TOXICITY RELATED TO IO IN LUNG CANCER
|
|
|
- Fay Cameron
- 5 years ago
- Views:
Transcription



1 TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico city, Mexico

2 1947 Sidney Farber ( ) Aminopterine: Folic acid Inh Acute Lympholastic Leukemia Schiller JH et al N Engl J Med 2002; 346:92-98

3 The Magic Bullet

4 TKI s efficacy FLAURA Immunotherapies Efficacy KEYNOTE 024 ALEX COMBOS: CM 227 & KN 189
5



6 BUT. THEY HAVE DIFFERENT TOXICITY PROFILE ALTHOUGH BETTER TOLERATED CHEMO IO tkitkis Habanero Chili Spicy ++++/++++ Chipotle Chili Spicy ++/++++ Poblano Chili Spicy +/++++
7 IO monotherapy and Combo Toxicity TKI s Toxicity

8 IO monotherapy and Combo Toxicity TKI s Toxicity

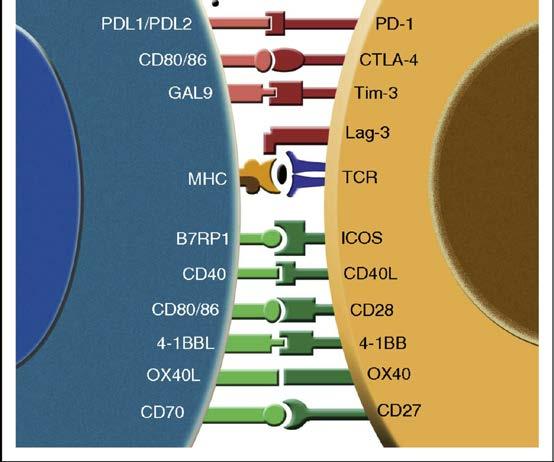
9 Cancer Immunity Cicle
10
11
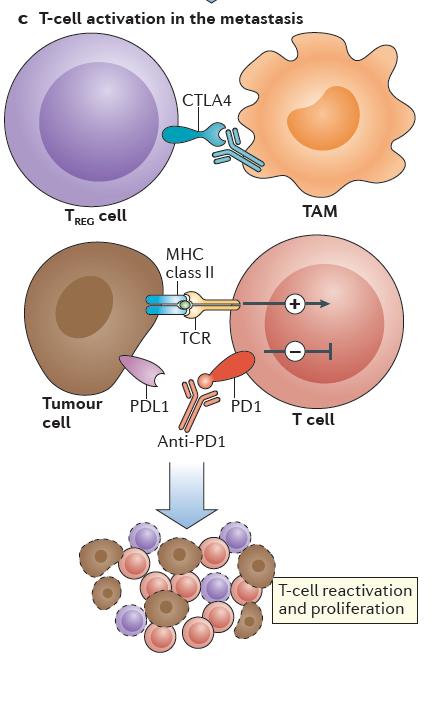
12 Cancer Immunity Cicle CTLA-4 is expressed on regulatory T cells (TREG), a type of T cell that suppresses the immune response in the tumour microenvironment. CTLA-4 blockade results in a broad, nonspecific activation of an immune response CTLA-4 PD-1/PD-L1 PD-L1 is frequently upregulated on the tumour cell surface. By targeting T cells more specifically in the tumour microenvironment and tissues, treatment with PD-1 inhibition results in a more restricted spectrum of adverse events compared with CTLA-4 blockade
13
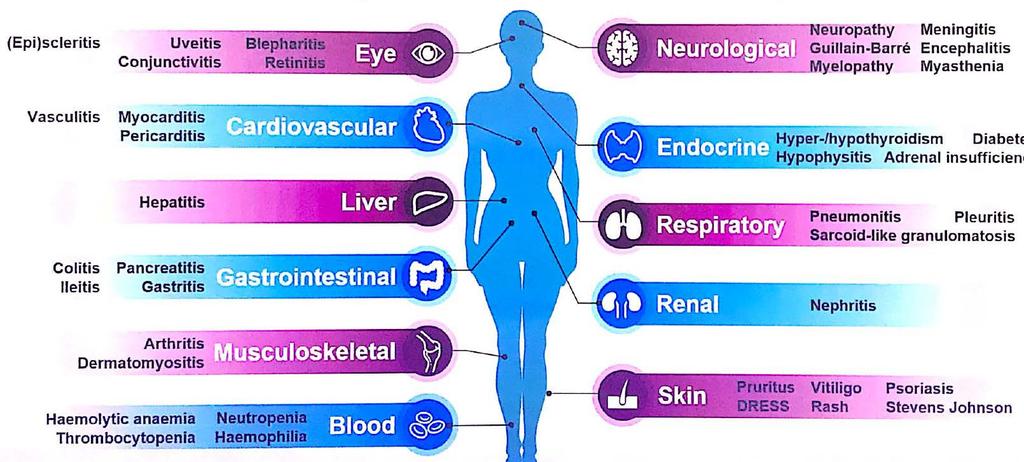
14 Immune-related adverse events can affect any organ system The frequency of iraes following immunotherapy is probably underestimated. Most clinical trials follow patients for only a brief time of enrollment Some iraes can have a delayed onset: Thyroiditis (3 years after initiation of anti-ctla4) T1D (from weeks to decades) Champiat S et al. Ann Oncol 2016;27:559-74
15


16 PREVENTION: We know the most common General AEs
17 PREVENTION: We know IRAE s
18 ANTICIPATE: Know your patient: Measure & Grade General Endocrine Infectious Auto- Antibodies BASAL LABS CBC, Serum Electrolytes, Cr, Liver function Test TSH, T4, T3 HIV, HBV, HCV and CMV ANA, anti-thyiroid
19 WHAT WE LEARNED FROM MELANOMA: IMMUNE MEDIATED ANTICIPATE: Time Since Development of Adverse Events PD-1 Blockade
20 ANTICIPATE: Time Since Development of Adverse Events PD-1 Blockade

21 General Management of irae
22 General Management of Toxicities: IO GRADE Grade 2 Toxicity Grade 3 or 4 Withheld and should not be resumed until symptoms or toxicity is grade 1 or less Treatment with the checkpoint inhibitor should be permanently discontinued. CORTICOESTEROIDE Prednisone 0.5 mg/kg/day or equivalent should be started if symptoms do not resolve within a week High doses of corticosteroids (prednisone 1 to 2 mg/kg/day or equivalent) should be given. When symptoms subside to grade 1 or less, steroids can be gradually tapered over at least one month. If symptoms do not improve, after approximately three days with IV steroids, administer infliximab (5 mg/kg). If symptoms persist after the first infliximab dose, a second dose of infliximab (5 mg/kg) can be repeated two weeks after the initial dose.
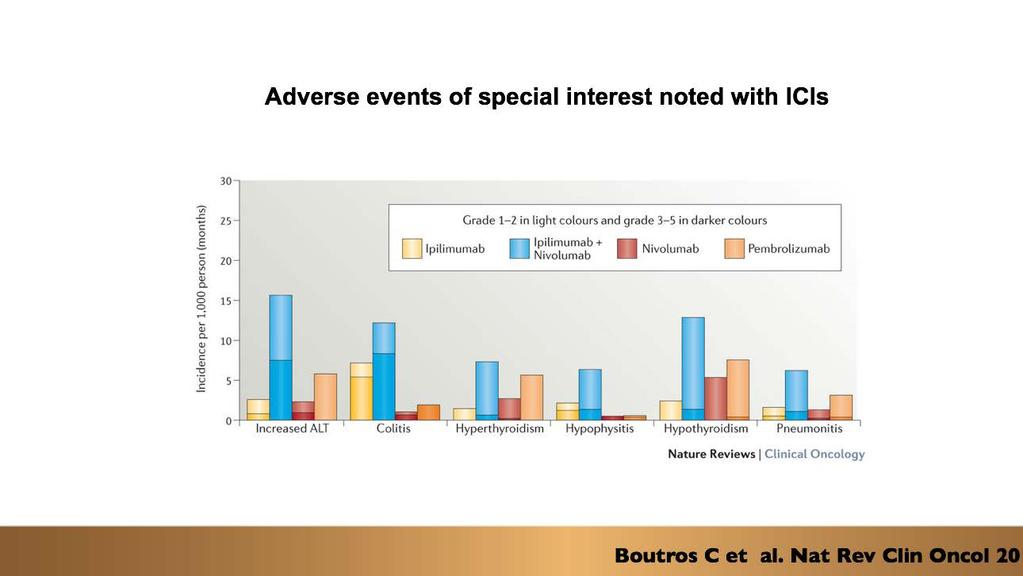
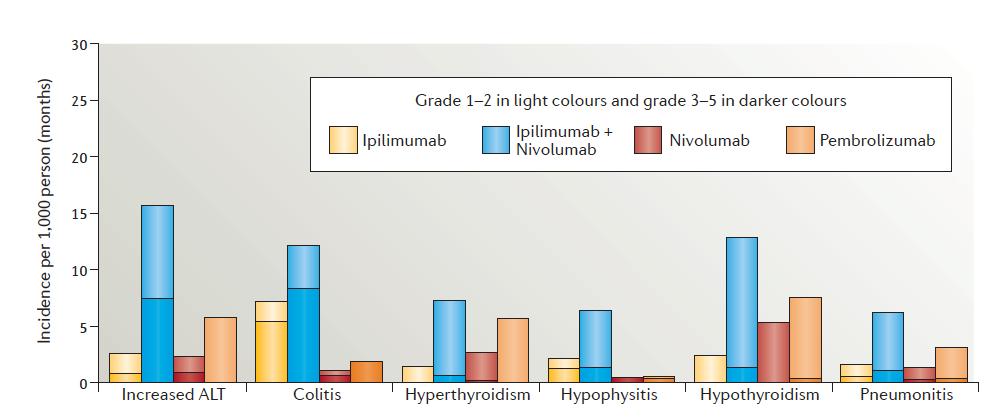
 38 Systematic Reviews + 166 primary studies met eligibility criteria Brahmer J et al J Clin")
23 TOXICITIES DUE TO CHECKPOINT INHIBITORS Multidisciplinary Group Only Info of IO (Not Combos with Chemo) 38 Systematic Reviews primary studies met eligibility criteria Brahmer J et al J Clin Oncol 2018
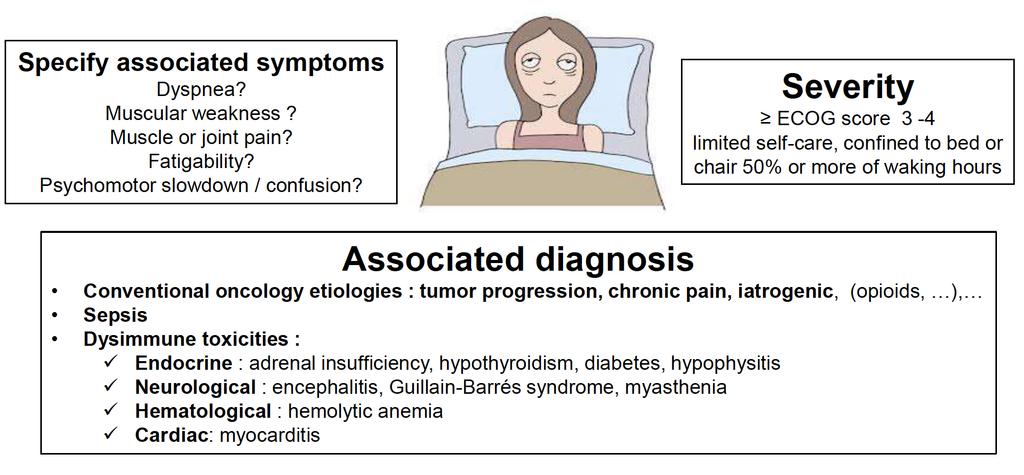
24 FATIGUE
25 Fatigue CLINICAL TRIAL N ALL GRADES 3-4 IPI + NIVO CHECMATE 227 NIVOLUMAB CHECKMATE CHECKMATE PEMBROLIZUMAB KEYNOTE 024 PEMBROLIZUMAB KEYNOTE 10 (2 mg/k) ATEZO + BEV + Che IMPOWER 150 ATEZO OAK DURVA + RT PACIFIC Pend Pend
26 Decreased Apetite CLINICAL TRIAL N ALL GRADES 3-4 IPI + NIVO CHECMATE 227 NIVOLUMAB CHECKMATE CHECKMATE PEMBROLIZUMAB KEYNOTE 024 PEMBROLIZUMAB KEYNOTE 10 (2 mg/k) ATEZO + BEV + Che IMPOWER 150 ATEZO OAK DURVA + RT PACIFIC Pend Pend 425 NR NR

27 Skin Reactions
28 *NR, probably due < 10% FRECUENCY OF RASH/INFLAMATORY DERMATITIS IN NSCLC TRIALS CLINICAL TRIAL N ALL GRADES 3-4 IPI + NIVO CHECMATE 227 NIVOLUMAB CHECKMATE % 1.6% % 0.8% CHECKMATE NR * NR* PEMBROLIZUMAB KEYNOTE 024 PEMBROLIZUMAB KEYNOTE 10 (2 mg/k) PEMBROLIZUMAB KEYNOTE 001 ATEZO + BEV + Che IMPOWER NR* NR* 339 NR* NR* PEND NR* ATEZO OAK DURVA + RT PACIFIC 425 NR * NR* % 0.2%

29 Grade Definition Management 1 Symptoms do not affect the quality of life or controlled with topical regimen and/or oral antipruritic 2 Inflammatory reaction that affects quality of life and requires intervention based on diagnosis 3 As G2 but with failure to respond to indicated interventions for a G 2 dermatitis 4 All severe rashes unmanageable with prior interventions and intolerable Continue ICPi Treat with topical emollients and/or mild-moderate potency topical corticosteroids Counsel patients to avoid skin irritants and sun exposure Consider holding ICPi and monitor weekly for improvement. If not resolved, interrupt treatment until skin AE has reverted to grade 1 Consider initiating prednisone 1 mg/kg. In addition, treat with topical emollients, oral antihistamines, and medium- to high potency topical corticosteroids Hold ICPi therapy and consult with dermatology. topical emollients, oral antihistamines, and high-potency topical corticosteroidsinitiate (methyl)prednisolone (or equivalent) 1-2 mg/kg Immediately hold ICPi and consult dermatology to determine appropriateness of resuming ICPi (methyl)prednisolone (or equivalent) dosed at 1-2 mg/kg Monitor closely for progression to severe cutaneous adverse reaction.



30 Not all skin toxicities are bad..... Re-pigmentation
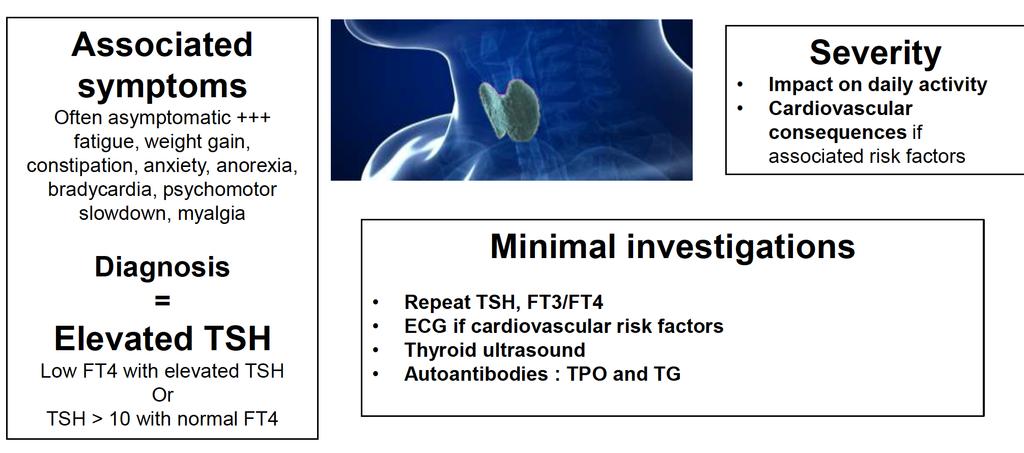
31 HYPOTHYROIDISM
32 Hypothyroidism **OAK Trial didn t report Hypothiroisism CLINICAL TRIAL N ALL GRADES 3-4 IPI + NIVO CHECMATE 227 NIVOLUMAB CHECKMATE CHECKMATE NR NR PEMBROLIZUMAB KEYNOTE 024 PEMBROLIZUMAB KEYNOTE 10 (2 mg/k) ATEZO + BEV + Che IMPOWER 150 ATEZO POPLAR** DURVA + RT PACIFIC < %

33 Hypothyroidism Grade Definition Management 1 TSH, 10 miu/l and asymptomatic 2 Moderate symptoms; able to perform ADL; TSH persistently. 10 miu/l 3-4 Severe symptoms, medically significant or lifethreatening consequences, unable to perform ADL Should continue ICPi with close follow-up and monitoring of TSH, FT4 May hold ICPi until symptoms resolve Prescribe thyroid hormone supplementation in symptomatic patients with any degree of TSH elevation or in asymptomatic patients with TSH levels that persist. Hold ICPi, supplementation, Endocrine consultation. May admit for IV therapy if signs of myxedema (bradycardia, hypothermia) Thyroid supplementation and reassessment as in G2
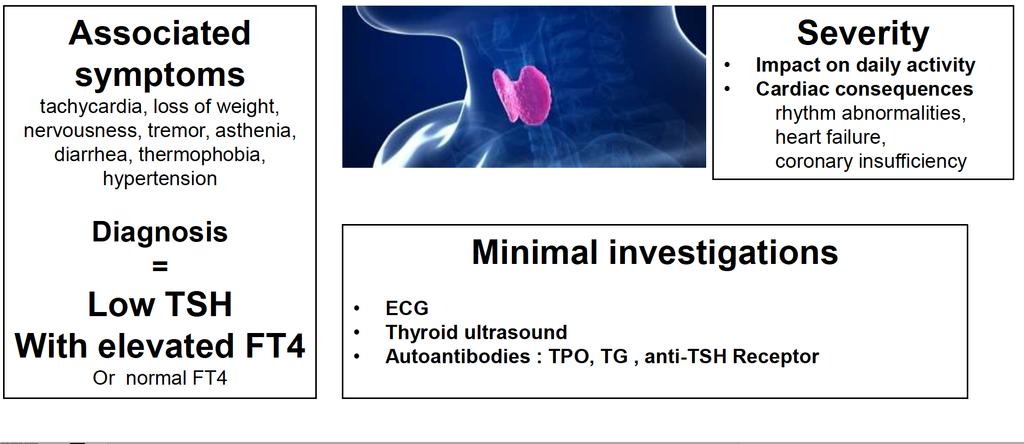
34 HYPERTHYROIDISM
35 Hyperthyroidism in IO NSCLC Trials CLINICAL TRIAL N ALL GRADES 3-4 IPI + NIVO CHECMATE 227 NIVOLUMAB CHECKMATE NR NR 391 NR NT CHECKMATE NR NR PEMBROLIZUMAB KEYNOTE 024 PEMBROLIZUMAB KEYNOTE 10 (2 mg/k) ATEZO + BEV + Che IMPOWER 150 ATEZO OAK DURVA + RT PACIFIC <1 425 NR NR 475 NR NR
36 Hyperthyroidism Grade Definition Management 1 Asymptomatic or mild symptoms 2 Moderate symptoms, able to perform ADL 3-4 Severe symptoms, medically significant or lifethreatening consequences, unable to perform ADL Can continue ICPi with close follow-up and monitoring of TSH, FT4 every 2-3 weeks Consider holding ICPi until symptoms return to baseline Consider endocrine consultation (eg, atenolol, propranolol) for symptomatic relief. Corticosteroids are not usually required to shorten duration and consider thionamide (methimazole or PTU) Refer to endocrinology for Graves disease Hold ICPi until symptoms resolve. Endocrine consultationb-blocker (eg, atenolol, propranolol) for symptomatic relief For severe symptoms or concern for thyroid storm, hospitalize patient and initiate prednisone 1-2 mg/kg/d or equivalent consider also use of SSKI or thionamide (methimazole or PTU).
37
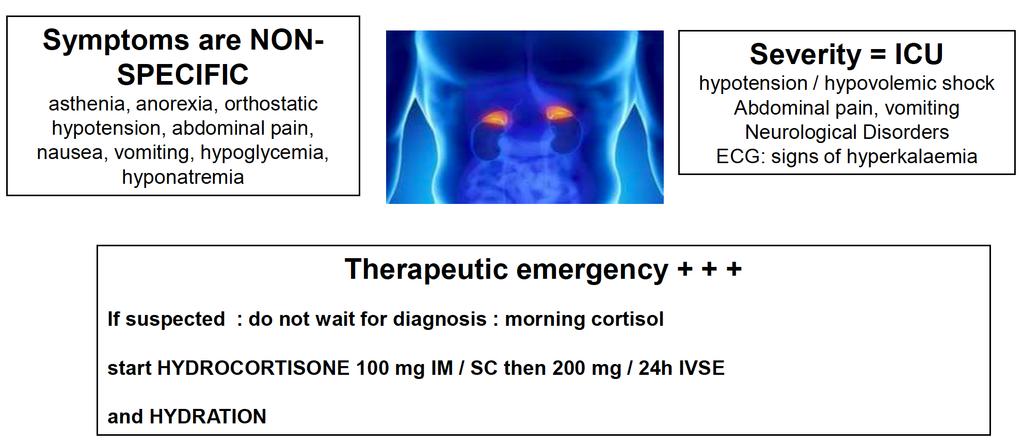
38 ADRENAL INSUFFICIENCY
39 Frecuency of Adrenal Insufficiency Between Trials NSCLC CLINICAL TRIAL N ALL GRADES 3-4 IPI + NIVO CHECMATE 227 NIVOLUMAB CHECKMATE <1 391 NR NR CHECKMATE PEMBROLIZUMAB KEYNOTE 024 PEMBROLIZUMAB KEYNOTE 10 (2 mg/k) ATEZO + BEV + Che IMPOWER 150 ATEZO OAK DURVA + RT PACIFIC 154 NR NR <1 425 NR NR
40 Adrenal Insufficiency Grade Definition Management 1 Asymptomatic or mild symptoms 2 Moderate symptoms, able to perform ADL Consider holding ICPi until patient is stabilized on replacement hormone. Endocrine consultation. Replacement therapy with prednisone (5-10 mg daily) or hydrocortisone (10-20 mg orally every morning, 5-10 mg orally in early afternoon). May require fludrocortisone (0.1 mg/d) for mineralocorticoid replacement in primary adrenal insufficiency Titrate dose up or down as symptoms dictate Hold ICPi until patient is stabilized on replacement hormone Endocrine consultation See in clinic or, for after hours, make an emergency department referral for normal saline (at least 2 L) and IV stress-dose corticosteroids on presentation (hydrocortisone 100 mg) taper stress-dose corticosteroids down to maintenance doses over 7-14 days after discharge. Maintenance therapy as in G1
41 Adrenal Insufficiency Grade Definition Management 3-4 Severe symptoms, medically significant or lifethreatening consequences, unable to perform ADL Hold ICPi until patient is stabilized on replacement hormone Endocrine consultation See in clinic or, for after hours, make an emergency department referral for normal saline (at least 2 L) and IV stress-dose corticosteroids on presentation(hydrocortisone 100 mg or dexamethasone 4 mg (if the diagnosis is not clear and stimulation testing will be needed) Taper stress-dose corticosteroids down to maintenance doses over 7-14 days after dischargemaintenance therapy as in G1

42 PNEUMONITIS

43 Naidoo et al, J Clin Oncol 2016 DIFFERENT PRESENTATIONS
44 Pneumonitis ** Placebo group had pneumonitis all grades 24.8 & grade (grade 5: 0.4%) CLINICAL TRIAL N ALL GRADES 3-4 IPI + NIVO CHECMATE 227 NIVOLUMAB CHECKMATE 227 NIVOLUMAB CHECKMATE 057 PEMBROLIZUMAB KEYNOTE 024 PEMBROLIZUMAB KEYNOTE 10 (2 mg/k) ATEZO + BEV + Che IMPOWER 150 ATEZO OAK DURVA + RT PACIFIC ** 576 NR NR 391 NR NR 287 NR NR
45 PNEUMONITIS
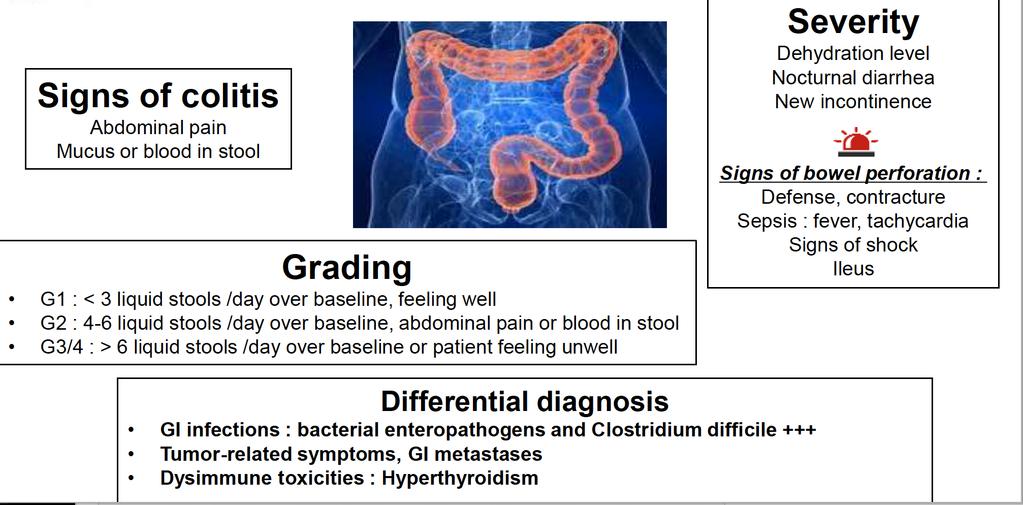
46 DIARRHEA/COLITIS
47 Frecuency of Colitis Between Trials in NSCLC CLINICAL TRIAL N ALL GRADES 3-4 IPI + NIVO CHECMATE 227 NIVOLUMAB CHECKMATE <1 391 NR NR CHECKMATE PEMBROLIZUMAB KEYNOTE 024 PEMBROLIZUMAB KEYNOTE 10 (2 mg/k) ATEZO + BEV + Che IMPOWER 150 ATEZO OAK DURVA + RT PACIFIC NR NR NR NR

48 Diarrhea/Colitis AMBULATORY HOSPITALIZED

49 Pillai R et al Cancer 2017
50




51 INSTITUTO NACIONAL DE ENFERMEDADES RESPIRATORIAS CENTRO MÉDICO ABC
CANCER IMMUNOTHERAPY. Pocket Guide
 CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
Management of Immune Checkpoint Inhibitor Related Toxicities
 Management of Immune Checkpoint Inhibitor Related Toxicities Katie Wolfram, PharmD Clinical Pharmacist, Oncology Memorial Hospital of South Bend A Webinar for HealthTrust Members November 12, 2018 Disclosures
Management of Immune Checkpoint Inhibitor Related Toxicities Katie Wolfram, PharmD Clinical Pharmacist, Oncology Memorial Hospital of South Bend A Webinar for HealthTrust Members November 12, 2018 Disclosures
Melanoma Immunotherapy. Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management
 Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
PEMBROLIZUMAB (KEYTRUDA ) for the treatment of advanced melanoma or previously treated NSCLC
 for the treatment of advanced melanoma or previously treated NSCLC") DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent Rate Day 1 Pembrolizumab 2mg/kg IV Infusion 100mL 0.9% Sodium Chloride* Or 100mL 5% Glucose* *Final concentration must be between 1 to 10mg/mL Over
DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent Rate Day 1 Pembrolizumab 2mg/kg IV Infusion 100mL 0.9% Sodium Chloride* Or 100mL 5% Glucose* *Final concentration must be between 1 to 10mg/mL Over
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS
 OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy: Toxicity Management. Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital
 Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
NECN CHEMOTHERAPY HANDBOOK PROTOCOL
 Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab
 BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab Protocol Code Tumour Group Contact Physician ULUAVPMB Lung Dr. Christopher Lee ELIGIBILITY: Advanced
BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab Protocol Code Tumour Group Contact Physician ULUAVPMB Lung Dr. Christopher Lee ELIGIBILITY: Advanced
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity. Disclosure Statement. Learning Objectives
 Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities
 Review Article on Lung Cancer Diagnostics and Treatments 2015: A Renaissance of Patient Care Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities Jeryl Villadolid
Review Article on Lung Cancer Diagnostics and Treatments 2015: A Renaissance of Patient Care Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities Jeryl Villadolid
MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS
 MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS John B.A.G. Haanen MD PhD CONTENT OF THIS PRESENTATION General aspects of immune related adverse events related to immune checkpoint
MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS John B.A.G. Haanen MD PhD CONTENT OF THIS PRESENTATION General aspects of immune related adverse events related to immune checkpoint
Managing immune related toxicity. Karijn Suijkerbuijk May 27 th 2017
 Managing immune related toxicity Karijn Suijkerbuijk May 27 th 2017 Disclosures Advisory role: BMS, Merck Travel support: Amgen, Novartis, Roche Whybother? Patients are dying from toxicity Eggermont ipilimumab
Managing immune related toxicity Karijn Suijkerbuijk May 27 th 2017 Disclosures Advisory role: BMS, Merck Travel support: Amgen, Novartis, Roche Whybother? Patients are dying from toxicity Eggermont ipilimumab
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
ATEZOLIZUMAB (TECENTRIQ )
") DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
 Hull and East Yorkshire Hospital NHS Trust Queen s centre for Oncology and Haematology Castle Hill Hospital HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
Hull and East Yorkshire Hospital NHS Trust Queen s centre for Oncology and Haematology Castle Hill Hospital HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
Adverse effects of Immunotherapy. Asha Nayak M.D
 Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Managing Checkpoint Inhibitor Toxicities. Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute
 Managing Checkpoint Inhibitor Toxicities Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute Approved Indications Ipilimumab Nivolumab Pembrolizumab* Atezolizumab Avelumab Durvalumab Ipi + Nivol
Managing Checkpoint Inhibitor Toxicities Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute Approved Indications Ipilimumab Nivolumab Pembrolizumab* Atezolizumab Avelumab Durvalumab Ipi + Nivol
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab
 BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab Protocol Code Tumour Group Contact Physician USMAVNIV Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab Protocol Code Tumour Group Contact Physician USMAVNIV Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
Nursing Perspective on iraes: Patient Education, Monitoring and Management
 Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
BCCA Protocol Summary for Treatment of Advanced Non-Small Cell Lung Cancer Using Nivolumab
 BCCA Protocol Summary for Treatment of Advanced Non-Small Cell Lung Cancer Using Nivolumab Protocol Code Tumour Group Contact Physician ULUAVNIV Lung Dr. Christopher Lee ELIGIBILITY: Advanced non-small
BCCA Protocol Summary for Treatment of Advanced Non-Small Cell Lung Cancer Using Nivolumab Protocol Code Tumour Group Contact Physician ULUAVNIV Lung Dr. Christopher Lee ELIGIBILITY: Advanced non-small
ATEZOLIZUMAB (TECENTRIQ ) in urothelial carcinoma
 in urothelial carcinoma") DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors
 New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors Farah Brasfield, MD Chair, Regional Chiefs of Oncology Kaiser Permanente Jennifer Chang, PharmD, MPH Supervisor, Drug Information Services
New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors Farah Brasfield, MD Chair, Regional Chiefs of Oncology Kaiser Permanente Jennifer Chang, PharmD, MPH Supervisor, Drug Information Services
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab
 BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab Protocol Code Tumour Group Contact Physician UGUAVNIV Genitourinary Dr. C. Kollmannsberger ELIGIBILITY:
BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab Protocol Code Tumour Group Contact Physician UGUAVNIV Genitourinary Dr. C. Kollmannsberger ELIGIBILITY:
Toxicity of Systemic Melanoma Therapies. Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney
 Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Complications of Immunotherapy
 Complications of Immunotherapy Sarah Norskog, PharmD, BCOP Oncology Pharmacy Specialist University of Colorado Hospital Disclosures I have no relevant financial relationships with commercial interests
Complications of Immunotherapy Sarah Norskog, PharmD, BCOP Oncology Pharmacy Specialist University of Colorado Hospital Disclosures I have no relevant financial relationships with commercial interests
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY
 ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Cancer Immunotherapy: Promises and Challenges. Disclosures
 Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes
 Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes Geoffrey T. Gibney, MD Associate Professor Co-leader, Melanoma Disease Group Lombardi Comprehensive Cancer Center
Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes Geoffrey T. Gibney, MD Associate Professor Co-leader, Melanoma Disease Group Lombardi Comprehensive Cancer Center
CANCER IMMUNOTHERAPY Presented by John A Keech Jr DO MultiCare Regional Cancer Center
 CANCER IMMUNOTHERAPY 2018 Presented by John A Keech Jr DO MultiCare Regional Cancer Center Successful anti-cancer immunity is autoimmunity Green, The Scientist, 2014 Immunotherapy strategies Cancer vaccines
CANCER IMMUNOTHERAPY 2018 Presented by John A Keech Jr DO MultiCare Regional Cancer Center Successful anti-cancer immunity is autoimmunity Green, The Scientist, 2014 Immunotherapy strategies Cancer vaccines
University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018
 University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is
University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is
CASE-BASED MANAGEMENT IN IMMUNO- ONCOLOGY
 CASE-BASED MANAGEMENT IN IMMUNO- ONCOLOGY Prof. Solange Peters, MD-PhD Cheffe de Service Oncologie Médicale & Clinique Thoracique CHUV- Lausanne & Institut Ludwig GENERAL QUESTIONS Your 62-yr-old patient,
CASE-BASED MANAGEMENT IN IMMUNO- ONCOLOGY Prof. Solange Peters, MD-PhD Cheffe de Service Oncologie Médicale & Clinique Thoracique CHUV- Lausanne & Institut Ludwig GENERAL QUESTIONS Your 62-yr-old patient,
Nivolumab Ipilimumab Combination Therapy
 INDICATIONS FOR USE: Nivolumab Ipilimumab Combination INDICATION ICD10 Regimen Code *Reimbursement Status Nivolumab in combination with ipilimumab is indicated for the treatment of advanced (unresectable
INDICATIONS FOR USE: Nivolumab Ipilimumab Combination INDICATION ICD10 Regimen Code *Reimbursement Status Nivolumab in combination with ipilimumab is indicated for the treatment of advanced (unresectable
Immunoterapia di 1 linea Evidenze e Prospettive Future
 Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
NCCP Chemotherapy Regimen
 INDICATIONS FOR USE: Pembrolizumab 2mg/kg INDICATION ICD10 Regimen Code *Reimbursement Status First line monotherapy for the treatment of advanced (unresectable or C43 00347a ODMS metastatic) melanoma
INDICATIONS FOR USE: Pembrolizumab 2mg/kg INDICATION ICD10 Regimen Code *Reimbursement Status First line monotherapy for the treatment of advanced (unresectable or C43 00347a ODMS metastatic) melanoma
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Nivolumab/Ipilimumab Combination Therapy for Renal Cell Carcinoma (RCC)
") Nivolumab/Ipilimumab Combination Therapy for Renal Cell Carcinoma (RCC) An HCP Tool From the Immuno-Oncology Essentials Initiative The combination of nivolumab (Opdivo ) and ipilimumab (Yervoy ) is approved
Nivolumab/Ipilimumab Combination Therapy for Renal Cell Carcinoma (RCC) An HCP Tool From the Immuno-Oncology Essentials Initiative The combination of nivolumab (Opdivo ) and ipilimumab (Yervoy ) is approved
Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP
 Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP") Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP Division of Medical Oncology and Hematology Bras Drug Development Program Princess Margaret Cancer Centre, Toronto,
Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP Division of Medical Oncology and Hematology Bras Drug Development Program Princess Margaret Cancer Centre, Toronto,
Nivolumab and Ipilimumab
 Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment
 Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Emily Borders, Pharm.D., M.S., BCOP Oncology Clinical Pharmacist Stephenson Cancer Center Faculty Disclosure Learning Objectives
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Emily Borders, Pharm.D., M.S., BCOP Oncology Clinical Pharmacist Stephenson Cancer Center Faculty Disclosure Learning Objectives
Pembrolizumab 200mg Monotherapy
 Pembrolizumab 200mg This regimen supercedes NCCP Regimen 00347 Pembrolizumab 2mg/kg as of September 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10 Regimen Code
Pembrolizumab 200mg This regimen supercedes NCCP Regimen 00347 Pembrolizumab 2mg/kg as of September 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10 Regimen Code
Non-Small Cell Lung Cancer Webinar. Thursday, September 13, p.m. EDT
 Non-Small Cell Lung Cancer Webinar Thursday, September 13, 2018 1 2 p.m. EDT 1 2 Webinar Faculty Julie R. Brahmer, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Patrick Forde, MD Johns
Non-Small Cell Lung Cancer Webinar Thursday, September 13, 2018 1 2 p.m. EDT 1 2 Webinar Faculty Julie R. Brahmer, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Patrick Forde, MD Johns
Nivolumab Monotherapy 240mg -14 days
 Nivolumab Monotherapy 240mg -14 days This regimen supercedes NCCP Regimen 00349 Nivolumab Monotherapy as of May 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10
Nivolumab Monotherapy 240mg -14 days This regimen supercedes NCCP Regimen 00349 Nivolumab Monotherapy as of May 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Atezolizumab Non-small cell lung cancer
 Systemic Anti Cancer Treatment Protocol Atezolizumab Non-small cell lung cancer PROTOCOL REF: MPHAATNSCLC (Version No: 1.0) Approved for use in: Locally advanced/metastatic non squamous or squamous non-small
Systemic Anti Cancer Treatment Protocol Atezolizumab Non-small cell lung cancer PROTOCOL REF: MPHAATNSCLC (Version No: 1.0) Approved for use in: Locally advanced/metastatic non squamous or squamous non-small
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Immune-Related Adverse Reaction (irar) Management Guide
 Management Guide") REGIMEN Immune-Related Adverse Reaction (irar) Management Guide OPDIVO as monotherapy is indicated for the treatment of locally advanced or metastatic squamous non-small cell lung cancer (NSCLC) with progression
REGIMEN Immune-Related Adverse Reaction (irar) Management Guide OPDIVO as monotherapy is indicated for the treatment of locally advanced or metastatic squamous non-small cell lung cancer (NSCLC) with progression
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Personalized Treatment Approaches for Lung Cancer
 Personalized Treatment Approaches for Lung Cancer California Thoracic Society 2018 Annual Carmel Conference January 27, 2018 Matthew Gubens, MD, MS Associate Professor of Medicine Chair, Thoracic Oncology
Personalized Treatment Approaches for Lung Cancer California Thoracic Society 2018 Annual Carmel Conference January 27, 2018 Matthew Gubens, MD, MS Associate Professor of Medicine Chair, Thoracic Oncology
7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Gastrointestinal Tract
 7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation.
7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation.
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Novel Therapies in Melanoma the Immunotherapy Approach
 2018 AAD Annual Meeting, San Diego, CA Novel Therapies in Melanoma the Immunotherapy Approach Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion & Melanoma Program Physician
2018 AAD Annual Meeting, San Diego, CA Novel Therapies in Melanoma the Immunotherapy Approach Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion & Melanoma Program Physician
KEYTRUDA is also indicated in combination with pemetrexed and platinum chemotherapy for the
 FDA-Approved Indication for KEYTRUDA (pembrolizumab) in Combination With Carboplatin and Either Paclitaxel or Nab-paclitaxel for the Firstline Treatment of Patients With Metastatic Squamous Non Small Cell
FDA-Approved Indication for KEYTRUDA (pembrolizumab) in Combination With Carboplatin and Either Paclitaxel or Nab-paclitaxel for the Firstline Treatment of Patients With Metastatic Squamous Non Small Cell
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management
 Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT YERVOY 5 mg/ml concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ml of concentrate contains
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT YERVOY 5 mg/ml concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ml of concentrate contains
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Dra. Omayra Reyes, MD. Hematologist- Oncologist. Introduction to Immuno Oncology
 Dra. Omayra Reyes, MD. Hematologist- Oncologist Introduction to Immuno Oncology Disclosure I have no conflicts of interest Objectives Review Basic concepts of onco- immunology. Recognize different mechanisms
Dra. Omayra Reyes, MD. Hematologist- Oncologist Introduction to Immuno Oncology Disclosure I have no conflicts of interest Objectives Review Basic concepts of onco- immunology. Recognize different mechanisms
Pharmacy Accreditation
 The Evolving Role of Specialty Pharmacists in Cancer Immunotherapy: New Pathways, Agents, Opportunities, and Challenges Patrick J. Medina, PharmD, BCOP Professor Department of Medicine Stephenson Cancer
The Evolving Role of Specialty Pharmacists in Cancer Immunotherapy: New Pathways, Agents, Opportunities, and Challenges Patrick J. Medina, PharmD, BCOP Professor Department of Medicine Stephenson Cancer
CRITICITÀ. Immunoterapia. Quadri clinici e gestione delle tossicità.
 Immunoterapia. Quadri clinici e gestione delle tossicità. CRITICITÀ Verona, 9 Aprile 2016 Daniela Iacono UOC Oncologia Medica Azienda Ospedaliera Sant Andrea Roma Immunotherapy : the new era in (N)SCLC
Immunoterapia. Quadri clinici e gestione delle tossicità. CRITICITÀ Verona, 9 Aprile 2016 Daniela Iacono UOC Oncologia Medica Azienda Ospedaliera Sant Andrea Roma Immunotherapy : the new era in (N)SCLC
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment
 Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Immunotherapy toxicities. Dr Fiona Taylor
 Immunotherapy toxicities Dr Fiona Taylor Outline Understand toxicities Anticipate toxicities Key steps to safely using and achieving the most benefits from immunotherapies for patients Manage toxicities
Immunotherapy toxicities Dr Fiona Taylor Outline Understand toxicities Anticipate toxicities Key steps to safely using and achieving the most benefits from immunotherapies for patients Manage toxicities
Toxicities of the anti-pd-1 and anti-pd-l1 immune checkpoint antibodies
 26: 2375 2391, 2015 doi:10.1093/annonc/mdv383 Published online 14 September 2015 Toxicities of the anti-pd-1 and anti-pd-l1 immune checkpoint antibodies J. Naidoo 1 *, D. B. Page 2,B.T.Li 3, L. C. Connell
26: 2375 2391, 2015 doi:10.1093/annonc/mdv383 Published online 14 September 2015 Toxicities of the anti-pd-1 and anti-pd-l1 immune checkpoint antibodies J. Naidoo 1 *, D. B. Page 2,B.T.Li 3, L. C. Connell
Rheumatology winter clinical symposium 9 th annual meeting Maui, Hawaii February
 New onset polyarthritis secondary to pembrolizumab [anti-pd1 antibody] in a patient with metastatic melanoma successfully treated with IL-6 receptor [IL-6R] inhibitor. Salvador R. Garcia1, MD; Adi Diab2,
New onset polyarthritis secondary to pembrolizumab [anti-pd1 antibody] in a patient with metastatic melanoma successfully treated with IL-6 receptor [IL-6R] inhibitor. Salvador R. Garcia1, MD; Adi Diab2,
How do weimplementimmunotherapyin routine practice? Lessons from the lung cancer experience
 How do weimplementimmunotherapyin routine practice? Lessons from the lung cancer experience Pr Alexis Cortot, M.D., Ph.D. Thoracic Oncology Department, CHRU Lille Institut of Biology, Lille TAO Paris,
How do weimplementimmunotherapyin routine practice? Lessons from the lung cancer experience Pr Alexis Cortot, M.D., Ph.D. Thoracic Oncology Department, CHRU Lille Institut of Biology, Lille TAO Paris,
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab
 BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab Protocol Code Tumour Group Contact Physician USMAVIPI Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab Protocol Code Tumour Group Contact Physician USMAVIPI Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
Immune-related adverse events with immune checkpoint inhibitors in thoracic malignancies: focusing on non-small cell lung cancer patients
 Review Article Immune-related adverse events with immune checkpoint inhibitors in thoracic malignancies: focusing on non-small cell lung cancer patients Jordi Remon 1, Laura Mezquita 2, Jesús Corral 3,
Review Article Immune-related adverse events with immune checkpoint inhibitors in thoracic malignancies: focusing on non-small cell lung cancer patients Jordi Remon 1, Laura Mezquita 2, Jesús Corral 3,
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD
 Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo
 U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo (nivolumab) in Patients with Previously Untreated Advanced Melanoma Application includes CheckMate -066,
U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo (nivolumab) in Patients with Previously Untreated Advanced Melanoma Application includes CheckMate -066,
Ipilimumab Monotherapy
 INDICATIONS FOR USE: Ipilimumab INDICATION ICD10 Regimen Code *Reimbursement Indicator Treatment of advanced (unresectable or metastatic) melanoma in adults C43 00105a ODMS *If a reimbursement indicator
INDICATIONS FOR USE: Ipilimumab INDICATION ICD10 Regimen Code *Reimbursement Indicator Treatment of advanced (unresectable or metastatic) melanoma in adults C43 00105a ODMS *If a reimbursement indicator
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
DOSING GUIDE. Indications. Important Safety Information. Enable the immune system. RECOGNIZE. RESPOND.
 DOSING GUIDE For patients with unresectable Stage III NSCLC following concurrent CRT For patients with locally advanced or metastatic UC previously treated with platinum-based therapy Enable the immune
DOSING GUIDE For patients with unresectable Stage III NSCLC following concurrent CRT For patients with locally advanced or metastatic UC previously treated with platinum-based therapy Enable the immune
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
Managing Adverse Events Associated with Immuno-oncologic Agents
 Managing Adverse Events Associated with Immuno-oncologic Agents Jennifer Diehl RN, BSN, OCN Cutaneous Oncology Program Moffitt Cancer Center Tampa, FL September 10, 2015 12-1 p.m. EST ICLIO ecourse 05
Managing Adverse Events Associated with Immuno-oncologic Agents Jennifer Diehl RN, BSN, OCN Cutaneous Oncology Program Moffitt Cancer Center Tampa, FL September 10, 2015 12-1 p.m. EST ICLIO ecourse 05
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS
 MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Cancer Immunotherapy
 Cancer Immunotherapy Early Recognition and Effective Management of Immune Related Adverse Events This slide deck in its original and unaltered format is for educational purposes and is current for the
Cancer Immunotherapy Early Recognition and Effective Management of Immune Related Adverse Events This slide deck in its original and unaltered format is for educational purposes and is current for the
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
7.5 Aseptic meningitis 7.6 Encephalitis 7.7 Transverse Myelitis
 MANAGEMENT OF IMMUNE-RELATED ADVERSE EVENTS IN PATIENTS TREATED WITH IMMUNE CHECKPOINT INHIBITOR THERAPY: AMERICAN SOCIETY OF CLINICAL ONCOLOGY CLINICAL PRACTICE GUIDELINE Toxicity Type Adverse Event Page
MANAGEMENT OF IMMUNE-RELATED ADVERSE EVENTS IN PATIENTS TREATED WITH IMMUNE CHECKPOINT INHIBITOR THERAPY: AMERICAN SOCIETY OF CLINICAL ONCOLOGY CLINICAL PRACTICE GUIDELINE Toxicity Type Adverse Event Page
Ipilimumab in Melanoma
 Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or