Pregnancy & Thyroid. Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University. Imam Reza weeky Conferance
|
|
|
- Penelope May
- 6 years ago
- Views:
Transcription
1 Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance
2 Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology & pregnancy Hypothyroidism & pregnancy Thyrotoxicosis & pregnancy Postpartum thyroid dysfunction
3 Thyroid adaptation during normal pregnancy Change in thyroid physiology Change in thyroid function tests
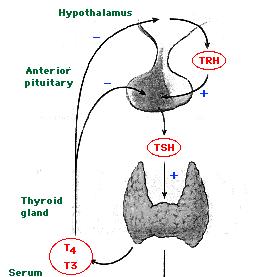
4 Thyroid physiology Increase in thyroxine binding globulin Stimulation of the TSH receptor by HCG
5
6
7 Thyroid Disease Spectrum Overt Hypothyroidism TSH >10 IU/mL, Free T 4 Low Subclinical Hypothyroidism TSH >2.5 IU/mL, Free T 4 Normal Euthyroid TSH IU/mL, Free T 4 Normal Hyperthyroidism TSH <0.2 IU/mL, Free T 3 /T 4 Normal or Elevated TSH, IU/mL.
8 Healthy pregnant women TSH = 0.03 to 0.1 mu/l
9 Trimester specific TSH First trimester Second Third 0.3-3
10 Hypothyroidism Overt Hypothyroidism elevated TSH, reduced free T4 Subclinical Hypothyroidism elevated TSH, normal free T4
11 Levothyroxine o.1 mg=100mcg Euthyrex 100 mcg, 50 mcg
12 Thyroid & Pregnancy: Hypothyroidism 85% will need increase in LT4 dose during pregnancy due to increased TBG levels (ave dose increase 48%) Risks: increased spont abort, HTN/preeclampsia, abruption, anemia, postpartum hemorrhage, preterm labour, baby SGA Fetal neuropsychological development (NEJM, 341(8): , Aug 31, 2001): Cognitive testing of children age 7-9 Untreated hyothyroid mothers vs. normal mothers: Average of 7 IQ points less in children Increased risk of IQ < 85 (19% vs. 5%) Retrospective study, data-dredging?
13 Thyroid peroxidase antibodies Anti TPO
14 LT4 dose adjustment in Pregnancy: - Optimize TSH preconception ( mu/l) - TSH at pregnancy diagnosis (~3-4 wk gestation), q1mos during 1 st 20 wks and after any LT4 dose change, q2mos 20 wks to term - Instruct women to take 2 extra thyroid pills/wk (q Mon, Thurs) for 29% dose increase once pregnancy suspected (+ commercial preg test) - If starting LT4 during preg: initial dose 2 ug/kg/d and recheck TSH q4wk until euthythyroid TSH Dose Adjustment TSH increased but < 10 Increase dose by 50 ug/d TSH TSH > 20 Increase dose by ug/d Increase dose by 100 ug/d
15 Goiter and Thyroid Nodules
16 Hyperthyroidism Overt Hyperthyroidism elevated free T4 and/ or free T3, Low TSH Subclinical Hyperthyroidism normal free T4, Low TSH
17 Thyrotoxicosis & Pregnancy Causes: Graves disease TMNG, toxic adenoma Thyroiditis Hydatiform mole Gestational hcg-asscociated Thyrotoxicosis Hyperemesis gravidarum hcg 60% TSH, 50% FT4 Resolves by 20 wks gestation Only Rx with ATD if persists > 20 wk
18 Graves Disease hcg-mediated (gestational transient thyrotoxicosis )
19 Indication for treatment Therapeutic options Goals of antithyroid drug therapy
20 Thyroid & Pregnancy: Normal Physiology Fetal thyroid starts working at wks T4 & T3 cross placenta but do so minimally Cross placenta well: MTZ > PTU TSH-R Ab (stim or block) ATD (PTU & MTZ): Fetal goitre (can compress trachea after birth) MTZ aplasia cutis scalp defects Other MTZ reported embryopathy: choanal atresia, esophageal atresia, tracheo-esophageal fistula Therefore do NOT use MTZ during pregnancy, use PTU instead
21 A good fetal outcome: Free T4 high normal range Lowest drug dose
22 Propylthiouracil ( PTU ) Methimazole Beta blockers
23 Dose and Monitoring T4 ( total ) mcg/dl TSH low normal
24 TSH High FT4 Low FT4 & FT3 High Low Low High 2 thyrotoxicosis Endo consult FT3, rt3 MRI, α-su 1 Hypothyroid If equivocal Central Hypothyroid TRH Stim. MRI, etc. 1 Thyrotoxicosis RAIU
25 Thyroid & Pregnancy: Normal Physiology Increased estrogen increased TBG (peaks wk 15-20) Higher total T4 & T3: normal FT4 & FT3 if normal thyroid fn. and good assay many automated FT4 assays underestimate true FT4 level (except Nichols equilibrium dialysis free T4 assay) if suspect your local FT4 assay is underestimating FT4 can check total T4 & T3 instead (normal pregnant range ~ 1.5x nonpregnant) hcg peak end of 1 st trimester, hcg has weak TSH agonist effect so may cause: slight goitre mild TSH suppression ( mu/l) in 9% of preg mild FT4 rise in 14% of preg
26 No TSH & FTI at end of 1 st trimester as expected from hcg effect Requirement to increase LT4 dose occurred between weeks 4-20 Despite exponential rise in estradiol throughout pregnancy (note y-axis units) TBG levels plateau at 20 wks

27 LT4 dose requirement tied to rising TBG levels (THBI inversely proportional to TBG level) By 10 wks need average increase of 29% LT4 dose By 20 wks need average increase of 48% LT4 dose No increase of dose beyond 20 wks required
, before 1 st prenatal")
28 * Regardless of cause of hypothyroidism (Hashimoto s, thyroidectomy) initial LT4 dose increase is usually required early (~ week 8), before 1 st prenatal visit!
29 Pregnancy: screen for thyroid dysfn? Universal screening not currently recommended: ACOG, AACE, Endo Society, ATA Controversial! Definitely screen: Goitre, FHx thyroid dysfn., prior postpartum thyroiditis, T1DM Ideally, check TSH preconception: mu/l: recheck TSH during 1 st trimester mu/l: do not need to recheck during preg If TSH not done preconception do at earliest prenatal visit: mu/l: hcg effect (9% preg), recheck in 5wk < 0.1 mu/l: recheck immediately with FT4, FT3, T4, T3
30 Thyrotoxicosis & Pregnancy Risks: Maternal: stillbirth, preterm labor, preeclampsia, CHF, thyroid storm during labor Fetal: SGA, possibly congenital malformation (if 1 st trimester thyrotoxicosis), fetal tachycardia, hydrops fetalis, neonatal thyrotoxicosis
31 Thyrotoxicosis & Pregnancy Diagnosis difficult: hcg effect: Suppressed TSH (9%) +/- FT4 (14%) until 12 wks Enhanced if hyperemesis gravidarum: 50-60% with abnormal TSH & FT4, duration to 20 wks FT4 assays reading falsely low T4 elevated due to TBG (1.5x normal) NO RADIOIODINE Measure: TSH, FT4, FT3, T4, T3, thyroid antibodies? Examine: goitre? orbitopathy? pretibial myxedema?
32 Pregnant & Suppressed TSH TSH < 0.1 TSH FT4, FT3, T4, T3 Thyroid Ab s Examine Still suppressed Recheck in 5 wks Normalizes Hyperemesis Gravidarum Very High TFT s: TSH undetectable very high free/total T4/T3 hyperthyroid symptoms no hyperemesis TSH-R ab + orbitopathy goitre, nodule/tmng pretibial myxedema Don t treat with PTU Abnormal TFT s past 20 wk Treat Hyperthyroidism (PTU)
33
34 Case 1 31 year old female G2P1A0, 11 weeks pregnant Well except fatigue Hb 108, ferritin 7 (Fe and LT4 interaction?) TSH 0.2 mu/l, FT4 7 pm Started on LT TSH < 0.01 mu/l FT4 12 pm, FT3 2.1 pm
35 Thyrotoxicosis & Pregnancy: Rx No RAI ever (destroy fetal thyroid) PTU Start 100 mg tid, titrate to lowest possible dose Monitor qmos on Rx: T4, T3, FT4, FT3 TSH less useful (lags, hcg suppression) Aim for high-normal to slightly elevated hormone levels T nm, T nm, FT pm 3 rd trimester: titrate PTU down & d/c prior to delivery if TFT s permit to minimize risk of fetal goitre Consider fetal U/S wk to R/O fetal goitre If allergy/neutropenia on PTU: 2 nd trimester thyroidectomy
36 Thyrotoxicosis & Lactation ATD generally don t get into breast milk unless at higher doses: PTU > mg/d MTZ > 20 mg/d Generally safe I prefer PTU > MTZ for preg lactating Take ATD dose just after breast-feeding Should provide 3-4h interval before lactates again
37 Neonatal Grave s Rare, 1% infants born to Graves moms 2 types: Transplacental trnsfr of TSH-R ab (IgG) Present at birth, self-limited Rx PTU, Lugol s, propanolol, prednisone Prevention: TSI in mom 2 nd trimester, if 5X normal then Rx mom with PTU (crosses placenta to protect fetus) even if mom is euthyroid (can give mom LT4 which won t cross placenta) Child develops own TSH-R ab Strong family hx of Grave s 3-6 mos 20% mortality, persistant brain dysfunction
38
39 Postpartum & Thyroid 5% (3-16%) postpartum women (25% T1DM) Up to 1 year postpartum (most 1-4 months) Lymphocytic infiltration (Hashimoto s) Postpartum Exacerbation of all autoimmune dx 25-50% persistant hypothyroidism Small, diffuse, nontender goitre Transiently thyrotoxic Hypothyroid
40
41 Postpartum & Thyroid Distinguish Thyrotoxic phase from Grave s: Rx: No Eye disease, pretibial myxedema Less severe thyrotoxic, transient (repeat thyroid fn 2-3 mos) RAI (if not breast-feeding) Hyperthyroid symptoms: atenolol mg od Hypothyroid symptoms: LT ug/d to start Adjust LT4 dose for symtoms and normalization TSH Consider withdrawal at 6-9 months (25-50% persistent hypothyroid, hi-risk recur future preg)
42 Postpartum & Thyroid Postpartum depression When studied, no association between postpartum depression/thyroiditis Overlapping symtoms, R/O thyroid before start antidepressents Screening for Postpartum Thyroiditis HOW: TSH q3mos from 1 mos to 1 year postpartum? WHO: Symptoms of thyroid dysfn. Goitre T1DM Postpartum thyroiditis with prior pregnancy
The Thyroid and Pregnancy OUTLINE OF DISCUSSION 3/19/10. Francis S. Greenspan March 19, Normal Physiology. 2.
 The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
Thyroid Disease in Pregnancy. Justin Moore, MD
 Thyroid Disease in Pregnancy Justin Moore, MD Case 1 22 yr old G1P0 female at 14 2/7 weeks presents with tremor Weight stable since first positive pregnancy test Some nausea, rare vomiting TSH 0.02 miu/l,
Thyroid Disease in Pregnancy Justin Moore, MD Case 1 22 yr old G1P0 female at 14 2/7 weeks presents with tremor Weight stable since first positive pregnancy test Some nausea, rare vomiting TSH 0.02 miu/l,
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy
 Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy Early diagnosis and good management of maternal thyroid dysfunction are essential to ensure minimal adverse effects on
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy Early diagnosis and good management of maternal thyroid dysfunction are essential to ensure minimal adverse effects on
Hyperthyroidism and Hypothyroidism in Pregnancy Guideline
 Aneurin Bevan University Health Board Hyperthyroidism and Hypothyroidism in Pregnancy Guideline N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed
Aneurin Bevan University Health Board Hyperthyroidism and Hypothyroidism in Pregnancy Guideline N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy.
 Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy. Early diagnosis and good management of maternal thyroid dysfunction is essential to ensure minimal adverse effects on
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy. Early diagnosis and good management of maternal thyroid dysfunction is essential to ensure minimal adverse effects on
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Review Article Management of Hyperthyroidism in Pregnancy: Comparison of Recommendations of American Thyroid Association and Endocrine Society
 Thyroid Research Volume 2013, Article ID 878467, 6 pages http://dx.doi.org/10.1155/2013/878467 Review Article Management of Hyperthyroidism in Pregnancy: Comparison of of American Thyroid Association and
Thyroid Research Volume 2013, Article ID 878467, 6 pages http://dx.doi.org/10.1155/2013/878467 Review Article Management of Hyperthyroidism in Pregnancy: Comparison of of American Thyroid Association and
THYROID DISEASE IN PREGNANCY
 THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Hypothyroidism in pregnancy. Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah
 Hypothyroidism in pregnancy Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah Agenda 1. Epidemiology and clinical characteristics of maternal hypothyroidism 2. Prevention and
Hypothyroidism in pregnancy Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah Agenda 1. Epidemiology and clinical characteristics of maternal hypothyroidism 2. Prevention and
Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, :30 PM
 Thyroxine Deficiency in Pregnancy Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, 2006 1:30 PM WHI Estrogen recap In http://courses.washington.edu/bonephys/opestrogen.html. from:
Thyroxine Deficiency in Pregnancy Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, 2006 1:30 PM WHI Estrogen recap In http://courses.washington.edu/bonephys/opestrogen.html. from:
Screening Babies at risk of Congenital Hyperthyroidism GL354
 1 Screening Babies at risk of Congenital Hyperthyroidism GL354 Approval and Authorisation Approved by Job Title Date Paediatric Clinical Governance Chair of paediatric Clinical Governance March 2016 Change
1 Screening Babies at risk of Congenital Hyperthyroidism GL354 Approval and Authorisation Approved by Job Title Date Paediatric Clinical Governance Chair of paediatric Clinical Governance March 2016 Change
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Update on Gestational Thyroid Disease. Aidan McElduff The Discipline of Medicine, The University of Sydney
 IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015
 NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015 CHIEF COMPLAINT 35 6/7 week F with goiter, born to a mother with Graves disease (GD) HPI 35 6/7 week F born
NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015 CHIEF COMPLAINT 35 6/7 week F with goiter, born to a mother with Graves disease (GD) HPI 35 6/7 week F born
Objectives. Medical Complications of Pregnancy. Potential Conflicts: None. Common Complicating Medical Conditions that Precede Pregnancy
 Medical Complications of Potential Conflicts: None Ellen W. Seely, M.D. Director of Clinical Research Endocrine-Hypertension Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Medical Complications of Potential Conflicts: None Ellen W. Seely, M.D. Director of Clinical Research Endocrine-Hypertension Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Hyperthyroïdie et Grossesse
 Club Thyroïde, Paris 9 juin 2018 Hyperthyroïdie et Grossesse De la Mère à l Enfant Professeur Juliane Léger Endocrinologie diabétologie Pédiatrique Centre de Référence des Maladies Endocriniennes de la
Club Thyroïde, Paris 9 juin 2018 Hyperthyroïdie et Grossesse De la Mère à l Enfant Professeur Juliane Léger Endocrinologie diabétologie Pédiatrique Centre de Référence des Maladies Endocriniennes de la
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Hyperthyroidism: Guidelines and Beyond. Douglas S Ross MD May Copyrighted slides omitted
 Hyperthyroidism: Guidelines and Beyond Douglas S Ross MD May 19 2018 Copyrighted slides omitted Abbott Laboratories Quest Diagnostics Disclosures Diagnosis Biochemical Assessment Biotin Interference Biotinylated
Hyperthyroidism: Guidelines and Beyond Douglas S Ross MD May 19 2018 Copyrighted slides omitted Abbott Laboratories Quest Diagnostics Disclosures Diagnosis Biochemical Assessment Biotin Interference Biotinylated
Thyroid Disease in Pregnancy: The Essentials. Elizabeth N. Pearce, MD, MSc
 Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
Case 1: 24 yo pregnant female presenting with abnormal TFTs and tachycardia RAJESH JAIN ENDORAMA 3/16/2017
 Case 1: 24 yo pregnant female presenting with abnormal TFTs and tachycardia RAJESH JAIN ENDORAMA 3/16/2017 Chief Complaint The ER calls about a 24 year old, 12 weeks pregnant. She presented with tachycardia
Case 1: 24 yo pregnant female presenting with abnormal TFTs and tachycardia RAJESH JAIN ENDORAMA 3/16/2017 Chief Complaint The ER calls about a 24 year old, 12 weeks pregnant. She presented with tachycardia
HYPOTHYROIDISM AND HYPERTHYROIDISM
 HYPOTHYROIDISM AND HYPERTHYROIDISM SHAHIDA PERVEEN, AMBREEN Post RN BSCN Semester II FACULTY SIR RAJA April 13, 016 Objectives: State the functions of thyroid hormone. Understand the pathologic mechanism
HYPOTHYROIDISM AND HYPERTHYROIDISM SHAHIDA PERVEEN, AMBREEN Post RN BSCN Semester II FACULTY SIR RAJA April 13, 016 Objectives: State the functions of thyroid hormone. Understand the pathologic mechanism
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Southern Derbyshire Shared Care Pathology Guidelines. Hyperthyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Thyroid gland defects. Dr. Tara Husain
 Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
How to manage hypothyroid disease in pregnancy
 For mass reproduction, content licensing and permissions contact Dowden Health Media. FIRST OF 2 PARTS How to manage hypothyroid disease in pregnancy Pregnancy complicated by hypothyroidism puts mother
For mass reproduction, content licensing and permissions contact Dowden Health Media. FIRST OF 2 PARTS How to manage hypothyroid disease in pregnancy Pregnancy complicated by hypothyroidism puts mother
Management of thyroid diseases in pregnancy
 34 Review Management of thyroid diseases in pregnancy 1 2010; 32: 34-38 Introduction Thyroid dysfunction is a common medical problem in pregnancy. Early recognition and optimal management leads to better
34 Review Management of thyroid diseases in pregnancy 1 2010; 32: 34-38 Introduction Thyroid dysfunction is a common medical problem in pregnancy. Early recognition and optimal management leads to better
4) Thyroid Gland Defects - Dr. Tara
 Thyroid Gland Defects - Dr. Tara") 4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Thyroid Function. Thyroid Antibodies. Analyte Information
 Thyroid Function Thyroid Antibodies Analyte Information - 1-2013-04-30 Thyroid Antibodies Determination of thyroid autoantibodies are, besides TSH and FT4, one of the most important diagnostic parameters.
Thyroid Function Thyroid Antibodies Analyte Information - 1-2013-04-30 Thyroid Antibodies Determination of thyroid autoantibodies are, besides TSH and FT4, one of the most important diagnostic parameters.
1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago. OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron
 urine pregnancy; sent home with iron") Anila Bindal, MD 1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron UCMC ER: abdomen doubled overnight, significant vaginal bleeding,
Anila Bindal, MD 1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron UCMC ER: abdomen doubled overnight, significant vaginal bleeding,
The Presence of Thyroid Autoantibodies in Pregnancy
 The Presence of Thyroid Autoantibodies in Pregnancy Dr. O Sullivan does not have any financial relationships with any commercial interests. KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY ENDORAMA
The Presence of Thyroid Autoantibodies in Pregnancy Dr. O Sullivan does not have any financial relationships with any commercial interests. KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY ENDORAMA
Hypothyroidism. Definition:
 Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
344 Thyroid Disorders
 344 Thyroid Disorders Definition/Cut-Off Value Thyroid dysfunctions that occur in pregnant and postpartum women, during fetal development, and in childhood are caused by the abnormal secretion of thyroid
344 Thyroid Disorders Definition/Cut-Off Value Thyroid dysfunctions that occur in pregnant and postpartum women, during fetal development, and in childhood are caused by the abnormal secretion of thyroid
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
Grave s disease (1 0 )
") THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
Review Article Think Thyroid - Think Life: Pregnancy with Thyroid Disorders
 Chettinad Health City Medical Journal Muthukumaran Jayapaul* Consultant Endocrinologist, Arka Center for Hormonal Health, Chennai, India Dr. Muthu Kumaran Jayapaul is a Consultant Endocrinologist and also
Chettinad Health City Medical Journal Muthukumaran Jayapaul* Consultant Endocrinologist, Arka Center for Hormonal Health, Chennai, India Dr. Muthu Kumaran Jayapaul is a Consultant Endocrinologist and also
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS
 LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
DAGNOSIS AND TREATMENT OF THYROID GLAND DISEASES IN PREGNANCY GUIDELINE AND RECOMMENDATIONS
 Svetlana Spremovic-Radjenovic 1 DAGNOSIS AND TREATMENT OF THYROID GLAND DISEASES IN PREGNANCY GUIDELINE AND RECOMMENDATIONS The field referred to thyroid gland diseases and pregnancy has recorded the fast
Svetlana Spremovic-Radjenovic 1 DAGNOSIS AND TREATMENT OF THYROID GLAND DISEASES IN PREGNANCY GUIDELINE AND RECOMMENDATIONS The field referred to thyroid gland diseases and pregnancy has recorded the fast
Common Causes of Hypothyroidism
 Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Should every pregnant woman be screened for thyroid disease?
 Should every pregnant woman be screened for thyroid disease? Tal Biron-Shental Rinat Gabbay-Benziv Is there a debate? Thyroid screening Guidelines Targeted case finding criteria Age > 30 years Personal
Should every pregnant woman be screened for thyroid disease? Tal Biron-Shental Rinat Gabbay-Benziv Is there a debate? Thyroid screening Guidelines Targeted case finding criteria Age > 30 years Personal
Thyroid Disease & Pregnancy Updates and Ongoing Questions
 Thyroid Disease & Pregnancy - 2018 Updates and Ongoing Questions Erik K. Alexander, MD Chief, Thyroid Section, Division of Endocrinology Brigham & Women s Hospital Professor of Medicine, Harvard Medical
Thyroid Disease & Pregnancy - 2018 Updates and Ongoing Questions Erik K. Alexander, MD Chief, Thyroid Section, Division of Endocrinology Brigham & Women s Hospital Professor of Medicine, Harvard Medical
Understanding thyroid function tests. Dr. Colette George
 Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Canadian Endocrine Review Course 2014
 Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Tapazole Methimazole Tablets, USP DESCRIPTION
 Tapazole Methimazole Tablets, USP DESCRIPTION TAPAZOLE (Methimazole Tablets, USP) (1-methylimidazole-2-thiol) is a white, crystalline substance that is freely soluble in water. It differs chemically from
Tapazole Methimazole Tablets, USP DESCRIPTION TAPAZOLE (Methimazole Tablets, USP) (1-methylimidazole-2-thiol) is a white, crystalline substance that is freely soluble in water. It differs chemically from
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
INFANT OF A MOTHER WITH GRAVES DISEASE. Endorama May 14 th, 2015 Carmen Mironovici, M.D.
 INFANT OF A MOTHER WITH GRAVES DISEASE Endorama May 14 th, 2015 Carmen Mironovici, M.D. Chief Complaint Newborn born to a mother with autoimmune hyperthyroidism HPI Male infant born at 39w 2d gestation
INFANT OF A MOTHER WITH GRAVES DISEASE Endorama May 14 th, 2015 Carmen Mironovici, M.D. Chief Complaint Newborn born to a mother with autoimmune hyperthyroidism HPI Male infant born at 39w 2d gestation
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG
 THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG What is the difference between thyrotoxicosis and hyperthyroidism Thyrotoxicosis Thyrotoxicosis is defined as the state of thyroid hormone excess and is
THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG What is the difference between thyrotoxicosis and hyperthyroidism Thyrotoxicosis Thyrotoxicosis is defined as the state of thyroid hormone excess and is
Thyroid function in pregnancy
 Published Online December 23, 2010 Thyroid function in pregnancy John H. Lazarus * Centre for Endocrine and Diabetes Sciences, Cardiff University School of Medicine, University Hospital of Wales, Heath
Published Online December 23, 2010 Thyroid function in pregnancy John H. Lazarus * Centre for Endocrine and Diabetes Sciences, Cardiff University School of Medicine, University Hospital of Wales, Heath
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Thyroid. Dr Jessica Triay November 2018
 Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Pearls and Pitfalls of Thyroid Diagnosis. Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS
 Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
PRACTICE BULLETIN ACOG
 ACOG PRACTICE BULLETIN CLINICAL MANAGEMENT GUIDELINES FOR OBSTETRICIAN GYNECOLOGISTS NUMBER 37, AUGUST 2002 (Replaces Practice Bulletin Number 32, November 2001) This Practice Bulletin was developed by
ACOG PRACTICE BULLETIN CLINICAL MANAGEMENT GUIDELINES FOR OBSTETRICIAN GYNECOLOGISTS NUMBER 37, AUGUST 2002 (Replaces Practice Bulletin Number 32, November 2001) This Practice Bulletin was developed by
Thyroid Dysfunction during Pregnancy: A Review of the Current Guidelines
 , pp: 130-136 (ISSN: 2455-1716) Impact Factor 2.4 MARCH-2016 Review Article (Open access) Thyroid Dysfunction during Pregnancy: A Review of the Current Guidelines Mustafa Al Abousi* Department of Endocrinology,
, pp: 130-136 (ISSN: 2455-1716) Impact Factor 2.4 MARCH-2016 Review Article (Open access) Thyroid Dysfunction during Pregnancy: A Review of the Current Guidelines Mustafa Al Abousi* Department of Endocrinology,
Thyroid Disorders. Hypothyroidism. Low Total T4 Antiseizure meds Glucocorticoids. Free T4. Howard J. Sachs, MD.
 Thyroid Disorders Free T4 Low Total T4 Antiseizure meds Glucocorticoids Hypothyroidism Howard J. Sachs, MD www.12daysinmarch.com Primary Hypothyroidism High TSH Low free T4 Primary = End organ failure
Thyroid Disorders Free T4 Low Total T4 Antiseizure meds Glucocorticoids Hypothyroidism Howard J. Sachs, MD www.12daysinmarch.com Primary Hypothyroidism High TSH Low free T4 Primary = End organ failure
Nausea & Vomiting in Pregnancy. Ashley Robbins, MD, FACOG Associate Clinical Professor, KUSM-W
 Nausea & Vomiting in Pregnancy Ashley Robbins, MD, FACOG Associate Clinical Professor, KUSM-W Nausea and Vomiting in Pregnancy Prevalence of nausea in pregnancy 50-80% Prevalence of vomiting and retching
Nausea & Vomiting in Pregnancy Ashley Robbins, MD, FACOG Associate Clinical Professor, KUSM-W Nausea and Vomiting in Pregnancy Prevalence of nausea in pregnancy 50-80% Prevalence of vomiting and retching
Dianne S Cheung, MD FACE Assistant Clinical Professor UCLA Health David Geffen School of Medicine CA-AACE Chapter Secretary
 Dianne S Cheung, MD FACE Assistant Clinical Professor UCLA Health David Geffen School of Medicine CA-AACE Chapter Secretary No Financial Disclosures Objectives Which thyroid labs to order and interpret?
Dianne S Cheung, MD FACE Assistant Clinical Professor UCLA Health David Geffen School of Medicine CA-AACE Chapter Secretary No Financial Disclosures Objectives Which thyroid labs to order and interpret?
GOITER and Shortness of Breath. Case A: GOITER. Learning Objectives. Common Thyroid Disorders for
 2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
Requesting and Management of abnormal TFTs.
 Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
HYPOTHYROIDISM IN CHILDREN. IAP UG Teaching slides
 HYPOTHYROIDISM IN CHILDREN 1 OBJECTIVES Introduction Congenital hypothyroidism Etiology, clinical features, diagnosis, approach, treatment and prognosis Acquired hypothyroidism Etiology, clinical features,
HYPOTHYROIDISM IN CHILDREN 1 OBJECTIVES Introduction Congenital hypothyroidism Etiology, clinical features, diagnosis, approach, treatment and prognosis Acquired hypothyroidism Etiology, clinical features,
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
 Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
JMSCR Vol 05 Issue 11 Page November 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.98 Effect of Overt and Subclinical Hypothyroidism
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.98 Effect of Overt and Subclinical Hypothyroidism
Clinical Guideline MANAGEMENT OF INFANTS BORN TO MOTHERS WITH GRAVES DISEASE AND AT RISK OF THYROTOXICOSIS
 Clinical Guideline MANAGEMENT OF INFANTS BORN TO MOTHERS WITH GRAVES DISEASE AND AT RISK OF THYROTOXICOSIS Date of First Issue 18/07/2016 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline MANAGEMENT OF INFANTS BORN TO MOTHERS WITH GRAVES DISEASE AND AT RISK OF THYROTOXICOSIS Date of First Issue 18/07/2016 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Hypothyroidism and Hyperthyroidism. Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018
 Hypothyroidism and Hyperthyroidism Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018 Disclosures: None related to this program or presentation Objectives: Hypothyroidism
Hypothyroidism and Hyperthyroidism Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018 Disclosures: None related to this program or presentation Objectives: Hypothyroidism
Pitfalls of TFTs Interpretation
 Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan
 HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
DRUGS. 4- Two molecules of DIT combine within the thyroglobulinto form L-thyroxine (T4)' One molecule of MIT & one molecule of DIT combine to form T3
' One molecule of MIT & one molecule of DIT combine to form T3") THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
Mastering Thyroid Disorders. Douglas C. Bauer, MD UCSF Division of General Internal Medicine
 Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Neonatal Thyrotoxicosis Management of babies born to mothers with a history of hyperthyroidism (Grave s Disease)
") MCN for Neonatology West of Scotland Neonatal Guideline Neonatal Thyrotoxicosis Management of babies born to mothers with a history of hyperthyroidism (Grave s Disease) This document is applicable to all
MCN for Neonatology West of Scotland Neonatal Guideline Neonatal Thyrotoxicosis Management of babies born to mothers with a history of hyperthyroidism (Grave s Disease) This document is applicable to all
Thyroid Management. Evolving Controversy - Science, Dogma, Opinion. The Ogden Surgical Medical Society May 2016
 Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Endocrinology in Primary Care. HN Buch
 Endocrinology in Primary Care HN Buch Endocrinology in Primary Care Death by Powerpoint HN Buch Agenda Endocrine Condition Primary v Secondary Care Initial management Follow up Focus of Discussion Hypothyroidism
Endocrinology in Primary Care HN Buch Endocrinology in Primary Care Death by Powerpoint HN Buch Agenda Endocrine Condition Primary v Secondary Care Initial management Follow up Focus of Discussion Hypothyroidism
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
Understanding the Thyroid and Pregnancy
 FERTILITY nurses first Understanding the Thyroid and Pregnancy Tamara Tobias, ARNP Human chorionic gonadotropin (hcg) and estrogen are two hormones that play an important role during pregnancy. They can,
FERTILITY nurses first Understanding the Thyroid and Pregnancy Tamara Tobias, ARNP Human chorionic gonadotropin (hcg) and estrogen are two hormones that play an important role during pregnancy. They can,
Hyperthyroidism, Inflammatory Disorders
 Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
THYROID DISEASE AND TESTING. Jack L. Snitzer, D.O., FACOI, FACE, CCD
 THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY
 THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
Page 1. Understanding Common Thyroid Disorders. Cases. Topics Covered
 Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
NEO SUMMIT. NEO Summit
 NEO Summit 2 nd April 2016, Puri, Orissa "Neo Summit was held at Upper Hotel Holiday Resort, Chakratirtha Road, Puri-752 002, Orissa, India. It was organized by of Asian Society of Continuing Medical Education.
NEO Summit 2 nd April 2016, Puri, Orissa "Neo Summit was held at Upper Hotel Holiday Resort, Chakratirtha Road, Puri-752 002, Orissa, India. It was organized by of Asian Society of Continuing Medical Education.
Slide notes: This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications,
 1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
Thyroid Function TSH Analyte Information
 Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
03-Dec-17. Thyroid Disorders GOITRE. Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms
 Thyroid Disorders GOITRE Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms 1 Physiological Goiter load on thyroid supply of I - limited stress due to:
Thyroid Disorders GOITRE Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms 1 Physiological Goiter load on thyroid supply of I - limited stress due to:
Management of Common Thyroid Disorders
 Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Thyroid Diseases. Q1: The most common thyroid function disorder is? Q2: The most sensitive test for thyroid function is?
 Thyroid Diseases Scott Urquhart, PA-C Clinical Instruct., George Washington Univ. PA Program Adjunct Clinical Prof., James Madison Univ. PA Program Diabetes and Thyroid Associates. Fredericksburg, Virginia
Thyroid Diseases Scott Urquhart, PA-C Clinical Instruct., George Washington Univ. PA Program Adjunct Clinical Prof., James Madison Univ. PA Program Diabetes and Thyroid Associates. Fredericksburg, Virginia
Screening and subsequent management for thyroid dysfunction pre-pregnancy and during pregnancy for improving maternal and infant health(review)
") Cochrane Database of Systematic Reviews Screening and subsequent management for thyroid dysfunction pre-pregnancy and during pregnancy for improving maternal and infant health(review) SpencerL,BubnerT,BainE,MiddletonP
Cochrane Database of Systematic Reviews Screening and subsequent management for thyroid dysfunction pre-pregnancy and during pregnancy for improving maternal and infant health(review) SpencerL,BubnerT,BainE,MiddletonP