Delirium and Dementia
|
|
|
- Gervais Long
- 5 years ago
- Views:
Transcription

1 Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network
2 Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased impairment Return to baseline is questionable


3 Acute Care Stress Blender Poor sleep C Confusion At-Risk Older Adult A Assessment M Method







4 CAM - Confusion Assessment Method A and B A B Acute onset + Fluctuating course Inattention Often discounted as person s normal. C or D C D Disorganized thinking Altered level of consciousness NEED to KNOW BASELINE





5 Confusion Assessment Method (CAM) Delirium is often discounted as the person s normal C D Disorganized thinking Altered level of consciousness To detect delirium, we need to know their baseline

6 Stop & Watch Early delirium detection Supports communication Reduces acute care admissions Complete Stop and Watch Early Warning Tool: available from Med- Pass.com 2011 Florida Atlantic University


7 Delirium Information for Patients and Families


8 Delirium Risk Assessment Prevent the explosion!
 Heart rate and contraction strength Movement (muscle contraction)")
9 Delirium and Brain Neurotransmitters Blocking of neurotransmitters can effect: Learning and memory REM sleep cycle regulation Neuroendocrine function Smooth muscle (intestines, bladder, arteries) Heart rate and contraction strength Movement (muscle contraction) Sweat glands
 Stress increases demand for acetylcholine Many medications block")
10 Acetylcholine and Delirium Acetylcholine powers up the brain Acetylcholine levels are lower in older adults (90% lower in Alzheimer's) Stress increases demand for acetylcholine Many medications block acetylcholine


11 Anticholinergic Cognitive Burden (ACB) Anticholinergic = medication that blocks acetylcholine Many commonly prescribed medications have anticholinergic properties (some strong, some weaker) Taking multiple medications with anticholinergic properties adds up to a higher cognitive burden

12 Medications and Delirium 5 or more medications = higher risk of delirium and falls
13 Prescribing Cascade (example) High Blood Pressure Edema caused by peripheral vasodilation Treated with Ca 2+ channel blocker Heart failure treated with 2 diuretics Incontinence caused by increased urinary output Fracture caused by a fall Overactive Bladder treated with antimuscarinic (very anticholinergic) Agitation and pain treated with haloperidol, morphine, dimenhydrinate Delirium

14 Medication Reconciliation What kinds of questions do we need to ask about medications? Whose job is it to evaluate medications? How/when does your team assess medications e.g. with higher risk than benefit, or prescribing cascades? How are patients and families involved in conversations around medications?


15 Pharmacologic Restraint Management Worksheet (Form 19676)

16 Dehydration and Delirium Dehydration: Lowers blood pressure Increases risk of falls Damages brain cells Increases risk of urinary tract infections and constipation Risks for Dehydration with Aging & Dementia Decreased thirst, confusion, impaired swallow

17 Dehydration, Drugs and Delirium Diuretics Sedatives and antipsychotics Drug induced diarrhea e.g. laxatives, acidblocking drugs, metformin, motility drugs, antibiotics, digoxin (at toxic levels) Drugs for bone density (Esophageal swelling and ulceration from incomplete swallowing)


18 Hydration Strategies What are some of your hydration strategies? What is your experience with hypodermoclysis? How do you measure hydration? Thickened fluids and dehydration


19 Nutrition and Delirium Healthy brain function requires many essential nutrients Acetylcholine production requires choline, found in eggs, meat, fish, cruciferous vegetables (e.g. broccoli), milk Delirium risk increases with malnutrition: e.g. lower levels of Vitamin B 12, iron, proteins

20 Malnutrition, Drugs and Delirium Pill Burden: nausea, loss of appetite, feel full, agitation Anticholinergic burden: sedation, decreased gastrointestinal motility Olfactory disturbances with many common medications Impaired nutrient absorption


21 Urinary tract infections are frequently misdiagnosed in the elderly For information and resources see Treatment with antibiotics has many unwanted side-effects Misdiagnosis means underlying cause of delirium is missed PUSH FLUIDS for 24 hours

22 Sepsis-associated mortality per Canadians Older adult age ranges
23
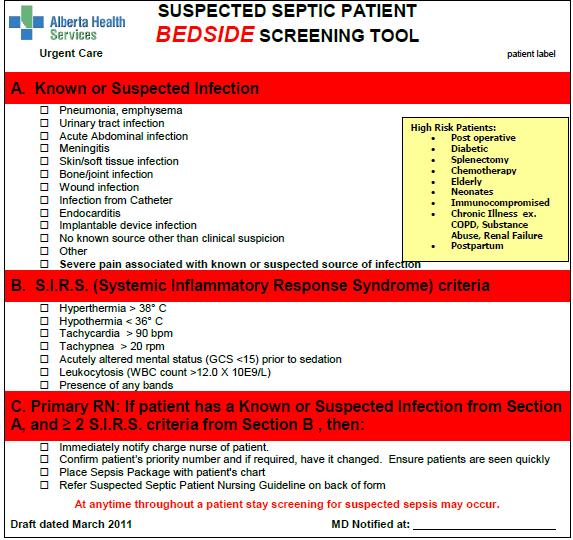
24 A. Known or Suspected Infection Pneumonia, emphysema Urinary tract infection Acute abdominal infection Meningitis Skin/soft tissue infection Bone/joint infection Wound infection Infection from catheter Endocarditis Implantable device infection High Risk Patients Post-Operative Diabetic Splenectomy Chemotherapy Elderly Neonates Immunocompromised Chronic Illness (e.g. COPD, Substance Abuse, Renal Failure) Postpartum No known source other than clinical suspicion Other Severe pain associated with known or suspected source of infection
25 B. SIRS CRITERIA (Systemic Inflammatory Response Syndrome) Hyperthermia > 38 O C Hypothermia < 36 O C Tachycardia > 90 bpm Tachypnea >20 / min Acutely altered mental status (GCS <15) prior to sedation Leukocytosis (WBC count >12 X 10E9/L0 Presence of any bands
26 SIRS - Considerations for Older Adults Hyperthermia > 38 O C Hypothermia < 36 O C 1.3 O C change from baseline (consider Normal Aging Changes, Medications) Tachycardia >90 bpm Tachypnea >20 min GCS <15 Leukocytosis (WBC>12) Presence of any bands Heart Rate change from baseline (consider Normal Aging Changes and Medication effects) Respiratory Rate change from baseline Delirium detection (e.g. CAM) Leukocytosis Bands

27 Stress Prevention Strategies Assess for discomfort e.g. pain, urine retention Avoid physical restraints Support sleep Reduce noise and overstimulation Consistent caregivers Meaningful activities Therapeutic napping


 Minimize fluid")

28 Surgery and Delirium Prevention Post-Op Pre-Op Nutrition Limited fasting! Patient education Carbohydrate loading Appropriate analgesia Medication review Operative Appropriate analgesia Minimal access surgery Normal temperature Minimal anaesthesia ( freezing & epidurals vs going under ) Minimize fluid replacement Early removal of tubes and drains Early nutrition Early ambulation Nausea and vomiting prophylaxis (cautious) Appropriate (and pre-emptive) analgesia F/U after discharge


29 Acetylcholine and Parkinson s Disease Parkinson s disease and the resulting medications increase risk of delirium Best treatment is to reduce Parkinson s medications.

 may be more effective.")
30 End of Life Delirium Current practice supports antipsychotics at end of life Evidence is unfolding to suggest supportive nursing care and gentle hydration (e.g. hypodermoclysis) may be more effective. (Agar et al, 2016)


31 Do antipsychotics treat delirium? Antipsychotic may cause or worsen delirium Antipsychotics are a last resort when: Distressing/dangerous psychosis and non-pharmacologic strategies are ineffective Psychosis is an obstacle to crucial treatment Short term (e.g. one dose) while treating underlying causes Low dose: e.g to 0.5 mg haloperidol (Haldol) Antipsychotics do not treat delirium.


32 Those with dementia are already at increased risk of delirium Delirium has many causes, including: Too many medications Dehydration Malnutrition Stress Infection Surgery Parkinsons Disease Summary While delirium is a multifactorial process, it is estimated that medications alone may account for 12%-39% of all cases of delirium. Alagiakrishnan and Wiens 2004


33 DELIRIUM is a MEDICAL EMERGENCY Like chest pain Like anaphylaxis Like stroke Intervene IMMEDIATELY
34 Site Assessment What are you already doing well? Where do you have room for improvement? What are your priorities and next steps?
Prevention of Delirium in Dementia
 Prevention of Delirium in Dementia Appropriate Use of Antipsychotics Project Seniors Health Strategic Clinical Network (SCN) In collaboration with Addiction & Mental Health SCN Introduce your team/family
Prevention of Delirium in Dementia Appropriate Use of Antipsychotics Project Seniors Health Strategic Clinical Network (SCN) In collaboration with Addiction & Mental Health SCN Introduce your team/family
Black holes taped on floor Redirection Music and activities Yellow straps across the door Remind other residents to use call bell when she comes in
 Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Medications are Additive (Anticholinergic) Diane W. Healey, M.D. Center for Healthy Aging March 10, 2017
 Diane W. Healey, M.D. Center for Healthy Aging March 10, 2017") Medications are Additive (Anticholinergic) Diane W. Healey, M.D. Center for Healthy Aging March 10, 2017 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed.
Medications are Additive (Anticholinergic) Diane W. Healey, M.D. Center for Healthy Aging March 10, 2017 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed.
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Patient Information VERSACLOZ (VER sa kloz) (clozapine) Oral Suspension
 (clozapine) Oral Suspension") Patient Information VERSACLOZ (VER sa kloz) (clozapine) Oral Suspension Read this Patient Information before you start taking VERSACLOZ and each time you get a refill. There may be new information. This
Patient Information VERSACLOZ (VER sa kloz) (clozapine) Oral Suspension Read this Patient Information before you start taking VERSACLOZ and each time you get a refill. There may be new information. This
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Seniors Health Strategic Clinical Network Restraint as a Last Resort
 Seniors Health Strategic Clinical Network Restraint as a Last Resort Elder Friendly Care 2018 Alberta Health Services, Seniors Health Strategic Clinical Network Disclaimer, Copyright and Creative Commons
Seniors Health Strategic Clinical Network Restraint as a Last Resort Elder Friendly Care 2018 Alberta Health Services, Seniors Health Strategic Clinical Network Disclaimer, Copyright and Creative Commons
Management of UTIs for older adults >65 years residing in care homes
 Good Practice Guidance for CARE STAFF 1,2,3 : Management of UTIs for older adults >65 years residing in care homes UTI - What is it? A urinary tract infection (UTI) is an infection in any part of the urinary
Good Practice Guidance for CARE STAFF 1,2,3 : Management of UTIs for older adults >65 years residing in care homes UTI - What is it? A urinary tract infection (UTI) is an infection in any part of the urinary
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Chapter Goal. Learning Objectives 9/12/2012. Chapter 36. Geriatrics. Use assessment findings to formulate management plan for geriatric patients
 Chapter 36 Geriatrics Chapter Goal Use assessment findings to formulate management plan for geriatric patients Learning Objectives Describe dependent & independent living environments Identify local resources
Chapter 36 Geriatrics Chapter Goal Use assessment findings to formulate management plan for geriatric patients Learning Objectives Describe dependent & independent living environments Identify local resources
DELIRIUM. Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine
 DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
Nursing Process Focus: Patients Receiving Levodopa (Larodopa)
") Assessment Prior to administration: Obtain complete health history including allergies, drug history and possible drug interactions. Obtain baseline evaluation of severity of Parkinson s disease to determine
Assessment Prior to administration: Obtain complete health history including allergies, drug history and possible drug interactions. Obtain baseline evaluation of severity of Parkinson s disease to determine
CRACKCast E181 Approach to the Geriatric Patient
 CRACKCast E181 Approach to the Geriatric Patient Italicized text refers to passages quoted from Rosen s Emergency Medicine (9 th Ed). Key concepts: We are in the midst of a silver tsunami, with 10,000
CRACKCast E181 Approach to the Geriatric Patient Italicized text refers to passages quoted from Rosen s Emergency Medicine (9 th Ed). Key concepts: We are in the midst of a silver tsunami, with 10,000
Full details and resource documents available:
 Clinical & Regulatory News by Pharmerica Urinary Tract Infection (UTI) Second Most Common Cause of Hospital Readmission within 30 days UTIs are prevalent and account for up to 22% of infections in LTC,
Clinical & Regulatory News by Pharmerica Urinary Tract Infection (UTI) Second Most Common Cause of Hospital Readmission within 30 days UTIs are prevalent and account for up to 22% of infections in LTC,
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
There s No Place like Home
 THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
Residents Who Don t Sleep
 Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Chapter 20. Assisting With Nutrition and Fluids
 Chapter 20 Assisting With Nutrition and Fluids Food and water: Are physical needs Basics of Nutrition Are necessary for life A poor diet and poor eating habits: Increase the risk for diseases and infection
Chapter 20 Assisting With Nutrition and Fluids Food and water: Are physical needs Basics of Nutrition Are necessary for life A poor diet and poor eating habits: Increase the risk for diseases and infection
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine)
") Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine) Potential Nursing Diagnoses Ineffective Therapeutic Regimen Management Risk for Activity Intolerance, related to side effect of drug
Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine) Potential Nursing Diagnoses Ineffective Therapeutic Regimen Management Risk for Activity Intolerance, related to side effect of drug
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Prescribing Drugs to the Elderly
 Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Delirium: A Condition of All Ages. Delirium, also known as acute confusional state, Definition. Epidemiology
 Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Philippa Parish Nutrition BSc (Hons) Dip ION MBANT NTC & CNHC Registered Practitioner Phone: Mobile:
 Dip ION MBANT NTC & CNHC Registered Practitioner Phone: Mobile:") Philippa Parish Nutrition BSc (Hons) Dip ION MBANT NTC & CNHC Registered Practitioner Phone: 0117 9863700 Mobile: 07970 950 839 E-mail: philippaparish@blueyonder.co.uk Web: www.philippaparish.com Hydration
Philippa Parish Nutrition BSc (Hons) Dip ION MBANT NTC & CNHC Registered Practitioner Phone: 0117 9863700 Mobile: 07970 950 839 E-mail: philippaparish@blueyonder.co.uk Web: www.philippaparish.com Hydration
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care
 Summary document for Primary Care") Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Appendix E: Continence Care and Bowel Management Program Training Presentation. Audience: For Registered Staff Release Date: December 22, 2010
 Appendix E: Continence Care and Bowel Management Program Training Presentation Audience: For Registered Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Appendix E: Continence Care and Bowel Management Program Training Presentation Audience: For Registered Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Fluid and Electrolytes P A R T 2
 Fluid and Electrolytes P A R T 2 Fluid Shifts Extracellular fluid distribution is dynamic Interstitial fluid formation is continuous Venous system Large veins (capacitance vessels) Small veins (capacitance
Fluid and Electrolytes P A R T 2 Fluid Shifts Extracellular fluid distribution is dynamic Interstitial fluid formation is continuous Venous system Large veins (capacitance vessels) Small veins (capacitance
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Nursing Home Antimicrobial Stewardship Guide Determine Whether To Treat
 Nursing Home Antimicrobial Stewardship Guide Determine Whether To Treat Toolkit 3. Minimum Criteria for Common Infections Toolkit Tool 1. Sample Policy Protocol for Three Common Infections [DATE] [NAME
Nursing Home Antimicrobial Stewardship Guide Determine Whether To Treat Toolkit 3. Minimum Criteria for Common Infections Toolkit Tool 1. Sample Policy Protocol for Three Common Infections [DATE] [NAME
Gastrointestinal. Issues in ElderCare. TCHP Education. Consortium. Part of the ElderCare: Healthcare for the Aging Series
 TCHP Education Consortium Gastrointestinal Issues in ElderCare Part of the ElderCare: Healthcare for the Aging Series TCHP Education Consortium, 2004, 2007 This educational activity expires December 31,
TCHP Education Consortium Gastrointestinal Issues in ElderCare Part of the ElderCare: Healthcare for the Aging Series TCHP Education Consortium, 2004, 2007 This educational activity expires December 31,
PSYCHOTROPIC SOLUTIONS
 PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine
 Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Constipation An Overview. Definition Physiology of GI tract Etiology Assessment Treatment
 CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
Delirium and cognitive impairment in the perioperative
 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
SPASMEX FORTE 5mg tablets
 PACKAGE LEAFLET: INFORMATION FOR THE USER SPASMEX FORTE 5mg tablets TROSPIUM This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for a medicine, which outlines
PACKAGE LEAFLET: INFORMATION FOR THE USER SPASMEX FORTE 5mg tablets TROSPIUM This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for a medicine, which outlines
UND GERIATRIC MEDICINE FELLOWSHIP CURRICULUM ACUTE CARE
 LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
University of Hawaii Center on Aging
 University of Hawaii Center on Aging. Supported in part by a cooperative agreement No. 90AL0011-01-00 from the Administration on Aging, Administration for Community Living, U.S. Department of Health and
University of Hawaii Center on Aging. Supported in part by a cooperative agreement No. 90AL0011-01-00 from the Administration on Aging, Administration for Community Living, U.S. Department of Health and
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
The in-hospital management of COPD-exacerbation includes three core processes:
 Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Public Dissemination Effective: January 2018
 Board of Pharmacy Specialties Board Certified Geriatric Pharmacist (BCGP) Detailed Content Outline 1. GENERAL PRINCIPLES OF AGING (20%) A. Apply the knowledge of physiologic changes associated with aging
Board of Pharmacy Specialties Board Certified Geriatric Pharmacist (BCGP) Detailed Content Outline 1. GENERAL PRINCIPLES OF AGING (20%) A. Apply the knowledge of physiologic changes associated with aging
It Takes a Village: Caring for Veterans with Advanced Dementia
 It Takes a Village: Caring for Veterans with Advanced Dementia Eric Widera, MD Professor, Division of Geriatrics, UCSF Blog and Podcast: www.geripal.org In our village, what tasks should we be confident
It Takes a Village: Caring for Veterans with Advanced Dementia Eric Widera, MD Professor, Division of Geriatrics, UCSF Blog and Podcast: www.geripal.org In our village, what tasks should we be confident
The Resident Who Screams
 The Resident Who Screams Case study........................................... A 72 year old female has diagnoses of dementia, optic nerve atrophy, irritable bowel syndrome and history of a TIA and DVT.
The Resident Who Screams Case study........................................... A 72 year old female has diagnoses of dementia, optic nerve atrophy, irritable bowel syndrome and history of a TIA and DVT.
Cognitive enhancers PINCH ME. Anticholinergic burden BPSD. Agitation, Aggression and antipsychotics
 Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist
 Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Preventing Falls in Older Adults A Matter of Safety
 Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Delirium Assessment and management in relation to falls risk in hospital
 Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Drugs that poison the elderly
 Drugs that poison the elderly Brent Tipping Sub-specialist Geriatrician and Specialist Physician Division of Geriatric Medicine, Department of Medicine University of the Witwatersrand To treat or not to
Drugs that poison the elderly Brent Tipping Sub-specialist Geriatrician and Specialist Physician Division of Geriatric Medicine, Department of Medicine University of the Witwatersrand To treat or not to
Updates to CMS SOM rules on Psychosocial Issues, Deficiency Categorization, and Psychotropic Medication Use
 Updates to CMS SOM rules on Psychosocial Issues, Deficiency Categorization, and Psychotropic Medication Use Stephen Eide R. Ph Oni Kinberg LCSW, MSSW Updates to the SOM On March 25, 2016 CMS sent out updates
Updates to CMS SOM rules on Psychosocial Issues, Deficiency Categorization, and Psychotropic Medication Use Stephen Eide R. Ph Oni Kinberg LCSW, MSSW Updates to the SOM On March 25, 2016 CMS sent out updates
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Updates in Geriatrics. Christopher R. Carpenter, MD, FACEP, AGSF October 24, 2018
 Updates in Geriatrics Christopher R. Carpenter, MD, FACEP, AGSF October 24, 2018 Disclosure of Relationships Deputy Editor-in-Chief Academic Emergency Medicine Editorial Board ACP Journal Club Journal
Updates in Geriatrics Christopher R. Carpenter, MD, FACEP, AGSF October 24, 2018 Disclosure of Relationships Deputy Editor-in-Chief Academic Emergency Medicine Editorial Board ACP Journal Club Journal
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Western University of Health Sciences, College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of
 Western University of Health Sciences, College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Topic UAN# Target Audience A
Western University of Health Sciences, College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Topic UAN# Target Audience A
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the ACS NSQIP/American Geriatrics Society
 Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the ACS NSQIP/American Geriatrics Society Sanjay Mohanty, MD; Ronnie A. Rosenthal, MS,MD; Marcia M. Russell, MD;
Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the ACS NSQIP/American Geriatrics Society Sanjay Mohanty, MD; Ronnie A. Rosenthal, MS,MD; Marcia M. Russell, MD;
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
THE ELDERLY PATIENT - an introduction
 THE ELDERLY PATIENT - an introduction 10 th October 2015 Dr. Anupama Roy Chowdhury Consultant, Dept of Geriatric Medicine, CGH OVERVIEW Presentations of disease in the elderly Geriatric Giants Immobility
THE ELDERLY PATIENT - an introduction 10 th October 2015 Dr. Anupama Roy Chowdhury Consultant, Dept of Geriatric Medicine, CGH OVERVIEW Presentations of disease in the elderly Geriatric Giants Immobility
Community Paramedic Training Program
 Date: March 2015 Page 1 of 5 Community Paramedic Training Program Training Program Components A. Classroom Training - The Community Paramedic (CP) training course (Appendix 1 Training Curriculum) was developed
Date: March 2015 Page 1 of 5 Community Paramedic Training Program Training Program Components A. Classroom Training - The Community Paramedic (CP) training course (Appendix 1 Training Curriculum) was developed
Falls Prevention Best Practice
 Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Delirium. Script. So what are the signs and symptoms you are likely to see in this syndrome?
 Delirium Script Note: Script may vary slightly from the audio. Slide 2 Index Definition About delirium Signs and symptoms of delirium Why delirium occurs Risk Factors and causes of delirium Conditions
Delirium Script Note: Script may vary slightly from the audio. Slide 2 Index Definition About delirium Signs and symptoms of delirium Why delirium occurs Risk Factors and causes of delirium Conditions
SEPSIS INFORMATION BOOKLET. A life-threatening condition triggered by infection
 SEPSIS INFORMATION BOOKLET SEPSIS is A life-threatening condition triggered by infection It affects the function of the organs and is most effectively treated if recognised early If you have infection
SEPSIS INFORMATION BOOKLET SEPSIS is A life-threatening condition triggered by infection It affects the function of the organs and is most effectively treated if recognised early If you have infection
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Instruct patient and caregivers: Need for constant monitoring Potential complications of drug therapy
 Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart