Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
|
|
|
- Penelope Alexander
- 5 years ago
- Views:
Transcription


1 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC

2
3 No Conflict of Interest
4
5 157 patients
6 157 patients 6 transplanted
7 Criteria Liver Transplant Palliative Care Approach
8 Criteria Liver Transplant = Palliative Care Approach
9
10
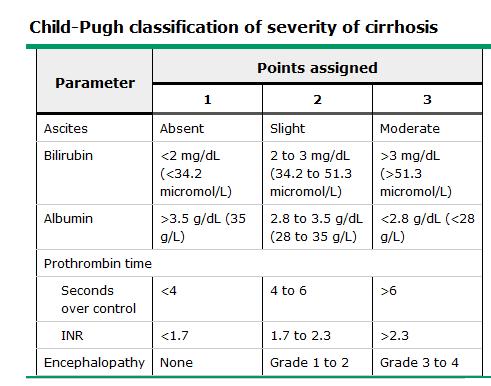
11 advanced chronic liver disease when the limits of medical therapy have been reached. AASLD 2013
12 Patients should be selected if expected survival in the absence of transplantation is one year or less, or if the patient had an unacceptable quality of life because of liver disease. EASL 2015
13 Patients should be selected if expected survival in the absence of transplantation is one year or less, or if the patient had an unacceptable quality of life because of liver disease. EASL 2015

14

15 An approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychological and spiritual.
16 Liver Transplant Palliative Care Patient with ESLD
17 Hawley, 2014
18 Hawley, 2014
19 Compensated Cirrhosis

20 Compensated Cirrhosis 6-12 years
21 Compensated Cirrhosis Decompensated Cirrhosis 6-12 years
22 Compensated Cirrhosis Decompensated Cirrhosis 6-12 years 2 years
23
24
25
26
27
28 Class A Class B Class C
29 100% 1 year survival 80% 45% Class A Class B Class C
")
30 Model for End-Stage Liver Disease (MELD) Score
31
32 15
33
34 20-25% Death

35 5-10% Clinical Deterioration
36 < 2 months
37 10%
38 well enough to undergo evaluation and listing, but sick enough to have developed signs of progression to a terminal state. Fox, 2014
39 Liver Transplant Palliative Care Patient with ESLD
40 Liver Transplant + Palliative Care Patient with ESLD

41 Hawley, 2014
42 Treating patients with end-stage liver disease: Are we ready?
43
44 Treating patients with end-stage liver disease: Are we ready?
45 Patient Care
46 ESLD Patient Care
47 Patient Care ESLD Cancer
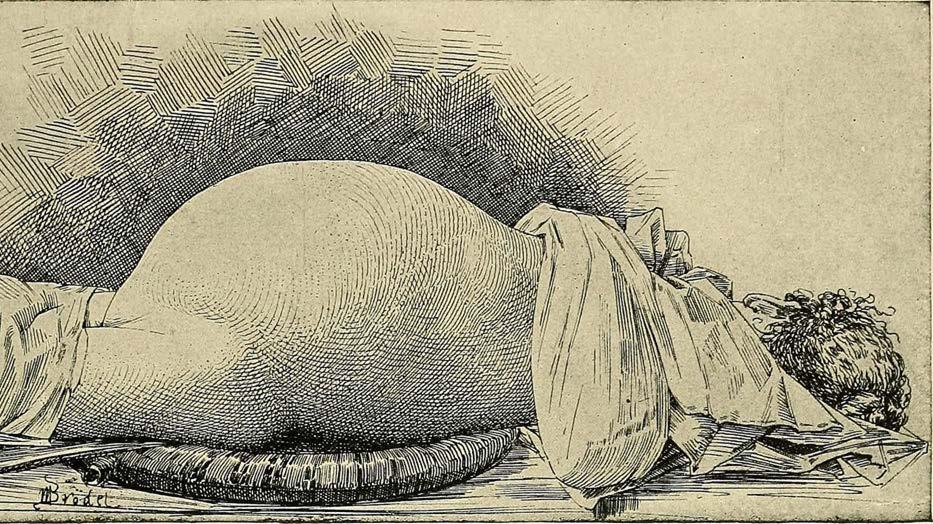
48 Ascites Cirrhotic Cardiomyopathy Gastroesophageal Varices Hepatic Encephalopathy Hepatic Hydrothorax Hepatocellular Carcinoma Hepatopulmonary Syndrome Hepatorenal Syndrome Portal Vein Thrombosis Portopulmonary hypertension Spontaneous Bacterial Peritonitis
49 Ascites Cirrhotic Cardiomyopathy Gastroesophageal Varices Hepatic Encephalopathy Hepatic Hydrothorax Hepatocellular Carcinoma Hepatopulmonary Syndrome Hepatorenal Syndrome Portal Vein Thrombosis Portopulmonary hypertension Spontaneous Bacterial Peritonitis
50
51 Portal Hypertension vs Non-Portal Hypertension
52
53
54
55 Portal Hypertension vs Non-Portal Hypertension
56
57 Spirinolactone 5:2 ratio Furosemide
58 Furosemide

59 Furosemide X

60 Spirinolactone 100mg : 40mg Furosemide

61 < 2gm / day
62
63 Large Volume Paracentesis (>5L)


64 6-8gm of Albumin per extra liter Large Volume Paracentesis (>5L)
65 Malignancy Cirrhosis
66 Malignancy Cirrhosis Peritoneovenous Shunting
67 Malignancy Cirrhosis Peritoneovenous Shunting Transjugular Intrahepatic Portosystemic Shunt (TIPS)
68
69 Portal Vein

70 Hepatic Vein Portal Vein
71 Ascites Cirrhotic Cardiomyopathy Gastroesophageal Varices Hepatic Encephalopathy Hepatic Hydrothorax Hepatocellular Carcinoma Hepatopulmonary Syndrome Hepatorenal Syndrome Portal Vein Thrombosis Portopulmonary hypertension Spontaneous Bacterial Peritonitis
72
")
73 Ammonia (NH3)

74

75
76
77

78
79
80 Bloodstream
81 Bloodstream Ammonia (NH3)
82 Bloodstream Ammonia (NH3)
83 Bloodstream Ammonia (NH3) Ammonium (NH4+)
84 Bloodstream Ammonia (NH3) Ammonium (NH4+)
85 Bloodstream Lactulose 30-45mL PO TID-QID Ammonia (NH3) Ammonium (NH4+)
86 Bloodstream Ammonia (NH3) Ammonium (NH4+)

")
87 Bloodstream Rifaximin 550mg PO BID or 400mg TID Ammonia (NH3) Ammonium (NH4+)
88



89
90 (Peng et al., 2018)
91 (Peng et al., 2018)
92 (Peng et al., 2018)

93 (Peng et al., 2018)
94




95 Always prescribe lactulose



96



97 Go REALLY low and REALLY slow
98

99
100 Opioids Codeine Tramadol Morphine Hydromorphone Oxycodone Fentanyl Methadone
101 Opioids Codeine Tramadol Morphine Hydromorphone Oxycodone Fentanyl Methadone

102
103 NSAIDs Acetaminophen Gabapentin Pregabalin Nortriptyline Carbamazepine Non-Opioids
104 NSAIDs Acetaminophen Gabapentin Pregabalin Nortriptyline Carbamazepine Non-Opioids

105 Patient Care ESLD Cancer

106 Ascites Cirrhotic Cardiomyopathy Gastroesophageal Varices Hepatic Encephalopathy Hepatic Hydrothorax Hepatocellular Carcinoma Hepatopulmonary Syndrome Hepatorenal Syndrome Portal Vein Thrombosis Portopulmonary hypertension Spontaneous Bacterial Peritonitis

107
108
109
110
111 Treating patients with end-stage liver disease: Are we ready?
112 Treating patients with end-stage liver disease: Are YOU ready?

113 Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
PALLIATIVE CARE IN END-STAGE LIVER DISEASE
 PALLIATIVE CARE IN END-STAGE LIVER DISEASE Ken S. Ota, DO Family Medicine Banner Good Samaritan Medical Center Learning Objectives: Describe the common bio-psycho-social issues in end-stage liver disease
PALLIATIVE CARE IN END-STAGE LIVER DISEASE Ken S. Ota, DO Family Medicine Banner Good Samaritan Medical Center Learning Objectives: Describe the common bio-psycho-social issues in end-stage liver disease
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
The Importance of Diagnosing Covert Hepatic Encephalopathy
 The Importance of Diagnosing Covert Hepatic Encephalopathy Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council
The Importance of Diagnosing Covert Hepatic Encephalopathy Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
This survey aims to look at individual practice and can be completed by any healthcare professional.
 This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia
 Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Evaluating HIV Patient for Liver Transplantation. Marion G. Peters, MD Professor of Medicine University of California San Francisco USA
 Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY
 COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Ontario s Adult Referral and Listing Criteria for Liver Transplantation
 Ontario s Adult Referral and Listing Criteria for Liver Transplantation Version 3.0 Trillium Gift of Life Network Ontario s Adult Referral & Listing Criteria for Liver Transplantation PATIENT REFERRAL
Ontario s Adult Referral and Listing Criteria for Liver Transplantation Version 3.0 Trillium Gift of Life Network Ontario s Adult Referral & Listing Criteria for Liver Transplantation PATIENT REFERRAL
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
Program Disclosure. This program is supported by an educational grant from Salix Pharmaceuticals.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Liver Failure. The most severe clinical consequence of liver disease is liver failure:
 Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12:
 Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility
 Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
CHAPTER 7. End Stage Liver Disease in the ICU: Walking a Tightrope. Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing
 CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
4/3/2014. Elizabeth Thompson, PharmD April Understand the importance of the liver and basic physiology.
 Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Transjugular Intrahepatic
 Transjugular Intrahepatic Portosystemic Shunt (TIPS): A Clinical and Procedural Review Mark R. Werley, M.D. and John Briguglio, M.D. Lancaster Radiology Associates, Ltd. INTRODUCTION This article reviews
Transjugular Intrahepatic Portosystemic Shunt (TIPS): A Clinical and Procedural Review Mark R. Werley, M.D. and John Briguglio, M.D. Lancaster Radiology Associates, Ltd. INTRODUCTION This article reviews
Management in Cirrhosis
 Management in Cirrhosis Outline Introduction Cause of cirrhosis and management General management in cirrhosis Management complication and surveillance Clue of Chronic Liver Disease and Cirrhosis Risk
Management in Cirrhosis Outline Introduction Cause of cirrhosis and management General management in cirrhosis Management complication and surveillance Clue of Chronic Liver Disease and Cirrhosis Risk
Managing Cirrhosis. Cirrhosis of the liver is a progressive, fibrosing. Ascites. By Cameron Ghent, MD, FRCPC. Complications of Cirrhosis
 Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Complications of Cirrhosis
 What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting?
 Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Ascites. Matthew Johnson M.D.
 Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
CIRRHOTIC MANAGEMENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Course Handouts & Post Test
 End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Transplant Hepatology
 Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Hepatopulmonary Syndrome: An Update
 Hepatopulmonary Syndrome: An Update Michael J. Krowka MD Professor of Medicine Division of Pulmonary and Critical Care Division of Gastroenterology and Hepatology Mayo Clinic Falk Liver Week October 11,
Hepatopulmonary Syndrome: An Update Michael J. Krowka MD Professor of Medicine Division of Pulmonary and Critical Care Division of Gastroenterology and Hepatology Mayo Clinic Falk Liver Week October 11,
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present:
 and the International Coalition of Hepatology Education Providers (IC-HEP) present:") The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatic Encephalopathy Hepatic Encephalopathy:
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatic Encephalopathy Hepatic Encephalopathy:
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Complications of Portal Hypertension A Practical Management Approach
 Complications of Portal Hypertension A Practical Management Approach Advances in Liver Disease 2018: A Year in Review 12/8/18 Richard Kalman, MD Assistant Professor of Medicine SKCM Einstein Healthcare
Complications of Portal Hypertension A Practical Management Approach Advances in Liver Disease 2018: A Year in Review 12/8/18 Richard Kalman, MD Assistant Professor of Medicine SKCM Einstein Healthcare
Liver Transplantation: The End of the Road in Chronic Hepatitis C Infection
 University of Massachusetts Medical School escholarship@umms UMass Center for Clinical and Translational Science Research Retreat 2012 UMass Center for Clinical and Translational Science Research Retreat
University of Massachusetts Medical School escholarship@umms UMass Center for Clinical and Translational Science Research Retreat 2012 UMass Center for Clinical and Translational Science Research Retreat
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL
 DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
Treatment of Overt Hepatic Encephalopathy: Focus on Outpatient Management
 Treatment of Overt Hepatic Encephalopathy: Focus on Outpatient Management Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation
Treatment of Overt Hepatic Encephalopathy: Focus on Outpatient Management Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation
The MELD Score in Advanced Liver Disease: Association with Clinical Portal Hypertension and Mortality
 The MELD Score in Advanced Liver Disease: Association with Clinical Portal Hypertension and Mortality Sammy Saab, 1,2 Carmen Landaverde, 3 Ayman B Ibrahim, 2 Francisco Durazo, 1,2 Steven Han, 1,2 Hasan
The MELD Score in Advanced Liver Disease: Association with Clinical Portal Hypertension and Mortality Sammy Saab, 1,2 Carmen Landaverde, 3 Ayman B Ibrahim, 2 Francisco Durazo, 1,2 Steven Han, 1,2 Hasan
Thank you. for supporting this program. For additional CME offerings, please visit
 Thank you for supporting this program For additional CME offerings, please visit www.chronicliverdisease.org Accredited by: Disease Burden Patient Discharges with Cirrhosis* Hospital Discharges Associated
Thank you for supporting this program For additional CME offerings, please visit www.chronicliverdisease.org Accredited by: Disease Burden Patient Discharges with Cirrhosis* Hospital Discharges Associated
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed?
 CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Medicine. Differential Clinical Impact of Ascites in Cirrhosis and Idiopathic Portal Hypertension
 Medicine OBSERVATIONAL STUDY Differential Clinical Impact of Ascites in Cirrhosis and Idiopathic Portal Hypertension Hitoshi Maruyama, MD, PhD, Takayuki Kondo, MD, PhD, Tadashi Sekimoto, MD, PhD, and Osamu
Medicine OBSERVATIONAL STUDY Differential Clinical Impact of Ascites in Cirrhosis and Idiopathic Portal Hypertension Hitoshi Maruyama, MD, PhD, Takayuki Kondo, MD, PhD, Tadashi Sekimoto, MD, PhD, and Osamu
Program Disclosure. A maximum of 1.5 contact hours may be earned for successful completion of this activity.
 Program Disclosure This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through
Program Disclosure This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
Current Liver Allocation Policies
 C Current Liver Allocation Policies Policy 3.6 Organ Distribution 3.6 Allocation of Livers. Unless otherwise approved according to Policies 3.1.7 (Local and Alternative Local Unit), 3.1.8 (Sharing Arrangement
C Current Liver Allocation Policies Policy 3.6 Organ Distribution 3.6 Allocation of Livers. Unless otherwise approved according to Policies 3.1.7 (Local and Alternative Local Unit), 3.1.8 (Sharing Arrangement
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
The Leeds Teaching Hospitals NHS Trust Transjugular Intrahepatic Portosystemic Shunt (TIPS)
") n The Leeds Teaching Hospitals NHS Trust Transjugular Intrahepatic Portosystemic Shunt (TIPS) Information for patients Your liver doctor has recommended that you have a Transjugular Intrahepatic Portosystemic
n The Leeds Teaching Hospitals NHS Trust Transjugular Intrahepatic Portosystemic Shunt (TIPS) Information for patients Your liver doctor has recommended that you have a Transjugular Intrahepatic Portosystemic
Entrustable Professional Activity
 Entrustable Professional Activity 1. EPA Title: Care of infants, children and adolescents with acute and chronic s 2. Description of Activity Practicing subspecialists must be trained to care for children
Entrustable Professional Activity 1. EPA Title: Care of infants, children and adolescents with acute and chronic s 2. Description of Activity Practicing subspecialists must be trained to care for children
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Diagnostic Procedures. Measurement of Hepatic venous pressure in management of cirrhosis. Clinician s opinion
 5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
Management of Portal Vein Thrombosis With and Without Cirrhosis
 Management of Portal Vein Thrombosis With and Without Cirrhosis Dominique-Charles Valla Service d Hépatologie,Hôpital Beaujon, APHP, Université Paris-Diderot, Inserm CRB3 Extrahepatic Portal Vein Obstruction
Management of Portal Vein Thrombosis With and Without Cirrhosis Dominique-Charles Valla Service d Hépatologie,Hôpital Beaujon, APHP, Université Paris-Diderot, Inserm CRB3 Extrahepatic Portal Vein Obstruction
EDUCATION PRACTICE. Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation?
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:931 935 EDUCATION PRACTICE Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation? VANDANA KHUNGAR* and SAMMY SAAB*,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:931 935 EDUCATION PRACTICE Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation? VANDANA KHUNGAR* and SAMMY SAAB*,
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5
 RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on
The Association Between the Serum Sodium Level and the Severity of Complications in Liver Cirrhosis
 ORIGINAL ARTICLE DOI: 10.3904/kjim.2009.24.2.106 The Association Between the Serum Sodium Level and the Severity of Complications in Liver Cirrhosis Jong Hoon Kim, June Sung Lee, Seuk Hyun Lee, Won Ki
ORIGINAL ARTICLE DOI: 10.3904/kjim.2009.24.2.106 The Association Between the Serum Sodium Level and the Severity of Complications in Liver Cirrhosis Jong Hoon Kim, June Sung Lee, Seuk Hyun Lee, Won Ki
Pain Management Management in Hepatic Hepatic and and Renal Dysfunction
 Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of
 Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Sign up to receive ATOTW weekly -
 HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
Portal hypertension and ascites
 Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Therapeutic Approaches to Cirrhotic versus Pre-Cirrhotic NASH
 www.alacrita.com Therapeutic Approaches to Cirrhotic versus Pre-Cirrhotic NASH 2nd Annual NASH Summit Europe October 23-24, 2018 Frankfort, Germany Peter G. Traber, MD Partner, Alacrita Consulting Alacrita
www.alacrita.com Therapeutic Approaches to Cirrhotic versus Pre-Cirrhotic NASH 2nd Annual NASH Summit Europe October 23-24, 2018 Frankfort, Germany Peter G. Traber, MD Partner, Alacrita Consulting Alacrita
A Retrospective Analysis of the Current Hospice Criteria for Decompensated Cirrhosis Patients. Compared to the MELD-Na Score. Natalie M.
 Running head: HOSPICE CRITERIA FOR CIRRHOSIS PATIENTS A Retrospective Analysis of the Current Hospice Criteria for Decompensated Cirrhosis Patients Compared to the MELD-Na Score by Natalie M. Fisher Thesis
Running head: HOSPICE CRITERIA FOR CIRRHOSIS PATIENTS A Retrospective Analysis of the Current Hospice Criteria for Decompensated Cirrhosis Patients Compared to the MELD-Na Score by Natalie M. Fisher Thesis
Disclosures. Management of Chronic, Non- Terminal Pain. Learning Objectives. Outline. Drug Schedules. Applicable State Laws
 Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Pharmacology in Liver Disease. Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant
 Pharmacology in Liver Disease Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant Objectives Outline the drug management for patients with: Ascites Spontaneous Bacterial Peritonitis
Pharmacology in Liver Disease Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant Objectives Outline the drug management for patients with: Ascites Spontaneous Bacterial Peritonitis