Case Report Effective Endovascular Stenting of Malignant Portal Vein Obstruction in Pancreatic Cancer
|
|
|
- Hugo Parker
- 5 years ago
- Views:
Transcription
1 HPB Surgery Volume 2009, Article ID , 5 pages doi: /2009/ Case Report Effective Endovascular Stenting of Malignant Portal Vein Obstruction in Pancreatic Cancer Christian M. Ellis, Sadashiv Shenoy, Alan Litwin, Stephanie Soehnlein, and John F. Gibbs RoswellPark CancerInstitute,State Universityof NewYork at Buffalo, Buffalo, NY 14263, USA Correspondence should be addressed to John F. Gibbs, john.gibbs@roswellpark.org Received 3 April 2009; Accepted 24 July 2009 Recommended by Christos Dervenis We report herein the case of a patient successfully treated by transhepatic portal venous stent placement for malignant portal vein obstruction with associated gastric and small bowel varices and repeated gastrointestinal bleeding. CT angiography and portography showed severe portal vein obstruction from recurrent pancreatic cancer 15 months following pancreaticoduodenectomy with tumor encasement and dilated collateral veins throughout the gastric and proximal small bowel wall as the suspected cause of the GI bleeding. Successful transhepatic endovascular stent placement of the splenic vein at the portal vein confluence followed by balloon dilation was performed with immediate decompression of the gastric and small bowel varices and relief of GI hemorrhage in this patient until his death four months later. The treatment for patients with this dilemma can prove to be difficult, but as we have shown endovascular stenting of the portal system is an effective treatment option. Copyright 2009 Christian M. Ellis et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 1. Introduction Pancreatic cancer remains a major oncologic challenge making up 2% of all new cancer cases and 6% of cancer deaths in the United States [1]. Although some cancer centers report up to 20% 5-year survival rate after pancreaticoduodenectomy, the outlook, morbidity, and mortality for this disease remain bleak [2]. Therefore, in patients who develop recurrent metastatic disease, new methods of treatment and palliation are necessary to improve their quality of life. In cases of malignant portal venous obstruction from tumor, such as in hepatocellular carcinoma, cholangiocarcinoma, and pancreatic cancer endovascular stents have demonstrated the ability to relieve symptoms associated with this type of presentation [3]. We report the case of a patient after pancreaticoduodenectomy who developed near complete splenic vein obstruction with symptomatic gastric and small bowel mesenteric varices that was revascularized by transhepatic placement of an endovascular stent into the splenic vein (SV) at the portal vein (PV) confluence. 2. Case Report A 58-year-old man was referred to our institution for a suspicious mass within the neck of the pancreas with a dilated pancreatic duct and evidence of chronic pancreatitis identified by abdominal computed tomography (CT). An endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP) identified adult diagnosed pancreatic divisum with a 2.5 cm mass within the neck of the pancreas and pancreatic duct stricture. A fine needle aspiration (FNA) of this area showed only chronic inflammation and a CA 19-9 level returned within normal limits. Review at our institutional multidisciplinary conference led to recommendations for surgical resection, and ten months after his initial presenting symptoms, the patient underwent a pylorus-preserving pancreaticoduodenectomy. The final pathology revealed a specimen with chronic pancreatitis and one small focus of invasive carcinoma with perineural invasion. No tumor was identified in twenty-one lymph nodes. All surgical margins were negative for tumor. The patient made an uneventful recovery and afterward elected to forego any further adjuvant treatments. The patient did well while undergoing routine surveillance until approximately 15 months later when he began to experience mild to moderate abdominal discomfort and nausea. A repeat CT scan of the abdomen revealed a mass at the site of the previous surgical resection with narrowing of the PV confluence and extensive lymphadenopathy at the root of the mesentery. An ultrasound-guided biopsy of
")
 bleeding, requiring multiple blood transfusions, and on upper endoscopy was found to be due to varices of the proximal gastric wall,")

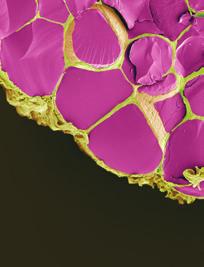
2 2 Figure 1: CT evidence of the recurrent pancreatic mass in the previous surgical bed (large arrow) and demonstration of obstruction of the splenic vein at the portal vein confluence (small arrow). this area confirmed recurrent well-differentiated adenocarcinoma, and the patient began concurrent chemoradiotherapy with continuous infusion 5-fluorouracil and external beam radiation therapy (EBRT) for a total dose of 54 Gy. On follow-up the patient developed upper gastrointestinal (GI) bleeding, requiring multiple blood transfusions, and on upper endoscopy was found to be due to varices of the proximal gastric wall, which appeared to extended through the anastamosis into the efferent jejunal limb. At the time of endoscopy there was no evidence of active bleeding, and so we elected to proceed with medical management for the patient to include β-blockers and intravenous octreotide. During the same hospitalization the patient again developed variceal bleeding. We found that the recurrent pancreatic tumor had caused a high-grade neoplastic obstruction of the SV at the PV confluence and as a consequence resulted in mesenteric hypertension and gastric and small bowel varices that were refractory to our medical management (Figures 1, 2, and 3). Because of this treatment dilemma we sought the expertise of our interventional radiology department who confirmed the SV obstruction and dilated varices by transhepatic portography (Figure 4). They were then able to successfully treat the patient by transhepatic endovascular stenting of the SV obstruction with a 10 mm 42 mm wall stent followed by an 8 mm balloon dilation. Repeat splenic venography demonstrated the PV confluence to be patent with good flow across the stent along with dramatic decompression of the collateral gastric and small bowel varices (Figure 5). Immediately after the procedure the patient had no additional episodes of melena or hematemesis, and no further blood transfusions were required. Seven days following the procedure the patient was discharged home from the hospital tolerating an advancing diet. He died 4 months later from HPB Surgery Figure 2: CT angiography coronal plane reconstruction showing the portal vein system with obstruction from the recurrent pancreatic tumor at the portal vein confluence (white arrow) and resulting gastric and small bowel varices (black arrows). Figure 3: Isolated portal system reconstruction defining the obstruction of the splenic vein at the portal vein confluence (block arrow) and clear confirmation of the subsequent gastric and small bowel varices (normal arrows). natural progression of the malignancy. During this time, he did not experience any additional episodes of GI bleeding and remained relatively comfortable. 3. Discussion Pancreatic cancer remains an oncologic challenge where early metastatic relapse after complete resection is frequently encountered. Sperti et al reported local and hepatic recurrence rates of 72% and 62%, respectively, in patients undergoing curative resection [4]. In the current study,
 with dramatic decompression of the proximal varices (black")

3 HPB Surgery 3 Figure 4: Transhepatic portography characterizing the splenic vein obstruction from the recurrent pancreatic tumor (white arrow) with dilated varices proximally (black arrows). Figure 5: Transhepatic portography after endovascular stent placement and balloon dilation of the splenic vein obstruction (white arrow) with dramatic decompression of the proximal varices (black arrows). our patient presented with a 2.5 cm mass arising in the background of pancreatic divisum and chronic pancreatitis. On final pathology, he was found to have Stage I T1N0 disease. The only poor prognostic factor identified was perineural involvement. In a recent review, perineural invasion was noted in 70% of patients and was associated with a significantly poorer median disease free survival of 16.2 months [5]. We believe that the recurrence noted in our patient involved the extrapancreatic nerve plexus [6]. Alternatively, the site of recurrence may be argued secondary to occult multifocal pancreatic cancer. The lack of pancreatic intraepithelial neoplasia within the resected specimen and numerous follow-up imaging is against the later argument. Extrahepatic portal venous obstruction accounts for 5% 10% of all cases of portal hypertension, with neoplasms such as hepatocellular carcinoma and pancreatic and biliary cancer accounting for 15% 24% of those cases [3]. Cancer can lead to thrombosis of the portal venous system through a combination of factors including cancer-related prothrombogenic changes, tumor invasion, periportal fibrosis following surgery or radiotherapy, or more commonly from extrinsic compression or constriction from tumor mass [7, 8]. Other causes of portal hypertension from extrahepatic occlusion or thrombosis include infection complicated by peritonitis, liver abscess, biliary tract surgery, and congenital abnormalities [9]. Coagulopathies that lead to thrombosis and thrombophlebitis migrans can also be a cause [9]. Prehepatic portal hypertension from portal vein stenosis or occlusion secondary to malignant invasion is a difficult entity to diagnose and treat. This difficulty is exemplified by the fact that occlusion of the portal vein frequently does not produce an acute manifestation. The reasons are twofold why the blocking of portal blood flow, which accounts for two thirds of the total hepatic supply, results in few clinical manifestations. The first is because of the compensatory mechanism of vasodilation of the hepatic arterial system occurs in response to a decrease in portal vein flow [10]. Thesecondisaprocesstermedcavernous transformation,for which is the rapid development of tortuous collateral veins bypassing the thombosed or occluded portion of the portal vein that will usually become apparent within a matter of days [10]. Herein lies the manifestation most devastating to patients with portal venous obstruction. When symptoms do occur, they can present in a variety of ways [8, 10 12]. The most frequent manifestation resulting in patient s seeking medical attention is hematemesis or melena from the development of varices in the esophagus, stomach, small intestine, and colon, which can result in severe gastrointestinal bleeding and ultimately death [8, 11]. Janssen et al. retrospectively evaluated 172 patients (27% of patients had hepatobiliary or gastrointestinal malignancies) with extrahepatic portal vein thrombosis and found that an episode of bleeding from ruptured esophagogastric varices was the initial manifestation in 52 (30%) patients [12]. Furthermore, of the 130 patients tested, 104 patients demonstrated esophageal varices and 4 percent of those patients died from their variceal hemorrhage [12]. As exemplified by our patient, these cases can be a diagnostic and treatment dilemma, with treatment options being few due to rapid tumor growth and related diseases resulting in a very poor prognosis. Historically, treatments for such conditions have been radiation therapy or chemotherapy; however, resolution of the signs and symptoms may have a delayed period of effect up to 3 weeks [13]. These patients are typically not good surgical candidates due to their poor clinical status and therefore are in need of less invasive methods for palliating their symptoms. Endoscopic variceal sclerotherapy has been effective in treating varices of the esophagus and stomach but are ineffective for bleeding further down the gastrointestinal tract. By applying the same physiology of esophagogastric varices to the small bowel, some of these patients can be treated medically with octreotide, propanolol, and other forms of therapy such as chemoradiotherapy [14]. Even with these conservative therapies patients still require multiple hospitalizations from associated symptoms and suffer from prolonged episodes of bleeding, with always the risk of sudden death. As physicians treating cancer we should always seek ways in which to palliate our patients with as little disability as possible, and
4 4 HPB Surgery as shown with our patient percutaneous placed endovascular stents has permitted our ability to effectively treat these patients with this type of condition. We report here the successful SV at the PV confluence stenting of a patient with active variceal bleeding due to recurrent pancreatic cancer. A MEDLINE review of literature yields a total of 64 reported cases of portal vein stent placement, the first of which was by Harville et al. in 1991 [15]. They were able to establish portal vein patency and relief of massive lower GI hemorrhage from colonic varices in a patient with portal hypertension caused by extrahepatic obstruction from chronic pancreatitis. Mathias et al. demonstrated successful use of this technique in a patientwithportalvenousstenosisduetoencasementby pancreatic cancer resulting in portal venous hypertension and variceal bleeding [16]. Portal hypertension was relieved with no recurrent variceal bleeding during the 5 months before the patient died [16]. Watanabe et al. have shown in two patients with malignant portal stenosis that metallic stent implantation can reduce portal pressures dramatically resulting in normalization of liver function tests and reduction of ascites [13]. The largest series reported in literature is by Yamakodo et al. where they were able to place stents into the portal venous system via a percutaneous transhepatic route across 28 stenotic and 12 obstructive lesions [3]. They reported a mean followup period of 11.9 months (range, 2 61 months), during which 60% percent of the stents remained patent [3]. Stent occlusion was found in 40% of the patients, with a mean period until stent occlusion of 3.7 months (range, months) clearly showing an effectivemethod oftreatment in patients with short life expectancies [3]. Extrahepatic portal venous obstruction can be a major cause of portal hypertension and morbidity to these patients. It seems that in a selected patient population portal venous stents can be used affectively to palliate the symptoms caused by portal hypertension due to these types of conditions. Future studies, like the one by Yamakodo et al. showing that portal venous stent patency is prolonged when there is not substantial splanchnic vein involvement, are needed to further clarify and classify which group of patients with malignant portal venous involvement would benefit from such therapy [11]. At this time, it seems appropriate to consider stent placement when surgery is contraindicated, life expectancy is short, or other conservative methods of treatment have been exhausted. Portal venous stent placement provides rapid decompression of varices and palliation of symptoms with little morbidity to the patient helping to improve their quality of life and prognosis. We feel that it is important for physicians to be aware of the tools available for palliation and add them to their armitarium for the care of patients with such complex problems and devastating diseases. The presence of recurrence occurring at the superior mesenteric/portal venous confluence raises the question of initial portal vein resection. Although the indication and contraindication for portal vein resection has not universally defined, there are many reports addressing its benefit [6, 17 19]. The MD Anderson groups, who are known advocates of portal vein resection, have recently reported that this patient population have a higher likelihood of an R1 resection [20]. 4. Conclusion The treatment for patients with malignant superior mesenteric/portal vein obstruction and associated bleeding esophageal and gastric varies can prove to be difficult, but as we have shown endovascular stenting of the portal system is an effective treatment option. References [1] A. Jemal, R. Siegel, E. Ward, et al., Cancer statistics, 2008, CA: Cancer Journal for Clinicians, vol. 58, no. 2, pp , [2]C.J.Yeo,J.L.Cameron,K.D.Lillemoe,etal., Pancreaticoduodenectomy for cancer of the head of the pancreas: 201 patients, Annals of Surgery, vol. 221, no. 6, pp , [3] K. Yamakado, A. Nakatsuka, N. Tanaka, A. Fujii, N. Terada, and K. Takeda, Malignant portal venous obstructions treated by stent placement: significant factors affecting patency, Vascular and Interventional Radiology, vol. 12, no. 12, pp , [4] C. Sperti, C. Pasquali, A. Piccoli, and S. Pedrazzoli, Recurrence after resection for ductal adenocarcinoma of the pancreas, World Surgery, vol. 21, no. 2, pp , [5]D.K.Chang,A.L.Johns,N.D.Merrett,etal., Margin clearance and outcome in resected pancreatic cancer, Journal of Clinical Oncology, vol. 27, no. 17, pp , [6] A. Nakao, T. Fujii, H. Sugimoto, et al., Oncological problems in pancreatic cancer surgery, World Gastroenterology, vol. 12, no. 28, pp , [7] D.-C. Valla, B. Condat, and D. Lebrec, Spectrum of portal vein thrombosis in the West, Gastroenterology and Hepatology, vol. 17, supplement 3, pp. S224 S227, [8] J. Cohen, R. R. Edelman, and S. Chopra, Portal vein thrombosis: a review, American Medicine, vol. 92, no. 2, pp , [9] R. L. Vogelzang, S. G. Reddy, M. A. Braun, and A. A. Nemcek, Extrahepatic portal venous stenosis: treatment with percutaneous transhepatic stent placement, Vascular and Interventional Radiology, vol. 7, no. 2, pp , [10] A. Sobhonslidsuk and K. R. Reddy, Portal vein thrombosis: a concise review, American Gastroenterology, vol. 97, no. 3, pp , [11] K. Yamakado, A. Nakatsuka, N. Tanaka, et al., Portal venous stent placement in patients with pancreatic and biliary neoplasms invading portal veins and causing portal hypertension: initial experience, Radiology, vol. 220, no. 1, pp , [12] H. L. A. Janssen, A. Wijnhoud, E. B. Haagsma, et al., Extrahepatic portal vein thrombosis: aetiology and determinants of survival, Gut, vol. 49, no. 5, pp , [13] Y. Watanabe, M. Sato, Y. Abe, and S. Ueda, Metallic stents for low invasive recanalization of the portal veins with cancerous invasion first case report, Hepato-Gastroenterology, vol. 45, no. 20, pp , 1998.
5 HPB Surgery 5 [14] S. A. Shah, C. M. Mery, and M. J. Zinner, Small bowel varices from neuroendocrine tumor of the pancreas, Journal of Gastrointestinal Surgery, vol. 9, no. 7, pp , [15] L. E. Harville, F. J. Rivera, J. C. Palmaz, and B. A. Levine, Variceal hemorrhage associated with portal vein thrombosis: treatment with a unique portal venous stent, Surgery, vol. 111, no. 5, pp , [16] K. Mathias, U. Bolder, D. Lohlein, and H. Jager, Percutaneous transhepatic angioplasty and stent implantation for prehepatic portal vein obstruction, CardioVascular and Interventional Radiology, vol. 16, no. 5, pp , [17] L. E. Harrison, D. S. Klimstra, and M. F. Brennan, Isolated portal vein involvement in pancreatic adenocarcinoma: a contraindication for resection? Annals of Surgery, vol. 224, no. 3, pp , [18] S. D. Leach, J. E. Lee, C. Charnsangavej, et al., Survival following pancreaticoduodenectomy with resection of the superior mesenteric-portal vein confluence for adenocarcinoma of the pancreatic head, British Surgery, vol.85,no.5,pp , [19]T.J.Howard,N.Villanustre,S.A.Moore,et al., Efficacy of venous reconstruction in patients with adenocarcinoma of the pancreatic head, Gastrointestinal Surgery, vol. 7, no. 8, pp , [20] C.P.Raut,J.F.Tseng,C.C.Sun,etal., Impactofresection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinoma, Annals of Surgery, vol. 246, no. 1, pp , 2007.
















6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Portal vein stent placement for the treatment of postoperative portal vein stenosis: long-term success and factor associated with stent failure
 Kato et al. BMC Surgery (2017) 17:11 DOI 10.1186/s12893-017-0209-y RESEARCH ARTICLE Portal vein stent placement for the treatment of postoperative portal vein stenosis: long-term success and factor associated
Kato et al. BMC Surgery (2017) 17:11 DOI 10.1186/s12893-017-0209-y RESEARCH ARTICLE Portal vein stent placement for the treatment of postoperative portal vein stenosis: long-term success and factor associated
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Percutaneous Transhepatic Stent Placement in the Management of Portal Venous Stenosis After Curative Surgery for Pancreatic and Biliary Neoplasms
 Vascular and Interventional Radiology Original Research Kim et al. Transhepatic Stent Placement for Postsurgical Stenosis Vascular and Interventional Radiology Original Research Kyung Rae Kim 1 Gi-Young
Vascular and Interventional Radiology Original Research Kim et al. Transhepatic Stent Placement for Postsurgical Stenosis Vascular and Interventional Radiology Original Research Kyung Rae Kim 1 Gi-Young
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
 Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience
 Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary Mucinous Neoplasm
 Case Reports in Surgery Volume 2015, Article ID 816960, 4 pages http://dx.doi.org/10.1155/2015/816960 Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary
Case Reports in Surgery Volume 2015, Article ID 816960, 4 pages http://dx.doi.org/10.1155/2015/816960 Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما
 بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Imaging techniques in the diagnosis, staging and follow up of GI cancers. Moderators: Banke Agarwal, MD and Paul Schultz, MD
 Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Case Report Inferior Vena Cava Torsion and Stenosis Complicated by Compressive Pericaval Regional Ascites following Orthotopic Liver Transplantation
 Case Reports in Radiology Volume 2013, Article ID 576092, 4 pages http://dx.doi.org/10.1155/2013/576092 Case Report Inferior Vena Cava Torsion and Stenosis Complicated by Compressive Pericaval Regional
Case Reports in Radiology Volume 2013, Article ID 576092, 4 pages http://dx.doi.org/10.1155/2013/576092 Case Report Inferior Vena Cava Torsion and Stenosis Complicated by Compressive Pericaval Regional
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Case Report Computed Tomography Angiography Successfully Used to Diagnose Postoperative Systemic-Pulmonary Artery Shunt Narrowing
 Case Reports in Cardiology Volume 2011, Article ID 802643, 4 pages doi:10.1155/2011/802643 Case Report Computed Tomography Angiography Successfully Used to Diagnose Postoperative Systemic-Pulmonary Artery
Case Reports in Cardiology Volume 2011, Article ID 802643, 4 pages doi:10.1155/2011/802643 Case Report Computed Tomography Angiography Successfully Used to Diagnose Postoperative Systemic-Pulmonary Artery
Endoscopic Management of Biliary Strictures. Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center
 Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
WallFlex Stents Technique Spotlights
 WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper Intestinal Obstruction
 Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Frank Burton Memorial Update on Pancreato-biliary Cancers
 Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder in an Elderly Patient
 Case Reports in Surgery Volume 2015, Article ID 767196, 4 pages http://dx.doi.org/10.1155/2015/767196 Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder
Case Reports in Surgery Volume 2015, Article ID 767196, 4 pages http://dx.doi.org/10.1155/2015/767196 Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Case Report Coronary Artery Perforation and Regrowth of a Side Branch Occluded by a Polytetrafluoroethylene-Covered Stent Implantation
 International Scholarly Research Network Volume 2011, Article ID 212851, 4 pages doi:10.5402/2011/212851 Case Report Coronary Artery Perforation and Regrowth of a Side Branch Occluded by a Polytetrafluoroethylene-Covered
International Scholarly Research Network Volume 2011, Article ID 212851, 4 pages doi:10.5402/2011/212851 Case Report Coronary Artery Perforation and Regrowth of a Side Branch Occluded by a Polytetrafluoroethylene-Covered
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Intraoperative staging of GIT cancer using Intraoperative Ultrasound
 Intraoperative staging of GIT cancer using Intraoperative Ultrasound Thesis For Fulfillment of MSc Degree In Surgical Oncology By Abdelhalim Salah Abdelhalim Moursi M.B.B.Ch (Cairo University ) Supervisors
Intraoperative staging of GIT cancer using Intraoperative Ultrasound Thesis For Fulfillment of MSc Degree In Surgical Oncology By Abdelhalim Salah Abdelhalim Moursi M.B.B.Ch (Cairo University ) Supervisors
Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule
 Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma
 Case Reports in Otolaryngology Volume 2013, Article ID 384238, 4 pages http://dx.doi.org/10.1155/2013/384238 Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma Kunihiko Tokashiki, Kiyoaki
Case Reports in Otolaryngology Volume 2013, Article ID 384238, 4 pages http://dx.doi.org/10.1155/2013/384238 Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma Kunihiko Tokashiki, Kiyoaki
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
SECONDARIES: A PRELIMINARY REPORT
 HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
Slide 1. Slide 2. Slide 3 Pancreatic Cancer- Case #1. Endoscopic management of GI malignancy. Endoscopic approaches in GI malignancy- Agenda
 Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
CHOLANGIOCARCINOMA (CCA)
") CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
Стенты «Ella-cs» Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts»
 Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts» A. Esophageal Stenting and related topics 1 AMJG 2009; 104:1329 1330 Letters to Editor Early Tracheal Stenosis Post Esophageal Stent
Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts» A. Esophageal Stenting and related topics 1 AMJG 2009; 104:1329 1330 Letters to Editor Early Tracheal Stenosis Post Esophageal Stent
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Gastroenterology Fellowship Program
 Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy: A Report of Two Cases
 Case Reports in Surgery Volume 2013, Article ID 238675, 4 pages http://dx.doi.org/10.1155/2013/238675 Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy:
Case Reports in Surgery Volume 2013, Article ID 238675, 4 pages http://dx.doi.org/10.1155/2013/238675 Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy:
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Guidelines for the management of patients with pancreatic cancer periampullary and ampullary carcinomas
 v1 GUIDELINES Guidelines for the management of patients with pancreatic cancer periampullary and ampullary carcinomas Pancreatic Section of the British Society of Gastroenterology, Pancreatic Society of
v1 GUIDELINES Guidelines for the management of patients with pancreatic cancer periampullary and ampullary carcinomas Pancreatic Section of the British Society of Gastroenterology, Pancreatic Society of
Case 37 Clinical Presentation
 Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE. T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar
 ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar LEARNING OBJECTIVES q Through a series of cases illustrate the updated Atlanta symposium
ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar LEARNING OBJECTIVES q Through a series of cases illustrate the updated Atlanta symposium
Appendix 9: Endoscopic Ultrasound in Gastroenterology
 Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography (EUS) in gastroenterology. It includes standards for theoretical
Appendix 9: Endoscopic Ultrasound in Gastroenterology This curriculum is intended for clinicians who perform endoscopic ultrasonography (EUS) in gastroenterology. It includes standards for theoretical
Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel
 Case Reports in Vascular Medicine Volume 2015, Article ID 725168, 4 pages http://dx.doi.org/10.1155/2015/725168 Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel Alexander
Case Reports in Vascular Medicine Volume 2015, Article ID 725168, 4 pages http://dx.doi.org/10.1155/2015/725168 Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel Alexander
Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy
 Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Research Article The Utility of Repeat Endoscopic Ultrasound-Guided Fine Needle Aspiration for Suspected Pancreatic Cancer
 Gastroenterology Research and Practice Volume 2010, Article ID 268290, 4 pages doi:10.1155/2010/268290 Research Article The Utility of Repeat Endoscopic Ultrasound-Guided Fine Needle Aspiration for Suspected
Gastroenterology Research and Practice Volume 2010, Article ID 268290, 4 pages doi:10.1155/2010/268290 Research Article The Utility of Repeat Endoscopic Ultrasound-Guided Fine Needle Aspiration for Suspected
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
General Surgery PURPLE SERVICE MUHC-RVH Site
 Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Gastric Signet-Ring Cell Carcinoma: Unilateral Lower Extremity Lymphoedema as the Presenting Feature
 Clinical Image TheScientificWorldJOURNAL (2007) 7, 1189 1192 ISSN 1537-744X; DOI 10.1100/tsw.2007.199 Gastric Signet-Ring Cell Carcinoma: Unilateral Lower Extremity Lymphoedema as the Presenting Feature
Clinical Image TheScientificWorldJOURNAL (2007) 7, 1189 1192 ISSN 1537-744X; DOI 10.1100/tsw.2007.199 Gastric Signet-Ring Cell Carcinoma: Unilateral Lower Extremity Lymphoedema as the Presenting Feature
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Tom Eisele, Benedikt M. Muenz, and Grigorios Korosoglou. Department of Cardiology & Vascular Medicine, GRN Hospital Weinheim, Weinheim, Germany
 Case Reports in Vascular Medicine Volume 2016, Article ID 7376457, 4 pages http://dx.doi.org/10.1155/2016/7376457 Case Report Successful Endovascular Repair of an Iatrogenic Perforation of the Superficial
Case Reports in Vascular Medicine Volume 2016, Article ID 7376457, 4 pages http://dx.doi.org/10.1155/2016/7376457 Case Report Successful Endovascular Repair of an Iatrogenic Perforation of the Superficial
Tata Memorial Centre s opinion is summarized as follows: 1. Given the type 1 stricture (as mentioned in the structured summary), assessment
, assessment") March 5 th 2016 Dear Ms. Malti Sinha, Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online
March 5 th 2016 Dear Ms. Malti Sinha, Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Pancreatic Cancer. What is pancreatic cancer?
 Scan for mobile link. Pancreatic Cancer Pancreatic cancer is a tumor of the pancreas, an organ that is located behind the stomach in the abdomen. Pancreatic cancer does not always cause symptoms until
Scan for mobile link. Pancreatic Cancer Pancreatic cancer is a tumor of the pancreas, an organ that is located behind the stomach in the abdomen. Pancreatic cancer does not always cause symptoms until
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Case Report Reresection of Colorectal Liver Metastasis with Vena Cava Resection
 Case Reports in Surgery Volume 2016, Article ID 8173048, 4 pages http://dx.doi.org/10.1155/2016/8173048 Case Report Reresection of Colorectal Liver Metastasis with Vena Cava Resection Ali Tardu, Cuneyt
Case Reports in Surgery Volume 2016, Article ID 8173048, 4 pages http://dx.doi.org/10.1155/2016/8173048 Case Report Reresection of Colorectal Liver Metastasis with Vena Cava Resection Ali Tardu, Cuneyt
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
SURGERY? COMMON BILE DUCT STONES ERCP OR. Room 759. Maryland
 HPB INTERNATIONAL 277 alter the natural history of the disease, and delay or prevent the development or cirrhosis. Data from our unit as well as others suggests that to be the case. The current series,
HPB INTERNATIONAL 277 alter the natural history of the disease, and delay or prevent the development or cirrhosis. Data from our unit as well as others suggests that to be the case. The current series,
Case Report A Rare Case of Complete Stent Fracture, Coronary Arterial Transection, and Pseudoaneurysm Formation Induced by Repeated Stenting
 Case Reports in Cardiology Volume 2015, Article ID 192853, 4 pages http://dx.doi.org/10.1155/2015/192853 Case Report A Rare Case of Complete Stent Fracture, Coronary Arterial Transection, and Pseudoaneurysm
Case Reports in Cardiology Volume 2015, Article ID 192853, 4 pages http://dx.doi.org/10.1155/2015/192853 Case Report A Rare Case of Complete Stent Fracture, Coronary Arterial Transection, and Pseudoaneurysm
Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm
 Case Reports in Vascular Medicine, Article ID 716752, 4 pages http://dx.doi.org/10.1155/2014/716752 Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm Ahsan Syed Khalid,
Case Reports in Vascular Medicine, Article ID 716752, 4 pages http://dx.doi.org/10.1155/2014/716752 Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm Ahsan Syed Khalid,
Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus Irinotecan and Radiotherapy
 Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Peter I. Kalmar, 1 Peter Oberwalder, 2 Peter Schedlbauer, 1 Jürgen Steiner, 1 and Rupert H. Portugaller Introduction. 2.
 Case Reports in Medicine Volume 2013, Article ID 714914, 4 pages http://dx.doi.org/10.1155/2013/714914 Case Report Secondary Aortic Dissection after Endoluminal Treatment of an Intramural Hematoma of the
Case Reports in Medicine Volume 2013, Article ID 714914, 4 pages http://dx.doi.org/10.1155/2013/714914 Case Report Secondary Aortic Dissection after Endoluminal Treatment of an Intramural Hematoma of the
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Case Report Features of the Atrophic Corpus Mucosa in Three Cases of Autoimmune Gastritis Revealed by Magnifying Endoscopy
 Volume 2012, Article ID 368160, 4 pages doi:10.1155/2012/368160 Case Report Features of the Atrophic Corpus Mucosa in Three Cases of Autoimmune Gastritis Revealed by Magnifying Endoscopy Kazuyoshi Yagi,
Volume 2012, Article ID 368160, 4 pages doi:10.1155/2012/368160 Case Report Features of the Atrophic Corpus Mucosa in Three Cases of Autoimmune Gastritis Revealed by Magnifying Endoscopy Kazuyoshi Yagi,
ACUTE CHOLANGITIS AS a result of an occluded
 Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas
 CASE REPORT Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas Anand Patel, Louis Lambiase, Antonio Decarli, Ali Fazel Division of Gastroenterology
CASE REPORT Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas Anand Patel, Louis Lambiase, Antonio Decarli, Ali Fazel Division of Gastroenterology
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
 ISRN Cardiology, Article ID 825461, 4 pages http://dx.doi.org/10.1155/2014/825461 Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
ISRN Cardiology, Article ID 825461, 4 pages http://dx.doi.org/10.1155/2014/825461 Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report
 Case Reports in Urology Volume 2012, Article ID 728531, 4 pages doi:10.1155/2012/728531 Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report D. P. Ramaema,
Case Reports in Urology Volume 2012, Article ID 728531, 4 pages doi:10.1155/2012/728531 Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report D. P. Ramaema,
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
During the course of the 12 month fellowship, candidates will attend at least one international liver meeting (generally AASLD).
.") Hepatology and Liver Transplantation fellowship Length: 1 year Number of positions: 2 Type of fellowship: Clinical and Research Fellowship Director: Dr. Deschenes McGill University Health Centre Fellowship
Hepatology and Liver Transplantation fellowship Length: 1 year Number of positions: 2 Type of fellowship: Clinical and Research Fellowship Director: Dr. Deschenes McGill University Health Centre Fellowship
Case Report An Uncommon Cause of a Small-Bowel Obstruction
 Hindawi Case Reports in Gastrointestinal Medicine Volume 2017, Article ID 1628215, 4 pages https://doi.org/10.1155/2017/1628215 Case Report An Uncommon Cause of a Small-Bowel Obstruction Ali Zakaria, Bayan
Hindawi Case Reports in Gastrointestinal Medicine Volume 2017, Article ID 1628215, 4 pages https://doi.org/10.1155/2017/1628215 Case Report An Uncommon Cause of a Small-Bowel Obstruction Ali Zakaria, Bayan
Imaging Guided Biopsy. Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer
 Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma of Thyroid
 Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma