology) Patients with & without Dx of OSA pre treatment Exclusion Criteria: Other uncontrolled concomitant diseases History of nasopharyngeal surgery
18 Method: Patients without OSA diagnosis were evaluated by criteria for risk of OSA StopBang questionnaire ( > intermediate risk) Epworth Sleepiness Scale ( Score>10) All patients re-evaluated after surgical/ medically normalized growth hormone levels. Statistical analysis using PASW 18. IRB approved.
19 StopBang Questionnaire: S- Snore loudly? T- Tired, fatigued, or sleepy during daytime? O- Observed no breathing? P- High blood pressure? B- Body Mass Index (BMI) more than 35? A- Age over 50? N- Neck circumference greater than 40cm? G- Gender male? Low Risk : Yes 0-2 Intermediate Risk: Yes 3-4 High Risk: Yes 5-8
20 Epworth Sleepiness Scale: Chance of Dozing ( 0-3) 1. Sitting and Reading 2. Watching TV 3. Sitting, inactive in a public place (e.g. a theater or a meeting) 4. As a passenger in a car for an hour without a break 5. Lying down to rest in the afternoon when circumstances permit 6. Sitting and talking to someone 7. Sitting quietly after lunch without alcohol 8. In a car, while stopped for a few minutes in traffic 0-10 = normal
21 Results: N=52
22 Demographics N=52 Pre treatment Post Treatment Males Females Males Females Mean Age (years) Dx OSA # Meeting risk criteria * Total Duration of follow up 66 months Resolution 2 4 New diagnosis 2 2 * All patients meeting criteria referred for polysomnography
23 Results: Post-treatment Linear by linear association indicated increasing age was associated with a higher likelihood of meeting criteria or having a diagnosis of OSA (p=0.04) OSA prevalence same for both genders pre treatment ( X 2, p=0.19) Males were more likely to have a diagnosis of OSA after treatment for acromegaly (p=0.04). There was a significant reduction in the number of patients meeting risk criteria for OSA post treatment (P>0.001) There was no gender difference with respect to those meeting criteria for risk of OSA after treatment.

24 Post-operative Change in OSA Male Female resolution of OSA New Onset OSA

25 Prevalence of OSA Pre/Post Treatment for Acromegaly By Criteria Pre Pre Dx OSA 17 By criteria post Post Dx OSA
26 Correlations: Male Gender Post op OSA rs=0.3,p=0.04 Pre OSA Post op OSA rs=0.52,p= Higher Baseline IGF-1 OSA rs=-0.27,p=0.05 Post Op IGF-1 OSA rs=0.7,p=0.6 Post op Weight loss OSA rs=0.2,p=0.2
27 Conclusion Both males and females with acromegaly should be evaluated for sleep apnea A diagnosis of SDB or OSA may be a symptom of acromegaly particularly, in a young female SDB and OSA may persist post treatment for acromegaly despite normalization of growth hormone levels, particularly in males Some OSA risk factors such may resolve post treatment However, increasing age and BMI post treatment may be risk factors Validation in larger acromegaly patient populations recommended
28 References: Ramos-Levi, A.M & Marazuela, M. (2016). Sleep apnea syndrome in acromegalic patients: can morphological evaluation guide us to optimize treatment? Endocrine. 51(2):203-4.doi: /s Galerneua, L-M., Pepin, J-L., Borel, A-L., Chambre,O., Sapene,M., Stach,B., & Caron, P. (2016). Acromegaly in sleep apnoea patients: a large observational study of 755 patients. European Respiratory Journal,48: Powlson,A.S.,& Gurnell,M. (2016). Cardiovascular Disease and Sleep-Disordered Breathing in Acromegaly. Neuroendocrinology. 103(1): doi: / Melmed, S. (2009) Acromegaly pathogenesis and treatment. Journal of Clinical Investment,119, Mestron, A., Webb, S.M., Astorga, R., Benito, P., Catala, M., Gaztambide, S.,... Gilabert, M., (2004) Epidemiology, clinical characteristics, outcome, morbidity and mortality in acromegaly based on the Spanish Acromegaly Registry (Registro Espanol de Acromegalia, REA). Eur J Endocrinol, 151,
29 References: Sherlock, M., Reulen, R.C., Aragon-Alonso, A., Ayuk J, Clayton RN, Sheppard MC.,...Stewart,P., (2014) A paradigm shift in the monitoring of patients with acromegaly: last available growth hormone may overestimate risk. J Clin Endocrinol Metab, 99, Devita, M., Montemurro,S., Ramponi,S., Marvisi M., Villani,D., Raimondi,M.C,... Mondini S. (2016).Obstructive sleep apnea and its controversial effects on cognition. Journal of Clininical Experimental Neuropsycholgy.15:1-12. Silva, G.E., Goodwin, J.L., Vana,K.D., & Quan, S.F.,(2016). Obstructive Sleep Apnea and Quality of Life: Comparison of the SAQLI, FOSQ, and SF-36 Questionnaires. Southwest Journal of Pulmonary Critical Care. 3(3): Dutt, N., Janmeja, A.K., Prasanta Raghab Mohapatra, P.R., & Anup Kumar Singh,A.K., ( 2013). Quality of life impairment in patients of obstructive sleep apnea and its relation with the severity of disease. Lung India. 30(4): doi: /

30 Thank you. Questions?
Management of OSA in the Acute Care Environment. Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018
 Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea
 Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA
 WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA Wayne Driscoll Clinical Education Specialist 2 SLEEP APNEA IN THE NEWS Carrie Fisher died from sleep apnea, other factors, coroner says USA Today NJ Transit engineer
WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA Wayne Driscoll Clinical Education Specialist 2 SLEEP APNEA IN THE NEWS Carrie Fisher died from sleep apnea, other factors, coroner says USA Today NJ Transit engineer
The following questions are about your sleep. Please consider both what others have told you about your sleep and what you know yourself.
 Sleep History Form FORM CODE: SLE VERSION A 1/29/2009 PARTICIPANT ID NUMBER: CONTACT YEAR: 0 9 LAST NAME: INITIALS: INSTRUCTIONS: This form should be completed during the participant's clinic visit. ID
Sleep History Form FORM CODE: SLE VERSION A 1/29/2009 PARTICIPANT ID NUMBER: CONTACT YEAR: 0 9 LAST NAME: INITIALS: INSTRUCTIONS: This form should be completed during the participant's clinic visit. ID
Balboa Island Dentistry (949)
") Do You Snore? Are you always tired? Snoring is no laughing matter! It may be more than an annoying habit. It may be a sign of. How well do you sleep? Just about everyone snores occasionally. Even a baby
Do You Snore? Are you always tired? Snoring is no laughing matter! It may be more than an annoying habit. It may be a sign of. How well do you sleep? Just about everyone snores occasionally. Even a baby
Types of Sleep Studies 8/28/2018. Ronald S. Prehn, ThM, DDS. Type 1 Attended in-lab polysomnography (PSG) 18 leads
 18 leads") Ronald S. Prehn, ThM, DDS rprehn@tmjtexas.com Board Certified in Dental Sleep Medicine Board Certified in Orofacial Pain Types of Sleep Studies Type 1 Attended in-lab polysomnography (PSG) 18 leads Type
Ronald S. Prehn, ThM, DDS rprehn@tmjtexas.com Board Certified in Dental Sleep Medicine Board Certified in Orofacial Pain Types of Sleep Studies Type 1 Attended in-lab polysomnography (PSG) 18 leads Type
Sleep Diordered Breathing (Part 1)
") Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Obstructive sleep apnoea How to identify?
 Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential conflict of interest None Obstructive
Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential conflict of interest None Obstructive
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential
DECLARATION OF CONFLICT OF INTEREST Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential
What s the name of your position?
 What s the name of your position? What are some basic work responsibilities (e.g primarily front desk/administration, light lifting or heavy liftingplease indicate pounds)? CONSENT FORM FOR USE AND DISCLOSURE
What s the name of your position? What are some basic work responsibilities (e.g primarily front desk/administration, light lifting or heavy liftingplease indicate pounds)? CONSENT FORM FOR USE AND DISCLOSURE
Sleep Screening Questionnaire
 Version: SLPQV1 Sleep Screening Questionnaire OFFICE USE Patient ID: NAME: CURRENT DATE: / / DATE OF BIRTH: / / MALE FEMALE Referring Physician: Contact ID: Number Number #1 = the most severe symptom #1
Version: SLPQV1 Sleep Screening Questionnaire OFFICE USE Patient ID: NAME: CURRENT DATE: / / DATE OF BIRTH: / / MALE FEMALE Referring Physician: Contact ID: Number Number #1 = the most severe symptom #1
493 Blackwell Road, Suite 317-A, Warrenton, VA
 493 Blackwell Road, Suite 317-A, Warrenton, VA. 20186 Dear Sleep Study Patient, Attached is the patient questionnaire for your sleep study. Please complete and mail or fax the enclosed forms as soon as
493 Blackwell Road, Suite 317-A, Warrenton, VA. 20186 Dear Sleep Study Patient, Attached is the patient questionnaire for your sleep study. Please complete and mail or fax the enclosed forms as soon as
I would like for my patient to be seen in Sleep Medicine consultation and managed by the sleep physician. Yes No
 701 E. COUNTY LINE ROAD, SUITE 207. GREENWOOD, IN. 46143 OFFICE317-887-6400 FAX 317-887-6500 indianasleepcenter.com REFERRAL FOR SLEEP EVALUATION Patient Name:_ Phone: I would like for my patient to be
701 E. COUNTY LINE ROAD, SUITE 207. GREENWOOD, IN. 46143 OFFICE317-887-6400 FAX 317-887-6500 indianasleepcenter.com REFERRAL FOR SLEEP EVALUATION Patient Name:_ Phone: I would like for my patient to be
Sleep. Anil Rama, MD Medical Director, Division of Sleep Medicine The Permanente Medical Group
 Sleep Anil Rama, MD Medical Director, Division of Sleep Medicine The Permanente Medical Group Assistant Adjunct Clinical Faculty Stanford School of Medicine Circadian Rhythm of Sleep Body temperature 7
Sleep Anil Rama, MD Medical Director, Division of Sleep Medicine The Permanente Medical Group Assistant Adjunct Clinical Faculty Stanford School of Medicine Circadian Rhythm of Sleep Body temperature 7
Physician Dentist Collaboration
 Physician Dentist Collaboration Ronald S. Prehn, ThM, DDS Legal Perspective MD CAN LEGALLY MAKE PROPER DIAGNOSIS DDS CAN LEGALLY FABRICATE DENTAL SLEEP APPLIANCES Legal Perspective TWO PROFESSIONS WORK
Physician Dentist Collaboration Ronald S. Prehn, ThM, DDS Legal Perspective MD CAN LEGALLY MAKE PROPER DIAGNOSIS DDS CAN LEGALLY FABRICATE DENTAL SLEEP APPLIANCES Legal Perspective TWO PROFESSIONS WORK
The Implications of a Hospital Break Policy: A Comparison of Two Regional Hospitals Using Survey Data
 The Implications of a Hospital Break Policy: A Comparison of Two Regional Hospitals Using Survey Data Samantha M. Riedy, BS, RPSGT Experimental Psychology Doctoral Program Sleep and Performance Research
The Implications of a Hospital Break Policy: A Comparison of Two Regional Hospitals Using Survey Data Samantha M. Riedy, BS, RPSGT Experimental Psychology Doctoral Program Sleep and Performance Research
Assessment of Sleep Disorders DR HUGH SELSICK
 Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Baptist Health Floyd 1850 State Street New Albany, IN Sleep Disorders Center Lung & Sleep Specialists. Date of Birth: Age:
 Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Emergency Contact Information Name: Phone: Address: Employer Information Employer Name: Address/Street: City: Zip: Phone: Fax:
 SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS
 SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
DESERT CENTER FOR ALLERGY AND CHEST DISEASES HEALTH QUESTIONAIRE NAME. PAST MEDICAL PROBLEMS- Check mark if you have any of the following
 DESERT CENTER FOR ALLERGY AND CHEST DISEASES Pulmonary Medicine, Allergy/Immunology, Sleep Disorders Pulmonary Rehabilitation, Pulmonary Function Laboratory HEALTH QUESTIONAIRE NAME What is your presenting
DESERT CENTER FOR ALLERGY AND CHEST DISEASES Pulmonary Medicine, Allergy/Immunology, Sleep Disorders Pulmonary Rehabilitation, Pulmonary Function Laboratory HEALTH QUESTIONAIRE NAME What is your presenting
Outline. Major variables contributing to airway patency/collapse. OSA- Definition
 Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
 DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY") SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
Patient Adult Information History
 Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Instructions. If you make a mistake, put an "X" over the checkmark. Then put a checkmark in the correct box and draw a circle around that box.
 SLEEP HEART HEALTH STUDY SLEEP HABITS AND LIFESTYLE QUESTIONNAIRE Instructions Thank you for taking time to fill out the enclosed Sleep Habits Questionnaire. Please fill out the form completely. You may
SLEEP HEART HEALTH STUDY SLEEP HABITS AND LIFESTYLE QUESTIONNAIRE Instructions Thank you for taking time to fill out the enclosed Sleep Habits Questionnaire. Please fill out the form completely. You may
PULMONARY & CRITICAL CARE CONSULTANTS OF AUSTIN 1305 West 34 th Street, Suite 400, Austin, TX Phone: Fax:
 Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
Help I Have Problems with My Sleep!
 Help I Have Problems with My Sleep! Over An 85 Year Lifespan Sleep 31% Work 21% Exercise 1% Food and Drink 11% Sleep Is Important! You can survive without food for up to 2 months Without water 3-5 days
Help I Have Problems with My Sleep! Over An 85 Year Lifespan Sleep 31% Work 21% Exercise 1% Food and Drink 11% Sleep Is Important! You can survive without food for up to 2 months Without water 3-5 days
604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA SLEEP HISTORY QUESTIONNAIRE
 604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA 70301 985-493-4759 SLEEP HISTORY QUESTIONNAIRE DATE: / / NAME: AGE (First) (Middle) (Last) ADDRESS: (Street) (City) (State) (Zip) PHONE: Home( ) Work:( )
604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA 70301 985-493-4759 SLEEP HISTORY QUESTIONNAIRE DATE: / / NAME: AGE (First) (Middle) (Last) ADDRESS: (Street) (City) (State) (Zip) PHONE: Home( ) Work:( )
Welcome to the Koala Center for Sleep Disorders
 Welcome to the Koala Center for Sleep Disorders Your health is very important. We are honored to have the opportunity to join you on your wellness journey. In order to provide you with the comprehensive
Welcome to the Koala Center for Sleep Disorders Your health is very important. We are honored to have the opportunity to join you on your wellness journey. In order to provide you with the comprehensive
Sleep History Questionnaire. Sleep Disorders Center Duke University Medical Center. General Information. Age: Sex: F M (select one)
") Sleep History Questionnaire Sleep Disorders Center Duke University Medical Center Part I: General Information Name: Address: Date: Phone: Age: Sex: F M (select one) Education (years of school): Occupation:
Sleep History Questionnaire Sleep Disorders Center Duke University Medical Center Part I: General Information Name: Address: Date: Phone: Age: Sex: F M (select one) Education (years of school): Occupation:
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update
 OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
Associated Neurological Specialties and Sleep Disorder Center
 Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Sleep History Questionnaire
 Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep Questionnaire Name: Sex: Age: Da te: Da te of birth: Height: Weight: Neck siz e: Ref erring Physician: Primary Car e MD:
 www.myvcmf.com 1133 E. Stanley Blvd., Suite 101 Livermore, CA 94550 925 454-4280 5725 W. Las Positas Blvd., Suite 110 Pleasanton, CA 94588 925-416-6767 Sleep Questionnaire Name: Sex: Age: Da te: Da te
www.myvcmf.com 1133 E. Stanley Blvd., Suite 101 Livermore, CA 94550 925 454-4280 5725 W. Las Positas Blvd., Suite 110 Pleasanton, CA 94588 925-416-6767 Sleep Questionnaire Name: Sex: Age: Da te: Da te
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS
 WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine
 Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine PATIENT DEMOGRAPHICS Who is the Physician that referred you to us? Who is the primary care Physician? Date: Do you want this report
Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine PATIENT DEMOGRAPHICS Who is the Physician that referred you to us? Who is the primary care Physician? Date: Do you want this report
Sleep Disorders Diagnostic Center 9733 Healthway Drive, Berlin, MD , ext. 5118
 Sleep Questionnaire *Please complete the following as accurate as possible. Please bring your completed questionnaire, insurance card, photo ID, Pre-Authorization and/or Insurance referral form, and all
Sleep Questionnaire *Please complete the following as accurate as possible. Please bring your completed questionnaire, insurance card, photo ID, Pre-Authorization and/or Insurance referral form, and all
Sleep Apnea. Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa
 Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
HOW S YOUR HEART? GET A FREE HEART HEALTH CHECK ASK YOUR AMCAL PHARMACIST TODAY FREE. 10 minutes. No appointment needed
 HOW S YOUR HEART? GET A FREE HEART HEALTH CHECK FREE 10 minutes No appointment needed ASK YOUR AMCAL PHARMACIST TODAY START YOUR HEART HEALTH ASSESSMENT TODAY Name: Date: Your Amcal pharmacist: HEART HEALTH
HOW S YOUR HEART? GET A FREE HEART HEALTH CHECK FREE 10 minutes No appointment needed ASK YOUR AMCAL PHARMACIST TODAY START YOUR HEART HEALTH ASSESSMENT TODAY Name: Date: Your Amcal pharmacist: HEART HEALTH
PATIENT DEMOGRAPHICS
 PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
Telephone: Fax:
 PATIENT AUTHORIZATION TO RELEASE MEDICAL RECORDS AND DEMOGRAPHIC INFORMATION DATE: SS #: PATIENT NAME: BIRTHDATE: / / PATIENT ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE #: CELL PHONE #: REFERRING PHYSICIAN
PATIENT AUTHORIZATION TO RELEASE MEDICAL RECORDS AND DEMOGRAPHIC INFORMATION DATE: SS #: PATIENT NAME: BIRTHDATE: / / PATIENT ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE #: CELL PHONE #: REFERRING PHYSICIAN
MESA EXAM 5 ANCILLARY STUDY 113 SLEEP QUESTIONNAIRE DATA SET VARIABLE GUIDE
 MESA EXAM 5 ANCILLARY STUDY 113 SLEEP QUESTIONNAIRE DATA SET VARIABLE GUIDE Data Set name : Principal Investigator : Contact Information : MESAe5_SleepQ_20140617 Susan Redline sredline1@rics.bwh.harvard.edu
MESA EXAM 5 ANCILLARY STUDY 113 SLEEP QUESTIONNAIRE DATA SET VARIABLE GUIDE Data Set name : Principal Investigator : Contact Information : MESAe5_SleepQ_20140617 Susan Redline sredline1@rics.bwh.harvard.edu
SLEEP HISTORY QUESTIONNAIRE
 Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
130 Preston Executive Drive Cary, NC Ph(919) Fax(919) Page 1 of 6. Patient History
 Fax(919) Page 1 of 6. Patient History") 130 Preston Executive Drive Cary, NC 27513 Ph(919)462-8081 Fax(919)462-8082 www.parkwaysleep.com Page 1 of 6 Patient History *Please fill out in dark BLACK INK only. General Information Name Sex: Male
130 Preston Executive Drive Cary, NC 27513 Ph(919)462-8081 Fax(919)462-8082 www.parkwaysleep.com Page 1 of 6 Patient History *Please fill out in dark BLACK INK only. General Information Name Sex: Male
Littleton, CO Welcome Packet 8151 Southpark Lane, Suite 200 Littleton, CO 80120
 Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
The Agony or the Ecstasy. Familiar?
 The Agony or the Ecstasy Familiar? Snoring Related Complaints Drives wife from bedroom Girlfriend won t marry me Shakes entire house Ask me to leave movies and church Has had to leave boat so friends could
The Agony or the Ecstasy Familiar? Snoring Related Complaints Drives wife from bedroom Girlfriend won t marry me Shakes entire house Ask me to leave movies and church Has had to leave boat so friends could
Your physician has ordered a sleep study for you on. Your arrival time is scheduled for.
 Dear Patient: Your physician has ordered a sleep study for you on. Your arrival time is scheduled for. The Texas State Sleep Lab is located in the Health Professions Building on the Texas State University
Dear Patient: Your physician has ordered a sleep study for you on. Your arrival time is scheduled for. The Texas State Sleep Lab is located in the Health Professions Building on the Texas State University
Denver, CO Welcome Packet
 Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Sleep Center. Have you had a previous sleep study? Yes No If so, when and where? Name of facility Address
 Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
ANNUAL FOLLOW-UP QUESTIONNAIRE
 SLEEP HEART HEALTH STUDY - TUCSON ANNUAL FOLLOW-UP QUESTIONNAIRE - 2004 Dear Sleep Heart Health Study participant: Today s Date: / / Month Day Year Please take the time to complete and return this short
SLEEP HEART HEALTH STUDY - TUCSON ANNUAL FOLLOW-UP QUESTIONNAIRE - 2004 Dear Sleep Heart Health Study participant: Today s Date: / / Month Day Year Please take the time to complete and return this short
Intake Questionnaire
 Intake Questionnaire In order to make the best use of your appointment time, please complete this form prior to your initial appointment. What is your name? (Who filled in this form?) (Y= yes N=no DK=
Intake Questionnaire In order to make the best use of your appointment time, please complete this form prior to your initial appointment. What is your name? (Who filled in this form?) (Y= yes N=no DK=
SLEEP SCREENING QUESTIONNAIRE
 Patient Information 433 W. University Dr. Rochester, MI 48307 www.rochesteradvanceddentistry.com +1 248 656-2020 SLEEP SCREENING QUESTIONNAIRE Name: DOB: Age: Address: Employer: SS# Home Phone: Work Phone:
Patient Information 433 W. University Dr. Rochester, MI 48307 www.rochesteradvanceddentistry.com +1 248 656-2020 SLEEP SCREENING QUESTIONNAIRE Name: DOB: Age: Address: Employer: SS# Home Phone: Work Phone:
Sleep apnea. What is sleep apnea? What are the symptoms of sleep apnea? Symptoms during the day. Symptoms during sleep
 Sleep apnea Your doctor thinks you may have sleep apnea. The purpose of this fact sheet is to inform you about this disease. It also gives you details about the tests done to diagnose it and possible treatments.
Sleep apnea Your doctor thinks you may have sleep apnea. The purpose of this fact sheet is to inform you about this disease. It also gives you details about the tests done to diagnose it and possible treatments.
Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy
![Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy](/thumbs/96/127246551.jpg "Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy") Health Benefits Employee Services HBE Preventive Health - Sleep Assessment Form Please bring your completed assessment form to your appointment. To schedule an appointment please call 505 844-HBES (4237).
Health Benefits Employee Services HBE Preventive Health - Sleep Assessment Form Please bring your completed assessment form to your appointment. To schedule an appointment please call 505 844-HBES (4237).
Sleep History Questionnaire B/P / Pulse: Neck Circum Wgt: Pulse Ox
 2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
Patient Information. Name: Date of Birth: Address: Number & Street City State Zip Code. Home Number: ( ) Cell Number: ( )
 Cell Number: ( )") Patient Information Name: Date of Birth: Age: Address: Number & Street City State Zip Code Home Number: ( ) Cell Number: ( ) Social Security Number: Marital Status: Religion: Race: Height: Weight: Sex:
Patient Information Name: Date of Birth: Age: Address: Number & Street City State Zip Code Home Number: ( ) Cell Number: ( ) Social Security Number: Marital Status: Religion: Race: Height: Weight: Sex:
MLA HASS LUNG. SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA Phone: Fax:
 MLA HASS LUNG SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA 01453 Phone: 978-728-4641 Fax: 978-978-1382 MEICAL IRECTOR: Payam Aghassi, M, FCCP Thank you for your sleep study order! Attached
MLA HASS LUNG SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA 01453 Phone: 978-728-4641 Fax: 978-978-1382 MEICAL IRECTOR: Payam Aghassi, M, FCCP Thank you for your sleep study order! Attached
ANNUAL FOLLOW-UP QUESTIONNAIRE
 SLEEP HEART HEALTH STUDY - TUCSON ANNUAL FOLLOW-UP QUESTIONNAIRE - 2003 Dear Sleep Heart Health Study participant: Today s Date: / / Month Day Year Please take the time to complete and return this short
SLEEP HEART HEALTH STUDY - TUCSON ANNUAL FOLLOW-UP QUESTIONNAIRE - 2003 Dear Sleep Heart Health Study participant: Today s Date: / / Month Day Year Please take the time to complete and return this short
PATIENT QUESTIONNAIRE Boise Location 7272 W. Potomac Drive Boise, ID (208)
") PATIENT QUESTIONNAIRE Boise Location 7272 W. Potomac Drive Boise, ID 83704 (208)884-2922 ***Questionnaire MUST be completed PRIOR to arrival for appointment*** Today s Date / / / / Last First MI DOB Referring
PATIENT QUESTIONNAIRE Boise Location 7272 W. Potomac Drive Boise, ID 83704 (208)884-2922 ***Questionnaire MUST be completed PRIOR to arrival for appointment*** Today s Date / / / / Last First MI DOB Referring
Room # Critical Care & Pulmonary Consultants, P.C.
 Room # Critical Care & Pulmonary Consultants, P.C. Health History You have been scheduled for an appointment with Critical Care and Pulmonary Consultants, P.C. This health history will help us facilitate
Room # Critical Care & Pulmonary Consultants, P.C. Health History You have been scheduled for an appointment with Critical Care and Pulmonary Consultants, P.C. This health history will help us facilitate
Sleep Symptoms & History
 Sleep Symptoms & History In your own words, please tell us what brings you to the sleep clinic today? How long have you been experiencing your sleep problems? yrs. mos. To give us a precise understanding
Sleep Symptoms & History In your own words, please tell us what brings you to the sleep clinic today? How long have you been experiencing your sleep problems? yrs. mos. To give us a precise understanding
THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk PATIENT QUESTIONNAIRE
 THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk 55 Frid Street, Unit 7, Hamilton, Ontario L8P 4M3 Phone:905-529-2259 Fax: 905-529-2262 282 Linwell Road, Suite 118, St. Catharines, Ontario
THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk 55 Frid Street, Unit 7, Hamilton, Ontario L8P 4M3 Phone:905-529-2259 Fax: 905-529-2262 282 Linwell Road, Suite 118, St. Catharines, Ontario
Obstructive Sleep Apnea in Truck Drivers
 Rocky Mountain Academy of Occupational and Environmental Medicine Denver, Colorado February 6, 2010 Obstructive Sleep Apnea in Truck Drivers Philip D. Parks, MD, MPH, MOccH Medical Director, Lifespan Health
Rocky Mountain Academy of Occupational and Environmental Medicine Denver, Colorado February 6, 2010 Obstructive Sleep Apnea in Truck Drivers Philip D. Parks, MD, MPH, MOccH Medical Director, Lifespan Health
THE PERMANENTE MEDICAL GROUP
 Patient label here THE PERMANENTE MEDICAL GROUP Division of Sleep Medicine COMPLETED BY: PARENT/GUARDIAN CHILD/ADOLESCENT Age: Height: Weight: PEDIATRIC SLEEP QUESTIONNAIRE Thank you completing this questionnaire.
Patient label here THE PERMANENTE MEDICAL GROUP Division of Sleep Medicine COMPLETED BY: PARENT/GUARDIAN CHILD/ADOLESCENT Age: Height: Weight: PEDIATRIC SLEEP QUESTIONNAIRE Thank you completing this questionnaire.
New Patient Sleep Intake
 New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
PATIENTS DEMOGRAPHICS
 PATIENTS DEMOGRAPHICS Date: First Name MI Last Name Sex: M or F (Circle one) Age: Address: City: State: Zip Code: Home Telephone: Work Telephone: Cell/Pager No: Date of Birth: Single: Married: Social Security
PATIENTS DEMOGRAPHICS Date: First Name MI Last Name Sex: M or F (Circle one) Age: Address: City: State: Zip Code: Home Telephone: Work Telephone: Cell/Pager No: Date of Birth: Single: Married: Social Security
1960 FP CENTER FOR SLEEP DISORDERS
 1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
Home Sleep Testing Questionnaire
 Home Sleep Testing Questionnaire Patient Name: DOB: / / Gender: Male Female Study Date: / / Marital Status: Married Cohabitate Single Divorced Widow/Widower Email: Phone: Height: Weight: Neck Size: What
Home Sleep Testing Questionnaire Patient Name: DOB: / / Gender: Male Female Study Date: / / Marital Status: Married Cohabitate Single Divorced Widow/Widower Email: Phone: Height: Weight: Neck Size: What
Tracy Carbone, MD System Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL
 Tracy Carbone, MD System Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL Background Factors Which Increase the Risks for OSA in Pregnancy
Tracy Carbone, MD System Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL Background Factors Which Increase the Risks for OSA in Pregnancy
Mario Kinsella MD FAASM 10/5/2016
 Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
BMI: Family physician : Neck circumference (cm) Hypertension + 4 cm Snoring + 3 cm Witnessed apnea + 3cm Total
 Hypertension + 4 cm Snoring + 3 cm Witnessed apnea + 3cm Total") Last and first names: F M Date: Date of birth: / / YYYY MM DD Weight: kg /lbs Profession/job: Height: _ cm /ft.in. BMI:_ Family physician : ANC (adjusted neck circumference) : Neck circumference (cm) Hypertension
Last and first names: F M Date: Date of birth: / / YYYY MM DD Weight: kg /lbs Profession/job: Height: _ cm /ft.in. BMI:_ Family physician : ANC (adjusted neck circumference) : Neck circumference (cm) Hypertension
Robert E. McMichael, M.D. Medical Director Patient Instructions for a Diagnostic Sleep Study
 NORTH TEXAS SLEEP DISORDERS CENTER Neurology Associates of Arlington, P.A 811 West Interstate 20, Suite G12 Arlington, Texas 76017 (817) 419-6375 Fax (817) 419-6371 Robert E. McMichael, M.D. Medical Director
NORTH TEXAS SLEEP DISORDERS CENTER Neurology Associates of Arlington, P.A 811 West Interstate 20, Suite G12 Arlington, Texas 76017 (817) 419-6375 Fax (817) 419-6371 Robert E. McMichael, M.D. Medical Director
Bariatric Surgery Patient History Questionnaire
 Bariatric Surgery Patient History Questionnaire Your appointment will be delayed if this form is incomplete please print legibly Personal Information Name Date SSN# (for insurance purposes) - - Date of
Bariatric Surgery Patient History Questionnaire Your appointment will be delayed if this form is incomplete please print legibly Personal Information Name Date SSN# (for insurance purposes) - - Date of
Sleep Disorders and their management
 Clinical Stream Sleep Disorders and their management Dr Alex Bartle Programme. What happens in sleep, and why bother? The effects of sleep loss. Common sleep disorders Brief (but important ) questions.
Clinical Stream Sleep Disorders and their management Dr Alex Bartle Programme. What happens in sleep, and why bother? The effects of sleep loss. Common sleep disorders Brief (but important ) questions.
SLEEP SCREENING QUESTIONNAIRE
 SLEEP SCREENING QUESTIONNAIRE Please answer each question accurately and to the best of your knowledge, to help us obtain an accurate picture of your health and sleep issues, only this way will we be able
SLEEP SCREENING QUESTIONNAIRE Please answer each question accurately and to the best of your knowledge, to help us obtain an accurate picture of your health and sleep issues, only this way will we be able
Sleep Medicine Questionnaire
 Please bring this completed questionnaire with you to your sleep medicine appointment. Our sleep medicine staff strives to understand your sleep symptoms, which may be complex in nature. Thank you for
Please bring this completed questionnaire with you to your sleep medicine appointment. Our sleep medicine staff strives to understand your sleep symptoms, which may be complex in nature. Thank you for
Occupation: Usual Work Hours/Days: Referring Physician: Family Physician (PCP): Marital status: Single Married Divorced Widowed
: Marital status: Single Married Divorced Widowed") Name Social Security No. Last First MI Address Phone No. ( ) City State Zip Secondary No. ( ) Date of Birth Sex (M/F) Race Email County Primary Care Marital Status Single Divorced Married Widowed Employer
Name Social Security No. Last First MI Address Phone No. ( ) City State Zip Secondary No. ( ) Date of Birth Sex (M/F) Race Email County Primary Care Marital Status Single Divorced Married Widowed Employer
Humble Dreams Sleep Center. Humble, TX 77339
 Humble Dreams Sleep Center 8901 FM 1960 Bypass West, Ste. 306 Humble, TX 77339 Dear Humble Dreams Sleep Study Patient, Thank you for allowing Humble Dreams Sleep Center to provide your sleep study as requested
Humble Dreams Sleep Center 8901 FM 1960 Bypass West, Ste. 306 Humble, TX 77339 Dear Humble Dreams Sleep Study Patient, Thank you for allowing Humble Dreams Sleep Center to provide your sleep study as requested
A New, Clinically Proven Sleep Apnea Therapy for people unable to use CPAP.
 A New, Clinically Proven Sleep Apnea Therapy for people unable to use CPAP. Take Heart. If You Have OSA, You re Not Alone. Like you, more than 18 million Americans are estimated to have Obstructive Sleep
A New, Clinically Proven Sleep Apnea Therapy for people unable to use CPAP. Take Heart. If You Have OSA, You re Not Alone. Like you, more than 18 million Americans are estimated to have Obstructive Sleep
Sleep History Questionnaire
 Location South Loop Katy Steeplechase Fort Bend NAME ADDRESS PHONE SEX DOB AGE HEIGHT WEIGHT NECK COLLAR SIZE (inches) Do you have difficulty falling asleep? Is your sleep restless or disturbed? Do you
Location South Loop Katy Steeplechase Fort Bend NAME ADDRESS PHONE SEX DOB AGE HEIGHT WEIGHT NECK COLLAR SIZE (inches) Do you have difficulty falling asleep? Is your sleep restless or disturbed? Do you
WRHA Surgery Program. Obstructive Sleep Apnea (OSA)
") WRHA Surgery Program Obstructive Sleep Apnea (OSA) March 2010 Prepared by WRHA Surgery & Anesthesiology Programs Objectives 1. Define obstructive sleep apnea (OSA). 2. Purpose of the guidelines. 3. Identify
WRHA Surgery Program Obstructive Sleep Apnea (OSA) March 2010 Prepared by WRHA Surgery & Anesthesiology Programs Objectives 1. Define obstructive sleep apnea (OSA). 2. Purpose of the guidelines. 3. Identify
PEDIATRIC HISTORY FORM
 Lehigh Valley Health Network Pediatric Sleep Center PEDIATRIC HISTORY FORM Please answer the following questions frankly and accurately by filling in the blank or checking/circling the appropriate answer.
Lehigh Valley Health Network Pediatric Sleep Center PEDIATRIC HISTORY FORM Please answer the following questions frankly and accurately by filling in the blank or checking/circling the appropriate answer.
SLEEP DISORDERS CENTER QUESTIONNAIRE
 Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
Tallahassee Memorial Sleep Center Patient Questionnaire
 Tallahassee Memorial Sleep Center Patient Questionnaire Name _ Age Date Date of Birth Sex Height ft in Weight lbs Neck size inches (If known) Body Mass Index (BMI) (If known) Phone(s) (home) (work) (cell)
Tallahassee Memorial Sleep Center Patient Questionnaire Name _ Age Date Date of Birth Sex Height ft in Weight lbs Neck size inches (If known) Body Mass Index (BMI) (If known) Phone(s) (home) (work) (cell)
International Journal of Scientific & Engineering Research Volume 9, Issue 1, January ISSN
 International Journal of Scientific & Engineering Research Volume 9, Issue 1, January-2018 342 The difference of sleep quality between 2-channel ambulatory monitor and diagnostic polysomnography Tengchin
International Journal of Scientific & Engineering Research Volume 9, Issue 1, January-2018 342 The difference of sleep quality between 2-channel ambulatory monitor and diagnostic polysomnography Tengchin
Arizona Grand Medical Center 3777 Crossings Drive Prescott, AZ 86305
 Patient Information Arizona Grand Medical Center 3777 Crossings Drive Prescott, AZ 86305 Home Phone: Cell Phone: Last Name: First Name: MI Mailing Address: APT City/State/Zip Sex: Male Female Birthdate:
Patient Information Arizona Grand Medical Center 3777 Crossings Drive Prescott, AZ 86305 Home Phone: Cell Phone: Last Name: First Name: MI Mailing Address: APT City/State/Zip Sex: Male Female Birthdate:
The prevalence of daytime sleepiness in Greek adolescents in primary care
 RESEARCH ARTICLE The prevalence of daytime sleepiness in Greek adolescents in primary care Christos F. Kleisiaris 1, Maria Maniou 2, Aimilia Dragasi 3, Despoina Mitara 3, Michael Zografakis- Sfakianakis
RESEARCH ARTICLE The prevalence of daytime sleepiness in Greek adolescents in primary care Christos F. Kleisiaris 1, Maria Maniou 2, Aimilia Dragasi 3, Despoina Mitara 3, Michael Zografakis- Sfakianakis
EPWORTH SLEEPINESS SCALE
 EPWORTH SLEEPINESS SCALE Name: Sponsors last 4 of SSN#: DOB: Today s Date: Age (years): Gender (circle): MALE FEMALE How likely are you to doze off or fall asleep in the following situation, in contrast
EPWORTH SLEEPINESS SCALE Name: Sponsors last 4 of SSN#: DOB: Today s Date: Age (years): Gender (circle): MALE FEMALE How likely are you to doze off or fall asleep in the following situation, in contrast
PATIENT NAME: M.R. #: ACCT #: HOME TEL: WORK TEL: AGE: D.O.B.: OCCUPATION: HEIGHT: WEIGHT: NECK SIZE: GENDER EMERGENCY CONTACT: RELATIONSHIP: TEL:
 SLEEP DISORDERS INSTITUTE HOSPITAL: DePaul Building Street Address City, State Zip Tel: (202) 555-1212 Fax: (202) 555-1212 SLEEP QUESTIONNAIRE PATIENT NAME: M.R. #: ACCT #: STREET ADDRESS: CITY: STATE:
SLEEP DISORDERS INSTITUTE HOSPITAL: DePaul Building Street Address City, State Zip Tel: (202) 555-1212 Fax: (202) 555-1212 SLEEP QUESTIONNAIRE PATIENT NAME: M.R. #: ACCT #: STREET ADDRESS: CITY: STATE:
PEDIATRIC SLEEP EVALUATION
 PEDIATRIC SLEEP EVALUATION Directions: Please answer each of the following questions by writing in or choosing the best answer. This will help us know more about your family and your child. CHILD S INFORMATION
PEDIATRIC SLEEP EVALUATION Directions: Please answer each of the following questions by writing in or choosing the best answer. This will help us know more about your family and your child. CHILD S INFORMATION
Evaluation of Sleep Apnea and Chronic Pain Management Lauren E. Williams RN, BSN FNP-DNP Student East Carolina University
 Evaluation of Sleep Apnea and Chronic Pain Management Lauren E. Williams RN, BSN FNP-DNP Student East Carolina University 2017 NPSS Asheville, NC Background in Nursing & Pain Management Graduated with
Evaluation of Sleep Apnea and Chronic Pain Management Lauren E. Williams RN, BSN FNP-DNP Student East Carolina University 2017 NPSS Asheville, NC Background in Nursing & Pain Management Graduated with
General Information. Name Age Date of Birth. Address Apt. # City State Zip. Home Phone Work Phone. Social Security Number Marital Status
 Accredited Member Center of The American Academy of Sleep Medicine 400 Riverside Drive, Suite 1500, Bourbonnais, IL 60914 Phone (815) 933-2874 Fax (815) 939-9413 www.riversidemc.net/sleep General Information
Accredited Member Center of The American Academy of Sleep Medicine 400 Riverside Drive, Suite 1500, Bourbonnais, IL 60914 Phone (815) 933-2874 Fax (815) 939-9413 www.riversidemc.net/sleep General Information
Medical History Questionnaire
 Medical History Questionnaire OFFICE USE Patient ID: FORM DATE: / / NAME: DATE OF BIRTH: / / Allergens No known allergens Iodine Plastic Antibiotics Latex Sedatives Aspirin Local anesthetics Sleeping pills
Medical History Questionnaire OFFICE USE Patient ID: FORM DATE: / / NAME: DATE OF BIRTH: / / Allergens No known allergens Iodine Plastic Antibiotics Latex Sedatives Aspirin Local anesthetics Sleeping pills
Sleep Medicine Associates
 Date: Patient Name: DOB: Patient Height: _ Weight: _ lbs Referring Physician: Neck Size: Main Sleep Problems: 1. My main sleep complaint is: Trouble Sleeping at night Sleepy during the day Unusual behavior
Date: Patient Name: DOB: Patient Height: _ Weight: _ lbs Referring Physician: Neck Size: Main Sleep Problems: 1. My main sleep complaint is: Trouble Sleeping at night Sleepy during the day Unusual behavior
Pre-Test Questionnaire. Name: Sex: Age: Date of Birth: Height: ft. in. Weight: lbs Gain? Loss? of lbs over
 Pre-Test Questionnaire Date: Hospital # (Please Print) Name: Sex: Age: Date of Birth: Height: ft. in. Weight: lbs Gain? Loss? of lbs over Chief Complaints What problem(s) brings you to sleep disorders
Pre-Test Questionnaire Date: Hospital # (Please Print) Name: Sex: Age: Date of Birth: Height: ft. in. Weight: lbs Gain? Loss? of lbs over Chief Complaints What problem(s) brings you to sleep disorders
Programme. Why bother? The effects of sleep loss. Common Sleep Disorders, Identification and investigation Treatments
 Programme. Why bother? The effects of sleep loss. Common Sleep Disorders, Identification and investigation Treatments Brief (but important ) questions. Why bother? The three Pillars of health: - Nutrition
Programme. Why bother? The effects of sleep loss. Common Sleep Disorders, Identification and investigation Treatments Brief (but important ) questions. Why bother? The three Pillars of health: - Nutrition
PATIENT QUESTIONNAIRE Salem Sleep Medicine Please fill out completely
 PATIENT QUESTIONNAIRE Salem Sleep Medicine Please fill out completely Date: email address: First name: Middle: Last: Nickname: Ethnicity/Race (please circle): Black or African American Caucasian Hispanic
PATIENT QUESTIONNAIRE Salem Sleep Medicine Please fill out completely Date: email address: First name: Middle: Last: Nickname: Ethnicity/Race (please circle): Black or African American Caucasian Hispanic
Treatment-related changes in sleep apnea syndrome in patients with acromegaly: a prospective study
 Treatment-related changes in sleep apnea syndrome in patients with acromegaly: a prospective study Thalijn Wolters 1 *, Sean Roerink 1 *, Linda Drenthen 1, Jolanda van Haren- Willems 2, Guido van den Broek
Treatment-related changes in sleep apnea syndrome in patients with acromegaly: a prospective study Thalijn Wolters 1 *, Sean Roerink 1 *, Linda Drenthen 1, Jolanda van Haren- Willems 2, Guido van den Broek
Maintenance for Wakefulness Testing (MWT)
") Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness Testing (MWT) will begin on the morning of at 7 a.m. and will end at 5 p.m. ARRIVAL TIME: If you are not able to arrive
Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness Testing (MWT) will begin on the morning of at 7 a.m. and will end at 5 p.m. ARRIVAL TIME: If you are not able to arrive
The Epworth Sleepiness Scale (ESS), which asks an individual
, which asks an individual") Scientific investigations The Epworth Score in African American Populations Amanda L. Hayes, B.S. 1 ; James C. Spilsbury, Ph.D., M.P.H. 2 ; Sanjay R. Patel, M.D., M.S. 1,2 1 Division of Pulmonary, Critical
Scientific investigations The Epworth Score in African American Populations Amanda L. Hayes, B.S. 1 ; James C. Spilsbury, Ph.D., M.P.H. 2 ; Sanjay R. Patel, M.D., M.S. 1,2 1 Division of Pulmonary, Critical