Keynote Lecture: Optimal Management of HCV-HIV Coinfection
|
|
|
- Isabel Maxwell
- 6 years ago
- Views:
Transcription


1 THASL Annual Meeting 2015 Keynote Lecture: Optimal Management of HCV-HIV Coinfection 26 February 2015 Prof. Chutima Pramoolsiansap
2 Today s Talk HIV/HCV-coinfection Background and epidemiology When to start treatment and which regimens Management : Treat now or wait for future options? HCV Treatment landscape of oral DAA s AASLD/IDSA and EASL Treatment guidelines Treatment monitoring: efficacy, stopping rules, SVR-guided therapy, safety Drug drug interactions among HCV antivirals and HIV antiretroviral agents Summary: Optimizing treatment success for HIV/HCV-coinfected patients
3 Background and Epidemiology D:A:D Study: causes of death in patients followed HIV/HCV epidemiology Approximately 25% of HIV+ patients are coinfected with HCV 80% of HIV+ patients who inject drugs are coinfected with HCV All patients with HIV infection should be tested for HCV HIV+ patients are at 4.1 times the risk of HCV as HIV- patients HIV accelerates natural course of hepatitis C Liver disease associated with HCV infection become a leading cause of morbidity and mortality among HCV/HIV-coinfected patients Weber R, et al. Arch Intern Med. 2006;166: CDC. HIV and viral hepatitis. May Yaphe S, et al. Sex Transm Infect. 2012;88:

4 J Med Assoc Thai ;87: Am J Trop Med Hyg. 2010;83(2): Epidemiol. Infect. 2013;141: HIV-NAT, Thai Red Cross AIDS Research Centre, Thailand Prevalence of HIV/HCV coinfection Worldwide, approx. 30 % of HIV are coinfected with HCV. Burden of HIV/HCV in Asia 3.5 million HIV 32 million HCV % HCV prevalence in HIV 10.4% heterosexual MSM PWID Blood products PWID;People Who Inject Drugs 7 other In Asia, underestimation of HCV coinfection in HIV 65.3% had HCV testing. 17.7% had positive HCV Ab. Only 4.4% of those had received HCV PCR testing In Thailand, prevalence HIV/HCV coinfected patients was %
5 Chronic hepatitis B and C co-infection increased all-cause mortality in HAART-naive HIV patients in northern Thailand N= 755 HAART-naive HIV-infected patients, 700 (92.6%) patients with complete data Prevalence HCV/HIV and HBV/HIV coinfection: 3.3% and 11.9% Kaplan Meier survival probability HIV/HBV and HIV/HCV co-infection associated with a higher mortality with adjusted hazard ratios (ahrs) of 1.81 and 1.90, respectively. Epidemiol Infect 2013;141:
6 IL-28b (rs ) and HCV viral load between HIV/HCV and HCV monoinfection, Thailand 130HIV/HCV and 331 HCV monoinfection: GT3:47% ; GT1, 34% GT6:18% IL-28b (%) C/C C/T T/T Total HIV/HCV HCV mono P HCV RNA Median (IQR) 6.2( ) 6.7( ) 5.8(5.6, 6.5) <0.001 HCV RNA > 800,000 copies/ml 141 (58.75) 93(72.09) 48(43.24) <0.001 FibroScan, PKa 7.1( ) 8.5( ) 6.6( ) <0.001 <7.1 kpa, N(%) 220 ( 50.1) 33 (30.6) 187(56.5) < kpa, N (%) 91(20.7) 30 (27.8) 61(18.4) kpa, N (%) 60 (13.8) 19(17.6) 41 (12.4) >14 kpa, N(%) 68 (15.5) 26 (24.1) 42 (12.7) HIV/HCV coinfection: Higher viral load and more fibrosis 2/3 meet criteria for treatment; 1/4 require HCC screening Avihingsanon et al. APASL June


7 HIV/HCV coinfection HIV HCV viral production rates virions/day virions/day half-life < 6 hours 2.7 hours Single-stranded RNA viruses, like HIV and HCV, lack proofreading mechanisms, resulting in high mutational rates Compared with HCV monoinfected patients: HIV/HCV-coinfected patients have Less likely to clear viral infection More rapid rates of fibrosis Higher risk of hepatic decompensation

8 HIV/HCV double-trouble for liver



9 Goal of treatment of HCV infection AASLD 2014: To reduce all-cause mortality and liver-related health adverse consequences, including end-stage liver disease and hepatocellular carcinoma, by achievement of virologic cure as evidenced by an SVR. EASL 2014: To eradicate HCV infection to prevent hepatic cirrhosis, decompensation of cirrhosis, HCC, and death. In patients with cirrhosis, HCV eradication reduces the rate of decompensation and will reduce, albeit not abolish, the risk of HCC. In these patients surveillance for HCC should be continued (Recommendation A1)
10 HCV treatment SVR (%) FDA approved RBV PegIFN (BOC,TVR) IFN 6 mo IFN 12 mo IFN/R 6mo IFN/R 12 mo pegifn 12 mo Olysio (simeprevir) in November 2013 Sovaldi (sofosbuvir) in December 2013 Harvoni (ledipasvir and sofosbuvir) in October pegifn/r 12 mo 80 pegifn/r/ 1st gen. DAA pegifn/r/ Combination SOF or SMP DAAs Viekira Pak (ombitasvir, paritaprevir, ritonavir tab. co-packaged with dasabuvir) in December 2014 EU and Japan approved Daclatasvir in August 2014
11 Treatment of HIV/HCV coinfection
12 AASLD/IDSA Guidance: When to start treatment in HCV/HIV-coinfected patients Treatment is recommended for patients with chronic HCV infection Prioritized in patients at high risk for liver-related complications HCV/HIV coinfection, regardless of fibrosis stage High risk for transmitting HCV to others may decrease transmission and HCV disease prevalence MSM with high-risk sexual practices Active injection drug users AASLD and IDSA. HCV Management Guidance. September 2014.

13 Guidelines for use of antiretroviral agents in HIV-1-infected adults and adolescents ART should be initiated in most HIV/HCV-coinfected patients, regardless of CD4 count Naïve HIV/HCV coinfection CD4 counts <200 cells/mm3 CD4 counts >500 cells/mm3 ART regimen CD4 counts <200 cells/mm 3 had lower HCV treatment responses and higher toxicity rates to PegIFN/RBV than CD4 count > 350 cells/mm 3 (no data in DAAs) until patient is stable antihcv Rx Prefer defer ART until HCV treatment is completed to avoid drug-drug interactions antihcv Rx ART regimen EASL 2014:If the patient has severe immunodeficiency, with a CD4 count <200 cells/ll, should be improved using highly active antiretroviral therapy prior to commencing anti-hcv treatment Last updated November 13, 2014; last reviewed November 13,2014

14 AASLD 2014: Grading system used to rate the level of the evidence and strength of the recommendation for each recommendation

15 EASL 2014: Evidence grading used
16 Recommendation for treatment of HIV/HCV coinfection Indications for HCV treatment in HCV/HIV co-infected persons are identical to those in patients with HCV mono-infection (Recommendation A1) The same treatment regimens can be used in HIV-coinfected patients as in patients without HIV infection, as the virological results of therapy are identical (Recommendation A1)
17 Drugs treatment for HCV/HIV-coinfection Older Medications Pegylated Interferon PegIntron or Pegasys Ribavirin Older Direct Acting Antivirals Boceprevir (Victrelis) (2011) Telaprevir (Incivek) (2011) New Direct Acting Antivirals Olysio (simeprevir) in November 2013 Sovaldi (sofosbuvir) in December 2013 Harvoni (ledipasvir and sofosbuvir) in October 2014 Viekira Pak (ombitasvir, paritaprevir and ritonavir tablets co-packaged with dasabuvir ) in December 2014

18 Patients with SVR (%) PEG + RBV versus PEG versus INF + RBV in HCV & HIV APRICOT Study: Results APRICOT Study: SVR24 by Treatment Regimen and Genotype Peginterferon + Ribavirin Peginterferon + Placebo Interferon + Ribavirin All Genotype 1 Genotype 2 or 3 Torriani FJ, et. al. N Engl J Med. 2004;351:

19 Patients with SVR (%) Peginterferon + RBV versus Interferon + RBV in HCV & HIV RIBAVIC Study: Design N = 412; 48% genotype 1, CD4 >200 cells/mm 3 PegIFN alfa-2b 1.5 µg 1x/week + Ribavirin 800 mg/day vs IFN alfa-2b: 3 million IU 3x/week + Ribavirin 800 mg/day for 48 weeks Peginterferon + Ribavirin Interferon + Ribavirin RIBAVIC Study: SVR24 by Treatment Regimen and Genotype All Genotype 1 or 4 Genotype 2 or 3 or 5 Carrat F, et. al. JAMA. 2004;292:

20 SVR with PegIFN/RBV by Genotype: Coinfection vs Monoinfection *SVR rates for GT1 or GT4 unaffected by baseline viral titer. PegIFN/RBV for 48 weeks using 1000 mg or 1200 mg dose of pegifn resulted in higher rates of SVR compared with 24 weeks of therapy and/or 800 mg dose of pegifn. SVR Range, % PegIFN/RBV ( mg) HIV/HCV Coinfection HCV Monoinfection GT1 or GT4 GT2 or GT3 GT1 or GT4 GT2 or GT * Carrat F, et al. JAMA. 2004;292: Laguno M, et al. Hepatology. 2009;49: Chung RT, et al. N Engl J Med. 2004;351: Torriani FJ, et al. N Engl J Med. 2004;351: Núñez M, et al. AIDS Res Hum Retroviruses. 2007;23: Peginterferon alfa 2a [package insert].
21 PegIFN/RBV therapy in HIV/HCV-coinfected patients 2013 European treatment guidelines Wk 4 Wk 12 Wk 24 Wk 48 Wk 72 HCV RNA negative HCV RNA positive GT2/3 GT1/4** > 2 log drop in HCV RNA < 2 log drop in HCV RNA EACS Guidelines, Version 7.0. October 2013 Stop 24-wk therapy* HCV RNA negative HCV RNA positive GT2/3 GT1/4 Stop 48-wk therapy 72-wk therapy *In patients with baseline low viral load and minimal liver fibrosis. **Where no access to DAA available or high chances of cure even with dual therapy (favorable IL28B genotype, low HCV viral load, and no advanced fibrosis).
22 Drugs treatment for HCV/HIV-coinfection Older Medications Pegylated Interferon PegIntron or Pegasys Ribavirin Older Direct Acting Antivirals Boceprevir (Victrelis) (2011) Telaprevir (Incivek) (2011) New Direct Acting Antivirals Olysio (simeprevir) in November 2013 Sovaldi (sofosbuvir) in December 2013 Harvoni (ledipasvir and sofosbuvir) in October 2014 Viekira Pak (ombitasvir, paritaprevir and ritonavir tablets co-packaged with dasabuvir ) in December 2014
23 SVR (%) Telaprevir + PegIFN/RBV in GT1 HCV/HIV Coinfection Phase II randomized controlled trial Telaprevir TID + pegifn/rbv vs pegifn/rbv alone for 48 weeks HCV treatment-naive HIV+ patients with CD4 > 500 cells/mm 3 (N = 60) No HIV breakthrough Safety and tolerability Increased pruritus, headache, nausea, rash, and dizziness with telaprevir-based therapy Anemia: 18% in both groups SVR comparable to GT1 HCVmonoinfected patients (75%) Sulkowski MS, et al. Ann Intern Med. 2013;159: Jacobson IM, et al. N Engl J Med. 2011;364: n/n = / 7 11/ 16 12/ / 38 Telaprevir + PegIFN/RBV No ART EFV/TDF/FTC ATV/ritonavir + TDF/FTC Total 33 2/ / 8 4/ / 22 PegIFN/RBV
24 SVR (%) Boceprevir + PegIFN/RBV in GT1 HCV/HIV Coinfection Phase II randomized controlled trial 100 PegIFN/RBV lead-in 4 weeks then boceprevir + pegifn/rbv for 44 weeks vs pegifn/rbv alone for weeks 63 HCV treatment-naive HIV+ patients (N = 98) 60 All with HIV-1 RNA < 50 cells/ml on antiretroviral therapy 40 No difference in HIV breakthrough Safety and tolerability 29 Increased anemia, pyrexia, and 20 decreased appetite SVR comparable to GT1 HCVmonoinfected n/n = 40/64 10/34 patients (68%) 0 Boceprevir + PegIFN/RBV PegIFN/RBV Sulkowski M, et al. Lancet Infect Dis. 2013;13: Poordad F, et al. N Engl J Med. 2011;364:
25 Recommendations for coadministration of TVR and BOC in HCV/HIV-coinfection with select antiretroviral agents Antiretroviral Agent Telaprevir Boceprevir Europe US Europe US Atazanavir / ritonavir Monitor for hyperbilirubinemia Standard dose Case-by-case consideration Do not use Darunavir / ritonavir; fosamprenavir / ritonavir; lopinavir /ritonavir Not recommended Not recommended Not recommended Not recommended Raltegravir No dose adjustment No dose adjustment No dose adjustment No dose adjustment Efavirenz Increase dose (1125 mg q8h) Increase dose (1125 mg q8h) Not recommended Do not use Rilpivirine No dose adjustment No guidance No dose adjustment No dose adjustment Note: Telaprevir and boceprevir interact with CYP3A4/5 and p-glycoprotein.
26 Why is HCV therapy deferred in many HIV/HCV- coinfected patients? Dual therapy with interferon- and/or ribavirin-based regimen Lower rates of efficacy High incidence of adverse effects, and Limited access to therapy. Challenges anticipated approval of new agents Greater efficacy All-oral regimens Shorter duration Improved tolerability Fewer drug-drug interactions
27 New drugs treatment for HCV/HIV-coinfection Older Medications Pegylated Interferon PegIntron or Pegasys Ribavirin Older Direct Acting Antivirals Boceprevir (Victrelis) (2011) Telaprevir (Incivek) (2011) New Direct Acting Antivirals Olysio (simeprevir) in November 2013 Sovaldi (sofosbuvir) in December 2013 Harvoni (ledipasvir and sofosbuvir) in October 2014 Viekira Pak (ombitasvir, paritaprevir and ritonavir tablets co-packaged with dasabuvir ) in December 2014
 Excluded: boosted PIs, NNRTIs other")
28 C212 Study: Simeprevir + PegIFN/RBV in GT1 HCV/HIV Coinfection N= 106 HCV/HIV coinfected patients, 39 sites in 7 countries Baseline median CD4 = 629 cells/mm3, 88% on ART (VL < 50 cells/ml) Excluded: boosted PIs, NNRTIs other than RPV


29 C212 Study: Simeprevir + PegIFN/RBV in GT1 HCV/HIV Coinfection

30 C212 Study: Simeprevir + PegIFN/RBV in GT1 HCV/HIV Coinfection


31 Simeprevir: Drug Interactions with HIV Medications

32 Simeprevir: Drug Interactions
33 SVR12 (%) SVR12 (%) Sofosbuvir + PegIFN/RBV for 12 Wks in Treatment-Naive GT1 HCV Monoinfection and HCV/HIV Coinfection NEUTRINO: N=327 Single-arm study in HCV Monoinfection: SVR12 [1] Single-Arm Study in HCV/HIV Coinfection: SVR12 [2] n/n = 0 295/327 Overall 261/292 GT /19 13/15 4/4 GT1 GT1a GT1b 1. Lawitz E, et al. N Engl J Med. 2013;368: Rodriguez-Torres M, et al. ID Week Abstract 714.
 Cirrhosis at baseline: GT1, 4%; GT2/3 tx naive, 10%; GT2/3")
34 PHOTON-1: Sofosbuvir + RBV in HCV/HIV Coinfection N = 223, SOF + RBV for 12-wk (GT2/3 naive) or 24-week (GT1 t-naive, GT2/3 treatment experienced Stable ART (HIV-1 RNA < 50 copies/ml for > 8 wks before enrollment) Cirrhosis at baseline: GT1, 4%; GT2/3 tx naive, 10%; GT2/3 tx-exp d: 24%

35 PHOTON-1: Sofosbuvir + RBV in HCV/HIV Coinfection
; GT4 (n=31), 20% Compensated cirrhosis On ART with HIV RNA 50 copies/ml and CD4 >200 cell/mm 3 or not on ART if CD4 > 500 cell/mm")
36 Sofosbuvir plus Ribavirin for HCV-HIV Coinfection PHOTON-2 Trial: Treatment Arms N = 274 HCV-HIV coinfected patients; GT1 (n=112); GT2 (n=25); GT3 (n=106); GT4 (n=31), 20% Compensated cirrhosis On ART with HIV RNA 50 copies/ml and CD4 >200 cell/mm 3 or not on ART if CD4 > 500 cell/mm 3

37 Sofosbuvir plus Ribavirin for HCV-HIV Coinfection PHOTON-2 Trial: Treatment Arms

38 Sofosbuvir plus Ribavirin for HCV-HIV Coinfection PHOTON-2 Trial: Treatment Arms
39 Current Medications for HCV/HIV Older Medications Pegylated Interferon PegIntron or Pegasys Ribavirin Older Direct Acting Antivirals Boceprevir (Victrelis) (2011) Telaprevir (Incivek) (2011) New Direct Acting Antivirals Olysio (simeprevir) in November 2013 Sovaldi (sofosbuvir) in December 2013 Harvoni (ledipasvir and sofosbuvir) in October 2014 Viekira Pak (ombitasvir, paritaprevir and ritonavir tablets co-packaged with dasabuvir) in December 2014

40 New DAAs in HIV/HCV Coinfection ERADICATE trial: Harvoni (ledipasvir and sofosbuvir) in HIV/HCV coinfection TURQUOISE I: Paritaprevir/RTV/Ombitasvir + Dasabuvir + RBV in HIV/HCV coinfectiongt1 Ledipasvir Sofosbuvir Harvoni
 Oshinusi A,JAMA: 15 Feb")
41 Sofosbuvir-Ledipasvir in GT1 with HCV/HIV Coinfection NIAID ERADICATE Trial N = 50, Fibrosis stage 0-3 (patients with cirrhosis excluded) Oshinusi A,JAMA: 15 Feb 2015
 Common AE: nasal congestion 16%, myalgia 14%) Oshinusi A,JAMA: 15 Feb")
42 Sofosbuvir-Ledipasvir in GT1 with HCV/HIV Coinfection NIAID ERADICATE Trial: Results SVR 12: over all 98% 1 relapse in TE (resistance to LDV) Common AE: nasal congestion 16%, myalgia 14%) Oshinusi A,JAMA: 15 Feb 2015

43 Sofosbuvir-Ledipasvir Fix-Dose Combination +/- RBV ION-1, ION-2, and ION-3


44 Assumptions: 1) Production of new virions = ~10 12 /day 2) HCV genome length = ~9600 nucleotides 3) Error rate = ~10-5 /per nucleotide copied Therefore, average number of changes/genome = 0.096/replication cycle # of Nucleotide Changes How many DAAs do we need in HCV/HIV-coinfected patients? Probability # of Virions/Day x # of All Possible Mutants If the theory is right: should need 3 DAAs % of All Possible Mutants/Day x x x x x x x 10-5 Rong L, et al. Sci Transl Med. 2011;2:30-32.


45 New DAAs in HIV/HCV Coinfection Viekira pak Ombitasvir Paritaprevir Ritonavir booster for paritaprevir Dasabuvir TURQUOISE I: Ombitasvir / Paritaprevir / Ritonavir + Dasabuvir + RBV in HIV/HCV coinfection GT1

46 TURQUOISE I: Ombitasvir / Paritaprevir / Ritonavir + Dasabuvir + RBV in HIV/HCV Coinfection GT1 Phase II/III, RCT multicenter, 3D + RBV in naïve or previously treated with PEG + RBV, include cirrhosis Child A for 12 and 24 weeks; HCV-RNA >10,000 IU/ml. CD4 >200 cell/mm 3, HIV RNA < 40 copies/ml, receiving atarzanavir or raltegravir based regimen Sulkowski MS, JAMA : Feb23, 2015
, insomnia (19%), nausea (16%), headache (18%) Sulkowski MS, JAMA :")
47 TURQUOISE I: Ombitasvir / Paritaprevir / Ritonavir + Dasabuvir + RBV in HIV/HCV Coinfection GT1 N=63 SVR 12: 12 wk vs 24 wk 94% vs 92% 2 virological relapse or breakthrough 2 HCV reinfection Common AE: fatiuqe (48%), insomnia (19%), nausea (16%), headache (18%) Sulkowski MS, JAMA : Feb23, 2015

48 AbbVie Regimen Phase 3 Clinical Development Program
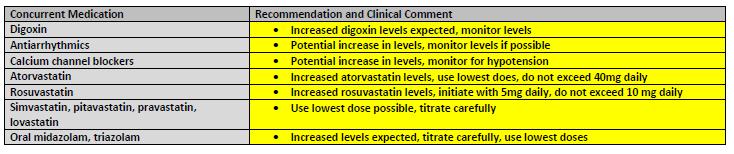
49 Drug Drug Interactions and Dose Recommendations Ombitasvir / Paritaprevir / Ritonavir + Dasabuvir Class Drug Recommendation During Coadministration Antiarrhythmics Antiarrhythmics Caution warranted during coadministration; therapeutic monitoring recommended Antifungals Ketoconazole Do not exceed daily ketoconazole 200 mg/day Voriconazole Coadministration not recommended unless justified by benefit risk ratio Calcium channel blockers Amlodipine Consider amlodipine dose reduction Corticosteroids Fluticasone Consider alternative corticosteroids Diuretics Furosemide Clinical monitoring and individualized therapy recommended HIV antivirals Atazanavir/RTV Administer atazanavir (without RTV) only in the morning HMG CoA reductase inhibitors Darunavir/RTV, Lopinavir/RTV Rilpivirine Rosuvastatin Pravastatin Coadministration not recommended Coadministration not recommended Rosuvastatin dose should not exceed 10 mg/day Pravastatin dose should not exceed 40 mg/day Ombitasvir/paritaprevir/ritonavir and dasabuvir [package insert].
50 Drug Drug Interactions and Dose Recommendations Ombitasvir / Paritaprevir / Ritonavir + Dasabuvir Class Drug Recommendation During Coadministration Immunosuppressants Cyclosporine Reduce cyclosporine dose to 1/5th of current dose, monitor Long-acting betaadrenoceptor agonists Narcotic analgesics Tacrolimus Salmeterol Buprenorphine/ naloxone Dose adjustment required; see prescribing information Coadministration not recommended No dose adjustment needed; closely monitor for sedation and cognitive effects PPIs Omeprazole Monitor for decreased omeprazole efficacy; increase if needed, not to exceed 40 mg/day omeprazole Sedative/hypnotics Alprazolam Clinical monitoring recommended; decrease dose as needed No dose adjustments needed with coadministration of the following with OMV/PTV/RTV + DSV: Digoxin, duloxetine, tenofovir DF/emtricitabine, escitalopram, methadone, progestin only contraceptives, raltegravir, warfarin, zolpidem Ombitasvir/paritaprevir/ritonavir and dasabuvir [package insert].
51 Contraindications and Selected Precautions: Ombitasvir / Paritaprevir / Ritonavir + Dasabuvir + RBV Not recommended for decompensated cirrhosis CTP-B: not recommended CTP-C: contraindicated Creatinine clearance CrCl > 30 ml/min, no dosage adjustment needed CrCl < 30 ml/min, consult with expert, limited safety and efficacy data available Contraindicated with drugs dependent on CYP3A for clearance, strong CYP3A and CYP2C8 inducers, strong CYP2C8 inhibitors Ribavirin contraindications and warnings/precautions apply Avoid if known hypersensitivity to ritonavir HCV/HIV coinfection: risk of HIV PI resistance Coinfected patients should be receiving suppressive ART AASLD/IDSA HCV Guidelines Ombitasvir/paritaprevir/ritonavir and dasabuvir [package insert].
52 Precautions: ALT Elevations ALT elevations of > 5 x ULN seen in ~ 1% of patients in clinical trials More common in women receiving ethinyl estradiol containing treatment Typically asymptomatic, in first 4 wks of therapy, declined in 2-8 wks with continued dosing of OMV/PTV/RTV + DSV Discontinue ethinyl estradiol prior to use of OMV/PTV/RTV + DSV May resume 2 wks after stopping OMV/PTV/RTV + DSV Coadminister with caution in patients receiving other estrogens Monitor hepatic labs at baseline, in first 4 wks, and after as needed Repeat and monitor if ALT elevated above baseline levels Consider discontinuation if ALT persistently > 10 x ULN; discontinue if ALT elevation accompanied by liver inflammation or increasing conjugated bilirubin, alkaline phosphatase, or INR Ombitasvir/paritaprevir/ritonavir and dasabuvir [package insert].
53 Optimal Management of HCV-HIV Coinfection Same recommendations as in HCV-monoinfected patients Treatment monitoring Monitoring of treatment efficacy Stopping (futility) rules Virological response-guided triple therapy Monitoring treatment safety Consider drug drug interactions Antiretroviral drug switches, when needed, should be done in collaboration with the HIV practitioner
54 2014 EASL Recommendations on Treatment of Hepatitis C Genotype 1,4 Sofosbuvir 400 mg/d + PEG + RBV x 12 wks Simeprevir 150 mg/d x 12 wks + PEG + RBV x 24 wks* (Q80K neg) Daclatasvir 60 mg/d +PEG + RBV + x weeks** (G 1b) IFN ineligible Sofosbuvir 400 mg/d + RBV x 24 weeks or Simeprevir 150 mg/d + Sofosbuvir 400 mg/d ± RBV x 12 wks Sofosbuvir 400 mg/d+ daclatasvir 60 mg/d x 12 weeks (naïve) or 24 weeks (TE**, failed PEG + RBV and either telaprevir or boceprevir) 2 Sofosbuvir 400 mg + RBV X weeks 3 Ribavirin and sofosbuvir 400 mg/d x 12 week or weeks (in cirrhosis, especiallyte) Sofosbuvir 400 mg/d and daclatasvir 60 mg/d 12 wks (naïve) or 24 wks (TE) Sofosbuvir 400 mg/d + PEG + RBV x 12 wks 5,6 Sofosbuvir 400 mg/d + PEG + RBV x 12 wks IFN ineligible Sofosbuvir 400 mg/d + RBV x 24 weeks April AASLD same recommndations, except no Daclatasvir-containing regimen *Treatment should be stopped if HCV RNA level is 25 IU/ml at treatment week 4, week 12 or week 24 **If HCV RNA level <25 IU/ml at week 4 and undetectable at week 10, PEG + RBV + daclatasvir 60 mg/d x 12 weeks then PEG + RBV x 12 weeks (total 24 weeks) TE; treatment experienced; weight-based ribavirin (1000 or 1200 mg/d in patients <75 kg or 75 kg, respectively
55 EASL 2014: Treatment monitoring Triple therapy: Stopping rules PegIFN-α, ribavirin and simeprevir Stop treatment if HCV RNA level is 25 IU/ml at treatment week 4, week 12 or week 24 (Recommendation A2) Virological response-guided therapy: pegifn-α, ribavirin and daclatasvir 0 4wk 10 wk 12 wk 24 wk HCV RNA <25 IU/ml undetectable Peg/RBV/daclatasvir Peg/R HCV RNA >25 IU/ml undetectable Peg/RBV/daclatasvir
56 2014 AASLD/IDSA/IAS-USA: HCV Treatment Guideline December 19, 2014 Revised for HCV/HIV Date: January 26, 2015 Population Regimen Duration GT 1a (3 options) GT 1b (3 options) SOF/LDV OMV/PTV/RTV-dasabuvir + RBV SOF + SMV SOF/LDV OMV/PTV/RTV-dasabuvir (naïve), add RBV (cirrhosis) SOF + SMV 12 wks 12 wks (naïve), 24 wks (cirrhosis) 12 wks (naïve), 24 wks(cirrhosis) 12 wks 12 wks 12 wks (naïve), 24 wks(cirrhosis) GT2 SOF + RBV 12 wks GT3 GT 4 (3 options) GT 5 GT 6 SOF + RBV pegifn/r/sof(alternative regimen) SOF/LDV OMV/PTV/RTV + RBV SOF + RBV pegifn/r/sof pegifn/r (alternative regimen) SOF/LDV pegifn/r/sof(alternative regimen) 24 wks 12 wks 12 wks 12 wks 24 wks 12 wks 48 wks 12 wks 12 wks American Association for the Study of Liver Diseases (AASLD), Infectious Diseases Society of America (IDSA), International Antiviral Society USA (IAS USA) SOF, sofosbuvir; RBV, ribavirin; LDV, ledipasvir; PTV, paritaprevir; RTV, ritonavir; OMV, ombitasvir; DSV, dasabuvir

57 AASLD 2014: Recommended monitoring during antiviral therapy. Recommendations for discontinuation of treatment because of lack of efficacy ALT Recommendations for discontinuation of treatment because of safety > 10 x ULN < 10 x ULN + symptomatic* Stop Rx < 10 x ULN + asymptomatic Closely monitor Repeat ALT at week 6 and week 8. *weakness, nausea, vomiting, or jaundice, or increased bilirubin, ALP, or INR
58 Monitoring treatment safety Patients receiving Peg IFN-α and ribavirin should be assessed for clinical side effects at each visit, while haematological side effects should be assessed at weeks 2 and 4 of therapy and at 4 to 8 week intervals thereafter Recommendation A1 Headache and fatigue have been reported with sofosbuvir Renal function should be checked regularly in patients receiving sofosbuvir Recommendation B1 Rashes and bilirubin elevations may be seen with simeprevir Recommendation A1 Eefficacy and toxicity of concurrent drugs given for comorbidities and potential drug-drug interactions should be monitored during treatment Recommendation A1 AASLD/IDSA HCV Guidelines 2015.

59 Antiretroviral Treatment Options for Patients on DAAs for Hepatitis C PI;Protease Inhibitors January 22, 2015

60 Antiretroviral Treatment Options for Patients on DAAs for Hepatitis C NNRTIs; nonnucleoside Reverse Transcriptase Inhibitors January 22, 2015

61 Antiretroviral Treatment Options for Patients on DAAs for Hepatitis C InSTIs;Integrase Strand Transfer Inhibitors, NRTIs; Nucleoside Reverse Transcriptase Inhibitors January 22, 2015
62 Summary Optimal Management of HCV-HIV Coinfection
63 Summary: Optimal Management of HCV/HIV Coinfection 2015 Same recommendations as in HCV-monoinfected patients (treatment naïve and - experienced patients), after recognizing and managing interactions with ARV. FDA-approved first-line pegifn-free regimens for GT 1, 2, 3, 4 PegIFN/RBV/SOF 12 weeks for GT5 and alternative treatment for GT3,6 PegIFN/RBV 48 weeks: alternative treatment for GT 5 The following regimens are NOT recommended for naive or -experienced PEG-IFN and RBV +/- telaprevir, boceprevir, or simeprevir, Monotherapy with PEG-IFN, RBV, or DAA Do not interrupt ARV Antiretroviral drug switches, when needed, should be done in collaboration with the HIV practitioner
64 Summary: Optimal Management of HCV/HIV Coinfection Consider drug drug interactions RBV should NOT be used with didanosine, stavudine, or zidovudine Simeprevir should NOT be used with EFV, ETR, NVP, cobicistat, or any HIV PI. LDV / SOF should NOT be used with cobicistat, EVG, tipranavir Potential for LDV-mediated increase TDF levels, especially if TDF used with RTV Avoid LDV if CrCl < 60 ml/min or if receiving TDF with RTV-boosted PI OMV/PTV/RTV + DSV; Need to adjust or withhold RTV if receiving a boosted PI Should NOT used with EFV, RPV, DRV, or RTV-boosted lopinavir. ETR; etravirine, NVP; nevirapine, EVG elvitegravir

65 Thank you
Antiviral treatment in Unique Populations
 Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
My HCV patient is co-infected with HIV: how to manage?
 EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
HIV and Hepatitis C: Advances in Treatment
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
Considerations for the management of Hepatitis C in patients with HIV co-infection
 Considerations for the management of Hepatitis C in patients with HIV co-infection Marcella Honkonen, PharmD, BCPS Sunday, February 22, 2012 at 10:15 AM AzPA Southwest Clinical Conference JW Marriott,
Considerations for the management of Hepatitis C in patients with HIV co-infection Marcella Honkonen, PharmD, BCPS Sunday, February 22, 2012 at 10:15 AM AzPA Southwest Clinical Conference JW Marriott,
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
Treatment of chronic hepatitis C in HIV co-infected patients
 Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Clinical Criteria for Hepatitis C (HCV) Therapy
 Therapy") Diagnosis Clinical Criteria for Hepatitis C (HCV) Therapy Must have chronic hepatitis C (HCV infection > 6 months), genotype and sub-genotype specified to determine the length of therapy; Liver biopsy
Diagnosis Clinical Criteria for Hepatitis C (HCV) Therapy Must have chronic hepatitis C (HCV infection > 6 months), genotype and sub-genotype specified to determine the length of therapy; Liver biopsy
HIV-HCV coinfection. Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland
 HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
Ombitasvir-Paritaprevir-Ritonavir + Dasabuvir (Viekira Pak)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ombitasvir-Paritaprevir-Ritonavir + Dasabuvir (Viekira Pak) Prepared by: Sophie Woolston, MD and David H. Spach, MD Last Updated: December 29, 2014 OMBITASVIR-PARITAPREVIR-RITONAVIR
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ombitasvir-Paritaprevir-Ritonavir + Dasabuvir (Viekira Pak) Prepared by: Sophie Woolston, MD and David H. Spach, MD Last Updated: December 29, 2014 OMBITASVIR-PARITAPREVIR-RITONAVIR
Hepatitis C Medications Prior Authorization Criteria
 Hepatitis C Medications Authorization Criteria Epclusa (/velpatasvir), Harvoni (ledipasvir/), Sovaldi (), Daklinza (daclatasvir), Zepatier (elbasvir/grazoprevir), Olysio (simeprevir), Viekira Pak (ombitasvir/paritaprevir/ritonavir;
Hepatitis C Medications Authorization Criteria Epclusa (/velpatasvir), Harvoni (ledipasvir/), Sovaldi (), Daklinza (daclatasvir), Zepatier (elbasvir/grazoprevir), Olysio (simeprevir), Viekira Pak (ombitasvir/paritaprevir/ritonavir;
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity. Patrick Ingiliz, Berlin
 Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity Patrick Ingiliz, Berlin Back in the days when HCV genotype 1 was the problem SVR (%) 100 90 80 70 60 50 40 30 20 10 0 35% PRESCO
Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity Patrick Ingiliz, Berlin Back in the days when HCV genotype 1 was the problem SVR (%) 100 90 80 70 60 50 40 30 20 10 0 35% PRESCO
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
HCV/HIV Coinfection ANTON AND MARGARET FUISZ CHAIR IN MEDICINE. HIV and HCV Share Risk Factors PREVALENCE OF CO-INFECTION BY RISK FACTOR 60%
 HCV/HIV Coinfection BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY HIV and HCV Share Risk Factors PREVALENCE
HCV/HIV Coinfection BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY HIV and HCV Share Risk Factors PREVALENCE
6/2/2015. Interactive Case-Based Presentations and Audience Discussion
 6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Case #1. Case #1. Case #1: Audience vote VS. The Great Debate: When to Treat HCV in our HIV coinfected patients
 Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World
 Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir) PHARMACY PRI AUTHIZATION Hepatitis C Clinical Guideline Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir) Harvoni
Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir) PHARMACY PRI AUTHIZATION Hepatitis C Clinical Guideline Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir) Harvoni
CENTENE PHARMACY AND THERAPEUTICS DRUG REVIEW 3Q17 July August
 BRAND NAME Technivie GENERIC NAME Ombitasvir/paritaprevir/ritonavir MANUFACTURER AbbVie, Inc. DATE OF APPROVAL February 27, 2017 PRODUCT LAUNCH DATE Already available on the market REVIEW TYPE Review type
BRAND NAME Technivie GENERIC NAME Ombitasvir/paritaprevir/ritonavir MANUFACTURER AbbVie, Inc. DATE OF APPROVAL February 27, 2017 PRODUCT LAUNCH DATE Already available on the market REVIEW TYPE Review type
Dr Janice Main Imperial College Healthcare NHS Trust, London
 BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Clinical Cases Hepatitis C Naïve Patients. Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona.
 Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
ICVH 2016 Oral Presentation: 28
 Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Pegylated Interferon Agents for Hepatitis C
 Applicable X X X X X X X Pegylated Interferon Agents for Hepatitis C Override(s) Prior Authorization Quantity Limit Initial for Monotherapy or Combination with Ribavirin based on Genotype, Status, or Co-Infection
Applicable X X X X X X X Pegylated Interferon Agents for Hepatitis C Override(s) Prior Authorization Quantity Limit Initial for Monotherapy or Combination with Ribavirin based on Genotype, Status, or Co-Infection
HIV-HCV Co-Infection. George Mason University Falls Church, Virginia. Overview. Prevalence of HCV co-infection Incidence and Recent Trends
 HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova
HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova
JOHNS HOPKINS HEALTHCARE
 JOHNS HOPKINS HEALTHCARE Subject: Clinical Criteria for Hepatitis C (HCV) Therapy Department: Pharmacy Lines of Business: PPMCO Policy Number: MEDS92 Effective Date: 04/15/2015 Revision Date: 08/15/2015
JOHNS HOPKINS HEALTHCARE Subject: Clinical Criteria for Hepatitis C (HCV) Therapy Department: Pharmacy Lines of Business: PPMCO Policy Number: MEDS92 Effective Date: 04/15/2015 Revision Date: 08/15/2015
HIV-HCV Co-Infection in Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School
 HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
HEPATITIS C. Mitchell L. Shiffman, MD, FACG Director. Liver Institute of Virginia. Richmond and Newport News, VA
 NEW TREATMENTS FOR HEPATITIS C Mitchell L. Shiffman, MD, FACG Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA Liver Institute of Virginia Education, Research
NEW TREATMENTS FOR HEPATITIS C Mitchell L. Shiffman, MD, FACG Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA Liver Institute of Virginia Education, Research
Treatment of Patients with HCV and HIV
 Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy
 Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Direct Acting Antivirals for the Treatment of Hepatitis C Infection
 Hepatitis C Core Curriculum, Module 2 Direct Acting Antivirals for the Treatment of Hepatitis C Infection Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Objectives Discuss the evolution of hepatitis C treatment
Hepatitis C Core Curriculum, Module 2 Direct Acting Antivirals for the Treatment of Hepatitis C Infection Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Objectives Discuss the evolution of hepatitis C treatment
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis B / Hepatitis C Peg-interferon Page 1 of 20 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis B / Hepatitis C Peg-interferon Hepatitis
Hepatitis B / Hepatitis C Peg-interferon Page 1 of 20 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis B / Hepatitis C Peg-interferon Hepatitis
Topic: Sovaldi, sofosbuvir Date of Origin: March 14, Committee Approval Date: August 15, 2014 Next Review Date: March 2015
 Medication Policy Manual Policy No: dru332 Topic: Sovaldi, sofosbuvir Date of Origin: March 14, 2014 Committee Approval Date: August 15, 2014 Next Review Date: March 2015 Effective Date: October 1, 2014
Medication Policy Manual Policy No: dru332 Topic: Sovaldi, sofosbuvir Date of Origin: March 14, 2014 Committee Approval Date: August 15, 2014 Next Review Date: March 2015 Effective Date: October 1, 2014
Global Prevalence of HBV, HCV, HIV
 Treatment of Patients with HCV and HIV Paul Y. Kwo, MD, FACG Professor of Medicine Stanford University email: pkwo@stanford.edu Global Prevalence of HBV, HCV, HIV 24 m Journal of Clinical Virology Page
Treatment of Patients with HCV and HIV Paul Y. Kwo, MD, FACG Professor of Medicine Stanford University email: pkwo@stanford.edu Global Prevalence of HBV, HCV, HIV 24 m Journal of Clinical Virology Page
British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2
 British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2 Systematic literature search 2.1 Questions and PICO criteria Data bases: Medline,
British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2 Systematic literature search 2.1 Questions and PICO criteria Data bases: Medline,
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Feeling right at home
 Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
HEPATITIS WEB STUDY. Treatment of Hepatitis C following Liver Transplantation
 HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
Treatment of Hepatitis C with sofosbuvir/ledipasvir (Harvoni )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University
 Bruce A. Luxon, MD, PhD, FACG Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University Dr. Luxon is on the speakers p bureau
Bruce A. Luxon, MD, PhD, FACG Bruce A. Luxon, MD, Ph.D. Anton and Margaret Fuisz Chair in Medicine Professor and Chair Department of Medicine Georgetown University Dr. Luxon is on the speakers p bureau
HCV Treatment in 2016: Genotypes 1, 2, and 3. Cody A. Chastain, MD October 12, 2016
 HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
Learning Objective. After completing this educational activity, participants should be able to:
 Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
Zepatier. (elbasvir, grazoprevir) New Product Slideshow
 New Product Slideshow") Zepatier (elbasvir, grazoprevir) New Product Slideshow Introduction Brand name: Zepatier Generic name: Elbasvir, grazoprevir Pharmacological class: HCV NS5A inhibitor + HCV NS3/4A protease inhibitor Strength
Zepatier (elbasvir, grazoprevir) New Product Slideshow Introduction Brand name: Zepatier Generic name: Elbasvir, grazoprevir Pharmacological class: HCV NS5A inhibitor + HCV NS3/4A protease inhibitor Strength
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Outpatient Pharmacy Effective Date: August 15, 2014
 Therapeutic Class Code: W5Y, W5V, W0B, W0D, W0A, W0E Therapeutic Class Description: Hepatitis C Virus nucleotide analog NS5B RNA Dependent Polymerase Inhibitor, Hepatitis C Virus NS3/4A Serine Protease
Therapeutic Class Code: W5Y, W5V, W0B, W0D, W0A, W0E Therapeutic Class Description: Hepatitis C Virus nucleotide analog NS5B RNA Dependent Polymerase Inhibitor, Hepatitis C Virus NS3/4A Serine Protease
Pharmacological management of viruses in obese patients
 Cubist Pharmaceuticals The Shape of Cures to Come Pharmacological management of viruses in obese patients Dr. Dimitar Tonev, Medical Director UKINORD 1 Disclosures } The author is a pharmaceutical physician
Cubist Pharmaceuticals The Shape of Cures to Come Pharmacological management of viruses in obese patients Dr. Dimitar Tonev, Medical Director UKINORD 1 Disclosures } The author is a pharmaceutical physician
Hepatitis C: The New World of Treatment
 Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Hepatitis C Virus: HIV/Hepatitis C Coinfection Wednesday, August 24, 2016
 Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Simeprevir + PEG + RBV in Treatment-Naïve Genotype 1 QUEST-1 Trial
 Phase 3 Treatment Naïve Simeprevir + in Treatment-Naïve Genotype 1 QUEST-1 Trial Jacobson IM, et al. Lancet. 2014;384:403-13. Simeprevir + PEG + Ribavirin for Treatment-Naïve HCV GT1 QUEST-1 Trial QUEST-1
Phase 3 Treatment Naïve Simeprevir + in Treatment-Naïve Genotype 1 QUEST-1 Trial Jacobson IM, et al. Lancet. 2014;384:403-13. Simeprevir + PEG + Ribavirin for Treatment-Naïve HCV GT1 QUEST-1 Trial QUEST-1
Hepatitis C Virus Clinical Criteria Update September 18, For: New York State Medicaid
 Hepatitis C Virus Clinical Criteria Update September 18, 2014 For: New York State Medicaid 1 Purpose Characterize the place in therapy for the agents utilized for management of chronic hepatitis C (CHC)
Hepatitis C Virus Clinical Criteria Update September 18, 2014 For: New York State Medicaid 1 Purpose Characterize the place in therapy for the agents utilized for management of chronic hepatitis C (CHC)
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Viral hepatitis in patients living with HIV: can we still speak of special population?
 Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients?
 Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients? Ira M. Jacobson, MD Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology
Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients? Ira M. Jacobson, MD Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology
HIV Infection with HCV Future Directions
 HIV Infection with HCV Future Directions Dr Ranjababu (Babu) Kulasegaram Consultant Physician in HIV/GU Medicine Guy s and St Thomas NHS Foundation Trust London, UK Presenter disclosure information Dr
HIV Infection with HCV Future Directions Dr Ranjababu (Babu) Kulasegaram Consultant Physician in HIV/GU Medicine Guy s and St Thomas NHS Foundation Trust London, UK Presenter disclosure information Dr
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
PEARL-I. Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4. Treatment Naïve and Treatment Experienced
 Phase 2b Treatment Naïve and Treatment Experienced Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4 PEARL-I Hézode C, et al. Lancet. 2015 March 30. [Epub ahead of print] PEARL-I: Study Design
Phase 2b Treatment Naïve and Treatment Experienced Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4 PEARL-I Hézode C, et al. Lancet. 2015 March 30. [Epub ahead of print] PEARL-I: Study Design
Treatment of Hepatitis C in HIV-Coinfected Patients. Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain
 Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Harvoni) Reference Number: CP.CPA.175 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Harvoni) Reference Number: CP.CPA.175 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Current State of Treatment for HCV. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 Activity Code FA376 Current State of Treatment for HCV Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives Upon completion of this presentation, learners should be
Activity Code FA376 Current State of Treatment for HCV Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives Upon completion of this presentation, learners should be
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Section 6: Treatment of Hepatitis C virus (HCV)
") Section 6: Treatment of Hepatitis C virus (HCV) Dr. Niklas Luhmann (Médecins du Monde) Training Hepatitis C and HR for PWUD, 9 th -13 th May 2016, Hanoi, Vietnam Learning objective of the session: understanding
Section 6: Treatment of Hepatitis C virus (HCV) Dr. Niklas Luhmann (Médecins du Monde) Training Hepatitis C and HR for PWUD, 9 th -13 th May 2016, Hanoi, Vietnam Learning objective of the session: understanding
Clinical Policy: Simeprevir (Olysio) Reference Number: CP.CPA.289 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.289 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: (Olysio) Reference Number: CP.CPA.289 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Olysio) Reference Number: CP.CPA.289 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Chronic Hepatitis C Drug Class Prior Authorization Protocol
 Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
New York State HCV Provider Webinar Series. Side Effects of Therapy
 New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
UPDATES IN HEPATITIS C
 UPDATES IN HEPATITIS C S A R A H N A I D O O, P H A R M, B C P S AP RI L 13, 2014 OBJECTIVES Be able to discuss changes in hepatitis c treatment Be able to provide recommendations to providers regarding
UPDATES IN HEPATITIS C S A R A H N A I D O O, P H A R M, B C P S AP RI L 13, 2014 OBJECTIVES Be able to discuss changes in hepatitis c treatment Be able to provide recommendations to providers regarding
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18
 Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18 Overview Hepatitis C Virus Prevalence Effects of Hepatitis C Prevention Diagnosis
Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18 Overview Hepatitis C Virus Prevalence Effects of Hepatitis C Prevention Diagnosis
Harvoni (sofosbuvir/ledipasvir
 Market DC Override(s) Prior Authorization Quantity Limit (sofosbuvir/ledipasvir) Approval Duration Based on Genotype, Treatment status, Baseline HCV RNA status, Cirrhosis status, Transplant status, or
Market DC Override(s) Prior Authorization Quantity Limit (sofosbuvir/ledipasvir) Approval Duration Based on Genotype, Treatment status, Baseline HCV RNA status, Cirrhosis status, Transplant status, or