Prescribing Opioid for. Opioid Naïve Patients AN OPIOD RX
|
|
|
- Dwain Jacobs
- 6 years ago
- Views:
Transcription
1 Prescribing Opioid for Opioid Naïve Patients AN OPIOD RX
2 Optimal Approach to Initiating Opioids for Chronic Non-Cancer Pain AN OPIOID RX Assessment biopsychosocial Non-opioid treatments Opioid risks vs. benefits Psychological assessment Informed consent (signed agreement) Order Urine Drug Testing (and other labs as required) Individualize opioid titration 50 mg and 90 mg MED Document outcomes of treatment Reassess and monitor regularly exit strategy if goals not met or problematic behaviours.
3 Assessment biopsychosocial Do a comprehensive assessment to ensure opioids are a reasonable choice and to identify risk/benefit balance for the patient Document results of history, physical exam and results of relevant investigations Formulate Differential and Working Diagnosis Document Pain Diagnosis (e.g. predominantly nociceptive or neuropathic) Assess Home Environment (e.g. co-inhabitants risk of misuse of Opioids) Involve family and/or caregiver in management (e.g. obtain consent from patients to communicate with family) /.
4 Non-Opioid treatments Maximize and Continue with Non-pharmacological therapies, including patient self-management and life style management (weight loss, exercise, nutrition, sleep hygiene) Non-Opioid analgesics and/or adjuvants, as appropriate Review Patient co-morbidities (e.g. renal function, cardiovascular risk, ) Concomitant medications with respect to potential drug interactions /.
5 Opioid risks vs. benefits Inform patient of their role in safe use and monitoring effectiveness Set Goals of Treatment (Improved Functions) and Realistic Expectations (e.g. 30 % decrease in pain scores) Inform patient of potential Nausea, constipation, drowsiness, dizziness, itching Adverse Effect on driving and operating machinery Medical complications such as sexual dysfunction, sleep apnea, opioidinduced hyperalgesia, and hormonal effects Overdose, diversion, addiction, withdrawal Potentiation of harm with alcohol.
6 Psychological assessment Consider a tool to diagnosis and monitor mental disorders (e.g. PHQ- 9 for depression) Assess both any past and present mental disorders Treat any present mental disorders before initiating Opioids Assess Suicide and/or Accidental overdose risk based on any mental disorders Taper or avoid benzodiazepines if Opioids are to be initiated Assess Sleep and Environmental Stressors (e.g. work environment)
7 Informed consent (signed agreement) Obtain Informed Consent about the prescribing of Opioids Discuss and have patient review/sign an Opioid Treatment Agreement Be explicit about characterizing opioid prescribing as a trial and that opioid therapy will be be discontinued if it is not effective or benefits are outweighed by harms
8 Order Urine Drug Testing (and other labs as required) Consider using urine drug screening (UDS) To set a baseline measure of substance use that may help assess risk for addiction For ongoing monitoring of the patient s compliance with Opioids prescribed Point of care testing, normal lab urine drug testing and gas chromatography can all be useful depending on the clinical situation
9 Individualize Opioid titration Initiate with a low dose; increase gradually; monitor Opioid effectiveness and recognize optimal dose. Watch for any emerging risks/complications to prevent unwanted outcomes including misuse and addiction Track daily dose in morphine equivalents (MED) per day Consult a colleague if daily morphine equivalent dose exceeds 90 mg Consider Immediate Release vs. Controlled Release Consider Abuse- Deterrent Formulation vs. Non Abuse-Deterrent Oral vs. Transdermal (Fentanyl must not be used in Opioid Naïve Patients)
10 Document outcomes of treatment Analgesic Effect and Score Adverse Effects Discussed and attempts to manage Affect (mood and cognitive function) Aberrant Behaviour (lost Rx s, requests for early refills) Activities of Daily Living (Effect of Treatment)
11 Reassess and monitor regularly Function and Pain Scores ( e.g. Brief Pain Inventory) Employment Recreational Activities Interpersonal Relationships Overall Quality of Life Any evidence of abuse, misuse or diversion
12 Exit Strategy A trial of opioid therapy implies an exit strategy is understood from the beginning Opioid Treatment Agreement indicates common reasons for either reduction of opioid dose (tapering to lower dose) or stopping opioids (tapering to Zero) o o o o o Misuse, Abuse or Diversion of Opioids Opioid Tolerance Opioid Induced Hyperalgesia Development of Co-Morbid Medical Conditions (sleep apnea, endocrine issues) Adverse Effects (constipation, other GI issues, cognitive issues,
13 Prescribing Opioid for Legacy Patients OPIOIDSAFE
14 Managing Opioids for CNCP (Legacy Patients) Obtain and Review Informed Consent Patient Risk Factors for Abuse and Harm Assessed and Re-Assessed Inform patient of Potential Harms and Adverse Effects Order Urine Drug Testing Investigate new and/or ongoing symptoms and signs Determine if Opioid Formulation or Type is to be changed Society concerns and Social Situation Reviewed Attempt to Taper Opioid Dose Function and Pain Scores Evaluated Exit Strategy Reviewed.
15 Obtain Informed Consent Obtain Informed Consent about the prescribing of Opioids Discuss and have patient review/sign an Opioid Treatment Agreement Maximize and Continue with Non-pharmacological therapies, including patient self-management and life style management (weight loss, exercise, nutrition, sleep hygiene) Non-Opioid analgesics and/or adjuvants, as appropriate /.
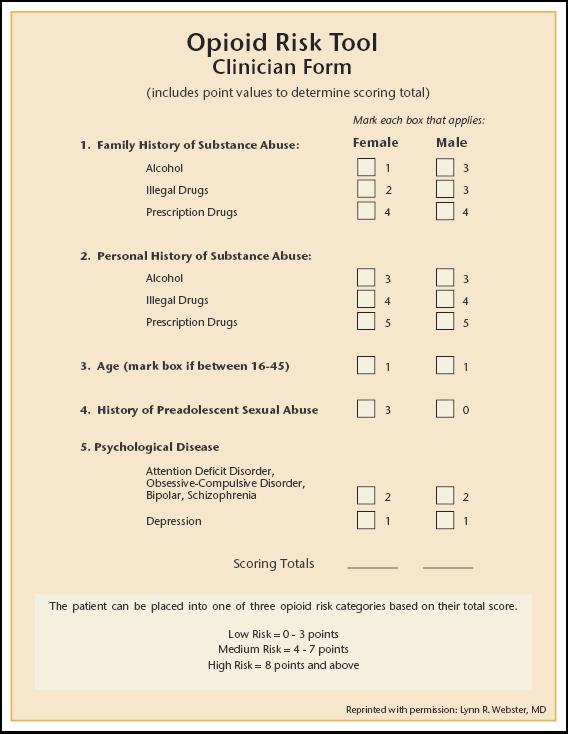
16 Patient Risk Factors for Abuse and Harm Assessed Medical co-morbidities are evaluated/addressed (e.g. sleep apnea, renal insufficiency,pregnancy, elderly) Mental health and psychosocial co-morbidities are evaluated/addressed For patients taking benzodiazepines, particularly for elderly patients, consider a trial of tapering Use a screening tool to determine the patient s risk for opioid addiction The Opioid Risk Tool (ORT) is widely used Treatment modified according to level of risk /.
17 Inform Patient of Potential Harms Inform patient of their role in safe use and monitoring effectiveness Inform patient of potential Nausea, constipation, drowsiness, dizziness, itching Adverse Effect on driving and operating machinery Medical complications such as sexual dysfunction, sleep apnea, opioidinduced hyperalgesia, and hormonal effects Overdose, diversion, addiction, withdrawal Potentiation of harm with alcohol.
18 Order Urine Drug Testing Consider using urine drug screening (UDS) To set a baseline measure of substance use that may help assess risk for addiction For ongoing monitoring of the patient s compliance with opioids prescribed Point of care testing, normal lab urine drug testing and gas chromatography can all be useful depending on the clinical situation
19 Investigate new and/or ongoing symptoms and signs Review History and Physical Exam Evaluate any new symptoms or exam abnormalities Review previous investigations Search for any treatable causes of increased pain and/or decreased function Consider specialist referral (orthopedics, rheumatology, etc.) Order appropriate testing based on results of clinical evaluation
20 Determine if Opioid Opioid Formulation or Type is to be Consider Immediate Release vs. Controlled Release Weak vs. Strong Opioids Consider Abuse- Deterrent Formulation vs Non Abuse-Deterrent Oral vs. Transdermal (Fentanyl must not be used in Opioid Naïve Patients)
21 Society concerns and Social Situation Reviewed Assess Home Environment (e.g. co-inhabitants risk of misuse of Opioids) Involve family and/or caregiver in management (e.g. obtain consent from patients to communicate with family Assess compliance (e.g. dosettes) Consider Take Home Naloxone Kit for patients at high risk of overdose Review storage of Opioids Consider abuse-deterrent formulations where appropriate
22 Attempt to Taper Opioid Dose Periodically discuss with patient and attempt to Taper opioid dose, especially if daily dose of opioid is above 90 MED Taper slowly in most cases (10 % per week) Provide patient with information sheet on dealing with symptoms of Opioid Withdrawal Goal is to reduce daily Opioid dose to dose that provides optimal pain relief and reduces risk of harm Consider Opioid Rotation as a method to reduce total daily Opioid Dose
23 Function Assessment and Re-assessment Consider a questionnaire ( e.g. Brief Pain Inventory) Employment Recreational Activities Interpersonal Relationships Overall Quality of Life
24 Exit Strategy A trial of opioid therapy implies an exit strategy is understood from the beginning Opioid Treatment Agreement indicates common reasons for either reduction of opioid dose (tapering to lower dose) or stopping opioids (tapering to Zero) o o o o o Misuse, Abuse or Diversion of Opioids Opioid Tolerance Opioid Induced Hyperalgesia Development of Co-Morbid Medical Conditions (sleep apnea, endocrine issues) Adverse Effects (constipation, other GI issues, cognitive issues,

25 Urine Drug Testing (UDT) in Pain Management Nov 5, 2017
26 Learning Objectives How and when to use urine drug testing (UDT) as part of a comprehensive management plan when prescribing opioids for chronic non-cancer pain Discuss how to manage unexpected UDT results

27 Urine Drug Testing (UDT) Management tool for patients treated with controlled substances or at risk for substance use May use UDT as an option for assessment and should be aware of benefits and limitations, appropriate test ordering and interpretation, and have a plan to use results
28 Prior to UDT Inform the patient Take careful history of medication/drug use in the past week Collect the sample in physicians office; ensure proper labelling

29 Point of Care Testing Rapid test performed in clinic e.g. urine dipsticks, cups Immunoassay drug screens are designed to classify substances as either present or absent according to a predetermined cut-off threshold When the amount of drug in the urine sample is equal to or exceeds the cut off concentration of a particular device, the outcome is a positive result POINT OF CARE (POC) LABORATORY TESTING COMPARISON

30 Laboratory Testing Specimen sent to laboratory Gas or Liquid Chromatography/ Mass Spectrometry is a more definitive laboratory based procedure to identify specific drug and/or metabolites and is needed in 3 instances: To specifically identify the drug; for example, that morphine is the opiate causing the positive immunoassay response To identify drugs not otherwise included in other testing To contest results disputed by the patient POINT OF CARE (POC) LABORATORY TESTING COMPARISON
31 Comparison - ADVANTAGES Point of Care -Immunoassay Rapid Results Concurrently test for multiple drug classes Very responsive for morphine and codeine Laboratory - Chromatography Identifies specific drug Confirmation of results More accurate for semisynthetic and synthetic opioids Does not cross react with poppy seeds POINT OF CARE (POC) LABORATORY TESTING COMPARISON
32 Validation Patients may tamper with urine samples to hide aberrant behaviours by: adding adulterants diluting the sample substituting another individuals sample for their own ingesting excessive water or diuretics prior to giving a sample Tests performed to improve the reliability of urine sample results NORMAL CHARACTERISTICS OF A URINE SPECIMEN Temperature (within 4 mins) Degrees Celcius ph Urinary Creatinine >20 mg/dl Specific Gravity >1.003
33 What To Do With Abnormal UDT Results: General Approach Take careful history of medication/drug use in the past week and discuss openly with the patient without being accusatory (potential for false positive and false negative) Check with lab re: potential error What kind of urine test was done? Interpret results in the context of the patient s clinical presentation and assessments Possibly ask the lab to re-run the sample with chromotgraphy if response still unclear UDT, urine drug test.

34 Unexpected Results Case Table of Contents 1 Is the patient taking the opioid I prescribed? 2 I didn t prescribe that! 3 I didn t expect to find that in your urine sample! 4 Did my patient tamper with the urine sample?
35 Unexpected Results Case 1 Is the patient taking the opioid I prescribed?
36 John 39 year old male Currently taking CR oxycodone resistant to crushing 40 mg q12h for chronic back pain On duloxetine 60 mg daily for some neuropathic features with effect Using some quetiapine 25 qhs to sleep ORT score: 8 1 for age 4 for use of THC in college, enough that he failed a semester, then righted himself and graduated, now denies using any 3 for Dad having an alcohol problem; folks split up when he was young due to it.

37 38
38 You do a routine urine on visit today Shows THC Negative for oxycodone, TCAs, benzodiazepines Now what do you do?
39 Would you? A) Fire him as he is lying to you? B) Tell him that you can no longer prescribe opioids as he is not taking them anyways? C) Confront him about the THC? D) Check when he last took CR oxycodone resistant to crushing? E) Call the lab to check the results? Take careful history of medication/drug use in the past week and discuss openly with the patient without being accusatory
40 Available at: Interpreting Unexpected Results of Urine Drug Screens Unexpected Result UDS negative for prescribed opioid Possible Explanations False negative Non-compliance Diversion Actions for the Physician Table B-3.1 Repeat test using chromatography; specify the drug of interest (e.g. oxycodone often missed by immunoassay) Take a detailed history of the patient s medication use for the preceding 7 days (e.g. could learn that patient ran out several days prior to test) Ask patient if they ve given the drug to others Monitor compliance with pill counts
41 John Restarted marijuana use and problems at work and home Financial issue selling CR oxycodone and some quetiapine CR oxycodone discontinued (should this be tapered?) Quetiapine prescribing decreased to 7days supply Offered resources for drug counselling and treatment programs Revised ORT score - High Risk Regular and random UDT
42 Unexpected Results Case 2 I didn t prescribe that!
43 Mary 66 year old female Spinal stenosis 2 failed surgeries in 1999 and 2006 Intolerant of NSAIDS/ COX-2 No personal of family history of drugs or alcohol No history of mental health issues
44 Mary Has taken acetaminophen 650 QID on a regular basis Reports constipation with acetaminophen/codeine 30mg (not filled Rx in 1 year) Reports significantly decreased QoL over last 6 months After exhausting more physical and psychological modalities, you are considering a trial of oxycodone 5mg
45 Mary Baseline UDT recommendation roadmap Do this on everyone UDS immunoassay is positive for benzodiazepines and opioids
46 Mary Now what do you do? Take careful history of medication/drug use in the past week and discuss openly with the patient without being accusatory
47 Available at: Interpreting Unexpected Results of Urine Drug Screens Table B-3.1 Unexpected Result Possible Explanations Actions for the Physician UDS positive for nonprescribed opioid or benzodiazepines False positive. Patient acquired opioids from other sources (doubledoctoring, street ) Repeat UDS regularly Ask the patient if they accessed opioids from other sources Assess for opioid misuse/addiction (See Guideline, Part B, Recommendation 12) Review/revise treatment agreement
48 Known Agents To Cause Interference in Urine Drug Test Results Opioids Marijuana Cocaine Amphetamines Benzodiazepines Dextromethorphan Diphenhydramine (methadone assay only) Poppy seeds Quinine Quinolone antibiotics Rifampin Verapamil (methadone assay only) Efavirenz Hemp seed NSAIDs PPIs Tolmetin Coca leaf tea Amantadine Bupropion Chlorpromazine Desipramine Labetalol Methylphenidate Phentermine Phenylephrine Pseudoephedrine Ranitidine Selegiline Tolmetin Trazodone Typical antipsychotics Oxaprozin Sertraline NSAID, non-steroidal anti-inflammatory drug. PPI, proton pump inhibitor. Adapted from Peppin JF, et al. Pain Med 2012;13: , Reisfield et al Ann Clin Lab Med 1997, Piergies et al Arch Path Lab Med 1997
49 Mary Explanation of Mary's results: Benzodiazepines: Occasionally takes her sisters diazepam 5mg pills Uses acetaminophen/codeine 8mg on a regular basis (up to 8 per day)
50 Mary Explanation of Mary's results: Benzodiazepines: Diazepam metabolizes to nordiazepam, temazepam and oxazepam. Opioids Codeine metabolizes to morphine
51 Benzodiazepines and Opioids Increases the risk of sedation, overdose, and diminished function in all patients, especially as age advances Benzodiazepines increase opioid toxicity and risk of overdose Canadian Guideline for Safe and Effective Use of Opioids for CNCP Part B
52 Mary The presence of a substance that we are not expecting to find can be used to educate patients on safety of drug interactions and toxicity Mary was counseled on the danger of acetaminophen toxicity and use of benzodiazepines Additional counseling points: Definition of misuse Information on safe storage, no sharing, safe disposal, etc. Opioid Treatment Agreement
53 Mary Treatment Plan Not start oxycodone prescriptions for now Explore reasons for benzodiazepine use and possible nonbenzodiazepine treatments for this (medication, psychological, behavioural) Repeat urine test in 3-4 weeks to ensure benzodiazepines are now negative (diazepam can remain positive for 3 weeks) Ensure Mary's daily acetaminophen intake is below a level of concern
54 Unexpected Results Case 3 I didn t expect to find that in your urine sample!
55 Frank 34 year old male C6-7 fracture from snowmobile accident subsequent fusion C5 to T1 PMHx ADD SHx Recently separated with 2 children Smoker 1 ppd ETOH max 3 per day and 15 per week Denies street drug use FHx mental illness - ADD
56 Frank Meds Oxycodone-acetaminophen 1-2 Q4h PRN 8 per day Meloxicam 15mg PO Qdaily Tx No change with physio, chiro, acupuncture VAS Neck pain 8/10 radiating to trapezius and shoulder bilaterally
57 Frank CAGE-AID Low Risk Opioid Risk Tool 4/7 moderate risk Male age Hx of ADD 2 Current depression 1
58 Assessment UDS immunoassay in office Opiates EDDP Oxycodone Cocaine TCA - negative negative positive positive negative Now what do you do? Take careful history of medication/drug use in the past week and discuss openly with the patient without being accusatory
59 Available at: Interpreting Unexpected Results of Urine Drug Screens Table B-3.1 Unexpected Result Possible Explanations Actions for the Physician UDS positive for illicit drugs (e.g. cocaine, cannabis) False positive Patient is occasional user or addicted to the illicit drug Cannabis is positive for patients THC:CBD (Sativex ) or using medical marijuana Repeat UDS regularly Assess for abuse/addiction and refer for addiction treatment as appropriate Ask about medical prescription of THC:CBD or medical marijuana access program
60 Known Agents To Cause Interference in Urine Drug Test Results Opioids Marijuana Cocaine Amphetamines Benzodiazepines Dextromethorphan Diphenhydramine (methadone assay only) Poppy seeds Quinine Quinolone antibiotics Rifampin Verapamil (methadone assay only) Efavirenz Hemp seed NSAIDs PPIs Tolmetin Coca leaf tea Amantadine Bupropion Chlorpromazine Desipramine Labetalol Methylphenidate Phentermine Phenylephrine Pseudoephedrine Ranitidine Selegiline Tolmetin Trazodone Typical antipsychotics Oxaprozin Sertraline NSAID, non-steroidal anti-inflammatory drug. PPI, proton pump inhibitor. Adapted from Peppin JF, et al. Pain Med 2012;13: , Reisfield et al Ann Clin Lab Med 1997, Piergies et al Arch Path Lab Med 1997
61 Frank Admitted to cocaine use intermittently Offered resources for drug counselling and treatment programs Revised ORT score - High Risk Regular and random UDT Treated with non opioid pharmaceuticals and modalities; or Structured opioid treatment with tight boundaries
62 Random UDTs When a patient steps out of bounds Explain need for good communication system patient cell # or answering system After seeing pt, choose some random dates and record on chart Receptionist writes down in a daily TO-DO list and calls pt by 10:00am to come in Patient has 24hrs to comply or violation
63 What if? He does not admit to the use? Denies it vehemently? Gets angry and defensive? What are your next options?
64 Unexpected Results Case 4 Did my patient tamper with the urine sample? If there is a will, there is a way Misuse, Abuse, and Diversion of prescription medications are great motivators to tamper with a UDT
65 Emma 57 year old female Chronic low back pain Diabetic polyneuropathy Rx with fentanyl transdermal patch 50ug/72 hours Pregabalin 150mg BID Nortriptyline 25mg for sleep and pain
66 Emma ORT Low Score of 2 as son has a history of drug abuse Opioid treatment agreement signed Never asks for early refills Never loses meds Random UDT annually negative for illicit drugs Always negative for fentanyl but active patch and old patch remnants seen on body
67 Emma Annual UDT January 2016 Negative for illicit drugs Negative for opioids Negative for fentanyl Specific Gravity (Normal is )
68 Emma Is Emma taking her fentanyl? Has her urine sample been tampered with? How else can you test for tampering? How do you address any concerns with Emma? Now what do you do? Take careful history of medication/drug use in the past week and discuss openly with the patient without being accusatory
69 Interpreting Unexpected Results of Urine Drug Screens Table B-3.1 Unexpected Result Possible Explanations Actions for the Physician Urine creatinine is lower than 2-3 mmol/liter (>20 mg/dl), specific gravity is <1.003 or sample is cold Patient added water to sample Delay in handling sample (urine cools within minutes) Repeat UDS Consider supervised collection or temperature testing Take a detailed history of the patient s medication use for the preceding 7 days Review/revise treatment agreement Available at:
 32-38 Degrees")
70 Validation Patients may tamper with urine samples to hide aberrant behaviours by: adding adulterants diluting the sample substituting another individuals sample for their own ingesting excessive water or diuretics prior to giving a sample Tests performed to improve the reliability of urine sample results NORMAL CHARACTERISTICS OF A URINE SPECIMEN Temperature (within 4 mins) Degrees Celcius ph Urinary Creatinine >20 mg/dl Specific Gravity >1.003
71 Emma Repeat UDS supervised if possible (female staff to observe) Emma admits that she is only using acetaminophen/codeine 8mg Her son (a known drug abuser) has been stealing her fentanyl patches and usually makes sure she has a new patch on the day before she sees you What do you do now?
72 Emma Discuss medication safety with Emma? Alternate plans for storage, or daily dispensing Consider changing medication to lower abuse risk or ingested with daily dispensing? Consider personal safety ramifications for Emma? Offer resources for support and safety plan. Consider legal issues in regards to the son? Plans may include other community resources. Consider Emma s safety in dealing with her son. Review patient responsibilities regarding the Opioid treatment agreement
73 Summary UDS is a recommendation in The Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain UDS point of care immunoassay and laboratory chromatography have different advantages/disadvantages and limitations Your first action with an unexpected result should be Take careful history of medication/drug use in the past week and discuss openly with the patient without being accusatory Each type of unexpected result has a DDx and appropriate physician actions
Urine Drug Testing (UDT) to Monitor Opioid Use. Feb 2018
 to Monitor Opioid Use. Feb 2018") Urine Drug Testing (UDT) to Monitor Opioid Use Feb 2018 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Urine Drug Testing (UDT) to Monitor Opioid Use Feb 2018 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Urine Drug Testing (UDT) in Pain Management. Nov 27, 2017
 in Pain Management. Nov 27, 2017") Urine Drug Testing (UDT) in Pain Management Nov 27, 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Urine Drug Testing (UDT) in Pain Management Nov 27, 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Urine Drug Testing (UDT) in Pain Management. Nov 5, 2017
 in Pain Management. Nov 5, 2017") Urine Drug Testing (UDT) in Pain Management Nov 5, 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Urine Drug Testing (UDT) in Pain Management Nov 5, 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Approaches to Responsible Opioid Prescribing. The Opioid Naïve Patient
 Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Urine Drug Testing Methods 3-5
 Urine Drug Testing Methods 3-5 Type of Test Logistics Pearls Initial Screening Test: Immunoassay Confirmatory Test: Gas chromatography-mass spectrometry (GCMS) + or Liquid chromatography-mass spectrometry
Urine Drug Testing Methods 3-5 Type of Test Logistics Pearls Initial Screening Test: Immunoassay Confirmatory Test: Gas chromatography-mass spectrometry (GCMS) + or Liquid chromatography-mass spectrometry
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
3/8/2018. Reasons for Doing UDT. UDT: A Tool in Risk Assessment. Faculty/Presenter Disclosure. Urine Drug Testing in Chronic Pain Management
 Urine Drug Testing in Chronic Pain Management March 8, 2018 Faculty/Presenter Disclosure Faculty: Andrew J Smith, MDCM Relationships with commercial interests: None to report Andrew J Smith, MDCM Staff
Urine Drug Testing in Chronic Pain Management March 8, 2018 Faculty/Presenter Disclosure Faculty: Andrew J Smith, MDCM Relationships with commercial interests: None to report Andrew J Smith, MDCM Staff
Urine Drug Testing. Methadone/Buprenorphine 101 Workshop. Ron Joe, MD, DABAM December 10, 2016
 Urine Drug Testing Methadone/Buprenorphine 101 Workshop Ron Joe, MD, DABAM December 10, 2016 Learning objectives Clarify the purpose of urine drug testing (UDT) Distinguish between UDT for detection of
Urine Drug Testing Methadone/Buprenorphine 101 Workshop Ron Joe, MD, DABAM December 10, 2016 Learning objectives Clarify the purpose of urine drug testing (UDT) Distinguish between UDT for detection of
Controlled Substances Evidence-based Tips for Improved Workflow: Diagnosis, Screening & Drug Testing
 Controlled Substances Evidence-based Tips for Improved Workflow: Diagnosis, Screening & Drug Testing Mississippi Primary Health Care Association Pearl, MS March 7, 2018 Scott Hambleton, MD, DFASAM Medical
Controlled Substances Evidence-based Tips for Improved Workflow: Diagnosis, Screening & Drug Testing Mississippi Primary Health Care Association Pearl, MS March 7, 2018 Scott Hambleton, MD, DFASAM Medical
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
The Utility of Urine Drug Screening
 The Utility of Urine Drug Screening Treating Addiction, Saving Lives Sea Cruises Bye Tazmania, still far from New Zealand February 8 th, 2018 Mandy Manak, MD FASAM, ISAM, CSAM, MRO Medical Director, ICDO
The Utility of Urine Drug Screening Treating Addiction, Saving Lives Sea Cruises Bye Tazmania, still far from New Zealand February 8 th, 2018 Mandy Manak, MD FASAM, ISAM, CSAM, MRO Medical Director, ICDO
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program North Sydney April 12, 2018 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program North Sydney April 12, 2018 This speaker has been asked to disclose to the audience any involvement with
Urine Drug Screening (UDS) Dr. Erica L. Weinberg December 2017
 Dr. Erica L. Weinberg December 2017") Urine Drug Screening (UDS) Dr. Erica L. Weinberg December 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any
Urine Drug Screening (UDS) Dr. Erica L. Weinberg December 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any
Testing for Controlled Substances
 Testing for illicit drugs Testing for Controlled Substances 1 Purposes: Employment Sports Screening medical eval. Legal Monitoring Treatment Probation Prescribing controlled substances Forensics 2 Drug
Testing for illicit drugs Testing for Controlled Substances 1 Purposes: Employment Sports Screening medical eval. Legal Monitoring Treatment Probation Prescribing controlled substances Forensics 2 Drug
10/16/2017. Objectives. Drug Testing Interpretation in Addiction Care. Background. Which is Nonadherent?
 Objectives Drug Testing Interpretation in Addiction Care Brandi Puet, Pharm.D. Describe the difference between immunoassay and confirmatory testing. List explanations for unexpected negative or positive
Objectives Drug Testing Interpretation in Addiction Care Brandi Puet, Pharm.D. Describe the difference between immunoassay and confirmatory testing. List explanations for unexpected negative or positive
Controlled Substance Monitoring in the Age of the Opioid Epidemic
 Controlled Substance Monitoring in the Age of the Opioid Epidemic Paul E. Hilliard, MS, MD Hospital Pain Committee Chair Department of Anesthesiology CME housekeeping I have no financial disclosures AKA,
Controlled Substance Monitoring in the Age of the Opioid Epidemic Paul E. Hilliard, MS, MD Hospital Pain Committee Chair Department of Anesthesiology CME housekeeping I have no financial disclosures AKA,
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain
 Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
1/26/2016. These are my own thoughts! Safe Workplace Safe Workforce Proven benefits of Stay At Work / Return To Work Process (SAW/RTW)
") Dr. Paul A. Farnan farnan@mail.ubc.ca HealthQuest Occupational Health Corporation Alliance Medical Monitoring I have no financial interests or affiliation with any pharmaceutical industry or manufacturer
Dr. Paul A. Farnan farnan@mail.ubc.ca HealthQuest Occupational Health Corporation Alliance Medical Monitoring I have no financial interests or affiliation with any pharmaceutical industry or manufacturer
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of Toronto
 Team Based Approaches to Chronic Pain Management: Opioid Stewardship Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of
Team Based Approaches to Chronic Pain Management: Opioid Stewardship Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Overview. Opioids and HIV Infection: From Pain Management to Addiction Treatment
 FORMATTED: 01/23/2017 New York, New York: February 24, 2017 Opioids and HIV Infection: From Pain Management to Addiction Treatment Chinazo Cunningham, MD, MS Professor of Medicine Albert Einstein College
FORMATTED: 01/23/2017 New York, New York: February 24, 2017 Opioids and HIV Infection: From Pain Management to Addiction Treatment Chinazo Cunningham, MD, MS Professor of Medicine Albert Einstein College
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Frequently Asked Questions: Opiate Dependency and Methadone Maintenance Treatment program follow-up
 Frequently Asked Questions: Opiate Dependency and Methadone Maintenance Treatment program follow-up Dr. Bhushan M. Kapur Associate Professor Department of Laboratory Medicine and Pathobiology, Faculty
Frequently Asked Questions: Opiate Dependency and Methadone Maintenance Treatment program follow-up Dr. Bhushan M. Kapur Associate Professor Department of Laboratory Medicine and Pathobiology, Faculty
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Pain Management Wrap-Up Chronic Care. David Tauben, MD Medicine Anesthesia & Pain Medicine
 Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Goals decided with patient: Mild-to-Moderate Pain First- line: codeine or tramadol Second-line: morphine, oxycodone or hydromorphone
 The Opioid Manager is designed to be used as a point of care tool for providers prescribing opioids for chronic non cancer pain. It condenses key elements from the ACanadian Opioid Guideline and can be
The Opioid Manager is designed to be used as a point of care tool for providers prescribing opioids for chronic non cancer pain. It condenses key elements from the ACanadian Opioid Guideline and can be
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
URINE DRUG TOXICOLOGY
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences URINE DRUG TOXICOLOGY Suzanne E. Rapp, MD GENERAL DISCLOSURES The University of Washington School of Medicine also
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences URINE DRUG TOXICOLOGY Suzanne E. Rapp, MD GENERAL DISCLOSURES The University of Washington School of Medicine also
California. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Objectives. When to Refer. PISA Physicians 1/25/17. Financial Disclosures: None. PISA & THMEP January 28, 2017 Kenneth B. Gossler M.D.
 1/25/17 PISA & THMEP January 28, 2017 Kenneth B. Gossler M.D. PISA Physicians Kenneth B. Gossler M.D. Education University of Arizona Med School 1992. THMEP Intern 1993 Anesthesiology Residency at Financial
1/25/17 PISA & THMEP January 28, 2017 Kenneth B. Gossler M.D. PISA Physicians Kenneth B. Gossler M.D. Education University of Arizona Med School 1992. THMEP Intern 1993 Anesthesiology Residency at Financial
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
PROJECT ECHO OPIOID USE DISORDER IN PREGNANT WOMEN
 PROJECT ECHO OPIOID USE DISORDER IN PREGNANT WOMEN 1 OPIOID USE DISORDER IN WOMEN Recognition & Prevention Date: August 14 th, Time: 8 am Presenters: Deepa Nagar MD, Andria Peterson PharmD Maternal Treatment
PROJECT ECHO OPIOID USE DISORDER IN PREGNANT WOMEN 1 OPIOID USE DISORDER IN WOMEN Recognition & Prevention Date: August 14 th, Time: 8 am Presenters: Deepa Nagar MD, Andria Peterson PharmD Maternal Treatment
Patient-Centered Urine Drug Testing. Douglas Gourlay, MD, MSc, FRCPC, FASAM
 Patient-Centered Urine Drug Testing Douglas Gourlay, MD, MSc, FRCPC, FASAM Declaration of Potential Conflict of Interest The content of this presentation is non- commercial and does not represent any conflict
Patient-Centered Urine Drug Testing Douglas Gourlay, MD, MSc, FRCPC, FASAM Declaration of Potential Conflict of Interest The content of this presentation is non- commercial and does not represent any conflict
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Urine Drug Testing to Monitor Opioid Use In Managing Chronic Pain
 Faculty Disclosure Henry C. Nipper, PhD, DABCC Dr. Nipper has listed no financial interest/arrangement that would be considered a conflict of interest. Urine Drug Testing to Monitor Opioid Use In Managing
Faculty Disclosure Henry C. Nipper, PhD, DABCC Dr. Nipper has listed no financial interest/arrangement that would be considered a conflict of interest. Urine Drug Testing to Monitor Opioid Use In Managing
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Striking a Balance: a provider perspective.
 Striking a Balance: a provider perspective kpfeifer@chcf.org Beth s story 38 years old, erratically employed Counseling doesn t help Chronic low back pain after car accident 8 Vicodin/day grew to 180 mg
Striking a Balance: a provider perspective kpfeifer@chcf.org Beth s story 38 years old, erratically employed Counseling doesn t help Chronic low back pain after car accident 8 Vicodin/day grew to 180 mg
Section I. Short-acting opioid Prior Authorization Criteria
 Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
Physician s Reference for Urine and Blood Drug Testing and Interpretation
 Physician s Reference for Urine and Blood Drug Testing and Interpretation DETECTIMED PANEL Urine (test code 70195) Screen Confirmation Screen Confirmation Alcohol Ethanol Amphetamines Amphetamine Methamphetamine
Physician s Reference for Urine and Blood Drug Testing and Interpretation DETECTIMED PANEL Urine (test code 70195) Screen Confirmation Screen Confirmation Alcohol Ethanol Amphetamines Amphetamine Methamphetamine
Utah. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Disclosures. You're in Control or Urine Control Clinical Pearls of Drug Testing Case Studies. 9/20/17
 You're in Control or Urine Control Clinical Pearls of Drug Testing Case Studies Jeffrey Fudin, BS, PharmD, FCCP, FASHP www.paindr.com Disclosures Astra Zeneca (Speakers Bureau) Collegium (Consultant) Daiichi
You're in Control or Urine Control Clinical Pearls of Drug Testing Case Studies Jeffrey Fudin, BS, PharmD, FCCP, FASHP www.paindr.com Disclosures Astra Zeneca (Speakers Bureau) Collegium (Consultant) Daiichi
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
PROVIDER BULLETIN. Published by Wyoming Workers Compensation Medical Case Management Unit October 21, 2015
 Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Linking Opioid Treatment in Primary Care. Roxanne Lewin M.D.
 Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain
 Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
EDUCATIONAL COMMENTARY METHADONE
 EDUCATIONAL COMMENTARY METHADONE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits see the Continuing Education
EDUCATIONAL COMMENTARY METHADONE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits see the Continuing Education
Gold Standard for Urine Drug Testin Urine Drug Testing Why U rine? Urine?
 Gold Standard for Urine Drug Testing Developed by TRMC Pain Management Center Jill Duffy, RN,BC Pam Kennell, RN, BC Heidi Beisch, RN Urine Drug Testing A DIAGNOSTIC tool For an OBJECTIVE test Based on
Gold Standard for Urine Drug Testing Developed by TRMC Pain Management Center Jill Duffy, RN,BC Pam Kennell, RN, BC Heidi Beisch, RN Urine Drug Testing A DIAGNOSTIC tool For an OBJECTIVE test Based on
Conflict of Interest Disclosure
 Patient Rx Drug Misuse and Abuse: Compliance Toxicology Monitoring in Clinical Practice Toxicology Staff Andrea Terrell, Ph.D., DABCC Chief Scientific Officer George Behonick, Ph.D., DABFT, Manager, FBU
Patient Rx Drug Misuse and Abuse: Compliance Toxicology Monitoring in Clinical Practice Toxicology Staff Andrea Terrell, Ph.D., DABCC Chief Scientific Officer George Behonick, Ph.D., DABFT, Manager, FBU
Opioids in the Management of Chronic Pain: An Overview
 Opioids in the Management of Chronic Pain: An Overview Appropriate treatment of chronic pain may include both pharmacologic and non-pharmacologic modalities. The Board realizes that controlled substances,
Opioids in the Management of Chronic Pain: An Overview Appropriate treatment of chronic pain may include both pharmacologic and non-pharmacologic modalities. The Board realizes that controlled substances,
Appropriate Prescribing of Opioids for Chronic Non Cancer Pain
 Appropriate Prescribing of Opioids for Chronic Non Cancer Pain Dr. Cheri Olson La Crosse Mayo Family Medicine Residency Assistant Professor of Family Medicine, Mayo Graduate School of Medicine Disclosure
Appropriate Prescribing of Opioids for Chronic Non Cancer Pain Dr. Cheri Olson La Crosse Mayo Family Medicine Residency Assistant Professor of Family Medicine, Mayo Graduate School of Medicine Disclosure
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
Corporate Medical Policy
 Corporate Medical Policy Drug Testing in Pain Management and Substance Abuse Treatment File Name: Origination: Last CAP Review: Next CAP Review: Last Review: drug_testing_in_pain_management_and_substance_abuse_treatment
Corporate Medical Policy Drug Testing in Pain Management and Substance Abuse Treatment File Name: Origination: Last CAP Review: Next CAP Review: Last Review: drug_testing_in_pain_management_and_substance_abuse_treatment
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN
 OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
Opioid Analgesics. Recommended starting dose for opioid-naïve patients
 Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Recognizing Narcotic Abuse and Addiction and Helping Those With It
 Recognizing Narcotic Abuse and Addiction and Helping Those With It Michael McNett, MD Medical Director for Chronic Pain Member, WI Med Society Opioid Subcommittee Ancient History 1995: OxyContin approved
Recognizing Narcotic Abuse and Addiction and Helping Those With It Michael McNett, MD Medical Director for Chronic Pain Member, WI Med Society Opioid Subcommittee Ancient History 1995: OxyContin approved
The Challenges of Opioid Dispensing
 The Challenges of Opioid Dispensing William R. Kirchain, PharmD, CDE XULA Instructor, Pharmacy Law President, Louisiana Pharmacists Association CDC Guideline for Prescribing Opioids for Chronic Pain United
The Challenges of Opioid Dispensing William R. Kirchain, PharmD, CDE XULA Instructor, Pharmacy Law President, Louisiana Pharmacists Association CDC Guideline for Prescribing Opioids for Chronic Pain United
Opioids: Use and Misuse/Steven Feinberg, MD; Scott Levy, MD, MPH, FACOEM
 Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
3/3/2015 CHRONIC PAIN MARGARET ZOELLERS, MSN, APRN
 CHRONIC PAIN MARGARET ZOELLERS, MSN, APRN 1 Pain that persists or recurs > 3-6 months Pain that persists >1 month after injury/event Commonly seems out of proportion to the physical process Cause may be
CHRONIC PAIN MARGARET ZOELLERS, MSN, APRN 1 Pain that persists or recurs > 3-6 months Pain that persists >1 month after injury/event Commonly seems out of proportion to the physical process Cause may be
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Welcome! Supreme Court of Ohio Specialized Dockets Conference. October 23-24, 2017
 Welcome! Supreme Court of Ohio Specialized Dockets Conference October 23-24, 2017 Drug Testing: Do you know enough to be dangerous? Presented by William L. Parker President & CEO American Court & Drug
Welcome! Supreme Court of Ohio Specialized Dockets Conference October 23-24, 2017 Drug Testing: Do you know enough to be dangerous? Presented by William L. Parker President & CEO American Court & Drug
Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 %
 Published on OpioidRisk (https://www.opioidrisk.com) Home > Results Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 % Question Results
Published on OpioidRisk (https://www.opioidrisk.com) Home > Results Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 % Question Results
Learning Objectives. Drug Testing 10/17/2012. Utilization of the urine drug screen: The good, the bad, and the ugly
 Utilization of the urine drug screen: The good, the bad, and the ugly Jennifer A. Lowry, MD Chief, Section of Medical Toxicology Children s Mercy Hospital Kansas City, MO Learning Objectives Describe the
Utilization of the urine drug screen: The good, the bad, and the ugly Jennifer A. Lowry, MD Chief, Section of Medical Toxicology Children s Mercy Hospital Kansas City, MO Learning Objectives Describe the
Q&A: Opioid Prescribing for Chronic Non-Malignant Pain
 NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Tapering Opioids Best Practices*
 Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Drug Testing in Pain Management and Substance Use Disorder Treatment
 Drug Testing in Pain Management and Substance Use Disorder Treatment Policy Number: 2.04.98 Last Review: 3/2018 Origination: 3/2017 Next Review: 3/2019 Policy Blue Cross and Blue Shield of Kansas City
Drug Testing in Pain Management and Substance Use Disorder Treatment Policy Number: 2.04.98 Last Review: 3/2018 Origination: 3/2017 Next Review: 3/2019 Policy Blue Cross and Blue Shield of Kansas City
September HCMC Toxicology Transition: Additional information and Frequently Asked Questions
 September 2016 HCMC Toxicology Transition: Additional information and Frequently Asked Questions Many clinicians have asked for more information about the Urine Drug Compliance Analysis (LAB8742) switch
September 2016 HCMC Toxicology Transition: Additional information and Frequently Asked Questions Many clinicians have asked for more information about the Urine Drug Compliance Analysis (LAB8742) switch
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
Vermont. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Effective Date: Approved by: Laboratory Executive Director, Ed Hughes (electronic signature)
") 1 Policy #: 803 (PLH-803-02) Effective Date: NA Reviewed Date: 4/11/2008 Subject: URINE DRUG SCREENS Approved by: Laboratory Executive Director, Ed Hughes (electronic signature) Approved by: Laboratory
1 Policy #: 803 (PLH-803-02) Effective Date: NA Reviewed Date: 4/11/2008 Subject: URINE DRUG SCREENS Approved by: Laboratory Executive Director, Ed Hughes (electronic signature) Approved by: Laboratory
Safe and Competent Opioid Prescribing
 MILITARY Military Safe and Competent Opioid Prescribing Education (M-SCOPE) Program Safe and Competent Opioid Prescribing For Providers Working with Veterans and Military Service Personnel Daniel P. Alford,
MILITARY Military Safe and Competent Opioid Prescribing Education (M-SCOPE) Program Safe and Competent Opioid Prescribing For Providers Working with Veterans and Military Service Personnel Daniel P. Alford,
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
Department of Veterans Affairs Network Policy No.: VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA
 Date: September 23, 2014 Long Beach, CA") Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Update on OXYCODONE. what can primary care do about the problem? 8 BPJ Issue 44
 Update on OXYCODONE what can primary care do about the problem? 8 BPJ Issue 44 Approximately 70% of people dispensed oxycodone in New Zealand are initiated on this medicine outside of general practice,
Update on OXYCODONE what can primary care do about the problem? 8 BPJ Issue 44 Approximately 70% of people dispensed oxycodone in New Zealand are initiated on this medicine outside of general practice,
No disclosures for any of the speakers!
 Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist Gabriel Paulian M.D Christopher Ong, M.D Yuliet Sanchez, M.D Uma Suryadevara, M.D No disclosures for any of the speakers!
Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist Gabriel Paulian M.D Christopher Ong, M.D Yuliet Sanchez, M.D Uma Suryadevara, M.D No disclosures for any of the speakers!
Chronic Opioid Therapy Safe Prescribing in Primary Care. Part 3
 Chronic Opioid Therapy Safe Prescribing in Primary Care Part 3 Michael Mangione, MD Chief of Anesthesia and Director of Pain Service VA Pittsburgh Health Care System Nancy Wiedemer,CRNP VISN 4 Pain Management
Chronic Opioid Therapy Safe Prescribing in Primary Care Part 3 Michael Mangione, MD Chief of Anesthesia and Director of Pain Service VA Pittsburgh Health Care System Nancy Wiedemer,CRNP VISN 4 Pain Management
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine
 INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
Caring for ME Webinar: Urine Drug Screening Speaker: Dr. Jonathan Fellers Tuesday, November 20, PM
 Caring for ME Webinar: Urine Drug Screening Speaker: Dr. Jonathan Fellers Tuesday, November 20, 2018 12 1 PM Audio is available through your computer speakers. Mission Maine Quality Counts is a nonprofit
Caring for ME Webinar: Urine Drug Screening Speaker: Dr. Jonathan Fellers Tuesday, November 20, 2018 12 1 PM Audio is available through your computer speakers. Mission Maine Quality Counts is a nonprofit
The Challenging Patient with Chronic Opioid Usage MD ACP Meeting
 The Challenging Patient with Chronic Opioid Usage. 2018 MD ACP Meeting Darius A. Rastegar, MD March 12, 2018 1 Prescribing Opioids: A question of balance Opioids are an effective treatment for acute pain.
The Challenging Patient with Chronic Opioid Usage. 2018 MD ACP Meeting Darius A. Rastegar, MD March 12, 2018 1 Prescribing Opioids: A question of balance Opioids are an effective treatment for acute pain.
Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM. Disclosures
 Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM Disclosures Dr. Bhatnagar: no disclosures to report Dr. Ewing: no disclosures to report 1 Our
Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM Disclosures Dr. Bhatnagar: no disclosures to report Dr. Ewing: no disclosures to report 1 Our
Opioid Analgesic Treatment Worksheet
 Opioid Analgesic Treatment Worksheet Aetna Better Health of Louisiana Fax: 1 844 699 2889 www.aetnabetterhealth.com/louisiana/providers/pharmacy LA Legacy Fee for Service (FFS) Medicaid Fax: 1 866 797
Opioid Analgesic Treatment Worksheet Aetna Better Health of Louisiana Fax: 1 844 699 2889 www.aetnabetterhealth.com/louisiana/providers/pharmacy LA Legacy Fee for Service (FFS) Medicaid Fax: 1 866 797
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Organizing your Practice for Efficient Pain Assessment. Session #4 Roman D. Jovey, MD
 Organizing your Practice for Efficient Pain Assessment Session #4 Roman D. Jovey, MD 2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Organizing your Practice for Efficient Pain Assessment Session #4 Roman D. Jovey, MD 2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
How Can a Methadone and an Opiate-Positive Immunoassay Result be Reconciled in a Patient Prescribed only OxyContin and Wellbutrin?
 190 Available online at www.annclinlabsci.org How Can a Methadone and an Opiate-Positive Immunoassay Result be Reconciled in a Patient Prescribed only OxyContin and Wellbutrin? Jude M. Abadie Department
190 Available online at www.annclinlabsci.org How Can a Methadone and an Opiate-Positive Immunoassay Result be Reconciled in a Patient Prescribed only OxyContin and Wellbutrin? Jude M. Abadie Department