University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018
|
|
|
- Dana Phelps
- 5 years ago
- Views:
Transcription
1 University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is to acknowledge that Sadia Ali, M.D. has disclosed that she does not have any financial interests or other relationships with commercial concerns related directly or indirectly to this program. Dr. Ali will not be discussing off label uses in this presentation.
2 Purpose and overview: Immune checkpoint inhibitors have revolutionized cancer care and are now successfully used to treat several types cancers. Their side effect profile is distinct form the traditional chemotherapy regimens, and include immune related adverse events. With their increased use, the frequency of these events is growing and has necessitated the development of a new form of multidisciplinary care. Immune related endocrinopathies can significantly affect patients outcome and require rapid recognition and treatment. The purpose of this talk is to identify and manage the most commonly encountered endocrinopathies associated with immune checkpoint inhibitors. At the conclusion of this lecture, the listener should be able to: 1) Understand the mechanism of action of immune checkpoint inhibitors; 2) Identify common endocrinopathies caused by immune checkpoint inhibitors; 3) Understand how to manage common Endocrinopathies including: hypophysitis, thyroid dysfunction and diabetes mellitus. Sadia Ali MD is an Assistant Professor and Clinical Chief of the Division of Endocrinology, Diabetes and Metabolism at UT Southwestern Medical Center. Her quality improvement work has improved the management of post-transplant glycemic management at Clements University Hospital and diabetes care quality metrics at the UTSW Internal Medicine Subspecialty Clinic for Endocrinology. She is interested in high value, patient centric, clinical care and enhancing the clinic infrastructure for the outpatient Endocrinology practice.
3 What are immune checkpoint inhibitors? Figure 1: Mechanism of Action of immune checkpoint inhibitors. Immune checkpoint blockade increases antitumor immunity by blocking intrinsic downregulators of immunity, such as cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed cell death 1 (PD-1) or its ligand, programmed cell death ligand 1 (PD-L1). Several immune checkpoint directed antibodies have increased overall survival for patients with various cancers and are approved by the Food and Drug Administration. CTLA-4 is expressed on the surface of most activated T lymphocytes during initial activation phase in lymphatic tissue by dendritic cells and other APCs. Its main action is inhibitory, regulating homeostasis and peripheral immune tolerance, by inhibiting activation of T lymphocytes though negative signaling. PD-1 is another co-inhibitory membrane receptor expressed on T-cells activated during the effector phase in peripheral tissues. The binding of PD-1 to PD-L1 and PD-L2 ligands that are expressed in tumor cells and tissue macrophages causes an inhibition of T-lymphocyte facilitating immune tolerance, thus preventing tumor rejection by the immune system.

4 Immune check point inhibitors are monoclonal antibodies that block these immune checkpoint proteins CTLA-4, PD -1 and PD-L1 leading to stimulation and proliferation of activated T-lymphocytes against tumor cells. The first immune checkpoint inhibitor approved by the FDA in 2011 was the CTLA-4 inhibitor, ipilumumab. Since then six checkpoint inhibitors have been approved for clinical practice across multiple tumor types. Figure 2: Immune checkpoint blocking antibodies approved by the FDA

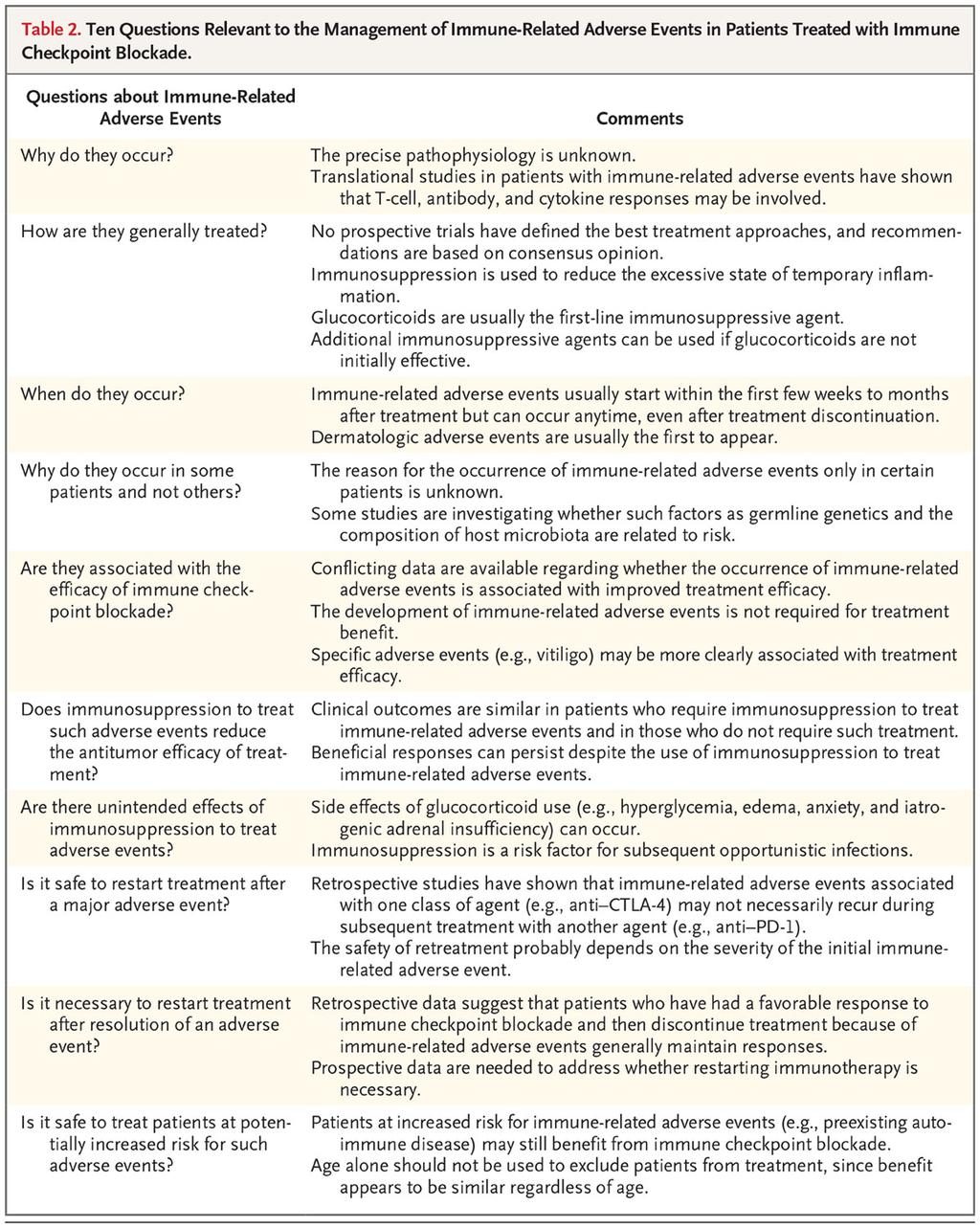
5 Immune related adverse events Figure 3: Immune related adverse events By increasing the activity of the immune system, immune checkpoint blockade can have inflammatory side effects, which are often termed immune-related adverse events. Although any organ system can be affected, immune-related adverse events most commonly involve the gastrointestinal tract, endocrine glands, skin, and liver. Less often, the central nervous system and cardiovascular, pulmonary, musculoskeletal, and hematologic systems are involved. Immune-related adverse events usually develop within the first few weeks to months after treatment initiation. However, these can present at any time, including after cessation of immune checkpoint blockade therapy, and may wax and wane over time.

6 Figure 4: Proposed mechanism of immune related adverse events. Patients treated with anti CTLA-4 therapy have immune related adverse events that differ from those in patients treated with anti PD-1, and the effects of anti CTLA-4 are generally more severe. For example, colitis and hypophysitis seem to be more common with anti CTLA-4 therapy, whereas pneumonitis and thyroiditis appear to be more common with anti PD-1 therapy. Although we do not know why organ-specific toxic effects differ between these two targets, reports of hypophysitis have identified the expression of CTLA-4 on normal pituitary cells, which may contribute to the toxicity of anti CTLA-4 therapy. Also, thyroid disorders can occur in patients receiving anti PD-1 therapy who have anti-thyroid antibodies. Another possibility is that PD-1 may be involved in maintaining self-tolerance, the process that keeps the immune system from attacking the person it was designed to protect. In addition, cytokines may be involved in the pathophysiology of immunerelated adverse events. One study identified elevated levels of interleukin-17 in patients with ipilimumab-induced colitis.
7 Generally speaking, immune-related adverse events result from excessive immunity against normal organs. A majority of immune-related adverse events are effectively treated by: 1) delaying or stopping the checkpoint inhibitor and/or 2) inducing temporary immunosuppression with agents such as oral glucocorticoids or additional immunosuppressants in more severe cases. Multidisciplinary collaboration can often be helpful in treating patients with immunerelated adverse events. Endocrine specific adverse events: Endocrine immune related adverse events include hypophysitis, primary or secondary thyroid disease, primary adrenal insufficiency, diabetes mellitus type 1 and rarely hypoparathyroidism. Hypophysitis: Incidence and Prevalence:
8 Pathogenesis: Although the precise mechanism for hypophysitis is not completely understood it is thought to be related to development of a process of immunological activation at the level of the pituitary gland. 1) Pituitary auto antibodies: Expression of CTLA-4 protein has been found on pituitary cells. Binding to CTLA-4 antibodies or Ipilimumab IgG is thought to lead to activation of classical complement pathway which then destroys pituitary cells. 2) Direct activation of T-cells results destruction of pituitary cells and inflammation and production of cytokines in response to cognate antigen. Clinical presentation: Hypophysitis generally appears between 6-10 weeks after starting treatment. The clinical manifestations of hypophysitis are related to 1) Structural changes associated with the enlargement of pituitary 2) Hormonal disturbances that occur as a result of pituitary inflammation. Clinical manifestations can be nonspecific and be related to the underlying malignancy or non-endocrine related adverse events. These include: - Headache - Hypotension - Hypoglycemia - Nausea - Weakness - Anorexia - Diarrhea. Lab abnormalities can include - Hyponatremia - Low AM cortisol, ACTH - Low free T4, TSH - Low prolactin, testosterone in men, and estrogen in premenopausal age group for women. Imaging: MRI of the pituitary gland may show mild to moderate diffuse pituitary enlargement. Chiasmatic compression was not seen in most studies. A normal pituitary gland on MRI does not rule out hypophysitis and management should be based on clinical presentation and evaluation of pituitary hormone levels.
9 Treatment: Severe Hypophysitis: headache and Na < 125 mg/dl 1) High Dose Steroids - Dexamethasone 4mg Q6hr or methylprednisolone/prednisone 1-2 mg/kg/day) 2) Fluid Resuscitation: - D5 or Normal Saline (hypoglycemia, hyponatremia, hypotension) - AVOID hypotonic fluids, e.g. D5W, D5 0.5% NaCl 3) Correct metabolic abnormalities: severe hyperkalemia - IV bicarb, rectal polystyrene resin, IV glucose and insulin Mild and Moderate Hypophysitis Hormone replacement therapy is the mainstay of treatment. 1) Secondary adrenal insufficiency: hydrocortisone can be started on replacement dose mg per daily divided into 2 doses through the day. Patients are educated about sick day rules to double dose of steroids. 2) Thyroid axis: start levothyroxine to be titrated based on FT4 lab values. 3) Gonadal axis: Testosterone replacement can be considered as outpatient for male patients for hypogonadism. 4) Growth hormone therapy is not instituted as it is not indicated due to underlying malignancy. Some authors have found an association between Ipilimumab induced hypophysitis and a better tumor response in patients with metastatic melanoma. Hypophysitis was accompanied by a greater survival 21.4 versus 9.7 months in these patients compared to those who did not develop it. Because steroid use and management of hypophysitis has also not shown to negatively influence the therapeutic benefit of immune checkpoint inhibitors.
10 Thyroid Dysfunction: Thyroid dysfunction includes thyroiditis with transient thyrotoxicosis, hypothyroidism which could be transient or long standing and subclinical disease (both hypo and hyperthyroidism) in an isolated or sequential way in the same patient over time. Rare cases of hyperthyroidism associated with Graves disease have been reported. Incidence: Time of onset: Median time of onset is 2 months but can be delayed up to 2-3 years after treatment initiation. Pathogenesis: Thyroid problems appear to occur as a result of immunological activation at the thyroid level which manifests as autoimmune /destructive thyroiditis induced by immunological and inflammatory mechanisms. A large majority of these patients were positive for anti-thyroglobulin and anti-thyroid peroxidase antibodies.
11 Clinical presentation: Clinical picture of thyrotoxicosis is usually mild and transient. TSH levels are low and free T4 is elevated. Patients may present with fatigue, anxiety, diarrhea and palpitations. Majority of patients after transient thyrotoxicosis develop hypothyroidism. Asthenia and fatigue are the main reported symptoms. Labs are consistent with low free T4 and elevated TSH for primary hypothyroidism and low free T4 and normal to low TSH in secondary hypothyroidism (from hypophysitis). Management: Thyroiditis with transient thyrotoxicosis can be managed symptomatically with beta blockers. Corticosteroids are sometimes used if being used for other iraes. Given the pathogenesis treatment with anti-thyroid drugs usually does not help unless thyroid stimulating immunoglobulins are positive. For symptomatic subclinical hypothyroidism and frank hypothyroidism with TSH > 8-10 and low free T4 hormone replacement therapy with levothyroxine is instituted and titrated based on labs for TSH and free T4. It is important not to rely on TSH for secondary hypothyroidism caused by hypophysitis. Autoimmune Diabetes: Immunotherapy has also been associated with autoimmune diabetes mellitus. This side effect is uncommon and has been reported with anti- PD-1 use and combined therapy but not with CTLA-4 alone. The incidence is < 1%. It may appear after a treatment period ranging from 1 week to upto 4 years. Patients present with hyperglycemia and occasionally with diabetic ketoacidosis. Hormone replacement therapy with basal and bolus insulin is instituted. Proposed pathogenic mechanism is infiltration of pancreatic islets with activated of T lymphocytes accompanied by production of anti- GAD and anti IA2 antibodies. Primary Adrenal Insufficiency/ Adrenalitis: Primary adrenal insufficiency is uncommon. Incidence varies from 0.3 to 1.5%. Before establishing its diagnosis, it is important to rule out metastatic infiltration of both adrenal glands as the cause for primary adrenal insufficiency. A bilateral reversible enlargement of the adrenal glands has been reported. It can present clinically with fatigue, diarrhea, chronic hyponatremia and hypotension. Laboratory findings are consistent with low cortisol, low DHEA-S, high ACTH.
12 Hormone replacement therapy is instituted with corticosteroids and mineralocorticoids which controls symptoms, restores metabolic abnormalities and allows continued immunotherapy treatment. Dose for corticosteroids (hydrocortisone mg/day divided in two doses) is usually sufficient. Principal of Immunotherapy re-challenge: NCCN guidelines Hypophysitis: Manifested by deficiency of TSH/ACTH and/or gonad-stimulating hormones, but without symptomatic pituitary swelling: immunotherapy may continue while replacement endocrine therapy is regulated. Hypophysitis accompanied by symptoms of pituitary swelling (eg headache, vision disturbance, and /or neurologic dysfunction): hold immunotherapy until resolution of symptoms after steroid therapy; consider resumption of immunotherapy after symptoms are controlled on steroid dose less than 10mg/day. Thyroid: No discontinuation required for hypothyroidism. For symptomatic hyperthyroidism resembling graves-like disease, consider holding immunotherapy and resuming after work up is complete and there is evidence of improvement in symptoms and TFTs. Primary Adrenal Insufficiency: After appropriate replacement endocrine therapy is instituted, immunotherapy may continue. DM Type 1 with DKA: Consider resuming once DKA has been corrected and glucose levels have been stabilized.
13
14 References: Iglesias P et al, Cancer immunotherapy-induced endocrinopathies: clinical behavior and therapeutic approach. Eur J of Int Med 47 (2018) Postow M et al, Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med 2018: 378: Cuckier P et al, Endocrine side effects of cancer immunotherapy. (2017) 24, T331-T347 Torino F et al, Endocrinological side effects of immune check point inhibitors. Curr Opin Oncol 2016:4: Joshi MN et al, Immune-checkpoint inhibitor related hypophysitis and endocrine dysfunction: clinical review. Clin Endocrinol 2016:3: Byun DJ et al, Cancer immunotherapy-immune checkpoint blockade and associated endocrinopathies. Nat Rev Endocrinol 2017; 13: Abdel-Rahman O et al, Risk of endocrine complications in cancer patients treated with immune check point inhibitors: a meta-analysis. Future Oncol 2016: 3: Ott PA et al, CTLA- and PD-1/PD-L1 blockade: new immunotherapeutic modalities with durable clinical benefit in melanoma patients. Clin Cancer Res 2013: 19: Ma W et al, Current status and perspectives in translation biomarker research for PD- 1/PD-L1 immune checkpoint blockade therapy. J Hematol Oncol 2016:27(9):47. Peterson JJ et al, Update on new therapies with immune checkpoint inhibitors. Clin J Oncol Nurs 2016:4: Min L et al, Ipilimumab induced autoimmune adrenalitis. Lancet Diabetes Endocrinol 2013;1: e15. Trainer H et al, Hyponatremia secondary to nivolumab-induced primary adrenal failure. Endocrinol Diabetes Metab Case Rep 2016: 16(0108). Faje A et al, Immunotherapy and hypophysitis: Clinical presentation, treatment, and biologic insights. Pituitary 2016; 1: Faje AT et al, Iplimumab induced hypophysitis: A detailed longitudinal analysis and a large cohort of patients with metastatic melanoma. J Clin Endocinol Metab 2014; 11: Sznol M et al, Endocrine-related adverse events associated with immune checkpoint blockade and expert insights on their management. Cancer Treatment Reviews 58 (2017)
15 Ito A et al, Clinical development of immune check point inhibitors. Biomed Res Int 2015; Morganstein DL et al, Thyroid abnormalities following the use of cytotoxic T-lymphocyte antigen-4and programmed death receptorprotein-1inhibitorsin the treatment of melanoma. Clin Endocrinol 2017;4: Thompson JA. New NCCN Guidelines: Recognition and Management of Immunotherapy-Related Toxicity. J Natl Compr Canc Netw May;16(5S):
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY
 ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
Adverse effects of Immunotherapy. Asha Nayak M.D
 Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy: Toxicity Management. Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital
 Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Case report: AVELUMAB INDUCING HYPOTHYROIDISM AND HYPOADRENALISM: A CASE REPORT AND REVIEW OF LITERATURE
 Case report: AVELUMAB INDUCING HYPOTHYROIDISM AND HYPOADRENALISM: A CASE REPORT AND REVIEW OF LITERATURE Kashif Aziz*, Amir Shahbaz, Muhammad Umair, Isaac Sachmechi Department of Medicine, Icahn School
Case report: AVELUMAB INDUCING HYPOTHYROIDISM AND HYPOADRENALISM: A CASE REPORT AND REVIEW OF LITERATURE Kashif Aziz*, Amir Shahbaz, Muhammad Umair, Isaac Sachmechi Department of Medicine, Icahn School
Nursing Perspective on iraes: Patient Education, Monitoring and Management
 Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
Melanoma Immunotherapy. Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management
 Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
CANCER IMMUNOTHERAPY Presented by John A Keech Jr DO MultiCare Regional Cancer Center
 CANCER IMMUNOTHERAPY 2018 Presented by John A Keech Jr DO MultiCare Regional Cancer Center Successful anti-cancer immunity is autoimmunity Green, The Scientist, 2014 Immunotherapy strategies Cancer vaccines
CANCER IMMUNOTHERAPY 2018 Presented by John A Keech Jr DO MultiCare Regional Cancer Center Successful anti-cancer immunity is autoimmunity Green, The Scientist, 2014 Immunotherapy strategies Cancer vaccines
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS
 OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
PEMBROLIZUMAB (KEYTRUDA ) for the treatment of advanced melanoma or previously treated NSCLC
 for the treatment of advanced melanoma or previously treated NSCLC") DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent Rate Day 1 Pembrolizumab 2mg/kg IV Infusion 100mL 0.9% Sodium Chloride* Or 100mL 5% Glucose* *Final concentration must be between 1 to 10mg/mL Over
DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent Rate Day 1 Pembrolizumab 2mg/kg IV Infusion 100mL 0.9% Sodium Chloride* Or 100mL 5% Glucose* *Final concentration must be between 1 to 10mg/mL Over
1* 2. Maria Jose Velasco Acuna and Kamal Shoukri. Department of Endocrinology, Saint Francis Hospital, Hartford, CT, USA
 CASE REPORT Ipilimumab Causing Autoimmune Hypophysitis : A Case Report 1* 2 Maria Jose Velasco Acuna and Kamal Shoukri 1 Department of Endocrinology and Metabolism, University of Connecticut School of
CASE REPORT Ipilimumab Causing Autoimmune Hypophysitis : A Case Report 1* 2 Maria Jose Velasco Acuna and Kamal Shoukri 1 Department of Endocrinology and Metabolism, University of Connecticut School of
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD
 ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Case Report Treatment of Ipilimumab Induced Graves Disease in a Patient with Metastatic Melanoma
 Case Reports in Endocrinology Volume 2016, Article ID 2087525, 4 pages http://dx.doi.org/10.1155/2016/2087525 Case Report Treatment of Ipilimumab Induced Graves Disease in a Patient with Metastatic Melanoma
Case Reports in Endocrinology Volume 2016, Article ID 2087525, 4 pages http://dx.doi.org/10.1155/2016/2087525 Case Report Treatment of Ipilimumab Induced Graves Disease in a Patient with Metastatic Melanoma
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Provide preventive counseling to parents and patients with specific endocrine conditions about:
 Endocrinology Description: The resident will become familiar with the diagnosis, management, and treatment of endocrine problems. The resident will evaluate patients with a multitude of endocrine problems,
Endocrinology Description: The resident will become familiar with the diagnosis, management, and treatment of endocrine problems. The resident will evaluate patients with a multitude of endocrine problems,
Management of Immune Checkpoint Inhibitor Related Toxicities
 Management of Immune Checkpoint Inhibitor Related Toxicities Katie Wolfram, PharmD Clinical Pharmacist, Oncology Memorial Hospital of South Bend A Webinar for HealthTrust Members November 12, 2018 Disclosures
Management of Immune Checkpoint Inhibitor Related Toxicities Katie Wolfram, PharmD Clinical Pharmacist, Oncology Memorial Hospital of South Bend A Webinar for HealthTrust Members November 12, 2018 Disclosures
TOXICITY RELATED TO IO IN LUNG CANCER
 TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico
TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico
Toxicity of Systemic Melanoma Therapies. Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney
 Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Endocrinology
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Endocrinology 1. GOAL: Understand the role of the pediatrician in preventing endocrine dysfunction, and in counseling and
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Endocrinology 1. GOAL: Understand the role of the pediatrician in preventing endocrine dysfunction, and in counseling and
NECN CHEMOTHERAPY HANDBOOK PROTOCOL
 Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
Atezolizumab Non-small cell lung cancer
 Systemic Anti Cancer Treatment Protocol Atezolizumab Non-small cell lung cancer PROTOCOL REF: MPHAATNSCLC (Version No: 1.0) Approved for use in: Locally advanced/metastatic non squamous or squamous non-small
Systemic Anti Cancer Treatment Protocol Atezolizumab Non-small cell lung cancer PROTOCOL REF: MPHAATNSCLC (Version No: 1.0) Approved for use in: Locally advanced/metastatic non squamous or squamous non-small
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity. Disclosure Statement. Learning Objectives
 Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director
 W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director It is our duty to each learner to honor your right to expect
W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director It is our duty to each learner to honor your right to expect
7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Gastrointestinal Tract
 7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation.
7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation.
Cancer Immunotherapy: Promises and Challenges. Disclosures
 Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities
 Review Article on Lung Cancer Diagnostics and Treatments 2015: A Renaissance of Patient Care Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities Jeryl Villadolid
Review Article on Lung Cancer Diagnostics and Treatments 2015: A Renaissance of Patient Care Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities Jeryl Villadolid
Ipilimumab in Melanoma
 Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
Type 1 Diabetes: Islet expressing GAD65 (green) with DAPI (Blue) Islet expressing Insulin (red) in 3D confocal imaging
 with DAPI (Blue) Islet expressing Insulin (red) in 3D confocal imaging") Type 1 Diabetes: Our group has been studying autoimmune diabetes for many years. Recently, we have developed a humanized mouse model of Type 1 Diabetes (T1D). We believe this model will help understand
Type 1 Diabetes: Our group has been studying autoimmune diabetes for many years. Recently, we have developed a humanized mouse model of Type 1 Diabetes (T1D). We believe this model will help understand
Title: Thyroid Abnormalities following the use of CTLA-4 and PD-1 Inhibitors in the
 Title: Thyroid Abnormalities following the use of CTLA-4 and PD-1 Inhibitors in the treatment of melanoma Short Title: Thyroid abnormalities following Immune Checkpoint Inhibitors in Melanoma DL Morganstein
Title: Thyroid Abnormalities following the use of CTLA-4 and PD-1 Inhibitors in the treatment of melanoma Short Title: Thyroid abnormalities following Immune Checkpoint Inhibitors in Melanoma DL Morganstein
ATEZOLIZUMAB (TECENTRIQ )
") DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
CANCER IMMUNOTHERAPY. Pocket Guide
 CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
Children s Hospital & Research Center Oakland. Endocrinology
 Children s Hospital & Research Center Oakland Endocrinology 5.22 GOAL: Prevention, Counseling and Screening (Endocrine). Understand the role of the pediatrician in preventing endocrine PC, MK, dysfunction,
Children s Hospital & Research Center Oakland Endocrinology 5.22 GOAL: Prevention, Counseling and Screening (Endocrine). Understand the role of the pediatrician in preventing endocrine PC, MK, dysfunction,
ATEZOLIZUMAB (TECENTRIQ ) in urothelial carcinoma
 in urothelial carcinoma") DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
Thyroid Screen (Serum)
") Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Immunotherapy Overview, Rationale, and Role in Clinical Practice
 Immunotherapy Overview, Rationale, and Role in Clinical Practice Financial Disclosure Bradi L. Frei, PharmD, BCOP, BCPS has no relevant financial relationships with commercial interests to disclose. OBJECTIVES
Immunotherapy Overview, Rationale, and Role in Clinical Practice Financial Disclosure Bradi L. Frei, PharmD, BCOP, BCPS has no relevant financial relationships with commercial interests to disclose. OBJECTIVES
The management of nivolumab-induced endocrine immune-related adverse events
 REVIEW ARTICLE Maria Stelmachowska-Banaś, Wojciech Zgliczyński Department of Endocrinology of the Postgraduate Medical Education Centre, Warsaw The management of nivolumab-induced endocrine immune-related
REVIEW ARTICLE Maria Stelmachowska-Banaś, Wojciech Zgliczyński Department of Endocrinology of the Postgraduate Medical Education Centre, Warsaw The management of nivolumab-induced endocrine immune-related
Immunotherapies. Supporting health professionals to safely care for patients receiving immunotherapy in the cancer setting.
 Immunotherapies Supporting health professionals to safely care for patients receiving immunotherapy in the cancer setting. INDEX Select a topic below for more information Principles of immunotherapy Classes
Immunotherapies Supporting health professionals to safely care for patients receiving immunotherapy in the cancer setting. INDEX Select a topic below for more information Principles of immunotherapy Classes
Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP
 Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP") Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP Division of Medical Oncology and Hematology Bras Drug Development Program Princess Margaret Cancer Centre, Toronto,
Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP Division of Medical Oncology and Hematology Bras Drug Development Program Princess Margaret Cancer Centre, Toronto,
Managing immune related toxicity. Karijn Suijkerbuijk May 27 th 2017
 Managing immune related toxicity Karijn Suijkerbuijk May 27 th 2017 Disclosures Advisory role: BMS, Merck Travel support: Amgen, Novartis, Roche Whybother? Patients are dying from toxicity Eggermont ipilimumab
Managing immune related toxicity Karijn Suijkerbuijk May 27 th 2017 Disclosures Advisory role: BMS, Merck Travel support: Amgen, Novartis, Roche Whybother? Patients are dying from toxicity Eggermont ipilimumab
Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
IMMUNOTHERAPY FOR CANCER A NEW HORIZON. Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust
 IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
Hormones by location
 Endocrine System Hormones by location Pineal Gland: Melatonin Feeling of sleepiness Hypothalamus: Hormones that stimulate or inhibit pituitary Temp., hunger, parenting attachment, thirst Pituitary Gland:
Endocrine System Hormones by location Pineal Gland: Melatonin Feeling of sleepiness Hypothalamus: Hormones that stimulate or inhibit pituitary Temp., hunger, parenting attachment, thirst Pituitary Gland:
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Dra. Omayra Reyes, MD. Hematologist- Oncologist. Introduction to Immuno Oncology
 Dra. Omayra Reyes, MD. Hematologist- Oncologist Introduction to Immuno Oncology Disclosure I have no conflicts of interest Objectives Review Basic concepts of onco- immunology. Recognize different mechanisms
Dra. Omayra Reyes, MD. Hematologist- Oncologist Introduction to Immuno Oncology Disclosure I have no conflicts of interest Objectives Review Basic concepts of onco- immunology. Recognize different mechanisms
9/22/2016. Introduction / Goals. What is Cancer? Pharmacologic Strategies to Treat Cancer. Immune System Modulation
 Immunomodulatory Therapies in Cancer Treatment Bill O Hara, PharmD, BCPS, BCOP Advanced Practice Pharmacist, Oncology/BMT Thomas Jefferson University Hospital Introduction / Goals What is Cancer? How can
Immunomodulatory Therapies in Cancer Treatment Bill O Hara, PharmD, BCPS, BCOP Advanced Practice Pharmacist, Oncology/BMT Thomas Jefferson University Hospital Introduction / Goals What is Cancer? How can
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy
 due to Cancer Immunotherapy") Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy Philip Mease MD Director, Rheumatology Clinical Research, Swedish- Providence St. Joseph Health Clinical Professor, University of Washington
Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy Philip Mease MD Director, Rheumatology Clinical Research, Swedish- Providence St. Joseph Health Clinical Professor, University of Washington
9/11/2012. Chapter 11. Learning Objectives. Learning Objectives. Endocrine Emergencies. Differentiate type 1 and type 2 diabetes
 Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Ch 8: Endocrine Physiology
 Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Rheumatology winter clinical symposium 9 th annual meeting Maui, Hawaii February
 New onset polyarthritis secondary to pembrolizumab [anti-pd1 antibody] in a patient with metastatic melanoma successfully treated with IL-6 receptor [IL-6R] inhibitor. Salvador R. Garcia1, MD; Adi Diab2,
New onset polyarthritis secondary to pembrolizumab [anti-pd1 antibody] in a patient with metastatic melanoma successfully treated with IL-6 receptor [IL-6R] inhibitor. Salvador R. Garcia1, MD; Adi Diab2,
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Critical illness and endocrinology. ICU Fellowship Training Radboudumc
 Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Chapter 12 Endocrine System (export).notebook. February 27, Mar 17 2:59 PM. Mar 17 3:09 PM. Mar 17 3:05 PM. Mar 17 3:03 PM.
.notebook. February 27, Mar 17 2:59 PM. Mar 17 3:09 PM. Mar 17 3:05 PM. Mar 17 3:03 PM.") Endocrine System Hormones Chemical messengers released directly into the bloodstream Regulate: *May have wide spread effect or only affect certain tissues ** : cells with receptors that respond to specific
Endocrine System Hormones Chemical messengers released directly into the bloodstream Regulate: *May have wide spread effect or only affect certain tissues ** : cells with receptors that respond to specific
Sample Type - Serum Result Reference Range Units. Central Thyroid Regulation Surrey & Activity KT3 4Q. Peripheral Thyroid D Function mark
 Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Medically Compromised Patients (Part II)
") Medically Compromised Patients (Part II) Ra ed Salma BDS, MSc, JBOMFS, MFDRCSI Endocrine Disorders I. Diabetes Mellitus (DM) Definition (WHO): - Chronic disease due to absolute or relative lack of insulin
Medically Compromised Patients (Part II) Ra ed Salma BDS, MSc, JBOMFS, MFDRCSI Endocrine Disorders I. Diabetes Mellitus (DM) Definition (WHO): - Chronic disease due to absolute or relative lack of insulin
Endocrinological Outcome Among Treated Craniopharyngioma Patients
 Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab
 BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab Protocol Code Tumour Group Contact Physician ULUAVPMB Lung Dr. Christopher Lee ELIGIBILITY: Advanced
BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab Protocol Code Tumour Group Contact Physician ULUAVPMB Lung Dr. Christopher Lee ELIGIBILITY: Advanced
I. Provide patient care that is compassionate, appropriate and effective for the prevention and treatment of endocrinologic disorders.
 Endocrinology Curriculum Goal Endocrinology is the diagnosis and care of disorders of the endocrine system. The principal endocrine problems handled by the general internist include goiter, thyroid nodules,
Endocrinology Curriculum Goal Endocrinology is the diagnosis and care of disorders of the endocrine system. The principal endocrine problems handled by the general internist include goiter, thyroid nodules,
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Nivolumab and Ipilimumab
 Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Immunotherapy Concept Turned Reality
 Authored by: Jennifer Dolan Fox, PhD VirtualScopics Inc. jennifer_fox@virtualscopics.com +1 585 249 6231 Immunotherapy Concept Turned Reality Introduction While using the body s own immune system as a
Authored by: Jennifer Dolan Fox, PhD VirtualScopics Inc. jennifer_fox@virtualscopics.com +1 585 249 6231 Immunotherapy Concept Turned Reality Introduction While using the body s own immune system as a
Tumor Immunity and Immunotherapy. Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School
 Tumor Immunity and Immunotherapy Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School Lecture Outline Evidence for tumor immunity Types of tumor antigens Generation of anti-tumor
Tumor Immunity and Immunotherapy Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School Lecture Outline Evidence for tumor immunity Types of tumor antigens Generation of anti-tumor
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Immune-Related Adverse Reaction (irar) Management Guide
 Management Guide") REGIMEN Immune-Related Adverse Reaction (irar) Management Guide OPDIVO as monotherapy is indicated for the treatment of locally advanced or metastatic squamous non-small cell lung cancer (NSCLC) with progression
REGIMEN Immune-Related Adverse Reaction (irar) Management Guide OPDIVO as monotherapy is indicated for the treatment of locally advanced or metastatic squamous non-small cell lung cancer (NSCLC) with progression
KEYTRUDA is also indicated in combination with pemetrexed and platinum chemotherapy for the
 FDA-Approved Indication for KEYTRUDA (pembrolizumab) in Combination With Carboplatin and Either Paclitaxel or Nab-paclitaxel for the Firstline Treatment of Patients With Metastatic Squamous Non Small Cell
FDA-Approved Indication for KEYTRUDA (pembrolizumab) in Combination With Carboplatin and Either Paclitaxel or Nab-paclitaxel for the Firstline Treatment of Patients With Metastatic Squamous Non Small Cell
Highlights from AACR 2015: The Emerging Potential of Immunotherapeutic Approaches in Non-Small Cell Lung Cancer
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab
 BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab Protocol Code Tumour Group Contact Physician USMAVNIV Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab Protocol Code Tumour Group Contact Physician USMAVNIV Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
Summary of risk management plan for OPDIVO (nivolumab)
") Summary of risk management plan for OPDIVO (nivolumab) This is a summary of the risk management plan (RMP) for OPDIVO. The RMP details important risks of OPDIVO, how these risks can be minimized, and how
Summary of risk management plan for OPDIVO (nivolumab) This is a summary of the risk management plan (RMP) for OPDIVO. The RMP details important risks of OPDIVO, how these risks can be minimized, and how
Chapter 20. Endocrine System Chemical signals coordinate body functions Chemical signals coordinate body functions. !
 26.1 Chemical signals coordinate body functions Chapter 20 Endocrine System! Hormones Chemical signals Secreted by endocrine glands Usually carried in the blood Cause specific changes in target cells Secretory
26.1 Chemical signals coordinate body functions Chapter 20 Endocrine System! Hormones Chemical signals Secreted by endocrine glands Usually carried in the blood Cause specific changes in target cells Secretory
Summary of risk management plan for OPDIVO (nivolumab)
") Summary of risk management plan for OPDIVO (nivolumab) This is a summary of the risk management plan (RMP) for OPDIVO. The RMP details important risks of OPDIVO, how these risks can be minimized, and how
Summary of risk management plan for OPDIVO (nivolumab) This is a summary of the risk management plan (RMP) for OPDIVO. The RMP details important risks of OPDIVO, how these risks can be minimized, and how
Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies. Michael A. Curran, Ph.D.
 Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies Michael A. Curran, Ph.D. MD Anderson Cancer Center Department of Immunology Disclosures I have research
Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies Michael A. Curran, Ph.D. MD Anderson Cancer Center Department of Immunology Disclosures I have research
Pituitary for the General Practitioner. Marilyn Lee Consultant physician and endocrinologist
 Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immunotherapy in lung cancer. Saurabh maji
 Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
PROBLEMS WITH REGULATION AND METABOLISM. Objectives A & P 8/11/2011
 PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors
 New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors Farah Brasfield, MD Chair, Regional Chiefs of Oncology Kaiser Permanente Jennifer Chang, PharmD, MPH Supervisor, Drug Information Services
New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors Farah Brasfield, MD Chair, Regional Chiefs of Oncology Kaiser Permanente Jennifer Chang, PharmD, MPH Supervisor, Drug Information Services
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013
 panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013 PITUITARY GLAND (HYPOPHYSIS CEREBRI) The master of endocrine glands master of endocrine glands It is a small oval
panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013 PITUITARY GLAND (HYPOPHYSIS CEREBRI) The master of endocrine glands master of endocrine glands It is a small oval
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Healthcare Professional. Frequently Asked. Questions. Brochure
 YERVOY (ipilimumab) Healthcare Professional Frequently Asked Questions Brochure YERVOY is indicated for the treatment of advanced (unresectable or metastatic) melanoma in adults. 1 This medicinal product
YERVOY (ipilimumab) Healthcare Professional Frequently Asked Questions Brochure YERVOY is indicated for the treatment of advanced (unresectable or metastatic) melanoma in adults. 1 This medicinal product
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing
 Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury
 Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
62-year-old woman with severe headache. Celeste Thomas November 1, 2012
 62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo
 U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo (nivolumab) in Patients with Previously Untreated Advanced Melanoma Application includes CheckMate -066,
U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo (nivolumab) in Patients with Previously Untreated Advanced Melanoma Application includes CheckMate -066,
NOTES 11.5: ENDOCRINE SYSTEM. Pages
 NOTES 11.5: ENDOCRINE SYSTEM Pages 1031-1042 ENDOCRINE SYSTEM Communication system that controls metabolism, growth, and development with hormones Maintains homeostasis Hormones: chemical messengers released
NOTES 11.5: ENDOCRINE SYSTEM Pages 1031-1042 ENDOCRINE SYSTEM Communication system that controls metabolism, growth, and development with hormones Maintains homeostasis Hormones: chemical messengers released
BAPTIST HEALTH SCHOOL OF NURSING NSG 3026A: CHILDREN S HEALTH
 J 1 BAPTIST HEALTH SCHOOL OF NURSING NSG 3026A: CHILDREN S HEALTH NURSING MANAGEMENT OF ENDOCRINE DYSFUNCTION: THEORETICAL SKILLS and KNOWLEDGE, SCIENTIFIC PRINCIPLES, CRITICAL THINKING, HEALTHCARE PROMOTION,
J 1 BAPTIST HEALTH SCHOOL OF NURSING NSG 3026A: CHILDREN S HEALTH NURSING MANAGEMENT OF ENDOCRINE DYSFUNCTION: THEORETICAL SKILLS and KNOWLEDGE, SCIENTIFIC PRINCIPLES, CRITICAL THINKING, HEALTHCARE PROMOTION,
For the Patient: USMAVNIV
 For the Patient: USMAVNIV Other Names: Treatment of Unresectable or Metastatic Melanoma Using Nivolumab U = Undesignated (requires special approval) SM = Skin and Melanoma AV = AdVanced NIV = NIVolumab
For the Patient: USMAVNIV Other Names: Treatment of Unresectable or Metastatic Melanoma Using Nivolumab U = Undesignated (requires special approval) SM = Skin and Melanoma AV = AdVanced NIV = NIVolumab
PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses
 PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses Patrick J. Medina, 1, * and Val R. Adams, 2 1 Department of Pharmacy: Clinical and Administrative Sciences, The
PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses Patrick J. Medina, 1, * and Val R. Adams, 2 1 Department of Pharmacy: Clinical and Administrative Sciences, The
For the Patient: USMAVPEM
 For the Patient: USMAVPEM Other Names: Treatment of Unresectable or Metastatic Melanoma Using Pembrolizumab U = Undesignated (requires special request) SM = Skin and Melanoma AV = Advanced PEM = Pembrolizumab
For the Patient: USMAVPEM Other Names: Treatment of Unresectable or Metastatic Melanoma Using Pembrolizumab U = Undesignated (requires special request) SM = Skin and Melanoma AV = Advanced PEM = Pembrolizumab
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER. Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia
 IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
Attached from the following page is the press release made by BMS for your information.
 June 2, 2015 Opdivo (nivolumab) Demonstrates Superior Survival Compared to Standard of Care (docetaxel) for Previously-Treated Squamous Non-Small Cell Lung Cancer in Phase III Trial (PRINCETON, NJ, May
June 2, 2015 Opdivo (nivolumab) Demonstrates Superior Survival Compared to Standard of Care (docetaxel) for Previously-Treated Squamous Non-Small Cell Lung Cancer in Phase III Trial (PRINCETON, NJ, May
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Endocrine Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Endocrine Revised: 11/2013 Endocrine system includes 8 major glands. 1. Pituitary (master gland)
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Endocrine Revised: 11/2013 Endocrine system includes 8 major glands. 1. Pituitary (master gland)