King s College Hospital NHS Foundation Trust. Acute on Chronic Liver Failure: Practical management outside the tertiary centre.
|
|
|
- Belinda Dawson
- 5 years ago
- Views:
Transcription

1 King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy Unit Institute of Liver Studies Kings College Hospital United Kingdom


2 ACLF & Practical Management
3 ACLF & Practical Management Admissions: Liver Critical Care Kings College Hospital 2016/17 n=1569 Hepatobiliary Surgery Acute liver failure Chronic liver disease Transplants Previous Transplants Non Liver Patients
4 ACLF & Practical Management Intensive Care National Audit and Research Centre (ICNARC) Extrapolated numbers of cirrhosis ICU admissions and ICU deaths per 100,000 population (England, Wales & NI) Year Admissions Deaths ICNARC 2015 McPhail et al Manuscript Submitted 2017
5 Directly standardised mortality rate per 100,000 ACLF & Practical Management Mortality from chronic liver disease, all ages, England, , Directly standardised mortality rate Number of deaths (persons) 6,000 5,000 4,000 3,000 2,000 1,000 0 Number of deaths (persons) Source: NHS Atlas of Variation in healthcare for people with liver disease 2017 (In press)
6 Acute on Chronic Liver Failure (ACLF): Practical management outside the tertiary centre. Overview: ACLF in the natural history of Chronic Liver Disease. Definitions Controversies ACLF: practical Issues in clinical care. Getting access to ICU: avoiding futility. Ward Interventions: preventing ACLF. ACLF: how can your Liver Unit help? Transfer Transplantation.
7 Natural History Chronic Liver Disease. Compensated Cirrhosis No ascites or overt HE ~ 5-10% patients / year Recompensation of hepatic function Decompensated Cirrhosis Ascites, HE, Variceal bleeding
8 Natural History Chronic Liver Disease. D Amico et al J Hepatology 2006;44:
9 Natural History Chronic Liver Disease Complication 1Year Mortality Variceal Bleeding 20% Ascites 29% Ascites and Variceal Bleeding 49% Hepatic Encephalopathy 64% Jepsen et al Hepatology 2010;51: n=466
10 Natural History Chronic Liver Disease. Compensated Cirrhosis No ascites or overt HE ~ 5-10% patients / year Recompensation of hepatic function Decompensated Cirrhosis Ascites, HE, Variceal bleeding ~ 30% hospitalised patients Resolution of organ failures Acute on Chronic Liver Failure (ACLF) Hepatic and Extra-hepatic organ failure? Up to 50% hospitalised patients Death
11 ACLF & Practical Management Acute on Chronic Liver Failure (ACLF) Acute on chronic liver failure is a syndrome in patients with chronic liver disease with or without cirrhosis which is characterized by acute hepatic decompensation resulting in liver failure (jaundice and prolongation of the INR) and one or more extra-hepatic organ failures that is associated with increased mortality within a period of 28 days from onset.. World Congress of Gastroenterology Gastroenterology 2014 ;147(1);4-10
12 ACLF & Practical Management Who are we discussing? Cirrhotic Precipitating event Bleeding / Sepsis / Drug effect Hepatic failure Jaundiced, coagulopathic Extra-hepatic organ failure Encephalopathy Hypotension Renal dysfunction
13 ACLF & Practical Management CANONIC: Chronic liver failure Acute On-chronic liver failure In Cirrhosis 29 Liver Units, 8 European Countries 1343 Hospitalised patients with cirrhosis Develop a definition and scoring system for ACLF. Moreau et al Gastroenterology :
14 ACLF & Practical Management
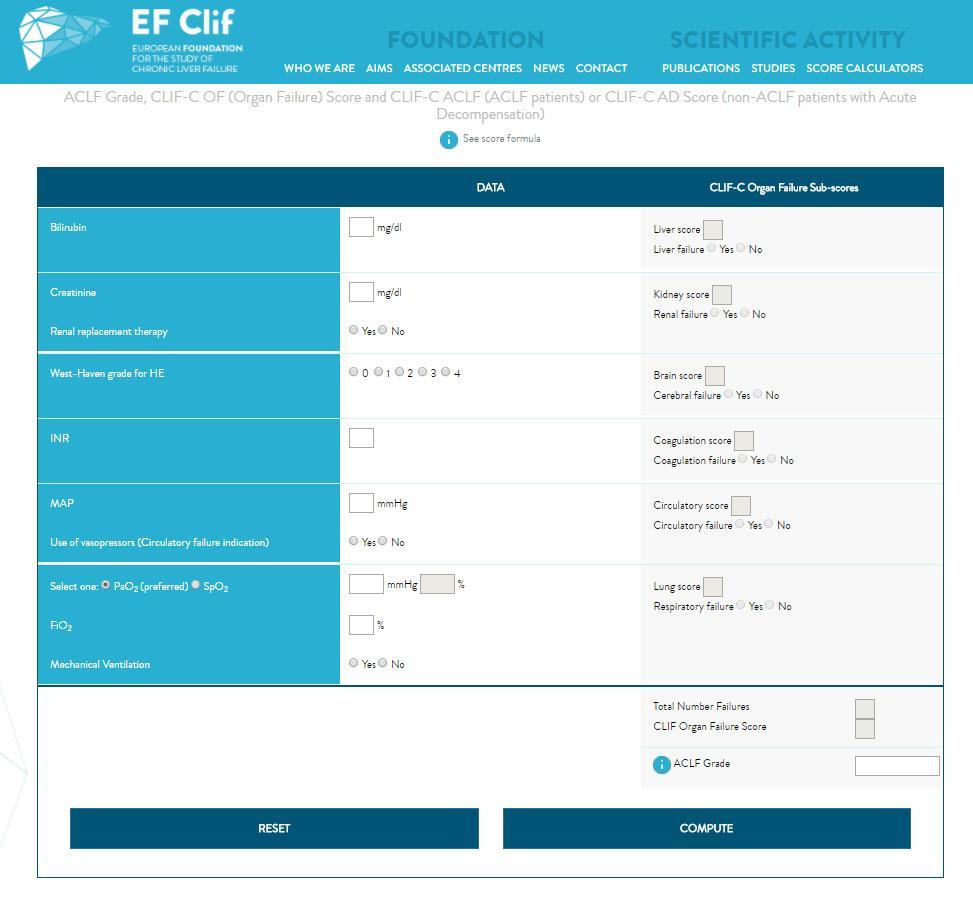
15 ACLF & Practical Management CLIF Organ Failures Organ System Hepatic Cerebral Renal Coagulation Circulation Respiratory Criteria Bilirubin 200 mmol / L Encephalopathy Grade 3 Creatinine 180 mmol/l and / or use of renal replacement therapy INR >2.5 and / or platelet count 20 x 109/L Use of vasopressor agents and / or terlipressin Ratio of partial pressure of oxygen/ inspired oxygen 200 or Ratio of Pulse oximetry saturation / inspired oxygen 214 Moreau et al Gastroenterology Jun;144(7): e9.
16 ACLF & Practical Management ACLF Grades ACLF-1 Renal or cerebral failure alone or renal dysfunction with other organ failure. ACLF-2 Two Organ Failures. ACLF-3 Three or More Organ Failures. Moreau et al Gastroenterology :
17 Mortality (%) ACLF & Practical Management ACLF Grade and Mortality No ACLF ACLF 1 ACLF 2 ACLF 3 28-Day 90-Day Moreau et al Gastroenterology :
18 % of ACLF Cases ACLF & Practical Management Reported Triggers to ACLF; Europe and China Reactivation HBV Bacterial Infection GI Bleed Active Alcohol Other Not Identifiable More than 1 CANONIC Shi et al CANONIC n=303 Gastro : Shi et al n=405 Hepatology :232-42
19 WBC x 10 9 /l CRP mg/l ACLF & Practical Management ACLF: Systemic Inflammation & Severity of Illness Inflammatory markers at enrolment in CANONIC Study. n=1343 Leucocyte Count C-Reactive Protein No ACLF ACLF 1 ACLF 2 ACLF No ACLF ACLF 1 ACLF 2 ACLF 3 Moreau et al Gastroenterology :
20 pg/ml ACLF & Practical Management Plasma Cytokine Concentrations according to Precipitating Event for ACLF Claria et al Hepatology (4) n=237 Measurements at study enrolment TNF-α Interleukin-6 Interleukin P<0.03 P< P<0.0001
21 ACLF & Practical Management ACLF: Definition Precipitating event, hepatic and extra-hepatic OF. High short term mortality. Key to research and defining practice. ACLF: Controversies Heterogeneous precipitants? Unified pathophysiology? No identifiable precipitants? Scores to instruct care?

22 ACLF & Practical Management. Critical Care: Inevitable Destination?
23 ACLF & Practical Management. Critical Care: Admission Impossible?
24 ACLF & Practical Management Escalation of care? NCEPOD 2013 Alcohol Related Liver Disease: Measuring the Units Both Advisors and clinicians identified patients in whom escalation of care was not received despite it being indicated....escalation of care should be actively pursued for patients with Alcohol-related Liver disease who deteriorate acutely and whose background functional status is good. There should be close liaison between the medical and critical care teams when making escalation decisions..



25 ACLF & Practical Management Escalation of care? Barriers to Critical Care: Aetiology.
26 ACLF & Practical Management Escalation of care? Barriers to Critical Care: Outcome Study Year n ICU Mortality Cholongitas et al % Alim Pharm Ther 2006;23: Fang et al % Neph Dial Trans 2008;23(6): Junea et al % J Crit Care 2009;24(3): Thompson et al % Aliment Pharmacol Ther 2010; 32: Das et al % Crit Care Med : Tu et al % Shock : Olemz et al % Ann Hepatol ; Levesque et al % J Hep : Frolich et al % J Crit Care ;6: 1131 McPhail et al % Clinical Gastro Hep 13(7)
27 ACLF & Practical Management Escalation of care? Barriers to Critical Care: Outcome Prognosis of cirrhotic patients admitted to intensive care unit: a meta-analysis. Weil et al Annals of Intensive Care :33 13 Studies 2532 patients Mortality ICU 43% Hospital 54% 6-Month 75%
28 ACLF & Practical Management Escalation of care? Barriers to Care: Resource Use Liver ITU Kings College Hospital ACLF admissions Patients 226 (42%) ICU mortality 80% 2 or more organ failures Average cost per Patient 28,409 Average cost per Survivor 23,206 Average cost per Non-survivor 37,329 Effective cost per Survivor 51,198 Shawcross et al J Hepatol 2012; 56(5):
29 ACLF & Practical Management Escalation of care? High resistance to ICU admission Constrained resources. Self inflicted aetiologies. High resource use and cost. ICU / Post-ITU Mortality high. Preconception of futility.
30 ACLF & Practical Management Escalation of care? Futile Critical Care? Mortality of cirrhotic patients admitted to LITU, Kings College Hospital n=971 p<0.001 Log-rank for comparison of Eras McPhail et al Clin Gastro Hep 2015;13:
31 ACLF & Practical Management Escalation of care? Avoiding Futility: Admission and level of support? Standard ICU considerations Age Co morbidity Functional / nutritional state Severity of acute illness Liver-specific considerations Liver disease severity Indication for admission
32 ACLF & Practical Management Escalation of care? Avoiding Futility: Age and Etiology? Weil et al Annals of Intensive Care :33
33 ACLF & Practical Management Escalation of care? Avoiding Futility: prognostic assessment? Scoring Tools Child-Pugh Classification (CPC) Model for End-stage Liver Disease (MELD) Sequential Organ Failure Assessment (SOFA) Chronic Liver Failure Score (CLIF)
34 ACLF & Practical Management Escalation of care? Avoiding Futility: prognostic assessment? Hospital Survival in ITU Admissions with Cirrhosis KCH n=933 Score AUROC (95% CI) CLIF ( ) SOFA ( ) APA II ( ) SAPS II ( ) MELD ( ) McPhail et al Clin Gastro Hep 2015;13:
35 ACLF & Practical Management Escalation of care? Avoiding Futility: prognostic assessment? Time of Assessment AUROC Score Admission 72 Hrs MELD SOFA CLIF-SOFA McPhail et al Clin Gastro Hep 2015;13:

36 ACLF & Practical Management Withdrawal of Care? Avoiding Futility: prognostic assessment. ACLF Scores to withdraw care? Hernaez et al Gut 2017; 61:

37 ACLF & Practical Management Avoiding Futility: Indications for Admission Variceal Bleeding Encephalopathy Renal failure
38 ACLF & Practical Management. Variceal Bleeding Avoiding Futility: Indication for Admission? P<0.001 McPhail et al Clin Gastro Hep 2015;13:
39 ACLF & Practical Management. Variceal Bleeding. Avoiding Futility: Indication for Admission? Weil et al Annals of Intensive Care :33
40 ACLF & Practical Management Variceal Bleeding Control the Airway Resuscitate Cultures and Antibiotics* Terlipressin* Endoscopic therapy* Band Ligation TIPS? *Evidence Base Level A
41 ACLF & Practical Management. Hepatic Encephalopathy Avoiding Futility: Indication for Admission? Critical Care Environment Nursing levels Compliance with Rx Airway Protection Seek Precipitant Fluids Treat Infection Minimise Medication Treat Constipation Adjunctive agents?
42 ACLF & Practical Management Hepatic Encephalopathy Avoiding Futility: Indication for Admission? Fichet et al J Crit Care 2009;24: Outcomes in 71 patients with CLD and ICU 45 with isolated HE: Median GCS 8/15 Median CPC 11 73% required intubation and ventilation Sole organ support ICU mortality 8.9%
43 ACLF & Practical Management. Hepatic Encephalopathy Complication 1Year Mortality Variceal Bleeding 20% Ascites 29% Ascites and Variceal Bleeding 49% Hepatic Encephalopathy 64% Jepsen et al Hepatology 2010;51: n=466
44 ACLF & Practical Management. Renal Failure. Renal Failure: Futile care? Cholongitis et al Eur J Gastroenterol Hepatol 21: Royal Free Hospital London ICU admissions with Cirrhosis (Mortality 62%) RRT/ Creatinine >300 micmol/l / Urine <500ml/24 hrs (ARF) ARF No ARF p n Mortality 91% 47% < Odds Ratio 13.1 (95% CI )
45 ACLF & Practical Management. Renal Failure. Weil et al Annals of Intensive Care :33
46 ACLF & Practical Management. Renal Failure. Renal Failure and Chronic Liver Disease: Heterogeneity. Martin-Llahi et al Gastro 2011:140: Patients with Cirrhosis and renal failure Serum Creatinine >1.5 mg/dl at 2 points within 48 hours Cause % 3 Month Survival Infection-related 46% 31% Hypovolaemia 32% 46% Hepato-renal 13% 15% Parenchymal 9% 73%

 Antibiotics Vasopressors Terlipressin Decompress")
47 ACLF & Practical Management. Renal Failure. Evolving Renal failure: Stop nephrotoxic therapies Volume expand Albumin (?) Antibiotics Vasopressors Terlipressin Decompress Paracentesis Critical Care review
48 ACLF & Practical Management. Renal Failure. Circulating Volume Expansion: Albumin? Thevenot et al Journal of Hepatology 2015(62); Multi-centre RCT. Hospitalised Cirrhotics with non-sbp sepsis (n=193) Daily 20% Albumin + SMT vs. SMT Renal Failure Survival
49 ACLF & Practical Management. Renal Failure. Vasoconstrictors: Terlipressin Systematic Review of Randomised Trials on Vasoconstrictor Drugs for Hepato-renal syndrome Gluud et al Hepatology 2010;51(2)
50 ACLF & Practical Management. Renal Failure: Early Intervention. Response to Terlipressin: Predictors Responders Non-responders p (n=12) (n=34) Creatinine (μmol/l) 256 (±71) 369 (± 194) <0.001 Urine Vol. (ml/24hrs) 880 (± 440) 496 (± 420) WBC 6.6 (± 3.5) 10.9 (± 8.1) EARLY Intervention Martin-Llahi M et al Gastroenterology 2008:134
51 ACLF & Practical Management. Prevention: Early Ward Intervention Cirrhosis and Outcome of Septic Shock Arabi et al Hepatology 2012 ;56: n=638 Cirrhosis and Septic Shock ICU Mortality 62% Adjusted OR p Inappropriate Antimicrobials 9.5 (4.3-21) <0.001 Single vs. Combination Rx 1.8 ( ) <0.05 Delay to Administration 1.1 ( ) <0.001
52 ACLF & Practical Management. Prevention: Early Ward Intervention Cirrhosis and Outcome of Septic Shock: Antibiotic Delay Arabi et al Hepatology 2012 ;56: Adjusted OR ; APACHE II, MELD, Immune compromise, Culture +ve
53 ACLF & Practical Management. Prevention: Early Ward Interventions. Timely and effective bedside review: Recognition of illness severity. Recognition of risk of deterioration. Escalation & Critical Care review. Antibiotic Therapy Prompt, appropriate. Intravenous Fluids Prescription Chart Review
54 ACLF & Practical Management. Critical Care Admission & Level of therapy? Standard ICU criteria Age Nutritional state & Physiologic reserve Co-morbidity Severity of acute illness Severity of underlying liver disease How severity is measured may not be important Response to therapy key Indication for admission Variceal bleeding Isolated HE
55 ACLF & Practical Management. Critical Care Admission & Level of therapy? Difficult decisions Is there a right answer? Resource considerations Give the patient the benefit of the doubt? Consider short and medium term prognosis. If in doubt, admit and treat Aggressive short term therapy Review after hours Set ceilings for therapy Consider withdrawal if no response.
56 Bed Occupancy ACLF & Practical Management. How can your Liver Unit Help? Bed Occupancy: Liver Intensive Therapy Unit, Kings College Hospital October 2016-May % 100% 80% 60% 40% 20% 0% Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17
57 ACLF & Practical Management. How can your Liver Unit help? Always happy to discuss (!) Getting early interventions right. ICU Admission / Escalation / withdrawal decisions. Consideration for Transfer Age Complexity Specialist Radiology / Endoscopy Transplant wait-listed patients Expedited Transplantation?
58 ACLF & Practical Management Futile Hospital Care? Cirrhosis: Hospital Mortality in USA Schmidt et al Gastroenterology 2015;148:

59 ACLF & Practical Management. How can your Liver Unit help? Expedited Transplantation?
60 90-Day Mortality ACLF & Practical Management. Expedited Transplantation? Inferior Outcomes 90-Day Patient Survival for First Elective Liver Transplant for Cirrhosis By Pre-LT status. United Kingdom n=7479 p< % 18% 16% 14% 12% 10% 8% 6% 4% 2% 0% Outpatient Inpatient; No Organ Failure Inpatient: Organ Failure Bernal et al Clinical Liver Disease 2017 In Press.
61 ACLF & Practical Management. Expedited Transplantation? Resource use and cost? Markley Earl et al Transplantation 2008;86: Cost analysis: Single Centre: 163 first transplants for CLD Pre-transplant ICU stay Median Cost / LT (IQR) No n=149 (91%) $81,134 (73,800-97,113) Yes n=14 (9%) $149,890 (132, ,964) p<0.0001
62 ACLF & Practical Management. Expedited Transplantation? Practicalities? Finklestedt et al Liver Transplantation : n= % Fulfilling ACLF Criteria (n=144) Not Evaluated (n=50) 67% Evaluated for LT (n=94) Not Listed (n=23) 49% Listed for LT (n=71) Waitlist Mortality 54% Died on Waitlist (n=36) 23% Underwent LT (n=33) Died (n=5) 19% Survived (n=28)
63 ACLF & Practical Management. Expedited Transplantation? An option only in a small minority Contraindications Waitlist deterioration Outcomes probably worse Highly selective use Previously assessed Young Seldom from ICU Minimal organ support
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
King s College Hospital NHS Foundation Trust. Acute Liver Disease: what you really need to know.
 King s College Hospital NHS Foundation Trust Acute Liver Disease: what you really need to know. William Bernal Professor of Liver Critical Care Liver Intensive Therapy Unit Institute of Liver Studies Kings
King s College Hospital NHS Foundation Trust Acute Liver Disease: what you really need to know. William Bernal Professor of Liver Critical Care Liver Intensive Therapy Unit Institute of Liver Studies Kings
Infections In Cirrhotic patients. Dr Abid Suddle Institute of Liver Studies King s College Hospital
 Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Acute Liver Failure. Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018
 Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Hepatology on the AMU
 Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
PACT module Acute hepatic failure. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management
 HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
NCEPOD - Measuring the Units; A review of patients who died with alcohol-related liver disease
 NCEPOD - Measuring the Units; A review of patients who died with alcohol-related liver disease Hospital Number Admission to hospital 5. Trusts should ensure that medical patients are reviewed by a consultant
NCEPOD - Measuring the Units; A review of patients who died with alcohol-related liver disease Hospital Number Admission to hospital 5. Trusts should ensure that medical patients are reviewed by a consultant
ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS.
 ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS. Vicente Arroyo 1, 2, Rajiv Jalan 2, 3 1 Institut de Investigacions Biomèdiques August Pi I Sunyer. University of Barcelona.
ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS. Vicente Arroyo 1, 2, Rajiv Jalan 2, 3 1 Institut de Investigacions Biomèdiques August Pi I Sunyer. University of Barcelona.
Title: CLIF-C ACLF score is a better mortality. patients with Acute on Chronic Liver Failure admitted to the ward
 Title: CLIF-C ACLF score is a better mortality predictor than MELD, MELD-Na and CTP in patients with Acute on Chronic Liver Failure admitted to the ward Authors: Rita Barosa, Lídia Roque Ramos, Marta Patita,
Title: CLIF-C ACLF score is a better mortality predictor than MELD, MELD-Na and CTP in patients with Acute on Chronic Liver Failure admitted to the ward Authors: Rita Barosa, Lídia Roque Ramos, Marta Patita,
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
PACT module Acute hepatic failure. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
CONTROLLED DOCUMENT. Cirrhosis Care Bundle CATEGORY: Clinical Guidelines. CLASSIFICATION: Clinical. Controlled Document CG201 Number:
 Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Korean Multicenter Cohort Study of Acute-on- Chronic Liver Failure : Korean Acute-on-Chronic Liver Failure Study (KACLiF)
") 2015 KASL Single Topic Symposium Korean Multicenter Cohort Study of Acute-on- Chronic Liver Failure : Korean Acute-on-Chronic Liver Failure Study (KACLiF) Do Seon Song Department of Internal Medicine,
2015 KASL Single Topic Symposium Korean Multicenter Cohort Study of Acute-on- Chronic Liver Failure : Korean Acute-on-Chronic Liver Failure Study (KACLiF) Do Seon Song Department of Internal Medicine,
Outcome Prediction for Critically Ill Egyptian Cirrhotic Patients in Liver Intensive Care Unit
 Med. J. Cairo Univ., Vol. 85, No. 4, June: 1571-1575, 2017 www.medicaljournalofcairouniversity.net Outcome Prediction for Critically Ill Egyptian Cirrhotic Patients in Liver Intensive Care Unit AMANY ABDEL-MAQSOD,
Med. J. Cairo Univ., Vol. 85, No. 4, June: 1571-1575, 2017 www.medicaljournalofcairouniversity.net Outcome Prediction for Critically Ill Egyptian Cirrhotic Patients in Liver Intensive Care Unit AMANY ABDEL-MAQSOD,
Critical care and cirrhosis: outcome and benefit Julia Wendon, William Bernal, Chris Willars and Georg Auzinger
 Critical care and cirrhosis: outcome and benefit Julia Wendon, William Bernal, Chris Willars and Georg Auzinger Institute of Liver Studies, Kings College Hospital, Denmark Hill, London, UK Correspondence
Critical care and cirrhosis: outcome and benefit Julia Wendon, William Bernal, Chris Willars and Georg Auzinger Institute of Liver Studies, Kings College Hospital, Denmark Hill, London, UK Correspondence
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
APPROPRIATE PATIENT SELECTION AS A KEY TO INCREASE THE BENEFIT/RISK RATIO FOR ELAD
 APPROPRIATE PATIENT SELECTION AS A KEY TO INCREASE THE BENEFIT/RISK RATIO FOR ELAD Ram Subramanian M.D. Hepatology and Critical Care Emory University School of Medicine Atlanta, USA OUTLINE Review the
APPROPRIATE PATIENT SELECTION AS A KEY TO INCREASE THE BENEFIT/RISK RATIO FOR ELAD Ram Subramanian M.D. Hepatology and Critical Care Emory University School of Medicine Atlanta, USA OUTLINE Review the
PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS
 PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS Dr. J. Fernández. Head of the Liver Unit Hospital Clinic Barcelona, Spain AEEH Postgraduate Course, Madrid, February 15 2017 Prevalence of
PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS Dr. J. Fernández. Head of the Liver Unit Hospital Clinic Barcelona, Spain AEEH Postgraduate Course, Madrid, February 15 2017 Prevalence of
Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis
 Thursday 11 th June 2015 Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis Dr Duncan Wyncoll Guy s & St Thomas NHS Trust, London Conflicts of Interest In
Thursday 11 th June 2015 Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis Dr Duncan Wyncoll Guy s & St Thomas NHS Trust, London Conflicts of Interest In
Adrenal Insufficiency in Patients with Liver Cirrhosis and Severe Sepsis: Effect on Survival after Treatment with Hydrocortisone ABSTRACT
 20 Original Article Adrenal Insufficiency in Patients with Liver Cirrhosis and Severe Sepsis: Effect on Survival after Treatment with Hydrocortisone Pattanasirigool C Prasongsuksan C Settasin S Letrochawalit
20 Original Article Adrenal Insufficiency in Patients with Liver Cirrhosis and Severe Sepsis: Effect on Survival after Treatment with Hydrocortisone Pattanasirigool C Prasongsuksan C Settasin S Letrochawalit
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Optimal management of ascites
 Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The Usefulness of Sepsis Biomarkers. Dr Vineya Rai Department of Anesthesiology University of Malaya
 The Usefulness of Sepsis Biomarkers Dr Vineya Rai Department of Anesthesiology University of Malaya 1 What is Sepsis? Whole Body Inflammatory State + Infection 2 Incidence and Burden of Sepsis in US In
The Usefulness of Sepsis Biomarkers Dr Vineya Rai Department of Anesthesiology University of Malaya 1 What is Sepsis? Whole Body Inflammatory State + Infection 2 Incidence and Burden of Sepsis in US In
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Systemic Inflammatory Response Syndrome and MELD Score in Hospital Outcome of Patients with Liver Cirrhosis
 168 Original Article Systemic Inflammatory Response Syndrome and MELD Score in Hospital Outcome of Patients with Liver Cirrhosis Ramin Behroozian 1*, Mehrdad Bayazidchi 1, Javad Rasooli 1 1. Department
168 Original Article Systemic Inflammatory Response Syndrome and MELD Score in Hospital Outcome of Patients with Liver Cirrhosis Ramin Behroozian 1*, Mehrdad Bayazidchi 1, Javad Rasooli 1 1. Department
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Management of critically-ill cirrhotic patients
 Management of critically-ill cirrhotic patients Pere Ginès 1,2, *, Javier Fernández 1,François Durand 2, Faouzi Saliba 3 1 Liver Unit, IMDiM, Hospital Clinic Barcelona, University of Barcelona and IDIBAPS
Management of critically-ill cirrhotic patients Pere Ginès 1,2, *, Javier Fernández 1,François Durand 2, Faouzi Saliba 3 1 Liver Unit, IMDiM, Hospital Clinic Barcelona, University of Barcelona and IDIBAPS
Current Concepts in Diagnosis and Management of Acute Liver Failure
 Current Concepts in Diagnosis and Management of Acute Liver Failure Oren Fix, MD, MSc, FACP, AGAF, FAASLD Medical Director, Liver Transplant Program Swedish Medical Center Seattle, WA Learning Objectives
Current Concepts in Diagnosis and Management of Acute Liver Failure Oren Fix, MD, MSc, FACP, AGAF, FAASLD Medical Director, Liver Transplant Program Swedish Medical Center Seattle, WA Learning Objectives
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
ASSESSMENT AND MANAGEMENT OF POTENTIAL LIVER TRANSPLANT CANDIDATES
 ASSESSMENT AND MANAGEMENT OF POTENTIAL LIVER TRANSPLANT CANDIDATES James YY Fung MBChB, MD, FRACP, FHKCP, FHKAM Consultant & Hon. Assoc. Professor Liver Transplant Center Department of Surgery, Queen Mary
ASSESSMENT AND MANAGEMENT OF POTENTIAL LIVER TRANSPLANT CANDIDATES James YY Fung MBChB, MD, FRACP, FHKCP, FHKAM Consultant & Hon. Assoc. Professor Liver Transplant Center Department of Surgery, Queen Mary
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Developed for Scotland by the National Plasma Product Expert Advisory Group. Clinical Guidelines for Human Albumin Use
 Approved by NPPEAG 28 May 2018 Reviewed 1 June 2018 To be reviewed 1 June 2020 Developed for Scotland by the National Plasma Product Expert Advisory Group Clinical Guidelines for Human Albumin Use 1 National
Approved by NPPEAG 28 May 2018 Reviewed 1 June 2018 To be reviewed 1 June 2020 Developed for Scotland by the National Plasma Product Expert Advisory Group Clinical Guidelines for Human Albumin Use 1 National
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Hepatorenal syndrome a defined entity with a standard treatment?
 Hepatorenal syndrome a defined entity with a standard treatment? Falk Symposium 162 Dresden - October 14, 2007 Alexander L. Gerbes Klinikum of the University of Munich Grosshadern Department of Medicine
Hepatorenal syndrome a defined entity with a standard treatment? Falk Symposium 162 Dresden - October 14, 2007 Alexander L. Gerbes Klinikum of the University of Munich Grosshadern Department of Medicine
Sepsis-3: clarity or confusion
 Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
KDIGO (Kidney Disease: Improving Global Outcomes) criteria as a predictor of hospital mortality in cirrhotic patients
 criteria as a predictor of hospital mortality in cirrhotic patients") KDIGO (Kidney Disease: Improving Global Outcomes) criteria as a predictor of hospital mortality in cirrhotic patients LIVER Murat Bıyık 1, Hüseyin Ataseven 1, Zeynep Bıyık 2, Mehmet Asil 1, Sami Çifçi
KDIGO (Kidney Disease: Improving Global Outcomes) criteria as a predictor of hospital mortality in cirrhotic patients LIVER Murat Bıyık 1, Hüseyin Ataseven 1, Zeynep Bıyık 2, Mehmet Asil 1, Sami Çifçi
Autoimmune Hepatitis: Defining the need for Liver Transplantation
 Autoimmune Hepatitis: Defining the need for Liver Transplantation Michael A Heneghan, MD, MMedSc, FRCPI. Institute of Liver Studies, King s College Hospital, London Outline Autoimmune Hepatitis Background
Autoimmune Hepatitis: Defining the need for Liver Transplantation Michael A Heneghan, MD, MMedSc, FRCPI. Institute of Liver Studies, King s College Hospital, London Outline Autoimmune Hepatitis Background
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
JMSCR Vol 05 Issue 11 Page November 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.33 Prevalence of Hyponatremia among patients
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.33 Prevalence of Hyponatremia among patients
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of
 Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Supplementary Online Content
 Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Update in abdominal Surgery in cirrhotic patients
 Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Alcoholic Hepatitis: Routine Screening for Early Recognition and Management. Juan Guerrero, MD
 Alcoholic Hepatitis: Routine Screening for Early Recognition and Management Juan Guerrero, MD Global Problem 1% of GNP of medium/high income countries Additional societal costs Disproportionately affects
Alcoholic Hepatitis: Routine Screening for Early Recognition and Management Juan Guerrero, MD Global Problem 1% of GNP of medium/high income countries Additional societal costs Disproportionately affects
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Type of intervention Treatment. Economic study type Cost-effectiveness analysis.
 Albumin dialysis in cirrhosis with superimposed acute liver injury: possible impact of albumin dialysis on hospitalization costs Hassanein T, Oliver D, Stange J, Steiner C Record Status This is a critical
Albumin dialysis in cirrhosis with superimposed acute liver injury: possible impact of albumin dialysis on hospitalization costs Hassanein T, Oliver D, Stange J, Steiner C Record Status This is a critical
Fluid balance in Critical Care
 Fluid balance in Critical Care By Dr HP Shum Nephrologist and Critical Care Physician Department of Intensive Care, PYNEH Fluid therapy is a critical aspect of initial acute resuscitation in critically
Fluid balance in Critical Care By Dr HP Shum Nephrologist and Critical Care Physician Department of Intensive Care, PYNEH Fluid therapy is a critical aspect of initial acute resuscitation in critically
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
Case Report: Acute-on-Chronic Liver Failure: Making the Diagnosis between Infection and Acute Alcoholic Hepatitis
 Diagnostic Problems in Hepatology 181 Case Report: Acute-on-Chronic Liver Failure: Making the Diagnosis between Infection and Acute Alcoholic Hepatitis Carmen Sendra, MD 1 Javier Ampuero, MD, PhD 1,2 Álvaro
Diagnostic Problems in Hepatology 181 Case Report: Acute-on-Chronic Liver Failure: Making the Diagnosis between Infection and Acute Alcoholic Hepatitis Carmen Sendra, MD 1 Javier Ampuero, MD, PhD 1,2 Álvaro
In the setting of liver failure & transplantation?
 ECMO: In the setting of liver failure & transplantation? Dr. Robert Loveridge MA LL.M MRCP FRCA FFICM Consultant in adult & liver intensive care medicine King s College Hospital NHS Foundation Trust What
ECMO: In the setting of liver failure & transplantation? Dr. Robert Loveridge MA LL.M MRCP FRCA FFICM Consultant in adult & liver intensive care medicine King s College Hospital NHS Foundation Trust What
Characteristics, Diagnosis and Prognosis of Acute-on-Chronic Liver. Failure in Cirrhosis Associated to Hepatitis B.
 Supplementary Appendix Characteristics, Diagnosis and Prognosis of Acute-on-Chronic Liver Failure in Cirrhosis Associated to Hepatitis B. Hai Li, Liu-Ying Chen, Nan-nan Zhang, Shu-Ting Li, Bo Zeng, Marco
Supplementary Appendix Characteristics, Diagnosis and Prognosis of Acute-on-Chronic Liver Failure in Cirrhosis Associated to Hepatitis B. Hai Li, Liu-Ying Chen, Nan-nan Zhang, Shu-Ting Li, Bo Zeng, Marco
Updates in Emergency Department Management of Sepsis
 Resident Journal Review Updates in Emergency Department Management of Sepsis Authors: Eli Brown, MD; Allison Regan, MD; Kaycie Corburn, MD; Jacqueline Shibata, MD Edited by: Jay Khadpe, MD FAAEM; Michael
Resident Journal Review Updates in Emergency Department Management of Sepsis Authors: Eli Brown, MD; Allison Regan, MD; Kaycie Corburn, MD; Jacqueline Shibata, MD Edited by: Jay Khadpe, MD FAAEM; Michael
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present:
 and the International Coalition of Hepatology Education Providers (IC-HEP) present:") The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatic Encephalopathy Hepatic Encephalopathy:
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatic Encephalopathy Hepatic Encephalopathy:
BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency
 BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency Medicine 1 NO CONFLICT OF INTEREST 2 We do not fully understand
BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency Medicine 1 NO CONFLICT OF INTEREST 2 We do not fully understand
Hepatorenal syndrome. Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover
 Hepatorenal syndrome Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical
Hepatorenal syndrome Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
According to European Association for the Study
 LIVER FAILURE/CIRRHOSIS/PORTAL HYPERTENSION Acute-on-Chronic Liver Failure Precipitated by Hepatic Injury Is Distinct From That Precipitated by Extrahepatic Insults Yu Shi, 1 Ying Yang, 1 Yaoren Hu, 2
LIVER FAILURE/CIRRHOSIS/PORTAL HYPERTENSION Acute-on-Chronic Liver Failure Precipitated by Hepatic Injury Is Distinct From That Precipitated by Extrahepatic Insults Yu Shi, 1 Ying Yang, 1 Yaoren Hu, 2
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia. Jess Hwang 11/8/12
 58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
Does this patient need ICU?
 Disclaimer Does this patient need ICU? Jacqueline M. Pflaum-Carlson, MD Department of Emergency Medicine Division of Critical Care Medicine Henry Ford Hospital Detroit, MI Not a comprehensive review Trauma
Disclaimer Does this patient need ICU? Jacqueline M. Pflaum-Carlson, MD Department of Emergency Medicine Division of Critical Care Medicine Henry Ford Hospital Detroit, MI Not a comprehensive review Trauma
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
London Strategic Clinical Networks. Quality Standard. Version 1.0 (2015)
") London Strategic Clinical Networks Quality Standard Version 1.0 (2015) Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net @LondonAKI Overview The management
London Strategic Clinical Networks Quality Standard Version 1.0 (2015) Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net @LondonAKI Overview The management
European. Young Hepatologists Workshop. Organized by : Quantification of fibrosis and cirrhosis outcomes
 supported by from Gilea Quantification of fibrosis and cirrhosis outcomes th 5 European 5 European Young Hepatologists Workshop Young Hepatologists Workshop August, 27-29. 2015, Moulin de Vernègues Vincenza
supported by from Gilea Quantification of fibrosis and cirrhosis outcomes th 5 European 5 European Young Hepatologists Workshop Young Hepatologists Workshop August, 27-29. 2015, Moulin de Vernègues Vincenza
Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010
 Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010 Background- Critical Care Critical Care originated in Denmark with Polio epidemic 1950s respiratory support alone Rapid
Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010 Background- Critical Care Critical Care originated in Denmark with Polio epidemic 1950s respiratory support alone Rapid
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Management of Decompensated Chronic Hepatitis B
 Management of Decompensated Chronic Hepatitis B Dr James YY Fung, FRACP, MD Department of Medicine The University of Hong Kong Liver Transplant Center Queen Mary Hospital State Key Laboratory for Liver
Management of Decompensated Chronic Hepatitis B Dr James YY Fung, FRACP, MD Department of Medicine The University of Hong Kong Liver Transplant Center Queen Mary Hospital State Key Laboratory for Liver
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
ORIGINAL ARTICLE. See Editorial on Page 384
 LIVER TRANSPLANTATION 18:405-412, 2012 ORIGINAL ARTICLE Comparison of the Sequential Organ Failure Assessment Score With the King s College Hospital Criteria and the Model for End-Stage Liver Disease Score
LIVER TRANSPLANTATION 18:405-412, 2012 ORIGINAL ARTICLE Comparison of the Sequential Organ Failure Assessment Score With the King s College Hospital Criteria and the Model for End-Stage Liver Disease Score
Complication of Portal Hypertension: should the patients in the waiting list be treated differently?
 Wilma Debernardi Venon Gastroepatologia, Az. Osp. San Giovanni Battista ditorino Complication of Portal Hypertension: should the patients in the waiting list be treated differently? Il sottoscritto dichiara
Wilma Debernardi Venon Gastroepatologia, Az. Osp. San Giovanni Battista ditorino Complication of Portal Hypertension: should the patients in the waiting list be treated differently? Il sottoscritto dichiara
CLIF Consortium. Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study
 Core Study") CLIF Consortium Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study Case Report Form (Final) Center: Investigator: Investigator s Signature: The highlighted information
CLIF Consortium Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study Case Report Form (Final) Center: Investigator: Investigator s Signature: The highlighted information
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Hepatology cases for the generalist. Will Gelson Consultant Hepatologist Addenbrooke s Hospital
 Hepatology cases for the generalist Will Gelson Consultant Hepatologist Addenbrooke s Hospital 30 y o man with upper GI haemorrhage Background heavy alcohol use Hxof 3 pint haematemesis P 100, BP 90/40,
Hepatology cases for the generalist Will Gelson Consultant Hepatologist Addenbrooke s Hospital 30 y o man with upper GI haemorrhage Background heavy alcohol use Hxof 3 pint haematemesis P 100, BP 90/40,
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES
 SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,