It s a bird, It s a plane, No It s a. Presented by Julie Kirkegaard & Miche Swofford
|
|
|
- Magnus Morrison
- 5 years ago
- Views:
Transcription




1 It s a bird, It s a plane, No It s a Presented by Julie Kirkegaard & Miche Swofford
2 55 year old woman admitted 11/23/2015 for colon cancer that metastasized to her liver History of 3 pregnancies Surgery was performed 11/23 to remove masses Exploratory laparotomy led to right hepatic lobectomy 10 hour surgery Lab values prior to surgery: PLT 180 TH/uL ( ) Hgb 12.3 g/dl ( )
3 Given three packed cells during surgery and a couple units of plasma later that evening Surgery goes well, Hgb and PLT counts are monitored for next several days 11/23 Post-Op Hgb 11.4/PLT 215,000 At midnight Hgb 8.5/PLT 115,000
4 11/ Hgb 7.3 and PLT 98,000 Transfused 2 RBCs and 1 PLT After transfusion Hgb 9.6 and PLT 70,000 Transfused 2 thawed plasma and 1 PLT
5 Nothing else transfused after 11/24 and patient values start rising 11/25 Hgb 8.3/PLT 65,000 11/26 Hgb 8.7/PLT 80,000 11/27 Hgb 9.6/PLT 111,000 11/28 Hgb 10.4/PLT 157,000 11/29 Hgb 10.1/PLT 146,000

6 11-30 Hgb 10 g and PLT count 1,000 Patient bleeding from nose Petechiae on arms, legs, thighs and trunk Couldn t move patient because would start bleeding
? Autoimmune response from platelet transfusion?")
7 What could have caused a sudden drop in the platelet count? Hematology/oncology consult on the case ITP - Idiopathic thrombocytopenic purpura? Medication related (Zosyn, famotidine, heparin)? Autoimmune response from platelet transfusion? Sample obtained and sent to Community Blood Center for investigation into possible platelet antibody
8 At CBC Sample received for investigation of autoimmune thrombocytopenia Platelet antibody screen and platelet bound IgG Platelet count was 2,000 Platelet count was too low to get a monolayer so no platelet bound IgG performed Platelet antibody screen was positive Reactive 8/8 with Capture P solid phase adherence assay ELISA assay showed HLA antibody and reactivity with 2 of 2 glycoprotein IIb/IIIa carrying the HPA-1a antigen
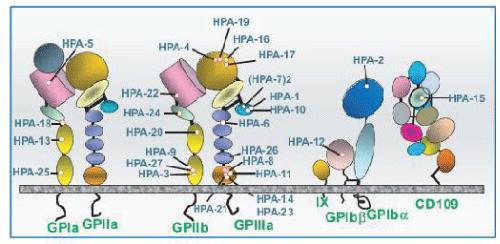
9 Human Platelet Antigens (HPA) 34 HPA expressed on 6 different glycoproteins GPIIb GPIIIa GPIa GP1bα GPIbβ CD109 Six biallelic systems covering 12 antigens HPA-1, -2, -3, -4, -5, other other HPA are low frequency or rare antigens
10 Platelet glycoproteins
11 GPIIb/IIIa Most abundant molecule on surface of platelets 20 of 34 HPAs reside on GPIIb/IIIa Receptor for ligands important in mediating hemostasis and inflammation GPIb/V/IX, GPIa/IIa and CD109 express remaining 14 HPAs
12 GPIIb/IIIa
13 HPA-1a Incidence of HPA-1a negative phenotype in Caucasians is ~2% Anti-HPA-1a most common cause of neonatal immune thrombocytopenia (NAIT) in Caucasians and African ancestry 85% of NAIT cases
14 Sample sent to NYBC for HPA-1a genotyping Patient was HPA-1a negative What do these test results and history suggest as a possible diagnosis??? Patient was transfused and with red cells, platelets and plasma PTP- post transfusion purpura
15 It s a Bird, It s a Plane, No It s a PTP is a rare syndrome characterized by development of dramatic severe self limiting thrombocytopenia and bleeding Purpuric rash, bruising, mucosal bleeding, gastrointestinal and urinary tract bleeding Duration of thrombocytopenia in untreated patients is about days Occurs 2-14 days after transfusion of blood products in patient s previously sensitized by pregnancy or transfusion PTP is an anamnestic response
16 Most commonly associated with transfusion of RBCs Also associated with platelets and plasma 30% of patients have major hemorrhage and mortality rate is 10-20% PTP caused by alloimmunization to human platelet specific antigens Most often HPA-1a (90% of cases) alone or in combination with abys to other platelet antigens on glycoprotein IIb/IIIa Other antibodies reported to cause PTP: HPA-1b, HPA-3a, HPA-3b, HPA-4a, HPA-5a, HPA-5b Incidence of 1 in 50,000 to 100,000 transfusions

17 Typically occurs in multiparous women but also reported rarely in men Female to male ration is 5:1 Patients who develop anti-hpa-1a often share certain HLA genotypes: HLA-B8 or HLA- DRB3*0101 and HLA-DQB1*0201 Similar to that seen in NAIT Platelet antibody destroys transfused and autologous platelets
18 Differential diagnosis includes consideration of other causes of thrombocytopenia: Autoimmune thrombocytopenia Drug induced thrombocytopenia Disseminated intravascular coagulation Heparin induced thrombocytopenia Thrombotic thrombocytopenia purpura Diagnosis confirmed by clinical presentation and detection of platelet specific alloantibodies Platelet genotype is helpful
19 3 theories why autologous plts destroyed Immune complexes bind to platelets through Fc receptor causing destruction of platelets Donor derived soluble plt glycoprotein adsorbed onto autologous platelets making them susceptible to immune destruction Immune response includes autoimmune component along with alloantibodies Causes both autologous and transfused antigen negative platelet destruction Most support for this theory
20 Treatment High dose IVIG (2g/Kg) alone or in combination with corticosteroids Usually results in plt count >100,000 in 3-5 days 85% response rate Mechanism of action of IVIG is thought to be due to: Anti-idiotype antibodies Fc receptor blockage Nonspecific binding of IG to platelet surface and/or Acceleration of IgG catabolism Plasma exchange may be helpful in patients who do not respond to IVIG
21 Treatment Splenectomy for those that do not respond Tx of antigen negative plts may be used in acute phase to help control bleeding but have decreased survival also Plt count will not go up and stay up
22 Prevention Recurrence of PTP after subsequent RBC transfusion is uncommon but has been reported Recommend RBC and platelet products from corresponding antigen negative donors on subsequent transfusions Value of this is unclear Washed red cells may offer some protection against recurrence Reports of PTP occurring after deglycerolized rejuvenated or washed red blood cells UK report described decrease in PTP cases after implementation of universal RBC leukoreduction
23 HPA-1a negative products Rare incidence of ~ 2% How do you test for them? Screen products at time of donation for HPA-1a Serologically No commercial antisera available Must have source of anti-hpa-1a Hard to find pure anti-hpa-1a without HLA antibodies also present Molecular Utilize DNA from donor CBC actively screens for HPA-1a negative donors
24 How do you get HPA-1a negative products Screen for HPA-1a negative platelets Limited amount of products donated in a day May take several days of random screening Some centers maintain donor lists of HPA-1a donors Call donors in to donate Must schedule donors Wait for release from processing Import HPA-1a negative platelets from other providers
25 Recap on patient: Previously has had a normal platelet count drops from surgery Given two units of platelets 11/24/2015 Platelet count remains normal for the next 5 days Sudden drop occurs on day 6 11/30/2015 Petechiae and nose bleeds CBC confirms platelet antibody HPA-1a antibody
26 Treatment plan for patient: Order for IVIG 50g dose of 1000 mg/kg once a day from 11/30-12/2 Zosyn and famotidine discontinued 11/30 in case medication related Afrin for nose bleeds (eases congestion and sinusitis) Transfuse HPA-1a negative platelets but want to avoid giving platelets as this may lead to further immune response Recommended to transfuse only during bleeding episodes Washed RBCs should be given Avoid plasma transfusions to avoid subsequent events
27 11/30 HPA-1a negative plt ordered from CBC to have on hand in the event of bleeding and/or a of PLT <10,000 12/1 Hgb 8.6/PLT 5,000 12/2 Hgb 9.7/PLT 0030 Doing well in AM, healing at surgical sight; no nose bleeds Afrin spray continued 12/2 Hgb 9.2/PLT 2038 Bleeding during bowel movement, blood in urine, vaginal 2000 HPA-1a negative PLT transfused at 2130
28 Hgb 8.4/PLT 0902 Hgb 9.0/PLT 39, Hgb 8.5/PLT 1,000 HPA-1a platelet ordered and given 2247 Discovered 50 g dose of IVIG was incorrect for patients weight and 110 g dose of 1000mg/kg given 12/4 and discontinued after one dose total of 4 IVIG doses 12/5 Hgb 7.2/PLT 18,000 12/5 1 saline washed HPA-1a negative RBC ordered from CBC to have on hand Unit not given expired 12-5 HPA-1a negative PLT ordered from CBC None available. CBC calling in donors to donate
29 12/6 Hgb 7.0/PLT 8,000 12/7 Hgb 7.2/PLT 12,000 12/8 Hgb 6.3/PLT 45,000 Platelet count increasing while hemoglobin drops One washed HPA-1a negative RBC is ordered and transfused 12/ Hgb 8.0/PLT 60,000 Further platelet transfusions cancelled as count is up
30 Patient outcome Pt hemodynamically stable (HgB 9.0 & PLT 139) and discharged 1819 Seen again in ED for post-surgical staph infection and admitted 12/14 Hepatic fluid collection Augmentin given for infection then discharged 12/17 no transfusions needed
31 Patient continually followed by Oncology for the next few months Lab work drawn a minimum of 2X a month Platelet count and hemoglobin remain stable and continue to rise No symptoms of bleeding Office visit about once a month
32 Waiting for patient to fully recover from surgery and infections to continue with cancer treatment 3/22/2016 Hgb 11.0 and PLT count 198,000 and patient states they now feel ready to move forward with chemotherapy treatment for next 4 months
33 Women with history of PTP may be at increased risk for having a pregnancy affected by neonatal alloimmune thrombocytopenia (NAIT) Increased risk of PTP in women who have previously had children with NAIT has not been reported


34 Official Lab Ninja Designated Blood Bank Brain PTP will not prevail!!
35 Objectives Discuss the clinical manifestations associated with post transfusion purpura Discuss the testing required to diagnose post transfusion purpura and the common antibodies associated with post transfusion purpura List the recommended treatment for post transfusion purpura and recommendations for blood products for transfusion
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Contemporary perspectives and initial management of pediatric ITP. William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA
 Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Blood Product Modifications: Leukofiltration, Irradiation and Washing
 1. Leukocyte Reduction Definitions and Standards: o Process also known as leukoreduction, or leukofiltration o Applicable AABB Standards, 25th ed. Leukocyte-reduced RBCs At least 85% of original RBCs
1. Leukocyte Reduction Definitions and Standards: o Process also known as leukoreduction, or leukofiltration o Applicable AABB Standards, 25th ed. Leukocyte-reduced RBCs At least 85% of original RBCs
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Instructor s Manual Chapter 26 Hematological Alterations. 1. A man and woman both test positive for the sickle cell trait. The couple asks the
 1 Instructor s Manual Chapter 26 Hematological Alterations Answers to Study Questions 1. A man and woman both test positive for the sickle cell trait. The couple asks the nurse how many of their children
1 Instructor s Manual Chapter 26 Hematological Alterations Answers to Study Questions 1. A man and woman both test positive for the sickle cell trait. The couple asks the nurse how many of their children
GOOD MORNING! Thursday, July Heidi Murphy, MD Leslie Carter-King, MD
 GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
UKGS TRANSFUSION SERVICE PRODUCTS AND AVAILABILITY
 Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Transfusion Management of IgA deficiency. Emily Coberly, MD Medical Director, Transfusion Services University of Missouri Columbia
 Transfusion Management of IgA deficiency Emily Coberly, MD Medical Director, Transfusion Services University of Missouri Columbia Our patient 63 year-old female with a duodenal stricture who was admitted
Transfusion Management of IgA deficiency Emily Coberly, MD Medical Director, Transfusion Services University of Missouri Columbia Our patient 63 year-old female with a duodenal stricture who was admitted
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
An Approach to the Patient Refractory to Platelets Transfusion. Harold Alvarez, MD
 Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY
 V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY Kharkov Regional Centre of Cardiovascular surgery V.N. Karazin Kharkov National University Department of Internal Medicine Immune thrombocytopenic purpura Abduyeva
V.N. KARAZIN KHARKOV NATIONAL UNIVERSITY Kharkov Regional Centre of Cardiovascular surgery V.N. Karazin Kharkov National University Department of Internal Medicine Immune thrombocytopenic purpura Abduyeva
Form 2033 R3.0: Wiskott-Aldrich Syndrome Pre-HSCT Data
 Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Has this patient's data been previously reported to USIDNET? USIDNET ID: Today's Date: - - Date of HSCT for which
Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Has this patient's data been previously reported to USIDNET? USIDNET ID: Today's Date: - - Date of HSCT for which
Use of Intravenous Anti-RhD Immunoglobulin (RhIG) in the Treatment of Primary Immune Thrombocytopenia
 in the Treatment of Primary Immune Thrombocytopenia") Use of Intravenous Anti-RhD Immunoglobulin (RhIG) in the Treatment of Primary Immune Thrombocytopenia KRISTINA WILLIAMS ABSTRACT Commercialized intravenous immunoglobulin (IVIG) products have been used
Use of Intravenous Anti-RhD Immunoglobulin (RhIG) in the Treatment of Primary Immune Thrombocytopenia KRISTINA WILLIAMS ABSTRACT Commercialized intravenous immunoglobulin (IVIG) products have been used
A sickle in a pickle! by Julie Kirkegaard, MT(ASCP)SBB Community Blood Center, KC, MO and Elizabeth Jones, MT(ASCP)BB Saint Luke s Hospital, KC, MO
SBB Community Blood Center, KC, MO and Elizabeth Jones, MT(ASCP)BB Saint Luke s Hospital, KC, MO") A sickle in a pickle! by Julie Kirkegaard, MT(ASCP)SBB Community Blood Center, KC, MO and Elizabeth Jones, MT(ASCP)BB Saint Luke s Hospital, KC, MO A couple of definitions! Sickle Cell Disease- an autosomal
A sickle in a pickle! by Julie Kirkegaard, MT(ASCP)SBB Community Blood Center, KC, MO and Elizabeth Jones, MT(ASCP)BB Saint Luke s Hospital, KC, MO A couple of definitions! Sickle Cell Disease- an autosomal
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
WISKOTT-ALDRICH SYNDROME. An X-linked Primary Immunodeficiency
 WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Dialogue between Clinician and Pathologist on CBC report
 Dialogue between Clinician and Pathologist on CBC report Dr. Seema Bhatwadekar Haematologist, Oncohaematologist & Transplant Physician Vadodara. CBC PBS Most important test to make probable diagnosis Crucial
Dialogue between Clinician and Pathologist on CBC report Dr. Seema Bhatwadekar Haematologist, Oncohaematologist & Transplant Physician Vadodara. CBC PBS Most important test to make probable diagnosis Crucial
The importance of thrombocytopenia and its causes
 SYSMEX EDUCATIONAL ENHANCEMENT AND DEVELOPMENT NO 4 2017 SEED HAEMATOLOGY The importance of thrombocytopenia and its causes Key words: Thrombocytopenia, thrombocytopenic, low levels of platelets What is
SYSMEX EDUCATIONAL ENHANCEMENT AND DEVELOPMENT NO 4 2017 SEED HAEMATOLOGY The importance of thrombocytopenia and its causes Key words: Thrombocytopenia, thrombocytopenic, low levels of platelets What is
POLICY NO. Printed copies are for reference only. Please refer to the electronic copy for the latest version.
 Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
8/28/2018. Disclosures. Objectives. None. Automation to PreciseType and Everything in Between
 Automation to PreciseType and Everything in Between Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles None Disclosures Objectives Describe the application of molecular testing
Automation to PreciseType and Everything in Between Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles None Disclosures Objectives Describe the application of molecular testing
Automation to PreciseType and Everything in Between. Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles
 Transfusion Medicine Children s Hospital Los Angeles") Automation to PreciseType and Everything in Between Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles None Disclosures Objectives Describe the application of molecular testing
Automation to PreciseType and Everything in Between Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles None Disclosures Objectives Describe the application of molecular testing
Bleeding Disorders.2 MS Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD
 Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Medical Surgical Review Handout- Hematology/Oncology 2016
 Medical Surgical Review Handout- Hematology/Oncology 2016 Overview Blood circulates in the cardiovascular system o Carries oxygen to the cells o Carries waste away from the cells Functions of blood o Transportation:
Medical Surgical Review Handout- Hematology/Oncology 2016 Overview Blood circulates in the cardiovascular system o Carries oxygen to the cells o Carries waste away from the cells Functions of blood o Transportation:
Specific Requirements
 Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Transfusion Reactions. Directed by M-azad March 2012
 Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
EDUCATIONAL COMMENTARY PLATELET DISORDERS
 EDUCATIONAL COMMENTARY PLATELET DISORDERS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Earn
EDUCATIONAL COMMENTARY PLATELET DISORDERS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Earn
TRANSFUSION REACTIONS
 14 TRANSFUSION REACTIONS 14.1 INTRODUCTION Transfusion of blood and blood products are reported to cause reactions during or after procedure specially in patients who receive multiple transfusions. These
14 TRANSFUSION REACTIONS 14.1 INTRODUCTION Transfusion of blood and blood products are reported to cause reactions during or after procedure specially in patients who receive multiple transfusions. These
PILOT STUDY OF ANTIGEN MATCHING FOR AUTOIMMUNE HEMOLYTIC ANEMIA
 PILOT STUDY OF ANTIGEN MATCHING FOR AUTOIMMUNE HEMOLYTIC ANEMIA Sharon Rice & Fred Plapp Saint Luke s Hospital Kansas City, MO CENTRALIZED TRANSFUSION SERVICE Antibody identification Antibody titer Antigen
PILOT STUDY OF ANTIGEN MATCHING FOR AUTOIMMUNE HEMOLYTIC ANEMIA Sharon Rice & Fred Plapp Saint Luke s Hospital Kansas City, MO CENTRALIZED TRANSFUSION SERVICE Antibody identification Antibody titer Antigen
Transfusion Practices and Creation of a Registry for Patients with Sickle Cell Disease within the Atlanta Sickle Cell Consortium
 Transfusion Practices and Creation of a Registry for Patients with Sickle Cell Disease within the Atlanta Sickle Cell Consortium Annie Winkler MD Assistant Professor, Emory University Department of Pathology
Transfusion Practices and Creation of a Registry for Patients with Sickle Cell Disease within the Atlanta Sickle Cell Consortium Annie Winkler MD Assistant Professor, Emory University Department of Pathology
INTRODUCTION TO SET FORTH APROACH TO MANAGING ADULTS TO SET FORTH APROACH PRIMARY ( PRIMARY AUTOIMMUNE) AUTOIMMUNE ITP FROM ASH & THE BRITISH
 AUTOIMMUNE ITP FROM ASH & THE BRITISH") HOW I TREAT IDIOPATHIC THROMBOCYTOPENIC PURPURA Dauglas B. Cines, James B Bussel. Blood Oktober 2005:106(7):2244-22512251 INTRODUCTION TO SET FORTH APROACH TO MANAGING ADULTS PRIMARY (AUTOIMMUNE) ITP FROM
HOW I TREAT IDIOPATHIC THROMBOCYTOPENIC PURPURA Dauglas B. Cines, James B Bussel. Blood Oktober 2005:106(7):2244-22512251 INTRODUCTION TO SET FORTH APROACH TO MANAGING ADULTS PRIMARY (AUTOIMMUNE) ITP FROM
For platelet control as individual as you
 For platelet control as individual as you Explore the possibilities of Immune Thrombocytopenic Purpura (ITP) treatment. Important Risk Information WARNING: INTRAVASCULAR HEMOLYSIS (IVH) Intravascular hemolysis
For platelet control as individual as you Explore the possibilities of Immune Thrombocytopenic Purpura (ITP) treatment. Important Risk Information WARNING: INTRAVASCULAR HEMOLYSIS (IVH) Intravascular hemolysis
QUICK REFERENCE Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP)
") QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
Immunohematology. Done by : Zaid Al-Ghnaneem
 Immunohematology Done by : Zaid Al-Ghnaneem Hello everyone, in this sheet we will talk mainly about immunohematology which is the reactions between our immune system with Antigens found mainly within blood
Immunohematology Done by : Zaid Al-Ghnaneem Hello everyone, in this sheet we will talk mainly about immunohematology which is the reactions between our immune system with Antigens found mainly within blood
Immunological transfusion reactions
 Immunological transfusion reactions Immunological transfusion reactions can be hemolytic or non-hemolytic in nature. Both types can be separated into acute (those occurring immediately after transfusion)
Immunological transfusion reactions Immunological transfusion reactions can be hemolytic or non-hemolytic in nature. Both types can be separated into acute (those occurring immediately after transfusion)
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Bleeding disorders. Hemostatic failure: Inappropriate and excessive bleeding either spontaneous or in response to injury.
 1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
Neutropenia Following Intravenous Immunoglobulin Therapy in Pediatric Patients with Idiopathic Thrombocytopenic Purpura
 ORIGINAL ARTICLE IJBC 2014;6(2): 81-85 Neutropenia Following Intravenous Immunoglobulin Therapy in Pediatric Patients with Idiopathic Thrombocytopenic Purpura Ansari S * 1, Shirali A 1, Khalili N 1, Daneshfar
ORIGINAL ARTICLE IJBC 2014;6(2): 81-85 Neutropenia Following Intravenous Immunoglobulin Therapy in Pediatric Patients with Idiopathic Thrombocytopenic Purpura Ansari S * 1, Shirali A 1, Khalili N 1, Daneshfar
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Management of platelet refractory patients, why does your patient keep on bleeding? Dr Colin Brown, H&I Dept, NHSBT Colindale
 Management of platelet refractory patients, why does your patient keep on bleeding? Dr Colin Brown, H&I Dept, NHSBT Colindale Pooled Platelets (Buffy Coat Derived) Adult dose from 4 ABO-identical donors
Management of platelet refractory patients, why does your patient keep on bleeding? Dr Colin Brown, H&I Dept, NHSBT Colindale Pooled Platelets (Buffy Coat Derived) Adult dose from 4 ABO-identical donors
Idiopathic Thrombocytopenic Purpura Presenting as Post-extraction Hemorrhage
 Idiopathic Thrombocytopenic Purpura Presenting as Post-extraction Hemorrhage Abstract Aim: The aim of this article is to present a case of idiopathic thrombocytopenic purpura (ITP) in order to emphasize
Idiopathic Thrombocytopenic Purpura Presenting as Post-extraction Hemorrhage Abstract Aim: The aim of this article is to present a case of idiopathic thrombocytopenic purpura (ITP) in order to emphasize
2. Does the patient have a diagnosis of chronic idiopathic thrombocytopenic purpura (ITP)?
?") Pharmacy Prior Authorization MERC CARE (MEDICAID) Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE (MEDICAID) Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
What You Need to Know About Blood Transfusion. Elianna Saidenberg May 2014
 What You Need to Know About Blood Transfusion Elianna Saidenberg May 2014 Objectives Why your doctor might order transfusion therapy Where does the blood come from The beginning of your transfusion Consent
What You Need to Know About Blood Transfusion Elianna Saidenberg May 2014 Objectives Why your doctor might order transfusion therapy Where does the blood come from The beginning of your transfusion Consent
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
A Patient s Guide to Blood Components and Products
 2014 A Patient s Guide to Blood Components and Products Contents What is a blood transfusion?... 1 Informed consent... 1 Frequently asked questions about blood transfusions... 2 What can I expect during
2014 A Patient s Guide to Blood Components and Products Contents What is a blood transfusion?... 1 Informed consent... 1 Frequently asked questions about blood transfusions... 2 What can I expect during
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Blood Component Therapy
 Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
CURRENT COURSE OFFERINGS
 The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
Immunohaematology: a branch of immunology that deals with the immunologic properties of blood.
 1 Immunohaematology: a branch of immunology that deals with the immunologic properties of blood. The red blood cells have on their surface hundreds of antigens and according to the antigen on their surface
1 Immunohaematology: a branch of immunology that deals with the immunologic properties of blood. The red blood cells have on their surface hundreds of antigens and according to the antigen on their surface
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Hemostatic System - general information
 PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
Hematologic Disorders. Assistant professor of anesthesia
 Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Transfusion Medicine Best Practices: Indications for Blood Components
 Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE (MEDICAID) Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE (MEDICAID) Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
BLEEDING DISORDERS Simple complement:
 BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition
 References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition") Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood lost by hemorrhage or to correct
Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood lost by hemorrhage or to correct
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Immunohematology (Introduction)
") Modified from Serotonin version Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood
Modified from Serotonin version Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood
Essentials of Blood Group Antigens and Antibodies
 Essentials of Blood Group Antigens and Antibodies Non-Medical Authorisation of blood Components Nov 2017 East Midlands Regional Transfusion Committee Transfusion Terminology Antigens and Antibodies Antibodies
Essentials of Blood Group Antigens and Antibodies Non-Medical Authorisation of blood Components Nov 2017 East Midlands Regional Transfusion Committee Transfusion Terminology Antigens and Antibodies Antibodies
Bleeding Disorders. Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph
 Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Transfusion Reactions: What? How? What now? Part II
 Transfusion Reactions: What? How? What now? Part II Margo Rollins, MD Assistant Professor of Pathology Emory University SOM Assistant Medical Director for Tissue, Transfusion & Apheresis Children s Healthcare
Transfusion Reactions: What? How? What now? Part II Margo Rollins, MD Assistant Professor of Pathology Emory University SOM Assistant Medical Director for Tissue, Transfusion & Apheresis Children s Healthcare
Immune Thrombocytopenia (ITP)
") Immune Thrombocytopenia (ITP) ITP - What is it? ITP is a blood disorder affecting platelets in the blood. Platelets are small cells in your blood that help your blood to clot. In ITP the body s immune
Immune Thrombocytopenia (ITP) ITP - What is it? ITP is a blood disorder affecting platelets in the blood. Platelets are small cells in your blood that help your blood to clot. In ITP the body s immune
Definitions of Current SHOT Categories & What to Report
 Definitions of Current SHOT Categories & What to Report Revised March 2011 1 ADVERSE EVENTS TERM DEFINITION WHAT TO REPORT IBCT - Wrong Blood Transfused (Incorrect Blood Component Transfused) Where a patient
Definitions of Current SHOT Categories & What to Report Revised March 2011 1 ADVERSE EVENTS TERM DEFINITION WHAT TO REPORT IBCT - Wrong Blood Transfused (Incorrect Blood Component Transfused) Where a patient
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
Nick Bandarenko, MD Duke University Transfusion Service
 Nick Bandarenko, MD Duke University Transfusion Service AN UNEXPECTED ADVERSE EVENT Case #1 3 month old 4.3kg boy with congenital heart malformation Ventricular Septal Defect (VSD) Failure to thrive and
Nick Bandarenko, MD Duke University Transfusion Service AN UNEXPECTED ADVERSE EVENT Case #1 3 month old 4.3kg boy with congenital heart malformation Ventricular Septal Defect (VSD) Failure to thrive and
When Selfies Go Bad!
 When Selfies Go Bad! Decoding Autoantibodies and Autoimmune Hemolytic Anemia D. Joe Chaffin, MD April 17, 2017 Outline Background Warm autoantibodies and WAIHA Cold autoantibodies and CAD Paroxysmal Cold
When Selfies Go Bad! Decoding Autoantibodies and Autoimmune Hemolytic Anemia D. Joe Chaffin, MD April 17, 2017 Outline Background Warm autoantibodies and WAIHA Cold autoantibodies and CAD Paroxysmal Cold
Blood Product Utilization A Mythbusters! Style Review. Amanda Haynes, DO 4/28/18
 Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol
 Blood Transfusion Routine Investigations ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol Full Group & Screen 2ml EDTA Can be stored at 2-8C
Blood Transfusion Routine Investigations ALL Blood Transfusion samples must be hand-written in accordance with the Trust's Blood Administration Protocol Full Group & Screen 2ml EDTA Can be stored at 2-8C
HENOCH SCHÖNLEIN PURPURA (VASCULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests (SC)
 IN CHILDREN Single choice tests (SC)") HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
HEMORRHAGIC DISORDERS
 XIII HEMORRHAGIC DISORDERS Lawrence L. K. Leung, M.D. Approach to Patients with Hemorrhagic Disorders Whereas many healthy people consider their bleeding and bruising excessive, patients with underlying
XIII HEMORRHAGIC DISORDERS Lawrence L. K. Leung, M.D. Approach to Patients with Hemorrhagic Disorders Whereas many healthy people consider their bleeding and bruising excessive, patients with underlying
Acute Immune Thrombocytopenic Purpura (ITP) in Childhood
 in Childhood") Acute Immune Thrombocytopenic Purpura (ITP) in Childhood Guideline developed by Robert Saylors, MD, in collaboration with the ANGELS team. Last reviewed by Robert Saylors, MD September 22, 2016. Key Points
Acute Immune Thrombocytopenic Purpura (ITP) in Childhood Guideline developed by Robert Saylors, MD, in collaboration with the ANGELS team. Last reviewed by Robert Saylors, MD September 22, 2016. Key Points
Pediatric Bleeding Disorders and Thrombocytopenia. David Simon, MD Pediatric Hematology/Oncology Kaiser Permanente Downey Medical Center
 Pediatric Bleeding Disorders and Thrombocytopenia David Simon, MD Pediatric Hematology/Oncology Kaiser Permanente Downey Medical Center 1 2 Case Presentations Case 1 12 month old male, no personal or family
Pediatric Bleeding Disorders and Thrombocytopenia David Simon, MD Pediatric Hematology/Oncology Kaiser Permanente Downey Medical Center 1 2 Case Presentations Case 1 12 month old male, no personal or family
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS TABLE OF RECOMMENDED TESTS. Type of Reaction Presentation Recommended Tests Follow-up Tests
 Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Wiskott-Aldrich Syndrome
 chapter 7 Wiskott-Aldrich Syndrome Wiskott-Aldrich syndrome is a primary immunodeficiency disease involving both T- and B-lymphocytes. In addition, the blood cells that help control bleeding, called platelets
chapter 7 Wiskott-Aldrich Syndrome Wiskott-Aldrich syndrome is a primary immunodeficiency disease involving both T- and B-lymphocytes. In addition, the blood cells that help control bleeding, called platelets
thrombopoietin receptor agonists and University of Washington January 13, 2012
 Tickle me eltrombopag: thrombopoietin receptor agonists and the regulation of platelet production Manoj Menon University of Washington January 13, 2012 Outline Clinical case Pathophysiology of ITP Therapeutic
Tickle me eltrombopag: thrombopoietin receptor agonists and the regulation of platelet production Manoj Menon University of Washington January 13, 2012 Outline Clinical case Pathophysiology of ITP Therapeutic
Jovona Powelson, B.S. MLT (ASCP) Director of Laboratories
 Director of Laboratories") Jovona Powelson, B.S. MLT (ASCP) Director of Laboratories Blood Products From the Donor to You Objectives Deliver a brief virtual tour of a blood center. Describe the number of donors needed to meet the
Jovona Powelson, B.S. MLT (ASCP) Director of Laboratories Blood Products From the Donor to You Objectives Deliver a brief virtual tour of a blood center. Describe the number of donors needed to meet the
CASE STUDIES IN CLINICAL APPLICATIONS OF THERAPEUTIC PLASMA EXCHANGE
 CASE STUDIES IN CLINICAL APPLICATIONS OF THERAPEUTIC PLASMA EXCHANGE Eric Rosa, MLS (ASCP) CM Medical Laboratory Scientist Transfusion Service April 18, 2018 Objectives Explain the process of a therapeutic
CASE STUDIES IN CLINICAL APPLICATIONS OF THERAPEUTIC PLASMA EXCHANGE Eric Rosa, MLS (ASCP) CM Medical Laboratory Scientist Transfusion Service April 18, 2018 Objectives Explain the process of a therapeutic
PROMACTA (eltrombopag olamine) oral tablet and oral suspension
 oral tablet and oral suspension") PROMACTA (eltrombopag olamine) oral tablet and oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
PROMACTA (eltrombopag olamine) oral tablet and oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Anemia (3).ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh
.ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh") Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Idiopathic Thrombocytopenic Purpura
 Idiopathic Thrombocytopenic Purpura Title of Guideline Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of idiopathic thrombocytopenic purpura Dr S Stokley, Consultant
Idiopathic Thrombocytopenic Purpura Title of Guideline Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of idiopathic thrombocytopenic purpura Dr S Stokley, Consultant
Blood Components Transfusion Criteria
 Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
What should I discuss with my health care provider before taking eltrombopag?
 1 of 6 6/10/2016 3:57 PM Generic Name: eltrombopag (el TROM boe pag) Brand Name: Promacta What is eltrombopag? Eltrombopag is a man-made form of a protein that increases production of platelets (blood-clotting
1 of 6 6/10/2016 3:57 PM Generic Name: eltrombopag (el TROM boe pag) Brand Name: Promacta What is eltrombopag? Eltrombopag is a man-made form of a protein that increases production of platelets (blood-clotting
Transfusion Medicine Potpourri. BUMC - Phoenix Internal Medicine Residents September 29, 2015
 Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Elements for a Public Summary
 VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Nanogam is intended to be used for the treatment of diseases in patients who are suffering from a shortage of immunoglobulins
VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Nanogam is intended to be used for the treatment of diseases in patients who are suffering from a shortage of immunoglobulins
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Immune Thrombocytopenic Purpura (ITP)
") Patient information Immune Thrombocytopenic Purpura Immune Thrombocytopenic Purpura (ITP) This leaflet is for adult patients diagnosed with Immune Thrombocytopenic Purpura also known as Immune Thrombocytopenia
Patient information Immune Thrombocytopenic Purpura Immune Thrombocytopenic Purpura (ITP) This leaflet is for adult patients diagnosed with Immune Thrombocytopenic Purpura also known as Immune Thrombocytopenia
NEOFEN 60 mg suppository
 PACKAGE LEAFLET: INFORMATION FOR THE USER NEOFEN 60 mg suppository IBUPROFEN This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for a medicine, which outlines
PACKAGE LEAFLET: INFORMATION FOR THE USER NEOFEN 60 mg suppository IBUPROFEN This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for a medicine, which outlines