Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
|
|
|
- Joan Booker
- 6 years ago
- Views:
Transcription

1 Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
2 No disclosures
3 Objectives To have an understanding of hyperthyroidism To have an understanding of the management of thyroid nodules To appreciate the effects amiodarone can have on the thyroid
4 A Case 46 yo female felt well until 3-4 months ago, when she developed heat intolerance, new anxiety, palpitations, mild dyspnea on exertion, and oligomenorrhea which she ascribed to being perimenopausal for several months Saw her internist when the anxiety and palpitations were keeping her awake at night, who ordered TFT s
5 Case #1 TSH <0.015 uiu/ml Free T4 5.1 ng/dl ( ) Free T pg/ml ( ) Referred to endocrinologist

6 Relationship between TSH and thyroid hormones Small changes in T4/T3 result in large changes in TSH ATA and AACE guidelines recommend checking all three if pre-test probability is high TSH that is completely suppressed is diagnostic of hyperthyroidism Only cases missed by just doing TSH: TSH-producing pituitary adenoma and thyroid hormone resistance
7 Our Patient s Physical Exam Exam: Thin, anxious appearing, Pulse 112 regular, BP 118/56. Skin warm, no eye signs, thyroid gland twice normal size (about 30 grams) firm texture with right side slightly larger than left, no thyroid bruit, mild weakness of hip flexors and shoulders, fine tremor of hands and tongue
 Gritty")

8 Eye signs 30% of patients with Graves show some signs of ophthalmopathy Exophthalmos (bulging eyes) Gritty sensation/redness Pressure/pain in eyes Puffy eyelids Light sensitivity Double vision Stare/lid lag with any thyrotoxic state
9 What is the Likeliest Diagnosis? Causes 10% 3% Graves 4% 1% 7% 75% Silent Thyroiditis Single Nodule Subacute Thyroiditis Multiple Nodules Other Adapted from slide from Peter Singer, MD
10 Hyperthyroidism in the Elderly vs. the Young Signs/Sx Age >70 Age <50 P-value Fatigue 56% 84% 0.01 Weight loss 50% 51% NS Tremor 44% 84% Anorexia 32% 4% Increased appetite 0% 57% Confusion 16% 0% Heat intolerance 15% 92% Nervousness 31% 84% J Am Geriatr Soc 44:50 53, 1996
11 Causes of Thyrotoxicosis Elevated RAIU Graves Toxic multinodular goiter Toxic adenoma TSH secreting pituitary tumor Hydatidaform mole Choriocarcinoma Suppressed RAIU Subacute thyroiditis Silent/painless thyroiditis Iodine induced thyrotoxicosis Radiation thyroiditis Exogeneous T4 or T3 Metastatic follicular thyroid cancer Struma ovarii
12 Role of Other Blood Tests in Diagnosis Ratio of Total T3:Total T4 Relatively more T3 is synthesized in hyperactive gland, so ratio is >20 in GD and TMNG and <20 in painless thyroiditis TSH-receptor antibodies (TRAb) and thyroid stimulating immunoglobulin (TSI) Thyroglobulin released along with thyroid hormone in all thyroiditis whereas release is suppressed in exogenous thyroid hormone administration
13 Role of Ultrasound in Diagnosis Guidelines suggest that ultrasound does not play a role in diagnosis However, most endocrinologists do them to stratify patients as to whether they have nodules that could be culprit RAIU Looking at vascularity that might suggest Graves Overall appearance of thyroid

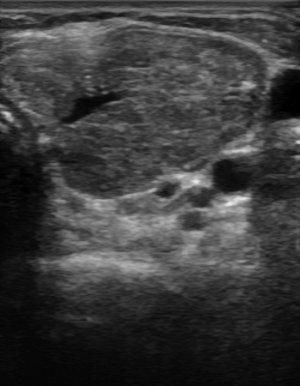
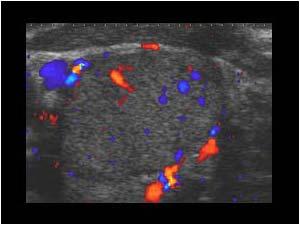
14 Our patient s ultrasound
15 Further imaging to help define cause Radioiodine uptake and scan should be done if clinical presentation is not consistent with Graves or there are nodules Uptake alone to get number to plan radioiodine dose Graves does not cause nodules!


16 Our Patient s Uptake and Scan
17 Thyroid Nodules Thyroid nodules in patients with Graves disease should be managed per 2009 ATA Guidelines Thyroid cancer occurs in Graves disease with a frequency of 2% or less Solid nodules larger than 1 cm should be evaluated by UGFNAB Smaller nodules should be evaluated if patient is a high risk patient (FH of thyroid cancer in 1 st degree relative, h/o XRT as child, PET positive nodules, MEN syndromes/fmtc)


18 Ultrasonographic features associated with increased risk of malignancy Hypoechoic Irregular borders Increased chaotic vascular flow Microcalcifications Nodule with tall, narrow shape



19 Ultrasonographic features associated with decreased risk of malignancy Hyperechoic Large coarse/eggshell calcifications Peripheral vascularity Spongiform appearance Comet-tail shadowing Pure cyst Halo
20 Cold nodules vs. toxic adenoma Toxic adenomas are almost never cancer and biopsy is not necessary Cold nodules carry a risk of cancer of 5% (95% of thyroid nodules are cold) Ultrasound-guided FNAB is recommended for: cold nodules that would meet criteria for FNAB in the setting of toxic MNG nodules occurring in the setting of Graves if meet criteria
21 Benign nodule Ultrasound-guided FNAB was performed of the nodule and it was benign Recommended followup for benign nodules Follow with serial US exam 6-18 months after initial FNA (due to false negative rate of up to 5% with FNAB) If size is stable (no more than 50% change in volume, or <20% increase in at least 2 dimensions) interval can be increased to 3-5 years Significant growth should prompt re-biopsy No role for TSH suppression with levothyroxine in iodine sufficient populations
22 Therapy for Hyperthyroidism B-blockers Thionamides Radioiodine ablation Thyroidectomy
23 Beta-Blockers Should be used initially in all patients with hyperthyroidism unless contraindications exist Block b-adrenergic activity responsible for palpitations, tremor, anxiety and heat intolerance Propranolol Atenolol/Metoprolol

24 Thionamides Methimazole mg daily PTU 100 mg three times/day Mild disease may require less FDA issued safety alert about PTU Get baseline CBC and liver panel prior to Rx Monitor thyroid function 4 weeks after initiation and then every 4-8 weeks until euthyroid FT4 and/or T3 are best early in disease Once euthyroid, every 2-3 months Treat for months and decrease dose as able Consider getting thyroid receptor antibodies prior to stopping to help predict durability of remission

25 MMI more effective than PTU JCEM 2007: 92:
26 Side Effects of Thionamides SE PTU MMI Minor Reactions (GI, rash, fever) 1-5% 1-5%( dose related Agranulocytosis % % Hepatotoxicity Hepatitis (can be fatal) Vasculitis ANCA + Rare Cholestatic (few deaths)
27 Medical Management of Hyperthyroidism-Factors Affecting Remission Factor Favorable Unfavorable Duration of sx Brief Long Family Hx Negative Positive Thyroid size Small Large Severity Mild Moderate/Severe Response to Tx Rapid Less so TSH response Normalizes Persistently low Smoking status Non-smoker Smoker TRAb Negative Positive
28 Graves Remission Rates Around 30% will have persistent remission after months of thionamide May be as high as 50-75% in those with mild disease Longer treatment with thionamide does not have effect on chances of attaining remission
29 Definitive Therapy- RAI vs. Surgery Toxic multinodular goiter treatment failure Thyroidectomy <1% failure rate RAI 20%risk for need for retreatment Toxic adenoma treatment failure Thyroidectomy <1% RAI 6-18% risk for persistent hyperthyroidism Graves treatment failure Thyroidectomy essentially 0% Most patients hypothyroid by 6 months after RAI, some will need 2 nd treatment
30 Risk of permanent hypothyroidism Toxic multinodular goiter 100% chance of hypothyroidism after total thyroidectomy progressive increase with RAI from 2% at one year posttx and 64% at 20 yrs post-tx Toxic adenoma 2.3% chance after hemithyroidectomy progressive increase with RAI from 7.6% at one year post-tx, 28% at 5 years, 46% at 10 years and 60% at 20 yrs post-tx
31 Back to our patient She opted to treat with methimazole 20 mg per day was prescribed along with Atenolol 2 months later, felt much better, had regained 6 lbs, palpitations, heat intolerance, dyspnea and tremor resolved. Atenolol was stopped TFT s: TSH 0.02, FT4 1.6, FT3 4.0
32 hy is her TSH still suppressed?
33 Our patient Over next 18 months, MMI was able to be weaned and stopped TRAb was negative just prior to stopping Remains in remission 2 years later, nodule has been stable in size
34 Summary Recognize symptoms (particularly atypical ones) of hyperthyroidism Workup nodules independently of Graves Treat with methimazole in most cases Monitor T4/T3 until euthyroid, then TSH Consider definitive treatment with RaI or surgery in appropriate cases

35

36 Amiodarone and the Thyroid Amiodarone Class III anti-arrhythmic drug Contains two iodine atoms, equating to 6 mg of iodine in a 200 mg per day dose
37 Intrinsic Drug effects Inhibits outer ring 5 -monoiodination of T4, thus decreasing T3 production, reverse T3 accumulates since not metabolized Metabolite of amiodarone blocks T3-receptor binding to nuclear receptors and decreases expression of some thyroid hormone-related genes May have direct toxic effect on thyroid follicular cells destructive thyroiditis

38 X X Nature Reviews Endocrinology 6, 34-41
39 Iodine effects Iodine is substrate for thyroid hormone synthesis Normal autoregulation (Wolff-Chaikoff effect) When intrathyroidal iodine reaches a critical high, iodine transport and thyroid hormone synthesis are transiently inhibited until intrathyroidal iodine stores return to normal
40 Patients with underlying thyroid disease= defects in autoregulation of iodine Autoimmune thyroid disease Fail to escape from the Wolff- Chaikoff effect Development of goiter and hypothyroidism in Hashimoto s Amelioration of Graves disease Autonomously functioning nodules or latent Graves Do not autoregulate iodine Addition of more substrate can results in excessive thyroid hormone synthesis and thyrotoxicosis (so called Jod-Basedow effect)
41 Amiodarone-Induced Hypothyroidism Transient changes in thyroid function in normal patients Overt hypothyroidism in 5% (TSH>10) Subclinical hypothyroidism in another 25% (TSH ) Patients with underlying Hashimoto s thyroiditis or positive TPO antibodies more likely to develop permanent hypothyroidism Up to 20% of amiodarone-treated patients
42 Monitoring Assess TSH at baseline, can consider checking TPO antibodies as well Assess TSH every 3-4 months thereafter, especially in those with high-normal TSH to begin with or TPO Begin treatment if TSH persistently elevated with low normal or low Free T4 Larger than normal dose may be required Retest patient if amiodarone discontinued
43 HYPERTHYROIDISM 2 types Type I AIT: increased synthesis of T3 and T4 Most have underlying MNG, some have latent Graves Type II AIT: destructive thyroiditis Patients without underlying thyroid disease Lasts several weeks to months Often followed by hypothyroid phase with eventual recovery in most patients
44 Clinical Manifestations Cardiac manifestations often masked due to B- blocking activity of Amiodarone Development/redevelopment of atrial arrhythmias in prior well-treated patient Exacerbation of ischemic heart disease or CHF Unexplained weight loss Restlessness Low grade fever
45 Difficulties with Diagnosis Iodine in amiodarone competes with the tracer used in RAI uptake/scan Therefore the majority of types I (and all II s) have uptakes less than 1% Other criteria Goiter- type I Serum Tg and IL-6 lower in patients with type I TSH-receptor antibodies- Graves Color flow Doppler ultrasound Increased vascularity- type I Decreased vascularity- type II
46 Whether to discontinue Amiodarone Assess necessity of it to control a life-threatening arrythmia Half life is 100 days so no immediate benefit Amio blocks T4 to T3 conversion, B-adrenergic receptors, and possibly T3 receptor so stopping it may worsen hyperthyroid sx and signs
47 Treatment of Type I AIT Thionamides- need higher than normal dose mg due to high intrathyroidal iodine stores Taper dose as able If amiodarone is discontinued, monitor urine iodine until normal, and then can consider cautiously tapering thionamide Radioiodine usually not an option Thyroidectomy for refractory cases
48 Treatment of Type II AIT Glucocorticoids mg of prednisone daily Continue for 1-3 months prior to tapering dose In one study 60% became euthyroid at one month
49 When cause is unclear Combination of methimazole 40 mg daily and prednisone 40 mg daily Rapid response suggests more of a type II AIT Poor response suggests type I
50 Summary Amiodarone can induce hypo or hyperthyroidism Hypothyroidism can be treated the same way one would treat Hashimoto s but often require larger doses Hyperthyroidism can be difficult to distinguish type, often combination Cannot do uptake and scan to determine type due to large iodine load Treatment can be with prednisone, thionamides or both depending on type

51
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Canadian Endocrine Review Course 2014
 Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Common Causes of Hypothyroidism
 Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Virginia ACP Clinical Update Thyroid Clinical Pearls. University of Virginia. Richard J. Santen MD
 Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
CHAPTER-II Thyroid Diseases. by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university
 CHAPTER-II Thyroid Diseases by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university Aspects That Will Be Addressed Hyperthyroidism Hypothyroidism Thyroiditis Hyperthyroidism
CHAPTER-II Thyroid Diseases by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university Aspects That Will Be Addressed Hyperthyroidism Hypothyroidism Thyroiditis Hyperthyroidism
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Disorders of the Thyroid Gland
 Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Mastering Thyroid Disorders. Douglas C. Bauer, MD UCSF Division of General Internal Medicine
 Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
19th Century Thyroidology
 1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Amiodarone Induced Thyrotoxicosis Treatment? (AIT)
") Amiodarone Induced Thyrotoxicosis Treatment? (AIT) Presentation of a Case Report Annelies Tonnelier Brigitte Velkeniers 14-12-2013 1 1. Background 1. Case report 2. Investigations 3. Diagnosis 4. Treatment
Amiodarone Induced Thyrotoxicosis Treatment? (AIT) Presentation of a Case Report Annelies Tonnelier Brigitte Velkeniers 14-12-2013 1 1. Background 1. Case report 2. Investigations 3. Diagnosis 4. Treatment
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
Effect of thyroid hormones of metabolism Thyroid Diseases
 Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Slide notes: This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications,
 1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
The Thyroid: No mystery. Just need all the pieces to the puzzle.
 The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan
 HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
Management of Common Thyroid Disorders
 Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders
 Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Thyroid Nodules: What to do next?
 Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Updates in Thyroid Disease. Thyroid Outline. Thyroid 10/5/2015. Leila Wing, MD. Endocrinology, Diabetes, and Metabolism
 Updates in Thyroid Disease Leila Wing, MD Endocrinology, Diabetes, and Metabolism Background Hypothyroidism Hyperthyroidism Thyroid nodules Thyroid Cancer Conclusions Resources/References Thyroid Outline
Updates in Thyroid Disease Leila Wing, MD Endocrinology, Diabetes, and Metabolism Background Hypothyroidism Hyperthyroidism Thyroid nodules Thyroid Cancer Conclusions Resources/References Thyroid Outline
61 yo M w/heart disease presenting in decompensated HF. 1/24/13 Jess Hwang
 61 yo M w/heart disease presenting in decompensated HF 1/24/13 Jess Hwang HPI 3 weeks worsening orthopnea, PND, DOE Referred to UCMC for transplant evaluation Found to have 100% afib burden 1 month prior
61 yo M w/heart disease presenting in decompensated HF 1/24/13 Jess Hwang HPI 3 weeks worsening orthopnea, PND, DOE Referred to UCMC for transplant evaluation Found to have 100% afib burden 1 month prior
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
4) Thyroid Gland Defects - Dr. Tara
 Thyroid Gland Defects - Dr. Tara") 4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid gland defects. Dr. Tara Husain
 Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid Gland. Patient Information
 Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Pathophysiology of Thyroid Disorders. PHCL 415 Hadeel Alkofide April 2010
 Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
THYROID DISEASES. CASE BASED WORKSHOP Z. Henry He, MD, PhD. Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School
 THYROID DISEASES CASE BASED WORKSHOP Z. Henry He, MD, PhD Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School DISCLOSURE I have no relevant financial disclosure OBJECTIVES
THYROID DISEASES CASE BASED WORKSHOP Z. Henry He, MD, PhD Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School DISCLOSURE I have no relevant financial disclosure OBJECTIVES
Understanding thyroid function tests. Dr. Colette George
 Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
AUGUST 25-27, 2017 UPDATE & BOARD REVIEW. acofp INTENSIVE. Evolving Issues in Endocrinology. Chris Pitsch, DO INNOVATIVE COMPREHENSIVE HANDS-ON
 acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Evolving Issues in Endocrinology Chris Pitsch, DO acofp Am eric an College
acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Evolving Issues in Endocrinology Chris Pitsch, DO acofp Am eric an College
Thyroiditis Diagnosis and Management issues. Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College
 Thyroiditis Diagnosis and Management issues Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College Definition Thyroiditis is a general term that refers to inflammation of the thyroid gland.
Thyroiditis Diagnosis and Management issues Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College Definition Thyroiditis is a general term that refers to inflammation of the thyroid gland.
Hyperthyroidism, Inflammatory Disorders
 Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Management of Thyroid Nodules. February 2 nd, 2018 Sarah Hopkins
 Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
THYROID AWARENESS. By: Karen Carbone. January is thyroid awareness month. At least 30 million Americans
 THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
Thyroid Disorders Towards a Healthy Endocrine System
 Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY
 THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY
 ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Hyperthyroidism: Guidelines and Beyond. Douglas S Ross MD May Copyrighted slides omitted
 Hyperthyroidism: Guidelines and Beyond Douglas S Ross MD May 19 2018 Copyrighted slides omitted Abbott Laboratories Quest Diagnostics Disclosures Diagnosis Biochemical Assessment Biotin Interference Biotinylated
Hyperthyroidism: Guidelines and Beyond Douglas S Ross MD May 19 2018 Copyrighted slides omitted Abbott Laboratories Quest Diagnostics Disclosures Diagnosis Biochemical Assessment Biotin Interference Biotinylated
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Iodine 131 thyroid Therapy. Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego
 Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Systemic Management of Graves Disease. Robert James Graves, M.D., FRCS ( ) Graves Disease: Endocrinopathy or Ophthalmopathy?
 Graves Disease: Endocrinopathy or Ophthalmopathy?") Systemic Management of Graves Disease Rona Z. Silkiss, M.D., FACS Associate Clinical Professor, UCSF Chief, Division of Ophthalmic Plastic and Orbital Surgery California Pacific Medical Center No financial
Systemic Management of Graves Disease Rona Z. Silkiss, M.D., FACS Associate Clinical Professor, UCSF Chief, Division of Ophthalmic Plastic and Orbital Surgery California Pacific Medical Center No financial
Thyroid Nodules. Objectives. Clinical Practice Guidelines for the Management of Thyroid Disorders
 9:45 1:45am Clinical Practice Guidelines for the Management of Thyroid Disorders SPEAKER Gregory Brent, MD Presenter Disclosure Information The following relationships exist related to this presentation:
9:45 1:45am Clinical Practice Guidelines for the Management of Thyroid Disorders SPEAKER Gregory Brent, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Thyroid Disease in Cardiovascular Patients
 Thyroid Disease in Cardiovascular Patients Stuart R. Chipkin, MD Research Professor, School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD Nothing to
Thyroid Disease in Cardiovascular Patients Stuart R. Chipkin, MD Research Professor, School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD Nothing to
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
THYROID DISEASE IN PREGNANCY
 THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
Sonographic Features of Thyroid Nodules & Guidelines for Management
 Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Pearls and Pitfalls of Thyroid Diagnosis. Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS
 Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Amiodarone Toxicities
 Amiodarone Toxicities Student Rounds Review Ashlie McGuire - Aug. 4, 2016 Amiodarone Use: Antiarrhythmic agent Supraventricular and ventricular tachycardia Favourable for HF patients due to minimal inotropic
Amiodarone Toxicities Student Rounds Review Ashlie McGuire - Aug. 4, 2016 Amiodarone Use: Antiarrhythmic agent Supraventricular and ventricular tachycardia Favourable for HF patients due to minimal inotropic
Graves Disease. What is Graves disease?
 Graves Disease What is Graves disease? The thyroid gland s production of thyroid hormones (T 3 and T 4 ) is triggered by thyroidstimulating hormone (TSH), which is made by the pituitary gland. Graves disease,
Graves Disease What is Graves disease? The thyroid gland s production of thyroid hormones (T 3 and T 4 ) is triggered by thyroidstimulating hormone (TSH), which is made by the pituitary gland. Graves disease,
THE THYROID BOOK. Medical and Surgical Treatment of Thyroid Problems
 THE THYROID BOOK Medical and Surgical Treatment of Thyroid Problems Trouble with Your Thyroid Gland The thyroid is a small gland in your neck that plays a big role in how your body functions. It impacts
THE THYROID BOOK Medical and Surgical Treatment of Thyroid Problems Trouble with Your Thyroid Gland The thyroid is a small gland in your neck that plays a big role in how your body functions. It impacts
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Some Issues in the Management of Hypothyroidism
 Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Approach to Thyroid Dysfunction in the Elderly
 Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
THYROID DISEASE AND TESTING. Jack L. Snitzer, D.O., FACOI, FACE, CCD
 THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
Thyroid Disease in Pregnancy: The Essentials. Elizabeth N. Pearce, MD, MSc
 Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS
 LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
Sample Type - Serum Result Reference Range Units. Central Thyroid Regulation Surrey & Activity KT3 4Q. Peripheral Thyroid D Function mark
 Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Optimal 131 I Therapy of Thyrotoxicosis SNMMI Annual Meeting, 6/26/2018
 RADIOACTIVE IODINE THERAPY FOR HYERTHYROIDISM Mark Tulchinsky, MD, FACNM, CCD Professor of Radiology and Medicine Division of Nuclear Medicine Penn State University Hospital I Love What I do, i.e. Nuclear
RADIOACTIVE IODINE THERAPY FOR HYERTHYROIDISM Mark Tulchinsky, MD, FACNM, CCD Professor of Radiology and Medicine Division of Nuclear Medicine Penn State University Hospital I Love What I do, i.e. Nuclear
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
The Thyroid and Pregnancy OUTLINE OF DISCUSSION 3/19/10. Francis S. Greenspan March 19, Normal Physiology. 2.
 The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
supraventricular (ectopic atrial) tachycardia: case report and review of the literature
 tachycardia: case report and review of the literature") Letter to the Editor Amiodarone-induced thyrotoxicosis with paroxysmal supraventricular (ectopic atrial) tachycardia: case report and review of the literature Zofia Kolesińska 1#, Katarzyna Siuda 1##,
Letter to the Editor Amiodarone-induced thyrotoxicosis with paroxysmal supraventricular (ectopic atrial) tachycardia: case report and review of the literature Zofia Kolesińska 1#, Katarzyna Siuda 1##,
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
35 yo F with Graves Disease. Endorama March 10, 2016 Mizuho Mimoto
 35 yo F with Graves Disease Endorama March 10, 2016 Mizuho Mimoto PHONE CALL: 35 F with recently diagnosed Graves Vomiting Persistent diarrhea with incontinence x 2 days Tremor Heart racing Subjective
35 yo F with Graves Disease Endorama March 10, 2016 Mizuho Mimoto PHONE CALL: 35 F with recently diagnosed Graves Vomiting Persistent diarrhea with incontinence x 2 days Tremor Heart racing Subjective
Endocrinology Sample Case
 120 Beulah Road, NE, Suite 200 Vienna, Virginia 22180 Toll Free: 800-336-0332 Fax: 703-255-6134 www.malpracticeexperts.com Endocrinology Sample Case Hyperthyroidism and Graves disease (thyrotoxicosis)
120 Beulah Road, NE, Suite 200 Vienna, Virginia 22180 Toll Free: 800-336-0332 Fax: 703-255-6134 www.malpracticeexperts.com Endocrinology Sample Case Hyperthyroidism and Graves disease (thyrotoxicosis)
Thyroid Diseases. Q1: The most common thyroid function disorder is? Q2: The most sensitive test for thyroid function is?
 Thyroid Diseases Scott Urquhart, PA-C Clinical Instruct., George Washington Univ. PA Program Adjunct Clinical Prof., James Madison Univ. PA Program Diabetes and Thyroid Associates. Fredericksburg, Virginia
Thyroid Diseases Scott Urquhart, PA-C Clinical Instruct., George Washington Univ. PA Program Adjunct Clinical Prof., James Madison Univ. PA Program Diabetes and Thyroid Associates. Fredericksburg, Virginia
Page 1. Understanding Common Thyroid Disorders. Cases. Topics Covered
 Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Thyroid disease for R2
 Thyroid disease for R2 Rungnapa Laortanakul, MD. 5 February 2013 Thyroid Thyrotoxicosis/Thyroiditis Amiodarone and thyroid dysfunction Thyroid storm Hypothyroidism Thyroid nodule Thyrotoxicosis Refers
Thyroid disease for R2 Rungnapa Laortanakul, MD. 5 February 2013 Thyroid Thyrotoxicosis/Thyroiditis Amiodarone and thyroid dysfunction Thyroid storm Hypothyroidism Thyroid nodule Thyrotoxicosis Refers
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Graves Disease in Pediatrics
 Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed