Guideline for Adult Insomnia
|
|
|
- Mark O’Brien’
- 5 years ago
- Views:
Transcription
1 Guideline for Adult Insomnia
2 Exclusions This guideline does not apply to: Children under the age of 18 Pregnant and lactating women Geriatric patients: While the general principles of the diagnosis and management of primary insomnia apply to all adult patients it is important to note that late life insomnia requires specific interventions not addressed in this guideline. Definitions 1. Acute Insomnia: Duration of 4 weeks or less 2. Chronic Insomnia: Duration of 4 weeks or more 3. Primary Sleep Disorder: A primary or intrinsic sleep disorder is one that arises out of the physiological processes of sleep. Examples of primary sleep disorders are obstructive sleep apnea, restless legs syndrome, periodic limb
3 movement disorder or parasomnias. 4. Secondary Insomnia: Secondary insomnia refers to difficulty initiating and/ or maintaining sleep that occurs as a result of or co-morbidly in conjunction with a medical, psychiatric or psychological process. Examples of secondary insomnia include: pain associated with rheumatoid arthritis that disrupts initiation and/ or maintenance of sleep, insomnia co-morbidly associated with a major depressive episode, or insomnia associated with an acute emotional stressor. 5. Primary Insomnia (also known as psychophysiologic insomnia (PPI): A disorder of somatized tension and learned sleep preventing associations that results in a complaint of insomnia and consequent daytime impairment. The conditioned negative associations regarding sleep tend to perpetuate the insomnia and are exacerbated by the patient s obsessive concern about their sleep.
4 6. Daytime Impairment: The daytime consequences of insomnia include: dysphoric states such as irritability, impaired cognition such as poor concentration and memory, and daytime fatigue. The daytime consequences of insomnia must have a substantial effect on the individual s quality of life to be considered significant. Recommendations 1. Acute Insomnia - Identify and address trigger(s) - Consider short-term pharmacotherapy with a sedative to prevent a chronic insomnia (nightly sedation for < 7 nights) - Address sleep hygiene issues and advice 2. Chronic Insomnia (see definitions) a. Without daytime impairment (refer to algorithm for management) b. With daytime impairment (refer to algorithm for management)
5 3. Primary Sleep Disorder (refer to algorithm for management) 4. Secondary Sleep Disorder (refer to algorithm for information) 5. Primary insomnia (refer to algorithm. Refer to the Alberta Clinical Practice Guideline:Adult Conditioned Insomnia Diagnosis to Management) PRACTICE POINT Successful management of the patient with primary insomnia is a function of appropriate guidance, advice and reassurance. Regular, brief follow-up visits at 2-4 week intervals to assess compliance, adherence and response to recommendations and pharmacotherapy provides the clinician with an accurate evaluation of the patient s motivation to manage THEIR problem.
6 Red Flags Major depressive episode Generalized anxiety or panic disorder Excessive daytime sleepiness (unexpected or irresistible sleepiness) resulting in imminent risk to the patient and/or society Substance abuse

7 Insomnia Screening Questionnaire: Insomnia Diagnosis
8 The Insomnia Screening Questionnaire is a screening tool used to guide the physician in the clinical evaluation of insomnia. It is used to screen for a primary sleep disorder as indicated in the Insomnia Algorithm. Based on the general rules below the physician should perform a more detailed clinical evaluation and/or refer where he/ she feels it is appropriate. Diagnostic Domains: 1) Insomnia: Q1-6 2) Psychiatric Disorders: Q7-10 3) Circadian Rhythm Disorder: Q11 4) Movement Disorders: Q ) Parasomnias Q14 6) Sleep Disordered Breathing (Sleep Apnea): Q15-17
9 General Guidelines for interpretation of the insomnia screening questionnaire: 1) Patients who answer 3, 4 or 5 on any question likely suffer from insomnia. If they answer 3, 4 or 5 to two or more items and have significant daytime impairment the insomnia requires further evaluation and management. If there is no evidence of a primary sleep disorder and/or no identifiable secondary cause of insomnia, this is conditioned insomnia. 2) Patients who answer 4 or 5 on Questions 6-9 should be further screened for psychiatric disorders as you would in your practice. Question 9 refers to somatization which is commonly associated with insomnia and may reflect an underlying somatoform disorder which requires specific treatment.
10 3) Patients who answer 4 or 5 on question 11 likely have a circadian rhythm disorder. Further questioning about shift work or a preference for a delayed sleep phase should be done. 4) An answer of 4 or 5 on either item is significant and likely contributing to the patient s symptoms of insomnia or nonrestorative sleep. Question 12 refers to restless legs syndrome and question 13 refers to periodic limb movement disorder. 5) An answer of 2-5 on question 14 should raise concern especially if the event or move-ment is violent or potentially injurious to the patient or bed partner. 6) Answering 4 or 5 on item 15 or 16 alone requires further clinical evaluation for sleep apnea. An answer of above 3 on questions 15 and 16 or 15 and 17 is also suspicious for sleep apnea and further evaluation should be done.
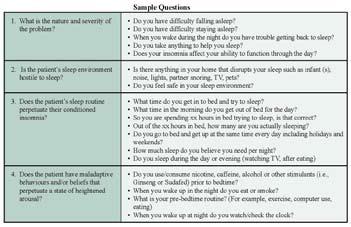
11 Primary Insomnia Evaluation The primary insomnia evaluation provides the clinician with a structured approach to the clinical evaluation of the patient s sleep. The sample questions can be used to characterize those aspects of the patients sleep behavior that contribute to the insomnia.
12
13 Primary Insomnia Management Recommendations The management of primary insomnia is based on the foundation of behavioural and cognitive non-pharmacologic strategies. Pharmacolo `gic interventions are adjunctive to the nonpharmacologic strategies. Adjunctive pharmacotherapy is used on a short-term (less than 7 to 14 days on a nightly basis) or intermittent (2-3 nights per week) for the sole purpose of preventing an exacerbation of the primary insomnia The patient must be an active participant in treatment process. Primary insomnia is a chronic illness that requires regular followup and monitoring to evaluate the patient s response to treatment and motivation to resolve the problem The goal of management is to provide the patient with the tools necessary to manage the chronic nature of the illness and minimize dependence on sedative medications.
14 Non-pharmacologic Non-pharmacologic therapies are effective in the management of primary insomnia especially when behavioural and cognitive techniques are used in combination. Behavioural techniques include sleep hygiene, sleep consolidation, stimulus control, and relaxation therapies. Cognitive techniques include cognitive behavioural therapy (CBT). Behavioural Therapies Sleep hygiene The following recommendations should be individualized to address patient needs/situation. PRACTICE POINT Initially, review of sleep behaviors and sleep hygiene advice with recommendations to adhere strictly to the principles of sleep hygiene will providea the clinician with an indication of the patient s motivation to change the behaviors that are perpetuating the insomnia.
15 Sleep Hygiene Advice: Avoid caffeine after lunch and alcohol within 6 hours of bedtime Avoid nicotine close to bedtime or during the night Engage in moderate physical activity but avoid heavy exercise within 3 hours of bedtime Avoid consuming excessive liquids or a heavy evening meal before bedtime Maintain a quiet, dark, safe, and comfortable sleep environment. Minimize noise and light Avoid a bedroom that is too hot or too cold Avoid watching/checking the clock
16 PRACTICE POINT Educate the patient about the following issues: Alcohol helps with sleep initiation, it impairs sleep maintenance and can exacerbate other sleep disorders Nicotine is a potent stimulant with a short half-life that induces awakenings as a result of withdrawal during the sleep period Smoking cessation aids (nicotine replacement products and bupropion) can cause insomnia Sleep consolidation Some insomnia patients spend excessive time in bed trying to attain more sleep. Sleep consolidation is accomplished by compressing the total time in bed to match the total sleep need of the patient. This improves the sleep efficiency.
17 Devise a sleep prescription with the patient: a fixed bedtime and wake time Determine the average total sleep time Prescribe the time in bed to current total sleep time plus 30 minutes The minimum sleep time should be no less than 5 hours. Set a consistent wake time (firmly fixed 7 days/ week) The bed time is determined by counting backwards from the fixed wake time (For example: a patient estimates the total sleep time to be 5-6 hours/night, the total time in bed is 8 hours/night for a sleep efficiency of 5.5/8 = 68%. The prescribed total sleep time would be hours/night, if the wake time is 6AM then the prescribed bedtime is 11-11:30 PM) For the first 2-4 weeks these times should remain consistent and the clinician should monitor the patients adherence to the program with sleep logs (see sleep log attachment)
18 Advise the patient that napping will reduce the depth and restorative quality of sleep the following night Once the patient is sleeping for >85 to 90 percent of the time spent in bed for two consecutive weeks, then the amount of time spent in bed is slowly increased by minute every week. If sleep efficiency of 90 percent is maintained, then therapy is successful. The average total sleep time for most people is between 6 and 8 hours a night. PRACTICE POINT Advise patients that the goal of treatment is to improve the continuity and restorative quality of sleep, not to make them 8-hour sleepers. More often than not the total sleep time will be less than 8 hours per night. Advise patients that they may suffer from daytime sleepiness in the initiation phase of compressing their sleep schedule
19 Stimulus control Stimulus control is designed to re-associate the bed/bedroom with sleep and to re-establish a consistent sleep-wake schedule. This is achieved by limiting activities that serve as cues for staying awake. The treatment consists of the following behavioural instructions: Eliminate non-sleep activities in the bedroom. Remove the TV and computer from the bedroom Use the bed and bedroom only for sleep and sex Go to bed only when sleepy, even if later than prescribed sleep schedule Get out of bed if not able to sleep within minutes - go to another room and relax. Return to bed only when sleepy Set alarm for agreed upon wake time Avoid excessive napping during the day - a brief nap (15-30 minutes) during the mid-
20 afternoon can be refreshing and is unlikely to disrupt nocturnal sleep. Anxiety Reducing Strategies and Relaxation therapies Relaxation therapy is designed to reduce physiological and psychological arousal to promote sleep. Recommended relaxation therapies must be individualized and include: Avoid arousing activities before bed (late night phone calls, work, watching TV Designate at least one hour before bedtime to help unwind from the day s stresses - dim light exposure and engage in relaxing activities Relaxation techniques such as deep breathing, light exercise, stretching, yoga and relaxation CDs can help promote sleep Stress management skills training and relaxation therapies such as progressive muscle relaxation, biofeedback, hypnosis,
21 meditation, imagery training, are usually provided by a trained professional (through books, videos, or face-to-face sessions Techniques for managing worry can be useful for some patients. This may include keeping a worry journal, scheduling worry time, challenging worried thinking, or seeking professional help Cognitive Therapies Cognitive behavioral therapy (CBT) CBT addresses the inappropriate beliefs and attitudes that perpetuate the insomnia. The goal of this technique/process is to identify dysfunctional sleep cognitions, challenge the validity of those cognitions, and replace those beliefs and attitudes with more appropriate and adaptive cognitions. Common faulty beliefs and expectations that can be modified include: Unrealistic sleep expectations (e.g., I need to have 9 hours of sleep each night )
22 Misconceptions about the causes of insomnia (e.g., I have a chemical imbalance causing my insomnia ) Amplifying the consequences (e.g., I cannot do anything after a bad night s sleep ) Performance anxiety and loss of control over ability to sleep (e.g., I am afraid of losing control over my ability to sleep ) Pharmacologic Pharmacotherapy should be considered an adjunctive therapy to cognitive and behavioural therapies in the comprehensive management of primary insomnia.
23 Principles of Treatment Pharmacotherapy is generally recommended at the lowest effective dose as short-term treatment lasting less than 7 days. Although long-term use of hypnotic agents is discouraged due to the potential for tolerance and dependence, there are specific situations and circumstances under which long term use of hypnotics may be appropriate. Short term (<7 consecutive nights): - Initially used to break the cycle of chronic insomnia and allow the patient to adapt to cognitive and behavioural interventions - Used to manage an exacerbation of previously controlled primary insomnia Long term intermittent (self administered therapy to decrease arousal and prevent relapse): - Used on a limited PRN basis (<3 times/ week) for occasional bouts of insomnia - Used on a scheduled basis (i.e., <3 times/ week) to ensure consistent adequate sleep
24 in a patient with chronic primary insomnia where the goal of therapy is to prevent relapse Therapeutic Options First-line Pharmacotherapy: Highest level of evidence supporting efficacy and safety Agents Recommended Dose Comments Zopiclone 3.75k-7.5 mg Short half-life provides lower risk of morning hang-over effect Metallic aftertaste most common adverse reaction Temazepam mg Intermediate half-life carries a low-moderate risk of morning hang-over effect
25 Second-line Pharmacotherapy: Moderate level of formal evidence. Extent of current use and favorable tolerability support use as second-line agents Trazodone mg Shorter half-life carries lower risk of morning hang-over effect Variable Evidence L Tryptophan 500 mg-2 gm Evidence supporting efficacy is Melatonin mg variable and insufficient. May be requested by individual patients Valerian mg looking for a natural source agent. Taken 60 minutes before bedtime
26 Diphenhydramine - Benadryl - Sleep Eze - Simply Sleep - Nytol - Unisom Dimenhydrinate - Gravol Doxylamine - Unisom 2 Other Non-Prescription Products Usual Dose mg hs Potential for serious side effects arising from anticholinergic properties (especially in elderly); residual daytime sleepiness, diminished cognitive function, dry mouth, blurred vision, constipation, urinary retention, etc mg hs mg hs These products are not intended for long term use and tolerance to sedative effects likely develops rapidly (3 days) Gravol not approved in Canada as a sleep aid
27 Not Recommended The following agents are not recommended for the management of conditioned insomnia except in cases where the agent is being used specifically to mange a co-morbidity such as depression. Antidepressants - mirtazapine, fluvoxamine, tricyclics Relative lack of evidence Amitriptyline Relative lack of evidence and significant adverse effects (such as weight gain) Antihistamines - chlorpheniramine Relative lack of evidence or excessive risk of daytime sedation, psychomotor impairment andanticholinergic toxicity Antipsychotics (Conventional or 1st-Generation) - chlorpromazine, methotrimeprazine, loxapine Relative lack of evidence and unacceptable risk of anticholinergic and neurological toxicity Antipsychotics (Atypical or 2nd-Generation) - risperidone, olanzapine, quetiapine Relative lack of evidence and unacceptable cost and risk of metabolic toxicity
28 PRACTICE POINT The foundation of the management of conditioned insomnia is behavioural and cognitive therapy. Ongoing evaluation of the patient s motivation to adhere to the behavioral and cognitive strategies is an important part of monitoring the patient s progress. Adherence to, and compliance with these strategies is usually effective and minimizes the potential for dependence on medication.
29 First Visit Prescribe behavioral and cognitive interventions Use sleep logs and diaries to monitor the patient s progress (see sleep log attachment) Consider pharmacotherapy based on the patient s sense of urgency, need for relief and willingness (motivation) to follow the behavioral and cognitive recommendations. FOLLOW-UP AT 2 4 WEEKS Evaluate sleep efficiency and daytime symptoms Reinforce behavioral interventions\ Review or reconsider pharmacotherapy 3 MONTH FOLLOW-UP If there is no progress or limited improvement referral to sleep medicine program or psychologist may be warranted
ADULT PRIMARY INSOMNIA
 Clinical Practice Guideline Adult Primary Insomnia: Diagnosis to Management 2007 Update This guideline was developed by a Clinical Practice Guidelines Working Group to assist physicians in the management
Clinical Practice Guideline Adult Primary Insomnia: Diagnosis to Management 2007 Update This guideline was developed by a Clinical Practice Guidelines Working Group to assist physicians in the management
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia
 Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Chronic Insomnia: DSM - V. Insomnia DSM - V. Patient Symptoms. Insomnia: Assessment and Overview of Management. Insomnia Management in the Digital Age
 Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Dr Alex Bartle. Sleep Well Clinic
 Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Treating Insomnia in Primary Care. Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team
 Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Insomnia % of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences)
") 10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
 COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
Insomnia. F r e q u e n t l y A s k e d Q u e s t i o n s
 Insomnia Q: What is insomnia? A: Insomnia is a common sleep disorder. If you have insomnia, you may: Lie awake for a long time and have trouble falling asleep Wake up a lot and have trouble returning to
Insomnia Q: What is insomnia? A: Insomnia is a common sleep disorder. If you have insomnia, you may: Lie awake for a long time and have trouble falling asleep Wake up a lot and have trouble returning to
WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT
 WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT Kristin E. Eisenhauer, PhD. Trinity University San Antonio, Texas I
WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT Kristin E. Eisenhauer, PhD. Trinity University San Antonio, Texas I
Insomnia. Dr Terri Henderson MBChB FCPsych
 Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
Insomnia treatment. Sleep hygiene education sleep hygiene teaches good sleeping habits. This includes:
 Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Sleep and Ageing. Siobhan Banks PhD. Body and Brain at Work, Centre for Sleep Research University of South Australia
 Sleep and Ageing Siobhan Banks PhD Body and Brain at Work, Centre for Sleep Research University of South Australia Health and Active Ageing, 22 nd September 2015 Sleep and Aging How does sleep change as
Sleep and Ageing Siobhan Banks PhD Body and Brain at Work, Centre for Sleep Research University of South Australia Health and Active Ageing, 22 nd September 2015 Sleep and Aging How does sleep change as
INDEX. Group psychotherapy, described, 97 Group stimulus control, 29-47; see also Stimulus control (group setting)
") Index Abdominal breathing, 70; see also Breathing; Relaxation therapy Activation, sleep drive/responsivity, 6-9 Age level; see also Elderly circadian rhythms and, 68-69 delayed sleep phase syndrome and,
Index Abdominal breathing, 70; see also Breathing; Relaxation therapy Activation, sleep drive/responsivity, 6-9 Age level; see also Elderly circadian rhythms and, 68-69 delayed sleep phase syndrome and,
 Sleep This factsheet is available in a downloadable PDF here. Table of Contents Introduction Insomnia How Long does Insomnia Last? How much Sleep should You get? Symptoms of Insomnia Causes of Insomnia
Sleep This factsheet is available in a downloadable PDF here. Table of Contents Introduction Insomnia How Long does Insomnia Last? How much Sleep should You get? Symptoms of Insomnia Causes of Insomnia
INSOMNIAS. Stephan Eisenschenk, MD Department of Neurology
 INSOMNIAS INSOMNIAS General criteria for insomnia A. Repeated difficulty with sleep initiation, duration, consolidation or quality. B. Adequate sleep opportunity, persistent sleep difficulty and associated
INSOMNIAS INSOMNIAS General criteria for insomnia A. Repeated difficulty with sleep initiation, duration, consolidation or quality. B. Adequate sleep opportunity, persistent sleep difficulty and associated
Facts about Sleep. Circadian rhythms are important in determining human sleep patterns/ sleep-waking cycle
 Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
A GUIDE TO BETTER SLEEP. Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions
 A GUIDE TO BETTER SLEEP Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions A GUIDE TO BETTER SLEEP Good sleep is one of life s pleasures. Most people can think of a time when they slept
A GUIDE TO BETTER SLEEP Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions A GUIDE TO BETTER SLEEP Good sleep is one of life s pleasures. Most people can think of a time when they slept
Faculty/Presenter Disclosure
 A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
YOU REALLY NEED TO SLEEP: Several methods to improve your sleep
 YOU REALLY NEED TO SLEEP: Several methods to improve your sleep Sleep is essential to our well-being. When humans fail to get good sleep over a period of time, numerous problems can occur. CAN T SLEEP!!
YOU REALLY NEED TO SLEEP: Several methods to improve your sleep Sleep is essential to our well-being. When humans fail to get good sleep over a period of time, numerous problems can occur. CAN T SLEEP!!
Cognitive Behavioral Therapy for Insomnia. Melanie K. Leggett, PhD, CBSM Duke University Medical Center
 Cognitive Behavioral Therapy for Insomnia Melanie K. Leggett, PhD, CBSM Duke University Medical Center Disclosures I have no relevant financial relationship with the manufacturers of any commercial products
Cognitive Behavioral Therapy for Insomnia Melanie K. Leggett, PhD, CBSM Duke University Medical Center Disclosures I have no relevant financial relationship with the manufacturers of any commercial products
Sleep and Parkinson's Disease
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
RECIPES FOR A GOOD NIGHT S SLEEP
 RECIPES FOR A GOOD NIGHT S SLEEP Maribeth Gallagher, PMHNP-BC, MS Hospice of the Valley Objectives: Describe the most common changes in sleep that occur in older adults. Discuss the possible negative effects
RECIPES FOR A GOOD NIGHT S SLEEP Maribeth Gallagher, PMHNP-BC, MS Hospice of the Valley Objectives: Describe the most common changes in sleep that occur in older adults. Discuss the possible negative effects
AGING CHANGES IN SLEEP
 OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
Sleep and Traumatic Brain Injury (TBI)
") Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Managing Insomnia Disorder A Review of the Research for Adults
 Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
How to Manage Insomnia with and without medications
 How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
CPT David Shaha, MC US Army
 CPT David Shaha, MC US Army None Thoughts and comments are my own and do not represent the official policy of the Department of the Army, Department of Defense, or United States Government. Clinical Case
CPT David Shaha, MC US Army None Thoughts and comments are my own and do not represent the official policy of the Department of the Army, Department of Defense, or United States Government. Clinical Case
Counter Control Instructions University of North Carolina Hospitals Sleep Disorders Center
 Counter Control Instructions 1. Stay in bed during the appropriated time period whether you are able to fall asleep or not. From to 2. Spend thirty minutes each day in the bed performing work, reading
Counter Control Instructions 1. Stay in bed during the appropriated time period whether you are able to fall asleep or not. From to 2. Spend thirty minutes each day in the bed performing work, reading
6/3/2015. Insomnia An Integrative Approach. Objectives. Why An Integrative Approach? Integrative Model. Definition. Short-term Insomnia
 Insomnia An Integrative Approach Jeffrey S. Jump, M.D. Medical Director CHI Memorial Integrative Medicine Associates Objectives Understand the importance of sleep to health Identify patients with insomnia
Insomnia An Integrative Approach Jeffrey S. Jump, M.D. Medical Director CHI Memorial Integrative Medicine Associates Objectives Understand the importance of sleep to health Identify patients with insomnia
일차진료에서불면증치료 김종우. Primary Insomnia : DSM-IV criteria 경희대학교의과대학정신과학교실 MEMO. Diagnostic Criteria for Insomnia (ICSD-2) 개원의와함께하는임상강좌
 개원의와함께하는임상강좌") 개원의와함께하는임상강좌 2011 일차진료에서불면증치료 경희대학교의과대학정신과학교실 김종우 Diagnostic Criteria for Insomnia (ICSD-2) International Classification of Sleep Disorders, 2nd Edition (ICSD-2) Primary Insomnia : DSM-IV criteria A. The
개원의와함께하는임상강좌 2011 일차진료에서불면증치료 경희대학교의과대학정신과학교실 김종우 Diagnostic Criteria for Insomnia (ICSD-2) International Classification of Sleep Disorders, 2nd Edition (ICSD-2) Primary Insomnia : DSM-IV criteria A. The
Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment
 Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment Session 1: Introduction and sleep assessment -Assess sleep problem (option: have client complete 20-item sleep questionnaire).
Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment Session 1: Introduction and sleep assessment -Assess sleep problem (option: have client complete 20-item sleep questionnaire).
Insomnia. St. Joseph s Annual Family Practice Refresher March 1, Robert J. Ostrander, M.D
 St. Joseph s Annual Family Practice Refresher March 1, 2018 Robert J. Ostrander, M.D If in bed I say, When shall I arise? then the night drags on; I am filled with restlessness until the dawn. Job 7:4
St. Joseph s Annual Family Practice Refresher March 1, 2018 Robert J. Ostrander, M.D If in bed I say, When shall I arise? then the night drags on; I am filled with restlessness until the dawn. Job 7:4
Introduction. v Insomnia is very prevalent in acute (30-50%) and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders.
 and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders.") Introduction v Insomnia is very prevalent in acute (30-50%) and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders. v Insomnia is a risk factor for psychiatric and medical
Introduction v Insomnia is very prevalent in acute (30-50%) and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders. v Insomnia is a risk factor for psychiatric and medical
Article printed from
 What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
MMG003 GUIDELINES FOR THE USE OF HYPNOTICS FOR THE TREATMENT OF INSOMNIA
 MMG003 GUIDELINES FOR THE USE OF HYPNOTICS FOR THE TREATMENT OF INSOMNIA Page 1 of 11 Table of Contents Why we need this Guideline... 3 What the Policy is trying to do... 3 Which stakeholders have been
MMG003 GUIDELINES FOR THE USE OF HYPNOTICS FOR THE TREATMENT OF INSOMNIA Page 1 of 11 Table of Contents Why we need this Guideline... 3 What the Policy is trying to do... 3 Which stakeholders have been
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
RESTore TM. Clinician Manual for Single User. Insomnia and Sleep Disorders. A step by step manual to help you guide your clients through the program
 RESTore TM Insomnia and Sleep Disorders Clinician Manual for Single User A step by step manual to help you guide your clients through the program Version 10 July, 2016 Table of Contents Introduction...
RESTore TM Insomnia and Sleep Disorders Clinician Manual for Single User A step by step manual to help you guide your clients through the program Version 10 July, 2016 Table of Contents Introduction...
Healthy Sleep Tips Along the Way!
 Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
The Reasons for Insomnia and the Ways to Fight It
 The Reasons for Insomnia and the Ways to Fight It Insomnia is a relatively common sleep disorder, which is indicated by insufficient duration or unsatisfactory quality of sleep over an extended period.
The Reasons for Insomnia and the Ways to Fight It Insomnia is a relatively common sleep disorder, which is indicated by insufficient duration or unsatisfactory quality of sleep over an extended period.
Improving Sleep: Promoting Sleep Hygiene Techniques
 University of Vermont ScholarWorks @ UVM Family Medicine Clerkship Student Projects College of Medicine 2018 Improving Sleep: Promoting Sleep Hygiene Techniques Katherine Clifford University of Vermont
University of Vermont ScholarWorks @ UVM Family Medicine Clerkship Student Projects College of Medicine 2018 Improving Sleep: Promoting Sleep Hygiene Techniques Katherine Clifford University of Vermont
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
SLEEP-WAKE DISORDERS: INSOMNIA. Prof. Paz Gía-Portilla
 SLEEP-WAKE DISORDERS: INSOMNIA Prof. Paz Gía-Portilla SLEEP-WAKE DISORDERS AND ICD-10 Chapter V: Mental and Behavioural Disorders F51. Non-organic sleep disorders Chapter VI: Nervous System Illnesses G47.
SLEEP-WAKE DISORDERS: INSOMNIA Prof. Paz Gía-Portilla SLEEP-WAKE DISORDERS AND ICD-10 Chapter V: Mental and Behavioural Disorders F51. Non-organic sleep disorders Chapter VI: Nervous System Illnesses G47.
Cognitive-Behavioral Therapy for Insomnia
 Wisconsin Department of Health Services Wisconsin Public Psychiatry Network Teleconference (WPPNT) This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau of Prevention,
Wisconsin Department of Health Services Wisconsin Public Psychiatry Network Teleconference (WPPNT) This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau of Prevention,
Insomnia treatment in primary care
 Insomnia treatment in primary care Daniel J. Buysse, MD UPMC Professor of Sleep Medicine Professor of Psychiatry and Clinical and Translational Science University of Pittsburgh School of Medicine buyssedj@upmc.edu
Insomnia treatment in primary care Daniel J. Buysse, MD UPMC Professor of Sleep Medicine Professor of Psychiatry and Clinical and Translational Science University of Pittsburgh School of Medicine buyssedj@upmc.edu
A good night s sleep
 A good night s sleep Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm A good night
A good night s sleep Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm A good night
Sleep Disorders. Guidance for Primary Care. National Advisory Group for Respiratory Managed Clinical Networks
 Sleep Disorders Guidance for Primary Care National Advisory Group for Respiratory Managed Clinical Networks Presentation Patient complaining of difficulty sleeping, ongoing fatigue, poor concentration
Sleep Disorders Guidance for Primary Care National Advisory Group for Respiratory Managed Clinical Networks Presentation Patient complaining of difficulty sleeping, ongoing fatigue, poor concentration
Parkinson s disease: & related sleep disorders
 Parkinson s disease: & related sleep disorders PFNCA Symposium March 24 2018 Zahra N Rezvani MD, PhD University of Maryland I have no financial interest with any entity producing marketing, re-selling,
Parkinson s disease: & related sleep disorders PFNCA Symposium March 24 2018 Zahra N Rezvani MD, PhD University of Maryland I have no financial interest with any entity producing marketing, re-selling,
Sleep Hygiene. William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA
 Sleep Hygiene William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA Why Is Sleep Important? Symptoms of Sleep Deprivation: Irritability / Poor Stress
Sleep Hygiene William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA Why Is Sleep Important? Symptoms of Sleep Deprivation: Irritability / Poor Stress
8/29/2013. Discuss Relation of Fatigue to Sleep Disturbance. Assessing and Treating Factors Contributing to Fatigue and Sleep Disturbance
 Timothy Pearman, Ph.D. Director, Supportive Oncology Robert H. Lurie Comprehensive Cancer Center Associate Professor of Medical Social Sciences and Psychiatry Northwestern University Feinberg School of
Timothy Pearman, Ph.D. Director, Supportive Oncology Robert H. Lurie Comprehensive Cancer Center Associate Professor of Medical Social Sciences and Psychiatry Northwestern University Feinberg School of
Reference document. Sleep disorders
 Reference document Sleep disorders Table of contents Introduction 2 Definition 2 Myths 2 Major determinants 2 Major sleep disorders 3 The consequences of sleep deprivation 3 Tips for better sleep 4 Conclusion
Reference document Sleep disorders Table of contents Introduction 2 Definition 2 Myths 2 Major determinants 2 Major sleep disorders 3 The consequences of sleep deprivation 3 Tips for better sleep 4 Conclusion
Dr Alex Bartle. Director Sleep Well Clinic
 Dr Alex Bartle Director Sleep Well Clinic 1 Fatigue in the Workforce The structure of sleep Fatigue and sleep Consequences of fatigue Management of Shiftwork Conclusion Sleep Architecture REM NREM Rapid
Dr Alex Bartle Director Sleep Well Clinic 1 Fatigue in the Workforce The structure of sleep Fatigue and sleep Consequences of fatigue Management of Shiftwork Conclusion Sleep Architecture REM NREM Rapid
Sleep and Students. John Villa, DO Medical Director
 Sleep and Students John Villa, DO Medical Director Objectives: Importance and Benefits of Sleep States and Stages of the Sleep Cycle Sleep Needs, Patterns and Characteristics for All Ages Healthy Sleep
Sleep and Students John Villa, DO Medical Director Objectives: Importance and Benefits of Sleep States and Stages of the Sleep Cycle Sleep Needs, Patterns and Characteristics for All Ages Healthy Sleep
SLEEP HISTORY QUESTIONNAIRE
 Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Modern Management of Sleep Disorders. If Only I Could Sleep Like I Did Before
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Contents. Page. Can t sleep 3. Insomnia 4. Sleep 5. How long should we sleep? 8. Sleep problems 9. Getting a better night s sleep 11
 I Cannot Sleep Contents Page Can t sleep 3 Insomnia 4 Sleep 5 How long should we sleep? 8 Sleep problems 9 Getting a better night s sleep 11 Treatment for insomnia 15 For more information 19 2 Can t sleep
I Cannot Sleep Contents Page Can t sleep 3 Insomnia 4 Sleep 5 How long should we sleep? 8 Sleep problems 9 Getting a better night s sleep 11 Treatment for insomnia 15 For more information 19 2 Can t sleep
HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS. To educate participants regarding the sleep wake cycle.
 HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS Talk about the relationship between depression, sleep, and health problems. To educate participants regarding the sleep wake cycle. To provide
HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS Talk about the relationship between depression, sleep, and health problems. To educate participants regarding the sleep wake cycle. To provide
RECOMMENDATIONS. TARGET POPULATION Adults. EXCLUSIONS Children under the age of 18 years Overnight/rotating shift workers
 ASSESSMENT TO MANAGEMENT OF ADULT INSOMNIA Clinical Practice Guideline December 2015 OBJECTIVE Clinicians in Alberta will know how to assess and diagnose insomnia; when insomnia can be effectively treated
ASSESSMENT TO MANAGEMENT OF ADULT INSOMNIA Clinical Practice Guideline December 2015 OBJECTIVE Clinicians in Alberta will know how to assess and diagnose insomnia; when insomnia can be effectively treated
OBJECTIVES. The psychiatric, medical, and neurologic causes of sleep problems. Office-based and objective methods of evaluating sleep
 SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
Question #1. Disclosures. CAPA 2015 Annual Conference. All of the following occur as we get older EXCEPT: Evaluating Patients with Insomnia
 Evaluating Patients with Roger D. Seheult, M.D. Pulmonary Critical Care Physician - Beaver Medical Group, Redlands California Assistant Clinical Professor of Medicine - Loma Linda University School of
Evaluating Patients with Roger D. Seheult, M.D. Pulmonary Critical Care Physician - Beaver Medical Group, Redlands California Assistant Clinical Professor of Medicine - Loma Linda University School of
John McLachlan. Clinical Lead Pulmonary Physiology & Sleep Medicine. President Elect, WA Branch Thoracic Society of Australia & NZ
 John McLachlan Respiratory & Sleep Physician @FSH Clinical Lead Pulmonary Physiology & Sleep Medicine Sleep Physician x 27 years Interest in Insomnia management President Elect, WA Branch Thoracic Society
John McLachlan Respiratory & Sleep Physician @FSH Clinical Lead Pulmonary Physiology & Sleep Medicine Sleep Physician x 27 years Interest in Insomnia management President Elect, WA Branch Thoracic Society
Objectives. Types of Sleep Problems in Developmental Disorders
 Objectives Sleep Problems in the Child with Neurodevelopmental Disorders AACPDM September 11, 2014 BRK-3 Golda Milo-Manson MD, MHSc, FRCP(C) Holland Bloorview Kids Rehabilitation Hospital Toronto, Canada
Objectives Sleep Problems in the Child with Neurodevelopmental Disorders AACPDM September 11, 2014 BRK-3 Golda Milo-Manson MD, MHSc, FRCP(C) Holland Bloorview Kids Rehabilitation Hospital Toronto, Canada
Get on the Road to Better Health Recognizing the Dangers of Sleep Apnea
 Get on the Road to Better Health You Will Learn About The importance and benefits of sleep Sleep deprivation and its consequences The prevalence, symptoms, and treatments for major sleep problems/ disorders
Get on the Road to Better Health You Will Learn About The importance and benefits of sleep Sleep deprivation and its consequences The prevalence, symptoms, and treatments for major sleep problems/ disorders
Emergency Contact Information Name: Phone: Address: Employer Information Employer Name: Address/Street: City: Zip: Phone: Fax:
 SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER
 Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER Disclosure: Financial - none Non-Financial - none Selected Topics Sleep epidemiology Sleep
Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER Disclosure: Financial - none Non-Financial - none Selected Topics Sleep epidemiology Sleep
May 27, Gosia Eve Phillips, MD
 May 27, 2015 Gosia Eve Phillips, MD Diplomate, American Board of Psychiatry and Neurology Assistant Professor of Medicine, Dalhousie University Medical Director, MedSleep Atlantic >50% of MS patients suffer
May 27, 2015 Gosia Eve Phillips, MD Diplomate, American Board of Psychiatry and Neurology Assistant Professor of Medicine, Dalhousie University Medical Director, MedSleep Atlantic >50% of MS patients suffer
PATIENT NAME: M.R. #: ACCT #: HOME TEL: WORK TEL: AGE: D.O.B.: OCCUPATION: HEIGHT: WEIGHT: NECK SIZE: GENDER EMERGENCY CONTACT: RELATIONSHIP: TEL:
 SLEEP DISORDERS INSTITUTE HOSPITAL: DePaul Building Street Address City, State Zip Tel: (202) 555-1212 Fax: (202) 555-1212 SLEEP QUESTIONNAIRE PATIENT NAME: M.R. #: ACCT #: STREET ADDRESS: CITY: STATE:
SLEEP DISORDERS INSTITUTE HOSPITAL: DePaul Building Street Address City, State Zip Tel: (202) 555-1212 Fax: (202) 555-1212 SLEEP QUESTIONNAIRE PATIENT NAME: M.R. #: ACCT #: STREET ADDRESS: CITY: STATE:
Littleton, CO Welcome Packet 8151 Southpark Lane, Suite 200 Littleton, CO 80120
 Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Session 5. Bedtime Relaxation Techniques and Lifestyle Practices for Improving Sleep
 Session 5 Bedtime Relaxation Techniques and Lifestyle Practices for Improving Sleep Lesson 1: Relaxation Techniques at Night and Lifestyle Practices That Improve Sleep Using Relaxation Techniques to Aid
Session 5 Bedtime Relaxation Techniques and Lifestyle Practices for Improving Sleep Lesson 1: Relaxation Techniques at Night and Lifestyle Practices That Improve Sleep Using Relaxation Techniques to Aid
Sleep Self-Assessment
 We are pleased you are taking the time to become more aware of your sleep patterns and discover strategies for improving your sleep. You deserve to get a good night s sleep we re here to help! The following
We are pleased you are taking the time to become more aware of your sleep patterns and discover strategies for improving your sleep. You deserve to get a good night s sleep we re here to help! The following
Sleep & Relaxation. Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique
 Sleep & Relaxation Sleep & Relaxation Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique Session 2 Dealing with unhelpful thoughts Putting these techniques together for better
Sleep & Relaxation Sleep & Relaxation Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique Session 2 Dealing with unhelpful thoughts Putting these techniques together for better
Many people with physical
 FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
Denver, CO Welcome Packet
 Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
HOW TO DEAL WITH SLEEP PROBLEMS
 The Handbook on Successful Ageing HOW TO DEAL WITH SLEEP PROBLEMS Up to 50% of the elderly complain of insomnia, but although such complaints are prevalent and are often accompanied by higher rates of
The Handbook on Successful Ageing HOW TO DEAL WITH SLEEP PROBLEMS Up to 50% of the elderly complain of insomnia, but although such complaints are prevalent and are often accompanied by higher rates of
Self care information on insomnia
 Self care information on insomnia 2 What is insomnia? Insomnia means poor sleep. It is defined as: Difficulty in getting to sleep Difficulty staying asleep Waking up too early Not feeling refreshed after
Self care information on insomnia 2 What is insomnia? Insomnia means poor sleep. It is defined as: Difficulty in getting to sleep Difficulty staying asleep Waking up too early Not feeling refreshed after
Let s Sleep On It. Session Overview. Let s Sleep On It. Welcome and Introductions Presenter: Rita Piper, VP of Wellness
 Let s Sleep On It Let s Sleep On It Welcome and Introductions Presenter: Rita Piper, VP of Wellness Session Overview Why Sleep is so Important Types of Sleep Common Sleep Disruptors Sleep Disorders Tips
Let s Sleep On It Let s Sleep On It Welcome and Introductions Presenter: Rita Piper, VP of Wellness Session Overview Why Sleep is so Important Types of Sleep Common Sleep Disruptors Sleep Disorders Tips
Insomnia Restoring Restful Sleep
 Insomnia Restoring Restful Sleep written by Harvard Medical School www.patientedu.org Nearly everyone has spent at least one night lying in bed wishing for sleep. But for many people, it s a nightly struggle.
Insomnia Restoring Restful Sleep written by Harvard Medical School www.patientedu.org Nearly everyone has spent at least one night lying in bed wishing for sleep. But for many people, it s a nightly struggle.
Psychological Sleep Services Sleep Assessment
 Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Sleep Health Center. You have been scheduled for an Insomnia Treatment Program consultation to further discuss your
 Sleep Health Center You have been scheduled for an Insomnia Treatment Program consultation to further discuss your sleep. In the week preceding your appointment, please take the time to complete the enclosed
Sleep Health Center You have been scheduled for an Insomnia Treatment Program consultation to further discuss your sleep. In the week preceding your appointment, please take the time to complete the enclosed
A Good Night s Sleep Participant s Guide
 FCD 08-002 September 2007 A Good Night s Sleep Participant s Guide "Sleep is better than medicine." --- English Proverb "The beginning of health is sleep." --- Irish Proverb "Disease and sleep keep far
FCD 08-002 September 2007 A Good Night s Sleep Participant s Guide "Sleep is better than medicine." --- English Proverb "The beginning of health is sleep." --- Irish Proverb "Disease and sleep keep far
Improving Your Sleep Course. Session 1 Understanding Sleep and Assessing Your Difficulties
 Improving Your Sleep Course Session 1 Understanding Sleep and Assessing Your Difficulties Course Information Session Details Sessions Session 1 Session 2 Session 3 Session 4 Optional Review Session 5 Session
Improving Your Sleep Course Session 1 Understanding Sleep and Assessing Your Difficulties Course Information Session Details Sessions Session 1 Session 2 Session 3 Session 4 Optional Review Session 5 Session
Biopsychosocial Characteristics of Somatoform Disorders
 Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Cognitive behavioural therapy for insomnia
 Cognitive behavioural therapy for insomnia Item type Authors Citation Publisher Journal Article Ruth, Alan Ruth A. Cognitive behavioural therapy for insomnia. Nurs Gen Prac 2014 May 29-30, 32 Nursing in
Cognitive behavioural therapy for insomnia Item type Authors Citation Publisher Journal Article Ruth, Alan Ruth A. Cognitive behavioural therapy for insomnia. Nurs Gen Prac 2014 May 29-30, 32 Nursing in
Dr Alex Bartle. Medical Director Sleep Well Clinic Christchurch
 Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 11:00-11:55 WS #113: Circadian Sleep Disorders 12:05-13:00 WS #125: Circadian Sleep Disorders (Repeated) Overview The Structure of Sleep
Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 11:00-11:55 WS #113: Circadian Sleep Disorders 12:05-13:00 WS #125: Circadian Sleep Disorders (Repeated) Overview The Structure of Sleep
How to Help Your Clients Get Better Sleep
 How to Help Your Clients Get Better Sleep Bonus Video 1 10-Point Checklist for Getting Better Sleep with Rubin Naiman, PhD How to Help Your Clients Get Better Sleep 2 10-Point Checklist for Getting Better
How to Help Your Clients Get Better Sleep Bonus Video 1 10-Point Checklist for Getting Better Sleep with Rubin Naiman, PhD How to Help Your Clients Get Better Sleep 2 10-Point Checklist for Getting Better
INSOMNIA IN GERIATRICS. Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow
 INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
th Ave NE Suite F Bellevue, WA Phone: (425) Fax: (425) Excessive Daytime Sleepiness
 Fax: (425) Excessive Daytime Sleepiness") 1414 116 th Ave NE Suite F Bellevue, WA 98004 Phone: (425) 451-8417 Fax: (425) 455-4089 Excessive Daytime Sleepiness Nearly everyone has days when they feel sleepy. But for some people, excessive sleepiness
1414 116 th Ave NE Suite F Bellevue, WA 98004 Phone: (425) 451-8417 Fax: (425) 455-4089 Excessive Daytime Sleepiness Nearly everyone has days when they feel sleepy. But for some people, excessive sleepiness
Self-care information on insomnia
 Self-care information on insomnia 2 What is insomnia? Insomnia means poor sleep. It is defined as: Difficulty in getting to sleep Difficulty staying asleep Waking up too early Not feeling refreshed after
Self-care information on insomnia 2 What is insomnia? Insomnia means poor sleep. It is defined as: Difficulty in getting to sleep Difficulty staying asleep Waking up too early Not feeling refreshed after
THIBODAUX REGIONAL SLEEP DISORDERS CENTER 604 N ACADIA ROAD, Suite 210 THIBODAUX, LA 70301
 Name:_ Date: Address: Phone (home): Work: Marital Status: Date of Birth: Height: Weight: In case of emergency contact: ************************************************************************ Social Security#:
Name:_ Date: Address: Phone (home): Work: Marital Status: Date of Birth: Height: Weight: In case of emergency contact: ************************************************************************ Social Security#:
Achieving better sleep
 Achieving better sleep A patient s guide 1 Sleep problems are common and affect a large proportion of people at some time in their lives. One question often asked is How much sleep do I need? for which
Achieving better sleep A patient s guide 1 Sleep problems are common and affect a large proportion of people at some time in their lives. One question often asked is How much sleep do I need? for which
WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?)
") Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?) CATHERINE MCCALL, MD
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?) CATHERINE MCCALL, MD
Sleep Deprivation: Understanding and Improving Your Sleep
 Sleep Deprivation: Understanding and Improving Your Sleep Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary It is rare for people to obtain
Sleep Deprivation: Understanding and Improving Your Sleep Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary It is rare for people to obtain
General Information. Name Age Date of Birth. Address Apt. # City State Zip. Home Phone Work Phone. Social Security Number Marital Status
 Accredited Member Center of The American Academy of Sleep Medicine 400 Riverside Drive, Suite 1500, Bourbonnais, IL 60914 Phone (815) 933-2874 Fax (815) 939-9413 www.riversidemc.net/sleep General Information
Accredited Member Center of The American Academy of Sleep Medicine 400 Riverside Drive, Suite 1500, Bourbonnais, IL 60914 Phone (815) 933-2874 Fax (815) 939-9413 www.riversidemc.net/sleep General Information
Optimal Sleep Using NeurOptimal -Insomnia Studies
 Optimal Sleep Using NeurOptimal -Insomnia Studies Edward B. O'Malley, PhD, FAASM Diplomate, American Board of Sleep Medicine Managing Director, Sleep HealthCare of CT Fairfield, CT eomalley@sleephelathcarect.com
Optimal Sleep Using NeurOptimal -Insomnia Studies Edward B. O'Malley, PhD, FAASM Diplomate, American Board of Sleep Medicine Managing Director, Sleep HealthCare of CT Fairfield, CT eomalley@sleephelathcarect.com
Sleep: What s the big deal?
 Rise & Shine: The Importance of Sleep Sleep: What s the big deal? Sleep affects every aspect of a child s physical, emotional, cognitive, and social development. 1 Sleep is the Primary Activity of the
Rise & Shine: The Importance of Sleep Sleep: What s the big deal? Sleep affects every aspect of a child s physical, emotional, cognitive, and social development. 1 Sleep is the Primary Activity of the
Tinnitus Activities Treatment. Sleep Session. Sleep 1
 Tinnitus Activities Treatment Sleep Session Sleep 1 Overview 1. Normal sleep patterns 2. Things that affect sleep 3. Daytime activities to facilitate sleep 4. Evening activities to facilitate sleep 5.
Tinnitus Activities Treatment Sleep Session Sleep 1 Overview 1. Normal sleep patterns 2. Things that affect sleep 3. Daytime activities to facilitate sleep 4. Evening activities to facilitate sleep 5.