Debate: Do We Need More HCV Drugs Con Standpoint
|
|
|
- Russell Alban Gallagher
- 6 years ago
- Views:
Transcription



1 Debate: Do We Need More HCV Drugs Con Standpoint 18 th Antivirals PK Workshop, Friday 16 th June 2017, Chicago Jürgen Rockstroh Department of Medicine I University Hospital Bonn, Bonn, Germany
2 Conflict of Interest: JKR Honoraria for lectures and/or consultancies from Abbott, AbbVie, Bionor, BMS, Cipla, Gilead, Janssen, Merck, Roche, ViiV. Research grants from Dt. Leberstiftung, DZIF, NEAT ID.



3 Debate» This debate is not about who is more beautiful but really do we need even more HCV DAAs than we already have. Seite 3
4 p7 HCV DAAs 5 UTR Core E1 E2 NS2 NS3 NS4B NS5A NS5B 3 UTR Protease Polymerase Ribavirin NS3 Protease Inhibitors NS5A Replication Complex Inhibitors NS5B NUC Inhibitors NS5B Non-NUC Inhibitors Telaprevir Boceprevir Simeprevir Paritaprevir Asunaprevir Grazoprevir Glecaprevir Voxilaprevir Daclatasvir Ledipasvir Ombitasvir Velpatasvir Elbasvir Pibrentasvir GS-5816 Ruzasvir Sofosbuvir VX-135 Uprifosbuvir ACH-3422 Dasabuvir Beclabuvir -previr -asvir -buvir
5

6 2016 EASL Guidelines G/P Summer 2017 for all genotypes Journal of Hepatology 2017;66:
7 SVR24 rate (%) Summary of EASL % J-M Pawlotsky

8 HCV therapy: Game over! A. Aghemo and M. Buti, Gastroenterology 2017 Seite 8
9 Debate: Do we need more HCV drugs?» More drugs, more competition and eventually lower prices.» Any special patient populations left?» Need for shorter treatment durations?» Need for better tolerated drugs?» Need for drugs with less drug-drug interactions?» How about treatment of DAA failures? Seite 9
10 Debate: Do we need more HCV drugs?» More drugs, more competition and eventually lower prices.» Any special patient populations left?» Need for shorter treatment durations?» Need for better tolerated drugs?» Need for drugs with less drug-drug interactions?» How about treatment of DAA failures? Seite 10
11 Box price of DAA in current use in Egypt as of April 2017 DAA Manufactuturer NCCVH Pharmacies Sofosbuvir Generic 450 LE (25$) Simeprevir Brand 1315 (73$) Daclatasvir Brand 1315 (73$) Daclatasvir Generic 60 LE (3$) OMB/PAR Brand 3050 LE (170$) SOF/LDV Brand 3050 LE (170$) SOF/LDV Generic Not available Price of ribavirin 1200mg/d for a month is 125 LE (7$) in NCCVH EASL 2017 Seite 11
12 Debate: Do we need more HCV drugs?» More drugs, more competition and eventually lower prices.» Any special patient populations left?» Need for shorter treatment durations?» Need for better tolerated drugs?» Need for drugs with less drug-drug interactions?» How about treatment of DAA failures? Seite 12
13 SVR12 (%) High SVR in adult patients with HIV/HCV co-infection treated with DAAs ALLY-2: 1 GT 1 4, TN & TE SOF + DCV ION-4: 2 GT 1 or 4, TE & TN LDV/SOF TURQUOISE-1, part 2: 3 GT 1 or 4, TN and TE OMV/PTV/RTV + DSV ± RBV C-EDGE: 4 GT 1, 4 or 6, TN GRZ/EBV /101 51/52 TN TE 12 weeks 0 322/3 217/ weeks 12 or 24 weeks 0 210/ Weeks 1. Wyles D, et al. N Engl J Med 2015;373:714 25; 2. Naggie S, et al. N Engl J Med 2015;373:705 13; 3. Rockstroh JK, et al. IAS 2016; Abstract # 10333; 4. Rockstroh JK, et al. Lancet HIV 2015;2:e NOT HEAD-TO-HEAD COMPARISONS Studies included non-cirrhotic and cirrhotic patients. TE: treatment-experienced
14 EXPEDITION-I Study: Next Generation Direct-Acting Antivirals Glecaprevir (formerly ABT-493) pangenotypic NS3/4A protease inhibitor Coformulated: G/P Pibrentasvir (formerly ABT-530) pangenotypic NS5A inhibitor In vitro: 1,2 Clinical PK & metabolism: High barrier to resistance Potent against common NS3 polymorphisms (e.g., positions 80, 155, and 168) and NS5A polymorphisms (e.g., positions 28, 30, 31 and 93) Synergistic antiviral activity Once-daily oral dosing with food Minimal metabolism and primary biliary excretion Negligible renal excretion (<1%) G/P is co-formulated and dosed once daily as three 100 mg/40 mg pills for a total dose of 300 mg/120 mg Glecaprevir was identified by AbbVie and Enanta. 1.Ng TI, et al. Antimicrobial Agents and Chemotherapy; 2017 (in press). 2.Ng TI, et al. Abstract 636. CROI, 2014


15 EXPEDITION-1 Study: Objective and Study Design Objective» Evaluate the efficacy and safety of G/P for 12 weeks in patients with HCV GT1, 2, 4, 5 or 6 infection and compensated cirrhosis G/P 300 mg/120 mg N=146 0 Week 24 Week 36 Week 12 Open-label Treatment SVR12 assessment Patients were enrolled at 40 study sites in Belgium, Canada, Germany, South Africa, Spain, and the United States G/P is coformulated and dosed once daily as three 100 mg/40 mg pills for a total dose of 300 mg/120 mg. Forns X, et al. 52nd EASL; Amsterdam, Netherlands; April 19-23, Abst. GS-006.
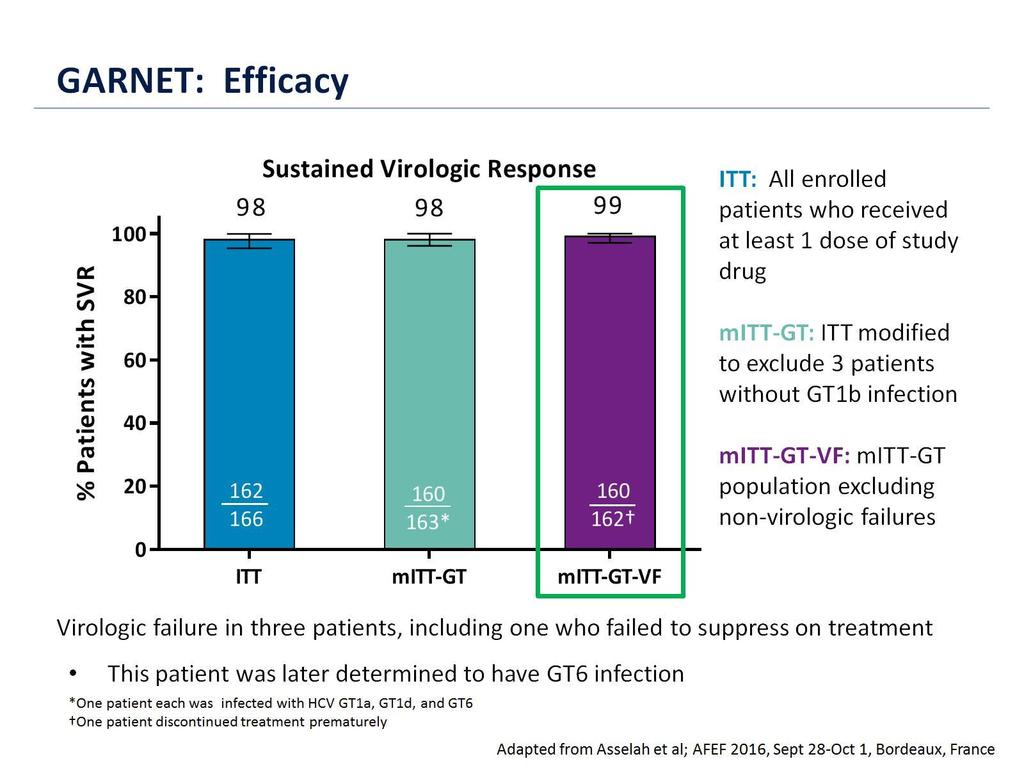
16 % Patients with SVR12 EXPEDITION-1 Study: SVR12 by Intent-to-Treat (ITT) Analysis GT1 GT2 GT4 GT5 GT6 Total *Patient with HCV GT1a infection relapsed at PTW8 - No treatment-emergent substitutions were present in NS3 - In NS5A, Y93N was present at baseline; Y93N, Q30R and H58D were present at the time of failure Forns X, et al. 52nd EASL; Amsterdam, Netherlands; April 19-23, Abst. GS-006.


17 SURVEYOR-II, Part 3: SVR12: GT3 98% of patients had HCV RNA <LLOQ by treatment week 4
18 SVR, % SVR12 (mfas) 100 Treatment- Treatment- naive experienced EBR/GZR + SOF + RBV (8 weeks) EBR/GZR + SOF (12 weeks) EBR/GZR + SOF (12 weeks) EBR/GZR + SOF + RBV (12 weeks) EBR/GZR + SOF (16 weeks) Relapse mfas excluded patients who discontinued treatment for reasons unrelated to study medication.
19 Any special patient populations left?» HIV coinfected (SVR >95%)» Renal insufficiency (SVR up to 99%)» Cirrhotics (SVR up to 99%)» GT3 treatment experineced with cirrhosis (SVR 96%)» Inherited blood disorders (SVR 94%)» Transplant patients (SVR >95%)» you name it Seite 19


20 So what does Nancy really think and that already in Seite 20
21 Debate: Do we need more HCV drugs?» More drugs, more competition and eventually lower prices.» Any special patient populations left?» Need for shorter treatment durations?» Need for better tolerated drugs?» Need for drugs with less drug-drug interactions?» How about treatment of DAA failures? Seite 21
22 SVR12 (%) 8-week LDV/SOF in non-cirrhotic, treatment naïve GT 1 patients: real-world confirmation of clinical data» *Two patients received LDV/SOF + RBV. LDV/SOF + RBV for 8 weeks is not licensed in the EU. ITT: intention-to-treat Real world virological response (>4000 patients) Post hoc analysis; per protocol; ITT analysis / / / / / 48 ION-3 ifi DHC-R Burman's US Com. pharmacy * -Centers 236/ 240 Kaiser LA 127/ 131 HCV Target 242/ 254 TRIO Cohort 1878/ 1975 VA 32/ 34 HEPA-C Registry 186/ 199 GECCO 238/ 258 Kaiser Permanente 1. Kowdley KV, et al. N Engl J Med 2014;370: ; 2. Buggisch P, et al. EASL 2016; Poster #SAT-243; 3. Buggisch P, et al. EASL 2016; Poster #SAT-241; 4. Qureshi K, et al. EASL 2016; Poster #SAT-192; 5. Marshall V, et al. AASLD 2015; Poster #1154; 6. Latt NL, et al. EASL 2016; Poster #SAT-227; 7. Terrault N, et al. AASLD 2015; Oral #94; 8. Curry M, et al. AASLD 2015; Poster #1046; 9. Ioannou GN, et al. Gastroenterology 2016;151:457 71; 10. Creso J, et al. EASL 2016; Poster #LBP-511; 11. Ingiliz P, et al. Clin Infect Dis 2016;doi: /cid/ciw567; 12. Lai JB, et al. EASL 2016; Poster #SAT-177
23

24 (2) non-inferiority (1) non-inferiority 2:1 Randomized ENDURANCE-3 Study: Objective and Study Design Treatment Period Arm A N = 233 G/P Post-treatment Period SVR12 Arm B N = 115 SOF + DCV SVR12 Arm C N = 157 G/P SVR Weeks Arm C: 8-week treatment duration Per discussion with regulatory authorities after phase 2 treatment data became available, an 8 week treatment Arm of G/P was added to the study design SVR12: Non-inferiority of 8 weeks of G/P compared to 12 weeks of G/P* *Endpoint was tested only after 12 weeks of G/P was determined non-inferior to 12 weeks of SOF + DCV Foster G, et al. 52nd EASL; Amsterdam, Netherlands; April 19-23, Abst. GS-007.
25 ENDURANCE-3 Study: Baseline Demographics and Clinical Characteristics Characteristic G/P 12 weeks N = 233 2:1 randomized Non-randomized SOF + DCV 12 weeks N = 115 G/P 8 weeks N = 157 Male, n (%) 121 (52) 52 (45) 92 (59) White race, n (%) 205 (88) 103 (90) 134 (85) Age, median years (range) 48 (22 71) 49 (20 70) 47 (20 76) BMI, median kg/m 2 (range) 25 (17 49) 25 (18 42) 26 (18 44) HCV RNA, median log 10 IU/mL (range) 6.1 ( ) 6.0 ( ) 6.1 ( ) History of injection drug use, n (%) 149 (64) 73 (63) 104 (66) Baseline fibrosis stage, n (%) F0 F1 201 (86) 97 (84) 122 (78) F2 12 (5) 8 (7) 8 (5) F3 20 (9) 10 (9) 27 (17) Subtype GT3a, n/n (%) * 226/229 (99) 113/113 (100) 154/155 (99) BMI, body mass index; DCV, daclatasvir; G/P, coformulated glecaprevir/pibrentasvir; GT, genotype; HCV, hepatitis C virus; SOF, sofosbuvir *HCV subtype determined by phylogenetic analysis; N = total number of patients with sequence data available Foster G, et al. 52nd EASL; Amsterdam, Netherlands; April 19-23, Abst. GS-007.
26 SVR12 (% Patients) ENDURANCE-3 Study: Results SVR12 by Intent-to-Treat (ITT) Analysis Treatment Duration G/P 12 weeks (1) non-inferior (2) non-inferior SOF + DCV 12 weeks G/P 8 weeks Non-inferiority: Lower bound of the confidence interval (CI) of the difference in SVR12 must be above -6%* (1) -1.2% (95% CI ) (2) -0.4% (97.5% CI ) Both G/P treatments met non-inferiority criteria for the primary endpoint *Conventional statistical methods were used in multiplicity comparison for determining non-inferiority Foster G, et al. 52nd EASL; Amsterdam, Netherlands; April 19-23, Abst. GS-007.
27 Debate: Do we need more HCV drugs?» More drugs, more competition and eventually lower prices.» Any special patient populations left?» Need for shorter treatment durations?» Need for better tolerated drugs?» Need for drugs with less drug-drug interactions?» How about treatment of DAA failures? Seite 27
28 DAAs were well-tolerated in clinical trials of HIV/HCV co-infected patients Adverse events common across all DAA regimens in HIV/HCV co-infection trials ALLY-2 DCV + SOF N=203 ION-4 LDV/SOF N=335 TURQUOISE-I Part 2 OMV/PTV/RTV + DSV ± RBV N=228 C-EDGE CO-INFECTION GRZ/EBV N=218 ASTRAL-5 SOF/VEL N=106 Fatigue 17% 21% 23% 13% 25% Headache 11% 25% 14% 12% 13% Diarrhoea 7% 11% 14% 7% 8% Nausea 13% 10% 20% 9% 7% D/C due to AE (2%) Wyles D, et al. N Engl J Med 2015;373:714 25; Rockstroh JK, et al. IAS 2016; Abstract # 10333; Naggie S, et al. N Engl J Med 2015;373:705 13; Rockstroh JK, et al. Lancet HIV 2015;2:e319 27; Brau N, et al. IAS 2016; Abstract #708 NOT HEAD-TO-HEAD COMPARISONS This table illustrate adverse events obtained between different regimens from different studies and are therefore not directly comparable as study populations are NOT matched
29 Debate: Do we need more HCV drugs?» More drugs, more competition and eventually lower prices.» Any special patient populations left?» Need for shorter treatment durations?» Need for better tolerated drugs?» Need for drugs with less drug-drug interactions?» How about treatment of DAA failures? Seite 29



30 Drug-drug Interactions between DAAs and ARVs Don`t undermine your own existence as a clinical pharmacologist.
31 Debate: Do we need more HCV drugs?» More drugs, more competition and eventually lower prices.» Any special patient populations left?» Need for shorter treatment durations?» Need for better tolerated drugs?» Need for drugs with less drug-drug interactions?» How about treatment of DAA failures? Seite 31
32 Re-treatment after failure to LDV/SOF 9 patients without SVR in ION-4 after 12 weeks of LDV/SOF Wk 0 Wk 12 Wk 24 Wk 36 LDV/SOF Failure N=9 LDV/SOF + RBV SVR12 GT NS5A RAVs Before Primary Study (%) NS5A RAVs at Virologic Rlapse After Primary Study (5) 1a None None Yes 1a None None Yes 1a L31M (>99), H58D (92) L31M (>99), H58D (92) Yes 1a Y93F (1), Y93N (10) Y93N (<99) Yes 1a L31M (>99), Y93N (<25) L31M (>99), Y93N (>99) Yes 1a* None Y93N (>99) Yes 1b Y93H (>99) L31I (11), Y93H (>99) Yes 1b None L31V (>99) Yes 1a None L31M (>99) No SRV12» SVR in 8/9» 1 relapse 4 weeks after EOT: GT1a, no cirrhosis Cooper C, et al. 23rd CROI; Boston, MA; February 22-25, Abst. 573.

33 % Patients with SVR12 (95% CI) C-SWIFT: Retreatment for 12 Weeks with EBR/GZR + SOF + RBV in GT1-infected Patients Who Relapsed on Short-duration DAA Therapy PURPOSE: Evaluate 12 weeks of EBR/GZR + SOF + RBV for HCV GT1-infected patients who failed prior treatment with EBR/GZR + SOF; shorter durations of 4, 6, or 8 weeks. RESULTS: SVR12 = 100% for retreatment of 12 weeks, regardless of cirrhosis, subgenotype, or baseline RAVs No discontinuations due to AEs or laboratory abnormalities The only AE occurring in > 10% of patients was fatigue (12%) SVR12: Overall and By Subgroup mfas / 23 Overall 18/ 18 No Cirrhosis 5/ 5 Yes Cirrhosis 15/ 15 4 weeks Prior treatment duration 6 or 8 weeks Prior treatment duration KEY MESSAGES: Addition of RBV, and lengthened treatment duration to 12 weeks improves SVR rates in patients who failed prior short-duration DAA therapy. If patients fail short-term treatment, other options are available. 8/ 8 5/ 5 No Baseline NS5A RAVs 18/ 18 Yes Baseline NS5A RAVs Excludes two patients lost to follow-up at Day 3 and treatment Week Lawitz E, et al. Presented at AASLD 2015; Poster #LB-12.
34 Debate: Do we need more HCV drugs?» More drugs, more competition and eventually lower prices. Price already down to 28$» Any special patient populations left? no» Need for shorter treatment durations? Already down to 8 weeks» Need for better tolerated drugs? DC in trials for adverse events < 1%» Need for drugs with less drug-drug interactions? All solvable with the help of a clinical pharmacologist» How about treatment of DAA failures? 3-drug combinations from 3 drug classes already available as salvage therapy Seite 34

35
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Is HCV drug resistance an issue?
 Is HCV drug resistance an issue? 5TH ASIAN CONFERENCE ON HEPATITIS&AIDS NANJING, CHINA 28-29 MAY 2016 FROM BASIC SCIENCE TO CLINICAL PRACTIC Jürgen Kurt Rockstroh Department of Medicine I, University Hospital
Is HCV drug resistance an issue? 5TH ASIAN CONFERENCE ON HEPATITIS&AIDS NANJING, CHINA 28-29 MAY 2016 FROM BASIC SCIENCE TO CLINICAL PRACTIC Jürgen Kurt Rockstroh Department of Medicine I, University Hospital
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
PIB. Next Generation Direct-Acting Antivirals. Collectively: G/P. Pibrentasvir (formerly ABT-530) pangenotypic NS5A inhibitor
 pangenotypic NS5A inhibitor") Surveyor-II, Part 3: Efficacy and Safety of Glecaprevir/Pibrentasvir (Abt-493/Abt-53) in Patients with Hepatitis C Virus Genotype 3 Infection with Prior Treatment Experience and/or Cirrhosis David L. Wyles,
Surveyor-II, Part 3: Efficacy and Safety of Glecaprevir/Pibrentasvir (Abt-493/Abt-53) in Patients with Hepatitis C Virus Genotype 3 Infection with Prior Treatment Experience and/or Cirrhosis David L. Wyles,
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Need to Assess HCV Resistance to DAAs: Is it Useful and When?
 Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Universal HCV treatment: Strategies for simplification
 Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
ICVH 2016 Oral Presentation: 28
 Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Management of HCV in Prior Treatment Failure
 Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
HIV/HCV coinfection. Jürgen K. Rockstroh, Department of Medicine I, Bonn University Hospital, Bonn, Germany
 HIV/HCV coinfection Jürgen K. Rockstroh, Department of Medicine I, Bonn University Hospital, Bonn, Germany Conflict of Interest Honoraria for lectures and/or consultancies from Abbott, AbbVie, Bionor,
HIV/HCV coinfection Jürgen K. Rockstroh, Department of Medicine I, Bonn University Hospital, Bonn, Germany Conflict of Interest Honoraria for lectures and/or consultancies from Abbott, AbbVie, Bionor,
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
HCV Update from AASLD 2016
 HCV Update from AASLD 2016 Ahmed Elsharkawy Consultant Hepatologist QE Birmingham Secretary and Chair-Elect of BVHG BHIVA/BVHG Feedback Meeting November 2016 Speaker Name Ahmed Elsharkawy Statement Speaking
HCV Update from AASLD 2016 Ahmed Elsharkawy Consultant Hepatologist QE Birmingham Secretary and Chair-Elect of BVHG BHIVA/BVHG Feedback Meeting November 2016 Speaker Name Ahmed Elsharkawy Statement Speaking
SURVEYOR-II Part 2 Study Design
 HIGH SVR RATES WITH + CO-ADMINISTERED FOR 8 WEEKS IN NON-CIRRHOTIC PATIENTS WITH HCV GENOTYPE 3 INFECTION A.J. Muir, S. Strasser, S. Wang, S. Shafran, M. Bonacini, P. Kwo, D. Wyles, E. Gane, S.S. Lovell,
HIGH SVR RATES WITH + CO-ADMINISTERED FOR 8 WEEKS IN NON-CIRRHOTIC PATIENTS WITH HCV GENOTYPE 3 INFECTION A.J. Muir, S. Strasser, S. Wang, S. Shafran, M. Bonacini, P. Kwo, D. Wyles, E. Gane, S.S. Lovell,
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Treatment of HCV : 100 % cure?
 Treatment of HCV : % cure? PHC 8 PARIS January 5th, 8 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief ISERM UMR 49, Hôpital Beaujon, Clichy, France. PHC 8 - www.aphc.info Disclosures Employee
Treatment of HCV : % cure? PHC 8 PARIS January 5th, 8 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief ISERM UMR 49, Hôpital Beaujon, Clichy, France. PHC 8 - www.aphc.info Disclosures Employee
Do We Need New HCV Drugs? YES
 Do We Need New HCV Drugs? YES Nancy Reau, MD Professor of Medicine Chief, Section of Hepatology Associate Director, Solid Organ Transplantation Rush University Medical Center Disclosures Consultation:
Do We Need New HCV Drugs? YES Nancy Reau, MD Professor of Medicine Chief, Section of Hepatology Associate Director, Solid Organ Transplantation Rush University Medical Center Disclosures Consultation:
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Case. 63 year old woman now with:
 Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
NEXT GENERATION DIRECT-ACTING ANTIVIRALS
 EFFICACY AND SAFETY OF GLECAPREVIR/PIBRENTASVIR IN PATIENTS CO-INFECTED WITH HEPATITIS C VIRUS AND HUMAN IMMUNODEFICIENCY VIRUS-1: THE EXPEDITION-2 STUDY J. Rockstroh, K. Lacombe, R. Viani, C. Orkin, D.
EFFICACY AND SAFETY OF GLECAPREVIR/PIBRENTASVIR IN PATIENTS CO-INFECTED WITH HEPATITIS C VIRUS AND HUMAN IMMUNODEFICIENCY VIRUS-1: THE EXPEDITION-2 STUDY J. Rockstroh, K. Lacombe, R. Viani, C. Orkin, D.
Learning Objective. After completing this educational activity, participants should be able to:
 Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Cases: Management of Hepatitis C in Prior Treatment Failure
 Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1
 Phase 3 Treatment-Naïve and Treatment-Experienced Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1 EXPEDITION-1: Study Features EXPEDITION-1 Trial Design: Open-label, single-arm,
Phase 3 Treatment-Naïve and Treatment-Experienced Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1 EXPEDITION-1: Study Features EXPEDITION-1 Trial Design: Open-label, single-arm,
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
Shorter Durations and Pan-genotypic Regimens The Final Frontier. Professor Greg Dore
 Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Expert Perspectives: Best of HCV from EASL 2015
 Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York
 Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
Felizarta, Bo Fu, Teresa Ng, Chih-Wei Lin, Federico Mensa Abstract 253. Pibrentasvir (formerly ABT-530) pangenotypic NS3/4A protease inhibitor
 pangenotypic NS3/4A protease inhibitor") ENDURANCE-1: A Phase 3 Evaluation of the Efficacy and Safety of 8- versus 12-week Treatment with Glecaprevir/ Pibrentasvir (formerly ABT-493/ABT-53) in HCV Genotype 1 Infected Patients with or without
ENDURANCE-1: A Phase 3 Evaluation of the Efficacy and Safety of 8- versus 12-week Treatment with Glecaprevir/ Pibrentasvir (formerly ABT-493/ABT-53) in HCV Genotype 1 Infected Patients with or without
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
HCV: The next 18 months. David L. Wyles, M.D. Associate Professor of Medicine UCSD
 HCV: The next 18 months David L. Wyles, M.D. Associate Professor of Medicine UCSD FIRST, A LOOK BACK WHAT DID I SAY LAST YEAR? My predictions for genotype 1: Multiple highly efficacious, well-tolerated,
HCV: The next 18 months David L. Wyles, M.D. Associate Professor of Medicine UCSD FIRST, A LOOK BACK WHAT DID I SAY LAST YEAR? My predictions for genotype 1: Multiple highly efficacious, well-tolerated,
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon
 HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon Supported by educational grants from AbbVie; Bristol-Myers Squibb; Gilead Sciences; Janssen Therapeutics; Merck & Co., Inc; and ViiV
HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon Supported by educational grants from AbbVie; Bristol-Myers Squibb; Gilead Sciences; Janssen Therapeutics; Merck & Co., Inc; and ViiV
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos
 Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran
 A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
HIV-HCV coinfection. Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland
 HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Glecaprevir-Pibrentasvir in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2)
") Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Current HCV Treatment by Genotype Ira M. Jacobson, MD
 Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
10/21/2016. David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado
 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado FORMATTED: 1/3/16
Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado FORMATTED: 1/3/16
David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado
 FORMATTED: 1/3/16 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? Atlanta, Georgia: October 2, 216 David L. Wyles, MD Chief, Division of Infectious Disease Denver Health
FORMATTED: 1/3/16 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? Atlanta, Georgia: October 2, 216 David L. Wyles, MD Chief, Division of Infectious Disease Denver Health
Update on Hepatitis C. Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017
 Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
What Should We Do With Difficult to Treat HCV Populations?
 What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Study Design - GT 1 Retreatment
 Retreatment of Patients Who Failed 8 or 12 Weeks of Ledipasvir/Sofosbuvir-Based Regimens With Ledipasvir/Sofosbuvir for 24 Weeks Eric Lawitz, Steven Flamm, Jenny C. Yang, Phillip S. Pang, Yanni Zhu, Evguenia
Retreatment of Patients Who Failed 8 or 12 Weeks of Ledipasvir/Sofosbuvir-Based Regimens With Ledipasvir/Sofosbuvir for 24 Weeks Eric Lawitz, Steven Flamm, Jenny C. Yang, Phillip S. Pang, Yanni Zhu, Evguenia
Glecaprevir-Pibrentasvir in Non-Cirrhotic Genotype 2 ENDURANCE-2
 Phase 3 Treatment Naïve or Experienced Glecaprevir-Pibrentasvir in Non-Cirrhotic Genotype 2 ENDURANCE-2 *ENDURANCE-2: Study Features ENDURANCE-2 Trial Design: Randomized, double-blind, placebo-controlled
Phase 3 Treatment Naïve or Experienced Glecaprevir-Pibrentasvir in Non-Cirrhotic Genotype 2 ENDURANCE-2 *ENDURANCE-2: Study Features ENDURANCE-2 Trial Design: Randomized, double-blind, placebo-controlled
Failure after treatment with DAAs: What to do? Marseille France 2-3 th June 2016
 Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Virological tools for hepatitis C: re-treatment and resistance. Joop Arends Will Irving. by author
 Virological tools for hepatitis C: re-treatment and resistance Joop Arends Will Irving Disclosures Joop Arends Advisory board: Gilead, Abbvie, Janssen, MSD, BMS (research) grants: Abbvie, BMS, MSD and
Virological tools for hepatitis C: re-treatment and resistance Joop Arends Will Irving Disclosures Joop Arends Advisory board: Gilead, Abbvie, Janssen, MSD, BMS (research) grants: Abbvie, BMS, MSD and
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
Disclosures. Advanced HCV management. Overview. Renal failure 1/10/2018. Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH
 Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Management of HCV in Decompensated Liver Disease
 Management of HCV in Decompensated Liver Disease Michael P. Manns Hannover Medical School (MHH) Department of Gastroenterology, Hepatology and Endocrinology Helmholtz Center for Infection Research (HZI),
Management of HCV in Decompensated Liver Disease Michael P. Manns Hannover Medical School (MHH) Department of Gastroenterology, Hepatology and Endocrinology Helmholtz Center for Infection Research (HZI),
IFN-free for Genotype 1 HCV: the current landscape. Prof. Graham R Foster
 IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
My HCV patient is co-infected with HIV: how to manage?
 EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
HCV Resistance Associated variants: impact on chronic hepatitis C treatment
 HCV Resistance Associated variants: impact on chronic hepatitis C treatment Dr. Stéphane Chevaliez Associate Professor of Medicine at the University of Paris-Est. History of Resistance in HCV Concern Only
HCV Resistance Associated variants: impact on chronic hepatitis C treatment Dr. Stéphane Chevaliez Associate Professor of Medicine at the University of Paris-Est. History of Resistance in HCV Concern Only
Hepatitis C: New Therapies in
 Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Individual Optmizaton of therapy. Graham R Foster Professor of Hepatology QMUL
 Individual Optmizaton of therapy Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novarts, Springbank,
Individual Optmizaton of therapy Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novarts, Springbank,
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
NS5A inhibitors: ideal candidates for combination?
 NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
Updates on the AASLD/IDSA HCV Guidance
 Updates on the AASLD/IDSA HCV Guidance Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University School of Medicine Durham, North Carolina Learning Objectives After attending this presentation,
Updates on the AASLD/IDSA HCV Guidance Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University School of Medicine Durham, North Carolina Learning Objectives After attending this presentation,
Treating Hepatitis C in Patients with Advanced Renal Disease
 Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
New York State HCV Provider Webinar Series. Treatment of HCV/HIV Co-Infection
 New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Objectives Review the epidemiology of HCV and HIV/HCV co-infection Discuss the burden of HIV/HCV co-infection Discuss the treatment
New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Objectives Review the epidemiology of HCV and HIV/HCV co-infection Discuss the burden of HIV/HCV co-infection Discuss the treatment
New Hepatitis C Antivirals
 New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support