ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
|
|
|
- Ruth Lambert
- 5 years ago
- Views:
Transcription
1 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015
2 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche
3 Natural History of ESLD Increasing liver fibrosis Development of HCC Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death Alcohol Hepatitis C/B NASH Cholestatic Autoimmune Variceal hemorrhage Ascites Encephalopathy Jaundice Compensated to Decompensated cirrhosis occurs 5-7% per year HCC, hepatocellular carcinoma; NASH, nonalcoholic steacohepatitis Garcia Tsao CCO Hepatitis.com 2008
4 Survival Time from First Liver Decompensation to Death in HCV Percent of patients Year survival HIV+ HIV- Decompensation with Ascites Encephalopathy Variceal bleed Synthetic dysfunction (INR, Bili, Alb) 44 Death during study 366/1037 HCV 100/180 HIV/HCV Risk factors for death: HIV Baseline CTP MELD >13 Age Pineda, Hepatology 2005
5 Manage ESLD Need to know if your patient has cirrhosis Need to know if compensated or decompensated Then need to manage complications

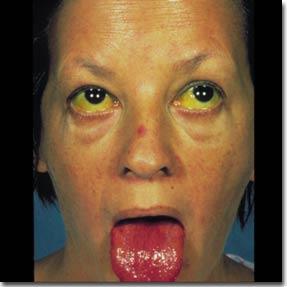


6 Diagnosing Cirrhosis Physical Exam
7 Diagnosing Cirrhosis Labs EXAM: Spider nevi, splenomegaly Most labs not helpful 50% Child s A normal AST:ALT often >1 Synthetic dysfunction Hypoalbuminemia Prolonged PT/ INR Hyperbilirubinemia Portal Hypertension Thrombocytopenia Leukopenia Anemia Renal dysfunction Elevated creatinine remember depends on muscle mass Hyponatremia with ascites

8 Diagnosing Cirrhosis Imaging Ultrasound poorly diagnoses cirrhosis In absence of portal hypertension Only 50% confirmed by Biopsy Increased echogenicity (ultrasound)= disease not F4 Surface nodularity Small nodular liver Hidden clues from radiology report of Portal HTN Ascites Portal/splenic/superior mesenteric vein thrombosis Portosystemic collaterals Splenomegaly
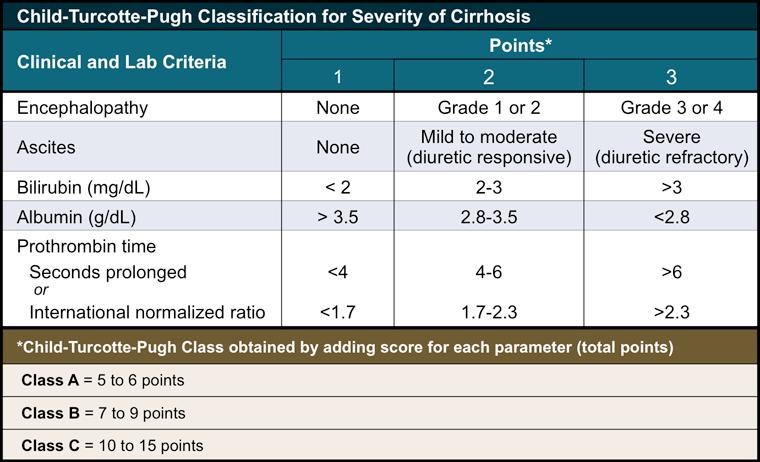
9 Prognosticating Decompensated Cirrhosis
 and allocation of donor livers.")
10 3-Month Mortality Based on CTP Wiesner R, Edwards E, Freeman R, et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124:91-6.
11 MELD and Liver Transplantation MELD Prioritization on liver transplant list Most IMPORTANT single value in prognostication Easy to calculate prior to referral MELD = 15 or greater Benefit from OLT Important predictor of liver-related outcomes

12 MELD INR Bilirubin Creatinine
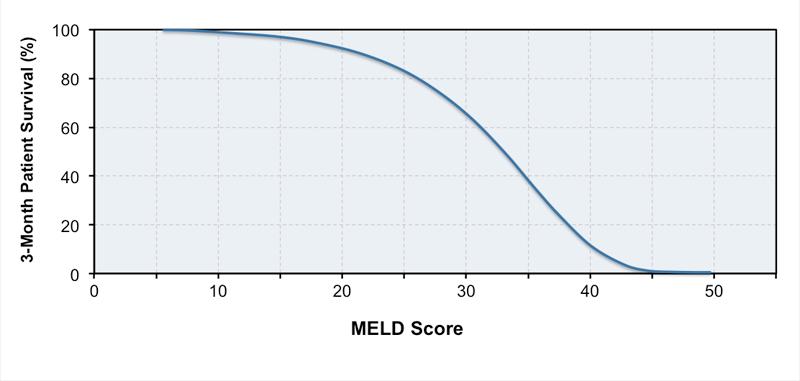
13 3-Month Survival Based on MELD
14 Steps in Assessing Cirrhosis 1. Clinical evidence of cirrhosis Labs (elevated INR, low albumin, bilirubin) Radiology evidence of portal HTN Exam (ascites, varices, encephalopathy) 2. Transient elastography 3. Noninvasive markers E.g. APRI Fib 4- uses AST, platelets, ALT 4. If further delineation is needed Liver biopsy with measurement of portal pressure Not needed in many/ most situations with HCV



15 Risk of Bleeding from Esophageal Varices Cirrhosis Risk of Bleeding Prevalence 35%-80% 25%-40% 50%-70% Survive 70% Rebleed 30%-50% Die
, Child B/C Medium or large varices")


16 Variceal Surveillance All cirrhotics require Esophagogastroduodenoscopy No varices Small varices (< 5 mm), Child B/C Medium or large varices Repeat endoscopy in 3 years (well compensated); in 1 year if decompensated No beta-blocker prophylaxis Nonselective Beta-blocker prophylaxis Child Class A, no red wales: beta blockers Child class B/C, red wales: beta blockers or band ligation Garcia-Tsao G, et al. Hepatology. 2007;46:


17 Varices Esophageal Gastric
18 Hepatic Venous Pressure to Predict Portal Hypertension 71 events in 41 patients Robic J Hep 2011: 100 pts followed for 2y: ETOH 38; v hep 28: 75 F3-4
19 Liver Stiffness to predict Portal Hypertension Robic J Hep 2011
20 Ascites Most common complication of cirrhosis Most common indication for hospitalization 15% with ascites die in 1 year 44% with ascites die in 5 years 85% of hospitalized patients with ascites have cirrhosis as cause of ascites AASLD guidelines 2012
21 Stages of ascites Diuretic-responsive ascites Refractory ascites Hyponatremia Hepatorenal syndrome (HRS) Each stage reflects a more deranged circulatory state.
22 When to tap ascites Diagnostic paracentesis with ALL new onset ascites (either inpatient or outpatient) FFP and/or platelets are NOT needed prior to the procedure 1% reported rate of abdominal wall hematoma with 71% having abnormal prothrombin time Runyon Hepatology 2012
23 Management of Ascites First-Line Therapy Tense ascites Paracentesis Refractory ascites 10 % Second-Line Therapy Repeated large volume paracentesis (LVP) TIPSS Sodium restriction ( <2 gm/24 hrs) and diuretics Liver transplantation Non-tense ascites- paracentesisis Diuretics: Spironolactone mg/day, furosemide mg/day or bumetanide 1 mg. Titrate stepwise to spironolactone 400 mg/day, furosemide 160 mg/day or bumetanide 4 mg/day as long as it is tolerated AT 2-WEEK INTERVALS (electrolytes)
24 Spontaneous bacterial peritonitis (SBP) Most common type of bacterial infection in hospitalized cirrhotic patients Clinical suspicion: <50%: fever, abdominal pain or tenderness, and leukocytosis unexplained encephalopathy, jaundice worsening renal failure Diagnose: tap ascites: WCC>500, PMN > 250 cells/mm 3 Place ascites in blood culture bottles Start treatment immediately before culture results
25 SBP treatment Cephalosporins 3rd gen ie cefotaxime 2g q8 Renal dysfunction is main cause of death prevented by the use of intravenous albumin (1.5g/kg day 1 and 1.0 g/kg day 3) if serum bilirubin > 4 mg/dl serum creatinine > 1 g/dl or blood urea nitrogen level > 30 mg/dl Prevent recurrence: ciprofloxacin, TMP/SMX, norfloxacin Primary prophylaxis: ciprofloxacin weekly if MELD >12 all subjects, >9 with HIV Runyon Hepatology 2012
26 Hepatorenal syndrome (HRS) Acute renal failure occurs in 14% to 25% of hospitalized patients with cirrhosis Most commonly prerenal failure (accounting for 60% to 80% of the cases) HRS is a form of prerenal failure results from vasodilatation and marked reduction in effective arterial blood volume leading to renal vasoconstriction occurs in patients with refractory ascites and/or hyponatremia.
27 Hepatorenal syndrome Type 1 HRS: rapidly progressive renal failure in 2 weeks with doubling serum creatinine to > 2.5 mg/dl or halving creatinine clearance to < 20 ml/min Prognosis: < 50% survival at 1 month Type 2 HRS: slowly progressive increase in serum creatinine > 1.5 mg/dl creatinine clearance of < 40 ml/mi or a urine sodium < 10 meq/d associated with ascites that is unresponsive to diuretic medications median survival: ~ 6 months
28 HRS treatment OLT Midodrine and octreotide HRS due to extreme splanchnic and systemic vasodilatation Drugs vasoconstriction Albumin to increase intravascular volume
29 Hepatic Encephalopathy Results from a combination of Portosystemic shunting and failure to metabolize neurotoxic substances Ammonia remains the most important neurotoxic substance but poorly correlates with stage


30 Precipitating Factors of HE Slide 30 of 56 Excess protein GI bleeding Sedatives / hypnotics TIPS Diuretics Temp Most no fever Infections Serum K + Plasma volume Azotemia Courtesy of AGA
31 Hepatic Encephalopathy Treatment aims to reduce production of NH3 from the colon through nonabsorbable disaccharides lactulose, lactitol, and lactose: 3-4 BM per day nonabsorbable antibiotics rifaximin 550 mg bid, neomycin rarely used Protein restriction promotes protein degradation and, if maintained for long periods, worsens nutritional status and decreases muscle mass No longer recommended
32 Correlation Between Ammonia and Encephalopathy Ong et al, Am J Medicine, 2003
33 Hepatocellular Carcinoma (HCC) Late complication of end-stage liver disease Exceptions: HBV seen in non cirrhotics Diagnosis by US, CT scan, MRI Histology is not essential Alpha-fetoprotein level may be elevated 20-40% with HCC have normal AFP 20-30% without HCC have abnormal AFP The higher the AFP, the more likely the diagnosis of HCC
34 Hepatocellular Carcinoma (HCC) Surveillance Screen all patients with cirrhosis for HCC Up to 8% risk of HCC/year Also HBV: male>40y and female HBV >50y (even if they don t have cirrhosis) Up to 0.6% risk of HCC/year Screen with ultrasound q 6 months No benefit to shortening interval??no benefit to screening with AFP In practice many still use cross-sectional imaging and AFP to screen as well Bruix et al Hepatology 2010

35 Quad phase CT Appearance of HCC Arterial Phase Arterial Phase Portal venous Phase washout Hypervascular lesion that washes out on portal venous phase
36 Treatment of HCC Resection Local-regional therapy TACE: transarterial chemoembolization RFA: radiofrequency ablation Ethanol ablation Liver transplantation Systemic Sorafenib
37 LOCAL REGIONAL THERAPIES FOR HCC CHEMOEMBOLIZATION Conventional and Drug-eluting beads ABLATION CHEMICAL Percutaneous ethanol injection (PEI) THERMAL Radiofrequency ablation (RFA) (Laparoscopic, percutaneous or open) Microwave/ Cryoablation RADIOEMBOLIZATION (YITTRIUM - 90)
38 Take Home: HCC Screen ALL patients with u/s q6 months if they have cirrhosis Usually radiographic diagnosis Biopsy rarely needed if classic imaging Cross-sectional imaging look for arterial enhancement and washout Treatment: Possibly curative : ablation, resection, transplant Palliative: TACE, sorafenib
39 End Stage Liver Disease 5% to 7% of Child s A cirrhotics decompensate per year Diagnosis of Child s A, even B cirrhosis may be subtle Screen for HCC Perform EGD Monitor closely on therapy HCV with Child s B can be treated- OLT back up plan
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Hepatology For The Nonhepatologist
 Hepatology For The Nonhepatologist Andrew Aronsohn, MD Associate Professor of Medicine University of Chicago Chicago, Illinois Learning Objectives After attending this presentation, learners will be able
Hepatology For The Nonhepatologist Andrew Aronsohn, MD Associate Professor of Medicine University of Chicago Chicago, Illinois Learning Objectives After attending this presentation, learners will be able
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
DISCLOSURES. This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea
 DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Evaluating HIV Patient for Liver Transplantation. Marion G. Peters, MD Professor of Medicine University of California San Francisco USA
 Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Program Disclosure. This program is supported by an educational grant from Salix Pharmaceuticals.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Care of the Patient With Cirrhosis
 REVIEW Care of the Patient With Cirrhosis Anitha Yadav, M.D., and Hugo E. Vargas, M.D. Caring for patients with cirrhosis involves multidisciplinary and timely management of several complications while
REVIEW Care of the Patient With Cirrhosis Anitha Yadav, M.D., and Hugo E. Vargas, M.D. Caring for patients with cirrhosis involves multidisciplinary and timely management of several complications while
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed?
 CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL
 DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease
 Slide 1 of 20 Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University
Slide 1 of 20 Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Initial Evaluation for HCV Therapy. Hope McGratty PA-C, MPH
 Initial Evaluation for HCV Therapy Hope McGratty PA-C, MPH Conflict of Interest Disclosure Statement None Who are we talking about today? Treatment naïve Chronic infection This patient seems complicated
Initial Evaluation for HCV Therapy Hope McGratty PA-C, MPH Conflict of Interest Disclosure Statement None Who are we talking about today? Treatment naïve Chronic infection This patient seems complicated
MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS
 MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS Mark W. Sonderup Division of Hepatology and Liver Laboratory Department of Medicine University of Cape Town & Groote Schuur Hospital Cirrhosis..
MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS Mark W. Sonderup Division of Hepatology and Liver Laboratory Department of Medicine University of Cape Town & Groote Schuur Hospital Cirrhosis..
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Module 1 Introduction of hepatitis
 Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY
 COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
Ascites. Matthew Johnson M.D.
 Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting?
 Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Hepatocellular Carcinoma (HCC)
") Title Slide Hepatocellular Carcinoma (HCC) Professor Muhammad Umar MBBS, MCPS, FCPS (PAK), FACG (USA), FRCP (L), FRCP (G), ASGE-M(USA), AGAF (USA) Chair & Professor of Medicine Rawalpindi Medical College
Title Slide Hepatocellular Carcinoma (HCC) Professor Muhammad Umar MBBS, MCPS, FCPS (PAK), FACG (USA), FRCP (L), FRCP (G), ASGE-M(USA), AGAF (USA) Chair & Professor of Medicine Rawalpindi Medical College
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Management of Liver Diseases: A Nonhepatologist s Viewpoint
 Management of Liver Diseases: A Nonhepatologist s Viewpoint Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Director, Viral Hepatitis Clinic Massachusetts General Hospital Boston,
Management of Liver Diseases: A Nonhepatologist s Viewpoint Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Director, Viral Hepatitis Clinic Massachusetts General Hospital Boston,
New York State HCV Provider Webinar Series
 New York State HCV Provider Webinar Series Overview of Fibrosis-Staging, Child s Pugh, MELD Scores Paul J Gaglio, MD, FACP, AGAF, FAASLD Director: Hepatology Outreach Professor of Medicine (in Surgery)
New York State HCV Provider Webinar Series Overview of Fibrosis-Staging, Child s Pugh, MELD Scores Paul J Gaglio, MD, FACP, AGAF, FAASLD Director: Hepatology Outreach Professor of Medicine (in Surgery)
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Assessment of Liver Function: Implications for HCC Treatment
 Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Dr. John C Rwegasha.FRCP(Lond),MSc, Muhimbili National Hospital Dar es Salaam Tanzania 15/09/2018 1
,MSc, Muhimbili National Hospital Dar es Salaam Tanzania 15/09/2018 1") Dr. John C Rwegasha.FRCP(Lond),MSc, Muhimbili National Hospital Dar es Salaam Tanzania 15/09/2018 1 No disclosures. 15/09/2018 2 Sub-Saharan Africa (SSA) has a high burden of morbidity and mortality resulting
Dr. John C Rwegasha.FRCP(Lond),MSc, Muhimbili National Hospital Dar es Salaam Tanzania 15/09/2018 1 No disclosures. 15/09/2018 2 Sub-Saharan Africa (SSA) has a high burden of morbidity and mortality resulting
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Hepatocellular Carcinoma: Epidemiology and Screening
 Hepatocellular Carcinoma: Epidemiology and Screening W. Ray Kim, MD Professor and Chief Gastroenterology and Hepatology Stanford University School of Medicine Case A 67 year old Filipino-American woman
Hepatocellular Carcinoma: Epidemiology and Screening W. Ray Kim, MD Professor and Chief Gastroenterology and Hepatology Stanford University School of Medicine Case A 67 year old Filipino-American woman
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
4/3/2014. Elizabeth Thompson, PharmD April Understand the importance of the liver and basic physiology.
 Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Pretreatment Evaluation
 Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of
 Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management
 HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Managing Cirrhosis. Cirrhosis of the liver is a progressive, fibrosing. Ascites. By Cameron Ghent, MD, FRCPC. Complications of Cirrhosis
 Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Tumor incidence varies significantly, depending on geographical location.
 Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
B C Outlines. Child-Pugh scores
 B C 2016-12-09 Outlines Child-Pugh scores CT MRI Fibroscan / ARFI Histologic Scoring Systems for Fibrosis Fibrosis METAVIR Ishak None 0 0 Portal fibrosis (some) 1 1 Portal fibrosis (most) 1 2 Bridging
B C 2016-12-09 Outlines Child-Pugh scores CT MRI Fibroscan / ARFI Histologic Scoring Systems for Fibrosis Fibrosis METAVIR Ishak None 0 0 Portal fibrosis (some) 1 1 Portal fibrosis (most) 1 2 Bridging
Surveillance for HCC Who, how Diagnosis of HCC Surveillance for HCC in Practice
 Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Acute Liver Failure. Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018
 Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Pretreatment Evaluation
 Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Validation of Clinical Outcomes in Electronic Data Sources
 Validation of Clinical Outcomes in Electronic Data Sources Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Center for Clinical Epidemiology and Biostatistics Center for Pharmacoepidemiology
Validation of Clinical Outcomes in Electronic Data Sources Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Center for Clinical Epidemiology and Biostatistics Center for Pharmacoepidemiology
Advances in percutaneous ablation for hepatocellular carcinoma
 Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
Organ allocation for liver transplantation: Is MELD the answer? North American experience
 Organ allocation for liver transplantation: Is MELD the answer? North American experience Douglas M. Heuman, MD Virginia Commonwealth University Richmond, VA, USA March 1998: US Department of Health and
Organ allocation for liver transplantation: Is MELD the answer? North American experience Douglas M. Heuman, MD Virginia Commonwealth University Richmond, VA, USA March 1998: US Department of Health and
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Alcoholic Hepatitis: Routine Screening for Early Recognition and Management. Juan Guerrero, MD
 Alcoholic Hepatitis: Routine Screening for Early Recognition and Management Juan Guerrero, MD Global Problem 1% of GNP of medium/high income countries Additional societal costs Disproportionately affects
Alcoholic Hepatitis: Routine Screening for Early Recognition and Management Juan Guerrero, MD Global Problem 1% of GNP of medium/high income countries Additional societal costs Disproportionately affects
Diagnostic Procedures. Measurement of Hepatic venous pressure in management of cirrhosis. Clinician s opinion
 5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
Cirrhosis Complications
 Cirrhosis Complications and Spontaneous Bacterial Peritonitis While these complications greatly increase mortality from decompensated cirrhosis, effective treatment is possible with early diagnosis. Vigilant
Cirrhosis Complications and Spontaneous Bacterial Peritonitis While these complications greatly increase mortality from decompensated cirrhosis, effective treatment is possible with early diagnosis. Vigilant
Liver transplantation: Hepatocellular carcinoma
 Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT.
 Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
Topics to be covered
 Caring for the patient with cirrhosis Role of the hospitalist Danielle Brandman, MD, MAS Associate Professor of Clinical Medicine Associate Program Director, Transplant Hepatology Fellowship October 18,
Caring for the patient with cirrhosis Role of the hospitalist Danielle Brandman, MD, MAS Associate Professor of Clinical Medicine Associate Program Director, Transplant Hepatology Fellowship October 18,
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
9th Paris Hepatitis Conference
 9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National