Thyroid and Adrenal Gland
|
|
|
- Erick Chambers
- 6 years ago
- Views:
Transcription





1 Thyroid and Adrenal Gland NAACCR Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar at your site, please collect their names and s. We will be distributing a Q&A document in about one week. This document will fully answer questions asked during the webinar and will contain any corrections that we may discover after the webinar. 2 Fabulous Prizes 3 1
2 Agenda Coding moment Submitting questions to the standard setters Thyroid Overview Collaborative Stage Data Collection System (CS) Quiz Exercise Adrenal Gland Overview CS Quiz Exercise Coding Moment SUBMITTING QUESTIONS TO STANDARD SETTERS Who do I submit questions to? That depends on the question! 2
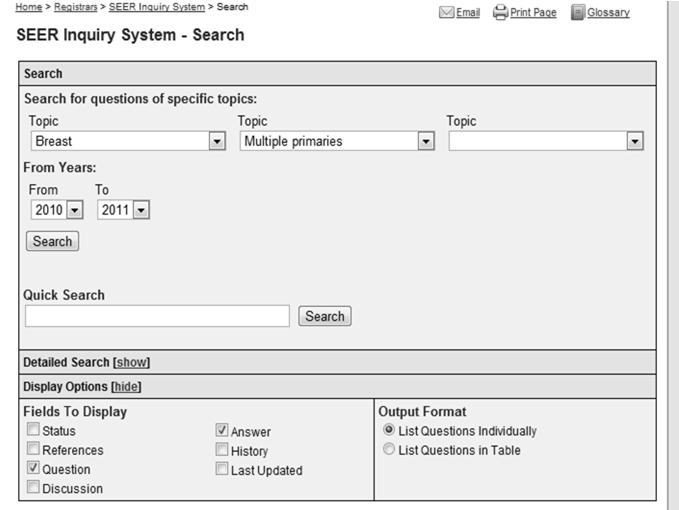
3 Questions for SEER Questions concerning the following topics should go to Ask a SEER Registrar Multiple primary rules ICD 0 3 ICD 10 Question for CAnswer Forum Questions concerning the following topics should go to the CAnswer Forum AJCC TNM Staging Collaborative Stage Submitting Questions to SEER 1. Search the SEER Inquiry System search 2. If you don t find an answer to your question, submit your question to Ask A SEER Registrar 3

4 4
5 5


6 Submitting Questions to the CAnswer Forum To search or submit questions on the CAnswer Forum go to 6

7 7

8 8
9 QUESTIONS? Thyroid OVERVIEW 9


10 The Numbers Estimated new cases and deaths from thyroid cancer in the United States in 2011: New cases: 48,020 Deaths: 1,740 Fifth most frequently occurring malignancy among women Fastest increasing cancer in both men and women National Cancer Intitute Endocrine Glands Illustration courtesy of the American Society of Clinical Oncology. Thyroid Gland C73.9 Parathyroid Gland C
11 Illustration courtesy of the American Society of Clinical Oncology. Thyroid Nodules Hot nodule Absorbs iodine on thyroid scan Cold Nodule Does not absorb iodine on thyroid scan Goiter Goiter An enlarged thyroid gland that may be diffuse or nodular 11




12 Level IB Level IA Base of Skull Level IIB Level IIA Hyoid Bone SEER Training Module Illustration courtesy of the American Society of Clinical Oncology. Level III Level IV 12


13 Level VA Level VB SEER Training Module Illustration courtesy of the American Society of Clinical Oncology. Level VI Level VII Illustration courtesy of the American Society of Clinical Oncology. 13
14 Thyroid Histology Follicular cells Thyroid hormone (thyroxine + triiodthyroxine) C cells (parafollicular cells) Calcitonin Lymphocytes Stromal cells Thyroid Histology Four Major Histologic Types Papillary carcinoma (includes follicular variant of papillary carcinoma) Follicular (includes Hurthle cell carcinoma) Medullary Carcinoma Undifferentiated or anaplastic carcinoma MPH Rules Other Required Histology Papillary and Follicular Combined with Combination Term Papillary carcinoma, follicular variant Medullary Follicular Mixed medullary follicular carcinoma Medullary Papillary Mixed medullary papillary carcinoma Code
15 Question A pathology report shows the right lobe of the thyroid with papillary microcarcinoma. Does microcarcinoma describe the size of the tumor or should this be coded to a different histology? SEER SINQ Answer For thyroid cancer only, the term micropapillary does not refer to a specific histologic type. It means that the papillary portion of the tumor is minimal or occult. SEER SINQ Question How is histology coded for a thyroid tumor described as predominantly papillary carcinoma, tall cell variant, follicular type? 15
16 Answer For cases diagnosed , assign code 8340 [Papillary carcinoma, follicular variant] according to rule H15 for Other Sites. "Predominantly" and "type" indicate specific histologies. "Variant" does not. See rule H13. The histology in this case is papillary and follicular. Tall cell variant is ignored. SEER SINQ Diagnosing Thyroid Cancer Physical exam Blood tests Check levels of thyroid stimulating hormone (TSH) Check levels of calcitonin Diagnosing Thyroid Cancer Imaging Ultrasound Radioiodine (thyroid) scan Positron emission tomography (PET) scan Octreotide scan Biopsy Fine needle aspiration Surgical 16
17 Treatment for Papillary and Follicular Carcinoma Surgery Lobectomy plus isthmusectomy (23) Thyroidectomy (50) Radioactive Iodine Treatment ( 131 I) Unresectable tumors Post thyroidectomy Treatment for Papillary and Follicular Carcinoma External Beam Radiation May be done with 131 I treatment for locoregional recurrence May be used as adjuvant therapy if tumor does not show uptake of iodine Thyroxin suppression of thyroid stimulating hormone (TSH) Question If a patient is taking Synthroid prior to being diagnosed with thyroid cancer and having total thyroidectomy, is Synthroid still coded as hormone therapy 1st course of treatment after cancer directed surgery? 17
18 Answer Yes, it is still considered 1st course treatment and the date of treatment would be the date of the patient's diagnosis of the thyroid malignancy. Treatment Medullary Carcinoma Total thyroidectomy and bilateral central neck dissection (level VI) Anaplastic Carcinoma Surgery if localized Thyroid COLLABORATIVE STAGE DATA COLLECTION SYSTEM V
19 CS Tumor Size: Thyroid Assignment of T1 and T2 categories is based on tumor size Physician s assignment of T category may be used to code CS Tumor Size if no other information is available Code 991 Stated as T1a with no other information on size Code 992 Stated as T1b or T1 NOS with no other information on size Code 994 Stated as T2 with no other information on size CS Extension: Thyroid All anaplastic thyroid carcinomas are considered T4 by AJCC Intrathyroidal: T4a Gross extrathyroid extension: T4b CS Extension: Thyroid Anaplastic thyroid carcinoma If CS Extension = 000, , 950, or 999 Histology = 8020, 8021, 8030, 8031, or 8032 OR Grade = 4 Then T category is based on value of CS Extension as shown in Histology Grade Extension AJCC Table CS Extension TNM Map 000 (In situ) T4NOS 200 (Multiple foci thyroid) T4a 405 (Stated as T1a) ERROR 450 (Extension to strap muscle) T4b 19
20 CS Extension: Thyroid In situ code (000) maps to unknown AJCC stage and in situ summary stage Assignment of T1 and T2 categories is based on tumor size Physician s assignment of T category may be used to code CS Extension if no other information is available Use codes 405, 410, 415, 420, 490, 560, 810, or 815 to code CS Extension based on a statement of T with no other extension information available CS Extension: Thyroid Assign code 300, localized NOS, only if info is not available to assign codes 100, 200, 400, 405, 410, 415, 420, or 490 CS Extension codes 405, 410, 415, 420, and 490 are not compatible with anaplastic carcinoma of the thyroid CS Extension: Thyroid Extension or invasion into tumor capsule Measure of tumor aggressiveness but tumor is still confined to thyroid Do not use code 400 (into thyroid capsule but not beyond) Extension or invasion into thyroid capsule Indicates extrathyroidal extension Assign code that describes the type of extrathyroidal extension 20
21 Pop Quiz: CS Tumor Size; CS Extension Final diagnosis: Multifocal papillary follicular carcinoma confined to right thyroid; pt1a What is the code for CS Tumor Size? 991: Stated as T1a with no other info on size 999: Unknown What is the code for CS Extension? 200: Multiple foci confined to thyroid 405: Stated as T1a with no other info on extension Pop Quiz: CS Tumor Size; CS Extension Right lobectomy, thyroid Tumor size: 1.7 x 1.2 cm Tumor focality: Single tumor Histologic type: Papillary carcinoma, predominantly follicular subtype Margins: Negative; closest 2 mm Tumor capsular invasion: Focally present Lymphatic invasion: None Extrathyroidal extension: None Tumor location: Center of right lobe Lymph nodes: None identified Stage I; pt1b cn0 cm0 Pop Quiz: CS Tumor Size; CS Extension What is the code for CS Tumor Size? : Stated as T1b or T1 NOS with no other info on size What is the code for CS Extension? 100: Single tumor confined to thyroid 400: Into thyroid capsule, but not beyond 410: Stated as T1b with no other info on extension 21
22 CS Lymph Nodes: Thyroid Includes lymph nodes defined as Levels I VI and Other by AJCC All node levels are regional for AJCC Nodes are divided into regional and distant for summary stage Involvement includes ipsilateral, bilateral, contralateral, and midline nodes CS Lymph Nodes: Thyroid Prognostic influence of nodal involvement Less in patients with well differentiated tumors (papillary, follicular) Some observed adverse prognosis in older age group Ominous prognosis for patients with medullary carcinoma CS Lymph Nodes: Thyroid Progression of lymph node involvement Code 120: Level VI anterior compartment Code 135: Levels II upper jugular; III middle jugular; IV lower jugular; V posterior triangle; VA spinal accessory; parapharyngeal; retroauricular; retropharyngeal; and suboccipital Code 155: Level VB transverse cervical Code 158: Level VII superior mediastinal Code 160: Levels IA submental; IB submandibular; facial; and parotid 22
23 CS Mets at DX: Thyroid Involvement of submental or submandibular nodes is coded in CS Lymph Nodes Distant metastasis occurs by hematogenous spread Most commonly to lungs and bones Pop Quiz: CS Lymph Nodes; CS Mets at DX FNA of nodule in right lobe of thyroid: well differentiated Hurthle cell carcinoma CT scan of neck: Malignant adenopathy to nodes including right anterior compartment nodes, right and left retropharyngeal nodes, and right submandibular nodes CT scan of chest: 3 metastatic nodules in the upper lobe of the right lung Pop Quiz: CS Lymph Nodes; CS Mets at DX What is the code for CS Lymph Nodes? 120: Level VI nodes (anterior compartment group) 135: Retropharyngeal nodes 160: Level IB (submandibular nodes) What is the code for CS Mets at DX? 12: Distant lymph nodes 40: Distant metastasis except distant lymph nodes 51: Distant metastasis plus distant lymph nodes 23
24 SSF1: Solitary vs. Multifocal Tumor Code 000 No evidence of primary tumor Code 010 Solitary tumor Physician assigns s suffix or descriptor to T category Tumor described as solitary, single, a single focus, or unifocal Code 020 Multifocal tumor Physician assigns m suffix or descriptor to T category Tumor described as multifocal or multicentric, or as having multiple foci Pop Quiz: SSF1 Thyroidectomy: Multiple foci of follicular carcinoma of right lobe; no nodules in left lobe What is the code for SSF1? 000: No evidence of primary tumor 010: Solitary tumor 020: Multifocal tumor Standard Setters SSF Requirements CS v02.03: Thyroid SSF1: Solitary vs. Multifocal Tumor CoC, SEER, Canadian Council of Cancer Registries Required NPCR Not required 24
25 QUIZ Adrenal Gland OVERVIEW The Numbers Adrenal gland primaries are rare Adrenocortical carcinoma affects 1 to 2 persons per million population. Median age at diagnosis is 44 years. National Institute on Health 25


26 Overview National Cancer Insitute Adrenal Gland Regional lymph nodes Aortic (para and peri aortic) Retroperitoneal, NOS Common metastatic sites Liver Lung Retroperitoneum 26
 Functioning tumors")
27 Adrenal Tumors Adrenal adenoma (8140/0) Typically asymptomatic May be referred to as incidentalomas if found incidentally on imaging Tumors larger than 5 6 cm are most likely malignant Metastasis Most common malignant tumors found in the adrenal gland are metastasis from other primaries Lung Melanoma Breast Primary Adrenal Malignancies Adrenocortical carcinoma (8370/3) Functioning tumors excrete excess steroid hormones Non functioning tumors do not excrete steroid hormones National Cancer Insitute Adrenocortical Carcinoma Adrenocortical carcinoma can be classified as follows: Differentiated: Functioning tumors are usually differentiated Anaplastic: Production of hormones by anaplastic tumors is rare Hormonal: Approximately 60% of adrenocortical carcinomas produce hormones 27
28 Adrenocortical Carcinoma Treatment Surgery Excisional biopsy Radical Nephrectomy Lymph node dissection Chemotherapy Mitotane External Beam Radiation For patients with localized disease that are not surgical candidates Medullary Primaries Malignant Pheochromocytoma (8700/3) Can release high levels of epinephrine Symptoms may include Headache Sweating Palpitations Surgery is treatment of choice Radiation and chemotherapy If disease is advanced or patient is not surgical candidate Neuroblastoma Neuroblastoma (9500/3) Arises from nerve tissue of adrenal glands Common pediatric cancer Usually in children under 5 years Often metastasis present at the time of diagnosis Treatment Surgery Radiation Chemotherapy BRM Targeted therapy 28

29 Adrenal Gland COLLABORATIVE STAGE DATA COLLECTION SYSTEM V02.03 CS Tumor Size: Adrenal Gland Assignment of T1 and T2 categories is based on tumor size Physician s assignment of T category may be used to code CS Tumor Size if no other information is available Code 995 Stated as T1 with no other information on tumor size Code 996 Stated as T2 with no other information on tumor size CS Extension: Adrenal Gland In situ code (000) maps to unknown AJCC stage and in situ summary stage Assignment of T1 and T2 categories is based on tumor size CS Extension code = T category is based on value of CS Tumor Size as shown in Extension Size Table 29

30 CS Extension: Adrenal Gland Physician s assignment of T category may be used to code CS Extension if no other information is available Use codes 200, 250, 400, or 810 to code CS Extension based on a statement of T with no other extension information available Assign code 300, localized NOS, only if info is not available to assign codes 100, 200, or 250 CS Extension: Adrenal Gland Code 400 Adjacent connective tissue Gerota s fascia CS Extension: Adrenal Gland Code 605 Adjacent organs/structures: Kidney Retroperitoneal structures including: Great vessels: aorta; inferior vena cava 30
 995: Stated as T1 with no other info on size What is the code for CS Extension?")
31 Pop Quiz: CS Tumor Size; CS Extension Final diagnosis: Adrenal cortical adenocarcinoma, 4.8 cm, confined to adrenal gland; pt1 What is the code for CS Tumor Size? 048: 4.8 cm (48 mm) 995: Stated as T1 with no other info on size What is the code for CS Extension? 100: Invasive carcinoma confined to adrenal gland 200: Stated as T1 with no other info on extension CS Lymph Nodes: Adrenal Gland 110: Pericaval node Adrenal glands 105: Aortic node Aorta Inferior vena cava Image source: SEER Training Website CS Mets at DX: Adrenal Gland Standard table for CS Mets at DX is used Common metastatic sites include liver, lung, and retroperitoneum 31
32 SSF2: Tumor Weight Code Description 000 No mass/tumor found grams (exact tumor weight including gland) grams or greater 988 Not applicable 998 No surgical resection of primary site 999 Unknown Pop Quiz: SSF2 Adrenalectomy: Adrenal gland with small focus of adrenal cortical carcinoma; weight is 45.2 grams What is the code for SSF2? SSF3: Vascular Invasion Code Description 000 Vascular invasion not present/not identified 010 Invasion of adrenal vein only 020 Invasion of renal vein only 030 Invasion of inferior vena cava (IVC) only 040 Invasion of renal vein (020) + adrenal vein (010) 050 Invasion of IVC (030) + adrenal vein (010) 060 Invasion of IVC (030) + renal vein (020) 070 Invasion of IVC (030) + renal vein (020) + adrenal vein (010) 988 Not applicable 991 Large vessel venous invasion, vein not specified 998 No surgical resection of primary site 999 Unknown 32
33 Pop Quiz: SSF3 Adrenalectomy: Adrenal gland with adrenal cortical carcinoma; lymph vascular invasion is present; no large vessel invasion What is the code for SSF3? 000: Vascular invasion not present/not identified 991: Large vessel venous invasion, vein not specified 999: Unknown Standard Setters SSF Requirements CS v02.03: Adrenal Gland SSF2: Tumor Weight CoC, SEER, NPCR Not required Canadian Council of Cancer Registries Collect if in pathology report SSF3: Vascular Invasion CoC, SEER, NPCR Not required Canadian Council of Cancer Registries Collect if in pathology report 33
34 Questions? 100 Coming up! 1/5/12 Collecting Cancer Data: Pancreas 2/2/12 Collecting Cancer Data: Lung And the winners of the fabulous prizes are. 101 Thank You!
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
COLLECTING CANCER DATE: THYROID AND ADRENAL GLAND
 COLLECTING CANCER DATE: THYROID AND ADRENAL GLAND 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATE: THYROID AND ADRENAL GLAND 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Thyroid Cancer Incidence & Image source: Thyroid ABC Health and Well Being Webinar Series 2 Anatomy
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Thyroid Cancer Incidence & Image source: Thyroid ABC Health and Well Being Webinar Series 2 Anatomy
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
NAACCR Webinar Series 1
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
10. HPV-Mediated (p16+) Oropharyngeal Cancer
 Oropharyngeal Cancer") 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
14. Mucosal Melanoma of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
NAACCR Webinar Series 1
 Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Lung /4/18. Please submit all questions concerning the webinar content through the Q&A panel.
 Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
NAACCR Webinar Series
 NAACCR 2009-2010 Webinar Series Collecting Cancer Data: Lip & Oral Cavity 8/5/2010 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes! NAACCR 2009/2010
NAACCR 2009-2010 Webinar Series Collecting Cancer Data: Lip & Oral Cavity 8/5/2010 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes! NAACCR 2009/2010
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Testicular Malignancies /8/15
 Collecting Cancer Data: Testis 2014-2015 NAACCR Webinar Series January 8, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Testis 2014-2015 NAACCR Webinar Series January 8, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
2018 Grade PEGGY ADAMO, RHIT, CTR OCTOBER 11, 2018
 1 2018 Grade PEGGY ADAMO, RHIT, CTR ADAMOM@MAIL.NIH.GOV OCTOBER 11, 2018 2 Acknowledgements Donna Hansen, CCR Jennifer Ruhl, NCI SEER Introduction 3 Histologic Type vs. Grade Credit: Dr. Kay Washington
1 2018 Grade PEGGY ADAMO, RHIT, CTR ADAMOM@MAIL.NIH.GOV OCTOBER 11, 2018 2 Acknowledgements Donna Hansen, CCR Jennifer Ruhl, NCI SEER Introduction 3 Histologic Type vs. Grade Credit: Dr. Kay Washington
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification
 Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Histology Coding ANSWERS
 Histology Coding ANSWERS 1.) Biopsy of a right thyroid nodule reveals papillary carcinoma. What is the ICD-O-3 code? a. 8050/3 - Papillary carcinoma b. 8260/3 - Papillary adenocarcinoma Rationale/comment:
Histology Coding ANSWERS 1.) Biopsy of a right thyroid nodule reveals papillary carcinoma. What is the ICD-O-3 code? a. 8050/3 - Papillary carcinoma b. 8260/3 - Papillary adenocarcinoma Rationale/comment:
LYMPHATIC DRAINAGE IN THE HEAD & NECK
 LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
YCN Thyroid NSSG. *** VALID ON DATE OF PRINTING ONLY - all guidelines available at *** page 1 of 8 version number: 1.
 YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
1. Protocol Summary Summary of Trial Design. IoN
 1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012
 Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]](/thumbs/82/86783199.jpg "Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]") CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Nasal Cavity CS Tumor Size (Revised: 02/03/2010)
") Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Canadian Scientific Journal. Intraoperative color detection of lymph nodes metastases in thyroid cancer
 Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
2018 IMPLEMENTATION UPDATE: WHAT S NEW IN STAGING FOR 2018?
 2018 IMPLEMENTATION UPDATE: WHAT S NEW IN STAGING FOR 2018? SESSION 2 10/20/17 Q&A Please submit all questions concerning webinar content through the Q&A panel. A recording of today s session, the Q&A,
2018 IMPLEMENTATION UPDATE: WHAT S NEW IN STAGING FOR 2018? SESSION 2 10/20/17 Q&A Please submit all questions concerning webinar content through the Q&A panel. A recording of today s session, the Q&A,
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report?
 for ovary, does it have to say the term surface on the path report?") Q&A Session for Collecting Cancer Data: Ovary Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report? A: We reviewed both the
Q&A Session for Collecting Cancer Data: Ovary Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report? A: We reviewed both the
Q: How do you clinically code the N if the nodes are stated to be positive on mammogram/us or other imaging? No biopsy of nodes was done.
 Q&A Breast Webinar Q: One of my investigators is interested in knowing when Oncotype DX data collection was implemented. That data is collected in SSFs 22 and 23. I remember that the SSFs for breast were
Q&A Breast Webinar Q: One of my investigators is interested in knowing when Oncotype DX data collection was implemented. That data is collected in SSFs 22 and 23. I remember that the SSFs for breast were
What is Thyroid Cancer? Here are four types of thyroid cancer:
 What is Thyroid Cancer? Thyroid cancer is a group of malignant tumors that originate from the thyroid gland. The thyroid is a gland in the front of the neck. The thyroid gland absorbs iodine from the bloodstream
What is Thyroid Cancer? Thyroid cancer is a group of malignant tumors that originate from the thyroid gland. The thyroid is a gland in the front of the neck. The thyroid gland absorbs iodine from the bloodstream
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
4/10/2018. SEER EOD and Summary Stage. Overview KCR 2018 SPRING TRAINING. What is SEER EOD? Ambiguous Terminology General Guidelines
 SEER EOD and Summary Stage KCR 2018 SPRING TRAINING Overview What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets SEER Summary Stage 2018 Site Specific
SEER EOD and Summary Stage KCR 2018 SPRING TRAINING Overview What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets SEER Summary Stage 2018 Site Specific
Renal Parenchymal Neoplasms
 Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
2010 Update. NAACCR Webinar Series 1 4/1/2010. Agenda. Access to 2010 Information. CSv2. Collecting Cancer Data: Soft Tissue Sarcoma
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Soft Tissue Sarcoma, Neuroendocrine Tumors (NET) and Gastrointestinal Stromal Tumors (GIST) Agenda Updates Soft Tissue Sarcoma Overview CSv2 MP/H
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Soft Tissue Sarcoma, Neuroendocrine Tumors (NET) and Gastrointestinal Stromal Tumors (GIST) Agenda Updates Soft Tissue Sarcoma Overview CSv2 MP/H
NAACCR Webinar Series 1. Instructors Q&A 10/6/2011. Collecting Cancer Data: Larynx Including Mucosal Melanoma of Larynx.
 NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Larynx Instructors Shannon Vann, CTR Jim Hofferkamp, CTR 2 Q&A Please submit all questions concerning webinar content through the Q&A panel. 3 NAACCR
NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Larynx Instructors Shannon Vann, CTR Jim Hofferkamp, CTR 2 Q&A Please submit all questions concerning webinar content through the Q&A panel. 3 NAACCR
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update
 thyroid carcinoma-an update") Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Kyle L. Ziegler, CTR. California Cancer Registry U.C. Davis Health System
 Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Coding Pitfalls 9/11/14
 Coding Pitfalls 2013 2014 NAACCR Webinar Series September 11, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Coding Pitfalls 2013 2014 NAACCR Webinar Series September 11, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Q&A. Fabulous Prizes. Collecting Cancer Data: Breast 4/4/13. NAACCR Webinar Series Collecting Cancer Data Breast
 Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Q&A. Fabulous Prizes. Collecting Cancer Data: Bone and Soft Tissue 1/10/113. NAACCR Webinar Series
 Collecting Cancer Data Bone & Soft Tissue NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data Bone & Soft Tissue NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging
 Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement
Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement