PMTCT UPDATE. AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM
|
|
|
- Arnold Bates
- 5 years ago
- Views:
Transcription
1 PMTCT UPDATE AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM
2 Outline Background Risk of MTCT Historical ARV interventions SA PMTCT program Rationale for changes Latest guidelines Expected outcomes
3 Background In 2009, children became newly infected with HIV globally and An estimated pregnant women died because of HIV. In contrast, in high-income countries the number of new HIV infections among children and maternal and child deaths due to HIV was virtually zero.
4 Progress in PMTCT- UNAIDS As of December 2012, over pregnant women living with HIV globally received ARV prophylaxis or treatment. Coverage of antiretroviral programmes for PMTCT (excluding the less-effective sd NVP regimen) increased from 57% (51 64%) in 2011 to 63% (57 70%) in Among pregnant women who needed antiretroviral therapy for their own health in 2012, 58% received HIV treatment lower than the 65% (61 70%) treatment coverage for adults overall.
5 Pmtct progress As a result of scaled-up HIV prevention services, the annual number of newly infected children in 2012 was ( ) in low- and middleincome countries, 35% lower than in 2009 From 2001 to 2012, there was a 52% decline in new HIV infections among children. Expanded access to services to PMTCT protected more than children from acquiring HIV from 2009 to The number of women newly infected with HIV declined by 44% from 2009 to 2012 in Ghana, by 23% in Uganda and by 21% in South Africa
6 Key elements of eliminating new HIV infections among children and keeping their mothers alive The Global Plan towards the elimination of new infections among children by 2015 and keeping their mothers alive recommends a set of priority actions under four key programmatic components: 1. Preventing new HIV infections among women of reproductive age. 2. Helping women living with HIV avoid unintended pregnancies. 3. Ensuring that pregnant women have access to HIV testing and counselling; and that those who test positive have access to antiretroviral medicines to prevent transmission during pregnancy, delivery or breastfeeding. 4. Providing HIV care, treatment and support for women, children living with HIV and their families. The Global Plan prioritizes scale-up in 22 priority countries that collectively account for almost 90% of pregnant women living with HIV
7 2011 UN Political Declaration on HIV/AIDS Targets and elimination commitments 1. Reduce sexual transmission by 50% by Reduce transmission of HIV among people who inject drugs by 50% by 2015 Eliminate new HIV infections among children by 2015 and substantially reduce AIDS-related maternal deaths Reach 15 million people living with HIV with lifesaving antiretroviral treatment by Reduce tuberculosis deaths in people living with HIV by 50% by Close the global AIDS resource gap by 2015 and reach annual global investment of US$ billion in low- and middle-income countries 7. Eliminate gender inequalities and gender-based abuse and violence and increase the capacity of women and girls to protect themselves from HIV 8. Eliminate stigma and discrimination against people living with and affected by HIV through promotion of laws and policies that ensure the full realization of all human rights and fundamental freedoms 9. Eliminate HIV-related restrictions on entry, stay and residence 10. Eliminate parallel systems for HIV-related services to strengthen integration of the AIDS response in global health and development efforts
8 If 90% of HIV positive pregnant women received combined ARV (50% started during the pregnancy and 40% started ART before the pregnancy) and 100% of those women received prophylaxis during breastfeeding HIV incidence was reduced by 50% among reproductive age women, and women living with HIV were able to meet their family planning needs the reduction in new child infections would still only reach an 83% reduction from 2009 levels in 2015.
9 Closer home There were approximately 34 [ ] million people living with HIV in Sub-Saharan Africa is the most affected region, with nearly 1 in every 20 adults living with HIV. (69% of all people living with HIV are living in this region). A s HIV epide i e ai s the iggest i the world, with an estimated 5.6 million HIV-positive people as of (This exceeds the number of people living with HIV in the entire Asian region).
10 2012

11

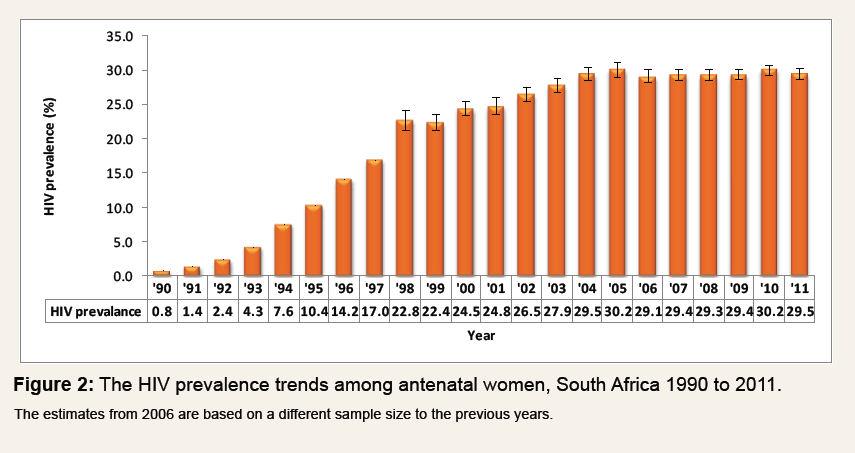
12 KZN PMTCT ANTENATAL HIV PREVALENCE, % 35% 41% 39% 25% 33% 35% 40% 38% 36% 42%
 Labor and Delivery Late Antenatal (36 wks to labor) 0% 20% 40% 60% 80% Proportion of infections")
13 Timing of MTCT (no intervention) Early Postpartum (0-6 months) Early Antenatal (<36 wks) Late Postpartum (6-24 months) Labor and Delivery Late Antenatal (36 wks to labor) 0% 20% 40% 60% 80% Proportion of infections 100%
14 Completed Trials: Focused on Prevention AP/IP Transmission AP 14 wks IP 28 wks 36 wks PP (baby, mother or both) 3d to 1 wk 6 wks 076 NonBF Thai (Harvard) NonBF Thai (Harvard) NonBF Thai (Harvard), BMS NonBF IvC (ANRS), PETRA, Thai (Harvard) BF/NonBF Thai (CDC), IvC (CDC) NonBF/BF PETRA, 012, SAINT BF PETRA BF AP: Minimum duration? Is it needed? IP: Work alone? PP: Minimal duration? Is it needed?
15 What did we know then? Perinatal HIV Clinical Trial Results U.S. AZT Trial ACTG % reduction in transmission 1998 Thai Bangkok short AP/IP AZT trial 50% reduction in transmission 1998 Cote d Ivoi e sho t AP/IP AZT trials 37% reduction in transmission (breastfeeding) 1999 PETRA AZT/3TC trial (6 wk results) 50% reduction with longest arm. 38% reduction with the IP/PP arm 2004 Thailand PHPT <2% AZT + NVP 2003 DITRAME % TR with AZT/3TC & IP/PP NVP 2002 Cote d Ivoi e DIT AME + 6.2% TR with AZT & IP/PP NVP 2000 Thailand Long vs short AZT regimens 4% TR in LL (non BF) 1999 Uganda 2-dose IP/PP NVP trial (HIVNET 012) 47% reduction in transmission (breastfeeding)
16 Evolvement of National PMTCT programme PMTCT April 2004 pilot sites of sd NVP and subsequently countrywide sd NVP 50%reduction intrapartum, overall transmission 14% ARV roll out introduced Feb pregn women <200 for HAART, others for sd NVP Scale up 2009 HAART for those <200 and the rest AZT from 28wks Revised in 2010 cut off for pregn women=cd 4 of 350 and AZT started at 14wks (5% MTCT) Amendment in April substitution of NVP with EFV April 2013 FDC for all infected (lifelong or until end of b/feeding)
17 /2010 ART eligible CD < 00 o 00 o <350 with WHO stage 4 ART eligible CD stage 3 or 4 0 o WHO If not ARV eligible: Option A: same as 2006, but start - AZT from 28wks + sd-nvp + AZT 3TC during labour and delivery Option B: Maternal 3 drug regimen + AZT + 3TC for 7 days postpartum Infant = AZT syrup for 1wk or 4 wks Infant 4 wks of AZT for all if maternal therapy <28wks regardless of maternal therapy No recommendation for mom or i fa t A V s if o eastfeedi g Mate al a d i fa t A V s if breastfeeding o
18 Why 350 Accounts for 40% of pregn HIV infected women Accounts for >75% of MTCT risk Accounts for >80% of pp transmission Accounts for 85% of maternal deaths within 2yrs of delivery Strong benefit for PMTCT during AN, intra and during b/feeding

19
20 OPTION B+ rationale Full integration and Simplification at the Primary Health Care Level Increased country readiness and experience Lower cost of drugs 3-in-1 intervention of PMTCT, treatment, and t eat e t as p eve tio.
21 New Guidelines Introduced 1st April 2013 Key changes: Prioritising of pregnant and breast feeding women FDC Phasing out of pre ART literacy classes Initiation of HAART as soon as diagnosis made
22 IMPLEMENTING NEW GUIDELINES
23 ALL WOMEN IN THE REPRODUCTIVE AGE GROUP Goals of interventions: Improve the quality of sexual and reproductive health services Improve access to family planning services Improve access to safer sex options Prevent transmission of HIV infection Improve access to HCT services to know HIV status
24 During pregnancy All women presenting to ANC must be seen Book early (<14 weeks) Group pre test counseling, Individual testing, and Individual post test counseling
25 ANTENATAL CARE Goals of interventions: I p ove the uality of the othe s health a d p eve t o tality Identify women who are HIV-positive including those who may seroconvert during pregnancy Ensure ALL women enter the PMTCT programme If HIV-infected then require prompt provision of ARVs and further counselling If HIV-uninfected require specific counselling and advice on repeat testing every 3 months after a negative test, and/or at 32 weeks, labour and through breastfeeding every 3 months ALL women to have TB screening Prevent mother-to-child transmission of HIV Provide ART, as soon as HIV positive status known, in pregnancy for maternal health and to reduce HIV transmission to the baby
26 LABOUR AND DELIVERY Goals of interventions: Provide HIV counselling and testing services to all women with unknown status Identify HIV-positive women Provide adequate PMTCT coverage Screen for TB in all women irrespective of HIV-status Continuity of care with prophylactic and treatment antiretroviral regimens Initiate neonates born to HIV-positive mothers with antiretroviral prophylaxis immediately at birth Establish safe infant feeding practices supporting exclusive breastfeeding and kangaroo mother care for all mothers and infants
27 POSTNATAL FOLLOW-UP OF MOTHER AND INFANT Goals of interventions: MOTHER: Provide follow-up post-partum care including a postnatal visit within 3 6 days for mother and baby I p ove the uality of the othe s health a d edu e o tality y i ludi g family planning counselling and cervical cancer screening where applicable Provide post-exposure prophylaxis of HIV for HIV-exposed infants Screen and where indicated exclude TB in mothers and infants Reduce postnatal HIV transmission through breastfeeding INFANT: Identify all HIV-exposed infants as early. - PCR HIV test for all symptomatic infants* anytime after birth and at 6 weeks (for asymptomatic infants) at routine EPI 6 week visit. (* Symptomatic Infants any infants displaying the following: failing to thrive (includes LBW), haematological abnormality like anaemia or thrombocytopaenia, congenital pneumonia, pneumonia, hepatosplenomegaly, extensive oral candidiasis, significant lymphadenopathy, any OIs) Identify all HIV-infected infants and start ART promptly (within 7 days)
28 Infants All infants born to HIV positive mothers: - start NVP as soon after birth as possible (within 72 hours postdelivery) and continue for 6 weeks. Infants of HIV infected women not on ART (treatment or prophylaxis) who are breastfeeding should continue daily NVP (ie beyond 6weeks) until one week after cessation of breast feeding.
29 Infant testing All HIV-exposed infants not on ART should have a rapid test at 18 months of age to confirm HIV status conferred by the 6week PCR test and 6 weeks post breast feeding test. All HIV-infected individuals should have provision of TB screening, INH prophylaxis, CTX prophylaxis, nutritional and psychosocial support, cervical cancer screening, family planning options, monitoring of CD4 cell count and, clinical staging. Mothers of unknown HIV status or who are HIV negative should be tested for HIV test at 6 weeks, 3 months, 9 months and one year postpartum, particularly if they are breast feeding. Note at initial PICT in the ANC, mothers would be consenting once for the protocol of initial and repeated HIV testing throughout HIV exposure so as to ensure that this is efficiently done without any requirement for further counselling unless indicated.
30 Figure 2: PMTCT Algorithm 1: for all women who are newly diagnosed as HIV positive anytime during pregnancy AND women who enter ANC with known HIV positive status and not yet on ART. First antenatal visit : HIV-positive not on ART (known and newly diagnosed) History & clinical assessment including for TB & WHO staging, Bloods sent for creatinine, CD4 If no active psychiatric illness or history of renal disease If active psychiatric illness or history of renal disease Start AZT 300mg same day (provided Hb >7g/dL) Start FDC (TDF, FTC/3TC, EFV) same day 1 week later : Review results of CD4, serum creatinine If se u eati i e 8 µ ol/l Check CD4 counts, WHO staging CD 0 o stage / CD4>350 or stage 1/2 Continue FDC as lifelong treatment forfurther management of pregnant women on AZT see figure 3 If serum creatinine >85 µmol/l: see Figure 4 Continue FDC as prophylaxis through antenatal, labour and delivery, postnatal till one week after complete cessation of breastfeeding
31 Figure 3 : PMTCT algorithm 2: Initiation of antiretrovirals during pregnancy in women with active psychiatric illness or history of renal disease If active psychiatric illness or history of renal disease Start AZT 300mg same day History, clinical assessment, WHO staging Bloods sent for serum creatinine, CD4 Routine antenatal care (including urine dipstix, Hb, RPR) If serum creatinine > 85 µmol/l: see Figure 4 1 week later Review results of CD4, serum creatinine If se u eati i e 8 µ ol/l Check CD4 counts, WHO staging CD 0 o stage / CD4>350 or stage 1/2 Requires alternate triple-drug regimen for lifelong treatment per adult guidelines TDF+ FTC+ NVP Use LPV/RTV in women with CD4 counts > 250cells/mm3 Continue AZT prophylaxis throughout pregnancy Intrapartum: Provide AZT 3 hourly during labour, Stat Dose NVP + TDF/FTC
32 PMTCT algorithm 3: Initiation of antiretrovirals during pregnancy in women with serum creatinine > 85 µmol/l: Check CD4 counts, WHO staging CD 0 o stage / CD4>350 or stage 1/2 treatment per adult guidelines: AZT+ 3TC+ EFV If haemoglobin <7g/dl AZT is contraindicated. Use ABC or D4T instead of AZT. Requires alternate triple-drug regimen for lifelong Continue AZT prophylaxis throughout pregnancy Intrapartum: Provide AZT 3 hourly during labour, STAT dose : NVP + TDF/FTC
33 PMTCT Algorithm 4: for all women who are newly diagnosed any time during the postnatal period. ostnatal visit: newly diagnosed HIV positive: History & clinical assessment including for TB & WHO staging, Bloods sent for creatinine, CD4 any time during the post natal period see algorithm 1 for further managmeent of mother. If no active psychiatric illness or history of nal disease: Start FDC (TDF, FTC/3TC, EFV) same day and Check status of infant feeding, Check baby HIV status (PCR) Return in 1 week to review results If currently breastfeeding the baby Check baby HIV status (PCR test before 18 months, and rapid HIV test Infant to be given NVP syrup for 7 days and after 18 months); Maternal bloods sent for creatinine, CD4, assess return for PCR test results within 7 days active psychiatric illness. for In case of exposure to BF at Baby PCR Negative: if PCR has done anytime before 6 weeks, a negative, please repeat PCR at 6 Baby PCR Positive:initiate treatm FDC (TDF, FTC/3TC, EFV) same day Start 1 week later : Review results of Maternal CD4, serum creatinine If se u eati i e 8 µ ol/l Check CD4 counts, WHO staging CD 0 o stage / CD4>350 or stage 1/2 Continue FDC as lifelong treatment Baby PCR Positive: initiate Treatment Baby PCR Negative: Continue NVP for 6 weeks If serum creatinine >85 µmol/l: see Figure 4 Continue FDC as prophylaxis through postnatal till one week after complete cessation of breastfeeding
34 HIV -ve Women who test HIV-negative anytime during antenatal, labour or postnatal periods are still considered part of the PMTCT programme and should receive post-test counselling and counselling on risk reduction interventions including involvement of partners or spouses, focusing mainly on how to maintain their HIVnegative status. They should continue to receive routine antenatal care, and should be encouraged to use condoms. They should be offered a repeat HIV test 12 weeks after the initial HIV test is negative and/or at 32 weeks or later gestation periods or in the labour ward, at the 6 week post natal visit, at 3, 6 and 12 months during breast feeding to detect those who may have sero-converted during pregnancy. They should have a symptom screen for TB at each visit.
35 Refusal / unbooked Women who choose not to be tested should e eive i dividual postefusal ou selli g a d e offe ed HIV testi g at eve y su se ue t visit i a non-coercive manner during the antenatal period. They should also be offered an HIV test at the onset of labour; if this is not possible, they should be offered testing shortly after childbirth. They should have a symptom screen for TB at each visit. Women who initially test negative and subsequently test positive during pregnancy should be initiated on FDC on same day of diagnosis. Further management as per figure 2 on page 8. Unbooked women reporting in labour should be counselled and tested for HIV during the first stage of labour, and if positive given a single dose of NVP and TDF and FTC and 3 hourly AZT until delivery. Postdelivery, start FDC and do routine tests (creatinine and CD4) and manage as per figure 2 on page 8.
36 For women taking Monitoring if on lifelong therapy TDF+3TC/FTC+EFV(FDC) Creatinine at 3, 6 and 12 months post-initiation Viral Load at 6 and 12 months post-initiation; CD4 at 12 months post-initiation AZT only Other triple-drug regiments Per adult ARV guidelines Monitoring if on prophylaxis only Creatinine at 3, 6 and 12 months post-initiation Haemoglobin 1, 2, 3 and 6 months post-initiation
37 REGIMENS Maternal regimens Woman 1st antental visit All women at first antenatal visit (any gestational age) Regimen FDC initiated immediately Continue the ART regimen If the woman is on a compatible regimen (EFV, 3TC TDF) change to FDC nd 2 antenatal visit (1 week later) Creatinine 85µmol/l Continue FDC Any CD4 cell count Comment If there is a contraindication to the FDC: Start AZT immediately and review within a week. (see figure 2algorithm) Currently on lifelong ART Check a VL when pregnancy diagnosed Creatinine > 85 µ mol/l TDF contraindicated (renal disease) If haemoglobin <7g/dl AZT is contraindicated. Use D4T instead of AZT. Refer for investigation for cause of renal disease Contraindication to EFV (active psychiatric illness) CD4 350cells/mm3 Contraindication to EFV (active psychiatric illness) CD4 > 350cells/mm3 AZT + 3TC + EFV TDF + FTC + NVP Substitute LPV/RTV for NVP in women with CD4 counts > 250cells/mm3 AZT in pregnancy sdnvp + sd TDF + FTC and AZT 3hrly in labour Labour Unbooked and presents in labour and tests HIV positive sdnvp + sd TDF + FTC and AZT 3hrly in labour start FDC after delivery if woman will breast feed Assess maternal ART eligibility before discharge
38 Infant Mother on lifelong ART or antenatal prophylaxis received (including TDF + 3TC/FTC + EFV or AZT) Mother did not get any ART before or during delivery and tests HIV positive post delivery Unknown maternal status because orphaned or abandoned Mother on AZT regimen (due to any contraindication to the FDC regimen) 1. Infant regimens Regimen NVP at birth and then daily for 6 weeks Comment If mother is breast feeding and not virally suppressed e.g. late booking or AZT mono-therapy continue NVP for infant throughout breast feeding until one week post cessation of breastfeeding, NVP as soon as possible and daily for 6 weeks Assess ART eligibility as soon as possible Give NVP immediately* Test infant with rapid HIV test. If positive continue NVP for 6 weeks. If negative discontinue NVP NVP at birth and then daily for 6 weeks. Follow up 6 week HIV DNA PCR Test infant with 6 week DNA PCR test. If negative and breastfeeding continue NVP till one week after complete cessation of breastfeeding * If rapid HIV test can be done within 2 hours, then wait for HIV result before commencing NVP
39 ARV Adult Dosing Guide Drug TDF (Tenofovir) Dosage 300mg daily d4t (Stavudine) 30mg 12hrly po 3TC (Lamivudine) FTC (Emtracitabine) NVP (Nevirapine) EFV (Efavirenz) 300mg daily 200mg daily 200mg dly po X 2 weeks then 200mg 12 hourly po For PMTCT purposes single dose (sdnvp) is used as a 200mg tablet given once. 600mg nocte Aluvia (lopinavir 200mg /ritonavir 50mg) 2 tabs 12 hourly (Lop400mg/Rit100mg) AZT (Zidovudine) 300mg 12 hourly po Notes Tenofovir is contraindicated if serum creatinine >85µmol/L during pregnancy (or creatinine clearance of <50ml/min in non-pregnant adults) All adult patients now receive 30mg regardless of weight Should be used with caution with TB treatment Avoid NVP if CD4 count >250cells/mm3 Avoid if active psychiatric illness Preferably taken with food. Boosting required with TB treatment Avoid if severe anaemia (Hb <8g/dl)
40 Breastfeeding Each pregnant woman should receive at least four antenatal counselling sessions on infant feeding. At every antenatal visit, HIV-negative women or women of unknown HIV status should be advised to exclusively breastfeed their babies during the first 6 months of life and encouraged to continue breastfeeding for up to 2 years and beyond. Every effort should be made to test all pregnant and breastfeeding women for HIV as outlined in the testing section of this document. Pregnant HIV negative women or women of unknown HIV status should be counselled to avoid mixed feeding their infants during their first six months of life as exclusive breastfeeding improves child survival.
41 Breastfeeding women living with HIV are advised to use antiretroviral medicines when breastfeeding their newborns. In 2012, antiretroviral coverage was substantially lower during the breastfeeding period (49%) than during pregnancy and delivery (62%). It is now estimated that half of all new episodes of HIV transmission to children occur during the breastfeeding period when the majority of lactating women are not receiving the prophylaxis necessary to prevent HIV transmission
42 HIV and maternal health / deaths

43 Global Map Depiction of Maternal Mortality Ratios, 2005 Map by the World Bank, based on data from WHO/UNICEF/UNFPA/World Bank 2007.Note: The regions exclude high income countries.
44 Saving Mothers Report Big m s ed co nd xn A EM H H PT N PR I PR S
45 CAUSES OF DEATH HIV POS v/s HIV NEG A EM H BS O H PT D /O PC P B PT PN EU M PR S POS NEG
46 Institutional mortality ratio for HIV 6x higher!! there were maternal deaths in SA. 80% were tested for HIV (of which 70% were infected) The Institutional MMR was / live births for HIV infected women compared to 75.46/ live births HIV uninfected women
47 Comparison of HIV status and causes of maternal death (using estimated IMMR per live births) Cause of death* HIV-negative Medical and surgical 11.5 disorders NPRIs 6.6 HIV-positive Unknown Ectopic pregnancy Miscarriage Hyperemesis gravidarum Anaesthetic complications Embolism Acute collapse, cause unknown Unknown Pregnancy-related sepsis Obstetric haemorrhage Hypertension Total 74.4 NPRI = non-pregnancy-related infection.
48 MORBIDITY For every death, there is 5-6x more morbidity (Severe acute maternal mortality underrepresented) mainly infective, including fever, endometritis, wound sepsis, etc However, immr higher in HIV infected even for non-infective causes
49 HIV status, HIV status n (%) HIV-negative (24.0) HIV-positive not requiring HAART 949 (19.5) AIDS not receiving HAART 938 (19.3) AIDS receiving HAART 882 (18.1) Declined 39 (0.8) Unknown 992 (20.4) HAART = highly active antiretroviral therapy. Probable cause of death (?? Other causes) (?late presentation) (?complications of ARV)
 APPEARS TO HAVE")
50 immr and HIV status (? Effect of HAART) APPEARS TO HAVE DECREASED BY 13%
51 A a d MDG s 1. To eradicate extreme poverty and hunger 2. To achieve universal primary education 3. To promote gender equality and empower women 4. To reduce child mortality 5. To improve maternal health 6. To combat HIV/AIDS, malaria and other diseases 7. To ensure environmental sustainability 8. To develop a global partnership for development between 1998 and 2007, the maternal mortality rate leapt from 150 to 625 deaths for each 100,000 live births. That means South Africa, sub- Saharan African's economic powerhouse, has no hope of meeting the U.N. MDG that require 38 deaths per 100,000 births by 2015
52 End
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM
 Dept of O+G NRMSM") Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
Updates on Revised Antiretroviral Treatment Guidelines Overview 27 March 2013
 Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Figure S1: Overview of PMTCT Options A and B. Prevention of Mother to Child HIV Transmission (PMTCT)
") Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV
 TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
Update on global guidelines. and emerging issues on perinatal HIV prevention. WHO 2013 Consolidated ARV Guidelines
 WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive:
 Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive: Rationale for the call to action, progress to date and dealing with realities Rene Ekpini, MD, MPH Senior Adviser,
Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive: Rationale for the call to action, progress to date and dealing with realities Rene Ekpini, MD, MPH Senior Adviser,
Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013
 Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013 The following document highlights the changes National department of Health ARV treatment guidelines
Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013 The following document highlights the changes National department of Health ARV treatment guidelines
The New National Guidelines. Feeding in the Context of HIV. Dr. Godfrey Esiru; National PMTCT Coordinator
 The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
hiv/aids Programme Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants
 hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE
 UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
Paediatric ART: eligibility criteria and first line regimens. (revised) Dave le Roux 13 August 2016
 Dave le Roux 13 August 2016") Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
The NEW ARV Guidelines FAQs
 The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
DEPARTMENT. Treatment Recommendations for. Pregnant and Breastfeeding Women: Critical Issues Consolidated ARV Guidelines. Dr.
 2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Dr Wendy Mphatswe SA HIV Clinician s Society Meeting 15 July 2017 Overview 1. HIV epidemic 2. HIV response (Fast Track) 3. Goal of therapy in pregnant and breastfeeding women
Using new ARVs in pregnancy Dr Wendy Mphatswe SA HIV Clinician s Society Meeting 15 July 2017 Overview 1. HIV epidemic 2. HIV response (Fast Track) 3. Goal of therapy in pregnant and breastfeeding women
treatment during pregnancy and breastfeeding
 treatment during pregnancy and breastfeeding Topics covered Introduction. Preventing parent-to-child transmission. AZT as a single therapy. Treatment begun late in pregnancy. Nevirapine for mothers and
treatment during pregnancy and breastfeeding Topics covered Introduction. Preventing parent-to-child transmission. AZT as a single therapy. Treatment begun late in pregnancy. Nevirapine for mothers and
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20
 Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
Infant feeding in the ARV era. Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital
 Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
PMTCT Max Kroon Mowbray Maternity Hospital Division of Neonatal Medicine School of Child and Adolescent Health University of Cape Town
 PMTCT 2010 Max Kroon Mowbray Maternity Hospital Division of Neonatal Medicine School of Child and Adolescent Health University of Cape Town Prevention of Mother-To-Child Transmission of HIV or Prevention
PMTCT 2010 Max Kroon Mowbray Maternity Hospital Division of Neonatal Medicine School of Child and Adolescent Health University of Cape Town Prevention of Mother-To-Child Transmission of HIV or Prevention
Objectives. Outline. Section 1: Interaction between HIV and pregnancy. Effects of HIV on Pregnancy. Section 2: Mother-to-Child-Transmission (MTCT)
") Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps
 Appendix 4 Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps Lynne M. Mofenson, MD Eunice Kennedy Shriver National Institute of
Appendix 4 Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps Lynne M. Mofenson, MD Eunice Kennedy Shriver National Institute of
Outline. Aim with PMTCT. How are children transmitted. Prevention of mother-to-child transmission of HIV. How does HIV transmit to children?
 Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION
 Abst#_O_01 DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION Hadiza Khamofu, 1 Edward Oladele, 1 Uche Ralph-Opara,
Abst#_O_01 DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION Hadiza Khamofu, 1 Edward Oladele, 1 Uche Ralph-Opara,
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA. Date
 CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
Linkages between Sexual and Reproductive Health and HIV
 Linkages between Sexual and Reproductive Health and HIV Manjula Lusti-Narasimhan Department of Reproductive Health and Research World Health Organization The HIV pandemic 25 years 1981 2006 Rationale for
Linkages between Sexual and Reproductive Health and HIV Manjula Lusti-Narasimhan Department of Reproductive Health and Research World Health Organization The HIV pandemic 25 years 1981 2006 Rationale for
Mother to Child HIV Transmission
 Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
Elimination of mother to child transmission of HIV: is the end really in sight? Lisa L. Abuogi, MD University of Colorado, Denver Dec 3, 2014
 Elimination of mother to child transmission of HIV: is the end really in sight? Lisa L. Abuogi, MD University of Colorado, Denver Dec 3, 2014 Outline Background History of prevention of mother to child
Elimination of mother to child transmission of HIV: is the end really in sight? Lisa L. Abuogi, MD University of Colorado, Denver Dec 3, 2014 Outline Background History of prevention of mother to child
Elijah Paintsil, MD, FAAP
 Roadmap to elimination of mother-to-child transmission of HIV in Ghana by 2015 Towards HIV Free Generation Elijah Paintsil, MD, FAAP Assistant Professor of Pediatrics & Pharmacology Yale School of Medicine,
Roadmap to elimination of mother-to-child transmission of HIV in Ghana by 2015 Towards HIV Free Generation Elijah Paintsil, MD, FAAP Assistant Professor of Pediatrics & Pharmacology Yale School of Medicine,
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
HIV Infection in Pregnancy. Francis J. Ndowa WHO RHR/STI
 HIV Infection in Pregnancy Francis J. Ndowa WHO RHR/STI FJN_STI_2005 Department of reproductive health and research Département santé et recherche génésiques Session outline Effect of pregnancy on HIV
HIV Infection in Pregnancy Francis J. Ndowa WHO RHR/STI FJN_STI_2005 Department of reproductive health and research Département santé et recherche génésiques Session outline Effect of pregnancy on HIV
The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT
 The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT Peter McDermott Managing Director, CIFF 19 th Board meeting, Geneva 6 th May 2009 Investment Criteria Measurable...change
The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT Peter McDermott Managing Director, CIFF 19 th Board meeting, Geneva 6 th May 2009 Investment Criteria Measurable...change
XVII INTERNATIONAL AIDS CONFERENCE MEXICO CITY, 3-8 August 2008 SCALING-UP NATIONAL PMTCT PROGRAM
 XVII INTERNATIONAL AIDS CONFERENCE MEXICO CITY, 3-8 August 2008 SCALING-UP NATIONAL PMTCT PROGRAM Phasing more efficacious ARV regimen for PMTCT in resource limited setting Lessons Learned from RWANDA
XVII INTERNATIONAL AIDS CONFERENCE MEXICO CITY, 3-8 August 2008 SCALING-UP NATIONAL PMTCT PROGRAM Phasing more efficacious ARV regimen for PMTCT in resource limited setting Lessons Learned from RWANDA
PREVENT TRANSMISSION OF HIV/AIDS PREGNANT WOMEN : LITERATUR REVIEW
 PREVENT TRANSMISSION OF HIV/AIDS PREGNANT WOMEN : LITERATUR REVIEW *Nunung Nurhayati STIKep PPNI Jawa Barat, Bandung, West Java Indonesia Email: nunky_adzra@yahoo.com ABSTRACT Baby risk be infected HIV/AIDS
PREVENT TRANSMISSION OF HIV/AIDS PREGNANT WOMEN : LITERATUR REVIEW *Nunung Nurhayati STIKep PPNI Jawa Barat, Bandung, West Java Indonesia Email: nunky_adzra@yahoo.com ABSTRACT Baby risk be infected HIV/AIDS
Sexual and Reproductive Health and HIV. Dr. Rita Kabra Training course in Sexual and Reproductive Health Research Geneva 2012
 Sexual and Reproductive Health and HIV Dr. Rita Kabra Training course in Sexual and Reproductive Health Research Geneva 2012 Global estimates of HIV-(2009) People living with HIV 33.3 million [31.4 35.3
Sexual and Reproductive Health and HIV Dr. Rita Kabra Training course in Sexual and Reproductive Health Research Geneva 2012 Global estimates of HIV-(2009) People living with HIV 33.3 million [31.4 35.3
Infertility Treatment and HIV
 Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Discontinuation of cart postpartum in a high prevalence district of South Africa in 2014
 Claessens et al. Implementation Science 2014, 9:139 Implementation Science STUDY PROTOCOL Open Access Discontinuation of cart postpartum in a high prevalence district of South Africa in 2014 Lore Claessens
Claessens et al. Implementation Science 2014, 9:139 Implementation Science STUDY PROTOCOL Open Access Discontinuation of cart postpartum in a high prevalence district of South Africa in 2014 Lore Claessens
Progress & challenges in PMTCT: The unfinished agenda
 Progress & challenges in PMTCT: The unfinished agenda Dr Chewe Luo MMED (Paed); MTropPaed; PhD; FRCP Senior Adviser and Team Leader Country Programme Scale Up HIV Section, Programme Division UNICEF NY,
Progress & challenges in PMTCT: The unfinished agenda Dr Chewe Luo MMED (Paed); MTropPaed; PhD; FRCP Senior Adviser and Team Leader Country Programme Scale Up HIV Section, Programme Division UNICEF NY,
Scholars Research Library. Changing trends of HIV infection in children with relation to the ongoing PPTCT programme
 Journal of Microbiology and Biotechnology Research Scholars Research Library (http://scholarsresearchlibrary.com/archive.html) ISSN : 2231 3168 CODEN (USA) : JMBRB4 Changing trends of HIV infection in
Journal of Microbiology and Biotechnology Research Scholars Research Library (http://scholarsresearchlibrary.com/archive.html) ISSN : 2231 3168 CODEN (USA) : JMBRB4 Changing trends of HIV infection in
Malaysian Consensus Guidelines on Antiretroviral Therapy Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh
 Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
The elimination equation: understanding the path to an AIDS-free generation
 The elimination equation: understanding the path to an AIDS-free generation James McIntyre Anova Health Institute & School of Public Health & Family Medicine, University of Cape Town Elimination of perinatal
The elimination equation: understanding the path to an AIDS-free generation James McIntyre Anova Health Institute & School of Public Health & Family Medicine, University of Cape Town Elimination of perinatal
Prevention of HIV in infants and young children
 WHO/HIV/2002.08 Original: English Distr.: General Prevention of HIV in infants and young children A major public health problem HIV among children is a growing problem, particularly in the countries hardest
WHO/HIV/2002.08 Original: English Distr.: General Prevention of HIV in infants and young children A major public health problem HIV among children is a growing problem, particularly in the countries hardest
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT
 PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
Infant feeding and HIV Policy, Evidence and Hospital Challenges
 Infant feeding and HIV Policy, Evidence and Hospital Challenges Max Kroon MMH/SCAH MY BRIEF Overview of infant feeding within the PMTCT program including national policy, feeding choices & research evidence
Infant feeding and HIV Policy, Evidence and Hospital Challenges Max Kroon MMH/SCAH MY BRIEF Overview of infant feeding within the PMTCT program including national policy, feeding choices & research evidence
To provide you with the basic concepts of HIV prevention using HIV rapid tests combined with counselling.
 Module 2 Integration of HIV Rapid Testing in HIV Prevention and Treatment Programs Purpose Pre-requisite Modules Learning Objectives To provide you with the basic concepts of HIV prevention using HIV rapid
Module 2 Integration of HIV Rapid Testing in HIV Prevention and Treatment Programs Purpose Pre-requisite Modules Learning Objectives To provide you with the basic concepts of HIV prevention using HIV rapid
Scaling up priority HIV/AIDS interventions in the health sector
 TOWARDS UNIVERSAL ACCESS? Scaling up priority HIV/AIDS interventions in the health sector Yves Souteyrand, WHO October 2011 Towards universal access targets UN General Assembly High level Meeting June
TOWARDS UNIVERSAL ACCESS? Scaling up priority HIV/AIDS interventions in the health sector Yves Souteyrand, WHO October 2011 Towards universal access targets UN General Assembly High level Meeting June
Ending mother to child transmission through community action. Ngashi Ngongo, MD, MPH Senior Health Advisor UNICEF New York
 Ending mother to child transmission through community action Ngashi Ngongo, MD, MPH Senior Health Advisor UNICEF New York PRESENTATION OUTLINE An historical perspective Learning from previous public health
Ending mother to child transmission through community action Ngashi Ngongo, MD, MPH Senior Health Advisor UNICEF New York PRESENTATION OUTLINE An historical perspective Learning from previous public health
The Global Fund & UNICEF Partnership
 The Global Fund & UNICEF Partnership Prof Michel D. Kazatchkine Executive Director UNICEF Executive Board February 9 th, 2011 The Global Fund Millennium Development Goals 1. Eradicate extreme poverty and
The Global Fund & UNICEF Partnership Prof Michel D. Kazatchkine Executive Director UNICEF Executive Board February 9 th, 2011 The Global Fund Millennium Development Goals 1. Eradicate extreme poverty and
Phase II clinical trial TEmAA. Didier Koumavi EKOUEVI, MD PhD (Principal Investigator)
") The combination of Tenofovir-Emtricitabine (Truvada ): a new antiretroviral (ARV) regimen for the prevention of mother-to-child transmission of HIV-1 (PMTCT) in resource-limited settings Phase II clinical
The combination of Tenofovir-Emtricitabine (Truvada ): a new antiretroviral (ARV) regimen for the prevention of mother-to-child transmission of HIV-1 (PMTCT) in resource-limited settings Phase II clinical
Tunisian recommendations on ART : process and results
 Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and
, Children, Adolescents and") The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2015 (Amended Version) The Western Cape Consolidated
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2015 (Amended Version) The Western Cape Consolidated
Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive
 Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive DR. Nicholas Muraguri OGW, MD,MPH, MBA, PhD (c) Director, Global Plan Secretariat www.zero-hiv.org
Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive DR. Nicholas Muraguri OGW, MD,MPH, MBA, PhD (c) Director, Global Plan Secretariat www.zero-hiv.org
Breast Feeding for Women with HIV?
 Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
Adolescents Living with HIV
 Adolescents Living with HIV Gary Reubenson Polokwane 22 August 2015 Conflicts of Interest No relevant conflicts of interest to declare Acknowledgements Karl Technau Lee Fairlie Gill Sorour HIV Clinicians
Adolescents Living with HIV Gary Reubenson Polokwane 22 August 2015 Conflicts of Interest No relevant conflicts of interest to declare Acknowledgements Karl Technau Lee Fairlie Gill Sorour HIV Clinicians
Dr Graham P Taylor Reader in Communicable Diseases
 HIV in Pregnancy Joint RCOG/BHIVA Multidisciplinary Conference Dr Graham Taylor Imperial College London Friday 20 January 2012, Royal College of Obstetricians and Gynaecologist, London Prevention of post-partum
HIV in Pregnancy Joint RCOG/BHIVA Multidisciplinary Conference Dr Graham Taylor Imperial College London Friday 20 January 2012, Royal College of Obstetricians and Gynaecologist, London Prevention of post-partum
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and
, Children, Adolescents and") The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2018 (Amended Version) The Western Cape Consolidated
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2018 (Amended Version) The Western Cape Consolidated
Children and AIDS Fourth Stocktaking Report 2009
 Children and AIDS Fourth Stocktaking Report 2009 The The Fourth Fourth Stocktaking Stocktaking Report, Report, produced produced by by UNICEF, UNICEF, in in partnership partnership with with UNAIDS, UNAIDS,
Children and AIDS Fourth Stocktaking Report 2009 The The Fourth Fourth Stocktaking Stocktaking Report, Report, produced produced by by UNICEF, UNICEF, in in partnership partnership with with UNAIDS, UNAIDS,
The 2017 Namibia ART Guidelines. Tadesse T. Mekonen, MD, MPH, AAF-HIV
 The 2017 Namibia ART Guidelines Tadesse T. Mekonen, MD, MPH, AAF-HIV Q1-Table 1 List at least four key new recommendations in the 2017 Namibian ART Guidelines Q2-Table-2 46yo, Male, on AZT/TDF/FTC/ATVr
The 2017 Namibia ART Guidelines Tadesse T. Mekonen, MD, MPH, AAF-HIV Q1-Table 1 List at least four key new recommendations in the 2017 Namibian ART Guidelines Q2-Table-2 46yo, Male, on AZT/TDF/FTC/ATVr
HIV. Transmission modes. Transmission modes in children. Prevention of mother-to-child transmission of HIV. HIV identified in 1983
 Prevention of mother-to-child transmission of HIV HIV identified in 1983 HIV AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia and wasting often combined Retrospectively,
Prevention of mother-to-child transmission of HIV HIV identified in 1983 HIV AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia and wasting often combined Retrospectively,
Challenges of HIV drug resistance in resource-limited settings
 Challenges of HIV drug resistance in resource-limited settings Marie-Louise Newell Professor of Global Health Faculty of Medicine and Faculty of Social and Human Sciences, University of Southampton, UK
Challenges of HIV drug resistance in resource-limited settings Marie-Louise Newell Professor of Global Health Faculty of Medicine and Faculty of Social and Human Sciences, University of Southampton, UK
ARV Consolidated Guidelines 2015
 ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
James McIntyre & Glenda Gray
 James McIntyre & Glenda Gray Thirty years of AIDS July 3, 1981 A generation in the shadow of AIDS... AIDS in South Africa First South African publication: 1983: two cases in homosexual men, both died in
James McIntyre & Glenda Gray Thirty years of AIDS July 3, 1981 A generation in the shadow of AIDS... AIDS in South Africa First South African publication: 1983: two cases in homosexual men, both died in
2013 progress report on the Global Plan
 2013 progress report on the Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive 210 000 the number of new HIV infections among children in (21
2013 progress report on the Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive 210 000 the number of new HIV infections among children in (21
Antiretroviral therapy for adults and adolescents KEY MESSAGES. HIV/AIDS Department BACKGROUND
 KEY MESSAGES New WHO Recommendations: Antiretroviral therapy for adults and adolescents The World Health Organization (WHO) is revising its guidelines on antiretroviral therapy (ART) for adults and adolescents.
KEY MESSAGES New WHO Recommendations: Antiretroviral therapy for adults and adolescents The World Health Organization (WHO) is revising its guidelines on antiretroviral therapy (ART) for adults and adolescents.
All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis. Against the motion
 All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis Against the motion Hermione Lyall Imperial Healthcare NHS Trust, London, UK Acknowledgements: Pat Tookey, Ali Judd, Claire
All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis Against the motion Hermione Lyall Imperial Healthcare NHS Trust, London, UK Acknowledgements: Pat Tookey, Ali Judd, Claire
Concept note. 1. Background and rationale
 Concept note Inter-Country Workshops for Strengthening Regional and National Human Capacity to Accelerate Scaling up of National PMTCT and Paediatric Care, Support and Treatment Programmes TOWARDS UNIVERSAL
Concept note Inter-Country Workshops for Strengthening Regional and National Human Capacity to Accelerate Scaling up of National PMTCT and Paediatric Care, Support and Treatment Programmes TOWARDS UNIVERSAL
Renewing Momentum in the fight against HIV/AIDS
 2011 marks 30 years since the first cases of AIDS were documented and the world has made incredible progress in its efforts to understand, prevent and treat this pandemic. Progress has been particularly
2011 marks 30 years since the first cases of AIDS were documented and the world has made incredible progress in its efforts to understand, prevent and treat this pandemic. Progress has been particularly
CCC ARV Dosing Recommendations for HIV-exposed infants Updated
 USERS NOTE: Please note this document does not provide guidance on overall decisionmaking regarding what medication(s) to use for HIV-exposed infants. This document is meant to facilitate ARV dosing for
USERS NOTE: Please note this document does not provide guidance on overall decisionmaking regarding what medication(s) to use for HIV-exposed infants. This document is meant to facilitate ARV dosing for
Prevention of Mother to Child Transmission of HIV: Our Experience in South India
 pg 62-66 Original Article Prevention of Mother to Child Transmission of HIV: Our Experience in South India Karthekeyani Vijaya 1, Alexander Glory 2, Solomon Eileen 3, Rao Sarita 4, Rao P.S.S.Sunder 5 1
pg 62-66 Original Article Prevention of Mother to Child Transmission of HIV: Our Experience in South India Karthekeyani Vijaya 1, Alexander Glory 2, Solomon Eileen 3, Rao Sarita 4, Rao P.S.S.Sunder 5 1
Update on PMTCT. African Health Profession Regulatory Collaborative for Nurses and Midwives. Johannesburg, Republic of South Africa, June 18-22, 2012
 PMTCT Update Update on PMTCT Margarett Davis, MD, MPH Chief, Maternal and Child Health Branch Division of Global HIV/AIDS Centers for Disease Control and Prevention (CDC) African Health Profession Regulatory
PMTCT Update Update on PMTCT Margarett Davis, MD, MPH Chief, Maternal and Child Health Branch Division of Global HIV/AIDS Centers for Disease Control and Prevention (CDC) African Health Profession Regulatory
Prevention of Mother-to-Child Transmission of HIV Infection
 HIV Curriculum for the Health Professional Prevention of Mother-to-Child Transmission of HIV Infection Michael A. Tolle, MD, MPH Daniel Dewey, MD Objectives 1. Describe the scope of mother-to-child transmission
HIV Curriculum for the Health Professional Prevention of Mother-to-Child Transmission of HIV Infection Michael A. Tolle, MD, MPH Daniel Dewey, MD Objectives 1. Describe the scope of mother-to-child transmission
SECTION WHAT PARLIAMENTARIANS CAN DO TO PREVENT PARENT-TO-CHILD TRANSMISSION OF HIV
 TO PREVENT PARENT-TO-CHILD TRANSMISSION OF HIV WHY PARENT-TO-CHILD TRANSMISSION? Some 800,000 children under the age of 15 contracted HIV in 2002, about 90 per cent through transmission from their mothers.
TO PREVENT PARENT-TO-CHILD TRANSMISSION OF HIV WHY PARENT-TO-CHILD TRANSMISSION? Some 800,000 children under the age of 15 contracted HIV in 2002, about 90 per cent through transmission from their mothers.
De la prévention à l élimination, le chemin parcouru en matière de transmission verticale. De la recherche aux recommandations OMS
 De la prévention à l élimination, le chemin parcouru en matière de transmission verticale De la recherche aux recommandations OMS 16 novembre, 2011 Pr François DABIS Bordeaux 1985 1997 (1) 1985 1997 (1)
De la prévention à l élimination, le chemin parcouru en matière de transmission verticale De la recherche aux recommandations OMS 16 novembre, 2011 Pr François DABIS Bordeaux 1985 1997 (1) 1985 1997 (1)
GLOBAL AIDS MONITORING REPORT
 KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
Treatment Optimization for EMTCT
 Treatment Optimization for EMTCT Dr Madeleine Muller With thanks to CN Mnyani and Linda-Gail Bekker SA HIV Clinician s Society Meeting 25 Nov 2017 Having children is one of the greatest joys and privileges
Treatment Optimization for EMTCT Dr Madeleine Muller With thanks to CN Mnyani and Linda-Gail Bekker SA HIV Clinician s Society Meeting 25 Nov 2017 Having children is one of the greatest joys and privileges
The Cumulative Incidence of HIV Infection in HIVexposed Infants with a Birth Weight of 1500g Receiving Breast Milk and Daily Nevirapine
 The Cumulative Incidence of HIV Infection in HIVexposed Infants with a Birth Weight of 1500g Receiving Breast Milk and Daily Nevirapine A retrospective, descriptive study conducted at Kalafong hospital,
The Cumulative Incidence of HIV Infection in HIVexposed Infants with a Birth Weight of 1500g Receiving Breast Milk and Daily Nevirapine A retrospective, descriptive study conducted at Kalafong hospital,
Elements of Reproductive Health
 SEXUAL& REPRODUCTIVE HEALTH and HIV/AIDS INTEGRATION: Issues for consideration Dr. Chris Baryomunsi, MP Parliament of Uganda Elements of Reproductive Health Safe motherhood Family Planning Prevention and
SEXUAL& REPRODUCTIVE HEALTH and HIV/AIDS INTEGRATION: Issues for consideration Dr. Chris Baryomunsi, MP Parliament of Uganda Elements of Reproductive Health Safe motherhood Family Planning Prevention and
Partnerships between UNAIDS and the Faith-Based Community
 Partnerships between UNAIDS and the Faith-Based Community Sally Smith- Partnership Adviser. Micah Network: Global Consultation-Churches Living with HIV Pattaya Thailand October 2008 UNAIDS Summary of 2008
Partnerships between UNAIDS and the Faith-Based Community Sally Smith- Partnership Adviser. Micah Network: Global Consultation-Churches Living with HIV Pattaya Thailand October 2008 UNAIDS Summary of 2008
Review of the Democratic Republic of the Congo (DRC) by the Committee on the Elimination of Discrimination Against Women (CEDAW)
 by the Committee on the Elimination of Discrimination Against Women (CEDAW)") Review of the Democratic Republic of the Congo (DRC) by the Committee on the Elimination of Discrimination Against Women (CEDAW) Submission: Elizabeth Glaser Pediatric AIDS Foundation June 2013 Introduction:
Review of the Democratic Republic of the Congo (DRC) by the Committee on the Elimination of Discrimination Against Women (CEDAW) Submission: Elizabeth Glaser Pediatric AIDS Foundation June 2013 Introduction:
1. Africa Centre for Health and Population Studies 2. London School of Hygiene and Tropical Medicine 3. University College London
 A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
Management of the HIV-Exposed Infant
 Management of the HIV-Exposed Infant Katherine Knapp, MD Medical Director, Perinatal Program Department of Infectious Diseases St. Jude Children s Research Hospital Disclosures No conflicts of interest
Management of the HIV-Exposed Infant Katherine Knapp, MD Medical Director, Perinatal Program Department of Infectious Diseases St. Jude Children s Research Hospital Disclosures No conflicts of interest
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
UPTAKE OF THE PREVENTION OF MOTHER- TO-CHILD-TRANSMISSION PROGRAMME AT A PRIMARY CARE LEVEL IN SEDIBENG DISTRICT
 UPTAKE OF THE PREVENTION OF MOTHER- TO-CHILD-TRANSMISSION PROGRAMME AT A PRIMARY CARE LEVEL IN SEDIBENG DISTRICT A Research Report Submitted to the Faculty of Health Sciences, University of the Witwatersrand
UPTAKE OF THE PREVENTION OF MOTHER- TO-CHILD-TRANSMISSION PROGRAMME AT A PRIMARY CARE LEVEL IN SEDIBENG DISTRICT A Research Report Submitted to the Faculty of Health Sciences, University of the Witwatersrand
TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES
 POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
HIV: A global perspective on epidemiology, diagnosis and prevention
 HIV: A global perspective on epidemiology, diagnosis and prevention Margaret McLees, M.D., DTMH Instructor, Division of Infectious Diseases Denver Health University of Colorado November 13, 2012 Outline
HIV: A global perspective on epidemiology, diagnosis and prevention Margaret McLees, M.D., DTMH Instructor, Division of Infectious Diseases Denver Health University of Colorado November 13, 2012 Outline
Clinical guidelines for antiretroviral management of HIV disease. Origins and history of the HIV epidemic
 Clinical guidelines for antiretroviral management of HIV disease Origins and history of the HIV epidemic Both known species of HIV, viz. HIV-1 and HIV-2 originated in Africa (HIV-1 from Central Africa
Clinical guidelines for antiretroviral management of HIV disease Origins and history of the HIV epidemic Both known species of HIV, viz. HIV-1 and HIV-2 originated in Africa (HIV-1 from Central Africa
Pediatric HIV Update NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
Technical Guidance Note for Global Fund HIV Proposals. TREATMENT - Antiretroviral Treatment-infants, children and adults
 Technical Guidance Note for Global Fund HIV Proposals TREATMENT - Antiretroviral Treatment-infants, children and adults May 2010 This technical brief is designed to provide key technical information to
Technical Guidance Note for Global Fund HIV Proposals TREATMENT - Antiretroviral Treatment-infants, children and adults May 2010 This technical brief is designed to provide key technical information to
Strategic use of antiretroviral drugs to prevent HIV transmission
 Strategic use of antiretroviral drugs to prevent HIV transmission 22th Tunisian Congress of Infectious Diseases 2nd Congress of Federation of Arab Societies of Clinical Microbiology and Infectious Diseases
Strategic use of antiretroviral drugs to prevent HIV transmission 22th Tunisian Congress of Infectious Diseases 2nd Congress of Federation of Arab Societies of Clinical Microbiology and Infectious Diseases
A Descriptive Study of Outcomes of Interventions to Prevent Mother to Child Transmission of HIV in Lusaka, Zambia
 ORIGINAL PAPER A Descriptive Study of Outcomes of Interventions to Prevent Mother to Child Transmission of HIV in Lusaka, Zambia Chibesa Shichitamba W, National Malaria Control Centre, Lusaka-Zambia ABSTRACT
ORIGINAL PAPER A Descriptive Study of Outcomes of Interventions to Prevent Mother to Child Transmission of HIV in Lusaka, Zambia Chibesa Shichitamba W, National Malaria Control Centre, Lusaka-Zambia ABSTRACT
HIV und AIDS- was gibt es Neues für die Arbeit vor Ort?
 HIV und AIDS- was gibt es Neues für die Arbeit vor Ort? Dr. med. Ralf Weigel Liverpool School of Tropical Medicine ralf.weigel@lstmed.ac.uk foring UPDATE 2017 Humanitäre Hilfe und Entwicklungszusammenarbeit
HIV und AIDS- was gibt es Neues für die Arbeit vor Ort? Dr. med. Ralf Weigel Liverpool School of Tropical Medicine ralf.weigel@lstmed.ac.uk foring UPDATE 2017 Humanitäre Hilfe und Entwicklungszusammenarbeit
2009 Revisions of WHO ART Guidelines. November 2009
 2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
Does screening of pregnant women prevent mother to child transmission of HIV? A study in nsukka urban area of Enugu State, Nigeria.
 Does screening of pregnant women prevent mother to child transmission of HIV? A study in nsukka urban area of Enugu State, Nigeria. *1 Momoh, M. A and **Ezugwuorie, O. J *Department of Pharmaceutics, Faculty
Does screening of pregnant women prevent mother to child transmission of HIV? A study in nsukka urban area of Enugu State, Nigeria. *1 Momoh, M. A and **Ezugwuorie, O. J *Department of Pharmaceutics, Faculty
2016 Perinatal Treatment Guidelines Update
 Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES?
 WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
INTERNAL QUESTIONS AND ANSWERS DRAFT
 WHO CONSOLIDATED GUIDELINES ON THE USE OF ANTIRETROVIRAL DRUGS FOR TREATING AND PREVENTING HIV INFECTION Background: INTERNAL QUESTIONS AND ANSWERS DRAFT At the end of 2012, 9.7 million people were receiving
WHO CONSOLIDATED GUIDELINES ON THE USE OF ANTIRETROVIRAL DRUGS FOR TREATING AND PREVENTING HIV INFECTION Background: INTERNAL QUESTIONS AND ANSWERS DRAFT At the end of 2012, 9.7 million people were receiving
Assessment of G8 Commitments on Maternal, Newborn and Child Health
 Assessment of G8 Commitments on Maternal, Newborn and Child Health Robin Lennox Researcher, G8 Research Group June 13, 2010 In January 2010, Canadian prime minister Stephen Harper announced that maternal,
Assessment of G8 Commitments on Maternal, Newborn and Child Health Robin Lennox Researcher, G8 Research Group June 13, 2010 In January 2010, Canadian prime minister Stephen Harper announced that maternal,
SPECIAL EVENT ON PHILANTHROPY AND THE GLOBAL PUBLIC HEALTH AGENDA. 23 February 2009, United Nations, New York Conference Room 2, 3:00 p.m. 6:00 p.m.
 SPECIAL EVENT ON PHILANTHROPY AND THE GLOBAL PUBLIC HEALTH AGENDA 23 February 2009, United Nations, New York Conference Room 2, 3:00 p.m. 6:00 p.m. ISSUES NOTE Improving the Health Outcomes of Women and
SPECIAL EVENT ON PHILANTHROPY AND THE GLOBAL PUBLIC HEALTH AGENDA 23 February 2009, United Nations, New York Conference Room 2, 3:00 p.m. 6:00 p.m. ISSUES NOTE Improving the Health Outcomes of Women and