A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
|
|
|
- Vivien Parrish
- 5 years ago
- Views:
Transcription


1 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D.
2 Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and immunohistochemistry Molecular analysis High resolution imaging Image-guided biopsies
3 Classification System Impacts Use of FNABs to Diagnosis Lymphomas Incorporation of cytomorphology, immunophenotype, genetic features, & clinical findings: 1994 Revised European-American Classification of Lymphoid Neoplasms (REAL) 2001 WHO Classification Updated 3 rd ed WHO Classification Updated 4 th ed WHO Classification Updated Re 4 th ed.

4 2017 WHO Classification of Haematopoietic and Lymphoid Tissues 17 new entities Mature B-cell NHL: T-cell NHL Hodgkin variants 5 5 WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues Rev 4 th ed.
 Assess adequacy of material for ancillary studies (FCM, molecular) AFIP Tumors of the Lymph Nodes and Spleen 2017.")
5 Small Needle Bxs in Dx Lymphomas Assess lymphadenopathy Primary diagnosis of lymphoma Diagnose recurrence of lymphoma Assess for transformation to higher grade lymphoma Diagnose secondary neoplasms Assess adequacy of lesion for additional sampling (i.e., necrosis, protocol studies) Assess adequacy of material for ancillary studies (FCM, molecular) AFIP Tumors of the Lymph Nodes and Spleen Series 4.
6 Advantages of Concurrent Core Needle Bx & FNA Both can be done in an outpatient setting Increase likelihood of Diff Dx with cyto & histo findings correlated Optimal for directing sampling (necrotic) Can assess the adequacy for ancillary studies In this era of small biopsies, optimal to obtain as much tissue as possible with one procedure
 One of the most referred to papers on FNAs in the workup of lymphomas HOWEVER, No ROSE, limited FLOW results, limited material, no workflow for triaging")
7 Only 12% of FNA had concordant with excisional bx (most common dx were atypical, non-dx and lymphoma without subtype); 29% given an acceptable classification (REAL/WHO) One of the most referred to papers on FNAs in the workup of lymphomas HOWEVER, No ROSE, limited FLOW results, limited material, no workflow for triaging FNAs 2004
8 Diagnosing Lymphomas on FNABs Requires knowledge of the most recent WHO classification; know the limitations of FNAB Multiparameter approach ROSE helpful in obtaining optimal material/ aspirator willing to aspirate for ancillary studies &/or core needle biopsy Workflow for proper handling of specimens Takes time & effort (can t sign out in 1 or 2 days) Collaboration -hematopathologist with expertise in flow cytometry

9 Triaging Small Needle Biopsies 1st 2nd
10 Challenges of Dx Lymphomas by FNABs Identifying cases with partial involvement Assessment of pattern in FL and MCL Grading follicular lymphoma; however, low vs. high is often achievable Diffuse large B-cell vs. Burkitt lymphoma CLL/SLL with prominent pseudofollicles vs. Richter syndrome Composite lymphomas AFIP Tumors of the Lymph Nodes and Spleen Series 4.
11 Challenges of Dx Lymphomas on FNABs AITL vs reactive lymphadenopathy AITL vs peripheral T-cell lymphoma (PTCL) Variants of ALK-positive ALCL ALK- ALCL vs classic Hodgkin lymphoma ALK-ALCL vs CD30+ PTDL Natural killer cell lymphoma Nodular predominant HL vs progressive transformation of germinal centers Nodular predominant HL vs T-cell rich LBCL Subclassification of HL AFIP Tumors of the Lymph Nodes and Spleen Series 4.
12 FREQUENCIES OF B-CELL LYMPHOMA SUBTYPES IN ADULTS MCL CLL/SLL MALT FOLLICULAR LYMPHOMA DLBCL Diffuse large B-cell Follicular lymphoma MALT lymphoma Mantle cell lyphoma CLL/SLL Primary med large B-cell High grade B, NOS Burkitt Splenic marginal zone Nodal marginal zone Lymphoplasmacytic WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Ed. Swerdlow S.
13 ??? Future of FNABs FNABs are optimal for mutational analysis in era of small bx & personalized medicine Aid in the further subtyping of lymphomas Prognostic marker Therapeutic indicator Need to collaborate with Hematopathology Advocates for LN FNABs
 Correlate cytology & ancillary studies Use WHO classification Coulter counter: evaluates # of")
14 Strategy For Obtaining Optimal Material for Ancillary Studies Immediate assessment with optimal preparations (Pap & DQ smears) Triage material for ancillary studies (optimal 5-10 million cells; 10 ml of RPMI+ media) Correlate cytology & ancillary studies Use WHO classification Coulter counter: evaluates # of mononuclear cells
15 Multiparameter Approach Clinical history - age, prior neoplasms, LN site & size, localized vs. general lymphadenopathy, systemic symptoms Cytomorphology - major cell type, cellularity, arrangement, background Ancillary studies
16 Ancillary Studies Flow Cytometry -Routinely send on all cases with clinical/radiographic suspicion of a lymphoma except for Hodgkin lymphoma** Gene Rearrangements Selected cases that have been difficult to classify by immunophenotyping or suspected T-cell lymphomas (rinse) Fluorescence in situ hybridization (FISH) Selected cases suspected lymphoma with a characteristic translocation that is difficult to classify (DQ slides, cytospin, cell block)
17

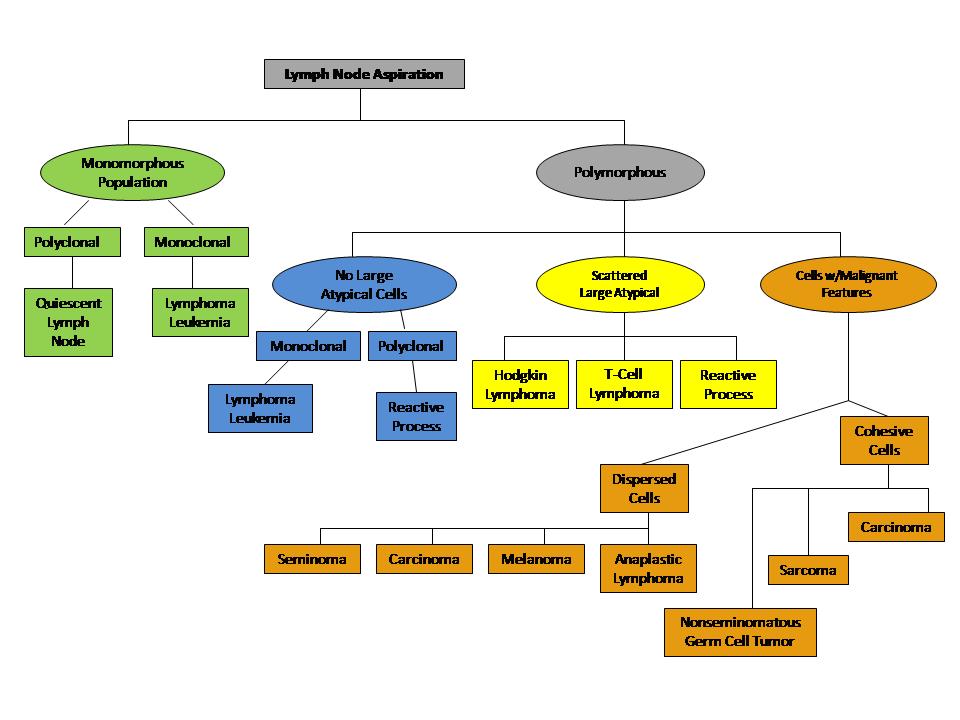
18 Lymph Node Cell Population Dendritic reticulum cells Cleave cells Tingible body macrophage Large non-cleaved cell
19 Differential Diagnosis of Monomorphous Lymphoid Population Based on Size Monomorphous Population of Lymphoid Cells Small Cells Reactive Lymph Node Small Lymphocytic Lymphoma Lymphoplasmacytic Lymphoma Follicular Lymphoma Mantle Cell Lymphoma Intermediate Cells Lymphoblastic Lymphoma Burkitt Lymphoma Large Cells Large Cell Lymphoma Follicular Lymphoma Grade 3 Blastoid variant mantle cell lymphoma


20 LYMPHOMAS COMPOSED OF SMALL CELLS?


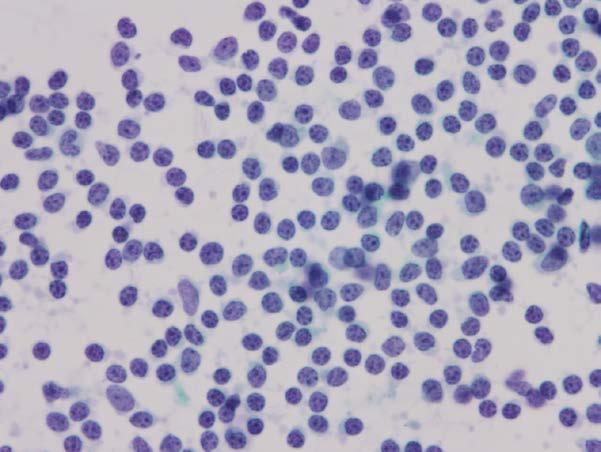
21 Case 1: 81 y/o with right axillary mass Paraimmunoblast Paraimmunoblast
22 Case 1: Differential Diagnosis Malignant Small lymphocytic lymphoma Follicular lymphoma, lowgrade Mantle cell lymphoma Lymphoplasmacytic lymphoma Hodgkin lymphoma (nodular lymphocyte predominant) Benign Reactive lymph node
23 Differential Diagnosis of Small Cell B-Cell Lymphomas LYMPHOMA IMMUNOPHENOTYPES CYTOGENETICS CD5 CD23 CD10 CD20 Small Lymphocytic Trisomy 12, del 13q14 Lymphoplasmacytic No specific abnormality Mantle Cell t(11;14)(q13;32) Marginal Zone MALT Trisomy 3; t(11;18)(q21;q21) Follicular, low grade - -/+ + + t(14;18)(q32;q21)
24 Case 1: Ancillary Studies 10 4 Flow Cytometry: CD20+ (dim), CD19+, CD5+ CD23+, CD200+, CD10-, FMC CD CD19 KAPPA LAMBDA 10 3 CD CD19 CD5 (weak +) Ki-67


,")






25 Case 1: Ancillary Studies 10 4 Flow Cytometry: CD20+ (dim), CD19+, CD5+ CD23+, CD200+, CD10-, FMC-7- CD FLOW CD19 KAPPA LAMBDA CYTOSPIN CD CD19 CD5 (weak +) Ki-67
26 Small Lymphocytic Lymphoma Accounts for 7% of non-hodgkin lymphomas Often associated with chronic lymphocytic leukemia Majority of patients are >50 years and have involvement of lymph nodes, liver and spleen Clinical course is indolent but not curable; may transform to large cell lymphoma & rarely HL
27 Things To Think About Typically SLL can be differentiated from other small lymphomas with immunophenotyping SLL with prominent pseudofollicles vs SLL accelerated phase /transformed LBCL may be challenging
28 Richter Syndrome 2-8% of pts with SLL/CLL transform 2-8% Diffuse large B-cell lymphoma 0.5% Hodgkin lymphoma Sudden onset of rapidly progressive lymphadenopathy & B symptoms: fever, night sweats, &/or weight loss Common sites: lymph nodes, BM, PB, spleen DLBCL: clonally related or unrelated to SLL/CLL immunophenotype Poor prognosis


29 Transformed Large B-cell Lymphoma in Patient with Hx of SLL/CLL TBM
30 FNA of Axillary LN with hx of CLL/SLL &


31 Metastatic Merkel to LN with SLL Squamous cell ca, Merkel cell ca, adenocarcinoma have been describes met to LN with SLL/CLL


32 Case 2: 70 y/o man with a 1.8 cm axillary nodule
33 Case 2: Differential Diagnosis Malignant Small lymphocytic lymphoma Follicular lymphoma, lowgrade Mantle cell lymphoma Lymphoplasmacytic lymphoma Hodgkin lymphoma (nodular lymphocyte predominant) Benign Reactive lymph node



34 Case 2: Ancillary Studies Immunophenotyping: Kappa light chain restricted, CD20+, CD19+, CD5+, CD10-, CD23-, CD200- H & E CB CyclinD1 Sox11
35 Mantle Cell Lymphoma Comprises about 4% of all non-hodgkin lymphomas Occurs primarily in men in 7 th decade and presents with generalized lymphadenopathy MCL should be distinguished from other small cell B-cell lymphomas, because clinically more aggressive Classic type composed of monomorphous small to medium-sized lymphocytes with irregular nuclei; other variants including blastoid, pleomorphic, MCL-HPI
 next to the CCND1 gene (11q13) which is thought to lead to overexpression of cyclin D1 No")
36 Mantle Cell Lymphoma Characteristic t(11;14)(q13;q32) translocation Reciprocal translocation results in the juxtaposition of the transcriptional enhancer on IgH locus (14q32) next to the CCND1 gene (11q13) which is thought to lead to overexpression of cyclin D1 No Fusion Dual Fusion
37 Things to Think About MCL is more aggressive than other small cell lymphomas Immunophenotyping important Patterns cannot be determined on FNAs (MCLs with mantle-zone pattern are considered to be more indolent and maybe tx ed differently than those with nodular & diffuse patterns) Blastoid & pleomorphic variants are more difficult to diagnosis on FNABs
38 Things to Think About CyclinD1 staining on cytospins is not as reliable as on cell block preparations Immunstaining for Cyclin D1 has been reported in some cases of HCL& plasma cell myeloma as well as histiocytes & many types of ca (breast, thyroid, colorectal, urinary bladder) Immunostaining for SOX11 has been reported in some cases of HCL, Burkitt lymphoma, & plasma cell myeloma Need Ki-67 to detect MCL with HPI, can t tell on cytomorphology alone

39 Case 3: 68 y/o man with a 9 cm pelvic mass
40 Case 3: Differential Diagnosis Benign Reactive Hyperplasia Malignant Follicular lymphoma MCL, SLL, MZL Partial involvement of lymphoma

41 Case 3: Ancillary Studies Flow Cytometry: Positive: Kappa light chain restricted, CD20, CD19, CD10, CD23 Negative: CD5, CD200, CD30 Ki-67: Approximately 10% of cells staining CD20 ->
42 Follicular Lymphoma Accounts for 35% of non-hodgkin B-cell lymphomas in US and 22% worldwide Usually occurs in older adults and primarily involves lymph nodes Composed of follicle center B-cells (cleaved and non-cleaved cells) type cells vary with grade
43 Follicular Lymphoma Immunophenotype: CD20+, CD19+, CD10+, CD5-, CD23+ (BCL-2+ and BCL- 6+; both need architecture to evaluate ) Update WHO classification defines 3 histologic grades based on number of centroblasts/hpf in tissue On cytology Low-grade (grade 1 & 2) High-grade (grade 3/Large cell lymphoma of follicle center cell origin)

44 Follicular Lymphoma Characteristic t(14;18)(q32;q21) translocation Reciprocal translocation results in the fusion of the IgH gene and the BCL2 gene leading to overexpression of the BCL2 protein On FISH, fusion signal; can be done on cytospin Dual fusion indicative of t (14;18)

45 Sensitivity for dx FL was 89% & 66% of LG FL; later increase to 94% if performed Review of not-graded: 45% LG, 35 % indetermine due to polymorphous lymphoid cells with increased large cells, & 20% scant cellularity Part-time faculty did not grade 54% vs full-time cytopathologist 19%

46 FNA: Follicular lymphoma, low-grade Bx: Follicular lymphoma, grade 1


47 FNA: Follicular lymphoma, NOS Bx: Follicular lymphoma, grade 1-2


48 FNA: Follicular lymphoma, suggestive of gr. 2-3 Bx: Follicular lymphoma, grade 3A
49 Case 3: Things to Think About FNA cannot reliably determine the pattern in FLs Grading FL on FNAs Low grade (grades 1 & 2) High grade (grades 3) Distinguishing between grades 1 & 2 or 2 & 3A can be problematic Subset with polymorphous population with increased large cells may be difficult to grade Can t reliably differentiate FL HG from CD10+ diffuse large cell lymphoma

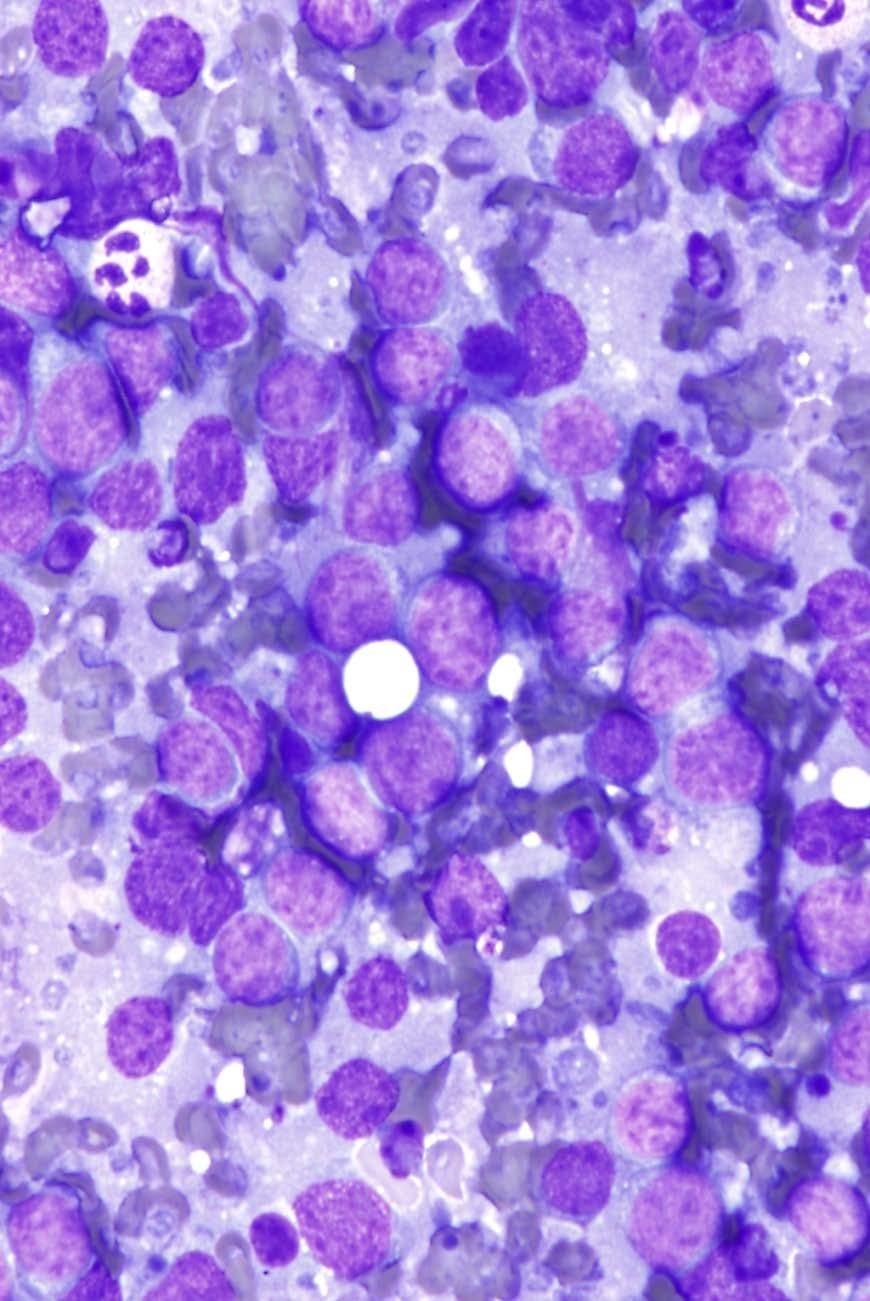
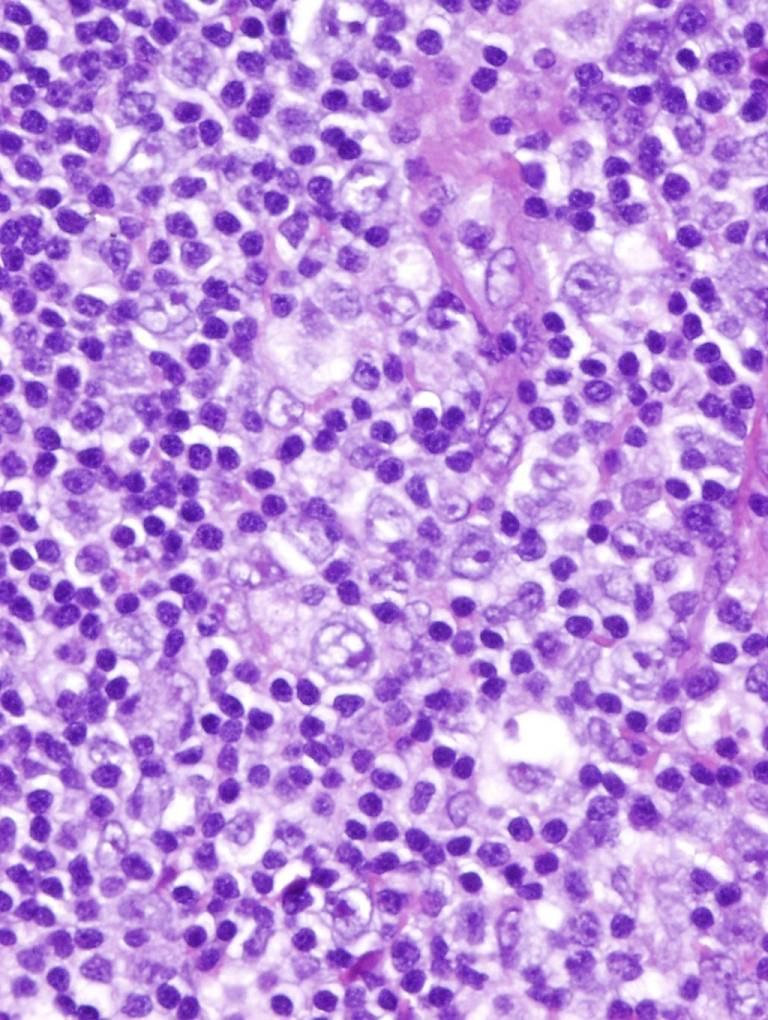
50 Case 4: 40 y/o man with abdominal lymphadenopathy
51 Case 4: Differential Diagnosis Burkitt lymphoma Diffuse Large B-cell lymphoma Morphologic variants Molecular variants Germinal center B-cell subtype Activated B-cell subtype High-grade B-cell Lymphoma High-grade B-cell lymphoma with MYC & BCL2 &/or BCL6 rearrangements High-grade B-cell lymphoma, NOS
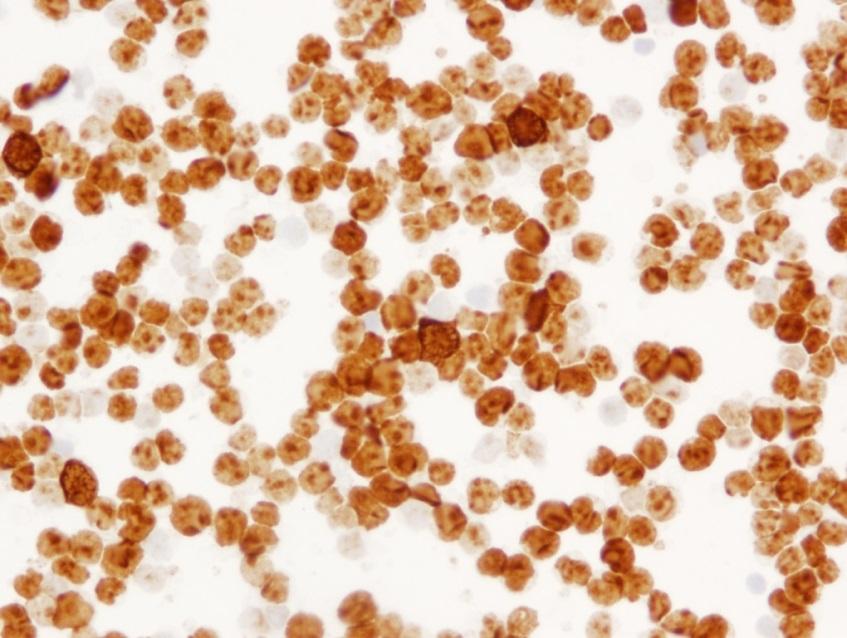
52 Case 4: Ancillary Studies Flow Cytometry Positive for CD20, CD22, CD19, CD10, CD38 Negative for CD5, CD3 Kappa light chain restricted Immunocytochemistry Ki-67 > 95% cells staining
, TdT-, >90% Ki-67 Often")
 or")
53 Burkitt Lymphoma B-cell Ag+, CD10+, EBER+ CD38+, (need architecture to assess BCL6+, BCL2-/+), TdT-, >90% Ki-67 Often associated with t(8;14)(q24;q32) results in MYC at 8q24 adjacent to heavy chain region on 14q32 and less frequently with t(2;8) or t(8;22) EBER Ki-67
54 Case 4: Things To Think About CD10+ BL can be misinterpreted as large B- cell lymphoma (LBCL) of germinal center origin Burkitt-like lymphoma with 11q aberration Some DLBCL can have round nuclei, cytoplasmic vacuoles, high mitotic index, and tingible body macrophages mimicking BL High-grade B-cell Lymphoma High-grade B-cell lymphoma with MYC & BCL2 &/or BCL6 rearrangements High-grade B-cell lymphoma, NOS

55 Diffuse Large B-cell Lymphoma with high-grade features



56 Case 5: 63 y/o woman had a hx of breast cancer 2 yr ago; now has a 2 cm axillary LN Ki-67


57 Case 5: Breast cancer 2 yrs earlier
58 Case 5: Rt. Breast FNA: Large B-cell Lymphoma (FCM: kappa restricted population positive for CD19, CD20, CD22, CD38, & CD44; negative for CD10, CD5, CD23, CD30; Ki67 >90%) Rt. Axilla FNA: Reactive polymorphous lymphoid tissue (FCM: Polytypic)

59 Large B-cell Lymphoma LBCL- no longer adequate dx for tx Morphologic variants: centroblastic, immunoblastic, anaplastic, other rare variants Molecular Subtypes Germinal center B-cell Better survival Activated B-cell Worse survival GCB ACB WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues 2017
60 Case 5: Things to Think About Previous clinical hx is important Cancer doesn t necessarily mean carcinoma Compare with previous cytology/histology Ancillary studies may be helpful in selected cases (unexplained lymphadenopathy) Ki-67 is elevated in reactive LNs


61 Case 6: 22 y/o man with a hx of Hodgkin lymphoma and now has 2 cm neck node
62 Case 6: Differential Diagnosis Benign Reactive LN Lymphoma Hodgkin lymphoma B-cell lymphoma Follicular lymphoma Marginal zone lymphoma T-cell lymphoma
63 Case 6: Ancillary Studies Flow cytometry: polytypic B-cells, immunophenotypically unremarkable T-cells and NK-cells Note: Fine needle aspiration with flow cytometry is an insensitive means of detecting certain types of lymphoma (most notably, T- cell rich large B-cell lymphoma, lymphocyte predominant Hodgkin lymphoma and some subtypes of T-cell lymphoma).
64 Reactive Hyperplasia Infections Draining primary tumors Following biopsy Autoimmune Idiopathic

65 Case 6: Histology
66 Case 6: Cytology & Histology FNA Dx: Atypical lymphoid proliferation, favor reactive process Excisional Bx: Prominent follicular and interfollicular hyperplasia with monocytoid B- cells and multiple neutrophilic microabscesses Comment: Warthin-Starry stain shows clusters & single rod-like organisms (possible Bartonella) in some microabscesses, cultures had no growth
67 Cat Scatch Disease Necrotizing inflammation cause by Bartonella B. henselae causes CSD in mostly immunocompetent pts 90% of pts report contact with cats Bacilli transmitted to humans through bite or scratch of infected cat Granuloma formation results from activation and accumulation of histiocytes Bacilli identified by Warthin-Starry stain; also serology
68 Case 6: Things To Think About Immunophenotyping can be helpful in assessing clonality FNA cannot reliably assess reactive lymphadenopathies with architectural features (Castleman dz, Kimura dz, Kikuchi-Fujumoto dz, Toxoplasmosis, others) Aspirated material can be sent for cultures
69 Conclusions A multiparameter approach is imperative to diagnose lymphoproliferative disorders by FNAB ROSE for triaging material for ancillary studies is optimal
70 Conclusions Most B-cell lymphomas can be subclassified with the aid of immunophenotyping and proliferation indices When in DOUBT, get more tissue, core it or take it OUT

71 THANK YOU FOR ATTENTION!
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Lymph node cytopathology : A practical approach to lymphoproliferative disorders
 Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms
 Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms Rana S. Hoda FINE NEEDLE ASPIRATION Introduction Fine needle aspiration (FNA) is a well-established
Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms Rana S. Hoda FINE NEEDLE ASPIRATION Introduction Fine needle aspiration (FNA) is a well-established
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Dispersed Cell Population & Lymphoglandular Bodies: Features of lymphoid aspirates FNA OF LYMPH NODES OF THE HEAD AND NECK
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF LYMPH NODES OF THE HEAD AND
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF LYMPH NODES OF THE HEAD AND
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Lymphoma Update: Lymphoma Update: What s Likely to be New in the New WHO. Patrick Treseler, MD, PhD University of California San Francisco
 Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
11/8/2018 DISCLOSURES. I have NO Conflicts of Interest to Disclose. UTILTY OF DETECTING PATTERNS
 Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
PhenoPath. Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA
 PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Diagnosis of lymphoid neoplasms has been
 Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
Approach to Core Biopsy Specimens
 BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Ruth L. Katz, M.D. Chief Research Cytopathology, Professor of Pathology, University of Texas. M.D. Anderson Cancer Center.
 Practical FNA in Lymphoma Diagnosis: What the Clinician wants to Know and How to Get There! Ruth L. Katz, M.D. Chief Research Cytopathology, Professor of Pathology, University of Texas M.D. Anderson Cancer
Practical FNA in Lymphoma Diagnosis: What the Clinician wants to Know and How to Get There! Ruth L. Katz, M.D. Chief Research Cytopathology, Professor of Pathology, University of Texas M.D. Anderson Cancer
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Low-grade B-cell lymphoma
 Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
9/28/2017. Follicular Lymphoma and Nodal Marginal Zone Lymphoma. Follicular Lymphoma Definition. Low-Grade B-Cell Lymphomas in WHO Classification
 and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo
 Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
GENETIC MARKERS IN LYMPHOMA a practical overview. P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute
 GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Tres
 Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Follicular Lymphoma: the WHO
 Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor
: Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor") HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD
 HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD") HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
Classification! Immunohistochemical classification of haematolymphoid tumours. Malignant lymphoproliferative diseases
 Immunohistochemical classification of haematolymphoid tumours Haematolymphoid Neoplasias: Leukaemia vs Lymphoma C L O N A L M A L I G N A N C I E S Stephen Hamilton-Dutoit Institute of Pathology Aarhus
Immunohistochemical classification of haematolymphoid tumours Haematolymphoid Neoplasias: Leukaemia vs Lymphoma C L O N A L M A L I G N A N C I E S Stephen Hamilton-Dutoit Institute of Pathology Aarhus
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,
: Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,") High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
Aggressive B-cell Lymphoma 2013
 Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting
 Original Article DOI: 10.21276/APALM.1364 CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting Sakthi Sankari S 1 *, Arjunan A 2, Bhuvaneswari M.G. 2, Sindhuja
Original Article DOI: 10.21276/APALM.1364 CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting Sakthi Sankari S 1 *, Arjunan A 2, Bhuvaneswari M.G. 2, Sindhuja
VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping
 VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping 1 12/4/2015 9:47:24 AM 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping
VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping 1 12/4/2015 9:47:24 AM 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping
VENTANA hematopathology solutions. Deliver diagnostic confidence
 VENTANA hematopathology solutions Deliver diagnostic confidence 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping hematological cancers 4 The importance
VENTANA hematopathology solutions Deliver diagnostic confidence 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping hematological cancers 4 The importance
Efficacy of cell block immunocytochemistry in the diagnostic workup of non hodgkin lymphoma-experience from a tertiary care hospital in North India
 Original Research Article DOI: 10.18231/2394-6792.2018.0041 Efficacy of cell block immunocytochemistry in the diagnostic workup of non hodgkin lymphoma-experience from a tertiary care hospital in North
Original Research Article DOI: 10.18231/2394-6792.2018.0041 Efficacy of cell block immunocytochemistry in the diagnostic workup of non hodgkin lymphoma-experience from a tertiary care hospital in North
A 64yo female with tuberculous empyema not improving on treatment: A tribute and farewell to Dr. Alphonse Kayembe
 A 64yo female with tuberculous empyema not improving on treatment: A tribute and farewell to Dr. Alphonse Kayembe Continuing Medical Education Announcement Harvard Medical School RSS 3081: Monthly BOTSOGO
A 64yo female with tuberculous empyema not improving on treatment: A tribute and farewell to Dr. Alphonse Kayembe Continuing Medical Education Announcement Harvard Medical School RSS 3081: Monthly BOTSOGO
Abstract. Anatomic Pathology / DIAGNOSIS AND SUBCLASSIFICATION OF PRIMARY AND RECURRENT LYMPHOMA
 Anatomic Pathology / DIAGNOSIS AND SUBCLASSIFICATION OF PRIMARY AND RECURRENT LYMPHOMA Diagnosis and Subclassification of Primary and Recurrent Lymphoma The Usefulness and Limitations of Combined Fine-Needle
Anatomic Pathology / DIAGNOSIS AND SUBCLASSIFICATION OF PRIMARY AND RECURRENT LYMPHOMA Diagnosis and Subclassification of Primary and Recurrent Lymphoma The Usefulness and Limitations of Combined Fine-Needle
Fine-Needle Aspiration Cytology in the Diagnosis of Lymphoma The Next Step
 Fine-Needle Aspiration Cytology in the Diagnosis of Lymphoma The Next Step Linda M. Sandhaus, MD Since 985, almost 2 articles have been published in the medical literature on the subject of fine-needle
Fine-Needle Aspiration Cytology in the Diagnosis of Lymphoma The Next Step Linda M. Sandhaus, MD Since 985, almost 2 articles have been published in the medical literature on the subject of fine-needle
Pulmonary biopsy specimens demonstrate
 A PRACTICAL APPROACH TO THE EVALUATION OF LYMPHOID AND PLASMA CELL INFILTRATES IN THE LUNG Fiona E. Craig, MD KEYWORDS Lymphoma Pulmonary Immunophenotyping Genotyping ABSTRACT Pulmonary biopsy specimens
A PRACTICAL APPROACH TO THE EVALUATION OF LYMPHOID AND PLASMA CELL INFILTRATES IN THE LUNG Fiona E. Craig, MD KEYWORDS Lymphoma Pulmonary Immunophenotyping Genotyping ABSTRACT Pulmonary biopsy specimens
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Pathology of the Lymphoid System
 Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Test Utilization: Chronic Lymphocytic Leukemia
 Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
I n the past 10 years, fine needle aspiration (FNA) cytology
 cytology") 821 ORIGINAL ARTICLE Fine needle aspiration cytology in the diagnosis of uncommon types of lymphoma F Mayall, A Darlington, B Harrison... See end of article for authors affiliations... Correspondence to:
821 ORIGINAL ARTICLE Fine needle aspiration cytology in the diagnosis of uncommon types of lymphoma F Mayall, A Darlington, B Harrison... See end of article for authors affiliations... Correspondence to:
5/16/2018 HEMATOPATHOLOGY FOR CYTOPATHOLOGISTS HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS I HAVE NOTHING TO C DISCLOSE
 HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium I HAVE NOTHING TO C DISCLOSE Kathryn
HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium I HAVE NOTHING TO C DISCLOSE Kathryn
Clinicopathologic features of 112 cases with mantle cell lymphoma
 Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
The next lymphoma classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno
 Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Classifications of lymphomas
 Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Unknown Case 6. Ann T. Moriarty, MD
 Unknown Case 6 Ann T. Moriarty, MD Unknown Case 6 61 year old male with an enlarged cervical lymph node. He has a history of lung carcinoma, renal cell carcinoma and lymphoma. Case 6 Image 1: Fine needle
Unknown Case 6 Ann T. Moriarty, MD Unknown Case 6 61 year old male with an enlarged cervical lymph node. He has a history of lung carcinoma, renal cell carcinoma and lymphoma. Case 6 Image 1: Fine needle
Workshop Case # 8 (H 4205/07)
") Workshop Case # 8 (H 4205/07) 53 y old male patient had a history of gastrectomy 15 years earlier for gastric carcinoma.on routine sonographic and CT control an enlarged lymph node was detected in the
Workshop Case # 8 (H 4205/07) 53 y old male patient had a history of gastrectomy 15 years earlier for gastric carcinoma.on routine sonographic and CT control an enlarged lymph node was detected in the
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas
 ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
WHO UPDATE ON LYMPHOMAS. Dr Priya Mary Jacob Asst Professor, Pathology.
 WHO UPDATE ON LYMPHOMAS Dr Priya Mary Jacob Asst Professor, Pathology 3 rd 4 th 4 th revised 2001 2008 2017 The Change The Significance of the Change- Diagnostic, Prognostic The Rationale behind the change.
WHO UPDATE ON LYMPHOMAS Dr Priya Mary Jacob Asst Professor, Pathology 3 rd 4 th 4 th revised 2001 2008 2017 The Change The Significance of the Change- Diagnostic, Prognostic The Rationale behind the change.
Low-Grade B-Cell Lymphomas in WHO Classification. Follicular Lymphoma Definition. Follicular Lymphoma Clinical Features 11/7/2017 DISCLOSURES
 Low-Grade B-Cell Lymphomas in WHO Classification DISCLOSURES I do not have anything to disclose Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6 % Small lymphocytic lymphoma/cll
Low-Grade B-Cell Lymphomas in WHO Classification DISCLOSURES I do not have anything to disclose Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6 % Small lymphocytic lymphoma/cll
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Successful flow cytometric immunophenotyping of body fluid specimens
 Successful flow cytometric immunophenotyping of body fluid specimens Fiona E. Craig, MD Division of Hematopathology Mayo Clinic Arizona 2017 MFMER slide-1 Financial disclosure No conflicts 2017 MFMER slide-2
Successful flow cytometric immunophenotyping of body fluid specimens Fiona E. Craig, MD Division of Hematopathology Mayo Clinic Arizona 2017 MFMER slide-1 Financial disclosure No conflicts 2017 MFMER slide-2
OUTLINE OF SHORT COURSE WHO CLASSIFICATION DEFINITION OF A LYMPHOMA. FOLLICULAR LYMPHOMA: Outline of Talk. FOLLICULAR LYMPHOMA: Outline of Talk
 OUTLINE OF SHORT COURSE WHO CLASSIFICATION B-CELL LYMPHOMAS: A PRACTICAL & COST-EFFECTIVE APPROACH TO DIAGNOSIS 1. WHO classification: Integrated approach to diagnosis 2. Practical & cost- effective approach
OUTLINE OF SHORT COURSE WHO CLASSIFICATION B-CELL LYMPHOMAS: A PRACTICAL & COST-EFFECTIVE APPROACH TO DIAGNOSIS 1. WHO classification: Integrated approach to diagnosis 2. Practical & cost- effective approach
, , 2011 HODGKIN LYMPHOMA
 European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
10/31/2017. Immunodeficiencies. Outline. Discuss EBV. Non-destructive Polymorphic Monomorphic Therapies Challenges
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
Thomas Hodgkin and Hodgkin lymphoma
 J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
11/2/2017. Immunodeficiencies. Joo Y. Song, MD Assistant Professor of Clinical Pathology. I have no financial disclosures.
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Lymphatic system component
 Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory. Dr Paula Waits Bristol Genetics Laboratory
 The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
FINALIZED SEER SINQ S NOVEMBER 2011
 : 20110133 Multiple primaries/heme & Lymphoid Neoplasms: A patient was diagnosed 7/31/08 with DLBCL (9680/3) (biopsy left supraclav. node), stage IIIB. Treated with chemo. 10/14/10 biopsy right supraclav.
: 20110133 Multiple primaries/heme & Lymphoid Neoplasms: A patient was diagnosed 7/31/08 with DLBCL (9680/3) (biopsy left supraclav. node), stage IIIB. Treated with chemo. 10/14/10 biopsy right supraclav.