Delirium in the Elderly
|
|
|
- Johnathan Warren
- 5 years ago
- Views:
Transcription


1 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine
2 Learning Objectives Identify the symptoms of delirium in the elderly Differentiate the most common causes of delirium in the elderly Demonstrate a treatment plan for delirium that combines environmental and pharmacologic modalities
3 Delirium Latin roots de meaning away from lira meaning furrow in a field ium meaning singular Literally means a going off the ploughed track, a madness
4 DSM IV-TR Criteria for Delirium A. Disturbance of consciousness (ie: reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention. B. A change in cognition (such as memory deficit, disorientation, language disturbance) or the development of a perceptual disturbance that is not better accounted for by a pre-existing, established, or evolving dementia. C. The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of the day. D. There is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by the direct physiological consequences of general medical condition.
5 DSM-V Proposed Criteria for Delirium A. Disturbance in level of awareness and reduced ability to direct, focus, sustain, and shift attention. B. A change in cognition, (such as deficits in orientation, executive ability, language, visuoperception, learning and memory) C. There is evidence from the history, physical examination or laboratory findings that the disturbance is caused by the direct physiologic consequences of a general medical condition. D. The disturbance develops over a short period of time (usually hours to a few days) and tends to fluctuate in severity during the course of a day.

6 Delirium: Consciousness normal wakefulness confusion stupor coma delirium
7 cognition Delirium is Acute dementia delirium time
8 conscious awareness Delirium Fluctuates lucid interval acute onset sundowning
9 Associated Symptoms visual hallucinosis motor agitation paranoid delusions combative behaviors reversed sleep/wake cycle
10 Delirium Subtypes Hyperactive delirium (30%) agitated, combative, assaultive withdrawal states, toxic-metabolic Hypoactive delirium (24%) apathetic, depressed, lethargic infectious causes Mixed delirium (46%) classic waxing and waning pattern wide differential of etiologies
11 Prevalence 15% Elderly patients on admission 40% Elderly patients during admission 50% Post hip fracture repair 60% Nursing home 80% Terminally ill
12 Risk Factors- Patient Characteristics Hospitalized elderly Cognitive impairment Lower education level (<8 th grade) Decreased functional status Comorbid medical conditions Malnutrition Depression
13 Perioperative Risk Factors Orthopedic (16-62%) > vascular (29-42%) > cardiac (8-42%) Urgent or emergent procedure Delayed surgery after hip fracture Preoperative hemodynamic instability Hypoxemia Electrolyte disturbances Transfusion requirement
14 Perioperative Risk Factors Sleep deprivation Urinary catheter Immobility Poorly controlled pain Polypharmacy (esp. benzos/ anticholinergics) Meperidine
15 Risk Factors- Medical Conditions Dementia Burns Abrupt discontinuation of alcohol or drugs Malnourishment Chronic hepatic disease Dialysis Parkinson's disease HIV infection Post-stroke status
16 Delirium Risk Factors Visual Impairment (3.51) Severe Illness (3.49) Cognitive Impairment (2.82) Inc. BUN/Cr (2.02) Relative Risk Inouye 1993
17 Rate of Delirium Rate (%) No. of Risk Factors Modified from Francis, 1992
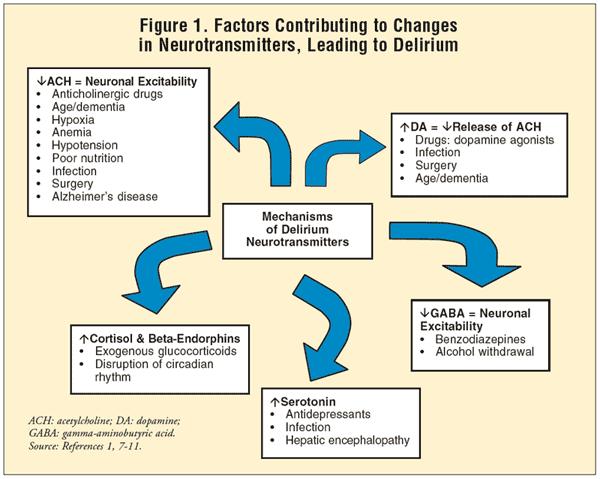
18 Pathogenesis Cholinergic deficiency Abnormalities in serotonin and melatonin Noradrenergic hyperactivity?neuronal damage- inflammation-induced edema hypoxia reduced synthesis of acetylcholine Global brain dysfunction- generalized slowing on EEG
19
20 Tip of the Iceberg Change in consciousness Low MMSE Hallucinations pneumonia cardiac dysrhythmia silent MI
21 Life Threatening Causes of Delirium Wernicke-Korsakoff syndrome Hypoxia Hypoglycemia Hypertensive encephalopathy Hyperthermia or hypothermia Intracerebral hemorrhage Meningitis/ encephalitis Poisoning Status epilepticus Data from Caplan JP, Cassem NH, Murray BG, et al. Delirium. In: Stern TA, ed. Mass. Gen. Hosp. comprehensive clinical psychiatry. Philadelphia: Mosby/ Elsevier; 2008.
22 Etiologies systemic disease infection metabolic derangement cardiovascular collagen/vascular toxicity medications drugs of abuse poisons withdrawal states post-operative states hip fracture repair cardiac surgery primary brain disease stroke trauma infection neoplasm vasculitis
23 Etiology in the Elderly Number of Cases Etiology Definite Probable Possible Total fluid imbalance infection drug toxicity metabolic sensory low perfusion withdrawal intracranial Total Modified from Francis 1992
24 Length of Stay Length of Stay Mean (SD) Patients Actual (days) Predicted (days) Excessive Hospital Stay (days) Pairedcomparison t Tests (P) Entire cohort 12.3 (13.5) 7.5 (3.3) 4.8 < Non-delirious 10.6 (10.1) 7.3 (3.4) 3.3 < Delirious 21.6 (23.7) 8.6 (2.3) 13.0 <0.03 Thomas 1988
25 Morbidity medical complications pneumonia dehydration decubiti unsafe behaviors falls self-extubation noncompliance
26 Significance Increased morbidity Increased mortality Longer hospital stays NH placement
27 Mortality 40% 30% 20% 22-76% 15% 25% 10% 0% in hospital 1 month 6 months
28 Treatment of Delirium Symptomatic Treatment Definitive Treatment
29 Symptomatic Treatment sensory aids education & reassurance orientation hydration & nourishment activity pharmacologic
30 Prevention of Delirium: cognitive impairment orientation board frequent re-orientation cognitively-stimulating activities sleep deprivation warm drink at bedtime relaxation tapes or music back massage noise reduction on the unit schedule adjustment to permit sleep Inouye 1999
31 Prevention of Delirium immobility ambulation or active ROM tid minimal use of catheters or restraints visual impairment glasses or magnifying lenses large-print books large phone keypads fluorescent tape on call bell Inouye 1999
32 Prevention of Delirium hearing impairment earwax disimpaction hearing aids portable amplifying devices other communication techniques dehydration early recognition and rehydration Inouye 1999
33 Prevention of Delirium N=852 pts 1st episode delirium total days delirium # episodes delirium delirium severity specialized delirium protocol usual care group significance 42 (9.9) 64 (15.0) p= p= p= (1.27) 3.52 (1.44) p=0.25 Inouye 1999

34 Avoid Restraint Use Physical restraints are associated with developing delirium Restraint use may actually increase fall risk. Restraint reduction was not associated with an increase in falls. Restraint use within delirium tremens associated with higher mortality
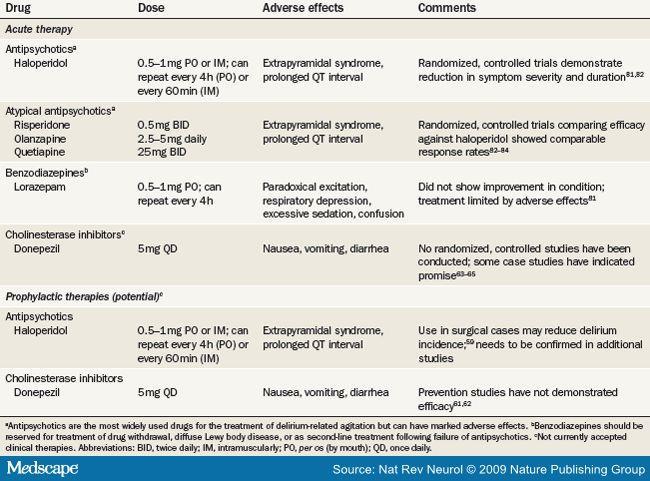
35 Pharmacologic Interventions haloperidol (Haldol) Geriatric dose: 0.25 to 1 mg IV q 8 hrs standing and 0.25 to 1 mg IV q 6 hrs prn. Watch QTc (cut-off 460 msec)- Torsades Contraindicated: DLB, Parkinson s dx, TD
36 Warnings on IV Haldol 9/2007 Higher doses and intravenous administration of haloperidol appear to be associated with a higher risk of QT prolongation and Torsades de Pointes. (at least 28 cases now reported) Because of this risk of Torsades de Pointes and QT prolongation, ECG monitoring is recommended if haloperidol is given intravenously. Haloperidol is not approved for
37 Prophylaxis of Delirium w/ Meds Study of haloperidol 0.5mg three times per day prophylaxis before elderly hip surgery: Reduced severity and duration of symptoms but not the incidence of delirium. Study of olanzepine 10mg vs placebo before elderly joint replacement patients Incidence of delirium significantly lower in tx arm However, delirium lasted longer/ more severe in tx arm Study of risperdone 1 mg upon awakening from elective cardiac surgery 20.6% absolute risk reduction of delirium
38 Pharmacologic Interventions Atypical Antipsychotics No controlled studies Anecdotal evidence Aripiprazole mg bid quetiapine mg in bid - tid risperdone mg bid olanzapine mg hs
39
40 Course of Delirium prodromal overt resolving 1-3 days days to months Cognitive changes may persist 6 months ADLS changes may persist 12+ months
41 Duration of Delirium: 21 days Elderly Koponen 1989
42 Delirium Recall % with Recall severe moderate mild Breitbart 2002
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Delirium Assessment and management in relation to falls risk in hospital
 Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Delirium in Cancer: Psychopharmacologic Management
 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Case 1. Delirium and a Neurologist s Approach to AMS in the Hospital Setting. (DSM-IV-TR) criteria for delirium 11/6/2010
 criteria for delirium 11/6/2010") Delirium and a Neurologist s Approach to AMS in the Hospital Setting S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Delirium and a Neurologist s Approach to AMS in the Hospital Setting S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
DELIRIUM. Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine
 DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
A Neurologist s Approach to Altered Mental Status
 A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Delirium and cognitive impairment in the perioperative
 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist
 Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Home Care and Hospice Association of New Jersey Annual Conference 2017
 Home Care and Hospice Association of New Jersey Annual Conference 2017 I D E N T I F I C A T I O N A N D M A N A G E M E N T O F D E L I R I U M E L I Z A B E T H M A G E R - O C O N N O R A C H P N DR
Home Care and Hospice Association of New Jersey Annual Conference 2017 I D E N T I F I C A T I O N A N D M A N A G E M E N T O F D E L I R I U M E L I Z A B E T H M A G E R - O C O N N O R A C H P N DR
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
POST STROKE DELIRIUM. Dr Janet Ballantyne
 POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
PSYCHOSOCIAL SYMPTOMS (DELIRIUM)
") PSYCHOSOCIAL SYMPTOMS (DELIRIUM) Rut Kiman MD, MSc Head Pediatric Palliative Care Team Hospital Nacional Prof. A. Posadas Buenos Aires -Argentina Senior Lecturer. Pediatric Department School of Medicine.
PSYCHOSOCIAL SYMPTOMS (DELIRIUM) Rut Kiman MD, MSc Head Pediatric Palliative Care Team Hospital Nacional Prof. A. Posadas Buenos Aires -Argentina Senior Lecturer. Pediatric Department School of Medicine.
Delirium and Dementia
 Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Delirium. Steve Ellen
 Delirium Steve Ellen MB, BS. M.Med. MD. FRANZCP Head, Consultation, Liaison & Emergency Psychiatry, Alfred Health. Associate Professor, Monash Alfred Psychiatry Research Centre, Central Clinical School,
Delirium Steve Ellen MB, BS. M.Med. MD. FRANZCP Head, Consultation, Liaison & Emergency Psychiatry, Alfred Health. Associate Professor, Monash Alfred Psychiatry Research Centre, Central Clinical School,
Organic Mental Disorders. Organic Mental Disorders. Axes. Damrongsak Bulyalert Department of Internal Medicine
 Organic Mental Disorders Damrongsak Bulyalert Department of Internal Medicine www.metadon.net 1 Organic Mental Disorders In DSM (Diagnostic and Statistical Manual of Mental Disorders), OMD includes Delirium,
Organic Mental Disorders Damrongsak Bulyalert Department of Internal Medicine www.metadon.net 1 Organic Mental Disorders In DSM (Diagnostic and Statistical Manual of Mental Disorders), OMD includes Delirium,
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
The triad of inpatient harm
 Delirium in hospital: Identification, prevention and management Dr Jonathan Treml Consultant Geriatrician Queen Elizabeth Hospital Birmingham, UK With thanks to Dr Thomas Jackson for some of the slides
Delirium in hospital: Identification, prevention and management Dr Jonathan Treml Consultant Geriatrician Queen Elizabeth Hospital Birmingham, UK With thanks to Dr Thomas Jackson for some of the slides
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine
 Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Interprofessional Webinar Series
 Interprofessional Webinar Series Assessment and Management of Delirium Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure Slide Pauline Lesage, MD, LLM,
Interprofessional Webinar Series Assessment and Management of Delirium Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure Slide Pauline Lesage, MD, LLM,
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Delirium: developing and implementing a multi-component intervention
 Delirium: developing and implementing a multi-component intervention Dr. Duncan Forsyth Consultant Geriatrician Addenbrooke s Hospital Cambridge University Hospitals NHS Foundation Trust Cambridge, England
Delirium: developing and implementing a multi-component intervention Dr. Duncan Forsyth Consultant Geriatrician Addenbrooke s Hospital Cambridge University Hospitals NHS Foundation Trust Cambridge, England
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Delirium and Care Giving
 Delirium and Care Giving Marianne McCarthy, PhD, RN Advanced Practice Nurse Sun Health Geriatric Fellowship Program Associate Professor Arizona State University Presentation Questions What happens when
Delirium and Care Giving Marianne McCarthy, PhD, RN Advanced Practice Nurse Sun Health Geriatric Fellowship Program Associate Professor Arizona State University Presentation Questions What happens when
Disclosures No financial conflicts of interest. Key Questions
 Hospital Delirium: New Evidence in Diagnosis & Treatment Ethan Cumbler MD, FHM, FACP Professor of Medicine Medical Director Acute Care For Elderly Unit University of Colorado School of Medicine Disclosures
Hospital Delirium: New Evidence in Diagnosis & Treatment Ethan Cumbler MD, FHM, FACP Professor of Medicine Medical Director Acute Care For Elderly Unit University of Colorado School of Medicine Disclosures
Alcohol withdrawal. Clinical features
 Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Delirium in Palliative care. Presentation to Volunteers 2016 David Falk
 Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Mental Health Nursing: Organic Disorders. By Mary B. Knutson, RN, MS, FCP
 Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
Ohio/Minnesota Collaborative
 Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Dementia, Depression, and Delirium 2.0 Contact Hours Presented by: CEU Professor
 Dementia, Depression, and Delirium 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Dementia, Depression, and Delirium 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Delirium. Case Vignette. Case Vignette (continued) Case Vignette (concluded) PG2 Core Curriculum July 10, Ian A. Cook, M.D.
 Case Vignette (concluded) PG2 Core Curriculum July 10, Ian A. Cook, M.D.") Delirium PG2 Core Curriculum July 10, 2006 Ian A. Cook, M.D. UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience & Human Behavior Case Vignette
Delirium PG2 Core Curriculum July 10, 2006 Ian A. Cook, M.D. UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience & Human Behavior Case Vignette