Nick Bandarenko, MD Duke University Transfusion Service
|
|
|
- Coral Watkins
- 5 years ago
- Views:
Transcription
1 Nick Bandarenko, MD Duke University Transfusion Service
2 AN UNEXPECTED ADVERSE EVENT
3 Case #1 3 month old 4.3kg boy with congenital heart malformation Ventricular Septal Defect (VSD) Failure to thrive and Congestive Heart Failure Presented for surgical VSD closure CPB circuit: Standard neonatal prime: 1 unit PRBCs (AS 3 4 days old, LR), 1 unit FFP NaHCO3, heparin, solumedrol, CalGlu
4 Case #1 RBC Special Needs for Neonatal (<4 month old) Cardiac Surgery Leukocyte reduced CPDA <10 days or if not available AS 3 then AS 1 (<14 days) Irradiated
5 Case #1 Baseline Labs ABG unremarkable Co-ox: Hb 9.7 g/dl, COHb 3.3%, lactate 1.4 mmol/l Sternotomy, pericardium dissected, aortic then SVC cannulation Uneventful CPB initiation, IVC cannulation rso 2 remained around baseline Activated Clotting Time (ACT) at 7 mins
6 Case #1 Pulse-oximeter: indirectly monitors the oxygen saturation of a patient's blood (as opposed to measuring oxygen saturation directly through a blood sample) by the oxy/deoxyhemoglobin ratio calculated from the ratio of the absorption of the red and infrared light during arterial contraction Limitation: Not a complete measure of respiratory sufficiency. A patient suffering from hypoventilation (poor gas exchange in the lungs) given 100% oxygen can have excellent blood oxygen levels while still suffering from respiratory acidosis due to excessive carbon dioxide. CO-oximeter measures absorption at additional wavelengths to distinguish CO from O 2 and determines the blood oxygen saturation more reliably

 100% O 2, Hb already high, flow")
7 Case #1 CDI % SaO 2 Ignored COHb initially Cerebral Oxygenation began declining for no obvious reason 2 nd ABG confirmed COHb (11%) 100% O 2, Hb already high, flow ~ mls/kg/min, 32C
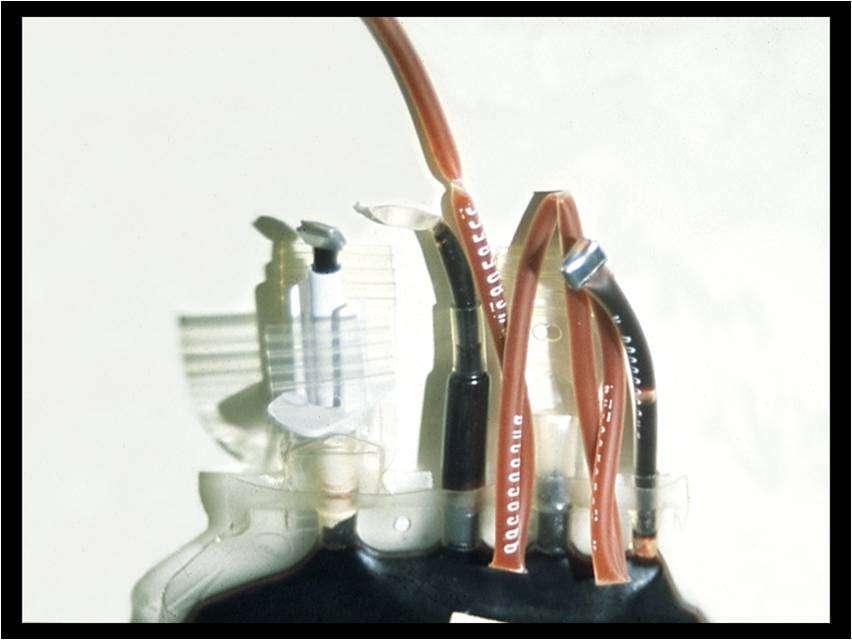
8 Case #1 Cerebral Oxygenation (Somanetics) continued to decline Ordered a new lead (wire) to monitor in case defective Considered possible sources of as source of COHb Checked head for signs of cerebral congestion Checked venous saturation (75%) Turned off forane gas as possible source Examined donor blood (very red unit of RBCs)
 Called Transfusion Service Began searching")
9 Case #1 Confirmed donor blood as source of COHb (COHb 15%!!) Called Transfusion Service Began searching literature
10 Case #1 COHb remained high during CPB VSD closed with dacron patch Performed partial exchange transfusion with a different unit of prbcs (cell saver washed) Removed 400mls and transfused 250mls

11 Case #1 Somanetics reading improved (sensor changed around this time)
12 Case #1 COHb 7.1% after partial exchange transfusion Weaned uneventfully XCL: 74 mins CPB: 135 mins Transferred to PCICU
13 Case #1 Lactate 1.4 mmol/l pre-cpb, up to 2.6 just prior to exchange tx, 1.9 immediately after exchange SVO 2 maintained ~75-80% throughout CPB run Normal SVO2 is 75%, which indicates that under normal conditions, tissues extract 25% of the oxygen delivered MAPs ~45mmHg COHb continued to decline to normal Discharged POD4
14 Lactate mmol/l / COHb % RSO2 Perfusion Parameters COHgB Lactate INVOS :38 8:44 CPB exch tx 9:33 10:18 10:46 11:02 Off cpb Time 12:10 13:20 17:30 23:
15 Carbon Monoxide (CO) Colorless, odorless, highly toxic gas Vehicle exhaust, fuel burning appliances, engine powered equipment, tobacco smoke, fire smoke, methane breakdown Leading cause of fatal poisoning in industrialized world Symptoms of poisoning resemble the flu CNS and myocardium most at risk w/ poisoning Produced naturally in the body from the breakdown of heme Multiple roles (memory, inflammation, liver, kidneys, heart) Chronic / Prolonged exposure can cause polycythemia
16 Carboxyhemoglobin (COHb) CO binds with Hb in blood to form carboxyhemoglobin (COHb) Hb affinity for CO is 240 times greater than for O 2 Decreases O 2 carrying capacity of blood and shifts OHDC to the left, leading to tissue hypoxia Fetal Hb takes up CO more readily - infants are more vulnerable to its effects Elimination: dissolved O 2 is eventually able to displace CO from Hb Half-life: 4-6 hrs on room air, 74+/-25 mins with 100% O 2
17 OHDC
18 Carboxyhemoglobinemia Elevated levels of COHb in blood known as carboxyhemoglobinemia Normal levels/high levels and effects 0-2.5% non-smokers, 0-10% smokers Overt symptoms ~20%, subtle symptoms at lower levels Serious toxicity ~ 25%, fatal ~70% Treatment: 100% O 2
19 Literature Review Blood bank studies in 80s recommended levels be reported on units Carboxyhemoglobin levels decreased as storage time increased (Uchida, 1990) Anecdotal case reports
20 9.4 kg VSD, primed w/ 150 mls PRBC COHb level of 3.7%, donor unit 7.2%, 100%O 2, remained high until following morning

21 468 units, avg COHb 0.78%, 48 units >1.5%, highest 12% Only units with levels <1.5% used for pediatric cardiac surgery



22
23 Discussion Donor: Increased Hb on first patient ABG and in donor unit may indicate prolonged CO exposure Smoker? CO leak at home or vehicle? Likes to grill in the garage?
24 Discussion The Transfusion Service contacted the Blood Donor Center Investigation of the blood donor revealed that he drove an old truck with a bad muffler The level of COHb in the donated unit suggested exposure to significant levels of CO. Prolonged CO exposure may cause polycythemia, hence the donor would likely have normal or high Hgb on pre-donation screening


25
26 Summary Can get COHb from donor blood Monitoring can be tricky/misleading CO Ox better than pulse Ox Visual Inspection of Unit- Implicated unit was noted to be bright red Consider intro-operative measurement of prbcs for COHb Specifically for neonatal cardiac surgery patients who are at greatest risk Report Discoveries that may implicate donor health to Blood Center! v


27

28 What is the name of our galaxy?
29 Visual Inspection of RBC units Is required to be performed when dispensing blood Cannot detect bacterial contamination Does not involve comparing integral segments to the tubing in continuity to the unit Can be bypassed on rare units of blood Is required by regulations but does not directly benefit patients

30

31 Obstetrical Disaster Averted
32 Case #2 KL is a 38 year old female with an past obstetrical history significant for 3 prior spontaneous abortions at 6, 10, and 12 weeks followed by a twin gestation with IUFD at 24 weeks of one twin and post partum death of the second twin shortly after term delivery Cause of fetal/neonatal death intracranial hemorrhage associated with thrombocytopenia
33 Most likely diagnosis is Inherited clotting disorder Hemolytic disease of newborn Bad luck Congenital malformation Neonatal alloimmune thrombocytopenia
34 Neonatal Alloimmune Thrombocytopenia (NAIT) Syndrome of immune destruction of platelets by maternal antibody In this case, anti-hpa-1 Analogous to HDFN which involves destruction of fetal red cells by maternal antibodies to RBC antigen Mother becomes sensitized during pregnancy to fetal platelet specific antigen inherited from father IgG specific for the platelet antigen is formed and crosses the placenta Most common cause of severe fetal/neonatal thrombocytopenia Affected infants at risk for major bleeding- ICP
35 Case #2- Previous Testing Patient- HPA-1 negative Father- HPA-1 positive (homozygous) HPA-1 is a common platelet antigen To date 23 platelet specific antigens have been described Associated with DNA polymorphisms Localized to glycoproteins on platelet surface HPA-1 (HPA-1a) is associated with GPIIIa Most frequent antigen implicated in NAIT is Pl A1 80% of cases Antigen prevalence 98%
36 NAIT Platelet antigen Percent of cases of NAIT HPA-1a 80% HPA-5b 10% HPA-1b 4% HPA-3a 2% Other 6%
37 NAIT Incidence of ICH 10-30% Half occur in utero Risk of ICH inversely proportional to platelet count Highest when plt < 100,000/uL Occasionally may have associated hydrops due to extramedullary hematopoeisis anemia without red cell incompatibility Once delivered follow platelet count which gradually increases as maternal antibody disappears over 2-3 weeks
38 Case #2 Treatment for NAIT ANTENATAL Intravenous gammaglobulin 1g/kg/week Steroids Goals- ameliorate fetal thrombocytopenia Prevent intracranial hemorrhage Cordocentesis (1-2 % mortality) Clinician must balance risk of the procedure with risk of ICH Monitoring of platelet count IUT of platelets Antigen negative CMV reduced risk Irradiated Blood supplier may have HPA-1 negative donors
39 Case #2 Patient presented to Duke at 33 weeks with premature Rupture of Membranes receiving weekly IVIG and steroids Resulted in prolonged hospitalization with planned c-section 1 month away Ultrasound normal No cordocentesis for monitoring fetal platelet count What arrangements did the Transfusion Service make with clinical team and the Blood Center?
40 Case #2 Transfusion of antigen negative platelets may be life-saving Clinical Service- To NOTIFY Transfusion Service of impending delivery Assess if more than 1 unit of platelet may be required for management of fetus Plan on immediate IV access if any signs of bleeding and to begin transfusion of plts (before plt count result) Transfusion Service- To MAINTAIN one HPA-1 negative platelet inventory at all times Leukoreduced for CMV reduced risk Irradiated to prevent GVHD Volume Reduce platelet when notified of impending delivery Rh + OK
41 Case #2 Blood Center- Coordinated HPA-1 negative donations Provided in date HPA-1 negative platelet product every 4-5 days
42 Case #2 Clinical Course of newborn platelet counts Delivery A 68 B 84 C 85 D 114 Day Day Day Day Day No anemia, no signs of bleeding bruising or petechiae No transfusion of platelets required! v
43 Up to 80% of NAIT cases are associated with which maternal antibody? Anti-HPA-3a Anti-HPA-1b Anti-HPA-1a Anti-HPA-5b Anti-HPA-4a
44 Transfusion Associated Fever
45 Case #3 LG is a 74 year old female who has been receiving chemotherapy for leukemia. The patient has been unresponsive to therapy and is transfusion dependent. She presents to clinic with a platelet count of 9 X 10 9 /L and her WBC count is 11 x 10 9 /L. Pre transfusion her vital signs are temperature C, BP - 156/70 mm Hg, and a pulse of 104. She is premedicated with benadryl and tylenol. The platelets are infused over 30 minutes Post transfusion vital signs are 37.8 C, BP 152/70 mmhg, P= 88, R= 20 There were no signs or symptoms of an adverse transfusion reaction. Thirty minutes following her transfusion, she complains of feeling cold, followed by rigors. Her temperature is 37.5 C.
46 Case #3 The patient is kept in the clinic, and at 4 hours and 40 minutes she shows signs of respiratory compromise. At 5 hours her platelet count is 47 X 10 9 /L and her WBC count is 6.6 X Her temperature is 39.5 C, blood cultures are drawn, broad spectrum antibiotics started At 6 hours following the completion of her transfusion, the patient becomes apneic while on the elevator going to the ICU, suffers a cardiopulmonary arrest and is pronounced dead. Blood cultures from the patient and the platelet bag both grew Staph. warneri.
47 Case #3 What type of transfusion reaction did she experience? Given the high fever, and the drop in WBC count, one should have suspected a septic transfusion reaction. The cultures confirmed this suspicion. How common is this type of reaction? The risk of symptomatic bacterial contamination is thought to be 1/2000
48 What additional step is critical when bacterial contamination is suspected? Quarantine other products from donation Investigate donor for risks Protect other transfusion recipients from potentially contaminated product Also, Notify FDA verbally within 24 hours and in writing within 7 days
49 A Classic Case
50 Case #4 49 year old female Receives a single unit of FFP prior to elective surgery No prior transfusion history 45 minutes into the infusion she develops Chills Fever (102 deg C) Shortness of breath
51 Case #4 Progressive respiratory deterioration and BP Required mechanical ventilation, O2 Support 96 hours later Clinical improvement apparent Pulmonary infiltrates on chest xray still noted 7 days later This represents a fairly classic transfusion reaction known as
52 TRALI Transfusion Related Acute Lung Injury Acute onset Hypoxemia FiO2 < 300 or SPO2 < 90% on RA or other clinical evidence of hypoxemia Bilateral infiltrates on CXR No evidence of circulatory overload No preexisting ALI before transfusion During or within 6 hrs of transfusion No temporal relationship to an alternative risk factor
53 Case #4 Transfusion Associated Lung Injury Outcome in this case: Donor Center followed up and determined implicated donor had HLA Classs I antibodies to HLA-A2, A23, A24 Negative for platelet neutrophil /granulocyte antibodies Donor was a 54 y.o., 290 donations with NO prior adverse reaction reported 3 pregnancies over 30 ago Patient was negative for all antibodies

54 Volume 50, August 2010 TRANSFUSION
55 CONTACT DONOR CENTER TO START A TRALI INVESTIGATION AMERICAN RED CROSS Contact the Donor and Client Services Center (DCSC) to report complications of a potential TRALI related event Patient care questions should be directed to the Medical Director at Carolinas Region. The Donor and Client Service Center can be notified at The fax number to the DCSC is
56 To begin a TRALI investigation: Possible Recipient Complication Transfusion Reaction Report completed by the reporting hospital received by the DCSC case investigator submitted to the regional MD for evaluation. REPORT ALL PRODUCTS involved to ensure holds are placed on all involved donor records. MUST BE DONE to prevent subsequent donations, quarantine products
57 TRALI work up - Samples to send ARC from recipient* 1. HLA/HNA antibody testing 2 red tops 2. HLA/HNA antigen typing 2 EDTA tubes 3. HLA antigen and HLA antibody testing 2 red tops and 2 EDTA tubes 4. TOTAL: 4 red tops, 4 EDTA *consult with Blood Supplier for specific sample requirements v
58 The most common cause of transfusionassociated mortality reported to the FDA is Intravascular Transfusion Rxn with ABO incompatibility Post Transfusion Purpura TA-GVHD TRALI Transfusion acquired infection
59 Incidence and Mortality of Noninfectious Complications of Transfusion COMPLICATION INCIDENCE MORTALITY (%) Intravascular hemolysis with ABO Incompatibility 1:33,000 5 TA-GVHD 1:400, TRALI 1: PTP 1:200,
60 Multi alloantibodies in an immunocompromised patient
61 Case #5 35 month old female with Di George Syndrome s/p thymus transplant being evaluated for BMT transplant Multiple transfusion for anemia associated with red cell aplasia Presents with Hgb of 7.6 g/dl (baseline 10.6 to 11.5) Shortness of breath and cough lung nodules +Antibody Screen h/o anti- C, Jka, e, and warm auto
62 Selection of RBC units Need help from ARC <1% of donor population compatible with this combination of antibodies Responsiveness of ARC with frozen units from local distribution center Familiarity with the patient from prior transfusion episodes Maintaining local frozen inventory in case needed by Duke or adjacent hospital for this patient
63 Selection of Units SCIDS Severe Combined Immunodeficiency Syndrome (SCIDS) a genetic disorder in which both "arms" (B cells and T cells) of the adaptive immune system are crippled, due to a defect in one of several possible genes Immuno-incompetent At risk for GVHD CMV other infections SPECIAL BLOOD NEEDS IRRADIATED, CMV Negative or CMV reduced risk (LR) v
64 The rationale for deglycerolizing frozen RBC s with extensive washing is that Glycerol. Is not approved by the FDA Is toxic to the kidneys Can cause anaphylaxis Can cause hemolysis Can cause thrombocytopenia

65 How many planets in the solar system have rings? Jupiter, Saturn, Uranus, and Neptune all have rings.
Transfusion Reactions. Directed by M-azad March 2012
 Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Medicine Potpourri. BUMC - Phoenix Internal Medicine Residents September 29, 2015
 Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Transfusion. Dr Will Dooley
 Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Boot Camp Transfusion Reactions
 Boot Camp Transfusion Reactions Dr. Kristine Roland Regional Medical Lead for Transfusion Medicine, VCH Objectives By the end of this session, you should be able to: Describe in common language the potential
Boot Camp Transfusion Reactions Dr. Kristine Roland Regional Medical Lead for Transfusion Medicine, VCH Objectives By the end of this session, you should be able to: Describe in common language the potential
Blood Product Modifications: Leukofiltration, Irradiation and Washing
 1. Leukocyte Reduction Definitions and Standards: o Process also known as leukoreduction, or leukofiltration o Applicable AABB Standards, 25th ed. Leukocyte-reduced RBCs At least 85% of original RBCs
1. Leukocyte Reduction Definitions and Standards: o Process also known as leukoreduction, or leukofiltration o Applicable AABB Standards, 25th ed. Leukocyte-reduced RBCs At least 85% of original RBCs
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy. Megan Boysen Osborn, MD, MHPE
 Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY
 EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
It s a bird, It s a plane, No It s a. Presented by Julie Kirkegaard & Miche Swofford
 It s a bird, It s a plane, No It s a Presented by Julie Kirkegaard & Miche Swofford 55 year old woman admitted 11/23/2015 for colon cancer that metastasized to her liver History of 3 pregnancies Surgery
It s a bird, It s a plane, No It s a Presented by Julie Kirkegaard & Miche Swofford 55 year old woman admitted 11/23/2015 for colon cancer that metastasized to her liver History of 3 pregnancies Surgery
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER?
 TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER? 1. Fatal blood transfusion reactions are most likely the result of: a. Circulatory overload b. ABO incompatible blood due to patient identification
TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER? 1. Fatal blood transfusion reactions are most likely the result of: a. Circulatory overload b. ABO incompatible blood due to patient identification
In The Name Of GOD ADVERSE REACTIONS OF TRANSFUSION
 In The Name Of GOD The 7 th international and 12 th national congress on quality improvement in clinical laboratories ADVERSE REACTIONS OF TRANSFUSION By Mehdi Allahbakhshian, PhD, Hematology and Blood
In The Name Of GOD The 7 th international and 12 th national congress on quality improvement in clinical laboratories ADVERSE REACTIONS OF TRANSFUSION By Mehdi Allahbakhshian, PhD, Hematology and Blood
Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*
 and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*") Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
COMPLICATIONS OF BLOOD TRANSFUSIONS. :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan
 COMPLICATIONS OF BLOOD TRANSFUSIONS :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan COMPLICATIONS OF TRANSFUSIONS Transfusion reaction may result from either : A. Immune transfusion reaction. B. Non
COMPLICATIONS OF BLOOD TRANSFUSIONS :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan COMPLICATIONS OF TRANSFUSIONS Transfusion reaction may result from either : A. Immune transfusion reaction. B. Non
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Blood Transfusion. Dr William Dooley
 Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
Check a Pulse! When to Question SpO 2, NIBP & EtCO 2 Readings
 Check a Pulse! When to Question SpO 2, NIBP & EtCO 2 Readings Mike McEvoy, PhD, RN, CCRN, NRP Professor Emeritus - Critical Care Medicine Albany Medical College Albany, New York Chair Resuscitation Committee
Check a Pulse! When to Question SpO 2, NIBP & EtCO 2 Readings Mike McEvoy, PhD, RN, CCRN, NRP Professor Emeritus - Critical Care Medicine Albany Medical College Albany, New York Chair Resuscitation Committee
Blood/Blood Component Utilization and Administration Annual Compliance Education
 Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Consent Laboratory Transfuse RBC
 Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Approach to a patient with suspected blood transfusion reaction. Raju Vaddepally, MD
 Approach to a patient with suspected blood transfusion reaction Raju Vaddepally, MD Goals Detection of Acute Transfusion Reactions (ATR) Clinical and Laboratory Evaluation of ATR Management of individual
Approach to a patient with suspected blood transfusion reaction Raju Vaddepally, MD Goals Detection of Acute Transfusion Reactions (ATR) Clinical and Laboratory Evaluation of ATR Management of individual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital
 Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Unit 5: Blood Transfusion
 Unit 5: Blood Transfusion Blood transfusion (BT) therapy: Involves transfusing whole blood or blood components (specific portion or fraction of blood lacking in patient). Learn the concepts behind blood
Unit 5: Blood Transfusion Blood transfusion (BT) therapy: Involves transfusing whole blood or blood components (specific portion or fraction of blood lacking in patient). Learn the concepts behind blood
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Definitions of Current SHOT Categories & What to Report
 Definitions of Current SHOT Categories & What to Report Revised March 2011 1 ADVERSE EVENTS TERM DEFINITION WHAT TO REPORT IBCT - Wrong Blood Transfused (Incorrect Blood Component Transfused) Where a patient
Definitions of Current SHOT Categories & What to Report Revised March 2011 1 ADVERSE EVENTS TERM DEFINITION WHAT TO REPORT IBCT - Wrong Blood Transfused (Incorrect Blood Component Transfused) Where a patient
Patient Blood Management. Marisa B. Marques, MD UAB Department of Pathology November 17, 2016
 Patient Blood Management Marisa B. Marques, MD UAB Department of Pathology November 17, 2016 Learning Objectives Upon completion of the session, the participant will: 1) Differentiate between the various
Patient Blood Management Marisa B. Marques, MD UAB Department of Pathology November 17, 2016 Learning Objectives Upon completion of the session, the participant will: 1) Differentiate between the various
Have you ever managed patients who have experienced an adverse reaction to transfusion?
 Have you ever managed patients who have experienced an adverse reaction to transfusion? A. Yes, often B. Yes, occasionally C. No A. 1 in 30 units? B. 1 in 100? C. 1 in 1000? D. 1 in 10,000? SHOT collects
Have you ever managed patients who have experienced an adverse reaction to transfusion? A. Yes, often B. Yes, occasionally C. No A. 1 in 30 units? B. 1 in 100? C. 1 in 1000? D. 1 in 10,000? SHOT collects
Non-Infectious Transfusion Reactions
 Non-Infectious Transfusion Reactions Transfusion Reactions ANY unfavorable consequence is considered a transfusion reaction of blood TX The risks of transfusion must be weighed against the benefits Transfusion
Non-Infectious Transfusion Reactions Transfusion Reactions ANY unfavorable consequence is considered a transfusion reaction of blood TX The risks of transfusion must be weighed against the benefits Transfusion
Transfusion Reactions
 Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
25/10/2017. Clinical Relevance of the HLA System in Blood Transfusion. Outline of talk. Major Histocompatibility Complex
 Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
TRANSFUSION REACTIONS
 14 TRANSFUSION REACTIONS 14.1 INTRODUCTION Transfusion of blood and blood products are reported to cause reactions during or after procedure specially in patients who receive multiple transfusions. These
14 TRANSFUSION REACTIONS 14.1 INTRODUCTION Transfusion of blood and blood products are reported to cause reactions during or after procedure specially in patients who receive multiple transfusions. These
3. Which of the following would be inconsistent with respiratory alkalosis? A. ph = 7.57 B. PaCO = 30 mm Hg C. ph = 7.63 D.
 Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
TRANSFUSION ASSOCIATED DISEASE, RECALL, OR COMPLICATION INVESTIGATION POLICY I. FATALITIES AND COMPLICATIONS ASSOCIATED WITH TRANSFUSION:
 I. FATALITIES AND COMPLICATIONS ASSOCIATED WITH TRANSFUSION: A. TRANSFUSION RELATED FATALITY: FDA and MEDIC must be notified immediately, and subsequently in writing, when a possible transfusion related
I. FATALITIES AND COMPLICATIONS ASSOCIATED WITH TRANSFUSION: A. TRANSFUSION RELATED FATALITY: FDA and MEDIC must be notified immediately, and subsequently in writing, when a possible transfusion related
Blood & Blood Product Administration
 Approved by: Blood & Blood Product Administration Addendum to: Corporate Policy VII-B-397 Transfusion of Blood Components and Products- Pediatric/Neonate Gail Cameron Senior Director Operations, Maternal,
Approved by: Blood & Blood Product Administration Addendum to: Corporate Policy VII-B-397 Transfusion of Blood Components and Products- Pediatric/Neonate Gail Cameron Senior Director Operations, Maternal,
ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol
 Blood Transfusion Routine Investigations ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol Full Group & Screen 2ml EDTA Can be stored at 2-8C
Blood Transfusion Routine Investigations ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol Full Group & Screen 2ml EDTA Can be stored at 2-8C
Appendix E Choose the sign or symptom that best indicates severe respiratory distress.
 Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
ADULT TRANSFUSION GUIDELINES ORDERED COMPONENT
 ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
Transfusion reactions. Jim Taylor Haematology SpR Sheffield
 Transfusion reactions Jim Taylor Haematology SpR Sheffield Pre questions 1. Platelet transfusions are more prone to bacterial contamination compared to red cells. T/F 2. Common causes of an acute transfusion
Transfusion reactions Jim Taylor Haematology SpR Sheffield Pre questions 1. Platelet transfusions are more prone to bacterial contamination compared to red cells. T/F 2. Common causes of an acute transfusion
Specific Requirements
 Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Transfusion Associated Acute Lung Injury (TRALI)
") Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Objectives Define Transfusion-Related Acute Lung Injury (TRALI) and the role of
Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Objectives Define Transfusion-Related Acute Lung Injury (TRALI) and the role of
Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc.
 Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc.") Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Objectives Define Transfusion-Related Acute Lung Injury (TRALI) and the role of
Transfusion Associated Acute Lung Injury (TRALI) Chris Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Objectives Define Transfusion-Related Acute Lung Injury (TRALI) and the role of
Transfusion Reactions:
 Transfusion Reactions: Melissa R. George, D.O., F.C.A.P. Medical Director, Transfusion Medicine & Apheresis Penn State Milton S. Hershey Medical Center Office: HG069, Phone: 717-531-4627 E-mail: mgeorge5@hmc.psu.edu
Transfusion Reactions: Melissa R. George, D.O., F.C.A.P. Medical Director, Transfusion Medicine & Apheresis Penn State Milton S. Hershey Medical Center Office: HG069, Phone: 717-531-4627 E-mail: mgeorge5@hmc.psu.edu
WRHA Blood Conservation Service WRHA Transfusion Practice Committee. TEAM TRANSFUSION Differential Diagnosis of Adverse Events
 WRHA Blood Conservation Service WRHA Transfusion Practice Committee TEAM TRANSFUSION Differential Diagnosis of Adverse Events MANITOBA ADVERSE EVENT REPORTING SYSTEM DATA FLOW REACTION Physician orders
WRHA Blood Conservation Service WRHA Transfusion Practice Committee TEAM TRANSFUSION Differential Diagnosis of Adverse Events MANITOBA ADVERSE EVENT REPORTING SYSTEM DATA FLOW REACTION Physician orders
Blood Transfusion. What is blood transfusion? What are blood banks? When is a blood transfusion needed? Who can donate blood?
 What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
Transfusion Reactions: What? How? What now? Part II
 Transfusion Reactions: What? How? What now? Part II Margo Rollins, MD Assistant Professor of Pathology Emory University SOM Assistant Medical Director for Tissue, Transfusion & Apheresis Children s Healthcare
Transfusion Reactions: What? How? What now? Part II Margo Rollins, MD Assistant Professor of Pathology Emory University SOM Assistant Medical Director for Tissue, Transfusion & Apheresis Children s Healthcare
Transfusion reactions illustrated
 Transfusion reactions illustrated Chapter 1 Transfusion practice 1 Procedure of transfusion practice In general, transfusion-associated incidents occur due to multiple errors, most of which occur in the
Transfusion reactions illustrated Chapter 1 Transfusion practice 1 Procedure of transfusion practice In general, transfusion-associated incidents occur due to multiple errors, most of which occur in the
Blood Transfusion Reactions
 Blood Transfusion Reactions Introduction Many individuals require blood components and blood products. As per the BC Transfusion Medicine Advisory Group (BCTMAG), a blood component is at therapeutic component
Blood Transfusion Reactions Introduction Many individuals require blood components and blood products. As per the BC Transfusion Medicine Advisory Group (BCTMAG), a blood component is at therapeutic component
Immunohematology (Introduction)
") Modified from Serotonin version Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood
Modified from Serotonin version Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood
The ABC s of Blood Components. Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service
SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service") The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition
 References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition") Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood lost by hemorrhage or to correct
Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood lost by hemorrhage or to correct
The Child with a Hematologic Alteration
 47 The Child with a Hematologic Alteration HELPFUL HINT Review the anatomy and physiology of the hematologic system in an anatomy and physiology textbook. MATCHING KEY TERMS Match the term with the correct
47 The Child with a Hematologic Alteration HELPFUL HINT Review the anatomy and physiology of the hematologic system in an anatomy and physiology textbook. MATCHING KEY TERMS Match the term with the correct
Immunohematology. Done by : Zaid Al-Ghnaneem
 Immunohematology Done by : Zaid Al-Ghnaneem Hello everyone, in this sheet we will talk mainly about immunohematology which is the reactions between our immune system with Antigens found mainly within blood
Immunohematology Done by : Zaid Al-Ghnaneem Hello everyone, in this sheet we will talk mainly about immunohematology which is the reactions between our immune system with Antigens found mainly within blood
CORD BLOOD TESTING AND HDFN A CASE STUDY. Eric Rosa, MLS (ASCP) CM University of Kansas Hospital April 20, 2016
 CM University of Kansas Hospital April 20, 2016") CORD BLOOD TESTING AND HDFN A CASE STUDY Eric Rosa, MLS (ASCP) CM University of Kansas Hospital April 20, 2016 BACKGROUND KU Hospital policy: run ABO/Rh (front) type + Direct Antiglobulin test on cord
CORD BLOOD TESTING AND HDFN A CASE STUDY Eric Rosa, MLS (ASCP) CM University of Kansas Hospital April 20, 2016 BACKGROUND KU Hospital policy: run ABO/Rh (front) type + Direct Antiglobulin test on cord
UKGS TRANSFUSION SERVICE PRODUCTS AND AVAILABILITY
 Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
BLOOD TRANSFUSION. Dr Lumka Ntabeni
 BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
CHAPTER 10 BLOOD GROUPS: ABO AND Rh
 CHAPTER 10 BLOOD GROUPS: ABO AND Rh The success of human blood transfusions requires compatibility for the two major blood group antigen systems, namely ABO and Rh. The ABO system is defined by two red
CHAPTER 10 BLOOD GROUPS: ABO AND Rh The success of human blood transfusions requires compatibility for the two major blood group antigen systems, namely ABO and Rh. The ABO system is defined by two red
Appendix D An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires:
 Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Clinical Relevance of the HLA System in Blood Transfusion. Dr Colin J Brown PhD FRCPath. October 2017
 Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
For more information about how to cite these materials visit
 Author(s): Robertson Davenport, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Robertson Davenport, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Carbon Monoxide Exposure: Dräger PAC 3500 & RAD-57
 Carbon Monoxide Exposure: Dräger PAC 3500 & RAD-57 Supersedes: 10-23-06 Effective: 12-02-13 PURPOSE Carbon monoxide poisoning is one of the single most common poisoning exposure in the United States. Carbon
Carbon Monoxide Exposure: Dräger PAC 3500 & RAD-57 Supersedes: 10-23-06 Effective: 12-02-13 PURPOSE Carbon monoxide poisoning is one of the single most common poisoning exposure in the United States. Carbon
QUICK REFERENCE Clinical Practice Guide on Red Blood Cell Transfusion
 QUICK REFERENCE 2012 Clinical Practice Guide on Red Blood Cell Transfusion Presented by the American Society of Hematology, adapted from Red Blood Cell Transfusion: A Clinical Practice Guideline from the
QUICK REFERENCE 2012 Clinical Practice Guide on Red Blood Cell Transfusion Presented by the American Society of Hematology, adapted from Red Blood Cell Transfusion: A Clinical Practice Guideline from the
7 ADVERSE REACTIONS TO TRANSFUSION. Version July 2004, Revised 5/26/05
 Version July 2004, Revised 5/26/05 Blood Bank Labsite Preface Table of Contents 1: General Information... 2: Providing Blood to OR... 3: Emergency Use... 4: Blood Components... 5: Utilization Review...
Version July 2004, Revised 5/26/05 Blood Bank Labsite Preface Table of Contents 1: General Information... 2: Providing Blood to OR... 3: Emergency Use... 4: Blood Components... 5: Utilization Review...
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Oxygen Saturation Monitors & Pulse Oximetry. D. J. McMahon rev cewood
 Oxygen Saturation Monitors & Pulse Oximetry D. J. McMahon 141105 rev cewood 2017-11-14 2 3 Key Points Oxygen Saturation Monitors & Pulse Oximetry : Role of hemoglobin in respiration Basic principle of
Oxygen Saturation Monitors & Pulse Oximetry D. J. McMahon 141105 rev cewood 2017-11-14 2 3 Key Points Oxygen Saturation Monitors & Pulse Oximetry : Role of hemoglobin in respiration Basic principle of
MB Guideline 7. Transfusion Reaction- Identification, Management and Reporting
 MB Guideline 7 Transfusion Reaction- Identification, Management and Reporting When any unexpected or untoward sign or symptom occurs during or shortly after the transfusion of a blood component, a transfusion
MB Guideline 7 Transfusion Reaction- Identification, Management and Reporting When any unexpected or untoward sign or symptom occurs during or shortly after the transfusion of a blood component, a transfusion
A transfusion reaction is any adverse effect of transfusion therapy which occurs during or after administration of a blood component
 Brenda C. Barnes, Ph.D., MT(ASCP)SBB 1/2015 1 A transfusion reaction is any adverse effect of transfusion therapy which occurs during or after administration of a blood component Transfusion of any blood
Brenda C. Barnes, Ph.D., MT(ASCP)SBB 1/2015 1 A transfusion reaction is any adverse effect of transfusion therapy which occurs during or after administration of a blood component Transfusion of any blood
ECMO vs. CPB for Intraoperative Support: How do you Choose?
 ECMO vs. CPB for Intraoperative Support: How do you Choose? Shaf Keshavjee MD MSc FRCSC FACS Director, Toronto Lung Transplant Program Surgeon-in-Chief, University Health Network James Wallace McCutcheon
ECMO vs. CPB for Intraoperative Support: How do you Choose? Shaf Keshavjee MD MSc FRCSC FACS Director, Toronto Lung Transplant Program Surgeon-in-Chief, University Health Network James Wallace McCutcheon
PCCN Review Hematology
 PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
CURRENT COURSE OFFERINGS
 The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
Risks of Smoking in Pregnancy
 Information leaflet on Risks of Smoking in Pregnancy Routine Antenatal Carbon Monoxide Recording 1 Risks of Smoking during Pregnancy Smoking is the single greatest cause of ill health and premature death
Information leaflet on Risks of Smoking in Pregnancy Routine Antenatal Carbon Monoxide Recording 1 Risks of Smoking during Pregnancy Smoking is the single greatest cause of ill health and premature death
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Chapter 06 Lecture Outline. See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes.
 Chapter 06 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright 2016 McGraw-Hill Education. 2012 Pearson Permission Education,
Chapter 06 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright 2016 McGraw-Hill Education. 2012 Pearson Permission Education,
Direct Antiglobulin Test (DAT)
") Exercise 8 Direct Antiglobulin Test (DAT) Objectives 1. State the purpose for performing the DAT. 2. State what a positive DAT indicates. 3. List the reagents which are used for performing the DAT. 4.
Exercise 8 Direct Antiglobulin Test (DAT) Objectives 1. State the purpose for performing the DAT. 2. State what a positive DAT indicates. 3. List the reagents which are used for performing the DAT. 4.
Management of TRALI. Handouts. Continuing Education 5/20/2015.
 Management of TRALI Christine Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Massimo Mangiola, Ph.D. Director of Special Services Rhode Island Blood Center Handouts http://www.immucor.com/enus/pages/educational-program-handouts.aspx
Management of TRALI Christine Beritela, MS, MT(ASCP)SBB Area Technical Consultant Immucor, Inc. Massimo Mangiola, Ph.D. Director of Special Services Rhode Island Blood Center Handouts http://www.immucor.com/enus/pages/educational-program-handouts.aspx
Functions of Blood. Transport. Transport. Defense. Regulation. Unit 6 Cardiovascular System: Blood
 Unit 6 Cardiovascular System: Blood Functions of Blood With each beat of the heart, approximately 75 ml of blood is pumped On average, the heart beats 70 times per minute Every minute, the heart pumps
Unit 6 Cardiovascular System: Blood Functions of Blood With each beat of the heart, approximately 75 ml of blood is pumped On average, the heart beats 70 times per minute Every minute, the heart pumps
Blood Component Therapy
 Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
RHESUS BLOOD GROUP SYSTEM (Author: Alvine Janse van Rensburg; ND Biomedical Technology-Microbiology, Haematology, Chemistry)
") RHESUS BLOOD GROUP SYSTEM (Author: Alvine Janse van Rensburg; ND Biomedical Technology-Microbiology, Haematology, Chemistry) Introduction The term Rh refers to a complex blood group system that comprised
RHESUS BLOOD GROUP SYSTEM (Author: Alvine Janse van Rensburg; ND Biomedical Technology-Microbiology, Haematology, Chemistry) Introduction The term Rh refers to a complex blood group system that comprised
The blood returns from the body and enters right atrium using the vena cava. It passes through the tricuspid valve to the right ventricle.
 The blood returns from the body and enters right atrium using the vena cava. It passes through the tricuspid valve to the right ventricle. From this camber, it passes through the pulmonary semilunar valve
The blood returns from the body and enters right atrium using the vena cava. It passes through the tricuspid valve to the right ventricle. From this camber, it passes through the pulmonary semilunar valve
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS NLBCP-006. Issuing Authority
 Government of Newfoundland and Labrador Department of Health and Community Services Provincial Blood Coordinating Program INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS Office of Administrative Responsibility
Government of Newfoundland and Labrador Department of Health and Community Services Provincial Blood Coordinating Program INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS Office of Administrative Responsibility
TRANSFUSION REACTION EVALUATION
 Lab Dept: Test Name: Transfusion Services TRANSFUSION REACTION EVALUATION General Information Lab Order Codes: Synonyms: CPT Codes: Test Includes: TRXR Transfusion Complication Workup; Hemolytic reaction
Lab Dept: Test Name: Transfusion Services TRANSFUSION REACTION EVALUATION General Information Lab Order Codes: Synonyms: CPT Codes: Test Includes: TRXR Transfusion Complication Workup; Hemolytic reaction
Chapter 13 The Blood
 Chapter 13 The Blood Copyright 2015 Wolters Kluwer Health Lippincott Williams & Wilkins Overview Key Terms agglutination erythrocyte lymphocyte albumin fibrin megakaryocyte anemia hematocrit monocyte antigen
Chapter 13 The Blood Copyright 2015 Wolters Kluwer Health Lippincott Williams & Wilkins Overview Key Terms agglutination erythrocyte lymphocyte albumin fibrin megakaryocyte anemia hematocrit monocyte antigen
From donor biology to donor health protection: Three (very) short stories
 short stories") From donor biology to donor health protection: Three (very) short stories Steven L. Spitalnik, M.D. Laboratory of Transfusion Biology Potential Conflicts of Interest Hemanext: Tioma, Inc: Advisory Board
From donor biology to donor health protection: Three (very) short stories Steven L. Spitalnik, M.D. Laboratory of Transfusion Biology Potential Conflicts of Interest Hemanext: Tioma, Inc: Advisory Board
TRANSFUSION REACTION AMONG THE BLOOD RECIPIENT - A STUDY OF 120 CASES
 TRANSFUSION REACTION AMONG THE BLOOD RECIPIENT - A STUDY OF 120 CASES Chowdhury FS 1, Biswas J 2, Siddiqui MAE 3, Hoque MM 4, Adnan SK 5 Abstract: Context: Blood transfusion is a life saving procedure.
TRANSFUSION REACTION AMONG THE BLOOD RECIPIENT - A STUDY OF 120 CASES Chowdhury FS 1, Biswas J 2, Siddiqui MAE 3, Hoque MM 4, Adnan SK 5 Abstract: Context: Blood transfusion is a life saving procedure.
How we View & Approach TACO
 How we View & Approach TACO Annual Blood Transfusion & Hemovigilance Symposium Ede, Netherlands May 22, 3014 Mark A. Popovsky, M.D. Chief Medical Officer, Haemonetics Corporation Associate Clinical Professor,
How we View & Approach TACO Annual Blood Transfusion & Hemovigilance Symposium Ede, Netherlands May 22, 3014 Mark A. Popovsky, M.D. Chief Medical Officer, Haemonetics Corporation Associate Clinical Professor,
ECLS Registry Form Extracorporeal Life Support Organization (ELSO)
") ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
In the United States, transfusion reactions are reported to occur. Global Prevalence. Evolution of Transfusion Practices
 Evolution of Transfusion Practices TRALI, TACO, and other Transfusion Complications Michael Rieker, DNP, CRNA Wake Forest Baptist Medical Center 1665 - The first Blood transfusions of record take place.
Evolution of Transfusion Practices TRALI, TACO, and other Transfusion Complications Michael Rieker, DNP, CRNA Wake Forest Baptist Medical Center 1665 - The first Blood transfusions of record take place.
Transfusion Limbo How Low Will You Go? Safely. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric