Using new ARVs in pregnancy
|
|
|
- Osborn Ford
- 5 years ago
- Views:
Transcription

1 Using new ARVs in pregnancy Dr Wendy Mphatswe SA HIV Clinician s Society Meeting 15 July 2017
2 Overview 1. HIV epidemic 2. HIV response (Fast Track) 3. Goal of therapy in pregnant and breastfeeding women 4. ART guidelines - SA Clinical ART guideline - WHO clinical guidelines 5. Recent advances - PrEP - Newer ART agents 6. Safety of ART in pregnancy 7. Conclusion
3
4
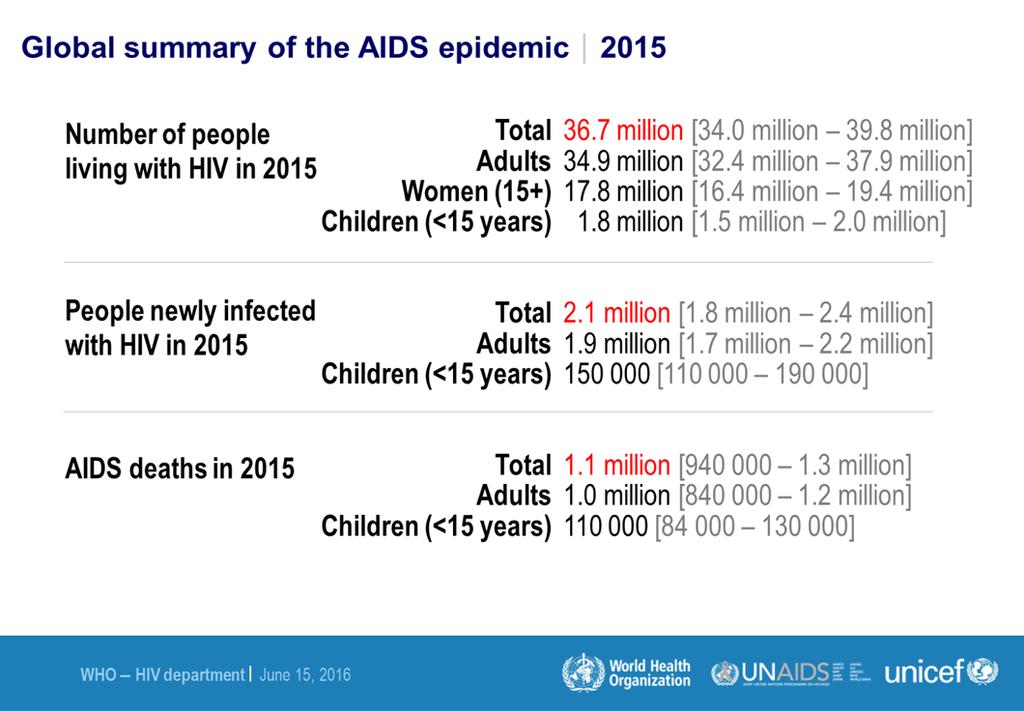
5 Overall context of the epidemic in SA South Africa currently accounts for 17% of the global burden of HIV infection. 66% of all new HIV infection are in sub-saharan Africa 6.4 million people living with HIV and AIDS in South Africa (12% of the population) > 3 million are on treatment South Africa also has the highest burden HIV positive pregnant women in the world. 1,200,000 babies born annually the HIV prevalence among pregnant women is 29.3%, almost 360,000 HIV exposed babies born every year. 2.4 million children orphaned due to AIDS
6 HIV RESPONSE

7 strategic targets By 2020, 90% of all people living with HIV will know their HIV status. By 2020, 90% of all people with diagnosed HIV infection will receive sustained antiretroviral therapy. By 2020, 90% of all people receiving antiretroviral therapy will have viral suppression.



8
9 Impact of the UNAIDS strategy Modelling suggests that achieving targets by 2020 will result in the end of AIDS by HIV treatment and viral suppression are critical to the control of the epidemic but this is not on its own. Preventative measures need alongside HIV treatment scale up need to be improved simultaneously. Prevention measures: emtct Condom usage Pre-exposure prophylaxis Medical Male Circumcision Focus on key vulnerable populations (Drug users/ MSM etc)
10 GOALS OF THERAPY IN PREGNANT AND BREASTFEEDING WOMEN
11 GOALS OF THERAPY IN PREGNANT AND BREASTFEEDING WOMEN Goal of therapy in pregnant women: Own health Reduce VL to an undetectable level, maintain VL suppression improve/preserve good immune status long term survival. Virtual elimination of mother to child transmission of HIV Intense monitoring of viral suppression during pregnancy and breastfeeding Rapid response in cases of patient with unsuppressed VL Intensify post-exposure prophylaxis in HIV exposed babies Early HIV diagnosis (repeat testing)
12 IMPACT OF ART ON MOTHER TO CHILD TRANSMISSION
13 Trends in reduction of MTCT: study results over time 1994 ACTG Bangkok AP/IP ZDV 2000 PHPT 2004: PHPT-2 HAART Transmission (%) Abidjan AP/IP ZDV 1999 PETRA AZT/3TC 1999 ZDV HIVNET 012 sdnvp ZDV + NVP 2002 DITRAME +1 ZDV + NVP 2003: DITRAME +1.1 ZDV/3TC+ NVP USA & Europe Thailand Africa
 Percentage (%) of pregnant women living with HIV accessing PMTCT services New HIV")
14 New HIV infections among children (aged 0 14 years) and percentage of pregnant women living with HIV receiving antiretroviral medicines (either prophylaxis or lifelong therapy) to prevent mother-to-child transmission, global, Number of new HIV infections among children (aged 0 14 years) Percentage (%) of pregnant women living with HIV accessing PMTCT services New HIV infections PMTCT coverage Global targets of new HIV infections Global PMTCT target Source: UNAIDS 2016 estimates. Note: In 2010, single-dose nevirapine was no longer included in ARV coverage as an effective regimen for the prevention of mother-to-child transmission.
 Six-week transmission rate Final transmission rate Source: UNAIDS 2016")
15 Six-week and final mother-to-child transmission rates, by country, 2015 Angola Chad Ghana Côte d Ivoire Democratic Republic of the Congo Cameroon Lesotho Malawi Kenya United Republic of Tanzania Zimbabwe Burundi Mozambique Zambia Namibia Swaziland Uganda Botswana South Africa Mother-to-child transmission rate (%) Six-week transmission rate Final transmission rate Source: UNAIDS 2016 estimates.

16 AIDS-related deaths among children by age group, global, Number 0 4 years 5 9 years years Source: UNAIDS 2016 estimates.
17 IMPACT OF ART ON MATERNAL MOTARLITY
18 18
19 Percentage of infants born to women living with HIV receiving a virologicaltest within the first two months of life, by country, 2015 Percentage (%) Source: 2016 Global AIDS Response Progress Reporting.
20 SA guidelines 2015
21 SA guidelines From January 2015, all HIV-infected pregnant and breastfeeding women initiated on an EFV-based FDC TDF+3TC (FTC)+EFV Regardless of CD4 count, WHO stage or infant feeding practice FDC continued for life once started WHO B+ PROGRAM UNIVERSAL TEST AND TREAT SINCE 2016
22 SA Guidelines
23
24 SA guidelines Second-line regimen Failing on a TDF-based 1st line regimen AZT + 3TC + LPV/r AZT + TDF + 3TC + LPV/r (4 drugs if HBV co-infected) Failing on a d4t or AZT-based 1st line regimen TDF + 3TC (or FTC) + LPV/r Dyslipidaemia or diarrhoea associated with LPV/r switch LPV/r to ATV/r
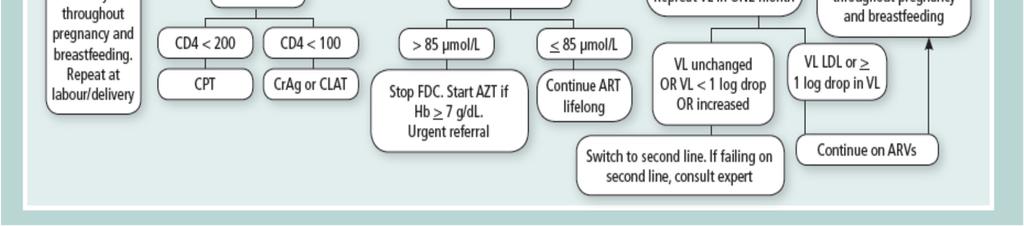
25 SA guidelines Threshold for treatment failure: VL>1000, adherence counselling, repeat VL in 1 month 2 nd VL undetectable or reduction in VL 1 log (10-fold), continue existing regimen VL unchanged or increased, switch to 2 nd line therapy
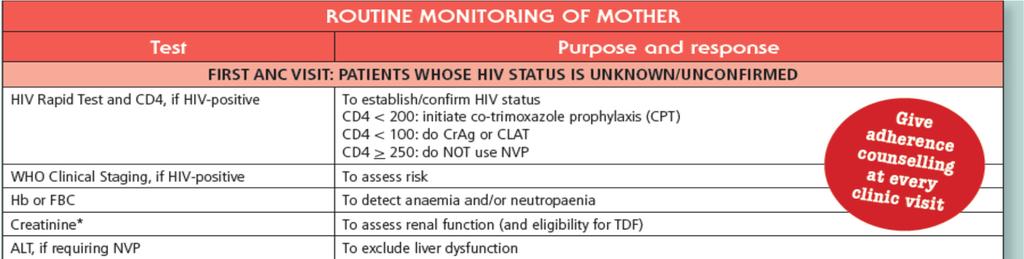
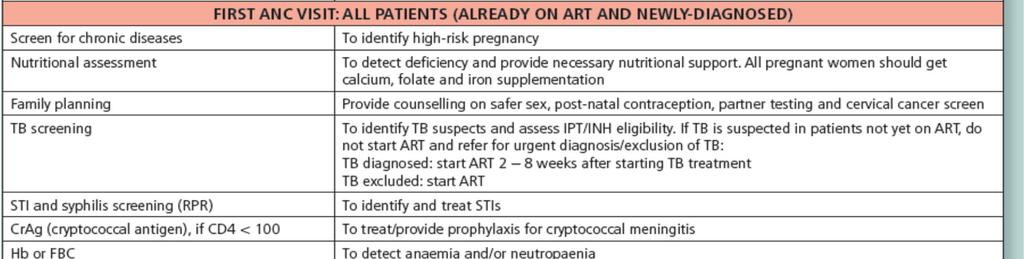
26 HIV positive women Baseline Work-up Clinical examination (WHO staging) Screen for active psychiatric illness Bloods: Creatinine and CD4 Follow-up in 1 week for these blood results All women, regardless of HIV status: TB and STI screen BANC: Hb, RPR/rapid TPHA, Rh, Urine dipstix, micronutrients Register on Momconnect 26
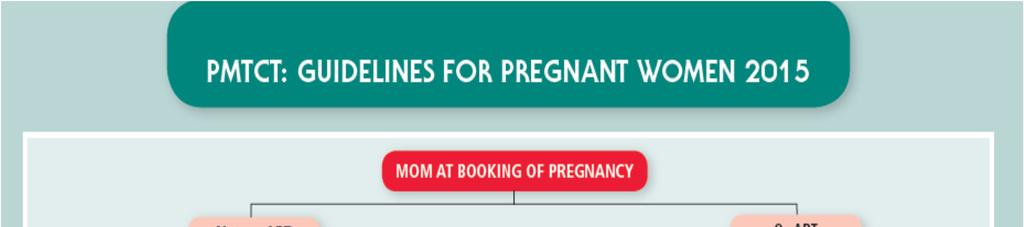
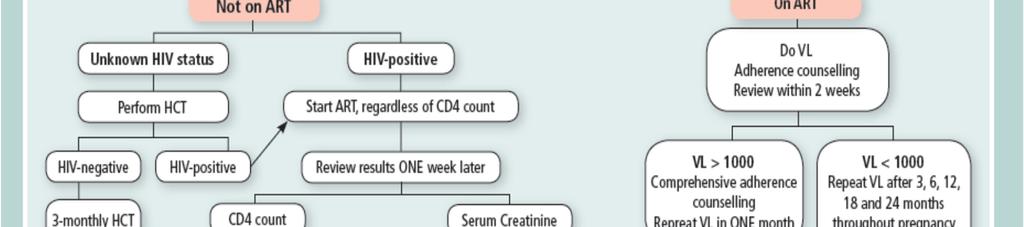
27 HIV positive women ART Initiation Initiate FDC (TDF/FTC/EFV) SAME DAY unless: 1. Concern about abnormal renal function 2. ACTIVE psychiatric illness 3. Newly diagnosed TB or high suspicion of active TB All women with contraindication to FDC initiation must receive AZT 300mg bdat their first visit No women leaves her first ANC visit without any ARV cover for PMTCT Arrange follow-up visit in ONE WEEK (blood results) 27
28 Contraindications to FDC(1) Suspected/Known Renal Dysfunction TDF associated with renal toxicity DO NOT initiate FDC same day if: Diabetes or hypertension Previous kidney condition requiring hospitalization (excluding UTI) 2+ proteinuria on urine dipstix Send for creatinine Initiate AZT 300mg bdsame DAY As long as Hb 7g/dl 28
29 Contraindications to FDC (2) Suspected/Known Renal Dysfunction Review in 1 week Creatinine normal: INITIATE FDC Creatinine 85μmol/L = HIGH RISK PREGNANCY Continue AZT 300mg bd Urgently REFER (or telephonically consult): Initiation of alternative lifelong triple drug regimen, including dose adjustment (usually ABC, 3TC, EFV) Investigation & management of renal disease Remember to work up those with 2+ proteinuria according to local protocols 29
30 Contraindications to FDC (3) Suspected/Known Renal Dysfunction IF woman initiated on FDC at first visit and Creatinine 85 μmol/l at review STOP FDC START AZT 300mg bd(if Hb 7g/dl) Urgently refer/discuss telephonically 30
31 Contraindications to FDC (4) Active Psychiatric Illness If a woman has ACTIVE/UNTREATED psychiatric disorder: DO NOT initiate FDC Provide AZT 300mg bd(if Hb 7g/dl) HIGH RISK PREGNANCY Urgently refer/discuss telephonically Initiation of alternative lifelong triple drug regimen (NVP or LPV/r, dependant on CD4 count, plus TDF and 3TC) Optimise management of psychiatric disorder ACTIVE psychiatric illness DOES NOT INCLUDE Depression Anxiety Known psychiatric patient well controlled/asymptomatic on treatment 31
32 TB (1) Screening Screen EVERY woman, regardless of HIV status, at EVERY visit for TB 32
 START IPT and pyridoxine Contraindications to IPT as per adult")
33 TB Screen Negative = IPT Negative TB screen (NO cough, fever, night sweats, weight loss/failure to gain weight) START IPT and pyridoxine Contraindications to IPT as per adult guidelines 33
34 Monitoring During Pregnancy and Breastfeeding VIRAL LOAD VIRAL LOAD VIRAL LOAD 34
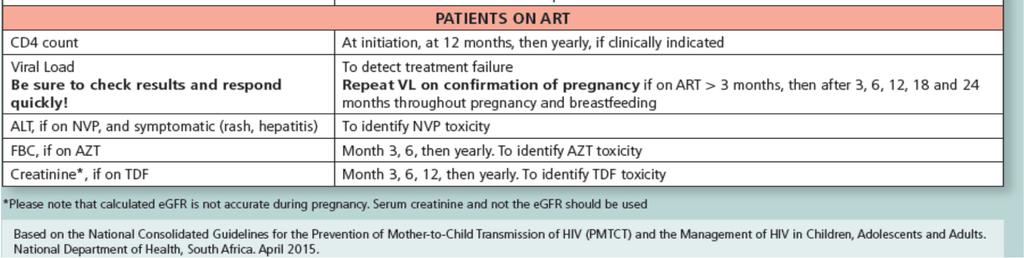
35 Viral Load Monitoring(1) Woman Already on ART 3 months and Conceives Viral Load to be repeated ON THE DAY OF PREGNANCY CONFIRMATION Regardless of when last done Need to know this woman is virally suppressed Review result within TWO WEEKS If virally suppressed: Continue on current regimen If on first line single ART agents with no contraindications (check creatinine) Switch to FDC (TDF/FTC/EFV) Provide adherence counselling including educating about the link between viral load and the risk of MTCT and safety of ART in pregnancy. 35
36 Viral Load Monitoring (2) Woman Newly Initiated on ART First viral load will be done THREE MONTHS after ART INITIATION Review results within TWO WEEKS We need to know this woman is suppressing on ART 36
37 Viral Load Monitoring (3) Women Who Are Virally Suppressed If Viral Load is < 1000 copies /ml Repeat Viral Load SIX MONTHLY: All viral load results should be reviewed within TWO WEEKS If concerns about poor adherence repeat viral load, regardless of when last done Women will return to annual viral load monitoring once she has stopped breastfeeding and is enrolled in standard adult ART care 37
38 Viral Load Monitoring (4) Women with Viral Load >1000 copies/ml Intensive adherence counselling Repeat Viral Load after ONE MONTH PLUS Hep B sag Hb/Creatinine(depending on predicted 2 nd line regimen) Viral load undetectable OR 1 log drop Continue with current ART regimen Monitor adherence closely Repeat viral load in 6 months, or sooner if concerns about adherence 38
39 Treatment failure: VL>1000, adherence counselling, repeat VL in 1 month 2 nd VL undetectable or reduction in VL 1 log (10-fold), continue existing regimen VL unchanged or increased, switch to 2 nd line therapy
40 Viral Load unchanged, increased or 1 log drop Switch to 2nd line Regimen as per adult guidelines CHECK HEPATITIS B sag result BEFORE switch Hep B -ve= 3 drug 2 nd line regimen Hep B +ve= 4 drug 2 nd line regimen INCLUDING TDF Infant to receive Hep B immunoglobulin and Hep B immunisation at birth Refer/discuss telephonically if woman already on 2 nd /3 rd line regimen or you are unsure what to do 40
41 Unchanged Other Monitoring Creatinine: 3, 6, 12 months and annually CD4: baseline, 12 months, not again If CD4 < 200 start Co-trimoxazole Or if WHO stage 2, 3 or 4 disease If CD4 < 100 send Cryptococcallatex antigenand follow available protocol and refer if screen positive 41

42 Labour and Delivery 42
43 HIV negative Repeat HIV test Regardless of when last done HIV status unknown Counsel and provide HIV test HIV positive on ART Continue ART with usual timing Labour and Delivery 43
44 Newly Diagnosed HIV Positive: Unbookedwomen & previously HIV negative In-labour management: Stat sdnvp Stat sdtruvada(ftc/tdf) 3 hourly AZT FDC dispensed before discharge to start the following day Counselling and adherence support Take CD4 and Creatinine Review results at 3-6 day post-natal visit Baby: Birth PCR 12 weeks NVP Repeat PCR at 14 weeks 44
45 Safe Delivery Techniques Avoid prolonged rupture of membranes Use assisted instrumental delivery only if absolutely indicated for obstetric reasons Invasive monitoring procedures not used in KZN Episiotomy only if essential Invasive suctioning of the neonate s nose and airway Meconium stained liquor suction under direct vision Caesarean section All HIV-positive women to receive prophylactic antibiotic If HIV-positive and not on ART, sdnvpand Truvada beforehand 45



46 Post-partum 46
47 Within one hour of delivery ALL Infants Skin-to-skin contact with mother asap Initiate exclusive breastfeeding Teach mother about kangaroo mother care As soon as possible after birth HIV-exposed infants Initiate infant prophylaxis Infant birth PCR 47
48 Testing Test When Who Where What 1 Birth All exposed Nursery/ Post natal ward PCR 2 NON- BF 10/52 Allexposed infants getting 6/52 NVP PHC Clinic PCR OR 14/52 Allexposed infants getting 12/52 NVP PHC Clinic PCR 3 6/52 post B/F All exposed infants who are B/F PHC Clinic PCR 4 18/12 All exposed infants PHC Clinic Rapid test 48

49 Most Infants These mothers are expected to be virally suppressed infant does not need extended NVP cover for breastfeeding 6 monthly maternal viral load monitoring essential URGENT intervention if Viral Load >1000 copies/ml beyond 6 weeks of breastfeeding 49
50 Infants who need additional prophylaxis 12weeks NVP Infants born to mothers who have not been on ART for long enough to be virally suppressed by the time the infant is 6 weeks old: < 4 weeks on ART Diagnosed in labour/delivery Diagnosed during breastfeeding and still breastfeeding 6 weeks NVP plus AZT Infants born to mothers who have been on ART for > 3 months and stillhave a viral load >1000 copies/ml. These women may have poor adherence These women may have ART resistance 50
51 Mothers Failing 2 nd /3 rd Line If mother has VL> 1000 copies/ml and is on SECOND or THIRD LINE therapy: This baby should preferably not be BREASTFED Prescribe infant formula (medically indicated) Need to ensure facilities have stock If formula not available: Careful counselling of mother Intensive adherence support Exclusive breastfeeding These mother-baby pairs should be referred/ telephonically discussed 51
52 Other Infants Orphaned/Abandoned with unknown maternal status Give NVP immediately Test infant with HIV rapid test If rapid test positive AND do birth PCR: continue NVP for 6 weeks If rapid test negative: stop NVP Non-breastfeedingmother diagnosed HIV positive > 72 hours after delivery No infant NVP Perform PCR at maternal diagnosis: If positive, initiate ART, CPT and confirm with second PCR If negative: continue with infant testing algorithm up to 18 months 52
53 After Delivery, Before Discharge Dispense minimum 8 weeks ART to mother Ensure mother understands about: ART adherence Infant prophylaxis dosage and adherence Exclusive breastfeeding Where and when to follow-up for herself plus her infant Discuss/offer contraception Clearly document management plan for mother-baby pair in RTHB 53
54 Infant Feeding All infants, regardless of maternal HIV status, should be exclusively breastfed Unless medically indicated: Mother or infant physically incapable Non-ART medications not suitable for breastfeeding Mother on 2 nd or 3 rd line therapy and viral load >1000 copies/ml These infants must receive PRESCRIBED FORMULA OR mother chooses not to breastfeed Support her choice Educate appropriately about formula feeding Ensure has resources to provide formula for baby 54
55 Breastfeeding Repeated feeding counselling reinforce messaging 6 months exclusive breastfeeding No water, pap, other solids Can give medication Introduction of complementary foods only from 6 months Continue breastfeeding: 12 months if mother HIV positive 24 months if mother HIV negative (remember repeat HIV testing!) 24 months if infant confirmed HIV positive 55
56 WHO guidelines 2015

57 WHO guidelines 2015
58 WHO guidelines 2016
59 WHO guidelines 2016 Recommendation applies to breastfeeding and non-breastfeeding populations Health benefits of universal ART for pregnant and breastfeeding women outweigh potential harm Health benefits immunological and clinical
60 WHO guidelines 2016 Pregnant or breastfeeding women Preferred 1 st line regimen TDF + 3TC (or FTC) + EFV Alternative 1 st line regimens AZT + 3TC + EFV (or NVP) TDF + 3TC (or FTC) + NVP ABC or boosted PIs (ATV/r, DRV/r, LPV/r) in special circumstances
61 WHO guidelines 2016 Pregnant or breastfeeding women Preferred 2 nd line regimen 2 NRTIs + ATV/r or LPV/r Alternative 2 nd line regimen 2 NRTIs + DRV/r (similar to adults and adolescents)
62 PRE-EXPOSURE PROPHYLAXIS IN PREGNANCY
63 WHAT IS PrEP? PrEPis the daily use of oral tenofovirdisoproxilfumarate (TDF) or coformulated TDF/emtricitabine(TDF/FTC) to prevent HIV acquisition. Effective in HIV populations is great risk of HIV acquisition Benefit in clinical practice if adherent Taken for sufficient duration of therapy Should be used in combination with other prevention tools eg. HIV and STI testing, condom and condom compatible lubricant dissemination, STI treatment, and risk reduction counselling. IT IS AN ADDITIONAL PREVENTION METHOD!!!
64 No mention of pregnancy No explicit description or outline of AT RISK POPULATIONS FOR HIV

65

66 2015 WHO RECOMMENDATIONS ON PREP Existing safety data supports the use of PrEPin pregnant and breastfeeding women who are at continuing substantial risk of HIV infection
67 WHO RECOMMENDATIONS ON PREP JULY 2017.
68 WHO RECOMMENDATIONS ON PREP
69 Challenges with PrEPin pregnancy and breastfeeding Assessment of risk of HIV acquisition - Tendency to underestimate or overestimate risk - PREVENTION PARADOX (individual risk vs population risk) - Absence of objective tools to assess risk Safety issues of ART exposure (risk vs benefit) in an HIV uninfected person BEARING IN MIND In SA approximately 4% of pregnant women who initially test HIV negative in early pregnancy are HIV positive later in pregnancy. New infection high viral load high risk for MTCT
70 NEWER HIV ARVS
71 Dolutegravir(DTG) Newer antiretrovirals Tenofoviralafenamide(TAF) Efavirenz400mg (EFV400)
72 Newer antiretrovirals Dolutegravir(DTG) - Possible use as part of 1 st line Rx instead of EFV - Late presentation in pregnancy rapid decline of VL (7 days vs 26 days in cart) - Intensify treatment (additional 4 th agent) - Drug resistance (PI based regimens still preferred in drug-resistance case) Tenofoviralafenamide(TAF) Efavirenz400mg (EFV400) No sufficient clinical experience of dolutegravir(dtg), tenofoviralafenamide(taf) or efavirenz400mg (EFV400) to recommend their use in pregnancy. Outcomes from births and assessment of congenital anomalies need to be evaluated from several hundred pregnant women.
73 1-log reduction, the median time to one-log RNA reduction was 8 days [Interquartile Range (IQR): 7, 14] in the INSTI group versus 35 days

74
75 ART EXPOSURE IN-UTERO
76 Issues of concern Risk of congenital abnormalities Pregnancy outcomes Cognitive and neurodevelopmental outcomes Altered immune activation
77 Safety concerns: ART exposure More fetusesand infants are exposed to multiple drugs ART from conception through to breastfeeding. Risks of EFV in first trimester: -Known to be associate with CNS abnornalitiesin animal studies and a recent observational study. -Ford et al. meta-analysis found no increased risk of overall birth defects in infants born to women on EFV [RR] 0.87; 95% [CI], ). -Data still insufficient to rule out low-incidence birth defects. Risk of preterm labour: -Watts et al: PI based regimens (USA) associated with increased risk of preterm birth started in 1 st trimester. No increased risk with NNRTI-based regimens, triple nucleoside regimens, or ARV exposure starting later in pregnancy. J Infect Dis 2013; 207:
78 Safety of EFV in pregnancy Previous concerns about risk of teratogenicity with use in the 1 st T Evidence was based on animal studies and retrospective case reports of neural tube defects in infants exposed to EFV in utero data from large observational studies don t show an increased risk of neural tube defects with EFV use in all trimesters of pregnancy
79
80 Safety of TDF in pregnancy Concerns about... o Congenital abnormalities o Growth restriction o Loss of bone mineral density (maternal and fetal) o Low birth weight o Preterm delivery o Pregnancy losses

 or change in HLZ (ß =.")
81 There was no association between duration of in utero TDF exposure per 1-week increment and change in FLZ (ß =.00; P =.51) or change in HLZ (ß =.00; P =.40).
82 These data suggest no association between duration of TDF exposure in utero and early linear growth.

83 Maternal tenofoviruse is associated with significantly lower neonatal BMC. The duration and clinical significance of this finding should be evaluated in longitudinal studies.
84 Safety concerns: ART exposure DART trial: No evidence that TDFhad adverse effects on pregnancy outcomes or on congenital, renal, bone, or growth abnormalities up to age 4 years. N= 226, 182 enrolled). PLoS Med 2012; 9:e Concern that in utero AZT exposure could be associated with paediatric mitochondrial disorders. Ultimatelyany ARV use during pregnancy is NOTwithout risk to the fetus. Surveillance for birth defects and adverse outcomes is warranted given the large number of women who will fall pregnant on ART with B+.
85 Adverse pregnancy outcomes
86 Adverse pregnancy outcomes Suggestion that cart is responsible for increased risk of adverse pregnancy outcomes Conflicting results from different studies: Different populations studied Available obstetric care Adjustment for confounders; selection of exposure categories?inflammatory effect of HIV infection (Li N, et al. JID2015)

87
88 Background Systematic review of studies from low-, middle- and high-income countries Studies done between January 1980 and June measure: to assess association between selected pregnancy outcomes and ART initiation pre-conception vs. after conception
89 Results 11 studies with mother infant pairs Women who started ART before conception significantly more likely to: deliver preterm (RR 1 20, 95% CI ) very preterm (1 53, ) have LBW infants (1 30, ) than were those who began ART after conception
90 CONCLUSION Lifelong ART for pregnant and breastfeeding women Universal ART Safety data of cart is encouraging and reassuring PrEPis recommended in pregnant and breastfeeding women who are at high risk for HIV acquisition Not enough experience with newer ART agents


91 No child should be born with HIV; No child should be an orphan because of HIV; No child should die due to lack of access to treatment. Ebube Sylvia Taylor, 11-years Nigeria THANK YOU
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM
 Dept of O+G NRMSM") Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive:
 Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive: Rationale for the call to action, progress to date and dealing with realities Rene Ekpini, MD, MPH Senior Adviser,
Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive: Rationale for the call to action, progress to date and dealing with realities Rene Ekpini, MD, MPH Senior Adviser,
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT
 PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
Figure S1: Overview of PMTCT Options A and B. Prevention of Mother to Child HIV Transmission (PMTCT)
") Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
Elijah Paintsil, MD, FAAP
 Roadmap to elimination of mother-to-child transmission of HIV in Ghana by 2015 Towards HIV Free Generation Elijah Paintsil, MD, FAAP Assistant Professor of Pediatrics & Pharmacology Yale School of Medicine,
Roadmap to elimination of mother-to-child transmission of HIV in Ghana by 2015 Towards HIV Free Generation Elijah Paintsil, MD, FAAP Assistant Professor of Pediatrics & Pharmacology Yale School of Medicine,
Elimination of mother to child transmission of HIV: is the end really in sight? Lisa L. Abuogi, MD University of Colorado, Denver Dec 3, 2014
 Elimination of mother to child transmission of HIV: is the end really in sight? Lisa L. Abuogi, MD University of Colorado, Denver Dec 3, 2014 Outline Background History of prevention of mother to child
Elimination of mother to child transmission of HIV: is the end really in sight? Lisa L. Abuogi, MD University of Colorado, Denver Dec 3, 2014 Outline Background History of prevention of mother to child
Progress & challenges in PMTCT: The unfinished agenda
 Progress & challenges in PMTCT: The unfinished agenda Dr Chewe Luo MMED (Paed); MTropPaed; PhD; FRCP Senior Adviser and Team Leader Country Programme Scale Up HIV Section, Programme Division UNICEF NY,
Progress & challenges in PMTCT: The unfinished agenda Dr Chewe Luo MMED (Paed); MTropPaed; PhD; FRCP Senior Adviser and Team Leader Country Programme Scale Up HIV Section, Programme Division UNICEF NY,
Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20
 Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive
 Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive DR. Nicholas Muraguri OGW, MD,MPH, MBA, PhD (c) Director, Global Plan Secretariat www.zero-hiv.org
Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive DR. Nicholas Muraguri OGW, MD,MPH, MBA, PhD (c) Director, Global Plan Secretariat www.zero-hiv.org
FAST-TRACK: HIV Prevention, treatment and care to End the AIDS epidemic in Lesotho by 2030
 Evidence informed, responsive and sustainable care FAST-TRACK: HIV Prevention, treatment and care to End the AIDS epidemic in Lesotho by 2030 Alti Zwandor UNAIDS Country Director Maseru, Lesotho 9 December
Evidence informed, responsive and sustainable care FAST-TRACK: HIV Prevention, treatment and care to End the AIDS epidemic in Lesotho by 2030 Alti Zwandor UNAIDS Country Director Maseru, Lesotho 9 December
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA. Date
 CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES?
 WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
MULHERES GRAVIDAS OPTION B+ PTV / EMTCT Dr ND NHLAPO
 MULHERES GRAVIDAS OPTION B+ PTV / EMTCT Dr ND NHLAPO Prevention of Mother to Child Transmission The new term is EMTCT!! Learning objectives Understand scope of problem in Sub saharanafrica Understand when
MULHERES GRAVIDAS OPTION B+ PTV / EMTCT Dr ND NHLAPO Prevention of Mother to Child Transmission The new term is EMTCT!! Learning objectives Understand scope of problem in Sub saharanafrica Understand when
Update on global guidelines. and emerging issues on perinatal HIV prevention. WHO 2013 Consolidated ARV Guidelines
 WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
Dr Graham P Taylor Reader in Communicable Diseases
 HIV in Pregnancy Joint RCOG/BHIVA Multidisciplinary Conference Dr Graham Taylor Imperial College London Friday 20 January 2012, Royal College of Obstetricians and Gynaecologist, London Prevention of post-partum
HIV in Pregnancy Joint RCOG/BHIVA Multidisciplinary Conference Dr Graham Taylor Imperial College London Friday 20 January 2012, Royal College of Obstetricians and Gynaecologist, London Prevention of post-partum
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
PMTCT UPDATE. AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM
 PMTCT UPDATE AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM Outline Background Risk of MTCT Historical ARV interventions SA PMTCT program Rationale for changes
PMTCT UPDATE AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM Outline Background Risk of MTCT Historical ARV interventions SA PMTCT program Rationale for changes
DEPARTMENT. Treatment Recommendations for. Pregnant and Breastfeeding Women: Critical Issues Consolidated ARV Guidelines. Dr.
 2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
Tunisian recommendations on ART : process and results
 Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
The NEW ARV Guidelines FAQs
 The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
The New National Guidelines. Feeding in the Context of HIV. Dr. Godfrey Esiru; National PMTCT Coordinator
 The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
treatment during pregnancy and breastfeeding
 treatment during pregnancy and breastfeeding Topics covered Introduction. Preventing parent-to-child transmission. AZT as a single therapy. Treatment begun late in pregnancy. Nevirapine for mothers and
treatment during pregnancy and breastfeeding Topics covered Introduction. Preventing parent-to-child transmission. AZT as a single therapy. Treatment begun late in pregnancy. Nevirapine for mothers and
Infertility Treatment and HIV
 Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
The 2017 Namibia ART Guidelines. Tadesse T. Mekonen, MD, MPH, AAF-HIV
 The 2017 Namibia ART Guidelines Tadesse T. Mekonen, MD, MPH, AAF-HIV Q1-Table 1 List at least four key new recommendations in the 2017 Namibian ART Guidelines Q2-Table-2 46yo, Male, on AZT/TDF/FTC/ATVr
The 2017 Namibia ART Guidelines Tadesse T. Mekonen, MD, MPH, AAF-HIV Q1-Table 1 List at least four key new recommendations in the 2017 Namibian ART Guidelines Q2-Table-2 46yo, Male, on AZT/TDF/FTC/ATVr
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE
 UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
Treatment Optimization for EMTCT
 Treatment Optimization for EMTCT Dr Madeleine Muller With thanks to CN Mnyani and Linda-Gail Bekker SA HIV Clinician s Society Meeting 25 Nov 2017 Having children is one of the greatest joys and privileges
Treatment Optimization for EMTCT Dr Madeleine Muller With thanks to CN Mnyani and Linda-Gail Bekker SA HIV Clinician s Society Meeting 25 Nov 2017 Having children is one of the greatest joys and privileges
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV
 TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
Updates on Revised Antiretroviral Treatment Guidelines Overview 27 March 2013
 Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
2009 Revisions of WHO ART Guidelines. November 2009
 2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT
 The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT Peter McDermott Managing Director, CIFF 19 th Board meeting, Geneva 6 th May 2009 Investment Criteria Measurable...change
The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT Peter McDermott Managing Director, CIFF 19 th Board meeting, Geneva 6 th May 2009 Investment Criteria Measurable...change
1. Africa Centre for Health and Population Studies 2. London School of Hygiene and Tropical Medicine 3. University College London
 A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
Outline. Aim with PMTCT. How are children transmitted. Prevention of mother-to-child transmission of HIV. How does HIV transmit to children?
 Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
Emerging Issues in HIV and Pregnancy. Lynne M. Mofenson, MD. HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation
 Emerging Issues in HIV and Pregnancy Lynne M. Mofenson, MD HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation Perinatal Transmission in the ART Era What s New? Antepartum ARV drug
Emerging Issues in HIV and Pregnancy Lynne M. Mofenson, MD HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation Perinatal Transmission in the ART Era What s New? Antepartum ARV drug
Scaling up priority HIV/AIDS interventions in the health sector
 TOWARDS UNIVERSAL ACCESS? Scaling up priority HIV/AIDS interventions in the health sector Yves Souteyrand, WHO October 2011 Towards universal access targets UN General Assembly High level Meeting June
TOWARDS UNIVERSAL ACCESS? Scaling up priority HIV/AIDS interventions in the health sector Yves Souteyrand, WHO October 2011 Towards universal access targets UN General Assembly High level Meeting June
Objectives. Outline. Section 1: Interaction between HIV and pregnancy. Effects of HIV on Pregnancy. Section 2: Mother-to-Child-Transmission (MTCT)
") Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
ARV Consolidated Guidelines 2015
 ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
2016 Perinatal Treatment Guidelines Update
 Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Update on PMTCT. African Health Profession Regulatory Collaborative for Nurses and Midwives. Johannesburg, Republic of South Africa, June 18-22, 2012
 PMTCT Update Update on PMTCT Margarett Davis, MD, MPH Chief, Maternal and Child Health Branch Division of Global HIV/AIDS Centers for Disease Control and Prevention (CDC) African Health Profession Regulatory
PMTCT Update Update on PMTCT Margarett Davis, MD, MPH Chief, Maternal and Child Health Branch Division of Global HIV/AIDS Centers for Disease Control and Prevention (CDC) African Health Profession Regulatory
Update on Option B+ Successes and Challenges. James McIntyre
 Update on Option B+ Successes and Challenges James McIntyre Anova Health Institute & School of Public Health & Family Medicine, University of Cape Town Do not be fooled: People make simple things complex
Update on Option B+ Successes and Challenges James McIntyre Anova Health Institute & School of Public Health & Family Medicine, University of Cape Town Do not be fooled: People make simple things complex
Paediatric ART: eligibility criteria and first line regimens. (revised) Dave le Roux 13 August 2016
 Dave le Roux 13 August 2016") Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
Mother to Child HIV Transmission
 Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION
 Abst#_O_01 DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION Hadiza Khamofu, 1 Edward Oladele, 1 Uche Ralph-Opara,
Abst#_O_01 DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION Hadiza Khamofu, 1 Edward Oladele, 1 Uche Ralph-Opara,
hiv/aids Programme Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants
 hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
MANAGING HIV IN CHILDREN: BEST PRACTICES
 MANAGING HIV IN CHILDREN: BEST PRACTICES Dr. Mo Archary Paediatric Infectious Diseases Specialist University of KwaZulu Natal/ King Edward VIII Hospital Overview Global state of paediatric ART Filling
MANAGING HIV IN CHILDREN: BEST PRACTICES Dr. Mo Archary Paediatric Infectious Diseases Specialist University of KwaZulu Natal/ King Edward VIII Hospital Overview Global state of paediatric ART Filling
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and
, Children, Adolescents and") The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2015 (Amended Version) The Western Cape Consolidated
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2015 (Amended Version) The Western Cape Consolidated
What s New. In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group
 What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013
 Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013 The following document highlights the changes National department of Health ARV treatment guidelines
Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013 The following document highlights the changes National department of Health ARV treatment guidelines
All [HIV-exposed] infants should receive oral antiretroviral prophylaxis for the entire duration of breastfeeding - CON
![All [HIV-exposed] infants should receive oral antiretroviral prophylaxis for the entire duration of breastfeeding - CON](/thumbs/93/111509999.jpg "All [HIV-exposed] infants should receive oral antiretroviral prophylaxis for the entire duration of breastfeeding - CON") All [HIV-exposed] infants should receive oral antiretroviral prophylaxis for the entire duration of breastfeeding - CON Amy Slogrove Stellenbosch University 10 th International HIV Pediatrics Workshop
All [HIV-exposed] infants should receive oral antiretroviral prophylaxis for the entire duration of breastfeeding - CON Amy Slogrove Stellenbosch University 10 th International HIV Pediatrics Workshop
2013 progress report on the Global Plan
 2013 progress report on the Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive 210 000 the number of new HIV infections among children in (21
2013 progress report on the Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive 210 000 the number of new HIV infections among children in (21
Review of recent changes in WHO and national paediatric care guidelines Dr. Chewe Luo UNICEF New York City, USA
 Review of recent changes in WHO and national paediatric care guidelines Dr. Chewe Luo UNICEF New York City, USA Review of recent changes in WHO and national paediatric care guidelines Dr. Chewe Luo MMed
Review of recent changes in WHO and national paediatric care guidelines Dr. Chewe Luo UNICEF New York City, USA Review of recent changes in WHO and national paediatric care guidelines Dr. Chewe Luo MMed
Infant feeding in the ARV era. Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital
 Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
HIV in the Next Generation: the Rocky Road to Elimination (focus on Africa)
") REALITY HIV in the Next Generation: the Rocky Road to Elimination (focus on Africa) Medical Research Council Clinical Trials Unit at University College London Di Gibb Diana.gibb@ucl.ac.uk Outline Millennium
REALITY HIV in the Next Generation: the Rocky Road to Elimination (focus on Africa) Medical Research Council Clinical Trials Unit at University College London Di Gibb Diana.gibb@ucl.ac.uk Outline Millennium
Towards an AIDS Free Generation
 Informal Board Meeting 18 January, 2011 Towards an AIDS Free Generation Craig McClure Chief, HIV and AIDS Achieving an AIDS-Free Generation UNAIDS Getting to Zero UNICEF MTSP The Unite for Children, Unite
Informal Board Meeting 18 January, 2011 Towards an AIDS Free Generation Craig McClure Chief, HIV and AIDS Achieving an AIDS-Free Generation UNAIDS Getting to Zero UNICEF MTSP The Unite for Children, Unite
Copyright 2011 Joint United Nations Programme on HIV/AIDS (UNAIDS) All rights reserved ISBN
 All rights reserved ISBN") UNAIDS DATA TABLES 2011 Copyright 2011 Joint United Nations Programme on HIV/AIDS (UNAIDS) All rights reserved ISBN 978-92-9173-945-5 UNAIDS / JC2225E The designations employed and the presentation of
UNAIDS DATA TABLES 2011 Copyright 2011 Joint United Nations Programme on HIV/AIDS (UNAIDS) All rights reserved ISBN 978-92-9173-945-5 UNAIDS / JC2225E The designations employed and the presentation of
Evolving Realities of HIV Treatment in Resource-limited Settings
 Evolving Realities of HIV Treatment in Resource-limited Settings Papa Salif Sow MD, MSc Department of Infectious Diseases University of Dakar, Senegal Introduction: ARV access in RLS Scale-up of ART has
Evolving Realities of HIV Treatment in Resource-limited Settings Papa Salif Sow MD, MSc Department of Infectious Diseases University of Dakar, Senegal Introduction: ARV access in RLS Scale-up of ART has
Renewing Momentum in the fight against HIV/AIDS
 2011 marks 30 years since the first cases of AIDS were documented and the world has made incredible progress in its efforts to understand, prevent and treat this pandemic. Progress has been particularly
2011 marks 30 years since the first cases of AIDS were documented and the world has made incredible progress in its efforts to understand, prevent and treat this pandemic. Progress has been particularly
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and
, Children, Adolescents and") The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2018 (Amended Version) The Western Cape Consolidated
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2018 (Amended Version) The Western Cape Consolidated
The elimination equation: understanding the path to an AIDS-free generation
 The elimination equation: understanding the path to an AIDS-free generation James McIntyre Anova Health Institute & School of Public Health & Family Medicine, University of Cape Town Elimination of perinatal
The elimination equation: understanding the path to an AIDS-free generation James McIntyre Anova Health Institute & School of Public Health & Family Medicine, University of Cape Town Elimination of perinatal
Obstetrics and HIV An Update. Jennifer Van Horn MD University of Utah
 Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
HIV und AIDS- was gibt es Neues für die Arbeit vor Ort?
 HIV und AIDS- was gibt es Neues für die Arbeit vor Ort? Dr. med. Ralf Weigel Liverpool School of Tropical Medicine ralf.weigel@lstmed.ac.uk foring UPDATE 2017 Humanitäre Hilfe und Entwicklungszusammenarbeit
HIV und AIDS- was gibt es Neues für die Arbeit vor Ort? Dr. med. Ralf Weigel Liverpool School of Tropical Medicine ralf.weigel@lstmed.ac.uk foring UPDATE 2017 Humanitäre Hilfe und Entwicklungszusammenarbeit
Prevention of Perinatal HIV Transmission
 Prevention of Perinatal HIV Transmission Emily Adhikari, MD Division of Maternal-Fetal Medicine Obstetrics and Gynecology University of Texas Southwestern Medical Center February 20, 2018 None Understand
Prevention of Perinatal HIV Transmission Emily Adhikari, MD Division of Maternal-Fetal Medicine Obstetrics and Gynecology University of Texas Southwestern Medical Center February 20, 2018 None Understand
TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES
 POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
Challenges of HIV drug resistance in resource-limited settings
 Challenges of HIV drug resistance in resource-limited settings Marie-Louise Newell Professor of Global Health Faculty of Medicine and Faculty of Social and Human Sciences, University of Southampton, UK
Challenges of HIV drug resistance in resource-limited settings Marie-Louise Newell Professor of Global Health Faculty of Medicine and Faculty of Social and Human Sciences, University of Southampton, UK
All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!!
 All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!! Lynne Mofenson MD Elizabeth Glaser Pediatric AIDS Foundation My Esteemed Opponent Will Likely
All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!! Lynne Mofenson MD Elizabeth Glaser Pediatric AIDS Foundation My Esteemed Opponent Will Likely
Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps
 Appendix 4 Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps Lynne M. Mofenson, MD Eunice Kennedy Shriver National Institute of
Appendix 4 Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps Lynne M. Mofenson, MD Eunice Kennedy Shriver National Institute of
HIV infection in pregnancy
 HIV infection in pregnancy Peter Brocklehurst National Perinatal Epidemiology Unit, University of Oxford What is the size of the problem? in the population as a whole? in women? in pregnant women? in children?
HIV infection in pregnancy Peter Brocklehurst National Perinatal Epidemiology Unit, University of Oxford What is the size of the problem? in the population as a whole? in women? in pregnant women? in children?
HIV Infection in Pregnancy. Francis J. Ndowa WHO RHR/STI
 HIV Infection in Pregnancy Francis J. Ndowa WHO RHR/STI FJN_STI_2005 Department of reproductive health and research Département santé et recherche génésiques Session outline Effect of pregnancy on HIV
HIV Infection in Pregnancy Francis J. Ndowa WHO RHR/STI FJN_STI_2005 Department of reproductive health and research Département santé et recherche génésiques Session outline Effect of pregnancy on HIV
Paediatric HIV Drug Resistance 26th-International-Workshop-on-HIV-Drug-Resistance-programme [2].tiff
![Paediatric HIV Drug Resistance 26th-International-Workshop-on-HIV-Drug-Resistance-programme [2].tiff](/thumbs/90/102413200.jpg "Paediatric HIV Drug Resistance 26th-International-Workshop-on-HIV-Drug-Resistance-programme [2].tiff") Paediatric HIV Drug Resistance 26th-International-Workshop-on-HIV-Drug-Resistance-programme- 20171031[2].tiff Mo Archary King Edward VIII Hospital / UKZN Paediatric Infectious Diseases Unit Overview State
Paediatric HIV Drug Resistance 26th-International-Workshop-on-HIV-Drug-Resistance-programme- 20171031[2].tiff Mo Archary King Edward VIII Hospital / UKZN Paediatric Infectious Diseases Unit Overview State
Investing for Impact Prioritizing HIV Programs for GF Concept Notes. Lisa Nelson, WHO Iris Semini, UNAIDS
 Investing for Impact Prioritizing HIV Programs for GF Concept Notes Lisa Nelson, WHO Iris Semini, UNAIDS Top 5 Lessons Learned 1 2 3 4 5 Prioritize within the allocation amount Separate above allocation
Investing for Impact Prioritizing HIV Programs for GF Concept Notes Lisa Nelson, WHO Iris Semini, UNAIDS Top 5 Lessons Learned 1 2 3 4 5 Prioritize within the allocation amount Separate above allocation
Can we make first line ART better?
 Can we make first line ART better? Dr David Stead Treatment Optimization HIV Clinicians Society Workshop 25 November 2017 With thanks to Francois Venter and the people who gave him slides Characteristics
Can we make first line ART better? Dr David Stead Treatment Optimization HIV Clinicians Society Workshop 25 November 2017 With thanks to Francois Venter and the people who gave him slides Characteristics
Accelerating Children s HIV Treatment (ACT): Rationale, Progress & Challenges
: Rationale, Progress & Challenges") Accelerating Children s HIV Treatment (ACT): Rationale, Progress & Challenges George Siberry, MD, MPH OGAC Senior Technical Advisor for Pediatrics March, 2016 Compared to Adults, Children (
Accelerating Children s HIV Treatment (ACT): Rationale, Progress & Challenges George Siberry, MD, MPH OGAC Senior Technical Advisor for Pediatrics March, 2016 Compared to Adults, Children (
2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents. When to Start and What ART to Use in 1 st and 2 nd Line December 2009
 2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents When to Start and What ART to Use in 1 st and 2 nd Line December 2009 Historic Evolution of CD4 Criteria for ART Initiation in
2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents When to Start and What ART to Use in 1 st and 2 nd Line December 2009 Historic Evolution of CD4 Criteria for ART Initiation in
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
De la prévention à l élimination, le chemin parcouru en matière de transmission verticale. De la recherche aux recommandations OMS
 De la prévention à l élimination, le chemin parcouru en matière de transmission verticale De la recherche aux recommandations OMS 16 novembre, 2011 Pr François DABIS Bordeaux 1985 1997 (1) 1985 1997 (1)
De la prévention à l élimination, le chemin parcouru en matière de transmission verticale De la recherche aux recommandations OMS 16 novembre, 2011 Pr François DABIS Bordeaux 1985 1997 (1) 1985 1997 (1)
Start Free Stay Free AIDS Free progress report
 Start Free Stay Free AIDS Free 217 progress report Copyright 217 Joint United Nations Programme on HIV/AIDS (UNAIDS) All rights reserved. The designations employed and the presentation of the material
Start Free Stay Free AIDS Free 217 progress report Copyright 217 Joint United Nations Programme on HIV/AIDS (UNAIDS) All rights reserved. The designations employed and the presentation of the material
Breast Feeding for Women with HIV?
 Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Prevention of Mother-to-Child Transmission of HIV Infection
 HIV Curriculum for the Health Professional Prevention of Mother-to-Child Transmission of HIV Infection Michael A. Tolle, MD, MPH Daniel Dewey, MD Objectives 1. Describe the scope of mother-to-child transmission
HIV Curriculum for the Health Professional Prevention of Mother-to-Child Transmission of HIV Infection Michael A. Tolle, MD, MPH Daniel Dewey, MD Objectives 1. Describe the scope of mother-to-child transmission
Overview of 2013 WHO consolidated ARV guidelines and update plans. Marco Vitoria HIV/AIDS Department WHO Geneva September 2014
 AMDS ANNUAL STAKEHOLDERS AND PARTNERS MEETING Overview of 2013 WHO consolidated ARV guidelines and update plans Marco Vitoria HIV/AIDS Department WHO Geneva September 2014 AMDS ANNUAL STAKEHOLDERS AND
AMDS ANNUAL STAKEHOLDERS AND PARTNERS MEETING Overview of 2013 WHO consolidated ARV guidelines and update plans Marco Vitoria HIV/AIDS Department WHO Geneva September 2014 AMDS ANNUAL STAKEHOLDERS AND
2015 PROGRESS REPORT ON THE GLOBAL PLAN
 2015 PROGRESS REPORT ON THE GLOBAL PLAN towards the elimination of new HIV infections among children and keeping their mothers alive 170 000 THE NUMBER OF NEW INFECTIONS AMONG CHILDREN IN 2014 8 OUT OF
2015 PROGRESS REPORT ON THE GLOBAL PLAN towards the elimination of new HIV infections among children and keeping their mothers alive 170 000 THE NUMBER OF NEW INFECTIONS AMONG CHILDREN IN 2014 8 OUT OF
Malaysian Consensus Guidelines on Antiretroviral Therapy Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh
 Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
AFRICAN PLAN TOWARDS THE ELIMINATION OF NEW HIV INFECTIONS AMONG CHILDREN BY 2015 AND KEEPING THEIR MOTHERS ALIVE
 AFRICAN PLAN TOWARDS THE ELIMINATION OF NEW HIV INFECTIONS AMONG CHILDREN BY 2015 AND KEEPING THEIR MOTHERS ALIVE Contents Foreword 4 List of abbreviations and acronyms 5 Introduction 6 Background 6 Rationale
AFRICAN PLAN TOWARDS THE ELIMINATION OF NEW HIV INFECTIONS AMONG CHILDREN BY 2015 AND KEEPING THEIR MOTHERS ALIVE Contents Foreword 4 List of abbreviations and acronyms 5 Introduction 6 Background 6 Rationale
The global plan to eliminate mother to child transmission (emtct) of HIV: challenges in integration and of therapeutic strategies
 of HIV: challenges in integration and of therapeutic strategies") Training Course in Sexual and Reproductive Health Research 2014 Module: Principles and Practice of Sexually Transmitted Infections Prevention and Care The global plan to eliminate mother to child transmission
Training Course in Sexual and Reproductive Health Research 2014 Module: Principles and Practice of Sexually Transmitted Infections Prevention and Care The global plan to eliminate mother to child transmission
Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya
 Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya KPA 2018 24-04-2018 Dr. Margaret Wainaina- Wafula Outline Introduction Evaluation of a child living with HIV. Standard
Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya KPA 2018 24-04-2018 Dr. Margaret Wainaina- Wafula Outline Introduction Evaluation of a child living with HIV. Standard
Ending mother to child transmission through community action. Ngashi Ngongo, MD, MPH Senior Health Advisor UNICEF New York
 Ending mother to child transmission through community action Ngashi Ngongo, MD, MPH Senior Health Advisor UNICEF New York PRESENTATION OUTLINE An historical perspective Learning from previous public health
Ending mother to child transmission through community action Ngashi Ngongo, MD, MPH Senior Health Advisor UNICEF New York PRESENTATION OUTLINE An historical perspective Learning from previous public health
Medical Challenges of HIV/AIDS pandemic: The WHO perspective. SOLTHIS HIV Forum
 Medical Challenges of HIV/AIDS pandemic: The WHO perspective SOLTHIS HIV Forum Marco Vitoria HIV/AIDS Department World Health Organization September 2013 Topic 2002 2003 2006 2010 2013 When to start 1
Medical Challenges of HIV/AIDS pandemic: The WHO perspective SOLTHIS HIV Forum Marco Vitoria HIV/AIDS Department World Health Organization September 2013 Topic 2002 2003 2006 2010 2013 When to start 1
Appendix 1: summary of the modified GRADE system (grades 1A 2D)
") Appendix 1: summary of the modified GRADE system (grades 1A 2D) 1A 1B 1C 1D 2A 2B 2C 2D Strong recommendation High-quality evidence Benefits clearly outweigh risk and burdens, or vice versa Consistent
Appendix 1: summary of the modified GRADE system (grades 1A 2D) 1A 1B 1C 1D 2A 2B 2C 2D Strong recommendation High-quality evidence Benefits clearly outweigh risk and burdens, or vice versa Consistent
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
HIV DIAGNOSTIC TESTS IN LOW- AND MIDDLE-INCOME COUNTRIES: FORECASTS OF GLOBAL DEMAND FOR
 HIV DIAGNOSTIC TESTS IN LOW- AND MIDDLE-INCOME COUNTRIES: FORECASTS OF GLOBAL DEMAND FOR 2015 2020 Presented by Vincent Habiyambere (WHO), Biyi Adesina (Avenir Health) and Meghan Wareham (CHAI) on behalf
HIV DIAGNOSTIC TESTS IN LOW- AND MIDDLE-INCOME COUNTRIES: FORECASTS OF GLOBAL DEMAND FOR 2015 2020 Presented by Vincent Habiyambere (WHO), Biyi Adesina (Avenir Health) and Meghan Wareham (CHAI) on behalf
Adolescents Living with HIV
 Adolescents Living with HIV Gary Reubenson Polokwane 22 August 2015 Conflicts of Interest No relevant conflicts of interest to declare Acknowledgements Karl Technau Lee Fairlie Gill Sorour HIV Clinicians
Adolescents Living with HIV Gary Reubenson Polokwane 22 August 2015 Conflicts of Interest No relevant conflicts of interest to declare Acknowledgements Karl Technau Lee Fairlie Gill Sorour HIV Clinicians
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis. Against the motion
 All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis Against the motion Hermione Lyall Imperial Healthcare NHS Trust, London, UK Acknowledgements: Pat Tookey, Ali Judd, Claire
All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis Against the motion Hermione Lyall Imperial Healthcare NHS Trust, London, UK Acknowledgements: Pat Tookey, Ali Judd, Claire
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
Labor & Delivery Management for Women Living with HIV. Pooja Mittal, DO Lisa Rahangdale, MD
 Labor & Delivery Management for Women Living with HIV Pooja Mittal, DO Lisa Rahangdale, MD Statistics for Perinatally Acquired HIV Timing of Perinatal HIV Transmission Most transmission occurs close to
Labor & Delivery Management for Women Living with HIV Pooja Mittal, DO Lisa Rahangdale, MD Statistics for Perinatally Acquired HIV Timing of Perinatal HIV Transmission Most transmission occurs close to