Laser eye surgery indications
|
|
|
- Gertrude Rodgers
- 6 years ago
- Views:
Transcription
1 Laser eye surgery indications Petros Smahliou, MD, FRCS, EBO Athens, March 2018
2 Laser eye surgery: Common Significant ametropia indications Anisometropia Anisoeikonia Intolerance of spectacle use (eg. High amount of astigmatism) Intolerance of contact lens use Life style
3 Age limits Over 18/20 years(?) old and stable refraction Under 60 years old (?) Under investigation treatments in chlildren for amblyopia Touch ups in elders after cataract operations
4 INCLUSION CRITERIA Age 18 /20 years or older Stable refraction of at least one year s duration Myopia up, diopters, Astigmatism up 6.00 diopters, Hyperopia up diopters
5 EXCLUSION CRITERIA absolute eye-related - Keratoconus - Herpetic keratitis, - Some corneal dystrophies or degenerations (Avellino or Granular, Lattice,Reiss-Bucklers) - Cataract, Glaucoma or other pathology, including scarring, lagophthalmos, dry eye, blepharitis, uveitis and macula problems - Unstable refraction
6 EXCLUSION CRITERIA relative eye-related Single eye or lazy eye (?) Very high, or low Ks Irregular astigmatism Controled glaucoma or glaucoma suspect Controled DM Previous AKs or RKs Drugs (isotretinoin, amiodarone, oestrogens) Mild dry eye Age less than 20 in male myopes
7 EXCLUSION CRITERIA general Atopy (severe & spread) Diabetes mellitus (uncontrolled) History of keloids Pregnancy or lactation Autoimmune disease (?) Immunosuppression or immunocompromised status Drugs (isotretinoin, amiodarone, oestrogens)
8 METHOD Technique according to refractive error Refraction Technique Myopia Hyperopia Astigmatism PRK dpt Contradiction? dpt LASIK dpt dpt dpt Femto LASIK dpt dpt dpt
9 PRK indications Low refractive errors (up to -4,00 dpt & - 2,00 dpt astgm) Contact sports (eg. boxing) Predisposition to trauma (martial arts, military) Anterior basement membrane dystrophy History of recurrent erosions Deep orbits (difficulty to obtain good suction) Patient preference
10 PRK indications Scleral buckles placed anteriorly Pterygia or naevae Thin and suspicious corneas Patients with moderate dry eye Best option for an inexperience refractive surgeon (simpler than Lasik)
11 Lasik indications High myopia(>6d) High astigmatism(>2d) Hyperopia Opt for fast recovery and no pain
12 So Which method to choose???
13 From Lasik to Femtosecond Lasik Advancement in laser technology Excellent precision Safer (and faster?) flap creation Thinner and different shape flaps Today is the safest method of refractive surgery
 Safer than conventional Lasik procedure Faster and better healing Less aberrations, better quality of")
14 Femtosecond Lasik VS Lasik Flap incision more accurate Reduced flap-related complications (free caps, irregular cuts) Safer than conventional Lasik procedure Faster and better healing Less aberrations, better quality of vision
15 Why choose Femto Lasik? Increased presicion with improved flap safety Better thickness predictability Capability of thinner flaps to accommodate thin corneas Greater surgeon choice and control over flap & thickness diameter Better vision
16 Why choose Femto Lasik? Stronger flap adherence Ability to abort and reapply the suction during flap creation Decreased incidence of epithelial ingrowth Lesser incidence of dry eyes or hemorrhage of the limbal vessels
17 Why choose Femto Lasik? Highest precision Homogenous flaps Uniform thickness & shape Better flap stability Accuracy when folded back Highest safety Eliminated complications Infections almost impossible Best possible outcomes Better results predictability than Lasik
18 Femtosecond Lasik additional indications & applications Cataract surgery Astigmatic keratotomies Intrastromal tunnels for rings Keratoplasties SMILE Treating presbyopia (radial lensotomy) Intrastromal ablations (intracor)
19 From PRK to Trans PRK Trans PRK (Transepithelial Photorefractive Keratectomy) No touch PRK The epithelium is removed by laser (no mechanically) Smoother tissue removal Smoother handling

20 Trans PRK
21 Trans PRK vs PRK Faster procedure Safer Less pain Faster recovery Less complications
22 When do Trans PRK? If the patient is not a good Lasik candidate (eg. Small eyes) Thin cornea (PRK X-tra) In anxious patients (afraid of Lasik procedure due to flap formation) In patients who have already undergone refractive surgery In CLX cases
23 When do Trans PRK? Trans PRK is a method with: Less chance of complications Long-term results comparable or better than Lasik Accuracy and ease on management
24 LASIK indications Initial corneal thickness in LASIK > 500 μm Initial corneal thickness in PRK > 470 μm Thickness norm < 50% (60%) Residual stroma thickness in LASIK Residual stroma thickness in PRK Depth removal Keratometry limits (for mechanical keratome) Keratometry limits (spherical aberration) > 300 μm > 400 μm < 135 μm dpt < dpt, > dpt Topography criteria Relatively and absolutely
25 Extreme refractive errors Myopia over -10,00 D (or less in thin corneas) and age 21 to 50 we prefer phakic IOLs Myopia over -10,00 D (or less in thin corneas) and age over 50 we prefer RLE Hypermetropia over +6 we prefer phakic IOLs if the AC depth is adequate, or RLE even in younger patients (multifocal IOL ) Combine with surface ablation
26 Pentacam HR inclusion criteria - Anterior float criteria: normal values: <+12μm (or10μm) suspicious: from12μm to15μm ΚCN : >15μm - Posterior float criteria: normal values: <+17μm suspicious: from18μm to20μm ΚCN : >20μm
27 Pentacam HR inclusion criteria2 Hight difference criterio: >5μm difference between anterior and posterior float Tongue like extensions - Pachymetry criteria - <470μ for PRK, <500μ for LASIK - TL inferior and more than 4mm of the GC - >30m difference between superior and inferior points - Topometric map: inferior qvalue>-0,55
28 Pentacam HR inclusion criteria3 - Keratometry criteria: - Kmax>48,5D - SRAX angle>22* - Kdif>3,00D with steepest the vertical merid - I-S Rabinowitz ratio >+2D - Rowsey s rule of 2% (Ks>45D, Kmax>2D between the two eyes) - Very high vertical coma
29 The most common display is a 4-map
30 4 map Anterior (Axial) sagittal Anterior elevation map Corneal thickness map Posterior elevation map
31 Corneal morphology Incidence of the morphology of topographic contour Central round shape 22.6% Central oval shape 20.8% Symmetrical bow tie 17.4% Asymmetric bow tie 49.6% Anomalous shape 7.1%
32 1-Anterior sagittal (axial)map Normal pattern 1- Symmetric bow tie pattern 2-Segments S and I are equal, 3- Their axes are aligned..
33 1-Anterior sagittal (axial)map Normal Parameters. At 5mm circle inferior power higher than superior less than 1.5D on the steep axis The superior point may rarely have a higher value than the inferior one; less than 2.50 D.
map Abnormal")
34 1-Anterior sagittal (axial)map Abnormal shapes
35 Important risky point in Anterior sagittal (axial)map 1-K>48D 2-Angulation 3-Astigmatism >6D in either surface 4-Against the rule astigmatism 5-Inferior superior asymmetry 6-Difference between the inferior and superior more than 1.50 D
map Angulations more")
36 1-Anterior sagittal (axial)map Angulations more than 30

37 1-Anterior sagittal (axial)map Asymmetric bow tie More lower steepness More than 1.5 D

38 1-Anterior sagittal (axial)map Asymmetric bow tie upper steepness difference more than 2.5D
map Asymetric +")
39 1-Anterior sagittal (axial)map Asymetric + angle
map Smile predisposed")
40 1-Anterior sagittal (axial)map Smile predisposed to ectasia

41 1-Anterior sagittal (axial)map junctional predisposed to ectasia
map Vortex predisposed")
42 1-Anterior sagittal (axial)map Vortex predisposed to ectasia
43 2-3-ANTERIOR AND POSTERIOR Shape. The normal shape is the hourglass Abnormal shapes Irregular, -Tongue-like extensions -Isolated islands ELEVATION MAP
44 2-3-ANTERIOR AND POSTERIOR Parameters.. The highest plus value within the central 5- mm zone; Normal values are <12 μm anterior <15 μm posterior Abnormal difference between front and back elevation more than 5u ELEVATION MAP

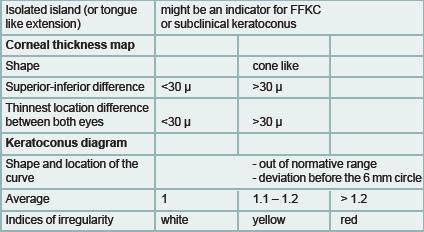
45 Normal shape is the hourglass Abnormal shapes include irregular, tongue-like extensions and isolated islands Abnormal isolated islands Abnormal shapes include irregular, tongue-like extensions

46 The cone can be localized using the The location may be -central, -eccentric, -peripheral elevation maps.

47 4-PACHYMETRY MAP Pattern The normal pattern is concentric The abnormal patterns include 1-Horizontaldisplacement, 2-dome-like, 3-globus, 4-and bell shapes

48 4-PACHYMETRY MAP Abnormal -Dome shape. -Displaced thinnest location

49 4-PACHYMETRY MAP Abnormal Horizontal displacement of corneal shape

50 4-PACHYMETRY MAP The bell shape seen in pellucid marginal degeneration
51 4-PACHYMETRY MAP Abnormal parameter 1- Abnormal less than 470 μm thickness at the TL with normal tomography, 2- Abnormal less than 500 μm thickness at the TL with abnormal tomography 0 μm.
52 4-PACHYMETRY MAP Abnormal parameter 3-Thickness Difference between bachy apex and thin. Loc.> 10u Early KC 4-Bachy apex Lower Location Y more than -500
 and inferior (I) points is 30 μm.")
53 4-PACHYMETRY MAP Abnormal parameter 5-Pachy. Thickness between superior(s) and inferior (I) points is 30 μm. At 5mm circle 6-Abnormal thickness at the TL between the patient s two eyes; more than 30 μm.

54 Thickness Profiles corneal thickness spatial profile (CTSP) The average progression of thickness starting from the TL to corneal periphery percentage thickness increase (PTI). The percentage of progression of the thickness The normal profile is a curved line plotted in red, following the black dotted curves, High average, Fast transition of thickness between the Low flat average corneal edema. A normal profile follows the normative curves with an average < 1.2 (red
 and ectatic disorders.. The average is usually high (> 1.1)")
55 Thickness Profiles Abnormal profiles include: a. Quick Slope The red curve leaves its course before the 6-mm zone. It is encountered in forme fruste keratoconus (FFKC) and ectatic disorders.. The average is usually high (> 1.1)

56 Thickness Profiles b. S-shape The red curve has a shape of an S. It is encountered in FFKC and ectatic disorders. The average is usually high (> 1.1).
 corneas such as Fuch s dystrophy and cornea Guttata.")
57 Thickness Profiles c. Flat shape The red curve takes a straight course. It is encountered in diseased thickened (oedematous) corneas such as Fuch s dystrophy and cornea Guttata. The average is low < 0.8 (red ellipse)

58 Thickness Profiles d. Inverted The red curve follows an upward course. It is encountered in some cases of PMD. The average is very low (< 0.8) and may take a minus value
59 Pupil Center Corneal thickness Location Important in decentration technique when treating hyperopia, astigmatism or corneal irregularities. They are also important to evaluate angle kappa. Normal x-coordinate 200 μm (or 5 ).
60 Pupil diameter Diameter of pupil in (photopicp mesopic scotopic). Adjusting optical zone(oz)diameter, mm larger than the scotopic pupil size.
61 5-K readings Normal maximum not more than 49D Normal minimum not less than 34D The normal difference between K max and the steep less than 1.00 D.
62 5-K readings Flat myopia The rule D correction reduces the flat K by 0.75 D. The final flat sim K should not go below D, or positive spherical aberration will be induced
63 5-K readings Steep Hyperopia The rule each 1.00 D correction increase the K max 1.20 D The final K max should not exceed D; otherwise, negative spherical aberrations are induced..

64 Measure the spherical aberration Measurement undertaken At 6mm diameter at 4 meridian Q value Sum. Vertical is most important (Normal vertical Aspheric cornea with least spherical apparition )


65 Q value (spherical aberration) -2 advanced keratoconus or after hyperopia correction+5-1 moderate keratoconus or after hyperopia correction Vertical normal Aspheric cornea with least spherical apparition 0 spherical cornea with spherical apparition +1 after correction of -5 myopia +2 after correction of -12 myopia

66
67 CONCLUSIONS Refractive surgery is safe and effective Strict anatomic and refractive rules apply Age considerations are important Impressive technological advancements Adhere to the guidelines Meticulous examination and measurements Better safe than sorry
68 Thank you

69
70 6-Topographic astigmatism.. Disparity between these Topographic and manifest astigmatism 1-misalignment during capture, 2-irregular astigmatism, 3-tear film disturbance, 4-corneal haze 5-lenticular astigmatism (including subtle cataract).
71 Disparity between Topographic astigmatism and manifest astigmatism. If lenticular astigmatism is present without cataract and there is disparity, avoid overcorrection or converting the orientation of the topographic astigmatism -/-3x180 corrected as -0.5/-2x180
72 Disparity between Topographic astigmatism and manifest astigmatism. For example, if the manifest astigmatism is X 180º and the topographic astigmatism is X 180º, correcting the full manifest astigmatism will induce X 90º, which the patient may not tolerate despite zero manifest refraction. In such a case, one of the recommendations is to correct X 180º and adjust the sphere to achieve the same spherical equivalent (eg, X 180º corrected to X 180º.
73 7-Pupil coordinates. The horizontal (x) coordinate of the pupil center reflects angle kappa. The normal value of the latter is less than 100 μm (<5 ). Angle kappa is important for the decentration technique used in hyperopic and highly astigmatic photorefractive correction. A large angle kappa can also explain the skew seen in some curvature and elevation patterns.
74 General guidelines Thickness Rules K-reading Rules Astigmatism Rules Pupil Center and Angle Kappa Rules
75 Thickness Rules Munnerlyn formula calculates the ablation depth (AD) for myopia and myopic astigmatism: AD (μm) = 1/3 (OZ diameter [mm])2 (intended correction [D])..

76 Scotopic The range of low light levels below cone threshold where visual responses has only rod signals Mesopic The range of intermediate light levels between cone threshold and rod saturation Photopic The range of high light levels above rod saturation where vision is mediated by signals from cone photoreceptors. Pupil diameter
77 Thickness Rules When Scotopic pupil >5.5mm Do Ablation OZ = 6.5 mm When Scotopic pupil <5mm Do Aplation OZ = 5.5 mm So 1D Ablate 14um. 1D Ablate 10um In small thickness save tissue
78 RSB Rule 1 Thickness Rules The RSB should be at least 300um
79 RSB Rule 2 Thickness Rules The AD should be at most 20% of the original corneal thickness at the TL..
80 RSB Rule 3 Thickness Rules In LASIK, the AD differs according to OZ diameter and laser profile. For easy calculations, 15 μm will be used... Aplation OZ = 5.5 mm 1D = 10um Ablation OZ = 6.5 mm 1D = 14um
81 Thickness Rules RSB Rule 4 For safety, Least ablation depth Most residual stromal bed.
82 RSB Rule 5 Thickness Rules AD In PRK, not to exceed 70-80μ to avoid haze, Corrected about 6 D(X15) Final residual stoma not less than 400um.
83 RSB Rule 6 Thickness Rules In LASIK and PRK, use the absolute sum of the spherical and cylindrical components 4 D sph/ 3 D = 7x15.
84 RSB Rule 7 Thickness Rules In hyperopic treatment the central ablation is zero, whereas the maximum AD is peripheral where the cornea is thick. Try correct up to +4 D by LASIK in order to minimize biomechanical response In general, the preoperative TL should be > 470 μm.
85 RSB Rule 8 Thickness Rules For calculations in mixed astigmatism, The equation should be converted into plus cylinder formula before calculating the RSB. +2 D sph/ 4 D cyl converted to 2 D sph/+4 D cyl RSB rules are applied on the 2 D sph
86 RSB Rule 9 Thickness Rules In WFGT profiles, the AD differs according to the type and severity of HOA(s). Therefore, AD and RSB should be calculated on site.
87 General guidelines Thickness Rules K-reading Rules Astigmatism Rules Pupil Center and Angle Kappa Rule
88 K-reading Rules First The recommended amount of correction should be calculated according to RSB rules Second then according to K-reading rules.
89 K-reading Rules Flat K Rule Correcting each 1 D reduces the flat K by 0.75 D. Final flat K according to the amount of myopic ablation should be > 34 D.
90 K-reading Rules K-max Rule Correcting each +1 D increases K-max by 1.2 D. K-max according to the amount of hyperopic ablation should be < 49 D.
91 Flat K Rule K-reading Rules K-max Rule Correcting each 1 D reduces the flat K by 0.75 D. Correcting each +1 D increases K-max by 1.2 D. The final flat K > 34 D. The final steep K < 49 D.
92 General guidelines Thickness Rules K-reading Rules Astigmatism Rules Pupil Center and Angle Kappa Rule

93 Astigmatism Rules Myopic Astigmatism Rules The astigmatic correction flattens the steep K and brings it to flat K Thereafter, the spherical correction flattens all.

94 Astigmatism Rules Hyperopic Astigmatism Rules the astigmatic correction steepens the flat K and brings it to steepk. Thereafter, the spherical correction steepens all.

95 Astigmatism Rules Mixed Astigmatism Rules The astigmatic correction steepens the flat K and brings it to steep K Thereafter, the spherical correction flattens all.
96 General guidelines Thickness Rules K-reading Rules Astigmatism Rules Pupil Center and Angle Kappa Rule

97 Pupil Center and Angle Kappa Rule Angle Kappa is the angle between the visual axis and the axis that passes through the pupil center.. Angle Kappa Angle kappa is considered significant when it is > 5 (x > 200 μm).

98
99 Large angle Kapa When angle kappa is > 100 μm (x > 200 μm), the capture should be repeated to exclude misalignment. 1-false positives or false negatives such as the skewed hourglass pattern in elevation maps. 2- When treating hyperopia or 2 D of astigmatism, optimal resul ts can be achieved when the center of ablation coincides with the optical axis of the eye. This can be achieved by decentering the ablation profile for the amount of angle kappa; this is called offset pupil or decentration. 3-Finally, decentered pupil (corectopia) is a case of concern, especially when PIOL implantation is indicated.
100 Thank you
101 -Keratometry readings (k1, k2)- -Radii of curvature (Rh, Rv), -Mean keratometry mm zone (Km),
102 Pachymetry data of the 1-Pupil center, 2- apex, 3- thinnest point, and their locations are followed by maximum curvature amount and location..

103 Isolated island in front or back with normal elevation

104 Topometric Map The most important is vertical inferior Normal < -0.5 Border line -0.5 and Abnormal> The most important sector is the 6 mm or 20 sector
Abdel Rahman ElSebaey, MD, PhD.
 Surface Ablation Refractive Surgery Abdel Rahman ElSebaey, MD, PhD. Menoufia University History Correction of optical defects of human eye started 1200 AD. Spherical error corrected by spectacle on 13
Surface Ablation Refractive Surgery Abdel Rahman ElSebaey, MD, PhD. Menoufia University History Correction of optical defects of human eye started 1200 AD. Spherical error corrected by spectacle on 13
Interpretation of corneal tomography
 Interpretation of corneal tomography Presented by Chameen Samarawickrama - Westmead Hospital - Liverpool Hospital - University of Sydney - University of New South Wales The University of Sydney Page 1
Interpretation of corneal tomography Presented by Chameen Samarawickrama - Westmead Hospital - Liverpool Hospital - University of Sydney - University of New South Wales The University of Sydney Page 1
Refractive Surgery Dilemma
 Refractive Surgery Dilemma Section Editor: lireza aradaran-rafii, MD CSE PRESENTTION 33-year-old man seeking refractive surgery presented with refractive error of -1.75-4.0 20 in the right and -0.75-2.5
Refractive Surgery Dilemma Section Editor: lireza aradaran-rafii, MD CSE PRESENTTION 33-year-old man seeking refractive surgery presented with refractive error of -1.75-4.0 20 in the right and -0.75-2.5
Intrastromal corneal ring
 Intrastromal corneal ring Kyriakidou Nantia M.D. Diathlasis Day Care Unit Scienti1ic Workshop of Diathlasis Day Care Unit 18-19 November, 2016 The Met Hotel Thessaloniki, Greece DAY CARE UNIT DIATHLASIS,
Intrastromal corneal ring Kyriakidou Nantia M.D. Diathlasis Day Care Unit Scienti1ic Workshop of Diathlasis Day Care Unit 18-19 November, 2016 The Met Hotel Thessaloniki, Greece DAY CARE UNIT DIATHLASIS,
Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB
 Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB Cleveland Clinic Cole Eye Institute OOS, Columbus, OH February, 2014 alkhawf@ccf.org NO FINANCIAL DISCLOSURES A Puzzle of an Eye
Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB Cleveland Clinic Cole Eye Institute OOS, Columbus, OH February, 2014 alkhawf@ccf.org NO FINANCIAL DISCLOSURES A Puzzle of an Eye
SCHWIND CAM Perfect Planning wide range of applications
 SCHWIND CAM Perfect Planning wide range of applications ORK-CAM PresbyMAX PTK-CAM 2 SCHWIND CAM the system solution The modular design of the SCHWIND CAM offers customised treatment planning for a uniquely
SCHWIND CAM Perfect Planning wide range of applications ORK-CAM PresbyMAX PTK-CAM 2 SCHWIND CAM the system solution The modular design of the SCHWIND CAM offers customised treatment planning for a uniquely
Doctors of Optometry Course Notes
 Doctors of Optometry Course Notes OD22 1 CE Contact Lens Management of the Irregular Cornea Monday, February 19, 2018 9:05 am 10:00 am Plaza A 2 nd Fl Presenter: Dr. Maria Walker Dr. Maria K. Walker earned
Doctors of Optometry Course Notes OD22 1 CE Contact Lens Management of the Irregular Cornea Monday, February 19, 2018 9:05 am 10:00 am Plaza A 2 nd Fl Presenter: Dr. Maria Walker Dr. Maria K. Walker earned
SCLERAL CONTACT LENSES EPSILON SCLERAL
 SCLERAL CONTACT LENSES EPSILON SCLERAL - Outstands due to multi aspheric variable eccentricity design - Fitted in two steps due to it s novel philosophy and diagnostic set - Reassures limbal stem cells
SCLERAL CONTACT LENSES EPSILON SCLERAL - Outstands due to multi aspheric variable eccentricity design - Fitted in two steps due to it s novel philosophy and diagnostic set - Reassures limbal stem cells
Recent concerns regarding the depth of tissue ablation with
 Volume Estimation of Excimer Laser Tissue Ablation for Correction of Spherical Myopia and Hyperopia Damien Gatinel, 1 Thanh Hoang-Xuan, 1 and Dimitri T. Azar 1,2 PURPOSE. To determine the theoretical volumes
Volume Estimation of Excimer Laser Tissue Ablation for Correction of Spherical Myopia and Hyperopia Damien Gatinel, 1 Thanh Hoang-Xuan, 1 and Dimitri T. Azar 1,2 PURPOSE. To determine the theoretical volumes
Simultaneous Topography-guided Surface Ablation with Collagen Cross-linking for Keratoconus
 IJKECD Case series Simultaneous Topography-guided Surface Ablation with Collagen 10.5005/jp-journals-10025-1124 Cross-linking for Keratoconus Simultaneous Topography-guided Surface Ablation with Collagen
IJKECD Case series Simultaneous Topography-guided Surface Ablation with Collagen 10.5005/jp-journals-10025-1124 Cross-linking for Keratoconus Simultaneous Topography-guided Surface Ablation with Collagen
Keratoconus Clinic. Optometric Co-management Opportunities
 Keratoconus Clinic Optometric Co-management Opportunities The Bochner Eye Institute established the first Keratoconus Clinic in Canada in 2008. The consultation and advanced imaging are OHIP covered. All
Keratoconus Clinic Optometric Co-management Opportunities The Bochner Eye Institute established the first Keratoconus Clinic in Canada in 2008. The consultation and advanced imaging are OHIP covered. All
pre-laser cut pre-laser cut Pre-operative Known and Potential Complications of SMILE Failure to obtain an adequate suction
 pre-laser cut! Known and Potential Complications of SMILE Failure to obtain an adequate suction Walter Sekundo Correct treatment pack size (S in myopic cases) Philipps University Marburg/Germany Use speculum
pre-laser cut! Known and Potential Complications of SMILE Failure to obtain an adequate suction Walter Sekundo Correct treatment pack size (S in myopic cases) Philipps University Marburg/Germany Use speculum
SCLERAL CONTACT LENSES 1. EPSILON SCLERAL
 SCLERAL CONTACT LENSES 1. EPSILON SCLERAL - Out stands due to multi aspheric variable eccentricity design - Fitted in two steps due to it s novel philosophy and diagnostic set - Reassures limbal stem cells
SCLERAL CONTACT LENSES 1. EPSILON SCLERAL - Out stands due to multi aspheric variable eccentricity design - Fitted in two steps due to it s novel philosophy and diagnostic set - Reassures limbal stem cells
Scleral Lenses: How do you know what is best
 Scleral Lenses: How do you know what is best Alan Kwok, OD, FAAO, FSLS Tar Vaz, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this
Scleral Lenses: How do you know what is best Alan Kwok, OD, FAAO, FSLS Tar Vaz, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this
Uday Devgan MD Private Practice, Devgan Eye Surgery, Los Angeles
 Irregular Astigmatism & honing your K incision Uday Devgan MD Private Practice, Devgan Eye Surgery, Los Angeles Uday Devgan MD Current Disclosures: Aaren Scientific: consultant Accutome Inc: royalties
Irregular Astigmatism & honing your K incision Uday Devgan MD Private Practice, Devgan Eye Surgery, Los Angeles Uday Devgan MD Current Disclosures: Aaren Scientific: consultant Accutome Inc: royalties
A procedure for Present and Future
 A procedure for Present and Future MOSTAFA M. SALAH MD PROFESSOR Head of Refractive Unit RESEARCH INSTITUTE OF OPHTHALMOGY CAIRO -EGYPT 1 THIN FLAP LASIK DEF. Creation of Intended regular thin flap less
A procedure for Present and Future MOSTAFA M. SALAH MD PROFESSOR Head of Refractive Unit RESEARCH INSTITUTE OF OPHTHALMOGY CAIRO -EGYPT 1 THIN FLAP LASIK DEF. Creation of Intended regular thin flap less
2/7/18. Disclosures: Laser K s: Keratectomy to Keratomileusis with a SMILE. Who Patients Are Listening to
 Disclosures: Laser K s: Keratectomy to Keratomileusis with a SMILE Glaukos Equinox Alcon Mitch Ibach OD, FAAO Vance Thompson Vision Who Patients Are Listening to Optometrist 36% People who've had surgery
Disclosures: Laser K s: Keratectomy to Keratomileusis with a SMILE Glaukos Equinox Alcon Mitch Ibach OD, FAAO Vance Thompson Vision Who Patients Are Listening to Optometrist 36% People who've had surgery
In Practice. Surgical Procedures Diagnosis New Drugs
 In Practice Surgical Procedures Diagnosis New Drugs 62 65 A New Carpet Over Broken Tiles Facing an eye with multiple, deep radial keratotomy cuts? Arun Gulani describes how the right mindset and technique
In Practice Surgical Procedures Diagnosis New Drugs 62 65 A New Carpet Over Broken Tiles Facing an eye with multiple, deep radial keratotomy cuts? Arun Gulani describes how the right mindset and technique
EUROTIMES ESCRS SUPPLEMENT FEBRUARY 2007
 Pentacam opens eyes to new diagnostic possibilities Scheimpflug based anterior segment tomography EUROTIMES ESCRS SUPPLEMENT FEBRUARY 2007 XXIV Congress of the ESCRS London, September 2006 Introduction
Pentacam opens eyes to new diagnostic possibilities Scheimpflug based anterior segment tomography EUROTIMES ESCRS SUPPLEMENT FEBRUARY 2007 XXIV Congress of the ESCRS London, September 2006 Introduction
The pinnacle of refractive performance.
 The pinnacle of refractive performance. WaveLight REFRACTIVE PORTFOLIO Advancing REFRACTIVE SURGERY Contoura Vision sets a new standard in LASIK outcomes More than 98% of patients would choose it again.
The pinnacle of refractive performance. WaveLight REFRACTIVE PORTFOLIO Advancing REFRACTIVE SURGERY Contoura Vision sets a new standard in LASIK outcomes More than 98% of patients would choose it again.
MEDICAL POLICY No R3 REFRACTIVE KERATOPLASTY / LASIK
 REFRACTIVE KERATOPLASTY / LASIK Effective Date: November 10, 2017 Review Dates: 7/07, 6/08, 6/09, 6/10, 8/10, 8/11, 8/12, 8/13, 8/14, 8/15, 8/16, 8/17 Date Of Origin: July 2007 Status: Current Summary
REFRACTIVE KERATOPLASTY / LASIK Effective Date: November 10, 2017 Review Dates: 7/07, 6/08, 6/09, 6/10, 8/10, 8/11, 8/12, 8/13, 8/14, 8/15, 8/16, 8/17 Date Of Origin: July 2007 Status: Current Summary
NEW VISION EYE CENTER
 Topographic Aberrometric Guided PRK For Keratoconus With Accelerated Corneal Cross-Linking Using Schwind AMARIS 750S Laser NEW VISION EYE CENTER Dr. Safwan Al Bayati FRCS (Glasgow) FICMS OPTH Consultant
Topographic Aberrometric Guided PRK For Keratoconus With Accelerated Corneal Cross-Linking Using Schwind AMARIS 750S Laser NEW VISION EYE CENTER Dr. Safwan Al Bayati FRCS (Glasgow) FICMS OPTH Consultant
Moving from Rx to measured
 Moving from Rx to measured The news magazine of the American Society of Cataract & Refractive Surgery Supplement to EyeWorld Daily News Sunday, May 7, 2017 Contoura Vision TopographyGuided Ablation Algorithms
Moving from Rx to measured The news magazine of the American Society of Cataract & Refractive Surgery Supplement to EyeWorld Daily News Sunday, May 7, 2017 Contoura Vision TopographyGuided Ablation Algorithms
POST-LASIK ECTASIA MANAGEMENT
 POST-LASIK ECTASIA MANAGEMENT A. John Kanellopoulos MD 1,2 1: Laservision.gr Clinical & Research Eye Institute, Athens, Greece 2: NYU Medical School Department of Ophthalmology, NY, NY Financial interests:
POST-LASIK ECTASIA MANAGEMENT A. John Kanellopoulos MD 1,2 1: Laservision.gr Clinical & Research Eye Institute, Athens, Greece 2: NYU Medical School Department of Ophthalmology, NY, NY Financial interests:
Management of Unpredictable Post-PRK Corneal Ectasia with Intacs Implantation
 Management of Unpredictable Post-PRK Corneal Ectasia with Intacs Implantation Mohammad Naser Hashemian, MD 1 Mahdi AliZadeh, MD 2 Hassan Hashemi, MD 1,3 Firoozeh Rahimi, MD 4 Abstract Purpose: To present
Management of Unpredictable Post-PRK Corneal Ectasia with Intacs Implantation Mohammad Naser Hashemian, MD 1 Mahdi AliZadeh, MD 2 Hassan Hashemi, MD 1,3 Firoozeh Rahimi, MD 4 Abstract Purpose: To present
Description of iatrogenic corneal ectasia in patients without traditional risk factors
 ARTICLE Description of iatrogenic corneal ectasia in patients without traditional risk factors Julio Ortega-Usobiaga, MD, PhD 1 ; Rosario Cobo-Soriano, MD, PhD 1 ; Fernando Llovet-Osuna, MD, PhD 1 ; Stephan
ARTICLE Description of iatrogenic corneal ectasia in patients without traditional risk factors Julio Ortega-Usobiaga, MD, PhD 1 ; Rosario Cobo-Soriano, MD, PhD 1 ; Fernando Llovet-Osuna, MD, PhD 1 ; Stephan
Cataract Surgery in the Patient with a History of LASIK or PRK
 Cataract Surgery in the Patient with a History of LASIK or PRK #56996-RS April 2018 Sebastian Lesniak, MD Matossian Eye Associates None Disclosures Bio Matossian Eye Associates, Hopewell NJ, 7/2015 Present
Cataract Surgery in the Patient with a History of LASIK or PRK #56996-RS April 2018 Sebastian Lesniak, MD Matossian Eye Associates None Disclosures Bio Matossian Eye Associates, Hopewell NJ, 7/2015 Present
CATARACT SURGERY AFTER RADIAL KERATOTOMY
 AFTER RADIAL KERATOTOMY How to avoid disappointment. BY BERNARD MATHYS, MD CATARACT SURGERY Radial keratotomy (RK; Figure 1) was a popular refractive surgical procedure to correct myopia in the 1970s and
AFTER RADIAL KERATOTOMY How to avoid disappointment. BY BERNARD MATHYS, MD CATARACT SURGERY Radial keratotomy (RK; Figure 1) was a popular refractive surgical procedure to correct myopia in the 1970s and
Research Article Risk Assessment for Corneal Ectasia following Photorefractive Keratectomy
 Hindawi Journal of Ophthalmology Volume 17, Article ID 24348, pages https://doi.org/.1155/17/24348 Research Article Risk Assessment for Corneal Ectasia following Photorefractive Keratectomy Nir Sorkin,
Hindawi Journal of Ophthalmology Volume 17, Article ID 24348, pages https://doi.org/.1155/17/24348 Research Article Risk Assessment for Corneal Ectasia following Photorefractive Keratectomy Nir Sorkin,
L. Spadea, R. Ferrante, F. Romani, A. Di Gregorio
 University of L Aquila Eye Clinic Head: Prof. Leopoldo Spadea ULTRAFAST EXCIMER LASER FOR TRANS-EPITHELIAL CUSTOMIZED PHOTOREFRACTIVE SURGERIES: CLINICAL RESULTS WITH 6 MONTHS FOLLOW UP L. Spadea, R. Ferrante,
University of L Aquila Eye Clinic Head: Prof. Leopoldo Spadea ULTRAFAST EXCIMER LASER FOR TRANS-EPITHELIAL CUSTOMIZED PHOTOREFRACTIVE SURGERIES: CLINICAL RESULTS WITH 6 MONTHS FOLLOW UP L. Spadea, R. Ferrante,
THE PENTACAM AXL. Improving Cataract Surgery Outcomes. Optical biometry and anterior segment tomography in one device
 Insert to November/December 2016 Sponsored by OCULUS THE PENTACAM AXL Improving Cataract Surgery Outcomes Optical biometry and anterior segment tomography in one device A New Way to Calculate IOL Power
Insert to November/December 2016 Sponsored by OCULUS THE PENTACAM AXL Improving Cataract Surgery Outcomes Optical biometry and anterior segment tomography in one device A New Way to Calculate IOL Power
LASER REFRACTIVE CENTER INFORMED CONSENT DOCUMENT SMALL INCISION LENTICULE EXTRACTION (SMILE)
") GENERAL INFORMATION The purpose of this document is to provide written information regarding the risks, benefits and alternatives of Small Incision Lenticule Extraction. This material serves as a supplement
GENERAL INFORMATION The purpose of this document is to provide written information regarding the risks, benefits and alternatives of Small Incision Lenticule Extraction. This material serves as a supplement
ONE THOUSAND WAVEFRONT GIDED TREATMENT ON MICROSCAN VISUM. Mickael Yablokov. I have no any financial interests in any products mentioned in this paper
 ONE THOUSAND WAVEFRONT GIDED TREATMENT ON MICROSCAN VISUM Mickael Yablokov I have no any financial interests in any products mentioned in this paper Ophthalmology clinic Eye Surgery, Kostroma, Russia Goal
ONE THOUSAND WAVEFRONT GIDED TREATMENT ON MICROSCAN VISUM Mickael Yablokov I have no any financial interests in any products mentioned in this paper Ophthalmology clinic Eye Surgery, Kostroma, Russia Goal
Premium Implant Options for the Cataract Patient. Justin Schweitzer, OD, FAAO Vance Thompson Vision Sioux Falls, South Dakota
 Premium Implant Options for the Cataract Patient Justin Schweitzer, OD, FAAO Vance Thompson Vision Sioux Falls, South Dakota Glaukos Bausch and Lomb Alcon Allergan Bio- Tissue TearScience Reichert Trends
Premium Implant Options for the Cataract Patient Justin Schweitzer, OD, FAAO Vance Thompson Vision Sioux Falls, South Dakota Glaukos Bausch and Lomb Alcon Allergan Bio- Tissue TearScience Reichert Trends
Louis Probst. Commitment to Optometry. Cycloplegic Exam. Steroid free PRK. LASIK Enhancements made Ridiculously Simple 8/18/2017
 Louis Probst LASIK Enhancements made Ridiculously Simple Louis E. Probst MD National Medical Director, TLC Chief Surgeon, Central Midwest, USA TLC surgeon 22 years 7 books, 80 chapters, 50 papers, 11 instruments
Louis Probst LASIK Enhancements made Ridiculously Simple Louis E. Probst MD National Medical Director, TLC Chief Surgeon, Central Midwest, USA TLC surgeon 22 years 7 books, 80 chapters, 50 papers, 11 instruments
Anterior segment imaging
 CET CONTINUING Sponsored by 1 CET POINT Anterior segment imaging Sundeep Vaswani, BSc (Hons), MCOptom 39 The anterior segment of the eye encompasses all structures from the front surface of the cornea
CET CONTINUING Sponsored by 1 CET POINT Anterior segment imaging Sundeep Vaswani, BSc (Hons), MCOptom 39 The anterior segment of the eye encompasses all structures from the front surface of the cornea
REFRACTIVE LENS SURGERY: WHEN AND WHY?
 REFRACTIVE LENS SURGERY: WHEN AND WHY? Symposium of the Hellenic Society of Intraocular Implant and Refractive Surgery Cairo, 14/3/2018 Pandelis A. Papadopoulos, MD, PhD, FEBO, FEBOS-CR Director, Ophthalmology
REFRACTIVE LENS SURGERY: WHEN AND WHY? Symposium of the Hellenic Society of Intraocular Implant and Refractive Surgery Cairo, 14/3/2018 Pandelis A. Papadopoulos, MD, PhD, FEBO, FEBOS-CR Director, Ophthalmology
Topo-Guided Custom Ablation (TGCA) and Corneal Collagen Cross-Linking (CCL) in treatment of advanced keratoectasia
 and Corneal Collagen Cross-Linking (CCL) in treatment of advanced keratoectasia") Topo-Guided Custom Ablation (TGCA) and Corneal Collagen Cross-Linking (CCL) in treatment of advanced keratoectasia Alekandar Stojanovic, MD University Hospital North Norway Tromsø, Norway Jia Zhang, MD
Topo-Guided Custom Ablation (TGCA) and Corneal Collagen Cross-Linking (CCL) in treatment of advanced keratoectasia Alekandar Stojanovic, MD University Hospital North Norway Tromsø, Norway Jia Zhang, MD
Cataract and cornea. Miltos O. Balidis PhD, FEBOphth,ICOphth ATHENS
 Cataract and cornea Miltos O. Balidis PhD, FEBOphth,ICOphth CATARACT and Stromal opacities Keratoplasty Keratoconus Endothelial pathology Scars PTK Trypan blue 0.01%. Work at the transparent side of cornea
Cataract and cornea Miltos O. Balidis PhD, FEBOphth,ICOphth CATARACT and Stromal opacities Keratoplasty Keratoconus Endothelial pathology Scars PTK Trypan blue 0.01%. Work at the transparent side of cornea
Innovation, Leadership, Passion for Perfection
 Innovation, Leadership, Passion for Perfection efocus P A C I F I C V I S I O N I N S T I T U T E Issue 052 415.922.9500 www.pacificvision.org May 2018 Bay Area optometrists observing topography-guided
Innovation, Leadership, Passion for Perfection efocus P A C I F I C V I S I O N I N S T I T U T E Issue 052 415.922.9500 www.pacificvision.org May 2018 Bay Area optometrists observing topography-guided
ADVANCED PLANNING DEVICES
 ADVANCED PLANNING DEVICES Surgeons discuss the strengths and weaknesses of four systems. The Galilei BY NEEL R. DESAI, MD It is no coincidence that the biometric analysis of potential refractive cataract
ADVANCED PLANNING DEVICES Surgeons discuss the strengths and weaknesses of four systems. The Galilei BY NEEL R. DESAI, MD It is no coincidence that the biometric analysis of potential refractive cataract
Clinical Policy: Refractive Surgery Reference Number: CP.MP. 391
 Clinical Policy: Refractive Surgery Reference Number: CP.MP. 391 Effective Date: November 2007 Last Review Date: January 2016 Coding Implications Revision Log See Important Reminder at the end of this
Clinical Policy: Refractive Surgery Reference Number: CP.MP. 391 Effective Date: November 2007 Last Review Date: January 2016 Coding Implications Revision Log See Important Reminder at the end of this
Bilateral Keratectasia 34 Years after Corneal Transplant
 24 Bilateral Keratectasia 34 Years after Corneal Transplant Xavier Valldeperas a, b Martina Angi b, c Vito Romano d Mario R. Romano b, e a Department of Ophthalmology, Hospital Universitari Germans Trias
24 Bilateral Keratectasia 34 Years after Corneal Transplant Xavier Valldeperas a, b Martina Angi b, c Vito Romano d Mario R. Romano b, e a Department of Ophthalmology, Hospital Universitari Germans Trias
Nature and Science 2017;15(11) Mohamed Elmoddather. MD
 Mohamed Elmoddather. MD") Outcome of PRK in Management of Post LISIK Residual Myopia and Myopic Astigmatism Mohamed Elmoddather. MD Ophthalmology Faculty of Medicine, Al-Azhar University, Assuit, Egypt shahdmsaleh@hotmail.com Abstract:
Outcome of PRK in Management of Post LISIK Residual Myopia and Myopic Astigmatism Mohamed Elmoddather. MD Ophthalmology Faculty of Medicine, Al-Azhar University, Assuit, Egypt shahdmsaleh@hotmail.com Abstract:
Our experience with Athens protocol - simultaneous topo-guided photorefractive keratectomy followed by corneal collagen cross linking for keratoconus
 International Journal of Research in Medical Sciences Shah S et al. Int J Res Med Sci. 2016 Jul;4(7):2639-2644 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20161924
International Journal of Research in Medical Sciences Shah S et al. Int J Res Med Sci. 2016 Jul;4(7):2639-2644 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20161924
Trans Epithelial Surface Ablation A personal reflection over a collective experience
 Trans Epithelial Surface Ablation A personal reflection over a collective experience Dr S Mughal MBChB MSc FRCS(Glasg) MRCOphth DRCOphth CertLRS SCHWIND USERS LECTURE, BOOTH C13 ESCRS CONGRESS LONDON 2014
Trans Epithelial Surface Ablation A personal reflection over a collective experience Dr S Mughal MBChB MSc FRCS(Glasg) MRCOphth DRCOphth CertLRS SCHWIND USERS LECTURE, BOOTH C13 ESCRS CONGRESS LONDON 2014
The two currently accepted methods for correcting
 New Technique Therapeutic Alloplastic Laser in situ Keratomileusis for Myopia Arturo Maldonado-Bas, MD; Ruben Pulido-Garcia, MD ABSTRACT BACKGROUND: A new technique, therapeutic alloplastic laser in situ
New Technique Therapeutic Alloplastic Laser in situ Keratomileusis for Myopia Arturo Maldonado-Bas, MD; Ruben Pulido-Garcia, MD ABSTRACT BACKGROUND: A new technique, therapeutic alloplastic laser in situ
Original Article High myopia as a risk factor for post-lasik ectasia: a case report
 Original Article High myopia as a risk factor for post-lasik ectasia: a case report Mona Harissi-Dagher, MD, a,b Sonja A. F. Frimmel, c and Samir Melki, MD, PhD a,d Author affiliations: a Massachusetts
Original Article High myopia as a risk factor for post-lasik ectasia: a case report Mona Harissi-Dagher, MD, a,b Sonja A. F. Frimmel, c and Samir Melki, MD, PhD a,d Author affiliations: a Massachusetts
Laser in situ keratomileusis (LASIK) has proven to be
 has proven to be") Autorefractometry after laser in situ keratomileusis Dimitrios S. Siganos, MD, PhD, Corina Popescu, MD, Nikolaos Bessis, DOpt, Georgios Papastergiou, MD Purpose: To correlate cycloplegic subjective refraction
Autorefractometry after laser in situ keratomileusis Dimitrios S. Siganos, MD, PhD, Corina Popescu, MD, Nikolaos Bessis, DOpt, Georgios Papastergiou, MD Purpose: To correlate cycloplegic subjective refraction
SynergEyes PS Practitioner Training
 SynergEyes PS Practitioner Training Post-Surgical Market For 30 years, visual scientists from around the world have struggled with the challenge of surgically correcting human refractive error. While great
SynergEyes PS Practitioner Training Post-Surgical Market For 30 years, visual scientists from around the world have struggled with the challenge of surgically correcting human refractive error. While great
Trans Epithelial Surface Ablation A personal reflection over a collective experience
 Trans Epithelial Surface Ablation A personal reflection over a collective experience Dr S Mughal MBChB MSc FRCS(Glasg) MRCOphth DRCOphth CertLRS 15th International SCHWIND User Meeting July 17-20, 2014
Trans Epithelial Surface Ablation A personal reflection over a collective experience Dr S Mughal MBChB MSc FRCS(Glasg) MRCOphth DRCOphth CertLRS 15th International SCHWIND User Meeting July 17-20, 2014
Contoura TM Vision Correction
 Contoura TM Vision Correction Fernando Faria Correia, Financial Disclosures: Alcon/Wavelight Cairo (Egypt) 26/01/2018 Topography-guided ablations Topography guided ablations Evolution from complicated
Contoura TM Vision Correction Fernando Faria Correia, Financial Disclosures: Alcon/Wavelight Cairo (Egypt) 26/01/2018 Topography-guided ablations Topography guided ablations Evolution from complicated
Medical Affairs Policy
 Medical Affairs Policy Service: Corneal Treatments and Specialized Contact Lenses (Corneal remodeling, Corneal transplant, Corneal collagen crosslinking, Intrastromal Rings- INTACS, Keratoconus treatments,
Medical Affairs Policy Service: Corneal Treatments and Specialized Contact Lenses (Corneal remodeling, Corneal transplant, Corneal collagen crosslinking, Intrastromal Rings- INTACS, Keratoconus treatments,
UPDATES OF REFRACTIVE SURGERY اليوم العلمي الثالث قسم البصريات كلية العلوم الصحية 14/3/2015
 UPDATES OF REFRACTIVE SURGERY اليوم العلمي الثالث قسم البصريات كلية العلوم الصحية 14/3/2015 1 Basic knowledge Refraction Refraction is the bending of light rays as they pass from one transparent medium
UPDATES OF REFRACTIVE SURGERY اليوم العلمي الثالث قسم البصريات كلية العلوم الصحية 14/3/2015 1 Basic knowledge Refraction Refraction is the bending of light rays as they pass from one transparent medium
Patient Information: laser vision correction
 Consultation Document Patient Information: laser vision correction April 2016 Contents Section page 1 What is Laser Vision Correction? 3 2 What are the benefits? 3 3 How much does laser vision correction
Consultation Document Patient Information: laser vision correction April 2016 Contents Section page 1 What is Laser Vision Correction? 3 2 What are the benefits? 3 3 How much does laser vision correction
US Trends in Refractive Surgery: The 2008 ISRS/AAO Survey
 US Trends in Refractive Surgery: The 2008 ISRS/AAO Survey Richard J. Duffey, MD ** David Leaming, MD Refractive Subspecialty Day Atlanta - November 8, 2008 ** TLCV provided partial funding for this survey
US Trends in Refractive Surgery: The 2008 ISRS/AAO Survey Richard J. Duffey, MD ** David Leaming, MD Refractive Subspecialty Day Atlanta - November 8, 2008 ** TLCV provided partial funding for this survey
~ 1 ~ CLINIQUE LASERVUE. Informed Consent Form for LASIK
 ~ 1 ~ CLINIQUE LASERVUE Informed Consent Form for LASIK Please read the following information and consent form very carefully. Your initials indicate that you understand all of the necessary patient information
~ 1 ~ CLINIQUE LASERVUE Informed Consent Form for LASIK Please read the following information and consent form very carefully. Your initials indicate that you understand all of the necessary patient information
efocus Issue 041 August 2011 Excellence in Co-Managed Care
 Issue 041 August 2011 efocus Excellence in Co-Managed Care P A C I F I C V I S I O N I N S T I T U T E Life in Focus 415.922.9500 www.pacificvision.org Pacific Vision Institute Video Workshop in Cataract
Issue 041 August 2011 efocus Excellence in Co-Managed Care P A C I F I C V I S I O N I N S T I T U T E Life in Focus 415.922.9500 www.pacificvision.org Pacific Vision Institute Video Workshop in Cataract
Photochemical corneal collagen cross-linkage using riboflavin and ultraviolet A for keratoconus and keratectasia
 Photochemical corneal collagen cross-linkage using riboflavin and ultraviolet A for keratoconus and keratectasia Issued: September 2013 guidance.nice.org.uk/ipg466 NICE has accredited the process used
Photochemical corneal collagen cross-linkage using riboflavin and ultraviolet A for keratoconus and keratectasia Issued: September 2013 guidance.nice.org.uk/ipg466 NICE has accredited the process used
Corneal Remodeling. Medical Coverage Policy. Related Coverage Resources. Table of Contents. Coverage Policy. Corneal Crosslinking
 Medical Coverage Policy Effective Date... 8/15/2018 Next Review Date... 8/15/2019 Coverage Policy Number... 0141 Corneal Remodeling Table of Contents Coverage Policy... 1 Overview... 3 General Background...
Medical Coverage Policy Effective Date... 8/15/2018 Next Review Date... 8/15/2019 Coverage Policy Number... 0141 Corneal Remodeling Table of Contents Coverage Policy... 1 Overview... 3 General Background...
JACK T. HOLLADAY, MD, MSEE, FACS (MODERATOR) MICHAEL W. BELIN, MD, FACS ARTURO S. CHAYET, MD MATTHIAS MAUS, MD PAOLO VINCIGUERRA, MD
 MICHAEL W. BELIN, MD, FACS ARTURO S. CHAYET, MD MATTHIAS MAUS, MD PAOLO VINCIGUERRA, MD") Next-Generation Technology for the Cataract & Refractive Surgeon Produced under an unrestricted educational grant from Oculus, Inc., and Oculus Optikgeraete GmbH. This monograph is based on an educational
Next-Generation Technology for the Cataract & Refractive Surgeon Produced under an unrestricted educational grant from Oculus, Inc., and Oculus Optikgeraete GmbH. This monograph is based on an educational
Interventional procedures guidance Published: 25 September 2013 nice.org.uk/guidance/ipg466
 Photochemical corneal collagen cross-linkage using riboflavin and ultraviolet A for keratoconus and keratectasia Interventional procedures guidance Published: 25 September 2013 nice.org.uk/guidance/ipg466
Photochemical corneal collagen cross-linkage using riboflavin and ultraviolet A for keratoconus and keratectasia Interventional procedures guidance Published: 25 September 2013 nice.org.uk/guidance/ipg466
Clinical experience of 9,000 small aperture Inlays for presbyopia correction
 Clinical experience of 9,000 small aperture Inlays for presbyopia correction Minoru Tomita, MD, PhD Shinagawa LASIK Center, Tokyo, Japan September 7 th, 2012, ISOP meeting in Tokyo, JAPAN 1,060,666 Femto
Clinical experience of 9,000 small aperture Inlays for presbyopia correction Minoru Tomita, MD, PhD Shinagawa LASIK Center, Tokyo, Japan September 7 th, 2012, ISOP meeting in Tokyo, JAPAN 1,060,666 Femto
CLINICAL SCIENCES. Management of Post-LASIK Corneal Ectasia With Intacs Inserts
 Management of Post-LASIK Corneal Ectasia With Intacs Inserts One-Year Results CLINICAL SCIENCES George D. Kymionis, MD, PhD; Charalambos S. Siganos, MD, PhD; George Kounis, BSc; Nikolaos Astyrakakis, OD;
Management of Post-LASIK Corneal Ectasia With Intacs Inserts One-Year Results CLINICAL SCIENCES George D. Kymionis, MD, PhD; Charalambos S. Siganos, MD, PhD; George Kounis, BSc; Nikolaos Astyrakakis, OD;
2/6/2018 RAPID FIRE PANEL: CO-MANAGEMENT OF UNUSUAL SITUATIONS IN CATARACT SURGERY. Andrew Siedlecki, M.D. Richard Orlando, M.D.
 POLL QUESTION: HOW DID YOU DEVELOP THE CLINICAL SKILLS TO CO MANAGE RAPID FIRE PANEL: CO-MANAGEMENT OF UNUSUAL SITUATIONS IN CATARACT SURGERY Andrew Siedlecki, M.D. Richard Orlando, M.D. A) Working in
POLL QUESTION: HOW DID YOU DEVELOP THE CLINICAL SKILLS TO CO MANAGE RAPID FIRE PANEL: CO-MANAGEMENT OF UNUSUAL SITUATIONS IN CATARACT SURGERY Andrew Siedlecki, M.D. Richard Orlando, M.D. A) Working in
Clear Advantage Vision Correction Center INFORMED CONSENT FOR LASIK AND FEMTOSECOND LASER
 Clear Advantage Vision Correction Center INFORMED CONSENT FOR LASIK AND FEMTOSECOND LASER PLEASE READ THE FOLLOWING PAGES CAREFULLY AND INITIAL AND SIGN WHERE INDICATED. PLEASE DO NOT SIGN ANY SECTION
Clear Advantage Vision Correction Center INFORMED CONSENT FOR LASIK AND FEMTOSECOND LASER PLEASE READ THE FOLLOWING PAGES CAREFULLY AND INITIAL AND SIGN WHERE INDICATED. PLEASE DO NOT SIGN ANY SECTION
Managing residual postoperative error
 Managing residual postoperative error Michael Amon Academic Teaching Hospital of St. John Vienna Sigmund Freud Private University Vienna Financial disclosure: Alcon Bausch&Lomb Bayer Johnson&Johnson Morcher
Managing residual postoperative error Michael Amon Academic Teaching Hospital of St. John Vienna Sigmund Freud Private University Vienna Financial disclosure: Alcon Bausch&Lomb Bayer Johnson&Johnson Morcher
Fitting Keratoconus and Other Complicated Corneas
 Fitting Keratoconus and Other Complicated Corneas Christine W Sindt OD FAAO Professor, Clinical Ophthalmology Director, Contact Lens Service University of Iowa Disclosure Consultant: ALCON Vision Care
Fitting Keratoconus and Other Complicated Corneas Christine W Sindt OD FAAO Professor, Clinical Ophthalmology Director, Contact Lens Service University of Iowa Disclosure Consultant: ALCON Vision Care
What Makes a Good. Refractive Procedures
 What Makes a Good Refractive Procedure? Surgeons discuss their preferred treatments for various refractive errors. By Frik J. Potgieter, MB ChB (Stell), FCS (SA), MMed (Pret), FRCS (Edin); David T.C. Lin,
What Makes a Good Refractive Procedure? Surgeons discuss their preferred treatments for various refractive errors. By Frik J. Potgieter, MB ChB (Stell), FCS (SA), MMed (Pret), FRCS (Edin); David T.C. Lin,
The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (9), Page
 Vol. 73 (9), Page") The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (9), Page 7580-7586 Outcome of PRK in Management of Post LISIK Residual Myopia and Myopic Astigmatism Department of Ophthalmology, Faculty
The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (9), Page 7580-7586 Outcome of PRK in Management of Post LISIK Residual Myopia and Myopic Astigmatism Department of Ophthalmology, Faculty
Comparison of Corneal Power and Intraocular Lens Power Calculation Methods after LASIK for Myopia
 Comparison of Corneal Power and Intraocular Lens Power Calculation Methods after LASIK for Myopia Seyed Mohammad Reza Taheri, MD 1 Azita Kheiltash, MD, MPH 2 Hassan Hashemi, MD 1,3 Abstract Purpose: To
Comparison of Corneal Power and Intraocular Lens Power Calculation Methods after LASIK for Myopia Seyed Mohammad Reza Taheri, MD 1 Azita Kheiltash, MD, MPH 2 Hassan Hashemi, MD 1,3 Abstract Purpose: To
INFORMED CONSENT FOR LASER IN SITU KERATOMILEUSIS ( LASIK )
") INFORMED CONSENT FOR LASER IN SITU KERATOMILEUSIS ( LASIK ) This information is to help you make an informed decision about having Laser In Situ Keratomileusis (LASIK), a laser vision correction procedure
INFORMED CONSENT FOR LASER IN SITU KERATOMILEUSIS ( LASIK ) This information is to help you make an informed decision about having Laser In Situ Keratomileusis (LASIK), a laser vision correction procedure
Preliminary Programme
 In conjunction with the Serbian Society of Cataract and Refractive Surgeons 9 11 February 2018 Preliminary Programme General Information Venue Sava Centar, Milentija Popovića 9, Beograd 11070, Serbia Local
In conjunction with the Serbian Society of Cataract and Refractive Surgeons 9 11 February 2018 Preliminary Programme General Information Venue Sava Centar, Milentija Popovića 9, Beograd 11070, Serbia Local
KNOW THE OPTIONS. Discover how the latest advances in vision correction can improve your sight.
 KNOW THE OPTIONS. LASIK VISIAN ICL PRK Discover how the latest advances in vision correction can improve your sight. Today, you can choose from several choices of permanent vision correction procedures
KNOW THE OPTIONS. LASIK VISIAN ICL PRK Discover how the latest advances in vision correction can improve your sight. Today, you can choose from several choices of permanent vision correction procedures
Comparison of Corneal Shape Changes and Aberrations Induced By FS-LASIK and SMILE for Myopia
 ORIGINAL ARTICLE Comparison of Corneal Shape Changes and Aberrations Induced By FS-LASIK and SMILE for Myopia Anders Gyldenkerne, MS; Anders Ivarsen, MD, PhD; Jesper Ø. Hjortdal, MD, PhD ABSTRACT PURPOSE:
ORIGINAL ARTICLE Comparison of Corneal Shape Changes and Aberrations Induced By FS-LASIK and SMILE for Myopia Anders Gyldenkerne, MS; Anders Ivarsen, MD, PhD; Jesper Ø. Hjortdal, MD, PhD ABSTRACT PURPOSE:
Comparison of Corneal and Anterior Chamber Parameters following Myopic laser in situ keratomileusis and photorefractive keratectomy by
 Comparison of Corneal and Anterior Chamber Parameters following Myopic laser in situ keratomileusis and photorefractive keratectomy by Pentacam as A New Imaging Technique Mohammad Ali Zare, MD 1 Hassan
Comparison of Corneal and Anterior Chamber Parameters following Myopic laser in situ keratomileusis and photorefractive keratectomy by Pentacam as A New Imaging Technique Mohammad Ali Zare, MD 1 Hassan
GUIDE TO CORRECTIVE EYE SURGERY. claritylaservision.com. 110, Avenue South West Calgary, Alberta T2V 4J2
 GUIDE TO CORRECTIVE EYE SURGERY claritylaservision.com 110, 1016 68 Avenue South West Calgary, Alberta T2V 4J2 OUR PHILOSOPHY The most important philosophy that Clarity Laser Vision believes in is that
GUIDE TO CORRECTIVE EYE SURGERY claritylaservision.com 110, 1016 68 Avenue South West Calgary, Alberta T2V 4J2 OUR PHILOSOPHY The most important philosophy that Clarity Laser Vision believes in is that
INFORMED CONSENT FOR PHOTOREFRACTIVE KERATECTOMY (PRK) AND ADVANCE SURFACE ABLATION (ASA)
 AND ADVANCE SURFACE ABLATION (ASA)") INFORMED CONSENT FOR PHOTOREFRACTIVE KERATECTOMY (PRK) AND ADVANCE SURFACE ABLATION (ASA) This information and the Patient Information booklet must be reviewed so you can make an informed decision regarding
INFORMED CONSENT FOR PHOTOREFRACTIVE KERATECTOMY (PRK) AND ADVANCE SURFACE ABLATION (ASA) This information and the Patient Information booklet must be reviewed so you can make an informed decision regarding
ADVANCES in REFRACTIVE, CORNEA, and CATARACT SURGERY UPDATE 2018
 efocus Innovation, Leadership, Passion for Perfection Issue 051 415.922.9500 www.pacificvision.org March 2018 ADVANCES in REFRACTIVE, CORNEA, and CATARACT SURGERY UPDATE 2018 Eye care has always been at
efocus Innovation, Leadership, Passion for Perfection Issue 051 415.922.9500 www.pacificvision.org March 2018 ADVANCES in REFRACTIVE, CORNEA, and CATARACT SURGERY UPDATE 2018 Eye care has always been at
Today s Checklist. What am I even looking at? Corneal procedures. Intacs. Post LASIK
 SURGERY WAS THE EASY PART Managing Post-Surgical Corneas with Specialty Contact Lenses Brooke Messer, O.D. Cornea and Contact Lens Institute of Minnesota Today s Checklist What might walk in my door? Challenges
SURGERY WAS THE EASY PART Managing Post-Surgical Corneas with Specialty Contact Lenses Brooke Messer, O.D. Cornea and Contact Lens Institute of Minnesota Today s Checklist What might walk in my door? Challenges
Clinical Approach To Refractive Errors. Dr. Faizur Rahman Associate Professor Peshawar Medical College
 Clinical Approach To Refractive Errors Dr. Faizur Rahman Associate Professor Peshawar Medical College Learning objectives By the end of this lecture the students would be able to; Correlate optics with
Clinical Approach To Refractive Errors Dr. Faizur Rahman Associate Professor Peshawar Medical College Learning objectives By the end of this lecture the students would be able to; Correlate optics with
Meet Libby. Corneal Dysgenesis, Degeneration, and Dystrophies Definitions. Dr. Victor Malinovsky
 Meet Libby Corneal Dysgenesis, Degeneration, and Dystrophies 2006 Dr. Victor Malinovsky Definitions Dysgenesis: (congenital anomalies) A development disorder that results in a congenital malformation of
Meet Libby Corneal Dysgenesis, Degeneration, and Dystrophies 2006 Dr. Victor Malinovsky Definitions Dysgenesis: (congenital anomalies) A development disorder that results in a congenital malformation of
ViΤAL Keratoconus Classification, The AMART (or SECRET) & Gregory Lens Projects
 & Gregory Lens Projects") ViΤAL Keratoconus Classification, The AMART (or SECRET) & Gregory Lens Projects Anastasios Charonis MD PhD Medical Director, AthensVision Eye Institute anastasioscharonis@athensvision.com Purpose: To
ViΤAL Keratoconus Classification, The AMART (or SECRET) & Gregory Lens Projects Anastasios Charonis MD PhD Medical Director, AthensVision Eye Institute anastasioscharonis@athensvision.com Purpose: To
Why Cataract and Refractive Surgeons Need the Pentacam Four surgeons discuss the device s value, including new software additions.
 Why Cataract and Refractive Surgeons Need the Pentacam Four surgeons discuss the device s value, including new software additions. Produced under an unrestricted educational grant from Oculus, Inc.. Extremely
Why Cataract and Refractive Surgeons Need the Pentacam Four surgeons discuss the device s value, including new software additions. Produced under an unrestricted educational grant from Oculus, Inc.. Extremely
A Patients Guide to Excimer Laser Refractive Surgery
 A Patients Guide to Excimer Laser Refractive Surgery March 2006 Contents 1. Introduction 2. Understanding your refractive error 3. Changing the eye s focus by surgery (refractive surgery) 4. Indications
A Patients Guide to Excimer Laser Refractive Surgery March 2006 Contents 1. Introduction 2. Understanding your refractive error 3. Changing the eye s focus by surgery (refractive surgery) 4. Indications
First Clinical Impressions on the Integrated Corneal Tomography and Corneal Deformation with Scheimpflug Imaging
 CASE SERIES First Clinical Impressions on 10.5005/jp-journals-10025-1151 the Integrated Corneal Tomography First Clinical Impressions on the Integrated Corneal Tomography and Corneal Deformation with Scheimpflug
CASE SERIES First Clinical Impressions on 10.5005/jp-journals-10025-1151 the Integrated Corneal Tomography First Clinical Impressions on the Integrated Corneal Tomography and Corneal Deformation with Scheimpflug
PresbyMax Outcomes in Myopia, Hyperopia, Emmetropia and Patients post Lasik
 PresbyMax Outcomes in Myopia, Hyperopia, Emmetropia and Patients post Lasik SCHWIND eye-tech-solutions Lunch Symposium Prof. Jorge L. Alió MD, PhD. UNIVERSIDAD MIGUEL HERNÁNDEZ VISSUM INSTITUTO OFTALMOLÓGICO
PresbyMax Outcomes in Myopia, Hyperopia, Emmetropia and Patients post Lasik SCHWIND eye-tech-solutions Lunch Symposium Prof. Jorge L. Alió MD, PhD. UNIVERSIDAD MIGUEL HERNÁNDEZ VISSUM INSTITUTO OFTALMOLÓGICO
Patient Selection IOL Power Calculation. Patient Selection. Biometry IOL-Power calculation using Vericalc 2.0. AC-Depth > 3.0 mm (FDA 3.
 Verisyse and VeriFlex Patient Selection IOL Power Verisyse and VeriFlex Iris Claw Technology for Correcting Refractive Errors in Phakic and Aphakic Eyes ESCRS 2011 Intructional Course 61 Josef Ruckhofer
Verisyse and VeriFlex Patient Selection IOL Power Verisyse and VeriFlex Iris Claw Technology for Correcting Refractive Errors in Phakic and Aphakic Eyes ESCRS 2011 Intructional Course 61 Josef Ruckhofer
Clinical Outcomes after Topography-based Corneal Laser Surgery with the. WaveLight Oculyzer and Topolyzer Platforms
 1 Clinical Outcomes after Topography-based Corneal Laser Surgery with the WaveLight Oculyzer and Topolyzer Platforms By Arthur B. Cummings, M.D. 1 and Nadia Mascharka, MSc 2 Corresponding Author: Arthur
1 Clinical Outcomes after Topography-based Corneal Laser Surgery with the WaveLight Oculyzer and Topolyzer Platforms By Arthur B. Cummings, M.D. 1 and Nadia Mascharka, MSc 2 Corresponding Author: Arthur
BY MICHAEL W. BELIN, MD
 Point/Counterpoint: The Pentacam Ve The Pentacam s rotating imaging provides a more accurate picture of the cornea. BY MICHAEL W. BELIN, MD It was not long ago that discussions concerned whether topography
Point/Counterpoint: The Pentacam Ve The Pentacam s rotating imaging provides a more accurate picture of the cornea. BY MICHAEL W. BELIN, MD It was not long ago that discussions concerned whether topography
Current European Guidelines for Refractive Surgery Ophthalmologists from across Europe describe their countries standards or accepted norms.
 Current European Guidelines for Refractive Surgery Ophthalmologists from across Europe describe their countries standards or accepted norms. BY DAMIEN GATINEL, MD, PHD; SUPHI TANERI, MD; SASKIA OEHLER,
Current European Guidelines for Refractive Surgery Ophthalmologists from across Europe describe their countries standards or accepted norms. BY DAMIEN GATINEL, MD, PHD; SUPHI TANERI, MD; SASKIA OEHLER,
White Paper. Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery
 White Paper Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery A Summary of Clinical Outcomes Andrea Petznick, Diplom-AO (FH), PhD Alcon
White Paper Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery A Summary of Clinical Outcomes Andrea Petznick, Diplom-AO (FH), PhD Alcon
Prof.Paolo Vinciguerra, M.D. 1, 2 Riccardo Vinciguerra, M.D Humanitas University 1. Humanitas Clinical and Research Center IRCS 2
 Prof.Paolo Vinciguerra, M.D. 1, 2 Riccardo Vinciguerra, M.D. 1-3 1 Humanitas University 1 Humanitas Clinical and Research Center IRCS 2 Columbus, Ohio State University 3 University of Insubria, Varese
Prof.Paolo Vinciguerra, M.D. 1, 2 Riccardo Vinciguerra, M.D. 1-3 1 Humanitas University 1 Humanitas Clinical and Research Center IRCS 2 Columbus, Ohio State University 3 University of Insubria, Varese
Clinical Policy Title: Corneal implants
 Clinical Policy Title: Corneal implants Clinical Policy Number: CCP.1257 Effective Date: April 1, 2017 Initial Review Date: August 17, 2016 Most Recent Review Date: August 30, 2018 Next Review Date: September
Clinical Policy Title: Corneal implants Clinical Policy Number: CCP.1257 Effective Date: April 1, 2017 Initial Review Date: August 17, 2016 Most Recent Review Date: August 30, 2018 Next Review Date: September
LASIK INFORMED CONSENT INITIAL TREATMENT
 LASIK INFORMED CONSENT INITIAL TREATMENT PLEASE READ THE FOLLOWING PAGES CAREFULLY AND INITIAL AND SIGN WHERE INDICATED. PLEASE DO NOT SIGN ANY SECTION THAT YOU HAVE NOT READ OR DO NOT UNDERSTAND. SECTION
LASIK INFORMED CONSENT INITIAL TREATMENT PLEASE READ THE FOLLOWING PAGES CAREFULLY AND INITIAL AND SIGN WHERE INDICATED. PLEASE DO NOT SIGN ANY SECTION THAT YOU HAVE NOT READ OR DO NOT UNDERSTAND. SECTION
CLINIQUE LASERVUE. Informed Consent Form for Photo-Refractive Keratectomy (PRK)
") CLINIQUE LASERVUE Informed Consent Form for Photo-Refractive Keratectomy (PRK) Please read the following information and consent form very carefully. Your initials indicate that you understand all of the
CLINIQUE LASERVUE Informed Consent Form for Photo-Refractive Keratectomy (PRK) Please read the following information and consent form very carefully. Your initials indicate that you understand all of the
Codes for Medically Necessary Contact Lenses
 Codes for Medically Necessary Contact Lenses CPT Codes for Medically Necessary Prescribing Preamble for the 9231X Codes The prescription of contact lenses includes specification of optical and physical
Codes for Medically Necessary Contact Lenses CPT Codes for Medically Necessary Prescribing Preamble for the 9231X Codes The prescription of contact lenses includes specification of optical and physical
Summary Recommendations for Keratorefractive Laser Surgery June 2013
 Summary Recommendations for Keratorefractive Laser Surgery June 2013 Background Laser assisted in-situ keratomileusis (LASIK) surgery is the most commonly performed keratorefractive surgery; altering the
Summary Recommendations for Keratorefractive Laser Surgery June 2013 Background Laser assisted in-situ keratomileusis (LASIK) surgery is the most commonly performed keratorefractive surgery; altering the
Imaging and Current/Future Technologies in Medicine & Primary Eye Care
 I. What s New in Imaging for the Primary Eye Care Practice A. Digital Refraction Analyzers B. Corneal Topography C. Optical Coherence Tomography (OCT) and Retinal Imaging D. Wide-Field Retinal Imaging,
I. What s New in Imaging for the Primary Eye Care Practice A. Digital Refraction Analyzers B. Corneal Topography C. Optical Coherence Tomography (OCT) and Retinal Imaging D. Wide-Field Retinal Imaging,
PHOTOREFRACTIVE KERATECTOMY (PRK) PATIENT INFORMATION BOOKLET
 PATIENT INFORMATION BOOKLET") 616.365.5775 www.keillasik.com PHOTOREFRACTIVE KERATECTOMY (PRK) PATIENT INFORMATION BOOKLET Please read this entire booklet. Discuss its contents with your doctor so that questions are answered to your
616.365.5775 www.keillasik.com PHOTOREFRACTIVE KERATECTOMY (PRK) PATIENT INFORMATION BOOKLET Please read this entire booklet. Discuss its contents with your doctor so that questions are answered to your