Case Report Nodular Lymphocyte Predominant Hodgkin Lymphoma versus T-Cell/Histiocyte-Rich Large B-Cell Lymphoma: A Diagnostic Challenge
|
|
|
- Silvester Powell
- 5 years ago
- Views:
Transcription
1 Case Reports in Pathology, Article ID , 5 pages Case Report Nodular Lymphocyte Predominant Hodgkin Lymphoma versus T-Cell/Histiocyte-Rich Large B-Cell Lymphoma: A Diagnostic Challenge Anton V. Rets and Susan R. S. Gottesman Department of Pathology, State University of New York Downstate Medical Center, 450 Clarkson Avenue, Brooklyn, NY 11203, USA Correspondence should be addressed to Susan R. S. Gottesman; susan.gottesman@downstate.edu Received 1 May 2014; Accepted 25 June 2014; Published 7 July 2014 Academic Editor: Piero Tosi Copyright 2014 A. V. Rets and S. R. S. Gottesman. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Lymphomas with overlapping histological features of two distinct entities cause difficulty in classification. Their classification is of particular significance when the two alternatives require different treatment modalities. We present a diagnostically challenging case of a nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) with features of T-cell/histiocyte-rich large B-cell lymphoma (THRLBCL). Our patient is a 39-year-old woman who presented with painless subclavicular and axillary lymphadenopathy. The biopsied lymph node showed diffuse architectural effacement and scattered large neoplastic cells with large irregular nuclei and prominent nucleoli. These cells were positive for CD20 and Bcl-6 and negative for CD15, CD30, IgD, and Bcl-2. The background cells were predominantly T lymphocytes, whereas B cells were markedly depleted. The lymph node was interpreted as NLPHL, consistent with THRLBCL-like variant. NLPHL, especially THRLBC-like variant, and de novo THRLBCL are characterized by significant morphologic and immunophenotypic overlap. Our case demonstrates a rare predominance of background T-cells in NLPHL and emphasizes the importance of thorough evaluation of multiple morphologic and immunophenotypic features as an essential approach for arriving at the correct diagnosis. 1. Introduction Current classification of lymphomas is based on a complex of clinical, morphological, immunophenotypic, and molecular criteria. Such an approach provides an accurate classification of the majority of lymphomas. There are, however, cases which are difficult to fit into a distinct category. They demonstrate overlapping features between groups of lymphomas of different prognostic significance and treatment modalities. In such cases, making a correct diagnosis is a challenging task. Commonly these neoplasms show features of Hodgkin lymphomas (classical or nodular lymphocyte predominant (NLPHL)) and diffuse large B-cell lymphomas (DLBCL) or the latter and Burkitt lymphoma [1, 2]. For some, the dilemma cannotberesolvedandaterm grayzonelymphoma has been used to designate such cases. Here we present a diagnostically challenging case of a lymphoma with features of NLPHL and T-cell/histiocyte-rich large B-cell lymphoma (THRLBCL) with an attempt to distinguish between them and summarize their unique and overlapping diagnostic features. 2. Case Presentation A 39-year-old obese woman presented with a painless 2 2 cm left subclavicular lymph node that she had had for 1-2 years. She denied any complaints, including B-symptoms, and her past medical and social histories were unremarkable. Physical examination revealed left supraclavicular and axillary lymphadenopathy and absence of hepatosplenomegaly. Peripheral blood was remarkable for mild normocytic normochromic anemia and mild neutropenia. PET scan demonstrated bulky supraclavicular and axillary lymphadenopathy (SUV 8.01 and resp.) with a neoplastic range hypermetabolic activity in the spleen and
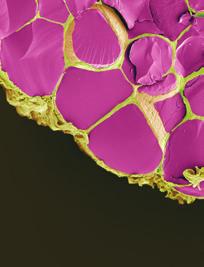
. CD3-positive cells comprise the predominant background population. Figure 2: Neoplastic cells (hematoxylin and eosin stain, 400x).")
. Highlighted B-cells are depleted and form loose clusters. Neoplastic cells strongly express CD20. porta hepatis (SUV 10.65 and 12.")


2 2 Case Reports in Pathology Figure 1: Biopsied lymph node architecture (hematoxylin and eosin stain, 40x). Vague nodules are present in the background of diffuse architectural effacement. Figure 3: Background cells (CD3 immunostain, 400x; inlet, 40x). CD3-positive cells comprise the predominant background population. Figure 2: Neoplastic cells (hematoxylin and eosin stain, 400x). Neoplastic cells with one or multiple large pleomorphic nuclei and prominent nucleoli are admixed with histiocytes and benign lymphocytes. Figure 4: CD20-positive cells (CD20 immunostain, 40x; inlet, 40x). Highlighted B-cells are depleted and form loose clusters. Neoplastic cells strongly express CD20. porta hepatis (SUV and 12.1 resp.), as well as in the gastrohepatic and internal iliac lymph nodes. Bone marrow involvement was also suspected; however, no morphological evidence of involvement was demonstrated in the sample submitted. Cytogenetic analysis of the bone marrow revealed no abnormalities in karyotype by G banding with conventional trypsin-giemsa technique and was negative for IGH/BCL1 and IGH/MYC translocation, as well as for rearrangements of BCL6, MALT1, ALK, and IGH genes by FISH. The architecture of the biopsied supraclavicular lymph node was effaced and demonstrated moderate fibrosis, hyalinosis, and capsular thickening. The overall histologic appearance was predominantly diffuse, although small vague nodules could be appreciated (Figure 1). The neoplastic cells were large and scattered throughout the lymph node; they also formed loose clusters admixed with macrophages and small mature lymphocytes. These neoplastic cells had one or multiple, large, irregular, multilobulated nuclei with vesicular chromatin and prominent eosinophilic or amphophilic nucleoli (Figure 2). Numerous mitotic figures, including atypical ones, were present. The neoplastic cells were positive for CD20 and Bcl-6 and negative for CD3, CD15, CD30, IgD, and Bcl-2. The background cells were predominantly T lymphocytes with CD20 : CD3 ratio of 1 : 10 (Figure 3). CD4+ population greatly outnumbered CD8+ cells (CD4 : CD8 ratio of 8 : 1). B-cells were markedly depleted and formed loose clusters (Figure 4). Besides a Bcl-6-positive B-cell population, these clusters contained a disrupted CD21-positive framework of follicular dendritic cells along with CD57 and PD1-positive T-cells, qualifying them as remnants of germinal centers. Occasional rosettes formed by PD1+ lymphocytes around the neoplastic cells were seen. The lymph node was interpreted as NLPHL, consistent with T-cell/histiocyte-rich large B-cell lymphomalike variant (NLPHL THRLBCL-like variant). The clinical presentation corresponded with Stage IV disease by Ann Arbor system with Cotswolds modifications [3]. The patient was treated with 6 cycles of ABVD therapy and showed an appropriate initial response. The long-term therapeutic effect cannot be yet assessed. 3. Discussion Our case illustrated a diagnostic struggle in differentiating between NLPHL and THRLBCL. The puzzling aspect of this case was a significant predominance of background T-cells over the B-cell population. This finding is exceptional in
3 Case Reports in Pathology 3 NLPHL, including its variants. NLPHL is usually characterized by background reactive B-cells predominating in the nodules, a feature of diagnostic importance, whereas, in a case of a THRLBCL, as the name suggests, T-cells are the main lymphoid population in the background. In fact, presence of neoplastic cells scattered in a T-cell and histiocyte-rich background devoid of small B-cells, observed in our case, is a prerequisite for the diagnosis of THRLBCL [4]. The diagnosis in this case, NLPHL THRLBCL-like variant, is an uncommon pattern of NLPHL. The morphologic resemblance of this neoplasm with THRLBCL poses a great diagnostic challenge. Distinguishing between these two entities is important because of the differences in their prognosis and treatment. Thus, NLPHL has an overall favorable prognosis, although worse clinical outcomes are expected in advanced stages. Historically, patients with NLPHL are treated like patients with classical Hodgkin lymphoma. Thus, limited field radiation therapy is the most common treatment forpatientswithanearlystagedisease[5, 6], whereas, in advanced-stage NLPHL, chemotherapy regimens may be preferred [7]. Unfortunately, up to 3 10% of cases progress to a DLBCL by 10 years [8]. THRLBCL, in contrast, is an aggressive neoplasm, prognostically comparable to DLBCL, not otherwisespecified [9], and the chemotherapy modalities are significantly more intensive than those used for NLPHL [10, 11]. Both NLPHL and THRLBCL are characterized by the presence of scattered large neoplastic B-cells in a background of benign lymphocytes and macrophages. The neoplastic cells of the former, also known as LP cells, have scant cytoplasm and one folded or multilobated nuclei with prominent, mostly basophilic nucleoli. Although LP cells may have a phenotype overlappingwithhodgkin-reed-sternberg(hrs)cells,they are usually positive for CD45, CD20, CD79a, and Bcl-6, lack expression of CD15, and often are CD30-negative. IgD expression, seen in roughly one third of NLPHL, but not in our case, is more common in young men. In fact, IgD positivity is a useful argument against de novo THRBCL [12].LargecellsinTHRLBCLmayresembleLPandHRS cells but usually have more pronounced pleomorphism. Their immunoprofile is very similar to the former, with the exception of less common expression of Bcl-6 and more frequent expression of IRF4/MUM1. It is nearly impossible to establish a correct diagnosis based on the neoplastic cell morphology alone. Histoarchitectureofthelymphnodeandthecomposition of the background cell populations provide the most reliable diagnostic features. The majority of NLPHLs demonstrate a nodular pattern. On rare occasions, diffuse architectural effacement may be seen, but even in that circumstance the background lymphocytes remain predominantly B-cells. Six distinct immunoarchitectural patterns of NLPHL have been described by Fan et al [13]. They include NLPHL-classic B-cell-rich pattern (A), serpiginous pattern (B), pattern with prominent extranodular LP cells (C), T-cell-rich pattern (D), diffuse (THRLBCL-like) pattern (E), and diffuse pattern with a B-cell rich background (F). Patterns C F may reflect an altered homing pattern of LP cells, with patterns D and E being associated with a T-cell-rich environment and progressive depletion of B-cells [14]. Presence of extranodular LP cells is believed to represent progression of nodular variant to diffuse pattern, with the latter being an independent predictor of relapse. Patients with variant NLPHL morphology, including THRLBCL-like, present in advanced stage (stage IIB and higher) as compared to cases with typical NLPHL pattern [14]. The THRLBCL-like pattern seen in our patient wasalsoassociatedwithanadvancedstageatpresentation, which reflects her long-standing history of undiagnosed NLPHL. Her delay in presenting for medical attention was most likely caused by her morbid obesity and absence of B- symptoms. Regardless of the pattern, evidence of vague nodular structures can be demonstrated by immunohistochemistry which discloses a follicular dendritic cell meshwork containing B-cells, histiocytes, and CD4/CD57/PD1-positive T-cells. The PD1+ cells tend to form rosettes around the neoplastic cells, which can be used as a diagnostic feature of NLPHL, as in our case. Although it is frequently seen in nodular forms of NLPHL, diffuse patterns, including NLPHL THRLBCLlike, may even fail to exhibit rosette formation adding to the diagnostic difficulty [15 17]. In contrast, THRLBCL demonstrates a diffuse T-cell and histiocyte-rich infiltrate with few scattered tumor cells. Within the T-cell population, CD8+ cells usually outnumber the CD4+ subset. Small B-cells are present in minimal numbers; their prominence, even in a diffuse distribution, strongly argues against THRLBCL [18]. The presence of B-cell nodules associated with follicular dendritic cells also supports a diagnosis of NLPHL over THRLBCL [18]. A summary of diagnostic features of NLPHL and THRLBCL is presented in Table 1. Despite morphological similarity, pathogenic relationship between NLPHL and THRLBCL remains controversial. The 2008 WHO Classification separates de novo THCRL- BCL from secondary THCRLBCL, which may arise from NLPHL (also known as THRLBCL-like NLPHL), since they may represent distinct but morphologically and immunophenotypically similar entities [19]. A possible biologic link has been supported by molecular overlap between tumor cells of NLPHL (including NLPHL-THRLBCL-like) and de novo THRLBCL [17], a lack of disease specific pattern of gene expression, and similarities in their gene expression profile [20]. On the other hand, NLPHL demonstrates higher average number of genomic imbalances (10.8 versus 4.7 in THRLBCL) [21], which does not support the theory of a de novo THRLBCL being a form of progression of NLPHL. Indeed, NLPHL THRLBCL-like may represent a progression of a more typical NLPHL as patients present in advanced stage, as in our case. 4. Conclusion NLPHL, especially THRLBC-like variant, and de novo THRLBCL are characterized by significant morphologic and immunophenotypic overlap. The composition of the background cell populations, usually a reliable feature to distinguish NLPHL from THRLBCL, may show a great
4 4 Case Reports in Pathology Table 1: Diagnostic features of NLPHL, THRLBCL, and our case. Criterion NLPHL TCHRLBCL Our case Clinical features Age Any, most commonly between 30 and 50 years old Middle age 39 years old Gender predilection Strong male predominance Male predominance Female Presentation Solitary peripheral lymphadenopathy Advanced disease with lymphadenopathy, liver, spleen, and bone marrow involvement Widespread peripheral lymphadenopathy with possible splenic, hepatic, and bone marrow involvement Neoplastic cells Distribution Nodular or diffuse and nodular Diffuse; vague nodularity is rare Diffuse and vaguely nodular Bcl-6 expression Present Less common Present IRF4/MUM1 expression Absent May be present Not performed IgD expression Present in approximately 1/3 cases Absent Absent Average number of genomic imbalances Not performed Background cells Predominant lymphocyte population B-cells T-cells T-cells B lymphocytes distribution Nodules Nodules are absent Vague nodules CD4+ T lymphocytes More prominent Less prominent Prominent CD4+ versus CD8+ T lymphocytes Mostly CD4+ Mostly CD8+ Mostly CD4+ Follicular center T lymphocytes (CD4+/CD57+/PD1+) Present Rare Present Follicular dendritic cell meshwork Present Absent Present PD1+ T lymphocyte rosettes Present, may be absent in around neoplastic cells THRLBC-like variant Absent Occasional rosettes are present degree of variability. Our case shows a rare predominance of the background T-cells in NLPHL and emphasizes the importance of thorough evaluation of multiple morphologic and immunophenotypic features as an essential approach for arriving at the correct diagnosis. Conflict of Interests The authors declare that there is no conflict of interests regarding the publication of this paper. References [1] E. S. Jaffe, H. Stein, S. H. Swerdlow et al., B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma, in WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues,S.H.Swerdlow,E.Campo,N.Harrisetal.,Eds.,pp , IARC, Lyon, France, 4th edition, [2] P. M. Kluin, N. L. Harris, H. Stein, and L. Leoncini, B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma, in WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues,S.H.Swerdlow,E.Campo,N.Harrisetal.,Eds.,pp , IARC, Lyon, France, 4th edition, [3]T.A.Lister,D.Crowther,S.B.Sutcliffeetal., Reportofa committee convened to discuss the evaluation and staging of patients with Hodgkin s disease: Cotsworlds meeting, Journal of Clinical Oncology,vol.7,no.11,pp ,1989. [4] L. Boudová, E. Torlakovic, J. Delabie et al., Nodular lymphocyte-predominant Hodgkin lymphoma with nodules resembling T-cell/histiocyte-rich B-cell lymphoma: differential diagnosis between nodular lymphocyte-predominant Hodgkin lymphoma and T-cell/histiocyte-rich B-cell lymphoma, Blood, vol. 102, no. 10, pp , [5] R. C. Chen, M. S. Chin, A. K. Ng et al., Early-stage, lymphocyte-predominant Hodgkin s lymphoma: patient outcomes from a large, single-institution series with long followup, Clinical Oncology, vol. 28, no. 1, pp , [6] V. Diehl, M. Sextro, J. Franklin et al., Clinical presentation, course, and prognostic factors in lymphocyte-predominant Hodgkin s disease and lymphocyte-rich classical Hodgkin s disease: report from the European Task Force on lymphoma project on lymphocyte-predominant Hodgkin s disease, Journal of Clinical Oncology,vol.17,no.3,pp ,1999. [7] G.P.Canellos, Whatistheappropriatesystemicchemotherapy for lymphocyte-predominant Hodgkin's lymphoma? Journal of Clinical Oncology, vol. 28, article e8, no. 1, [8] M. Al-Mansour, J. M. Connors, R. D. Gascoyne, B. Skinnider, andk.j.savage, Transformationtoaggressivelymphoma
5 Case Reports in Pathology 5 in nodular lymphocyte-predominant Hodgkin s lymphoma, Clinical Oncology,vol.28,no.5,pp ,2010. [9]S.Monti,K.J.Savage,J.L.Kutoketal., Molecularprofiling of diffuse large B-cell lymphoma identifies robust subtypes including one characterized by host inflammatory response, Blood,vol.105,no.5,pp ,2005. [10] S. J. Horning, E. Weller, K. Kim et al., Chemotherapy with or without radiotherapy in limited-stage diffuse aggressive non- Hodgkin s lymphoma: Eastern Cooperative Oncology Group Study 1484, Clinical Oncology, vol. 22, no. 15, pp , [11] F. Reyes, E. Lepage, G. Ganem et al., ACVBP versus CHOP plus radiotherapy for localized aggressive lymphoma, The New England Medicine,vol.352,no.12,pp ,2005. [12] L. Quintanilla-Martinez, D. de Jong, A. de Mascarel et al., Gray zones around diffuse large B cell lymphoma. conclusions based on the workshop of the XIV meeting of the European Association for Hematopathology and the Society of Hematopathology in Bordeaux, France, Hematopathology, vol. 2, no.4, pp ,2009. [13] Z.Fan,Y.Natkunam,E.Bair,R.Tibshirani,andR.A.Warnke, Characterization of variant patterns of nodular lymphocyte predominant Hodgkin lymphoma with immunohistologic and clinical correlation, The American Surgical Pathology, vol. 27, no. 10, pp , [14] S. Hartmann, D. A. Eichenauer, A. Plutschow et al., The prognostic impact of variant histology in nodular lymphocytepredominant Hodgkin lymphoma: a report from the German Hodgkin study group, Blood, vol.122,no.26,pp , [15]S.H.Nam-Cha,G.Roncador,L.Sanchez-Verdeetal., PD- 1, A follicular T-cell marker useful for recognizing nodular lymphocyte-predominant Hodgkin lymphoma, The American Surgical Pathology,vol.32,no.8,pp ,2008. [16] H. R. O. Churchill, G. Roncador, R. A. Warnke, and Y. Natkunam, Programmed death 1 expression in variant immunoarchitectural patterns of nodular lymphocyte predominant Hodgkin lymphoma: comparison with CD57 and lymphomas in the differential diagnosis, Human Pathology, vol.41,no.12, pp ,2010. [17] S.Hartmann,C.Doring,C.Jakobusetal., Nodularlymphocyte predominant Hodgkin lymphoma and T cell/histiocyte rich large B cell lymphoma endpoints of a spectrum of one disease? PLoS ONE, vol. 8, no. 11, Article ID e78812, [18] N. L. Harris, Shades of gray between large B-cell lymphomas and Hodgkin lymphomas: Differential diagnosis and biological implications, Modern Pathology, vol. 26, no. 1, pp. S57 S70, [19] C. De Wolf-Peeters, J. Delabie, E. Campo et al., T cell/histiocyte-rich large B-cell lymphoma, in WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues,S.H.Swerdlow, N. Harris, E. S. Jaffe et al., Eds., pp , IARC, Lyon, France, 4th edition, [20] V. Brune, E. Tiacci, I. Pfeil et al., Origin and pathogenesis of nodular lymphocyte-predominant Hodgkin lymphoma as revealed by global gene expression analysis, Experimental Medicine,vol.205,no.10,pp ,2008. [21] S.Franke,I.Wlodarska,B.Maesetal., Comparativegenomic hybridization pattern distinguishes T-cell/histiocyte-rich B-cell lymphoma from nodular lymphocyte predominance Hodgkin s lymphoma, The American Pathology, vol. 161, no. 5, pp ,2002.
















6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Nodular lymphocyte predominant Hodgkin lymphoma. Lymphoma Tumor Board. January 5, 2018
 Nodular lymphocyte predominant Hodgkin lymphoma Lymphoma Tumor Board January 5, 2018 Etiology Subtypes of Classical Hodgkin Lymphoma (chl)* Nodular sclerosing HL Most common subtype Composed of large tumor
Nodular lymphocyte predominant Hodgkin lymphoma Lymphoma Tumor Board January 5, 2018 Etiology Subtypes of Classical Hodgkin Lymphoma (chl)* Nodular sclerosing HL Most common subtype Composed of large tumor
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
, , 2011 HODGKIN LYMPHOMA
 European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
Leukaemia Section Short Communication
 Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL INIST-CNRS Leukaemia Section Short Communication Classification of Hodgkin lymphoma over years Antonino Carbone, Annunziata
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL INIST-CNRS Leukaemia Section Short Communication Classification of Hodgkin lymphoma over years Antonino Carbone, Annunziata
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma
 Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Case Report PAX5-Negative Classical Hodgkin Lymphoma: A Case Report of a Rare Entity and Review of the Literature
 Hindawi Case Reports in Hematology Volume 2017, Article ID 7531729, 4 pages https://doi.org/10.1155/2017/7531729 Case Report PAX5-Negative Classical Hodgkin Lymphoma: A Case Report of a Rare Entity and
Hindawi Case Reports in Hematology Volume 2017, Article ID 7531729, 4 pages https://doi.org/10.1155/2017/7531729 Case Report PAX5-Negative Classical Hodgkin Lymphoma: A Case Report of a Rare Entity and
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Diffuse variant of lymphocyte-predominant Hodgkin lymphoma: a diagnostic challenge
 J Hematopathol (2013) 6:145 150 DOI 10.1007/s12308-012-0162-8 CASE REPORT Diffuse variant of lymphocyte-predominant Hodgkin lymphoma: a diagnostic challenge Yuanming Zhang & Ihsane Ouansafi & Wayne Tam
J Hematopathol (2013) 6:145 150 DOI 10.1007/s12308-012-0162-8 CASE REPORT Diffuse variant of lymphocyte-predominant Hodgkin lymphoma: a diagnostic challenge Yuanming Zhang & Ihsane Ouansafi & Wayne Tam
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Thomas Hodgkin and Hodgkin lymphoma
 J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas
 ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Shades of gray between large B-cell lymphomas and Hodgkin lymphomas: differential diagnosis and biological implications
 & 2013 USCAP, Inc. All rights reserved 0893-3952/13 $32.00 S57 Shades of gray between large B-cell lymphomas and Hodgkin lymphomas: differential diagnosis and biological implications Nancy L Harris Department
& 2013 USCAP, Inc. All rights reserved 0893-3952/13 $32.00 S57 Shades of gray between large B-cell lymphomas and Hodgkin lymphomas: differential diagnosis and biological implications Nancy L Harris Department
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Tres
 Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma
 Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma Katherine Devitt, M.D., Benjamin Chen, M.D., Ph.D., Hongbo Yu, M.D., Ph.D., Bruce Woda, M.D. 1 1 Department
Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma Katherine Devitt, M.D., Benjamin Chen, M.D., Ph.D., Hongbo Yu, M.D., Ph.D., Bruce Woda, M.D. 1 1 Department
Anaplastic Large Cell Lymphoma (of T cell lineage)
") Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report of Neoadjuvant Use Enabling Complete Surgical Resection
 Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Follicular Lymphoma: the WHO
 Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Case Report Precursor B Lymphoblastic Lymphoma Involving the Stomach
 Volume 2013, Article ID 930918, 4 pages http://dx.doi.org/10.1155/2013/930918 Case Report Precursor B Lymphoblastic Lymphoma Involving the Stomach Masaya Iwamuro, 1,2 Yoshinari Kawai, 1 Yasuhide Yamawaki,
Volume 2013, Article ID 930918, 4 pages http://dx.doi.org/10.1155/2013/930918 Case Report Precursor B Lymphoblastic Lymphoma Involving the Stomach Masaya Iwamuro, 1,2 Yoshinari Kawai, 1 Yasuhide Yamawaki,
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA
 2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
IX. Is it only about MYC? How to approach the diagnosis of diffuse large B-cell lymphomas
 Hematological Oncology Hematol Oncol 2015; 33: 50 55 Published online in Wiley Online Library (wileyonlinelibrary.com).2217 Supplement Article IX. Is it only about MYC? How to approach the diagnosis of
Hematological Oncology Hematol Oncol 2015; 33: 50 55 Published online in Wiley Online Library (wileyonlinelibrary.com).2217 Supplement Article IX. Is it only about MYC? How to approach the diagnosis of
Case Report Pitfalls in the Diagnosis of Anaplastic Large Cell Lymphoma with a Small Cell Pattern
 Case Reports in Hematology Volume 23, Article ID 84253, 6 pages http://dx.doi.org/.55/23/84253 Case Report Pitfalls in the Diagnosis of Anaplastic Large Cell Lymphoma with a Small Cell Pattern Rowan L.
Case Reports in Hematology Volume 23, Article ID 84253, 6 pages http://dx.doi.org/.55/23/84253 Case Report Pitfalls in the Diagnosis of Anaplastic Large Cell Lymphoma with a Small Cell Pattern Rowan L.
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Case Report Nodular Lymphocyte-Predominant Hodgkin Lymphoma or T-cell/Histiocyte Rich Large B-cell Lymphoma: The Problem in Grey Zone Lymphomas
 www.ijcep.com/ijcep708008 Case Report Nodular Lymphocyte-Predominant Hodgkin Lymphoma or T-cell/Histiocyte Rich Large B-cell Lymphoma: The Problem in Grey Zone Lymphomas Frank X. Zhao Department of Pathology,
www.ijcep.com/ijcep708008 Case Report Nodular Lymphocyte-Predominant Hodgkin Lymphoma or T-cell/Histiocyte Rich Large B-cell Lymphoma: The Problem in Grey Zone Lymphomas Frank X. Zhao Department of Pathology,
PhenoPath. Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA
 PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome to Cutaneous Melanoma
 ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Case Report A Case of p63 Positive Diffuse Large B Cell Lymphoma of the Bladder
 Case Reports in Hematology Volume 2016, Article ID 4348208, 4 pages http://dx.doi.org/10.1155/2016/4348208 Case Report A Case of p63 Positive Diffuse Large B Cell Lymphoma of the Bladder Chelsey D. Deel,
Case Reports in Hematology Volume 2016, Article ID 4348208, 4 pages http://dx.doi.org/10.1155/2016/4348208 Case Report A Case of p63 Positive Diffuse Large B Cell Lymphoma of the Bladder Chelsey D. Deel,
Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management
 HODGKIN LYMPHOMA: NEW INSIGHTS AND NEW APPROACHES Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management Dennis A. Eichenauer 1,2 and Andreas Engert 1,2 1 First Department
HODGKIN LYMPHOMA: NEW INSIGHTS AND NEW APPROACHES Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management Dennis A. Eichenauer 1,2 and Andreas Engert 1,2 1 First Department
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Pathology of the Lymphoid System
 Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
During past decades, because of the lack of knowledge
 Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Table 1: Comparison of Immunohistologic Features of NLPHL and CHL
 USCAP Hematopathology Evening Specialty Conference CASE 1: Handout Yasodha Natkunam, M.D., Ph.D. Department of Pathology Stanford University School of Medicine INTRODUCTION Nodular lymphocyte predominant
USCAP Hematopathology Evening Specialty Conference CASE 1: Handout Yasodha Natkunam, M.D., Ph.D. Department of Pathology Stanford University School of Medicine INTRODUCTION Nodular lymphocyte predominant
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
Does the proliferation fraction help identify mature B cell lymphomas with double- and triple-hit translocations?
 Histopathology 2012, 61, 1214 1218. DOI: 10.1111/j.1365-2559.2012.04351.x SHORT REPORT Does the proliferation fraction help identify mature B cell lymphomas with double- and triple-hit translocations?
Histopathology 2012, 61, 1214 1218. DOI: 10.1111/j.1365-2559.2012.04351.x SHORT REPORT Does the proliferation fraction help identify mature B cell lymphomas with double- and triple-hit translocations?
Case Report Esophageal Plasmacytoma Diagnosed in a Patient Presenting with Cardiac Symptoms: A Novel Case
 Volume 2013, Article ID 121670, 4 pages http://dx.doi.org/10.1155/2013/121670 Case Report Esophageal Plasmacytoma Diagnosed in a Patient Presenting with Cardiac Symptoms: A Novel Case Cheryl Rimmer, 1
Volume 2013, Article ID 121670, 4 pages http://dx.doi.org/10.1155/2013/121670 Case Report Esophageal Plasmacytoma Diagnosed in a Patient Presenting with Cardiac Symptoms: A Novel Case Cheryl Rimmer, 1
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Research Article Stromal Expression of CD10 in Invasive Breast Carcinoma and Its Correlation with ER, PR, HER2-neu, and Ki67
 SAGE-Hindawi Access to Research International Breast Cancer Volume 20, Article ID 47957, 4 pages doi:0.406/20/47957 Research Article Stromal Expression of CD0 in Invasive Breast Carcinoma and Its Correlation
SAGE-Hindawi Access to Research International Breast Cancer Volume 20, Article ID 47957, 4 pages doi:0.406/20/47957 Research Article Stromal Expression of CD0 in Invasive Breast Carcinoma and Its Correlation
Mantle Cell Lymphoma
 HEMATOPATHOLOGY Original Article Mantle Cell Lymphoma Morphologic Findings in Bone Marrow Involvement JAY WASMAN, MD, 1 NANCY S. ROSENTHAL, MD,' AND DIANE C. FARHI, MD 2 Although mantle cell lymphoma (MCL),
HEMATOPATHOLOGY Original Article Mantle Cell Lymphoma Morphologic Findings in Bone Marrow Involvement JAY WASMAN, MD, 1 NANCY S. ROSENTHAL, MD,' AND DIANE C. FARHI, MD 2 Although mantle cell lymphoma (MCL),
Pathology of the Lymphoid System
 Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus Irinotecan and Radiotherapy
 Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma
 Case Reports in Otolaryngology Volume 2013, Article ID 384238, 4 pages http://dx.doi.org/10.1155/2013/384238 Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma Kunihiko Tokashiki, Kiyoaki
Case Reports in Otolaryngology Volume 2013, Article ID 384238, 4 pages http://dx.doi.org/10.1155/2013/384238 Case Report A Case of Primary Submandibular Gland Oncocytic Carcinoma Kunihiko Tokashiki, Kiyoaki
Case Report Mantle Cell Lymphoma Mimicking Rectal Carcinoma
 Case Reports in Hematology, Article ID 621017, 4 pages http://dx.doi.org/10.1155/2014/621017 Case Report Mantle Cell Lymphoma Mimicking Rectal Carcinoma Engin Kelkitli, 1 Hilmi Atay, 2 Levent YJldJz, 3
Case Reports in Hematology, Article ID 621017, 4 pages http://dx.doi.org/10.1155/2014/621017 Case Report Mantle Cell Lymphoma Mimicking Rectal Carcinoma Engin Kelkitli, 1 Hilmi Atay, 2 Levent YJldJz, 3
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child
 Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Clinicopathologic features of 112 cases with mantle cell lymphoma
 Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting
 Original Article DOI: 10.21276/APALM.1364 CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting Sakthi Sankari S 1 *, Arjunan A 2, Bhuvaneswari M.G. 2, Sindhuja
Original Article DOI: 10.21276/APALM.1364 CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting Sakthi Sankari S 1 *, Arjunan A 2, Bhuvaneswari M.G. 2, Sindhuja
Composite mantle cell and follicular lymphoma. A case report
 Human Pathology (2009) 40, 259 263 www.elsevier.com/locate/humpath Case study Composite mantle cell and follicular lymphoma. A case report Raquel B. Ilgenfritz MD a,, Agnès Le Tourneau MD a, Michel Arborio
Human Pathology (2009) 40, 259 263 www.elsevier.com/locate/humpath Case study Composite mantle cell and follicular lymphoma. A case report Raquel B. Ilgenfritz MD a,, Agnès Le Tourneau MD a, Michel Arborio
Case Report Autoimmune Hemolytic Anemia and Nodular Lymphocyte-Predominant Hodgkin Lymphoma: A Rare Association
 Case Reports in Hematology Volume 2013, Article ID 567289, 5 pages http://dx.doi.org/10.1155/2013/567289 Case Report Autoimmune Hemolytic Anemia and Nodular Lymphocyte-Predominant Hodgkin Lymphoma: A Rare
Case Reports in Hematology Volume 2013, Article ID 567289, 5 pages http://dx.doi.org/10.1155/2013/567289 Case Report Autoimmune Hemolytic Anemia and Nodular Lymphocyte-Predominant Hodgkin Lymphoma: A Rare
T Cell/Histiocyte-Rich Large B Cell Lymphoma of the Thymus: A Diagnostic Pitfall.
 Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pathology Faculty Publications Pathology 1-1-2016 T Cell/Histiocyte-Rich Large B Cell Lymphoma of the
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pathology Faculty Publications Pathology 1-1-2016 T Cell/Histiocyte-Rich Large B Cell Lymphoma of the
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule
 Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Differential cell counts in the histiocytic variant of lymphocytic predominance subtype of Hodgkin's
 Journal of Clinical Pathology, 1978, 31, 1234-1238 Differential cell counts in the histiocytic variant of lymphocytic predominance subtype of Hodgkin's disease FIONA I. SUTHERLAND, J. B. MAcGILLIVRAY,
Journal of Clinical Pathology, 1978, 31, 1234-1238 Differential cell counts in the histiocytic variant of lymphocytic predominance subtype of Hodgkin's disease FIONA I. SUTHERLAND, J. B. MAcGILLIVRAY,
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma
 T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
Protocol for the Examination of Specimens From Patients With Hodgkin Lymphoma*
 Protocol for the Examination of Specimens From Patients With Hodgkin Lymphoma* Version: Hodgkin 3.1.0.1 Protocol Posting Date: October 2013 This protocol is NOT required for accreditation purposes *This
Protocol for the Examination of Specimens From Patients With Hodgkin Lymphoma* Version: Hodgkin 3.1.0.1 Protocol Posting Date: October 2013 This protocol is NOT required for accreditation purposes *This
Solomon Graf, MD February 22, 2013
 Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Mediastinal B-cell Lymphomas
 Mediastinal B-cell Lymphomas A Spectrum of Diseases Wyndham H. Wilson, MD, PhD Mediastinal B-cell Lymphomas Nodular sclerosis Hodgkin Lymphoma Mediastinal grey zone lymphoma Primary mediastinal B-cell
Mediastinal B-cell Lymphomas A Spectrum of Diseases Wyndham H. Wilson, MD, PhD Mediastinal B-cell Lymphomas Nodular sclerosis Hodgkin Lymphoma Mediastinal grey zone lymphoma Primary mediastinal B-cell
Lymphoma Update: Lymphoma Update: What s Likely to be New in the New WHO. Patrick Treseler, MD, PhD University of California San Francisco
 Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Hodgkin Lymphomas: An Update
 Hodgkin Lymphomas: An Update Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center November 10 th, 2018 Disclosures Scientific Advisory Board, Allergan Inc, 2018 Hodgkin Lymphomas Classical Hodgkin
Hodgkin Lymphomas: An Update Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center November 10 th, 2018 Disclosures Scientific Advisory Board, Allergan Inc, 2018 Hodgkin Lymphomas Classical Hodgkin
A Unique Case of Nasal NK/T Cell Lymphoma with Frequent Remission and Relapse Showing Different Histological Features During 12 Years of Follow Up
 J Clin Exp Hematopathol Vol. 50, No. 1, May 2010 Case Study A Unique Case of Nasal NK/T Cell Lymphoma with Frequent Remission and Relapse Showing Different Histological Features During 12 Years of Follow
J Clin Exp Hematopathol Vol. 50, No. 1, May 2010 Case Study A Unique Case of Nasal NK/T Cell Lymphoma with Frequent Remission and Relapse Showing Different Histological Features During 12 Years of Follow
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
R. F. Falkenstern-Ge, 1 S. Bode-Erdmann, 2 G. Ott, 2 M. Wohlleber, 1 and M. Kohlhäufl Introduction. 2. Histology
 Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Citation International Journal of Hematology, 2013, v. 98 n. 4, p The original publication is available at
 Title Diagnostic challenges in a case of B cell lymphoma unclassifiable with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma Author(s) So, JCC; Yung, KH; Chu, ML; Wan,
Title Diagnostic challenges in a case of B cell lymphoma unclassifiable with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma Author(s) So, JCC; Yung, KH; Chu, ML; Wan,
11/8/2018 DISCLOSURES. I have NO Conflicts of Interest to Disclose. UTILTY OF DETECTING PATTERNS
 Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma of Thyroid
 Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
The Lymphomas. An overview..
 The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
Hematopathology Specialty Conference Case #1
 Hematopathology Specialty Conference Case #1 Robert (Bob) Ohgami, MD, PhD Assistant Professor Stanford University Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships
Hematopathology Specialty Conference Case #1 Robert (Bob) Ohgami, MD, PhD Assistant Professor Stanford University Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships
Evening specialty conference: Liver
 Evening specialty conference: Liver Joseph Misdraji, M.D. Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee)
Evening specialty conference: Liver Joseph Misdraji, M.D. Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee)